

Lymphoma & related disorders
Posttransplant lymphoproliferative disorders (PTLD)
PTLD-classic Hodgkin
Authors: Cade Arries, M.D., Elizabeth Courville, M.D.
Editorial Board Member: Roberto N. Miranda, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 20 October 2022
Last staff update: 9 May 2024
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Classical Hodgkin lymphoma PTLD

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Flow cytometry description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Arries C, Courville E. PTLD-classic Hodgkin. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaclassichodgkinptld.html. Accessed December 25th, 2024.
Definition / general
- Lymphoproliferation that fulfills the diagnostic criteria for classic Hodgkin lymphoma and arises in a patient after solid organ or hematopoietic stem cell transplant
- Classification is unaltered in the 2022 International Consensus Classification of Mature Lymphoid Neoplasms (Blood 2022;140:1229)
- In the 5th edition of the World Health Organization Classification of Hematolymphoid Tumors (WHO HAEM), the entity is classified based on a 3 part nomenclature for lymphomas that arise in the setting of immune deficiency / dysregulation (Leukemia 2022;36:1720)
Essential features
- Fulfills the diagnostic criteria for classic Hodgkin lymphoma
- Arises in a patient with a history of solid organ or allogeneic hematopoietic stem cell transplant
- Almost always Epstein-Barr virus (EBV)+
- Very rare; < 5% of all posttransplant lymphoproliferative disorders (PTLD)
ICD coding
- ICD-O: 9650/3 - Hodgkin lymphoma, NOS
Epidemiology
- Very rare; the least common major form of PTLD, accounting for < 5% of all PTLD (Cancer Treat Res 2015;165:305, Leuk Lymphoma 2017;58:633)
- Develops at any age
- Occurs in both solid organ and allogeneic hematopoietic stem cell transplant recipients
- Kidney and liver transplants are most commonly reported in the literature (Pediatr Transplant 2022;26:e14292)
Sites
- Lymph nodes are frequently involved, particularly in pediatric patients
- Less common in the transplanted organ, native solid organs and bone marrow (Am J Med 1989;87:218, Pediatr Transplant 2013;17:E168, Can Respir J 2015;22:144)
Pathophysiology
- PTLDs generally develop as a consequence of immune suppression and decreased T cell immune surveillance
- Classic Hodgkin lymphoma PTLD is almost always an EBV driven proliferation with only rare reports of EBV- (Surg Case Rep 2018;4:72)
- Higher risk among patients who acquire the EBV after organ transplant (Pediatr Transplant 2022;26:e14292)
- Has been reported to arise following diagnosis of polymorphic PTLD (Pediatr Transplant 2013;17:E168, Leuk Lymphoma 2020;61:3319)
- Exact pathophysiology of classic Hodgkin lymphoma PTLD is not entirely understood
Etiology
- PTLD CHL is an EBV driven disease; in chronic cases, elevated viral loads are detected (J Int Med Res 2020;48:300060520948758)
- Subset of cases shows mutations of JAK / STAT and NOTCH1 genes (Front Oncol 2022;11:790481)
Clinical features
- Can include lymphadenopathy, splenomegaly, fever, weight loss, night sweats or pancytopenia
- Patients have a history of solid organ or hematopoietic cell transplant
Diagnosis
- Diagnosis is made on lymph node biopsy (most common), with biopsy of extranodal tissue (less common) and on bone marrow biopsy (rarely)
Prognostic factors
- There are an insufficient number of cases to draw meaningful conclusions
Case reports
- 10 year old girl presented 9 years after kidney transplant (Pediatr Transplant 2004;8:87)
- 15 year old boy presented 6.5 years after polymorphic PTLD, 14.5 years after liver transplant (J Pediatr Hematol Oncol 2007;29:112)
- 16 year old boy presented 8 years after B cell PTLD, 14 years after heart transplant (Pediatr Transplant 2013;17:E168)
- 26 year old woman presented 3.5 years after allogeneic hematopoietic cell transplant (J Clin Exp Hematop 2009;49:45)
- 27 year old man presented 16 years after kidney transplant (Transpl Int 2006;19:338)
- 38 year old man presented 18 years after kidney transplant (Int J Hematol 2018;108:218)
Treatment
- Treatment strategies employed may be similar to those used in classic Hodgkin lymphoma arising in an immunocompetent individual (Evens: Non-Hodgkin Lymphoma - Pathology, Imaging and Current Therapy, 2015)
- Stanford V chemotherapy and radiation led to complete remission in children (Pediatr Blood Cancer 2019;66:e27803, Leuk Lymphoma 2017;58:633)
- EBV specific cytotoxic T lymphocytes (Curr Opin Infect Dis 2021;34:635)
Microscopic (histologic) description
- Resembles mixed cellularity subtype of classic Hodgkin lymphoma
- Effaced architecture or interfollicular pattern
- Variable interstitial fibrosis; less commonly with broad bands of sclerosis or capsular thickening
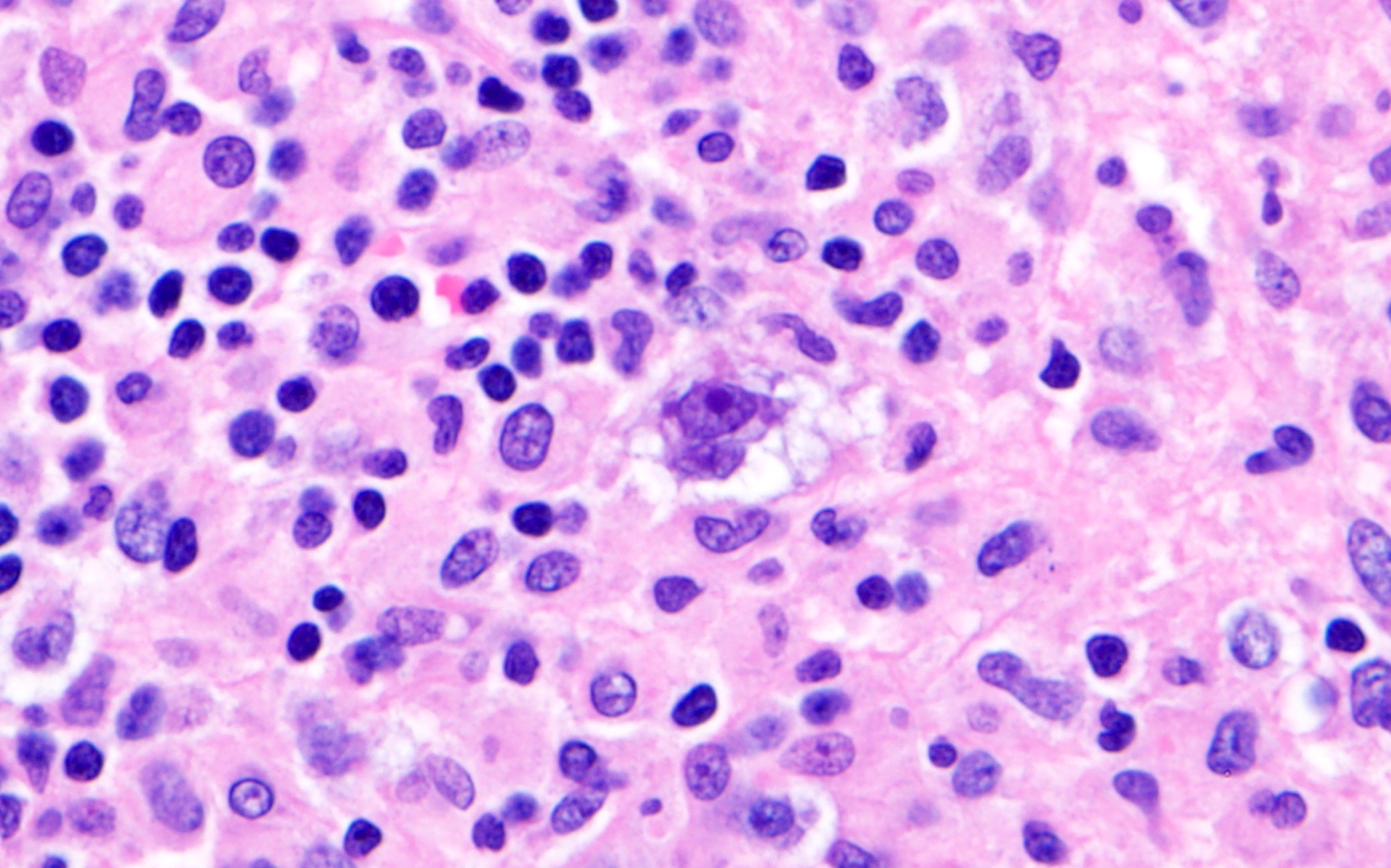
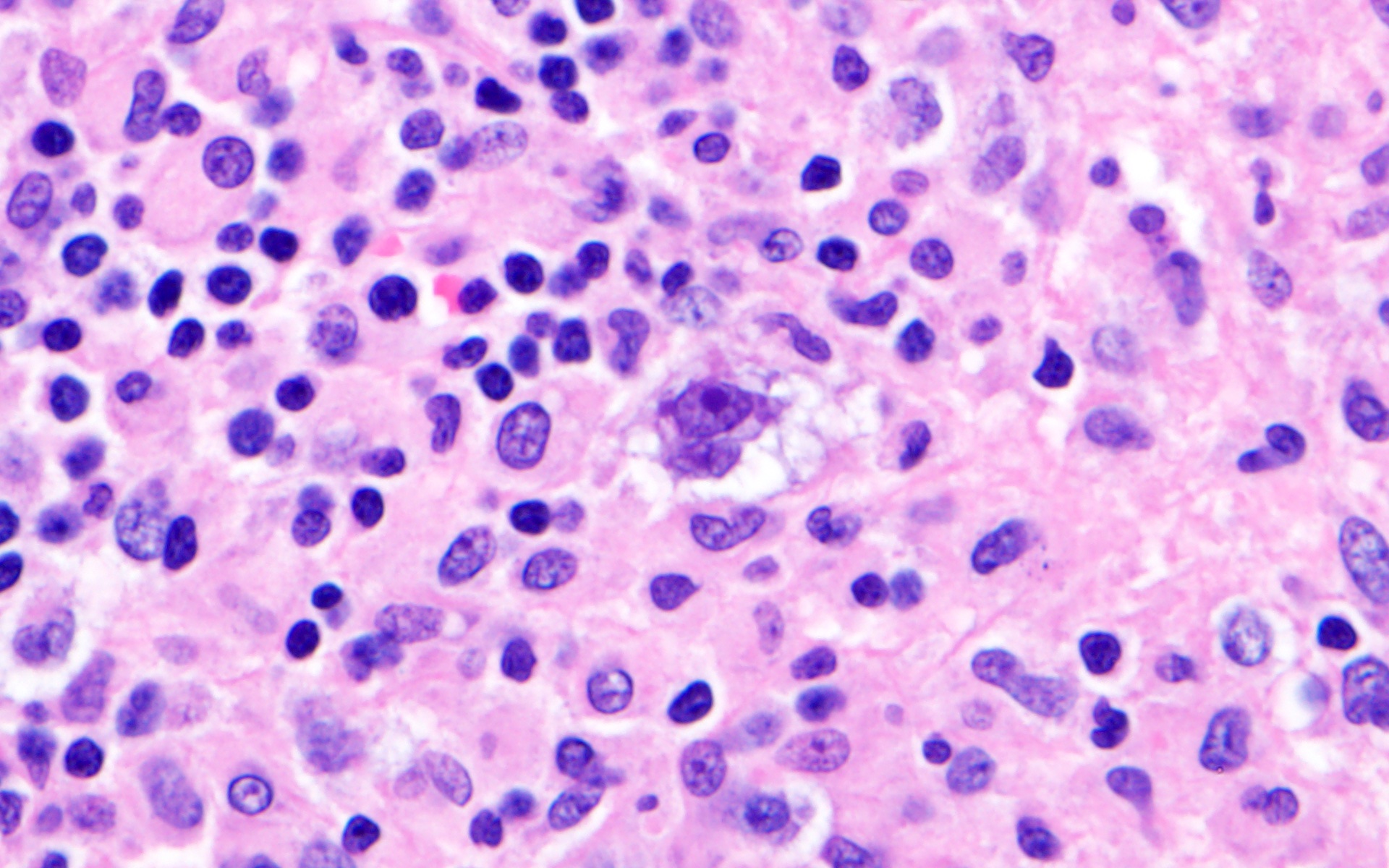
- Typical Hodgkin Reed-Sternberg cells are seen scattered in a mixed inflammatory background of eosinophils, histiocytes, lymphocytes and plasma cells
- Hodgkin Reed-Sternberg cells are large cells with irregular nuclear contours (occasionally bilobed) and frequently with prominent nucleoli
Microscopic (histologic) images
Contributed by Cade Arries, M.D.
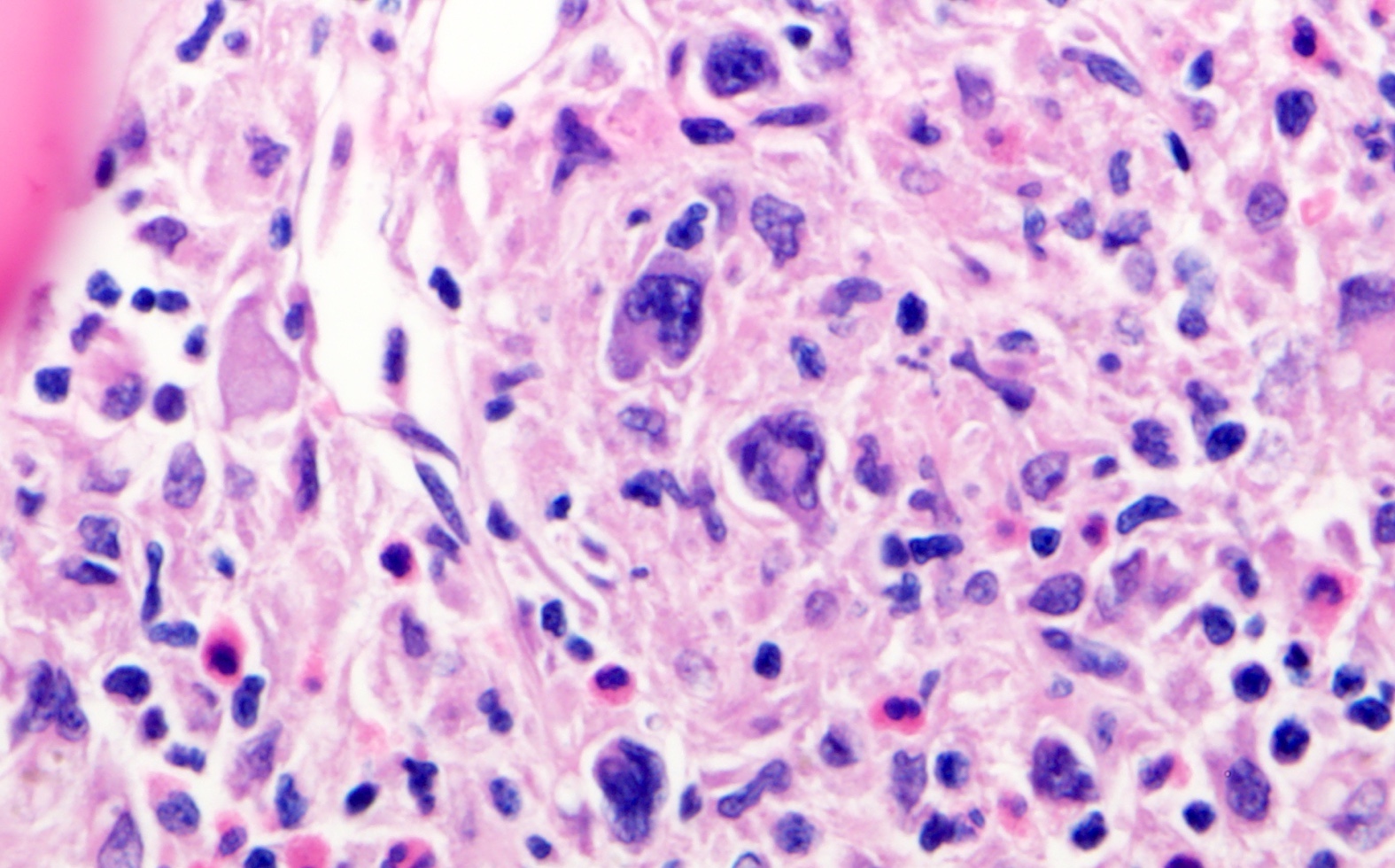
Bone marrow
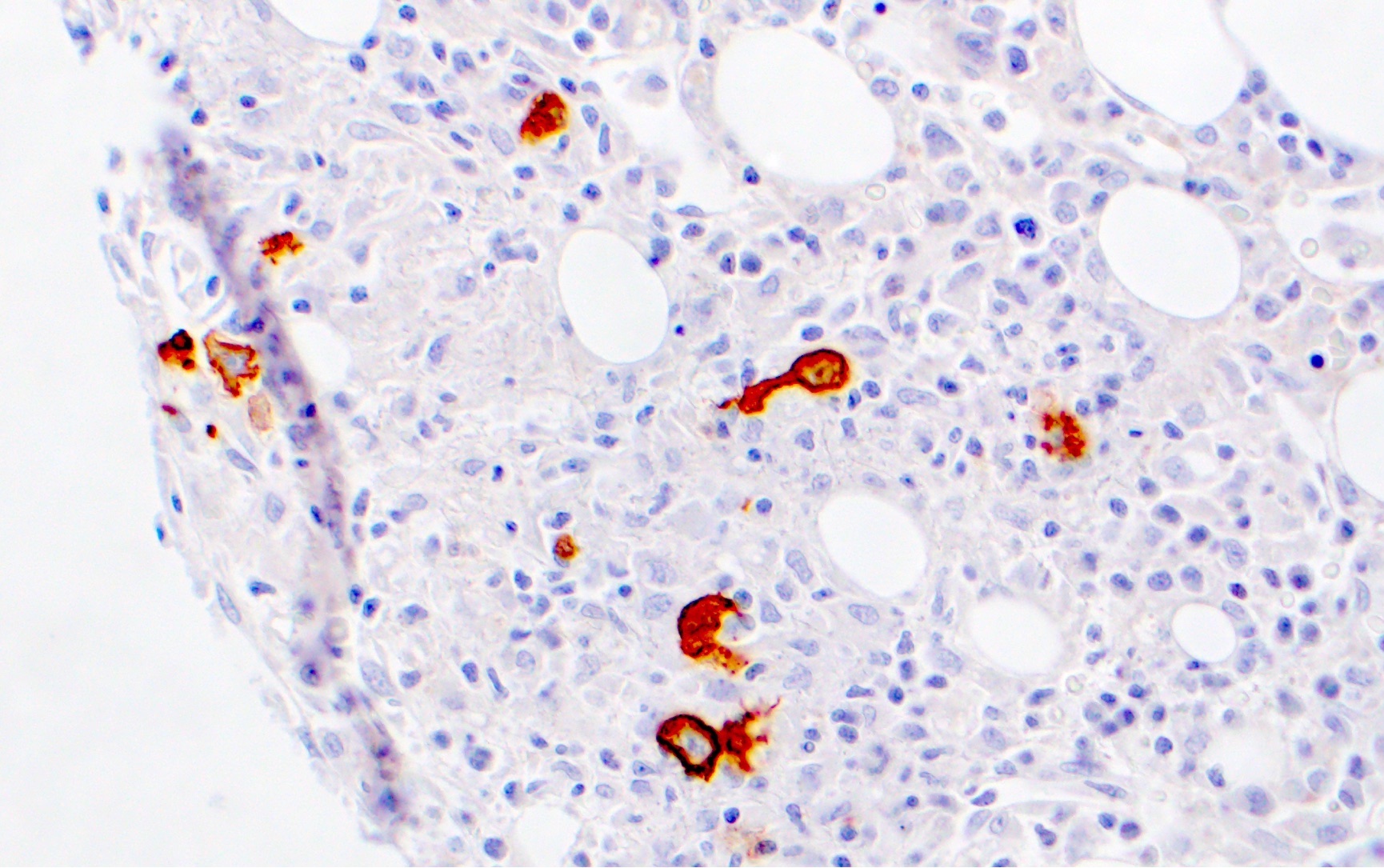
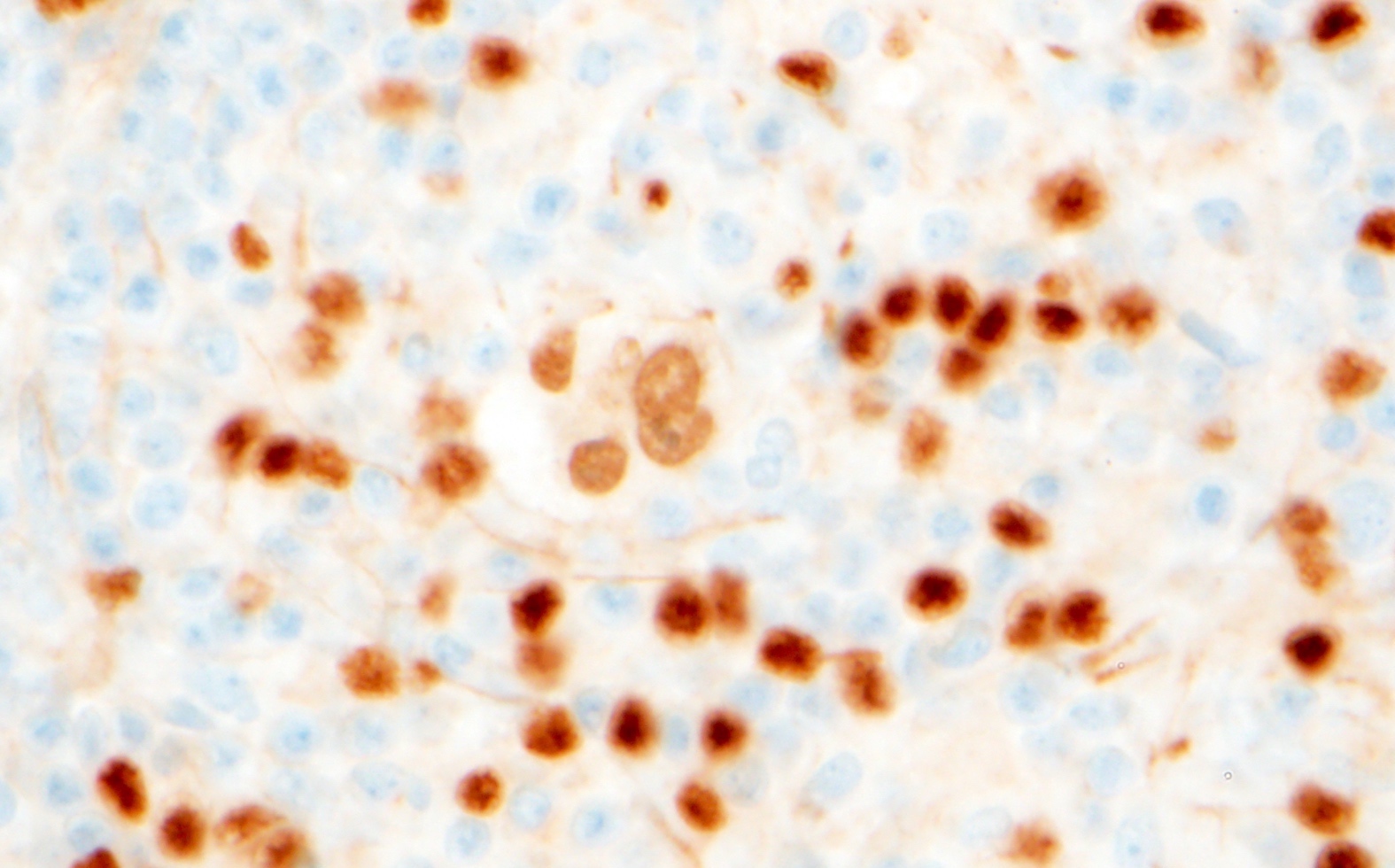
Bone marrow, CD30

Bone marrow, CD15
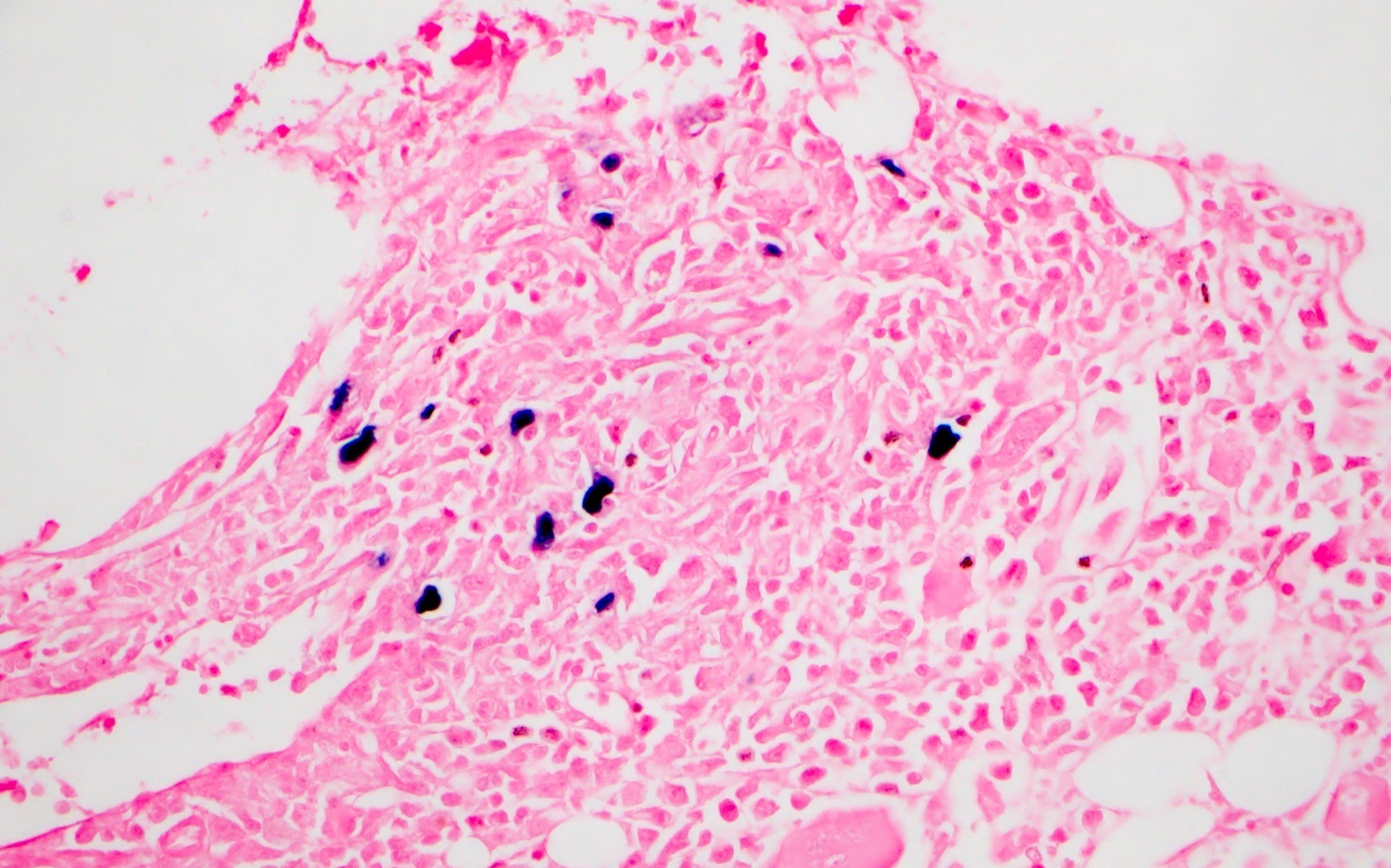
Bone marrow, EBER
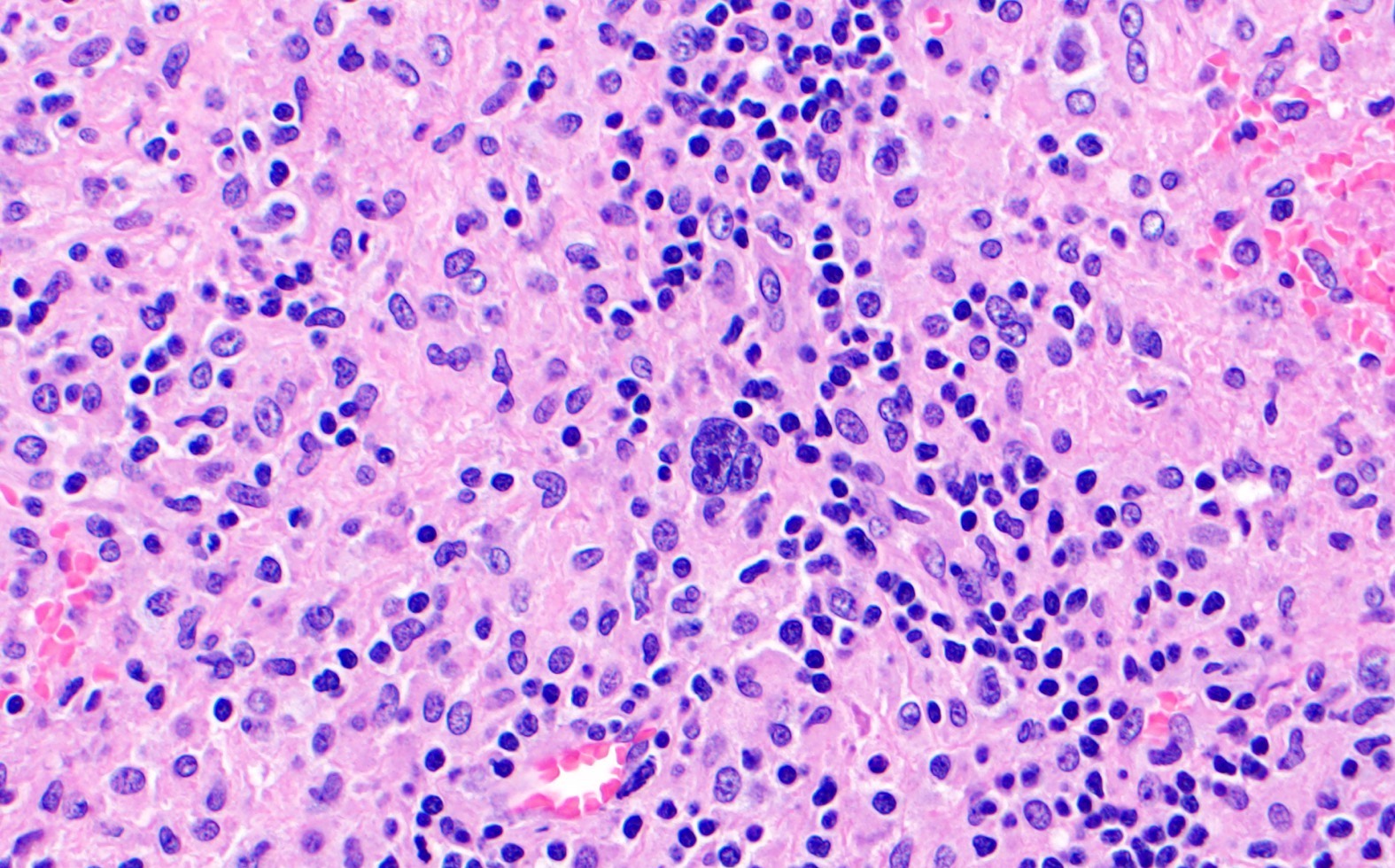
Lymph node
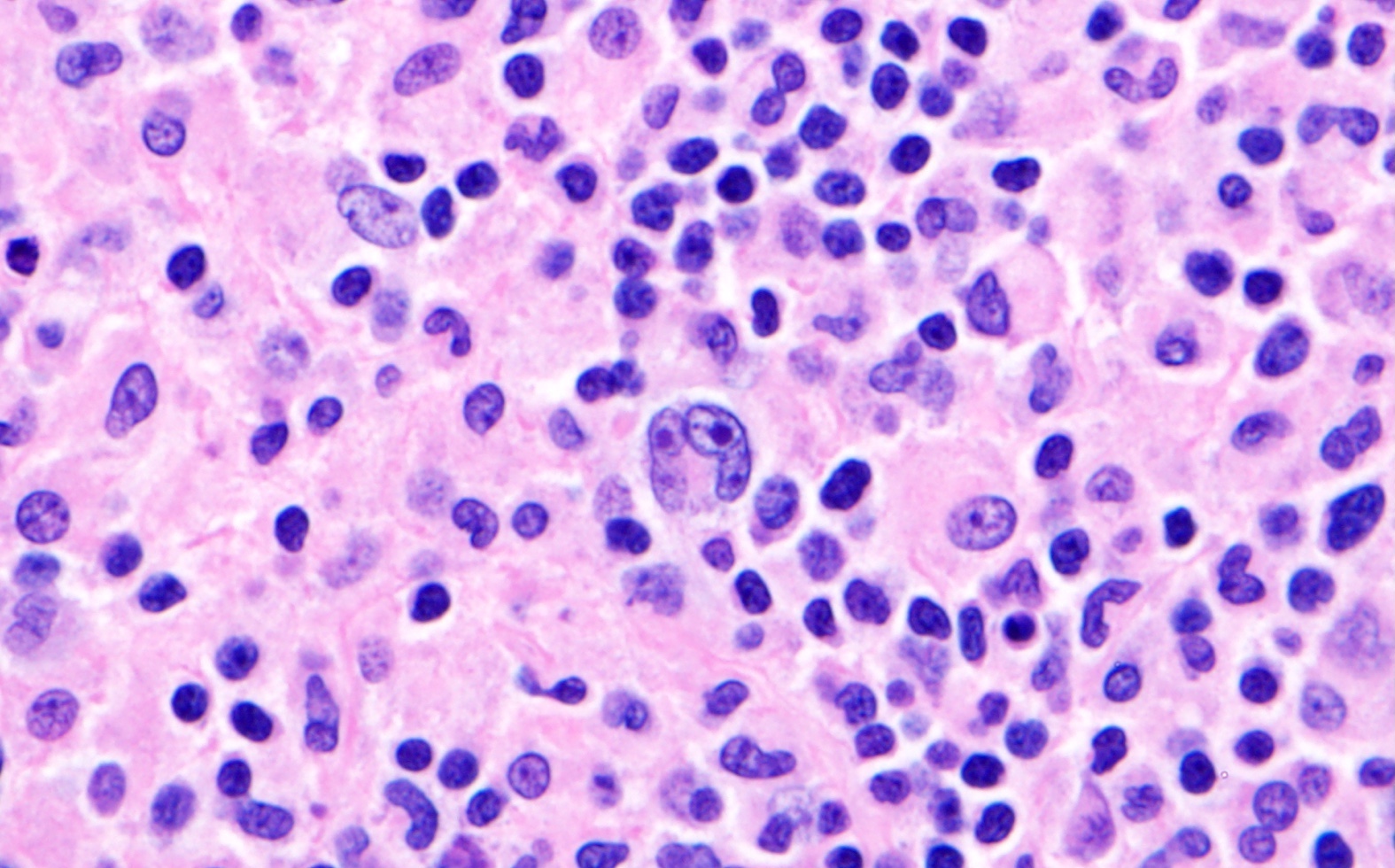
Lymph node

Lymph node, CD15

Lymph node, CD30
Lymph node, PAX5
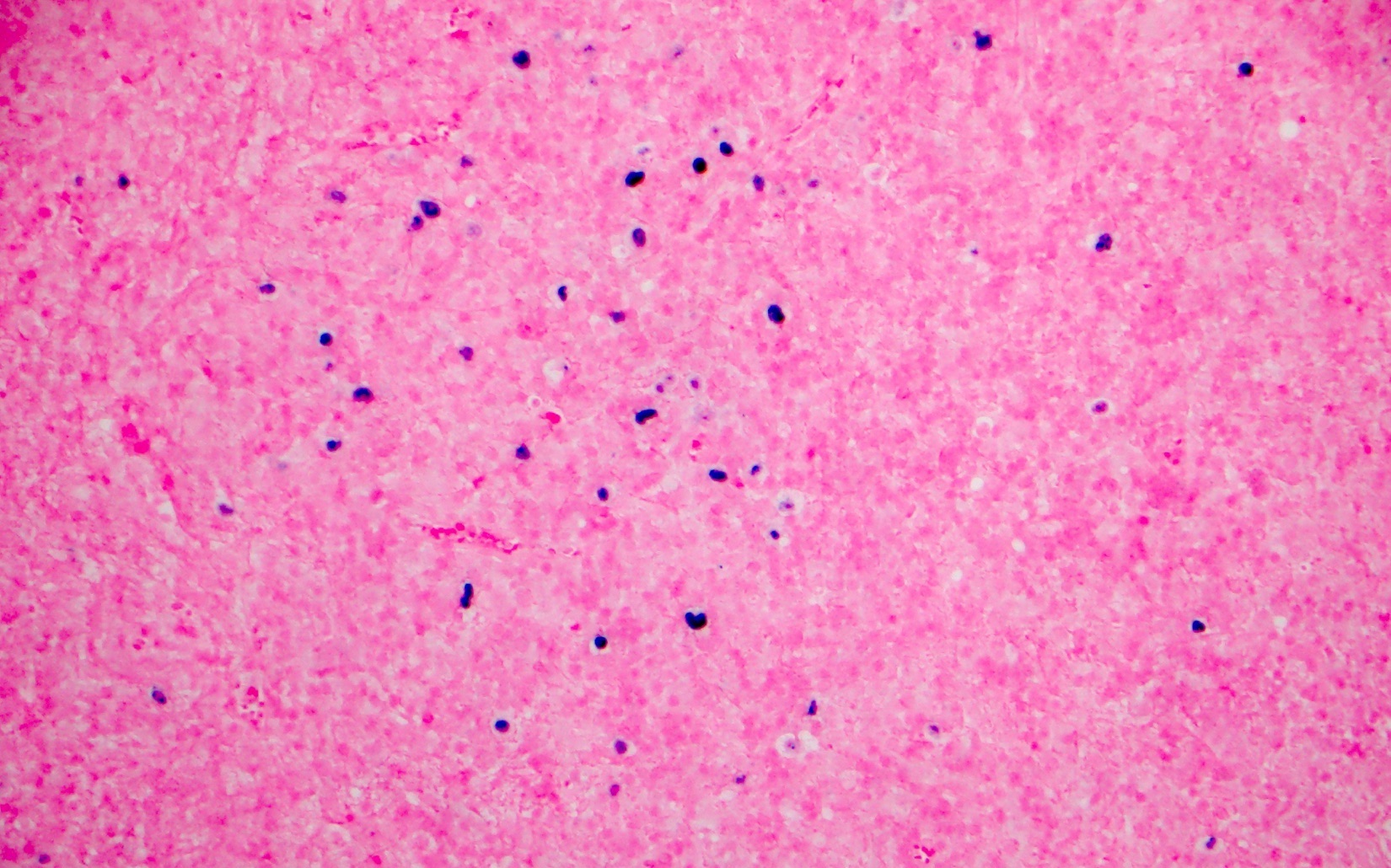
Lymph node, EBER
Positive stains
- In the Hodgkin Reed-Sternberg cells: PAX5 (dim), CD30 and CD15
- B cell markers BOB1, OCT2, CD79a are more commonly expressed in the large neoplastic cells of classic Hodgkin lymphoma PTLD versus classic Hodgkin lymphoma in immunocompetent hosts (100%, 86% and 50% compared with 6%, 14% and 10%, respectively) (Expert Opin Ther Targets 2009;13:1137)
- In situ hybridization for Epstein-Barr virus (EBV) encoded small RNA (EBER1) is almost always positive
Negative stains
Flow cytometry description
- Hodgkin Reed-Sternberg cells are not identified by routine flow cytometric immunophenotyping
- CD4:CD8 ratio of the background T cells may be increased (> 10:1) (Cytometry B Clin Cytom 2019;96:116)
Molecular / cytogenetics description
- Recurrent cytogenetic / oncogene abnormalities are unknown at this time
Sample pathology report
- Lymph node, cervical, excisional biopsy:
- Classic Hodgkin lymphoma posttransplant lymphoproliferative disorder, EBV positive (see comment)
- Comment: The morphologic and immunohistochemical findings fulfill the criteria for classic Hodgkin lymphoma. In this patient with a history of solid organ transplant, the findings are compatible with classic Hodgkin lymphoma posttransplant lymphoproliferative disorder. The Reed-Sternberg cells / variants are EBV+.
Differential diagnosis
- PTLD with some Hodgkin-like features, previously termed Hodgkin-like PTLD in the literature (J Pediatr Hematol Oncol 2007;29:112, Pediatr Dev Pathol 2004;7:348, Pediatr Transplant 2008;12:426):
- Reed-Sternberg-like cells are typically CD15- and CD20+ and associated with background small and intermediate sized EBV+ lymphoid cells
- Such cases are best classified as polymorphic PTLD or monomorphic PTLD depending on their overall features
- EBV+ mucocutaneous ulcer:
- Diagnostic consideration if lesion occurs at a mucocutaneous site (Semin Diagn Pathol 2018;35:236)
- Self limited ulceration of the mucosal or cutaneous surface in a patient with immunosuppression of various etiologies (Clin Lymphoma Myeloma Leuk 2019;19:e81)
- Band-like infiltrate of mature T cells at the base of the lesion
- Hodgkin / Reed-Sternberg-like cells show heterogeneous CD20 expression and are CD30+
- CD15 was negative in Hodgkin / Reed-Sternberg-like cells in series of cases arising after solid organ transplant (Am J Surg Pathol 2014;38:1522)
- Classic Hodgkin lymphoma arising in an immunocompetent individual:
- Microscopic features will be indistinguishable and clinical history is key
Additional references
Board review style question #1
A 45 year old man with a history of renal transplant presented with lymphadenopathy. A lymph node biopsy was performed. A representative image is shown. The large atypical cells are positive for CD30 and CD15 with dim PAX5 nuclear positivity and dim and variable CD20 expression. CD3 and CD45 are negative. What process is suggested by these morphologic and immunohistochemical findings?
- Classic Hodgkin lymphoma
- Diffuse large B cell lymphoma
- Florid follicular hyperplasia
- Polymorphic proliferation
Board review style answer #1
A. Classic Hodgkin lymphoma. The morphologic and immunohistochemical features are diagnostic of classic Hodgkin lymphoma. This is a rare disorder in the posttransplant setting and almost always shows EBV positivity by EBER in situ hybridization in the Reed-Sternberg cells / variants. In the context of solid organ transplantation, the posttransplant status and the presence or absence of viral association is noted in the interpretation. The exact nomenclature depends on the classification system used.
Comment Here
Reference: PTLD-classic Hodgkin
Comment Here
Reference: PTLD-classic Hodgkin
Board review style question #2
Which of the following is expected to be positive in the Hodgkin / Reed-Sternberg cells of classic Hodgkin lymphoma type posttransplant lymphoproliferative disorder (PTLD)?
- ALK1
- CD3
- CD45
- EBER in situ hybridization
Board review style answer #2
D. EBER in situ hybridization. The Hodgkin / Reed-Sternberg cells of classic Hodgkin lymphoma type posttransplant lymphoproliferative disorder are almost always EBV+ by EBER in situ hybridization. The other stains listed are negative.
Comment Here
Reference: PTLD-classic Hodgkin
Comment Here
Reference: PTLD-classic Hodgkin

