
Lymph nodes & spleen, nonlymphoma
Lymph nodes-inflammatory / reactive disorders
Castleman disease

Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Castleman disease lymph nodes

- Unusual heterogeneous group of lymphoproliferative disorders with some common morphological features involving lymph nodes or extranodal sites
- 3 histological types: hyaline vascular variant (HVCD), plasma cell variant (PCCD) and mixed hyaline vascular and plasma cell variant
- 3 distinct clinical entities:
- Unicentric Castleman disease (UCD): localized, stable and exhibiting hyaline vascular morphology (Cancer 1972;29:670)
- Multicentric Castleman disease (MCD): a systemic progressive disease with lymphadenopathy of multiple sites (Cancer 1985;56:2446)
- MCD is divided into idiopathic (iMCD) and human herpesvirus 8 associated (HHV8 MCD) (Blood 1995;86:1276)
- Histologically, most cases show features of plasma cell variant
- Oligocentric or regional Castleman disease: with involvement of 2 or 3 adjacent lymph node regions and clinical course like UCD (Blood Adv 2020;4:6039)
- Unusual heterogeneous group of lymphoproliferative disorders with some common morphological features involving lymph nodes or extranodal sites
- 3 distinct clinical entities: unicentric Castleman disease (UCD), multicentric Castleman disease (MCD) and oligocentric or regional Castleman disease
- MCD is divided into idiopathic (iMCD) and human herpesvirus 8 associated (HHV8 MCD)
- 3 histological types: hyaline vascular variant (HVCD), plasma cell variant (PCCD) and mixed hyaline vascular and plasma cell variant
- Clinical syndromes associated with MCD POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein spike, skin changes) and MCD TAFRO (thrombocytopenia, anasarca, fever, reticulin fibrosis, organomegaly)
- Castleman disease can show predisposition to certain neoplasms
- Angiofollicular hyperplasia
- Giant lymph node hyperplasia
- Unicentric Castleman disease (UCD)
- Multicentric Castleman disease (MCD)
- Idiopathic (iMCD)
- Human herpesvirus 8 associated (HHV8 MCD)
- Alternative / older terminology: Kaposi sarcoma herpesvirus associated (KSHV MCD)
- Hyaline vascular type (HVCD)
- Plasma cell type (PCCD)
- MCD POEMS (polyneuropathy, organomegaly, endocrinopathy, M protein spike, skin changes)
- MCD TAFRO (thrombocytopenia, anasarca, fever, reticulin fibrosis, organomegaly)
- ICD-10: D47. Z2 - Castleman disease
- UCD can affect all age groups and shows no gender difference with the median age of onset in the fourth decade (Hematol Oncol Clin North Am 2018;32:1)
- MCD affects patients of all ages with a median age of onset in the fifth to seventh decades
- HHV8 MCD affects mainly HIV positive individuals; however, individuals who are immunocompromised from other causes can also be affected (Leuk Lymphoma 2015;56:1252)
- HHV8 MCD in individuals who are HIV negative accounts for 2 - 50% of cases and this variation depends on the prevalence of HHV8 in the region (Blood 2020;135:1353)
- With the introduction of antiretroviral therapy (ART), the incidence of HHV8 MCD has increased
- Complex interplay between HIV and HHV8 and immune dysregulation of patients with HIV controlled by ART is thought to cause this increased incidence (Ann Oncol 2009;20:775)
- UCD is more common in childhood (75%) than iMCD and only rare cases of HHV8 MCD are reported in children (Pediatrics 2012;129:e199, Pediatr Blood Cancer 2019;66:e27613)
- UCD most commonly affects mediastinum; extrathoracic sites are also involved
- Presents as a solitary lymph node mass
- MCD affects multiple lymph node sites, predominantly in the cervical region
- Reference: Surg Pathol Clin 2019;12:849
- Etiopathogenesis remains not well known
- UCD
- Recent evidence suggests that UCD may be a neoplastic process involving follicular dendritic cells (Mod Pathol 2014;27:823)
- Among UCD patients, 17% have shown to harbor mutations in the gene PDGFRB encoding platelet receptor growth factor β (Leukemia 2019;33:1035)
- iMCD
- iMCD is proposed to involve autoinflammatory or autoimmune diseases, paraneoplastic syndromes or an unidentified viral infection leading to polyclonal lymphoproliferation and hypercytokinemia (Blood 2014;123:2924)
- Current concept is that a cytokine storm due to increased production of IL6 is associated with Castleman disease since patients have elevated levels of IL6 and symptoms improve with IL6 suppression (N Engl J Med 2020;383:2255)
- VEGF, IL1, IL2, CXCL13 and TNF have also been shown to play a role in the pathogenesis of iMCD (Blood 1994;83:2587, Br J Haematol 1999;104:482, Am J Hematol 2018;93:902)
- T cell activation, and activation of mTOR, JAK / STAT3 and type I interferon signaling pathways also thought to be pathogenetic mechanisms (J Clin Invest 2019;129:4451, Blood 2020;135:1673)
- HHV8 MCD
- HHV8 MCD occurs in HIV positive or negative individuals infected with HHV8 (Blood 2001;97:2130)
- HHV8 infected B cells in the mantle zones show expression of IgM lambda immunogobulins
- This is by the loss of Ig kappa due to the upregulation of V(D)J recombination mediated by RAG protein and Ig lambda expression by B lymphocytes with HHV8 infection (PLoS Pathog 2018;14:e1006967)
- HHV8 encodes several viral genes; the resulting viral proteins and microRNAs stimulate cell growth, proliferation and cell survival among the infected cells, as well as among the neighboring cells by a paracrine mechanism (J Clin Invest 2016;126:3165)
- HHV8 viral lytic protein expression is proposed to be the contributing pathobiological factor of HHV8 MCD (Am J Pathol 2000;156:743)
- High viral load in patients with HHV8 MCD suggests active viral replication (Blood 2000;96:2069)
- HHV8 viral protein vIL6 is expressed in high levels in plasmablasts surrounding lymphoid follicles (J Virol 1999;73:4181)
- Additionally, human cytokines are elevated in patients with HHV8 MCD, which is thought to be driven by the virus (Blood 2013;122:4189)
- Inflammatory cytokines like hIL6 and vIL6 cause anemia, fever and hypoalbuminemia (Blood 2013;122:4189)
- UCD: etiology is unclear
- iMCD: etiology is unclear
- HHV8 MCD: HHV8 infected endothelial cell proliferation and vascularization
- UCD: asymptomatic or an enlarging lymph node or mass; secondary symptoms related to the mass (compression or pain) (Blood 2020;135:1353)
- MCD: all subtypes of MCD show systemic inflammatory manifestations including fever, weight loss, anasarca, generalized lymphadenopathy and hepatomegaly
- Anemia, hypoalbuminemia, cytopenias and elevated inflammatory markers are common (Blood Adv 2021;5:1660)
- MCD POEMS: a syndrome characterized by peripheral neuropathy, organomegaly, skin changes and monoclonal paraproteins occurs in some patients with MCD (Blood 1994;83:2587)
- MCD TAFRO: another syndrome characterized by thrombocytopenia, ascites, fever, reticulin fibrosis and organomegaly usually in patients with normal immunoglobulin levels and mixed or hyaline vascular histology (Sci Rep 2017;7:42316)
- iMCD, NOS: shows elevated platelet counts and immunoglobulin levels and plasmacytic histology (Blood 2020;135:1353)
- Excisional biopsy of an affected lymph node with histopathological examination is the diagnostic modality of choice
- 18F fluorodeoxyglucose positron emission tomography (FDG PET) is used to exclude alternative diagnoses; also used to select the lymph node for biopsy (J Infect Dis 2015;212:1250)
- HHV8 MCD requires the pathologic features and HHV8 positivity
- iMCD is confirmed by integration of pathological findings and clinical syndrome; a diagnosis of iMCD requires exclusion of infectious, malignant and autoimmune disorders that can mimic iMCD (Blood 2017;129:1646)
- UCD: usually no laboratory abnormalities
- MCD subtypes: anemia, hypoalbuminemia, renal dysfunction and liver dysfunction, dysregulation of IL6 (increased) or other cytokines like VEGF, IL1 and TNFα (Nat Rev Dis Primers 2021;7:84)
- MCD TAFRO: thrombocytopenia (Hematol Oncol Clin North Am 2018;32:37)
- MCD: 18F FDG PET / CT shows increased uptake in the affected lymph nodes
- Lymph nodes are nonconfluent with a symmetric pattern and SUV ranging from 2 - 19
- Extramedullary involvement is demonstrated as pulmonary cysts, nodules and interstitial lung disease, hypermetabolic activity in spleen and bone marrow (Nucl Med Commun 2021;42:833)
Images hosted on other servers:

18F FDG PET / CT, HHV8 MCD
- UCD: localized and excellent response to therapy
- MCD: poorer prognosis, especially HIV positive patients and patients with MCD POEMS (Surg Pathol Clin 2019;12:849)
- Predilection for association with neoplasms (Surg Pathol Clin 2019;12:849, Blood 2020;135:1353, Indian J Pathol Microbiol 2021;64:302, Infection 2021;49:945)
- HVCD
- Follicular dendritic cell sarcoma
- Vascular tumors
- HHV8 MCD
- Kaposi sarcoma
- HHV8+ large B cell lymphoma
- Primary effusion lymphoma
- iMCD
- Classic Hodgkin lymphoma
- Diffuse large B cell lymphoma
- Mantle cell lymphoma
- Peripheral T cell lymphoma
- HVCD
- Other
- HVCD can develop indolent T lymphoblastic proliferations
- 26 year old woman with Castleman disease with AA amyloidosis (Medicine (Baltimore) 2020;99:e18978)
- 26 year old pregnant woman with Castleman disease and pemphigus (Medicine (Baltimore) 2021;100:e24990)
- 32 and 43 year old women with Castleman disease with spondyloarthritis treated with TNF alpha antagonist (Joint Bone Spine 2020;87:655)
- 35 year old woman with glycolytic hypermetabolism in Castleman disease by 18F FDG PET / CT (Clin Nucl Med 2020;45:868)
- 52 year old man with Castleman disease presenting as a chylous pleural effusion (Pathol Res Pract 2020;216:153209)
- 53 year old man with retroperitoneal mass (Int J Surg Case Rep 2020;70:24)
- 60 year old man with a hepatic mass and autoimmunity (Cancer Imaging 2019;19:53)
- 62 year old man with hypermetabolic mass of kidney (Clin Nucl Med 2021;46:510)
- 64 year old woman with multicentric Castleman disease and cryoglobulinemic vasculitis (J Dermatol 2021;48:e474)
- 82 year old woman with Castleman disease and eosinophilic dermatosis (Int J Dermatol 2020;59:e416)
- UCD
- Asymptomatic patients: expectant management and follow up for disease progression; resection
- Symptomatic patients: complete surgical resection (Br J Haematol 2021;195:328)
- Unresectable symptomatic UCD: volume reduction by debulking resection, embolization or cryoablation of feeding vessels, rituximab, steroids and radiation therapy and follow up evaluation is recommended to determine the possibility of complete resection (Br J Haematol 2021;195:328, Eur J Haematol 2021;107:484)
- MCD
- Asymptomatic patients: no therapeutic intervention but follow up is needed to detect disease progression
- Symptomatic patients: depending on the presentation and disease driver (Br J Haematol 2021;195:328)
- HHV8 MCD
- Antiretroviral therapy with HHV8 MCD specific therapy
- Cytotoxic chemotherapies are used: etoposide, vincristine, vinblastine, cyclophosphamide and liposomal doxorubicin
- Chemotherapy is used in combination with rituximab
- Antiherpesvirus therapy: gancyclovir, zidovudine, valganciclovir, pomalidomide
- Anti-hIL6 therapy: siltuximab and tocilizumab are under trial (Br J Haematol 2021;195:328)
- MCD POEMS
- Therapy for the plasma cell dyscrasia: consolidation with autologous stem cell transplant
- Patients without clonal plasmacytosis in bone marrow: radiation therapy
- Patients with disseminated bone marrow involvement: systemic chemotherapy followed by adjuvant radiation; melphalan and dexamethasone, cyclophosphamide dexamethasone, lenalidomide, thalidomide and bortezomib
- Daratumumab, BCMA CAR-T, bevacizumab (anti-VEGF), interferon alpha, tamoxifen, transretinoic acid, ticlopidine, argatroban and strontium 89 are also used in rare cases
- iMCD
- Surgery, steroids, rituximab, combination chemotherapy (CHOP [cyclophosphamide, doxorubicin, vincristine (Oncovin), prednisolone] or CVAD [cyclophosphamide, vincristine, adriamycin, etoposide]-like regimens and VDTPACE [Velcade (bortezomib), dexamethasone, thalidomide, cisplatinum, adriamycin, cyclophosphamide, etoposide]), autologous stem cell transplantation, anti-IL6 monoclonal antibodies (siltuximab and tocilizumab), bortezomib, thalidomide, anakinra (IL1 antagonist), interferon alpha and all transretinoic acid are used (Hematol Oncol Clin North Am 2018;32:89, Blood 2018;132:2115)
- MCD TAFRO
- Corticosteroids, rituximab, tocilizumab, cyclosporin A
- Thrombocytopenia: romiplostim and eltrombopag
- Other options: plasma exchange, high dose cyclophosphamide, thalidomide, lenalidomide, bortezomib rapamycin and combination chemotherapy such as CHOP (cyclophosphamide, doxorubicin, vincristine and prednisolone) (Ann Hematol 2022;101:485, Int J Hematol 2016;103:686)
- HHV8 MCD
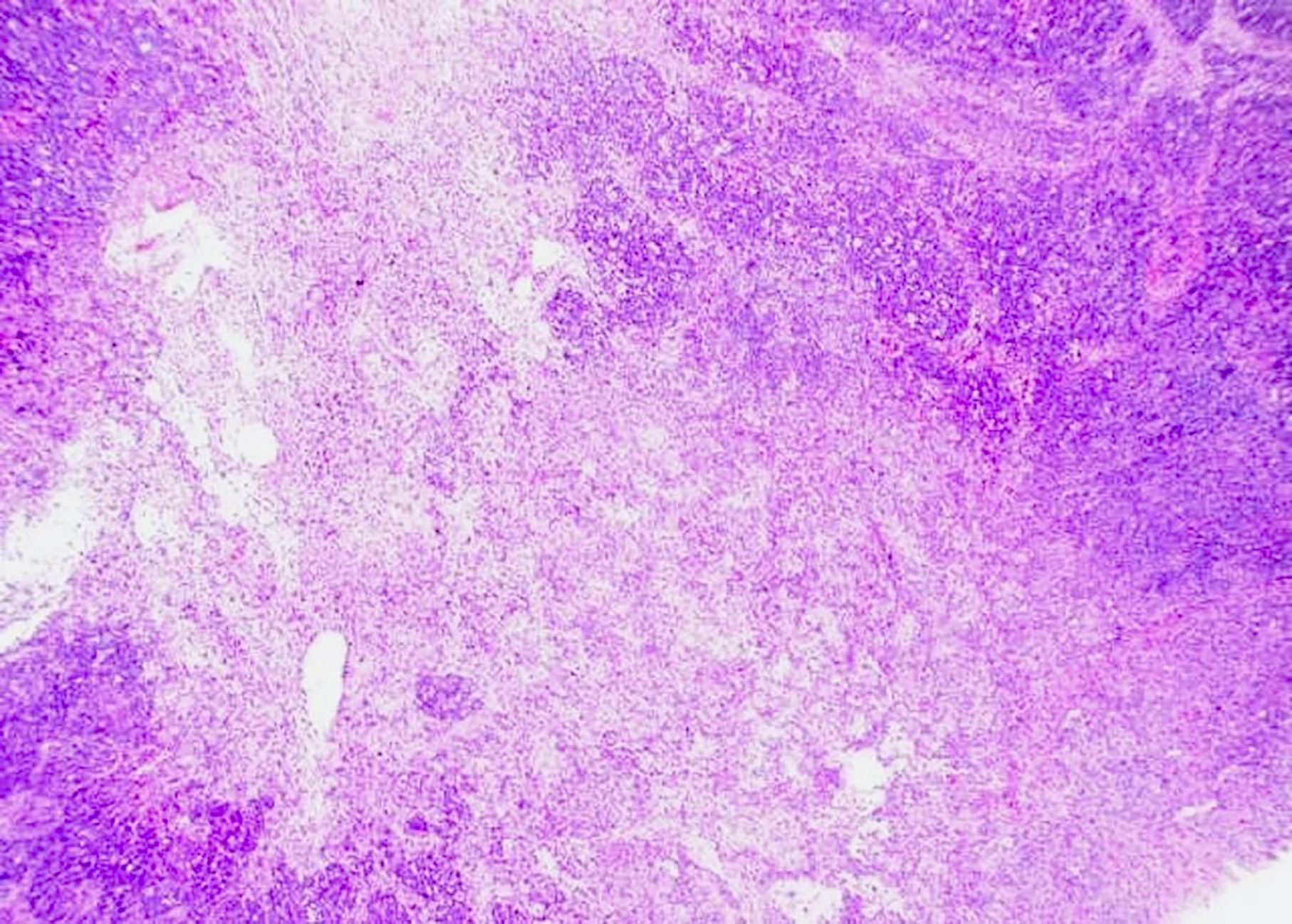
- UCD: enlarged lymph node, firm and white cut surface with or without calcification
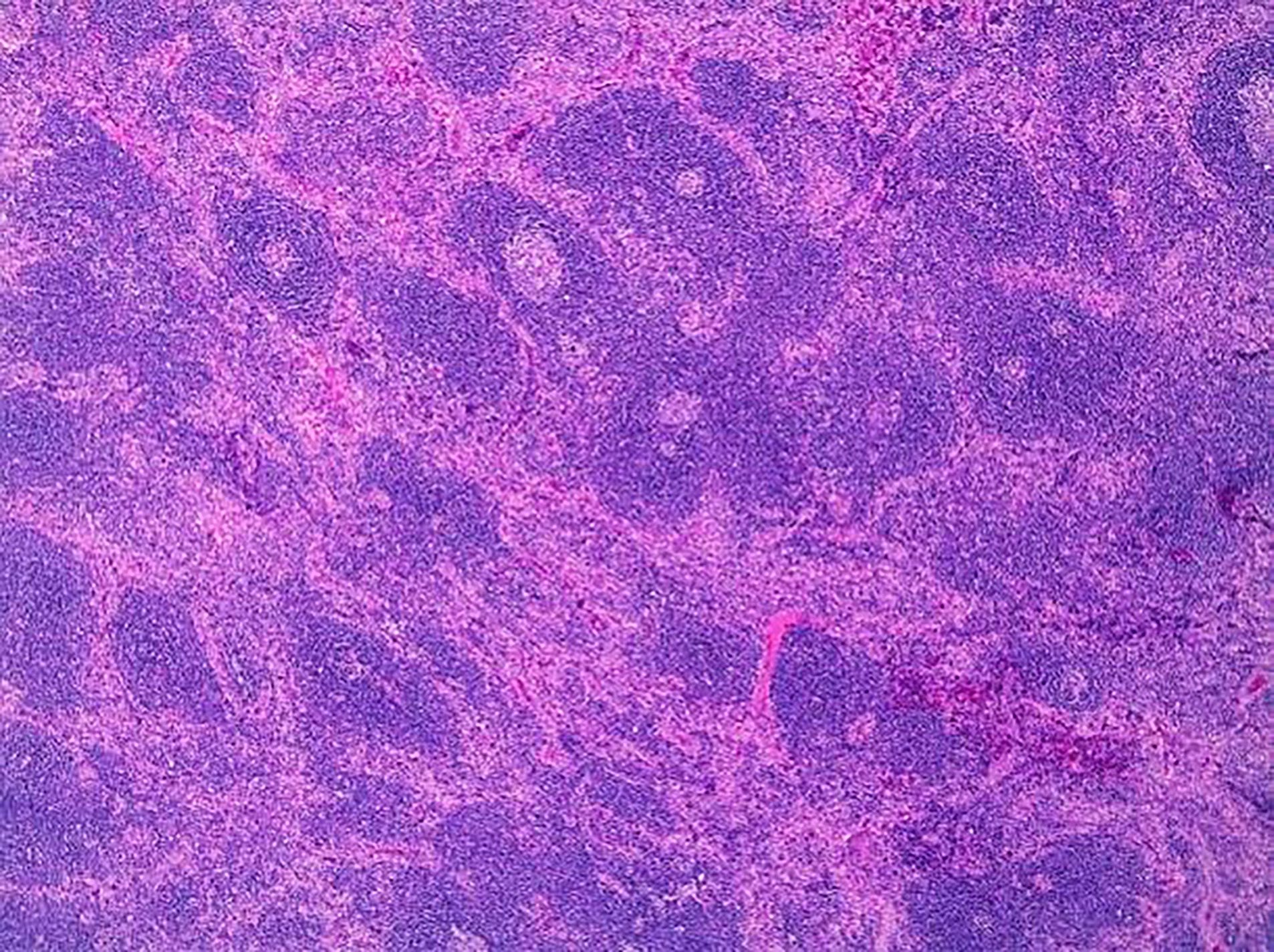
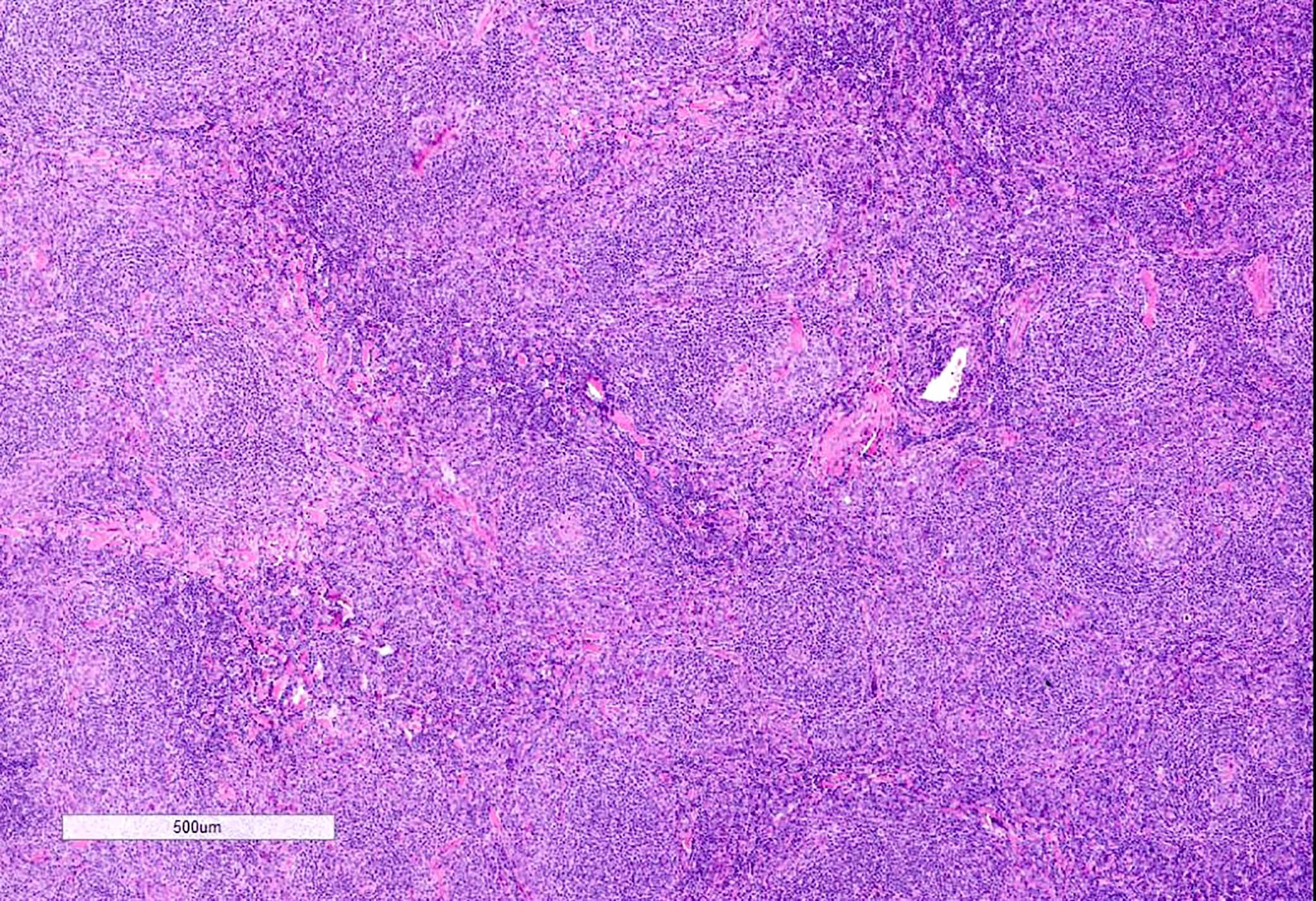
- HVCD is characterized by prominent vascular proliferation and hyalinization of the vessel walls
- There are follicular changes and interfollicular / stromal changes described; based on the predominance of changes in each of these sites divided into follicular HVCD and stroma rich Castleman disease (Virchows Arch A Pathol Anat Histopathol 1993;423:369)
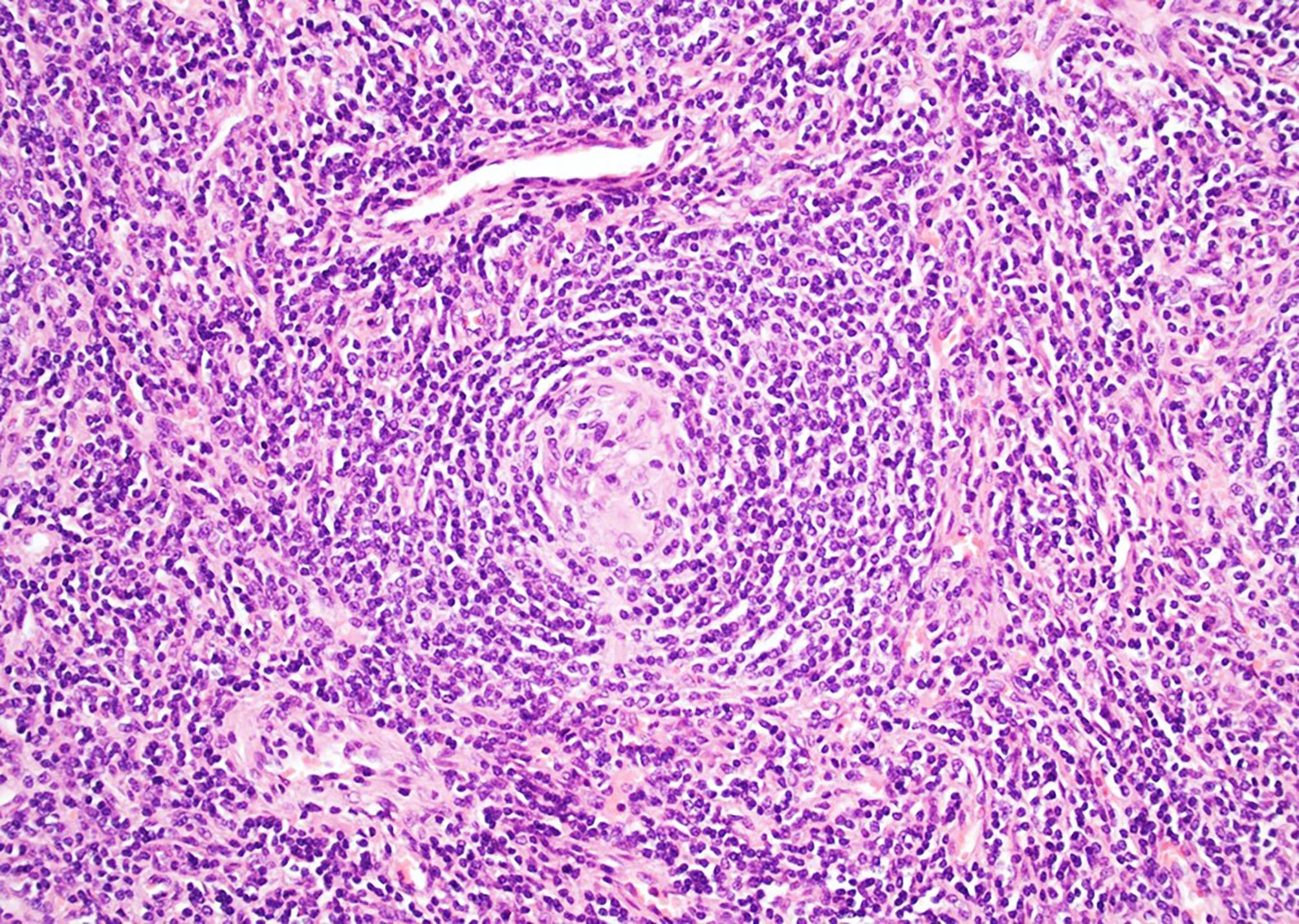
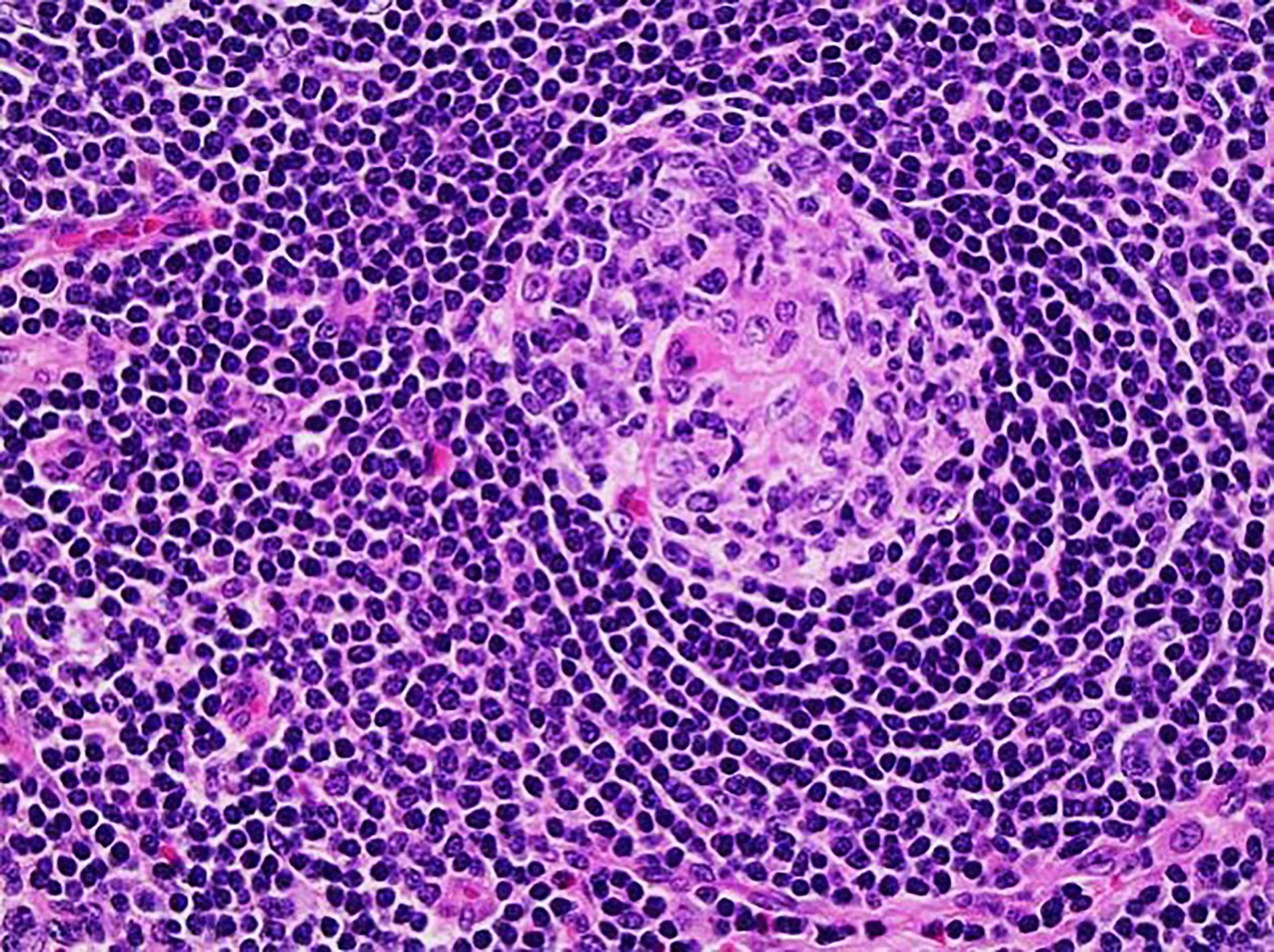
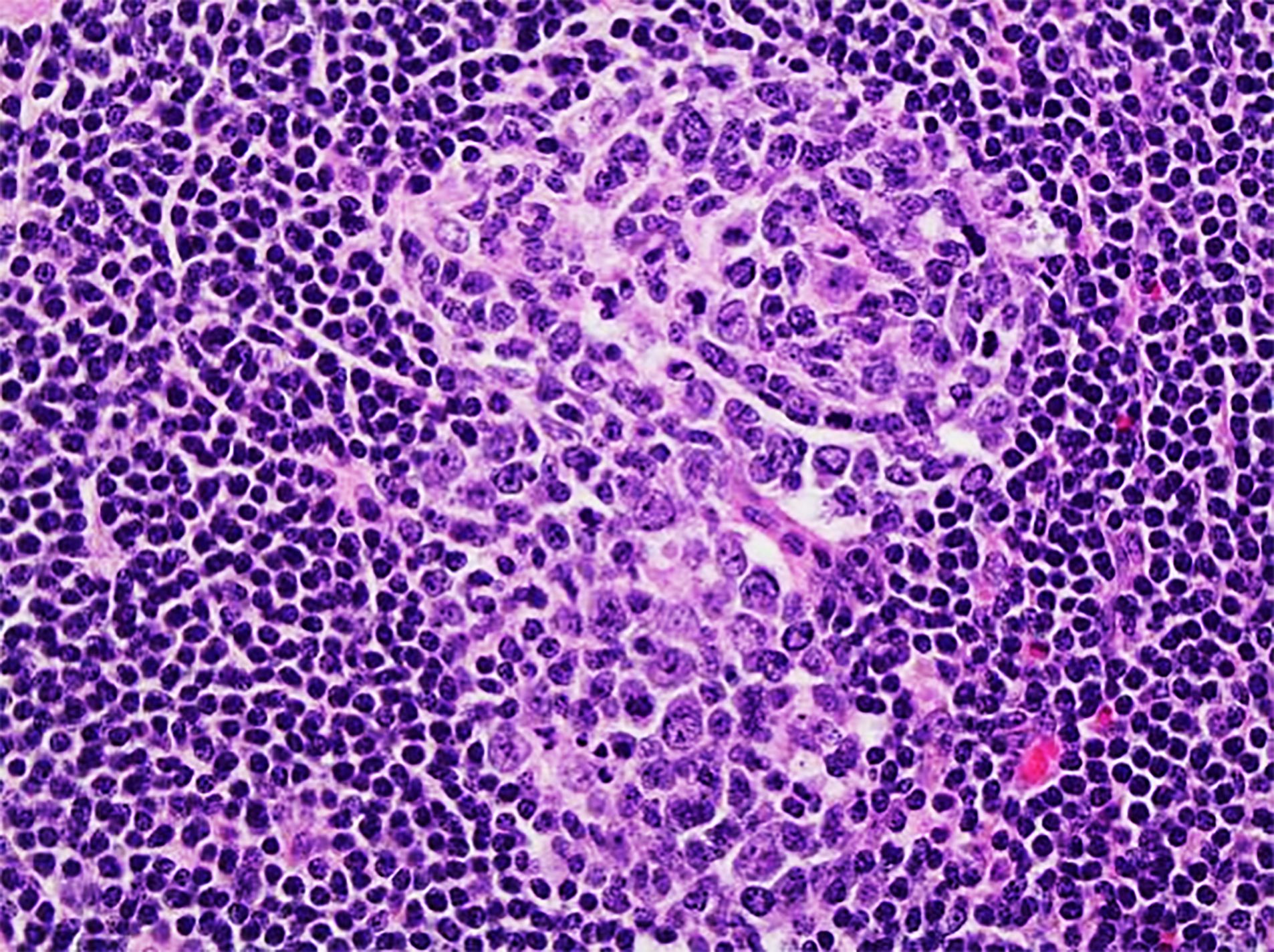
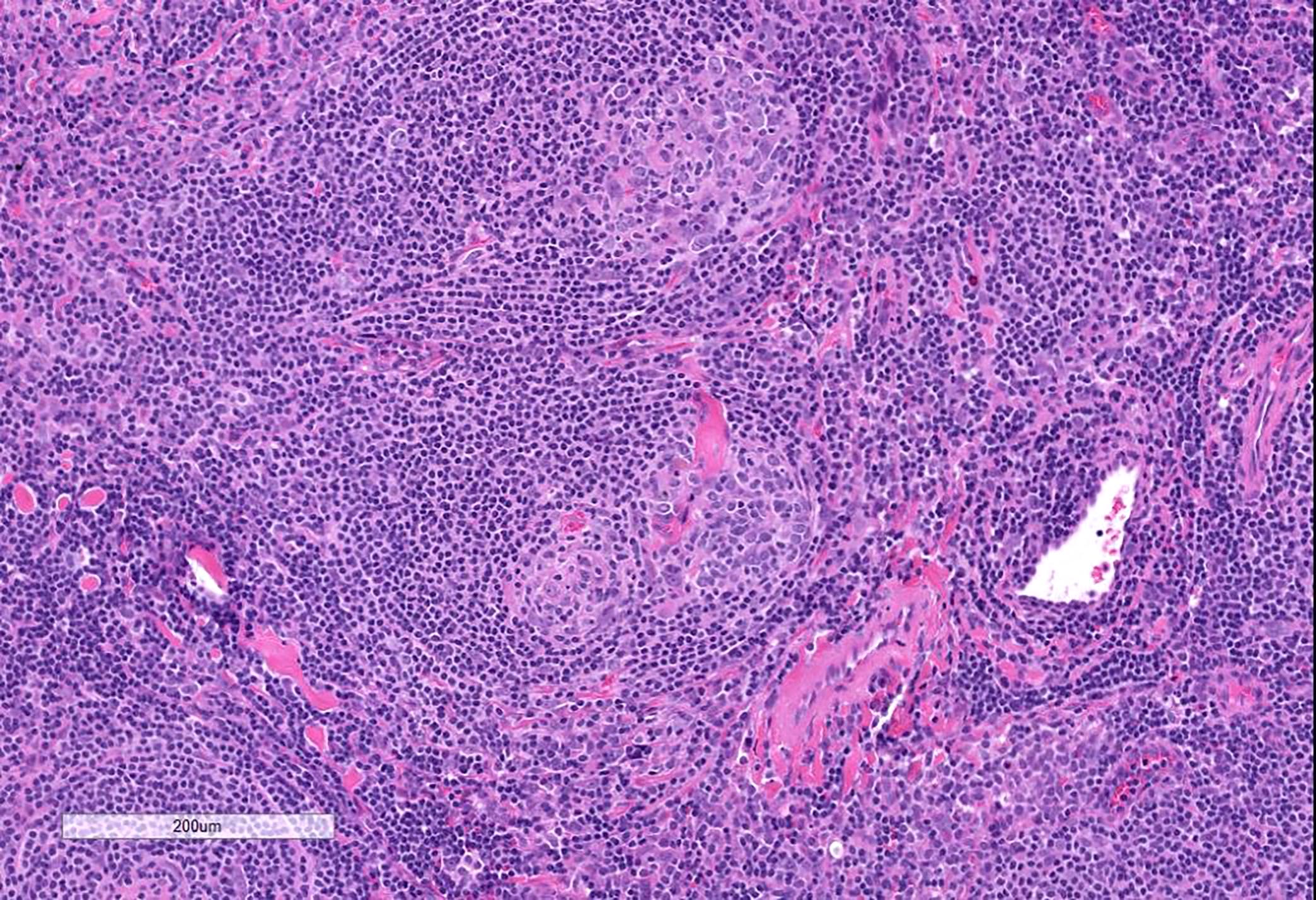
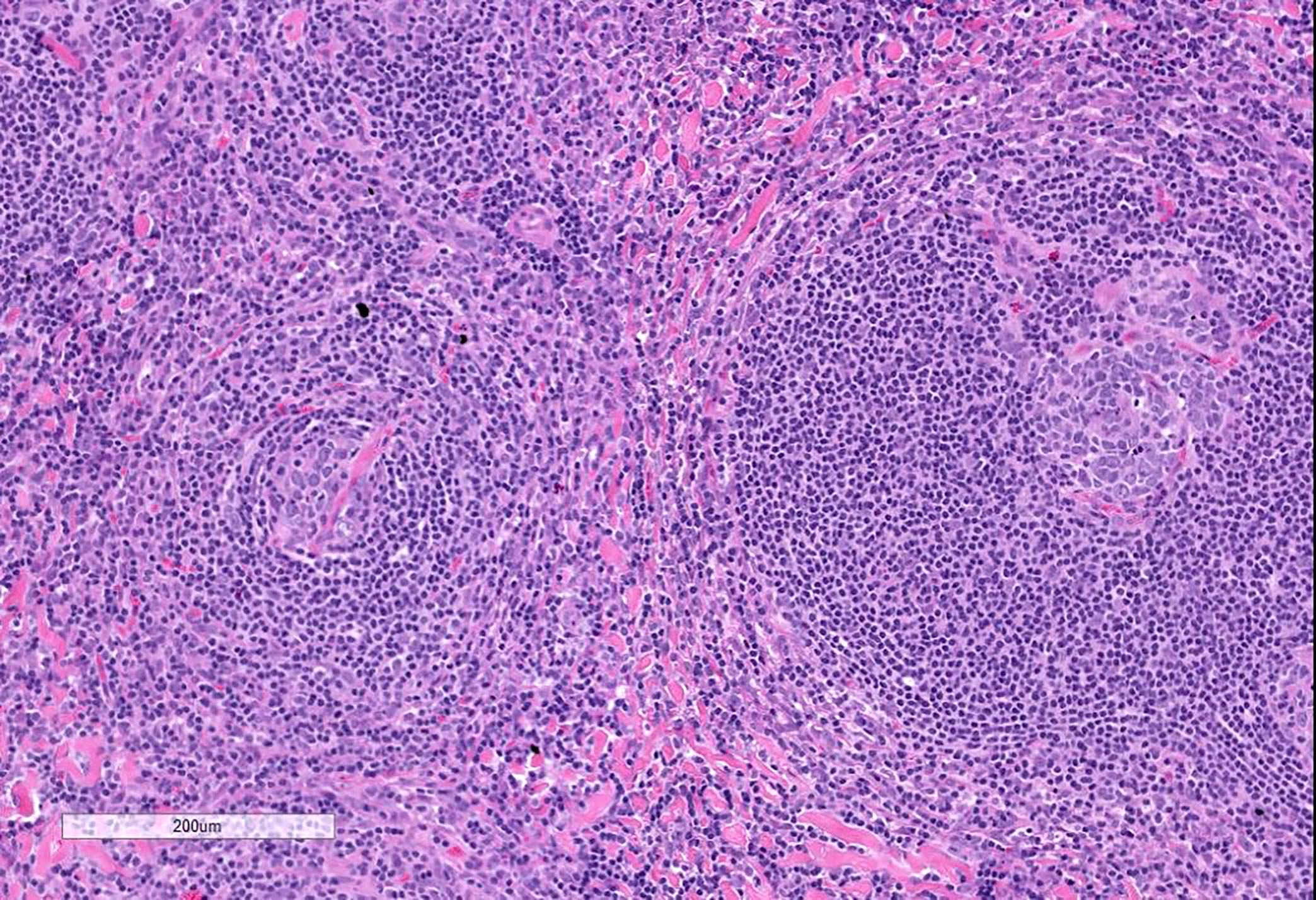
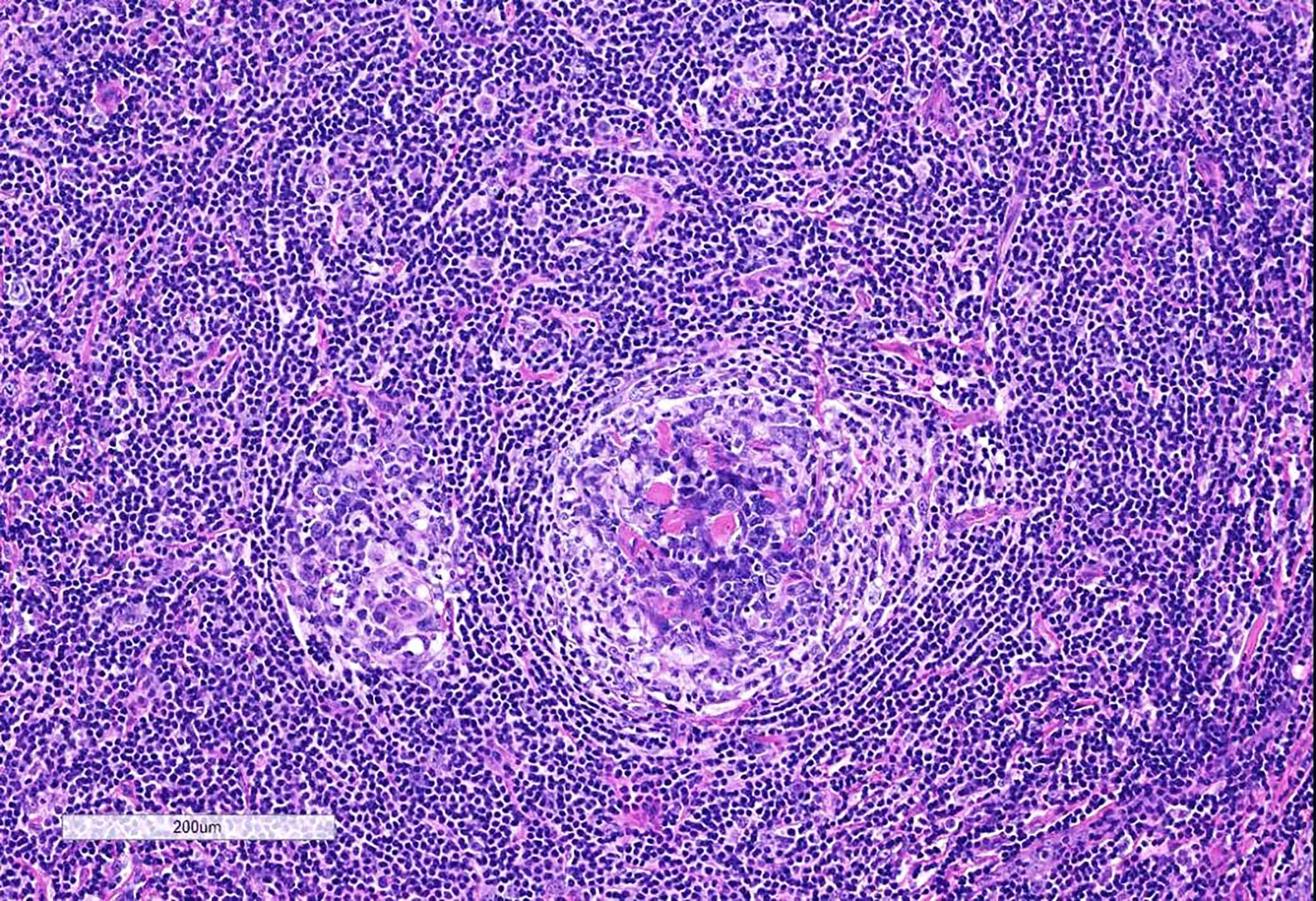
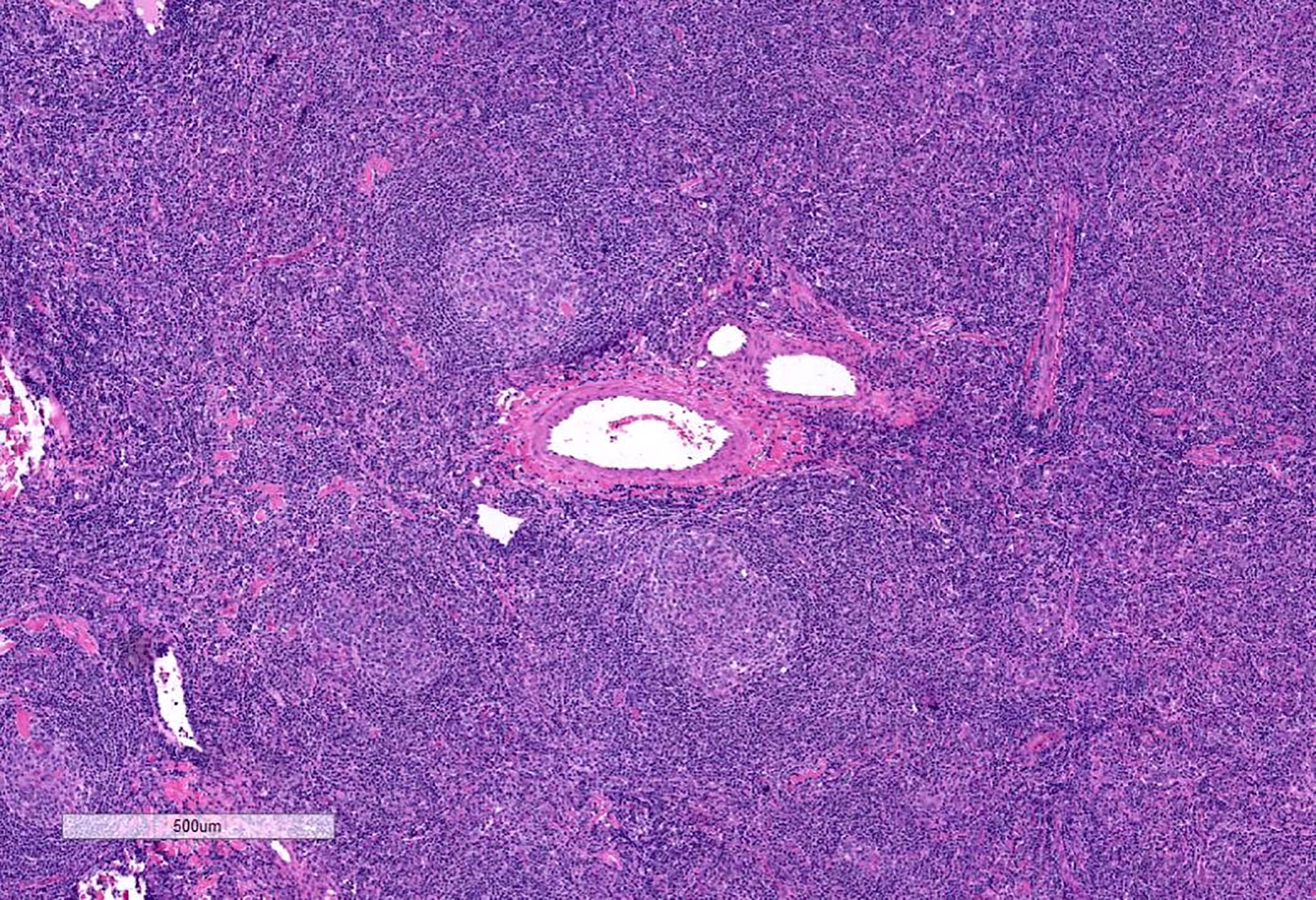
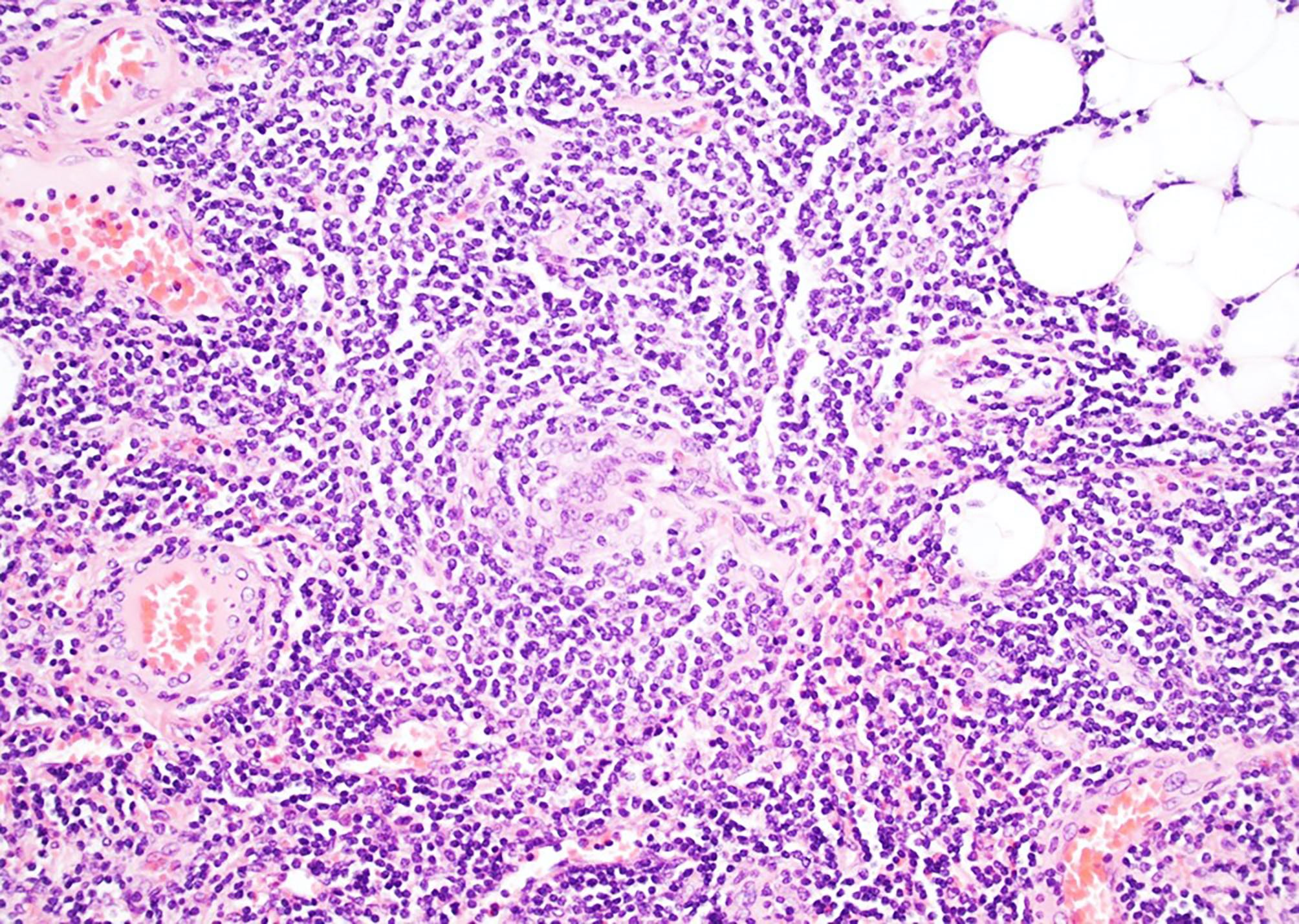
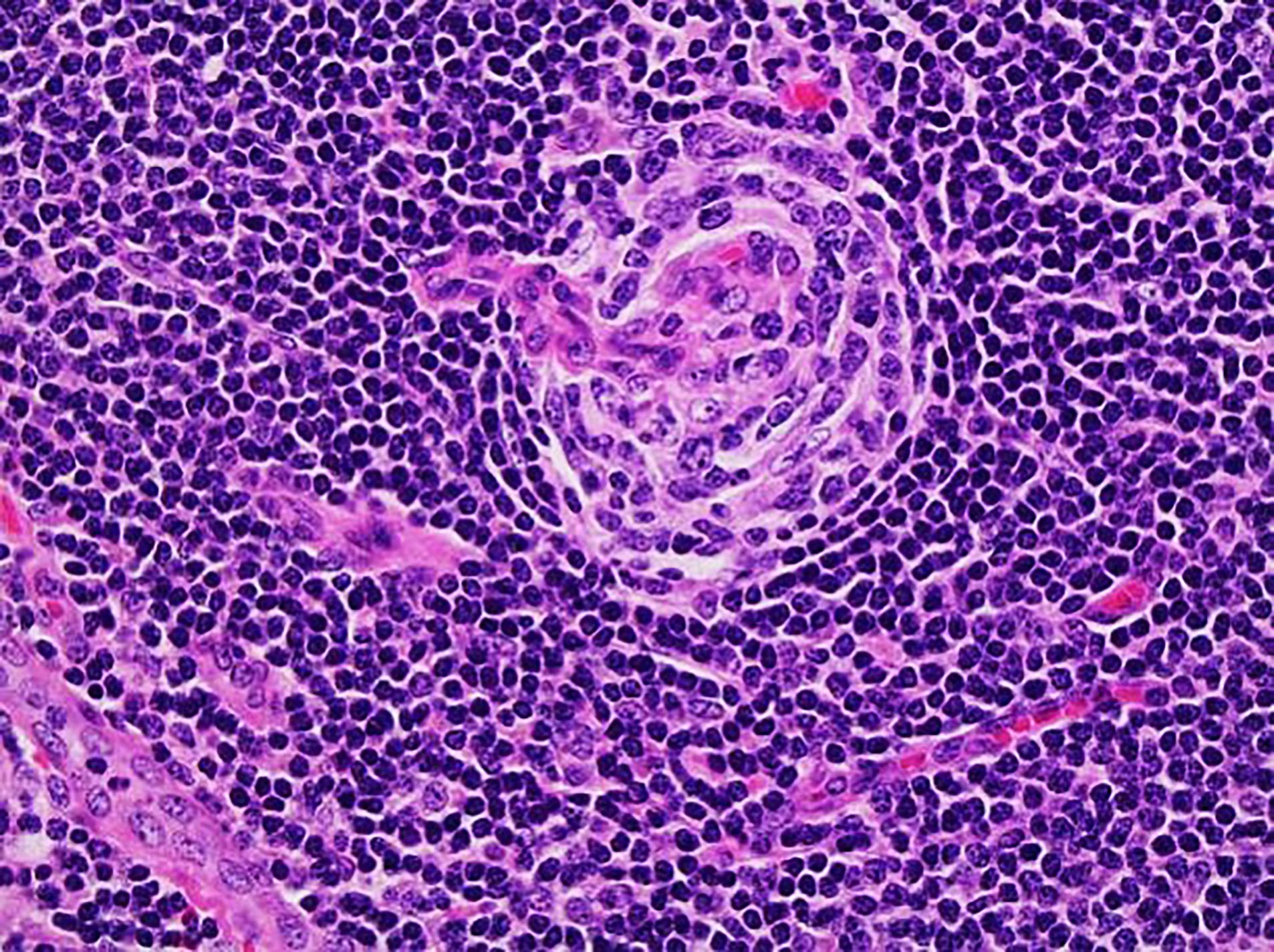
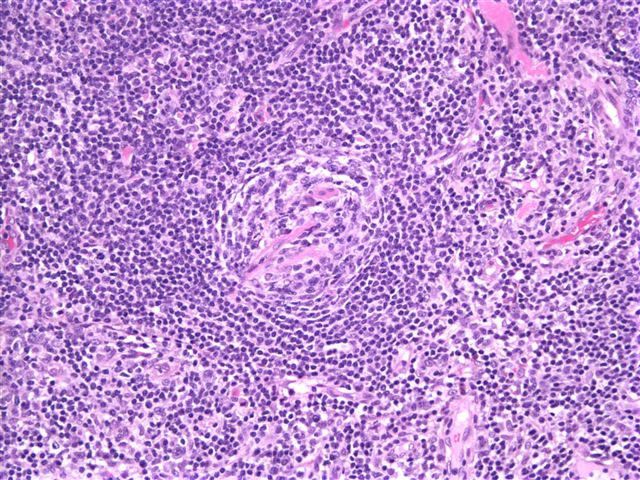
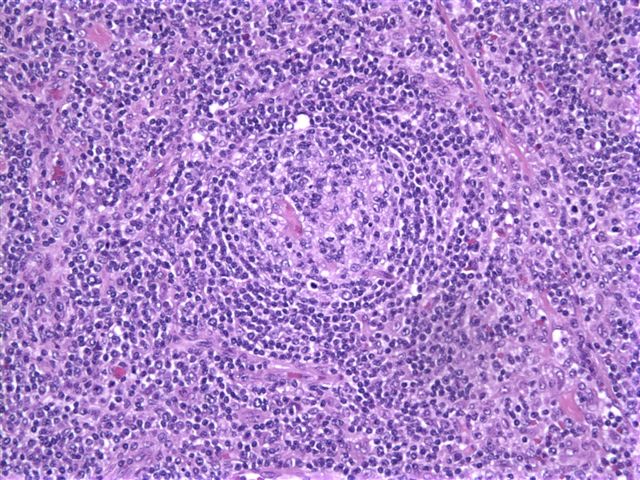
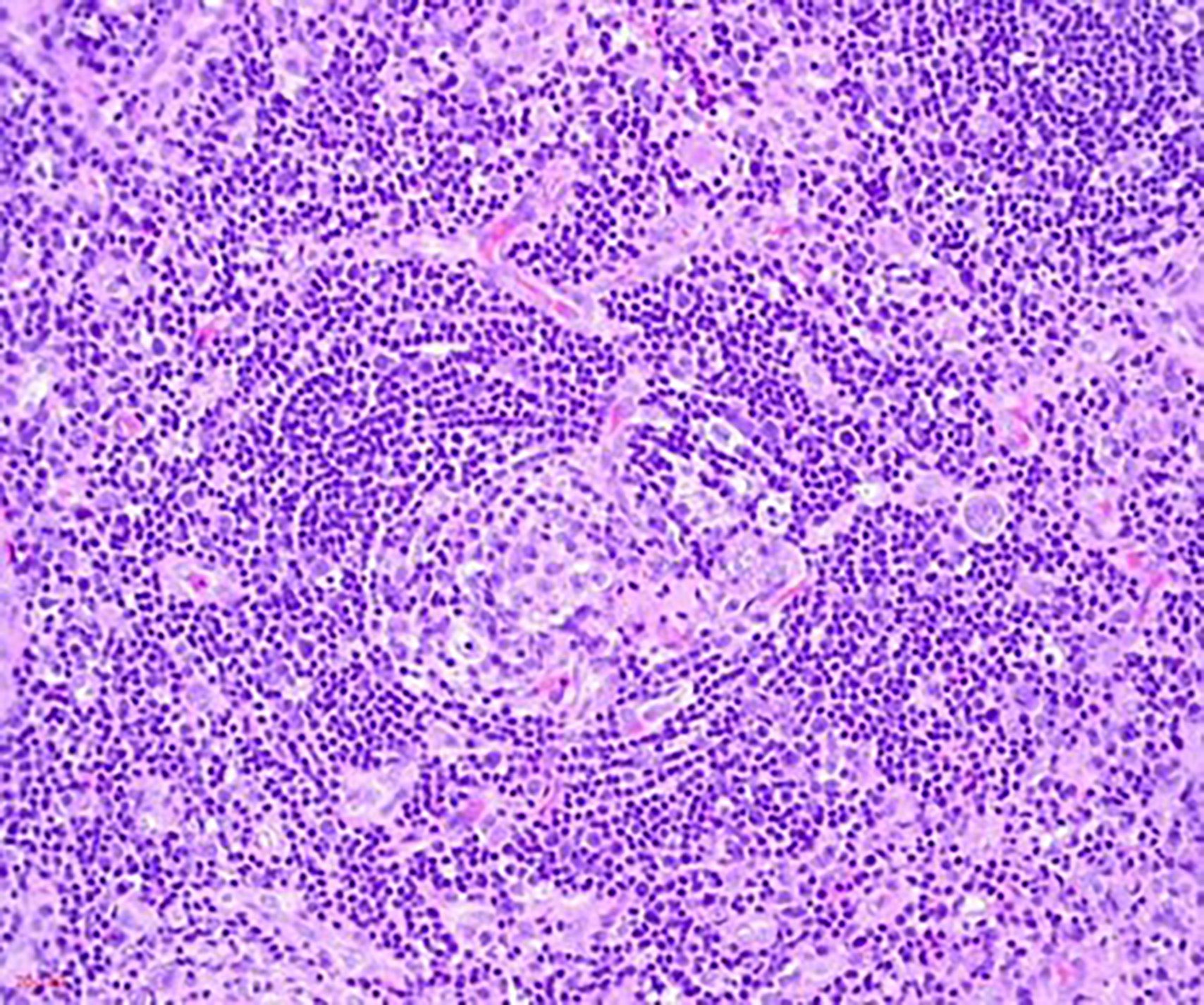
- Atretic germinal centers traversed by sclerotic penetrating vessels and hyalinization - lollipop follicles
- Mantle zones are thickened with lymphocytes arranged in layers - onion skin appearance
- Mantle zones may fuse and contain more than 1 germinal center - twinning
- Follicular dendritic cells may show proliferation and dysplastic features
- In the interfollicular areas, there is usually extensive vascular proliferation of high endothelial venules with perivascular hyalinization
- Clusters of plasmacytoid dendritic cells may be seen (Hum Pathol 2013;44:1003)
- Plasma cells, immunoblasts and eosinophils are seen in the interfollicular areas but no sheets of plasma cells
- Unapparent sinuses and obliteration of the subcapsular sinuses commonly seen
- Capsular thickening
- UCD - plasma cell type: rare (< 10% of UCDs) and MCD needs to be excluded (Surg Pathol Clin 2019;12:849)
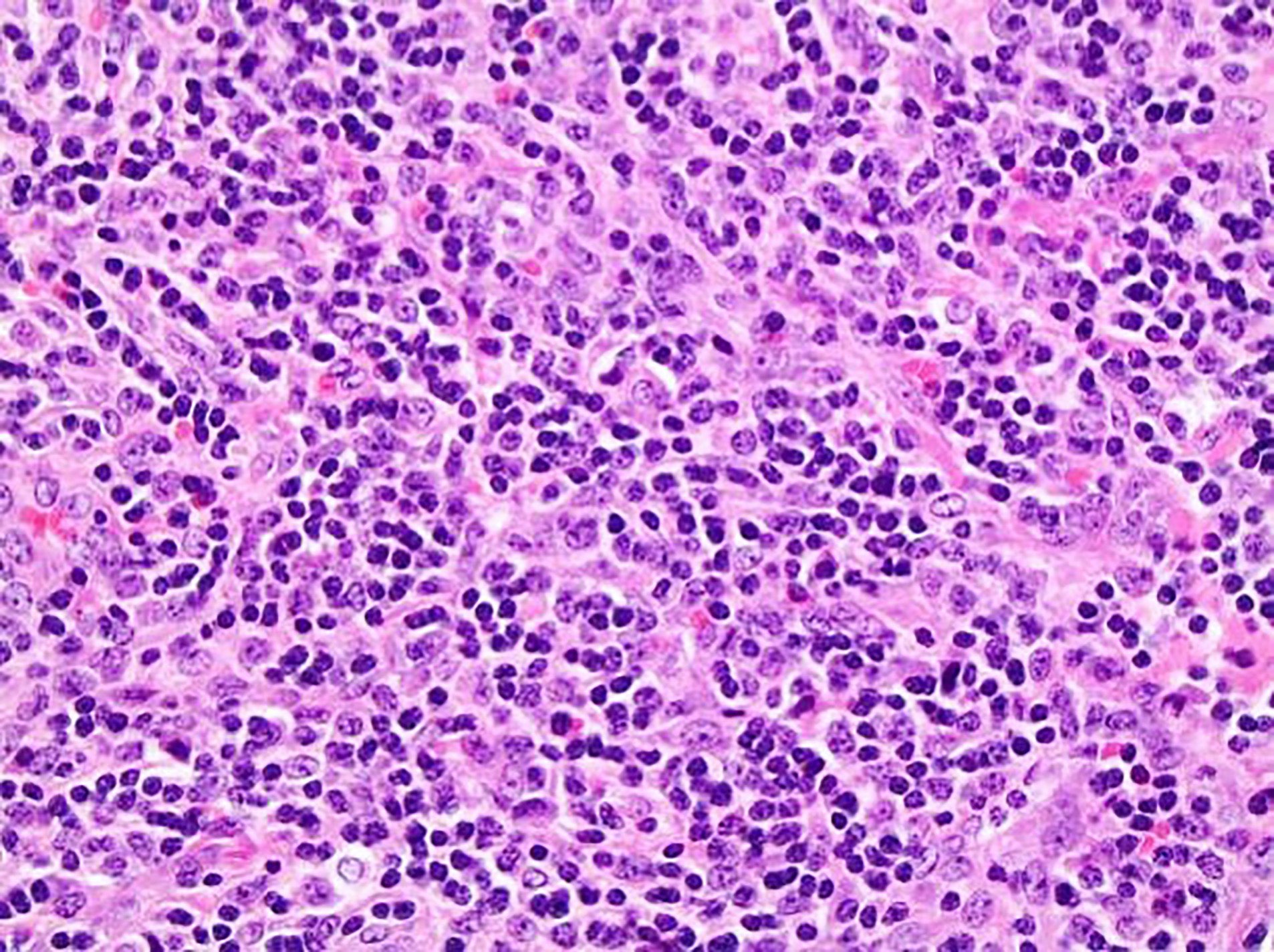
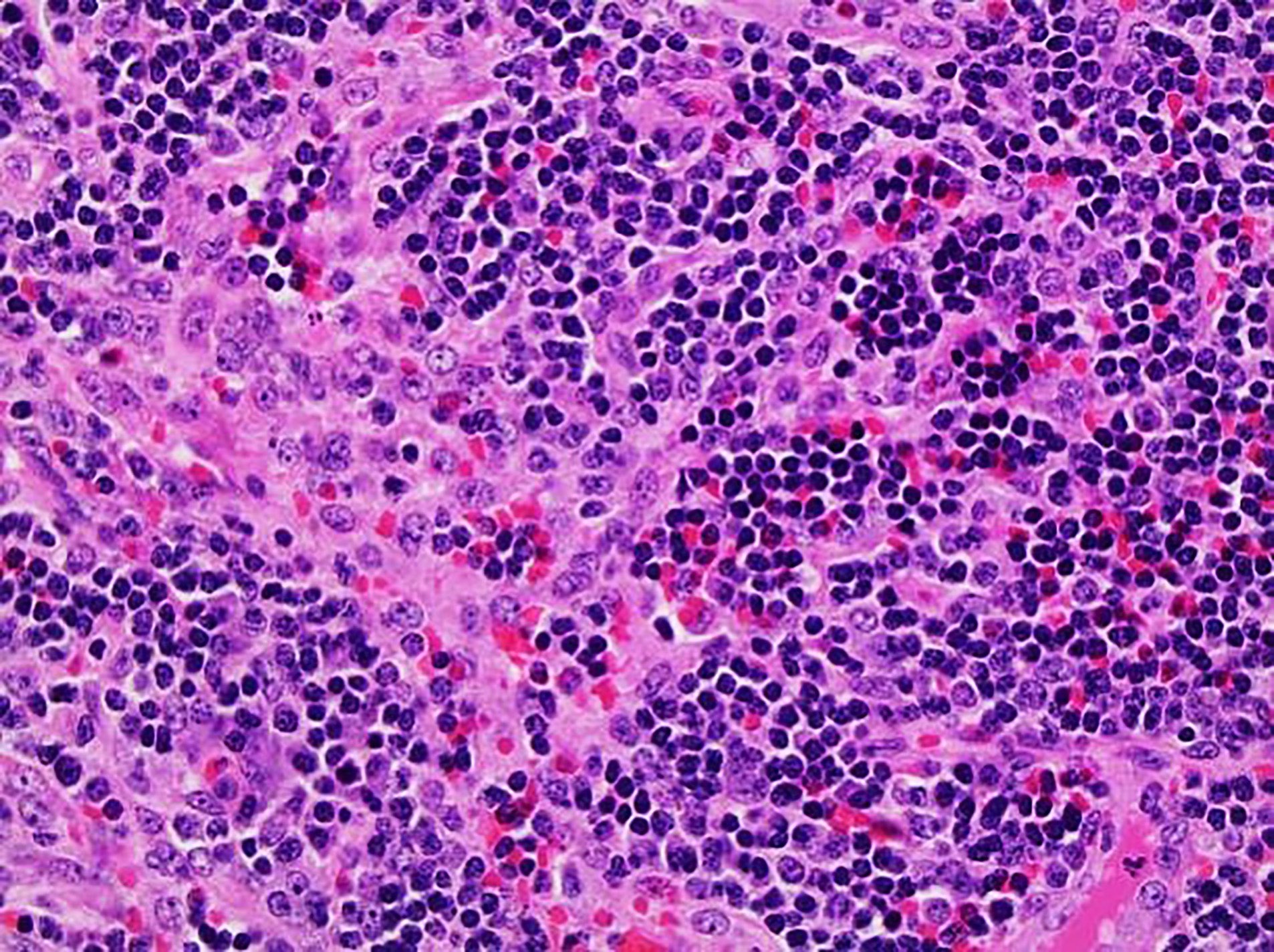
- Interfollicular areas and medulla containing sheets of small, mature plasma cells
- Hyperplastic follicles and a subset of the follicles with hyaline vascular features
- MCD can be hyaline vascular (rare < 10%) or plasmacytic but usually shows a mix of histological features of both plasma cell and hyaline vascular Castleman disease (Blood 2017;129:1658, Blood 2017;129:1646)
- Hypervascular without dysplastic follicular dendritic cells or sclerotic vessels
- Diffuse plasma cell proliferation, germinal center hyperplasia, some follicles may show hyaline vascular changes and patent sinuses
- HHV8 MCD (Am J Surg Pathol 2003;27:91)
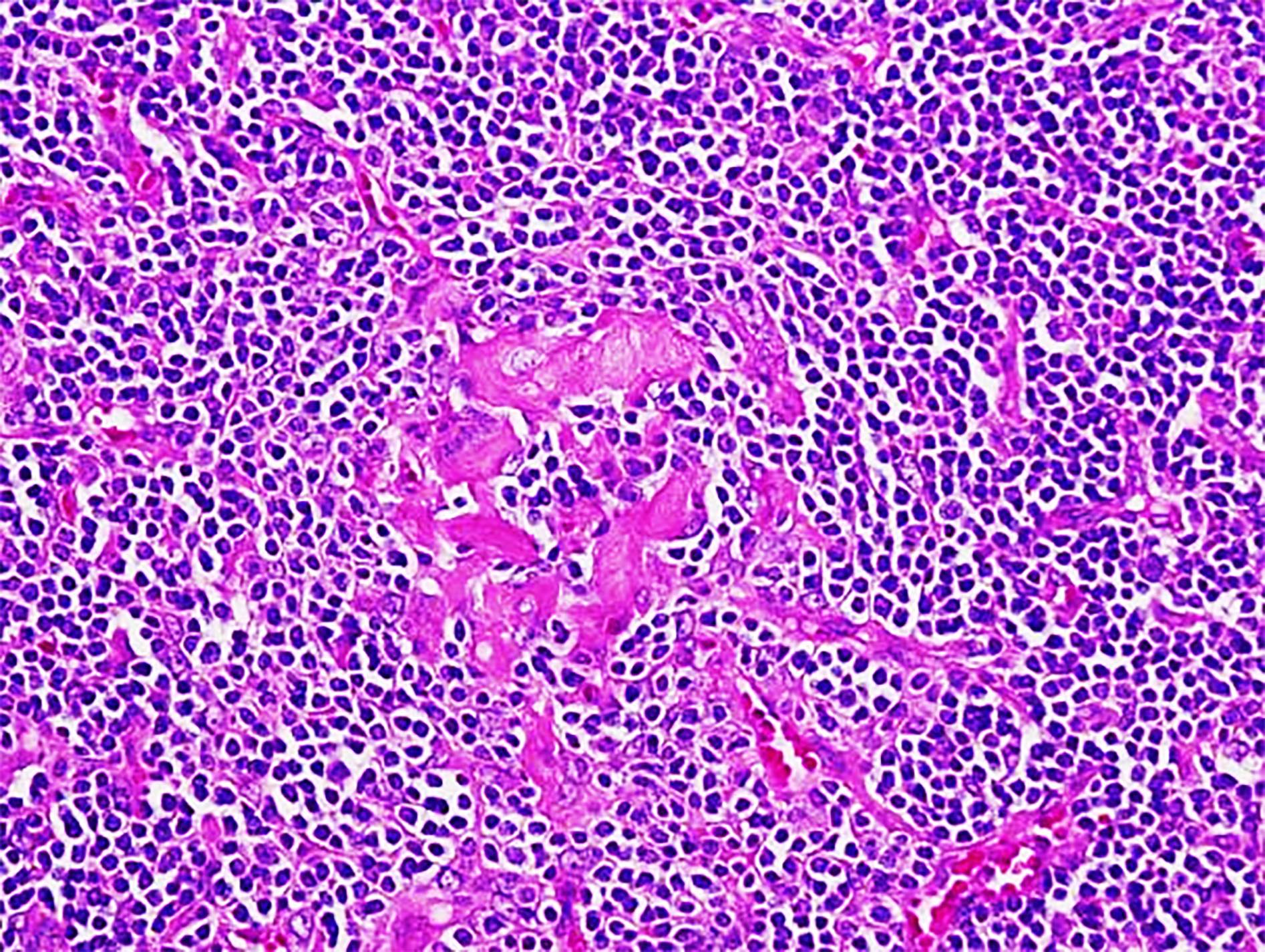
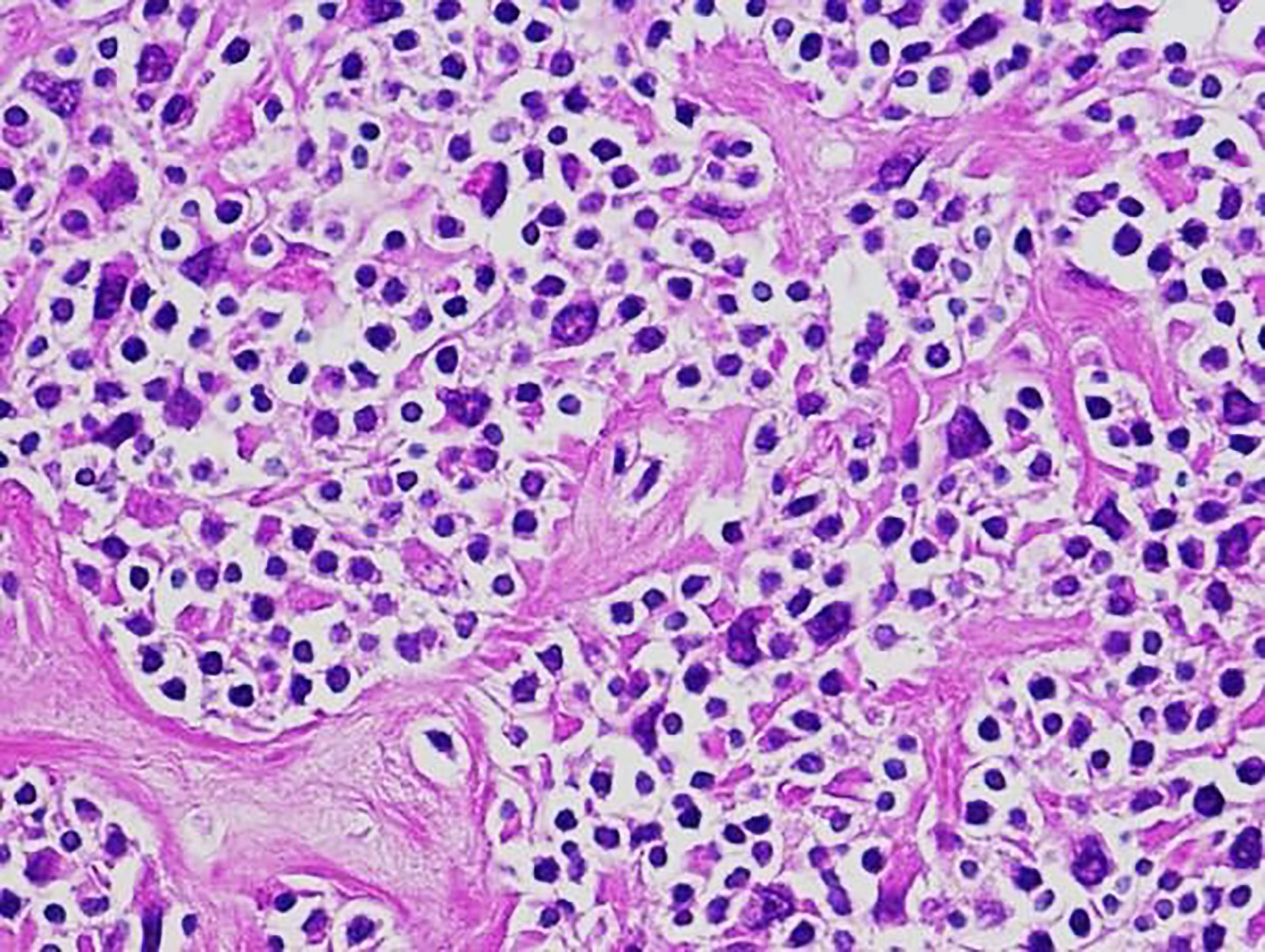
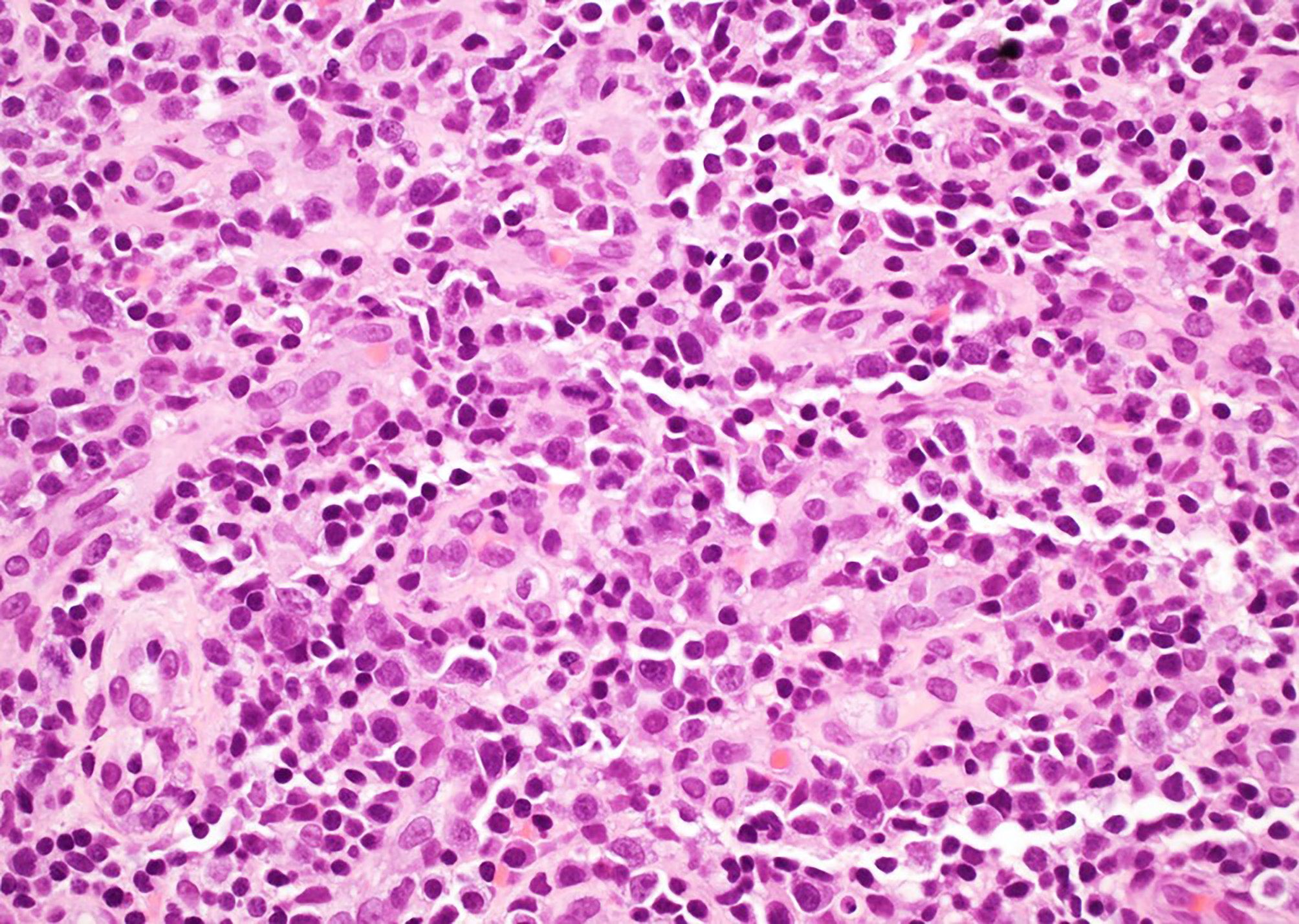
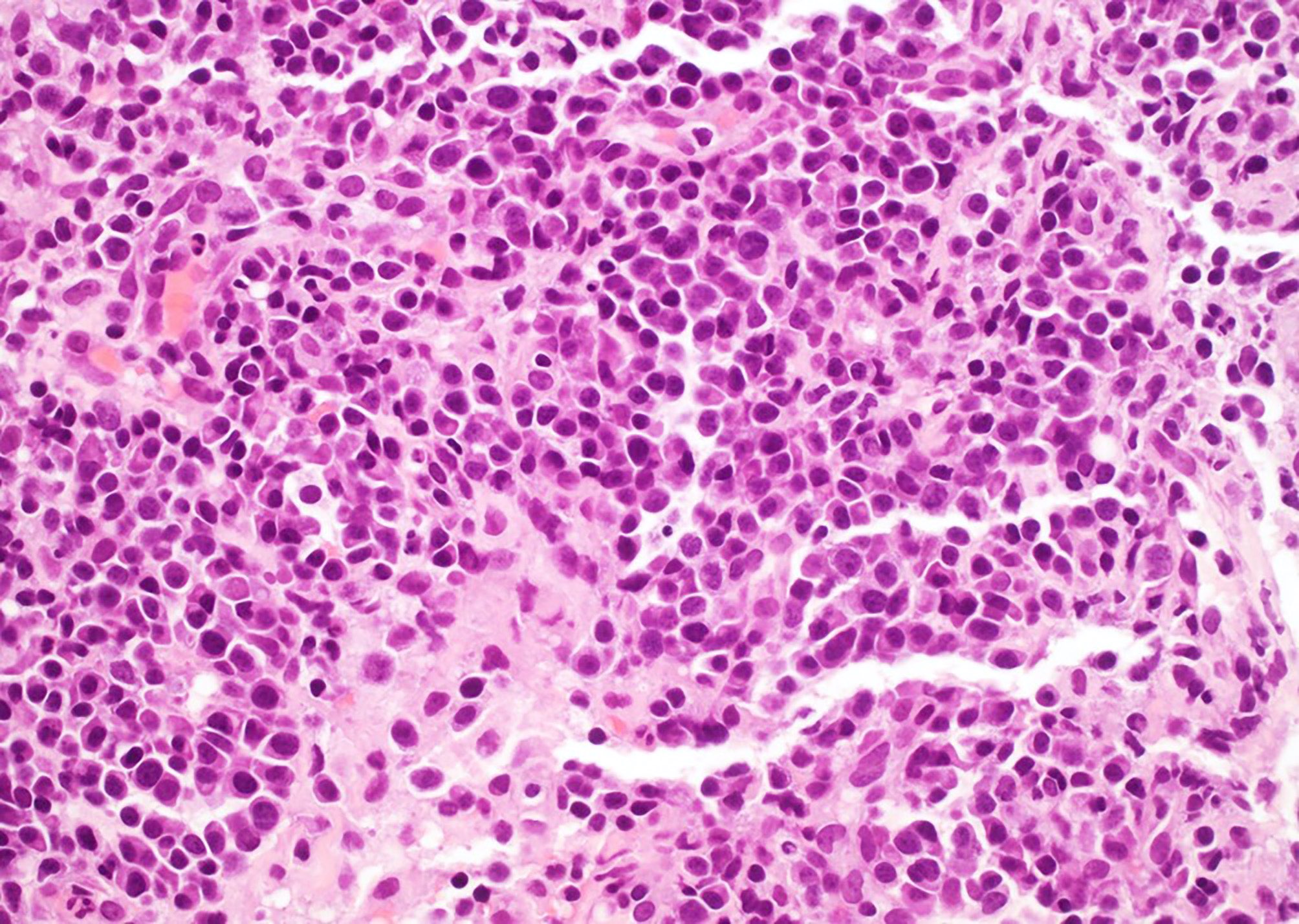
- Plasmacytic
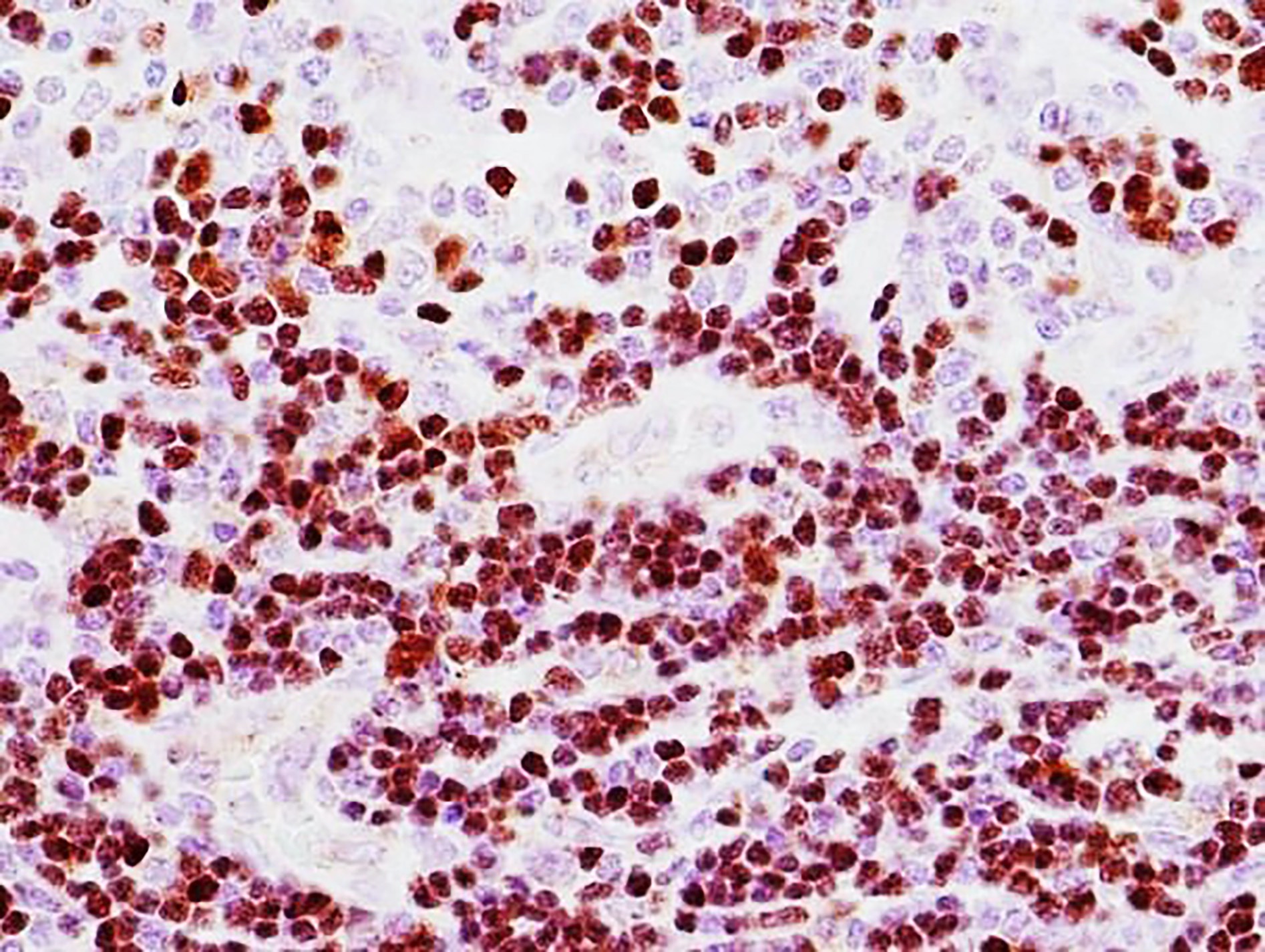
- HHV8 infected cells in the mantle zones show plasmablastic or immunoblastic morphology with large nuclei, vesicular chromatin and prominent nucleoli and lambda light chain restriction
- Polyclonal plasmacytosis
- TAFRO (Hematol Oncol Clin North Am 2018;32:37)
- Mixed hyaline vascular and plasmacytic
- Lymph nodes: hypervascular
- Bone marrow: reticulin fibrosis, megakaryocytic hyperplasia and emperipolesis
Contributed by Jayalakshmi Balakrishna, M.D., Amy Duffield, M.D., Ph.D., Tapan Bhavsar, M.D., Ph.D.,
Carlos Murga-Zamalloa, M.D. and Jackie D. Sublett II, M.D.
Hyaline vascular Castleman disease (HVCD)
Atretic follicles, interfollicular vascular proliferation
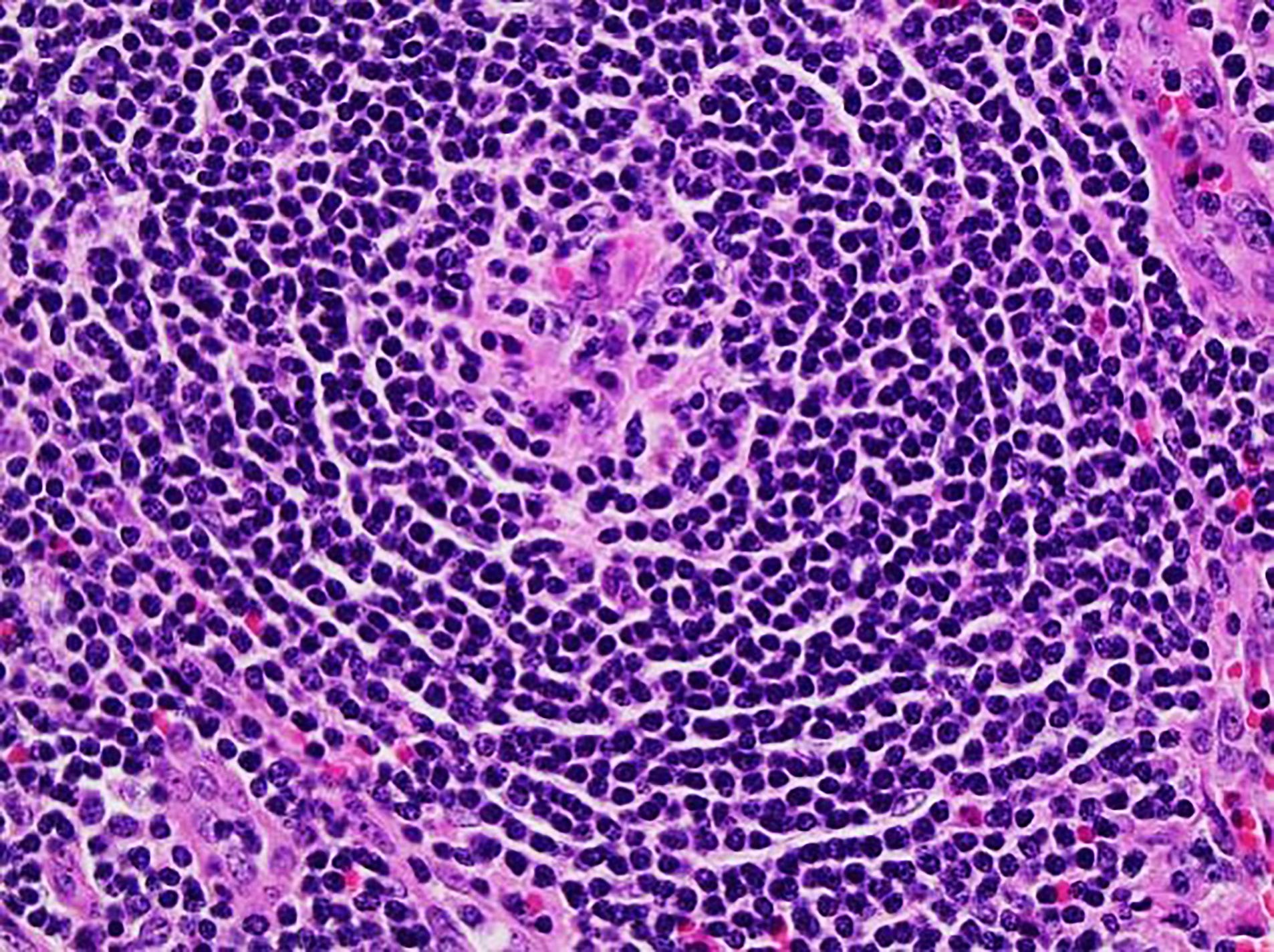
Atretic germinal center
Twinning of germinal center
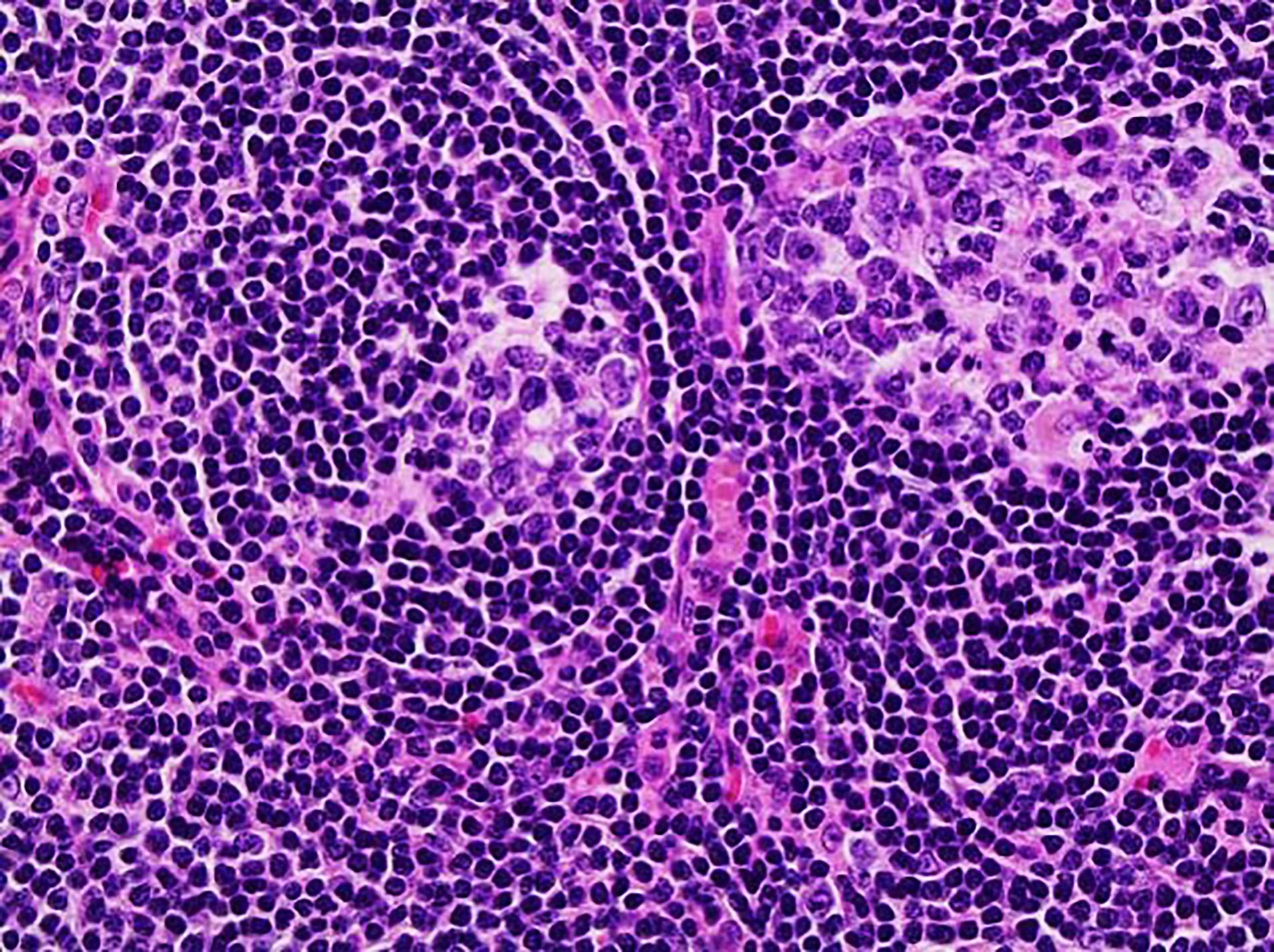
Twinning of germinal center
Twinning of germinal center, thickened mantle zones
Lollipop follicle, thickened mantle zones
Twinning of
germinal centers,
sclerosed
vessels
Thickened mantle zones
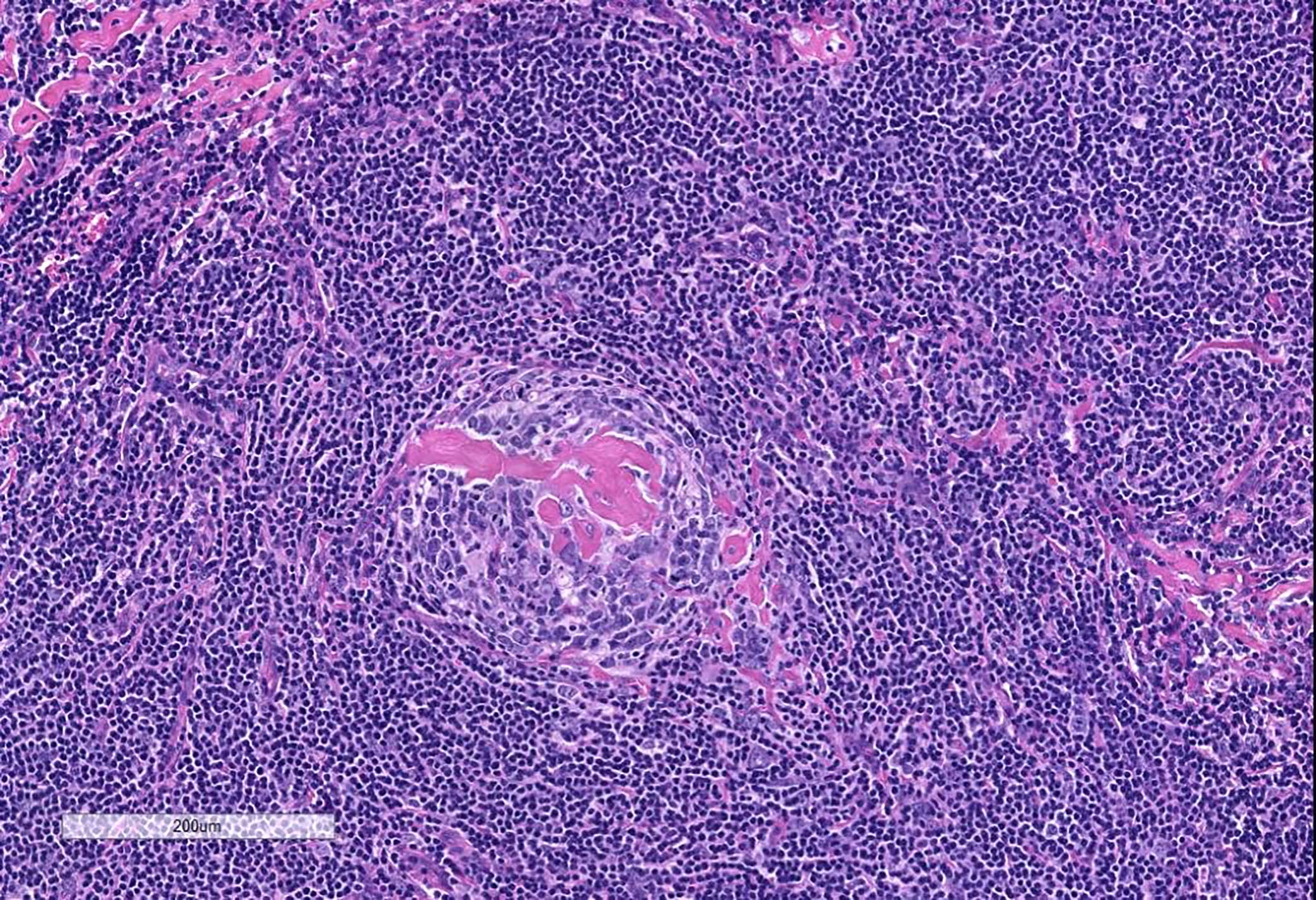
Sclerosed vessels
Vascular proliferation
Lollipop follicle
Atretic follicle

Proliferation of T lymphoblasts
Onion skin pattern

Twinning of germinal center, CD23
Interfollicular areas rich in T cells, CD3
Follicles and atretic germinal centers, CD20

Proliferation of TdT+ cells
Vascular proliferation, CD34
Interfollicular areas rich in T cells, CD5
Follicular dendritic cell meshworks, CD21
Low proliferation rate in interfollicular areas
Germinal centers, BCL6+
Plasma cells, CD138
Plasma cell Castleman disease (PCCD)
Aggregates of plasma cells
T cells in interfollicular areas, CD3
Atretic follicles, CD20

Aggregates of plasma cells, CD138
Vascular proliferation, ERG
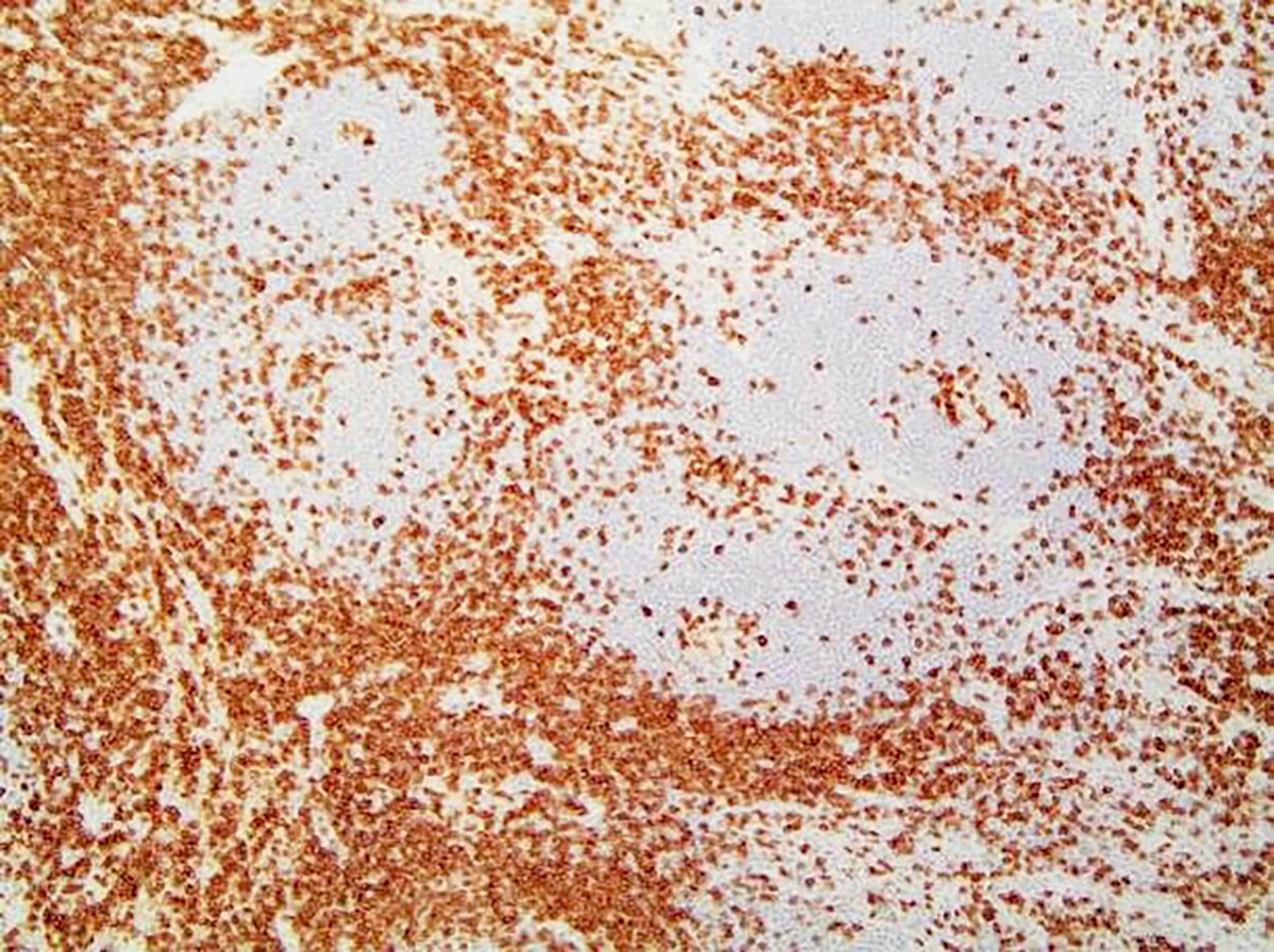
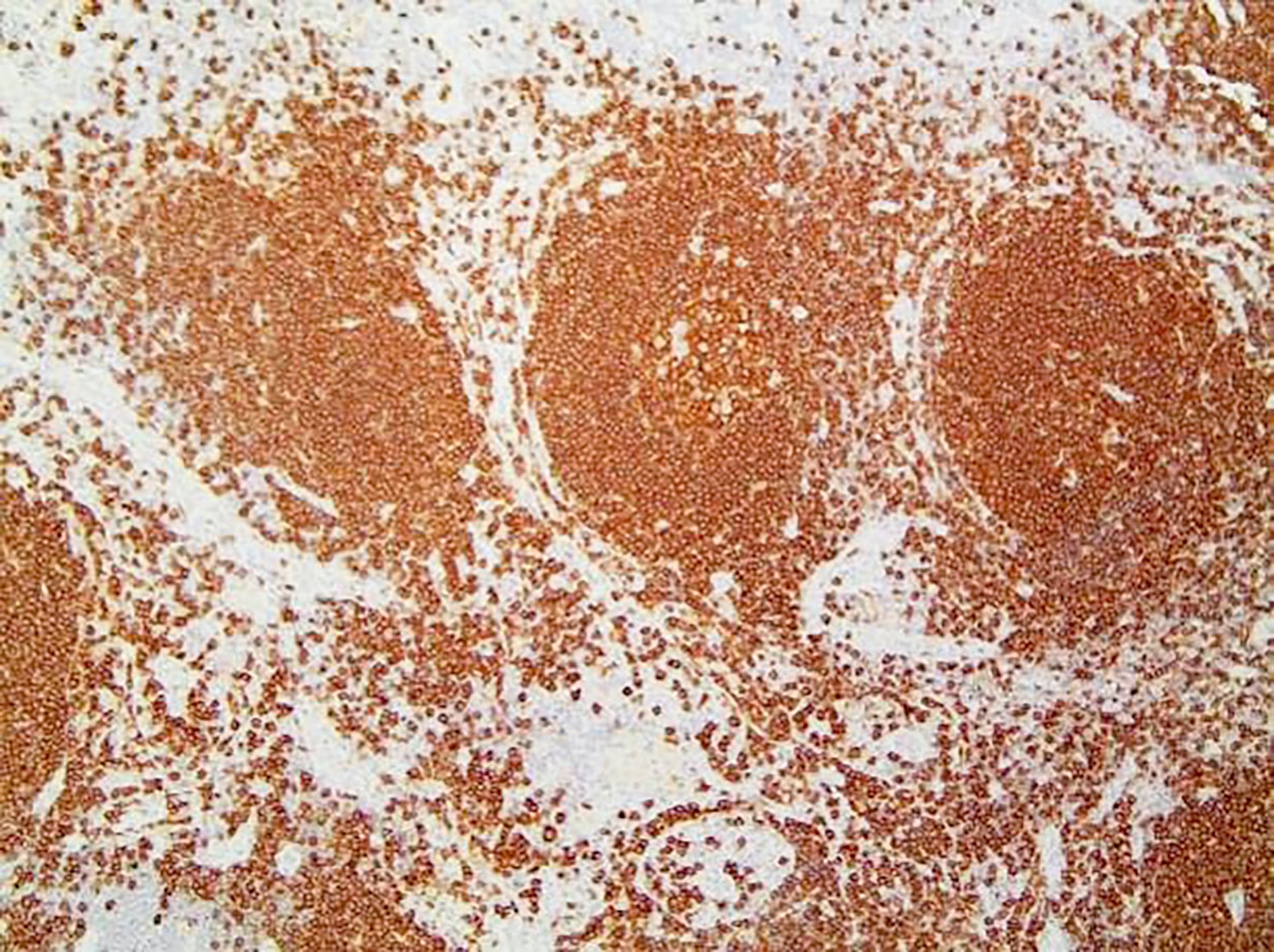
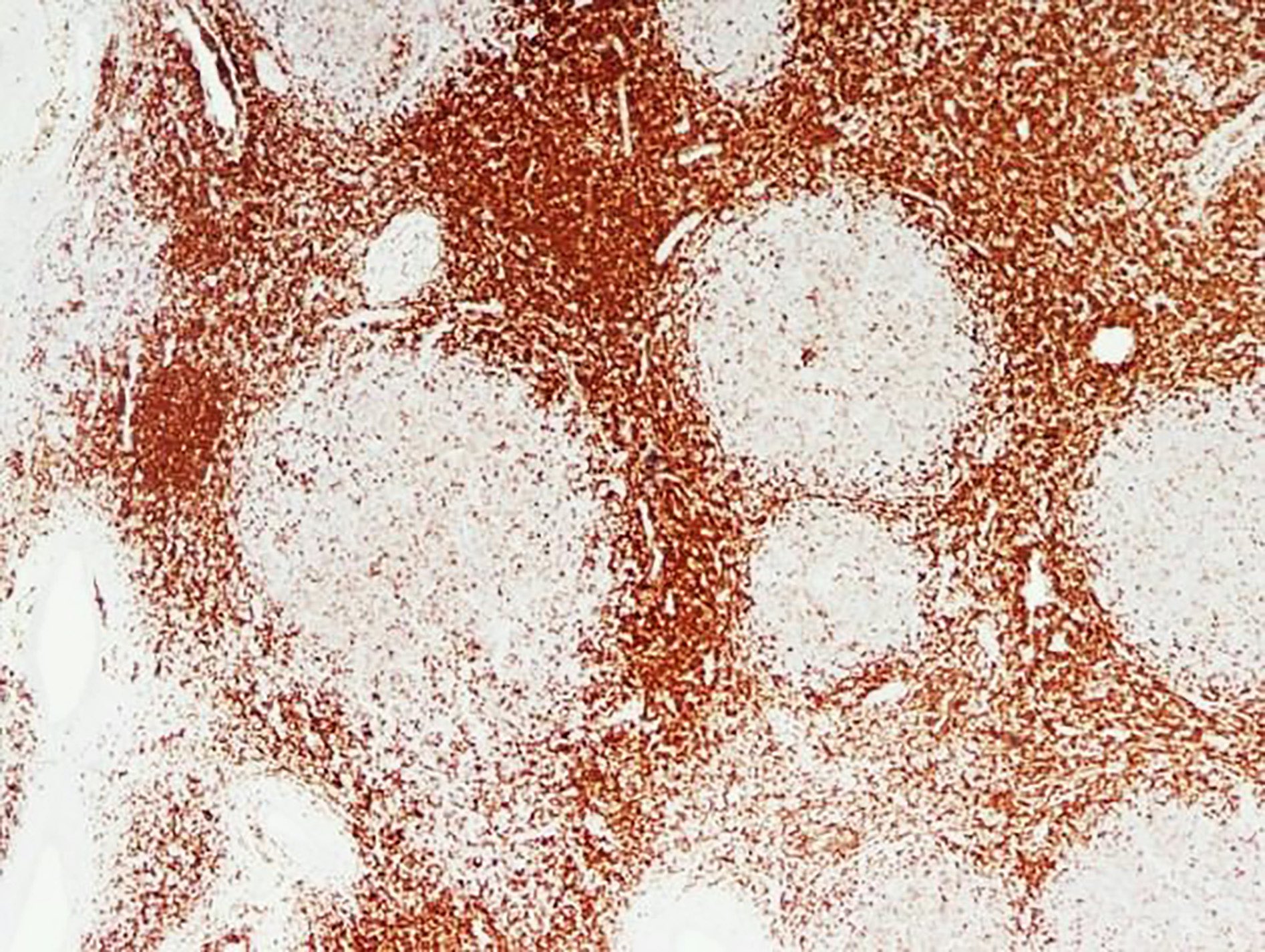
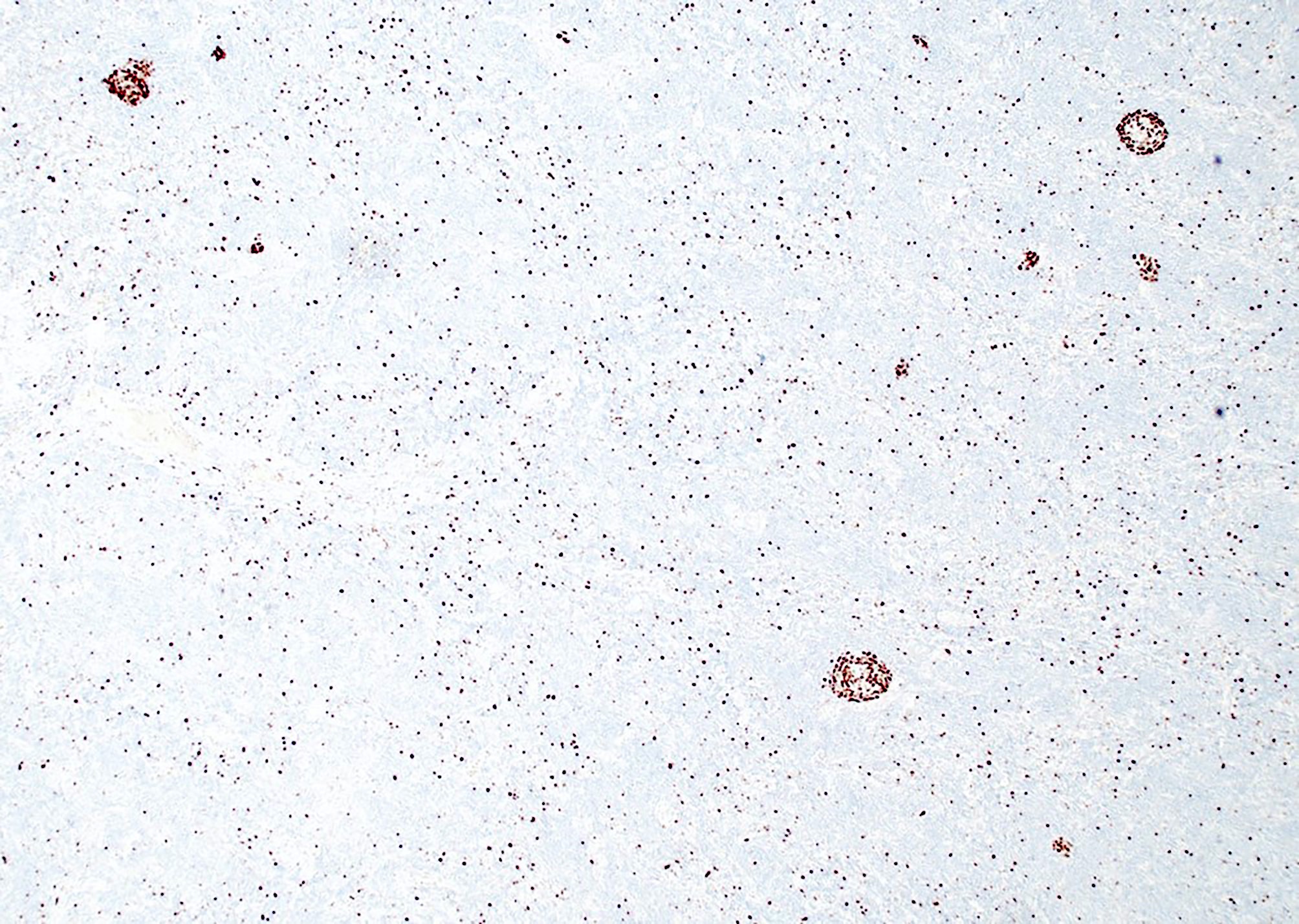
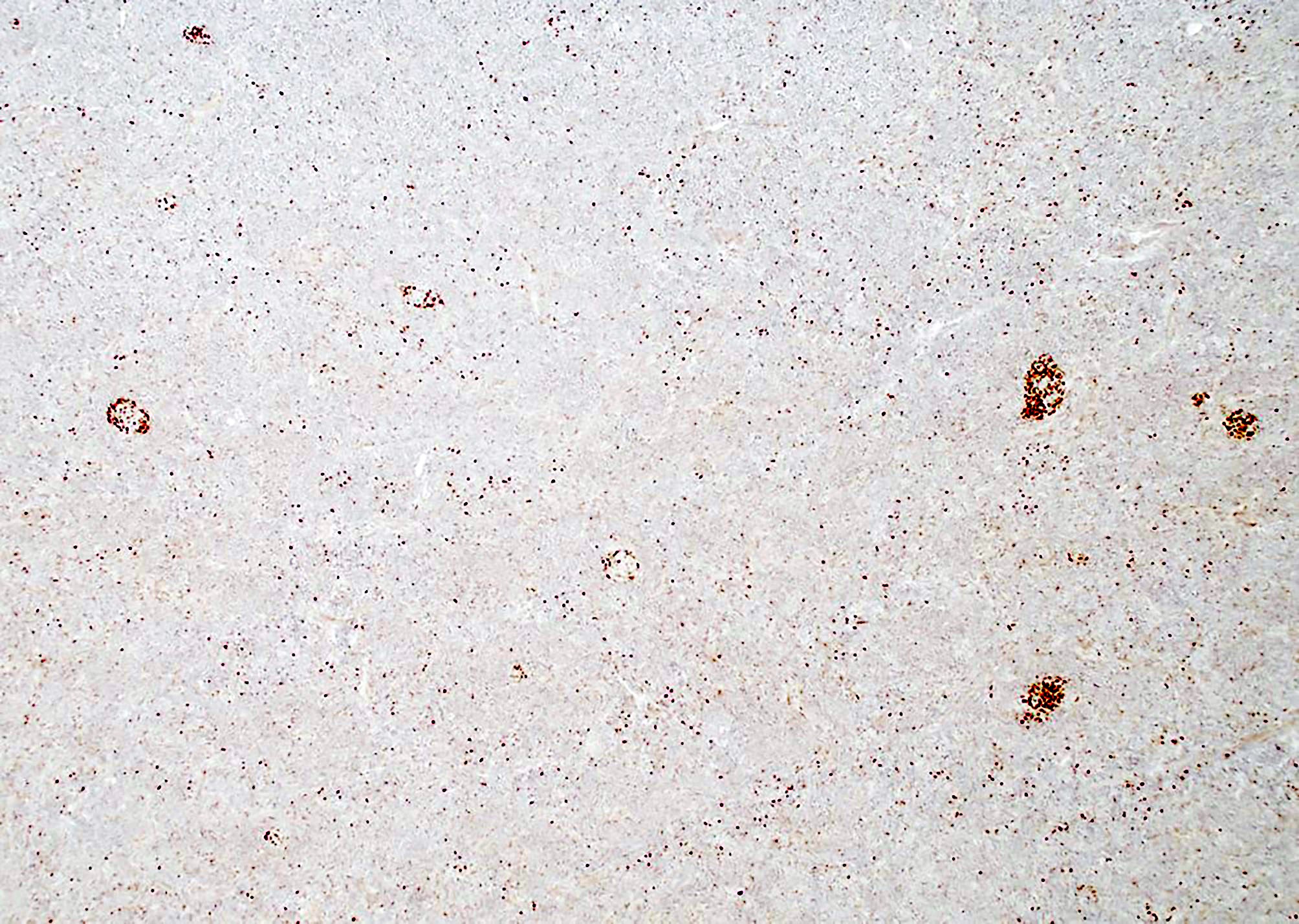
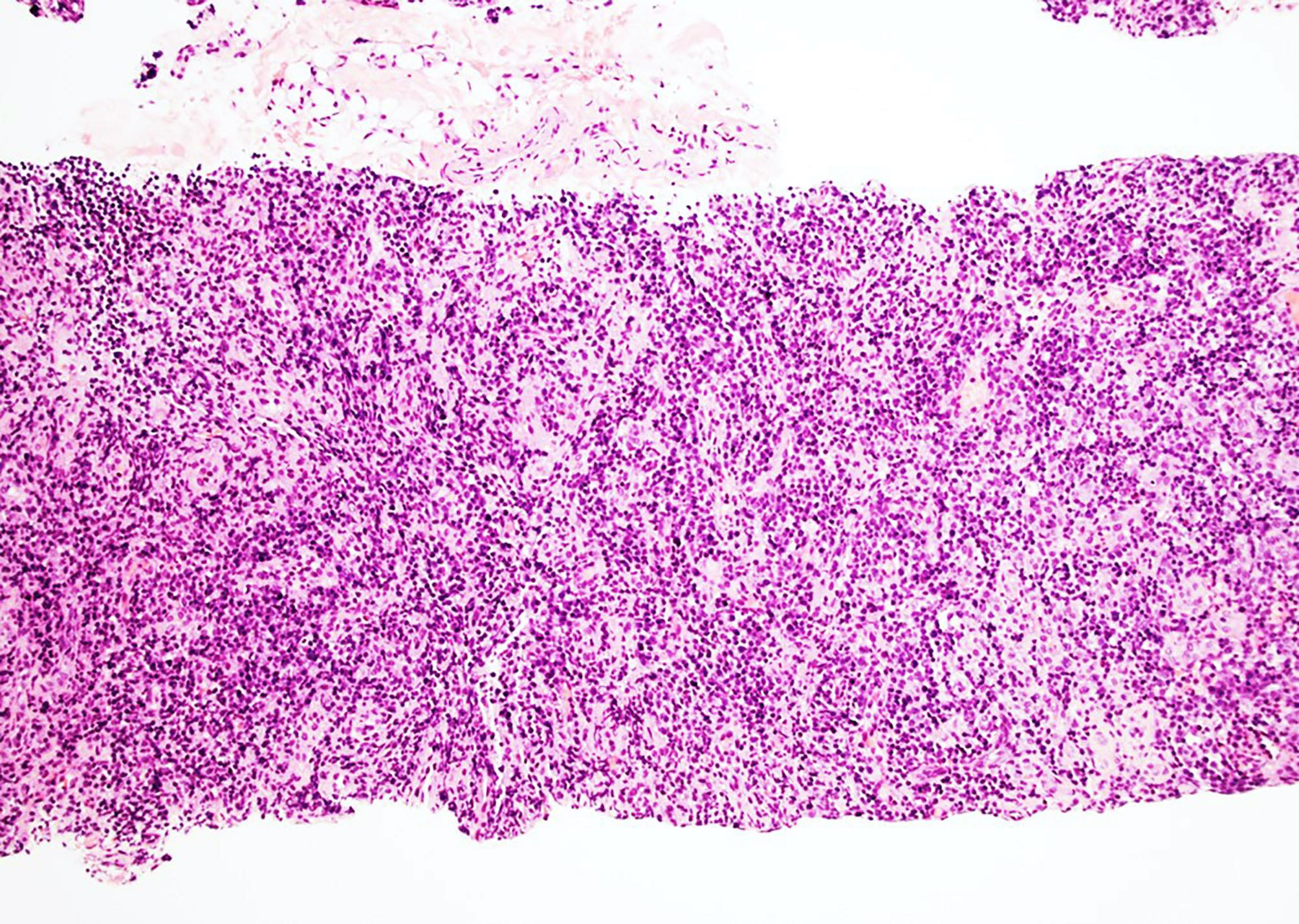
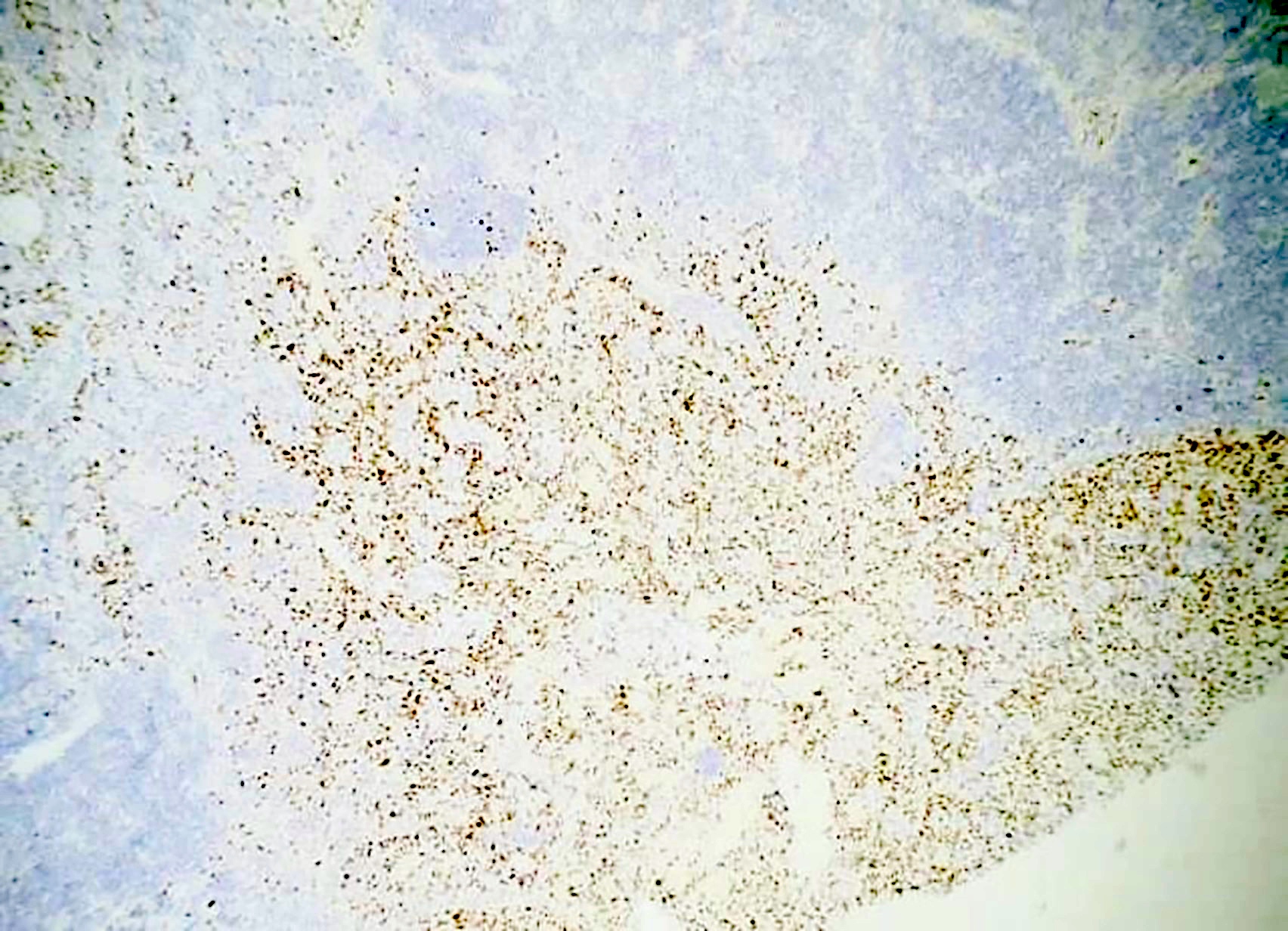
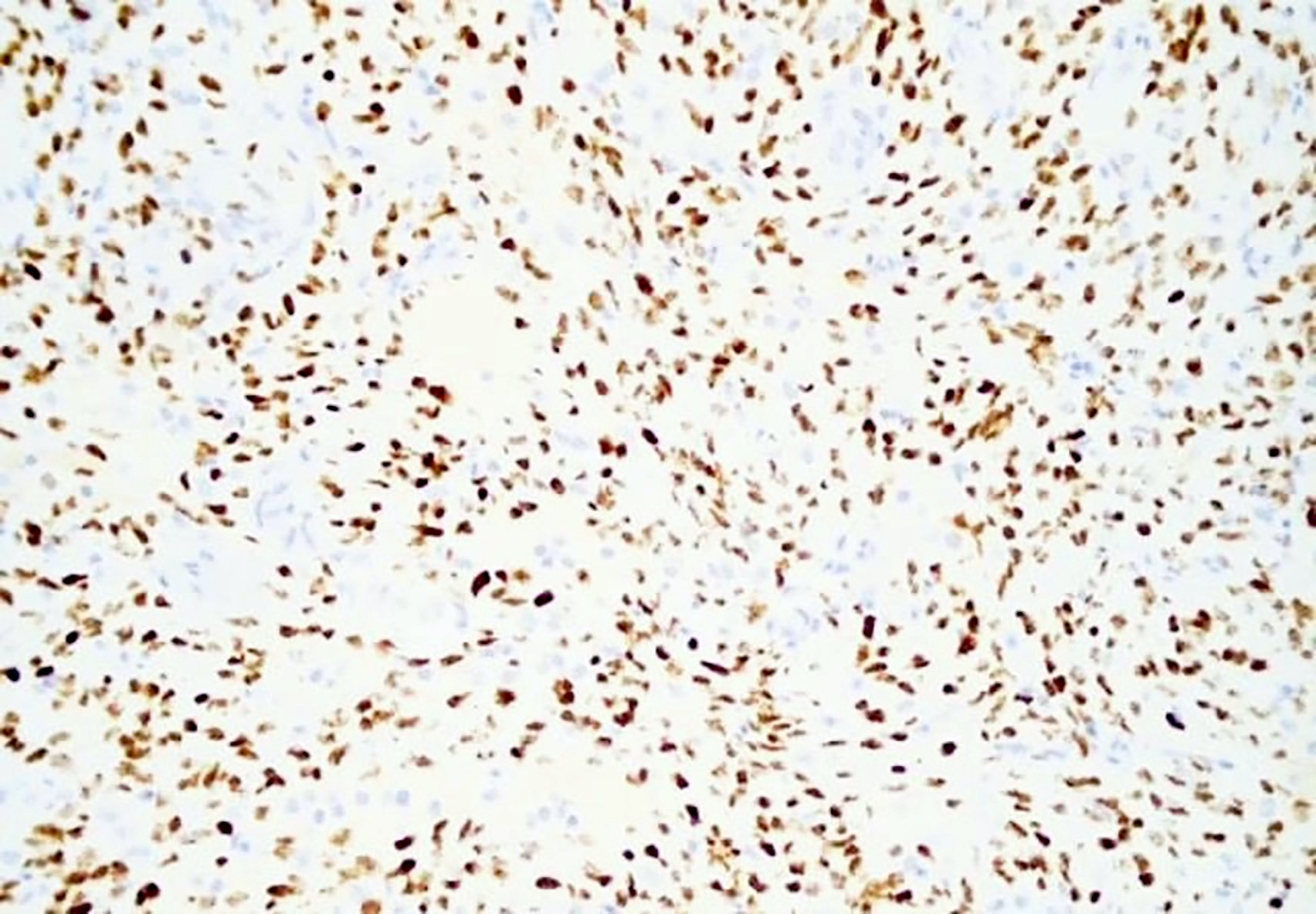
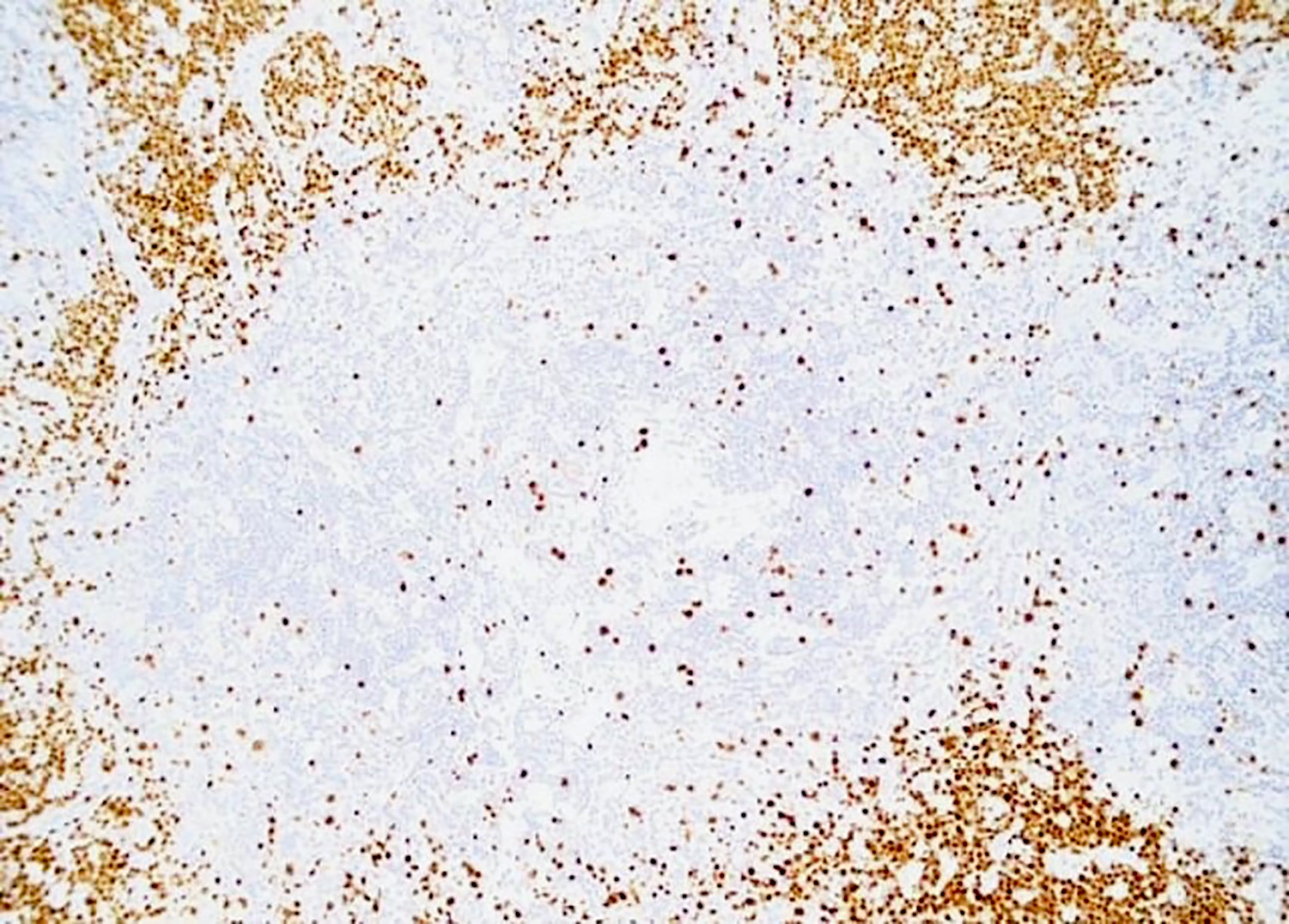
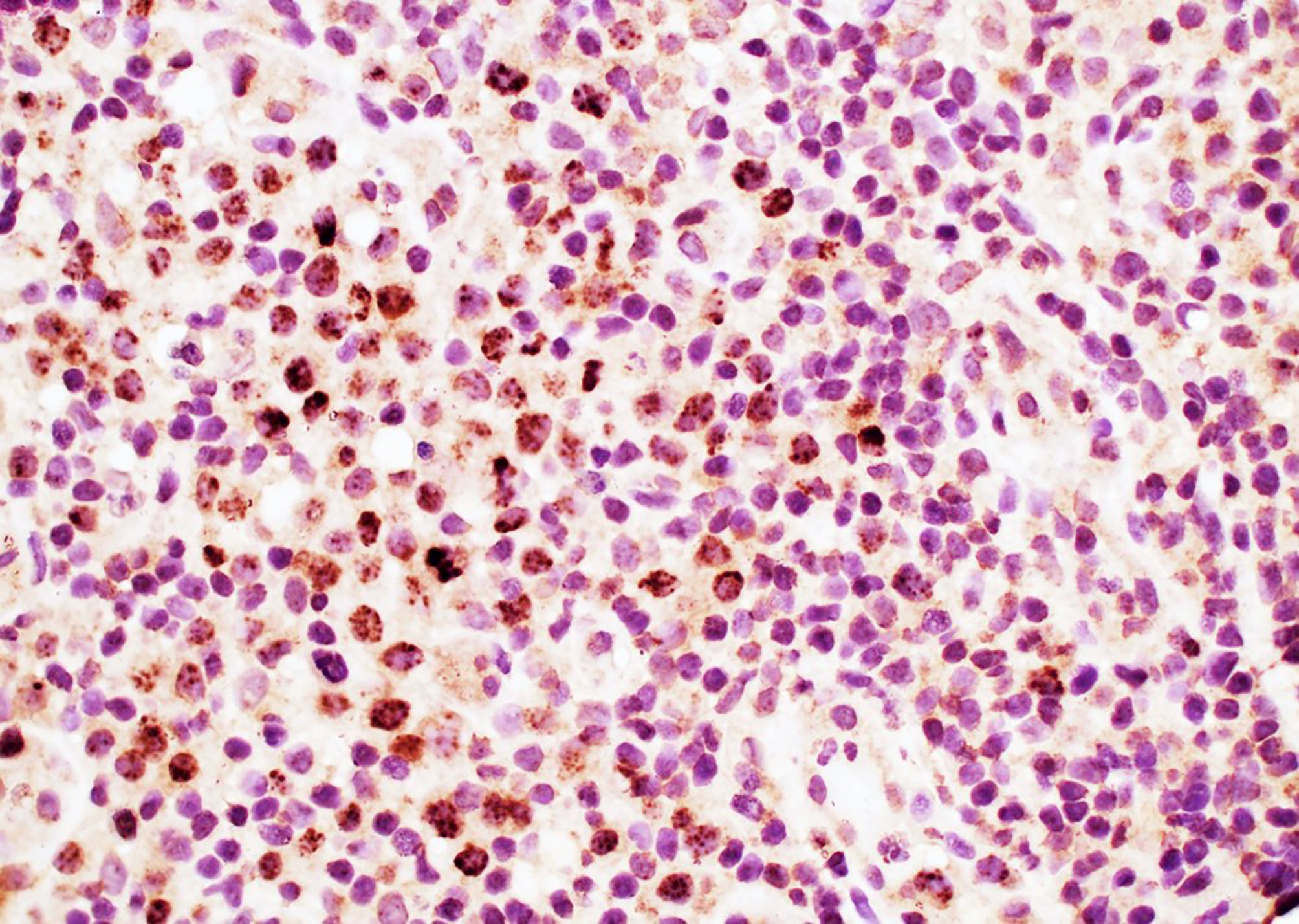
Human herpesvirus 8 associated multicentric Castleman disease (HHV8 MCD)
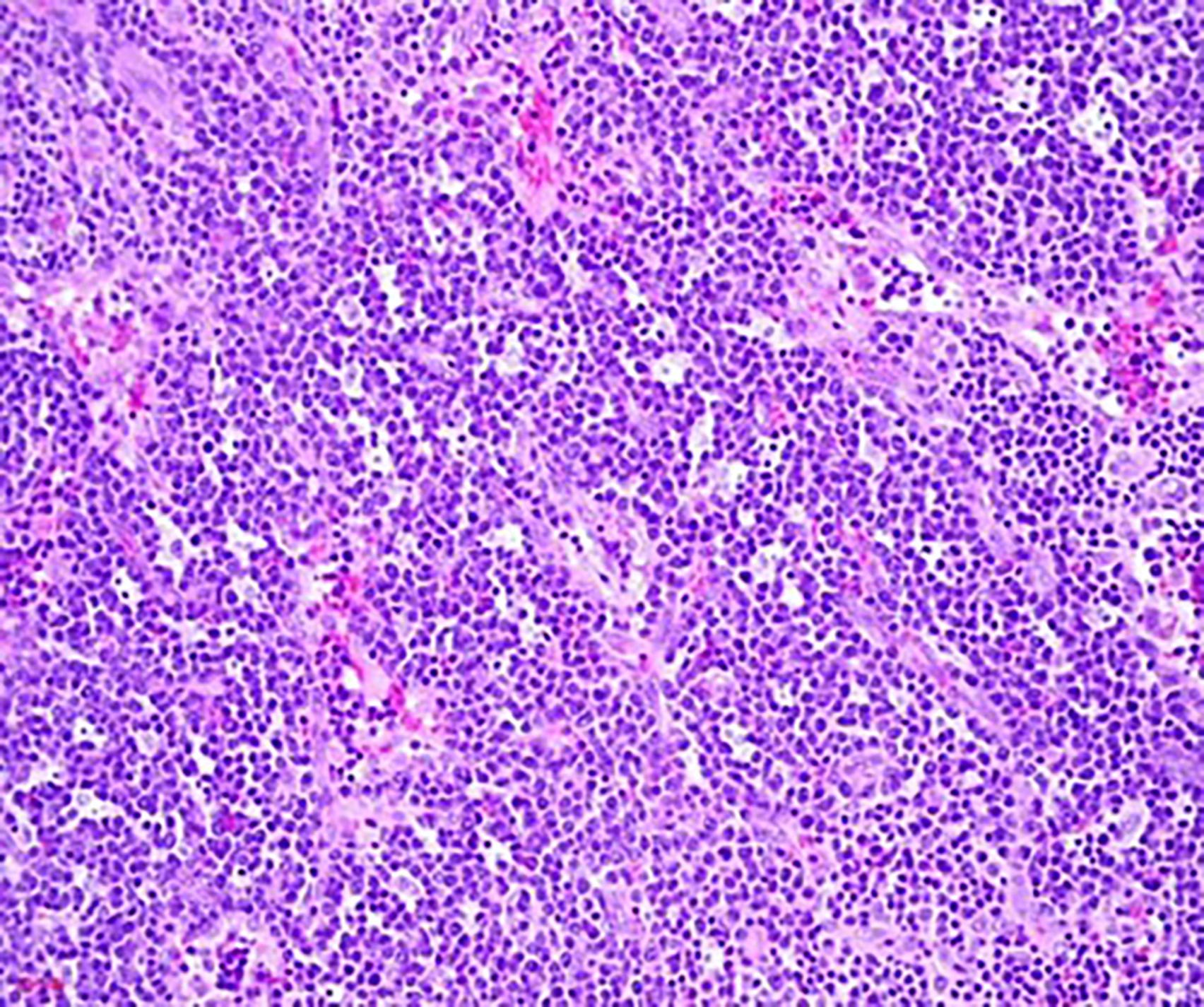
Aggregates of plasma cells
Atretic follicle, interfollicular plasma cell proliferation
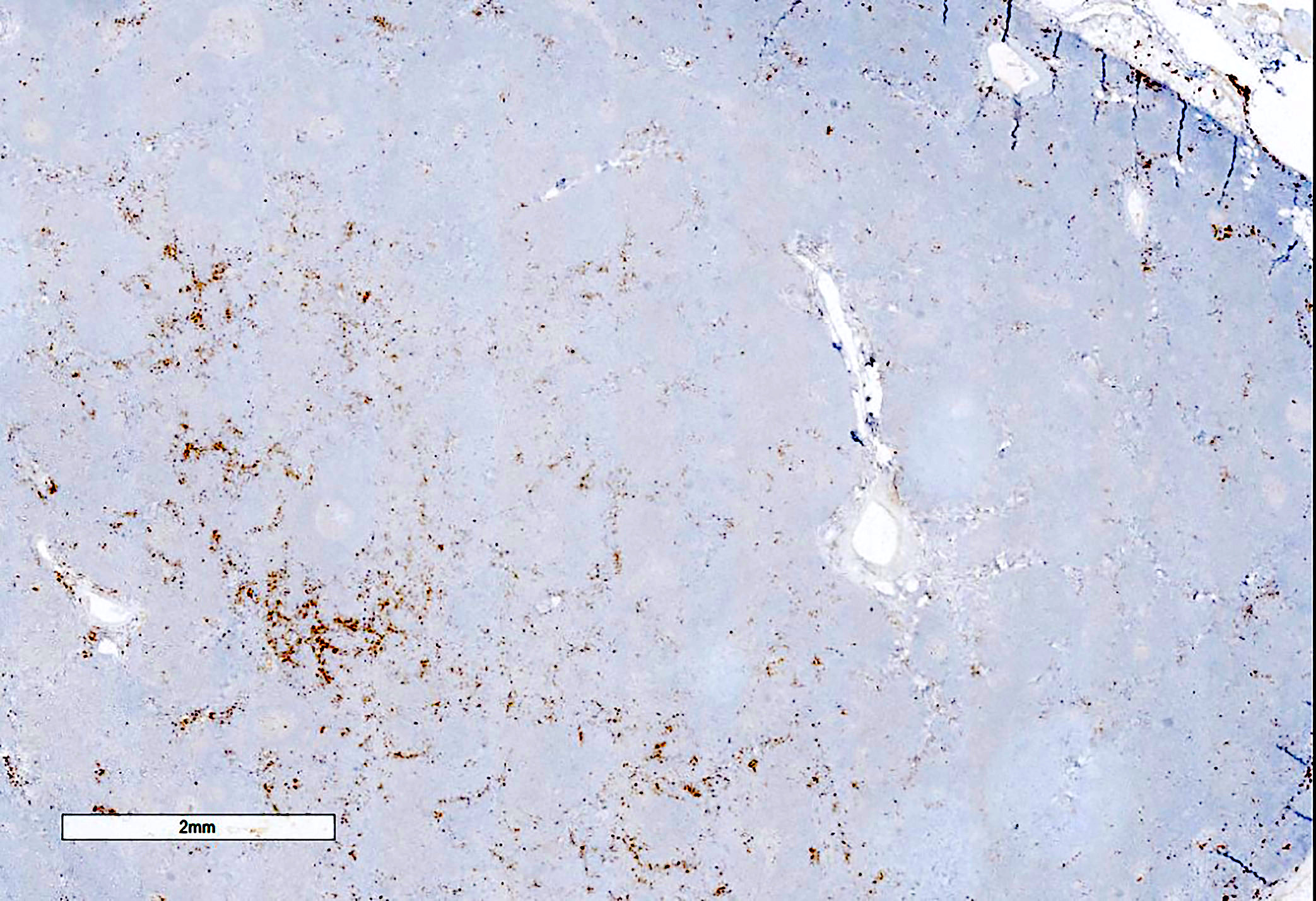
Kaposi sarcoma in a case of HHV8 MCD
Kaposi sarcoma in a case of HHV8 MCD, HHV8
Kaposi sarcoma in a case of HHV8 MCD, MUM1
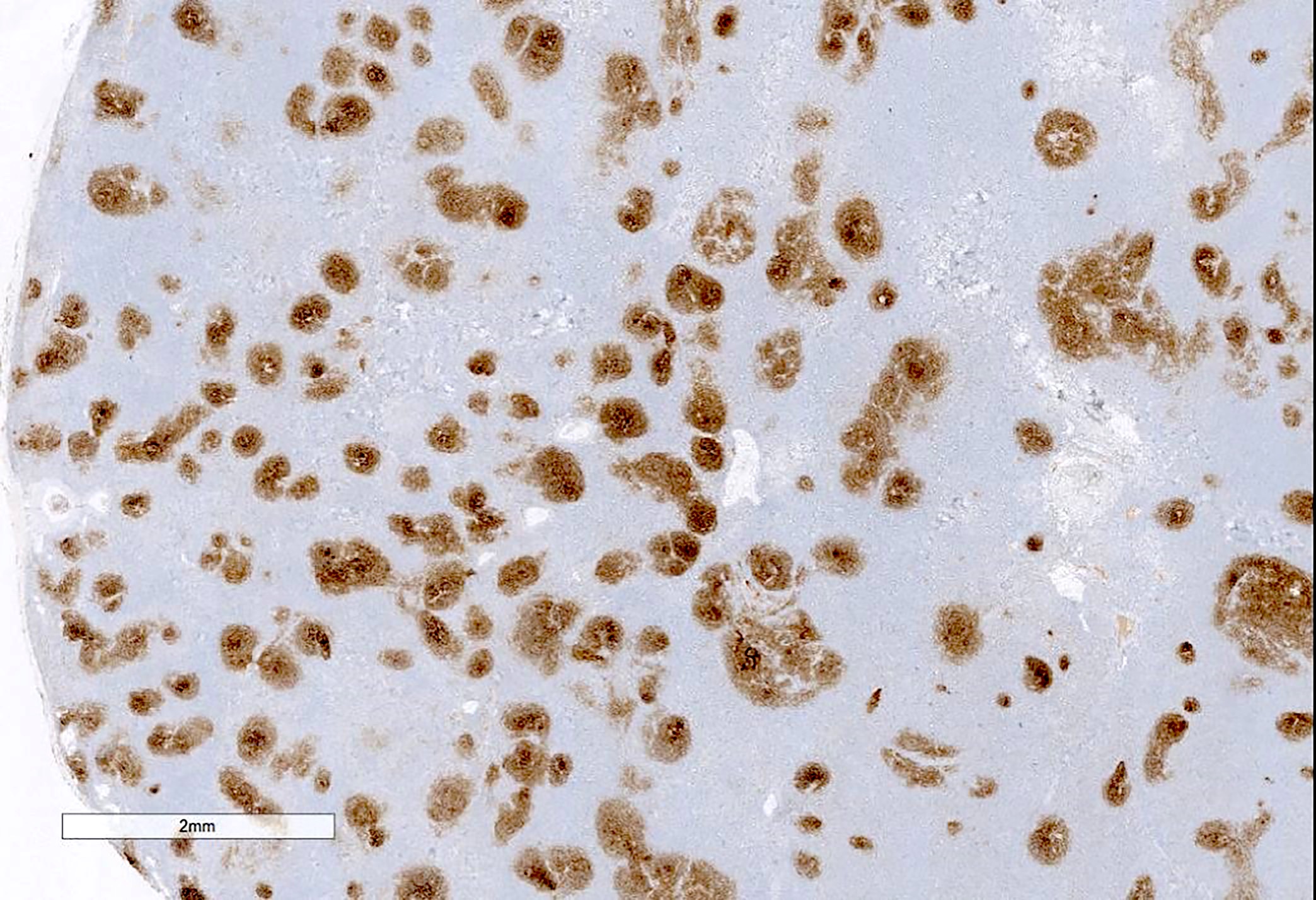
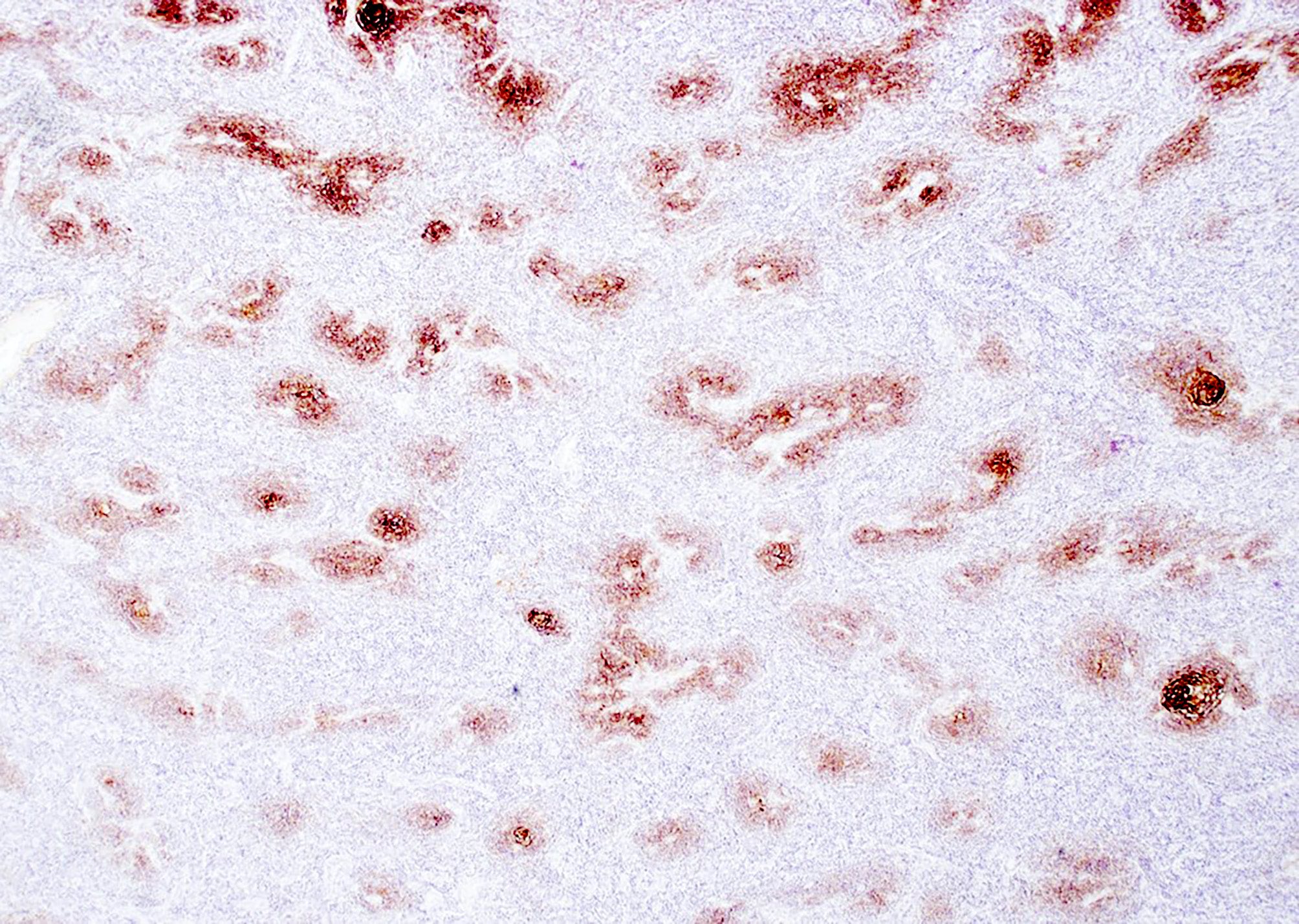
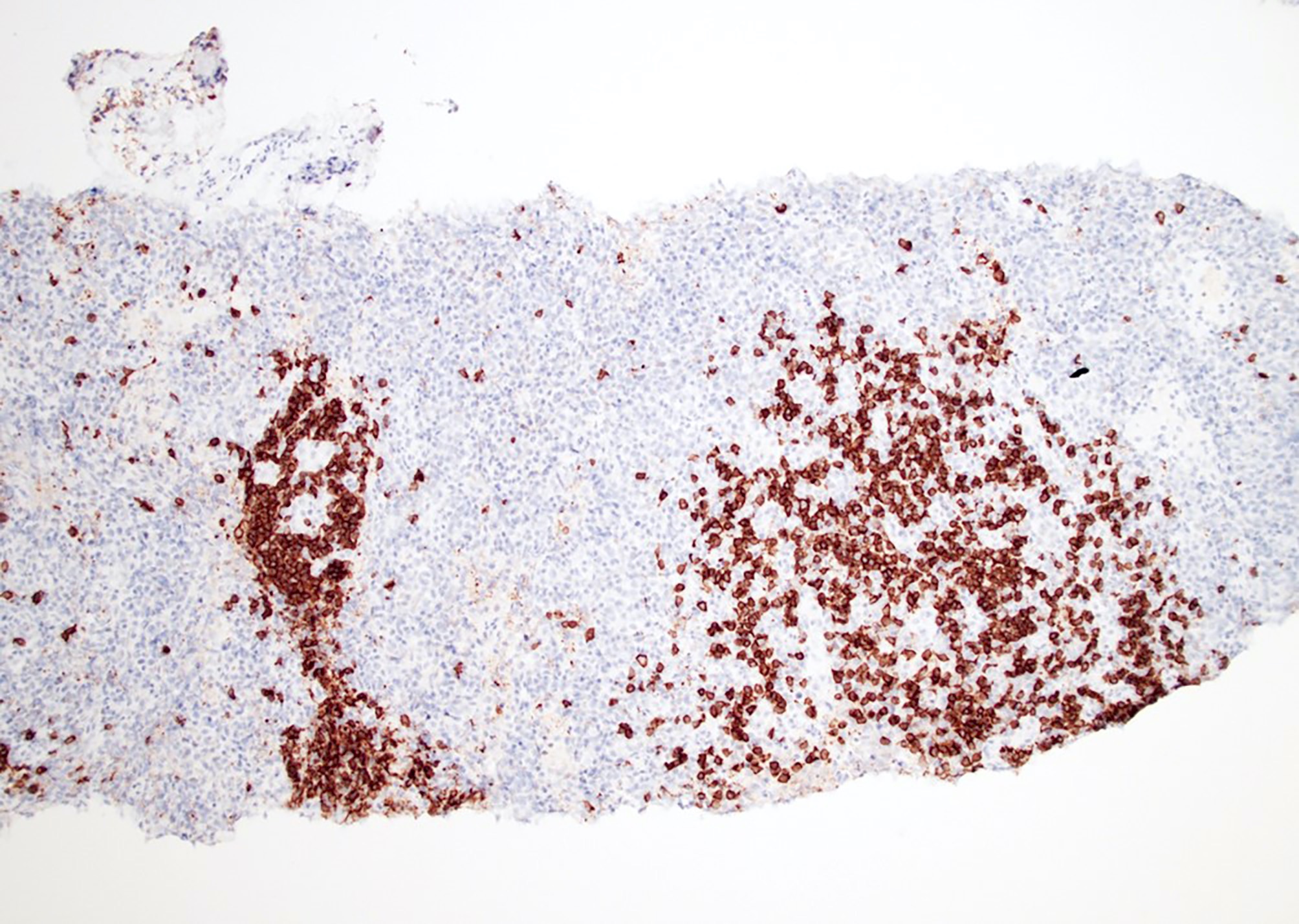
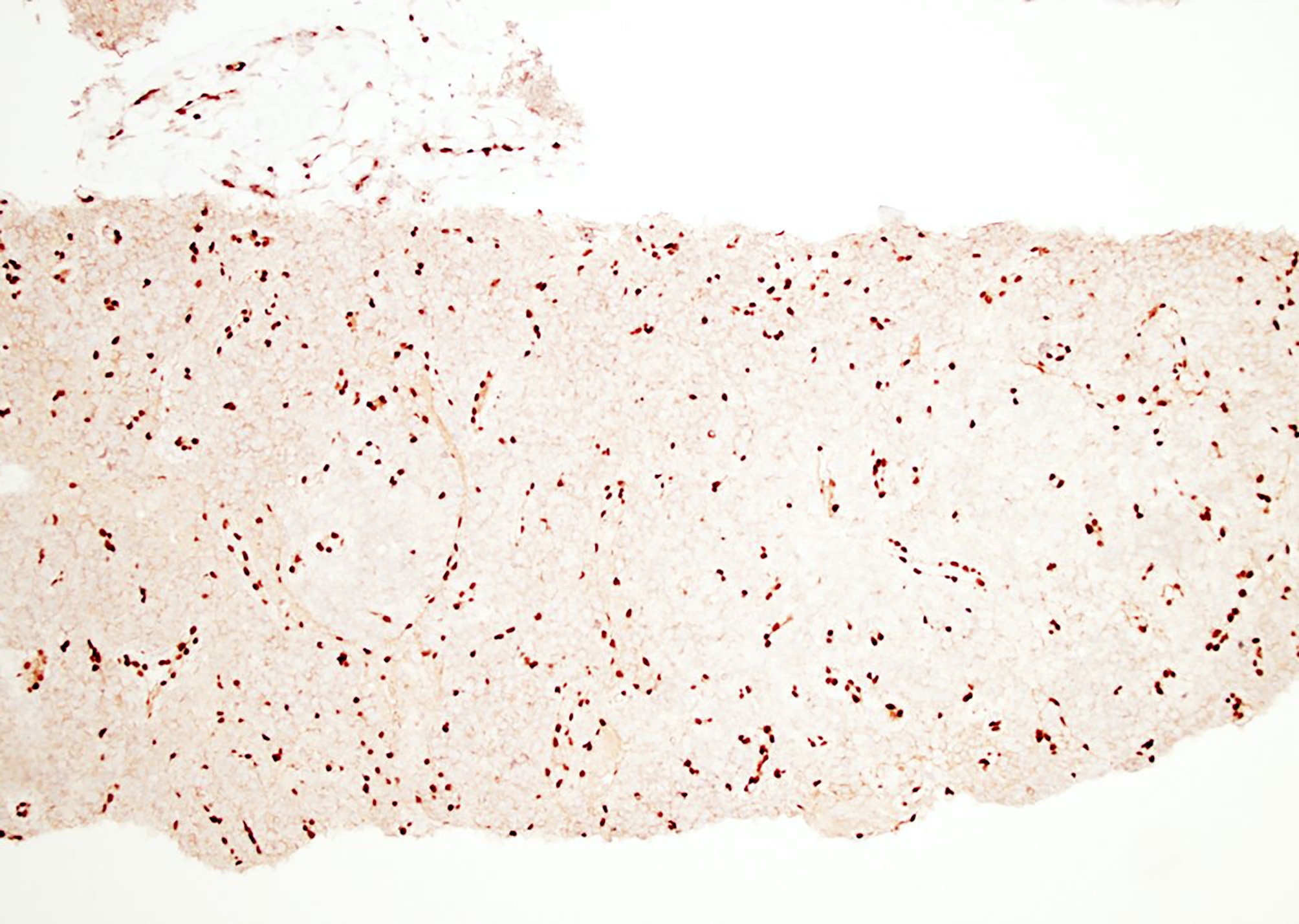
HHV8+ cells
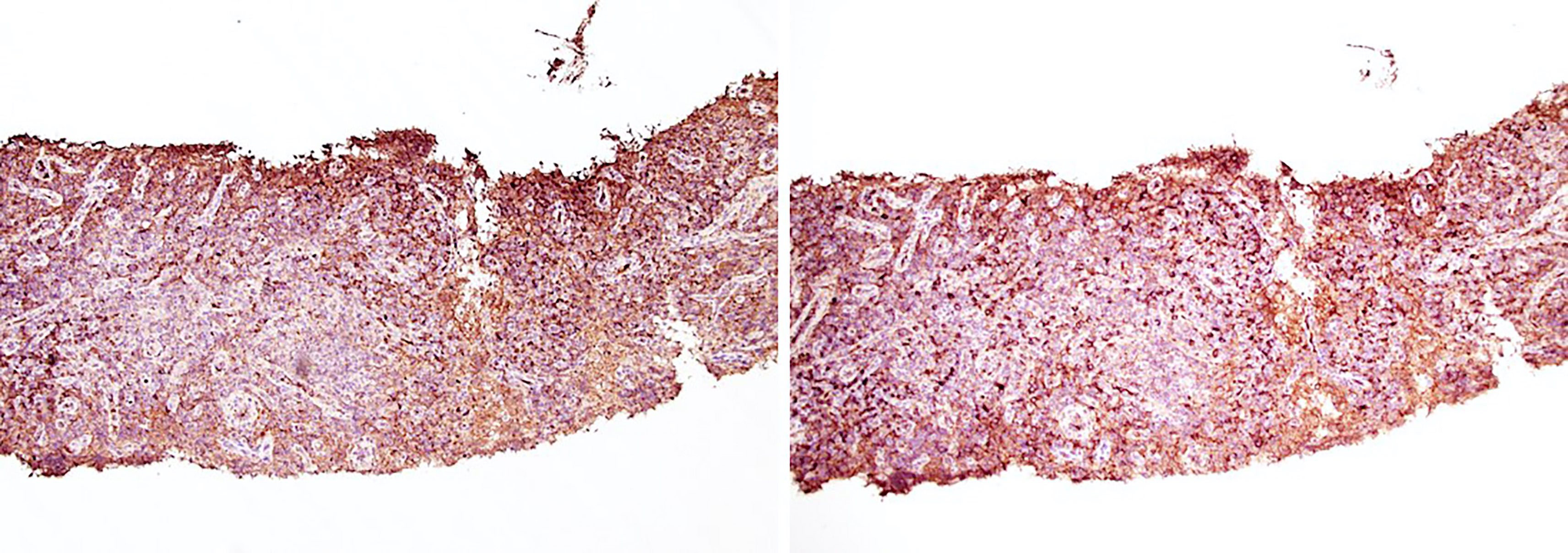
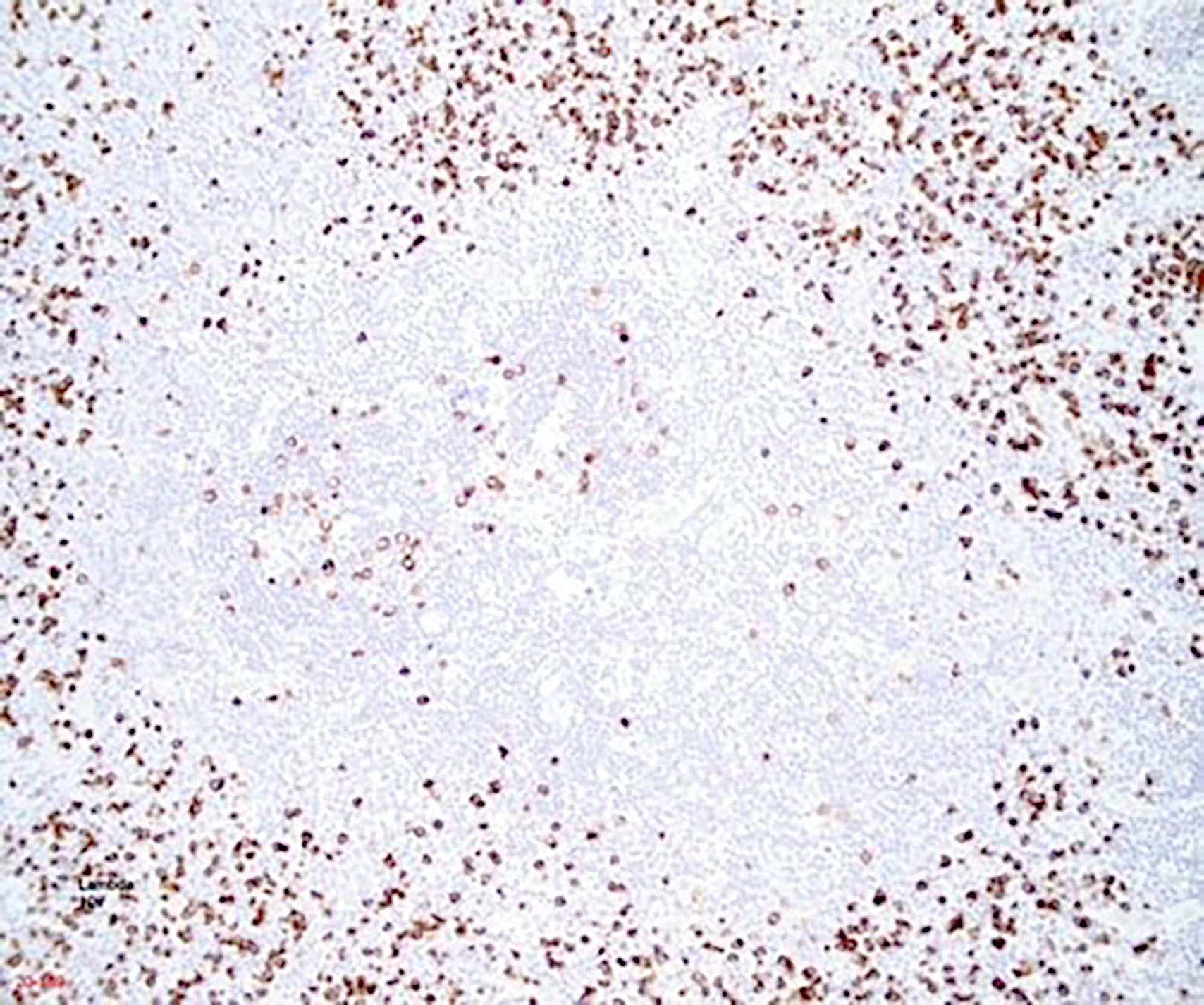
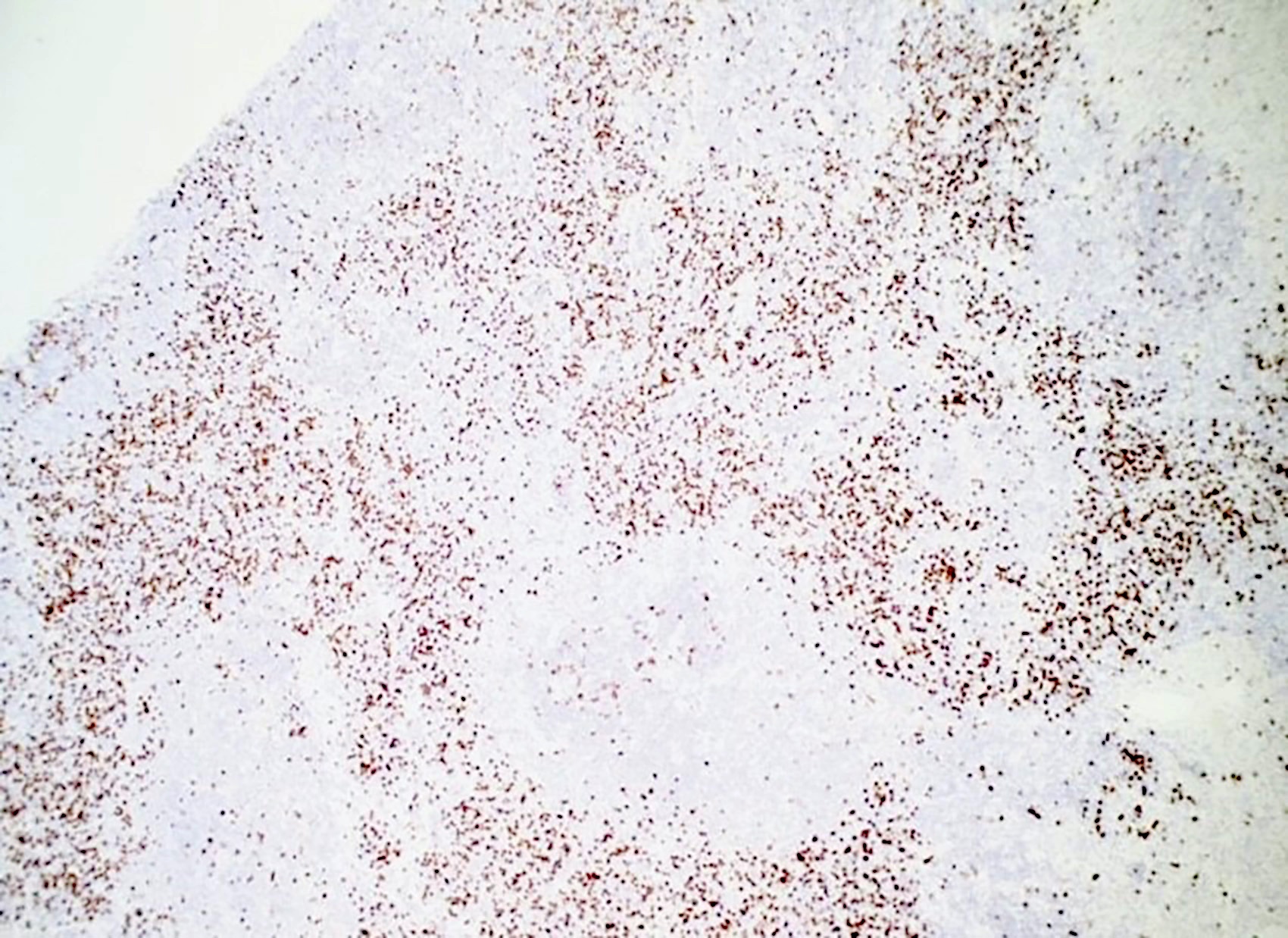
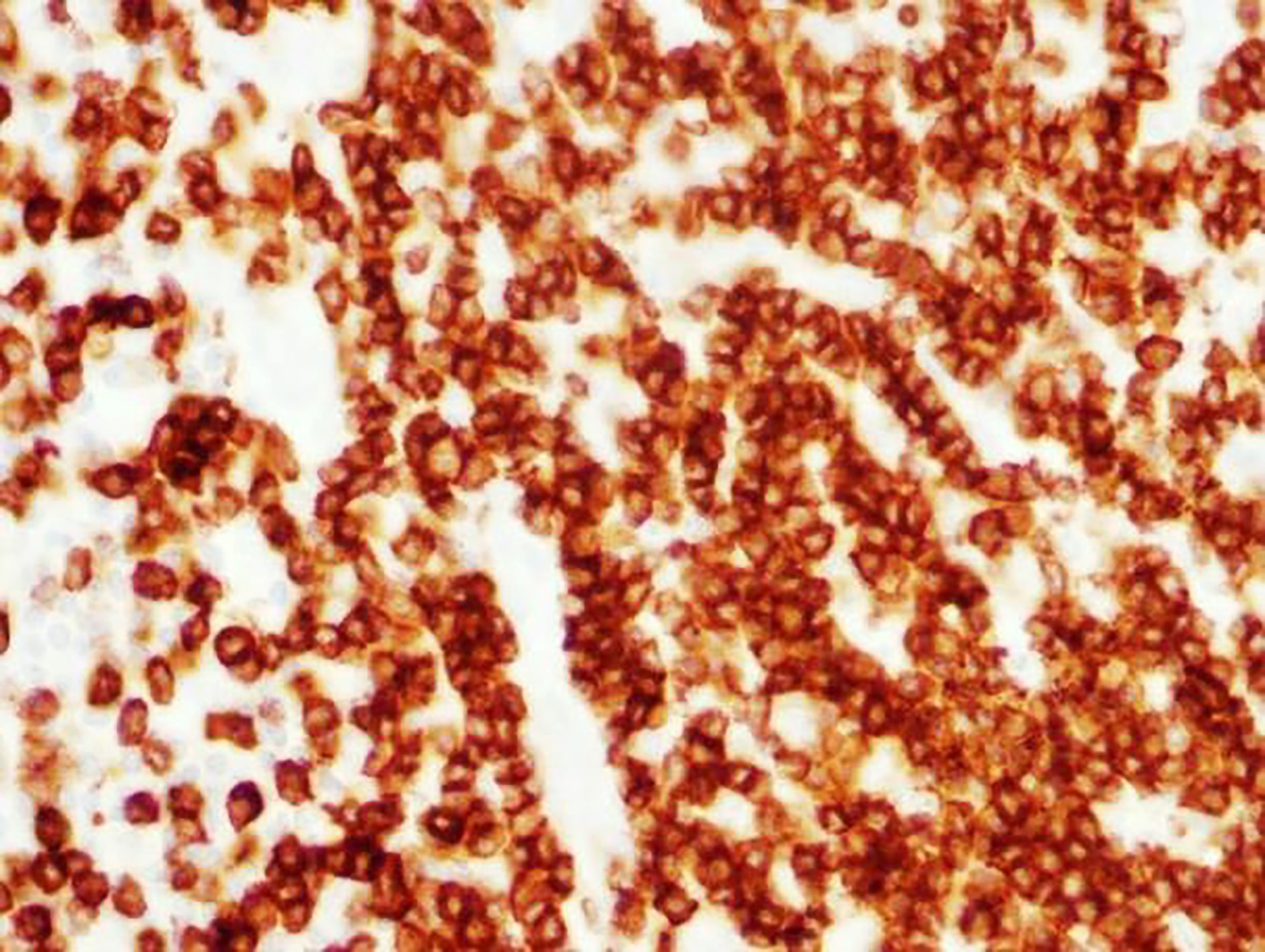
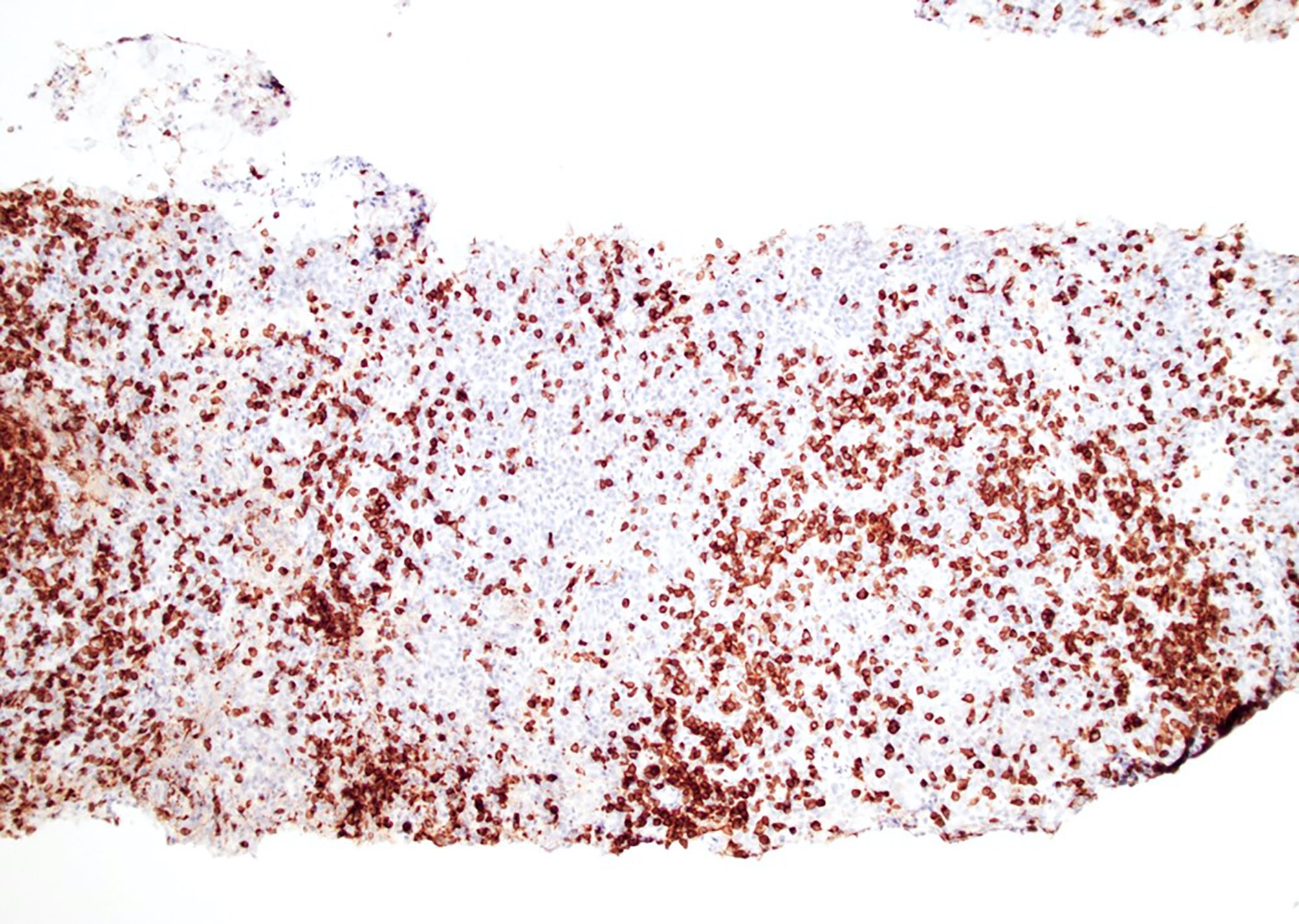
Lambda light chain predominance in plasma cells
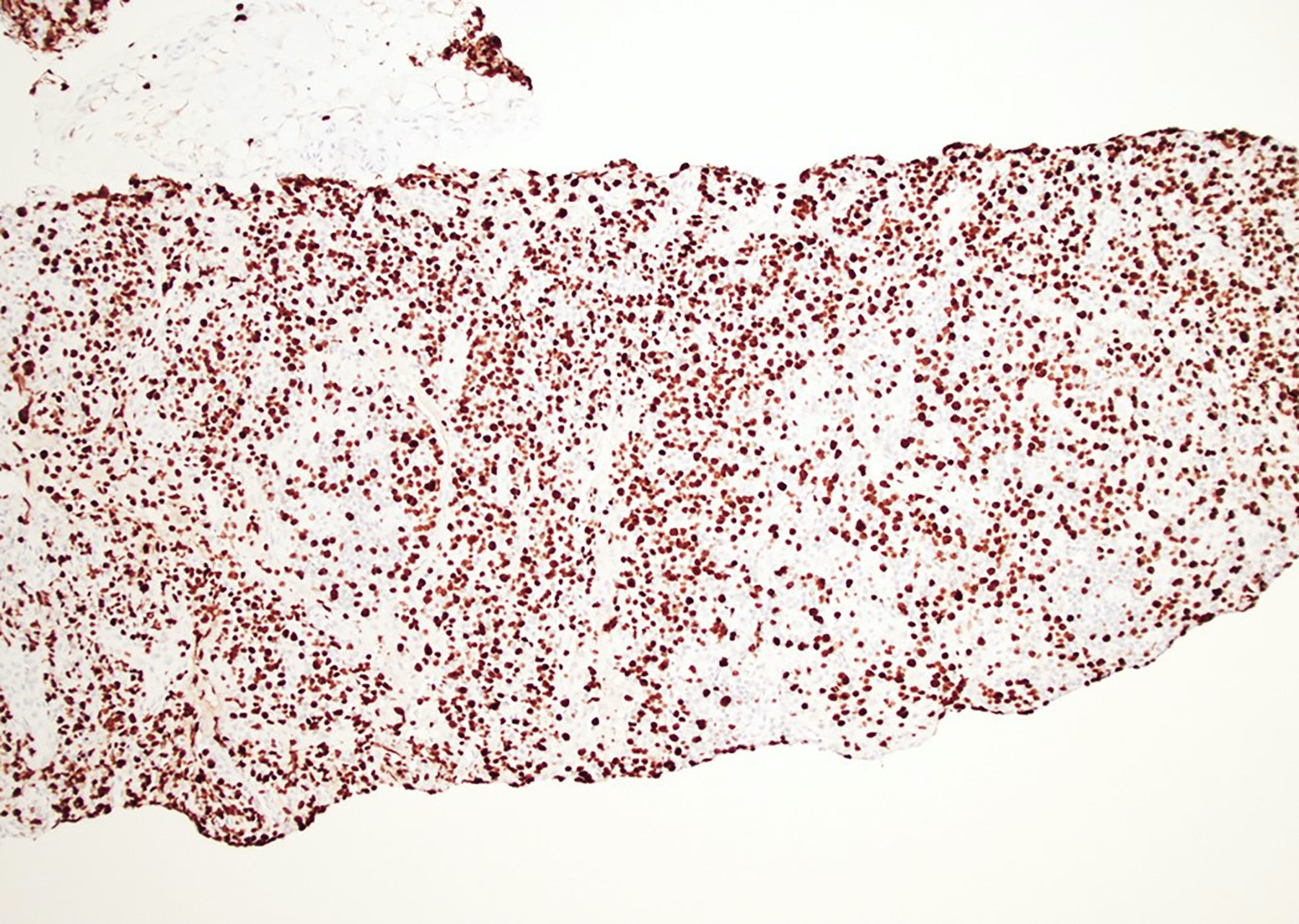
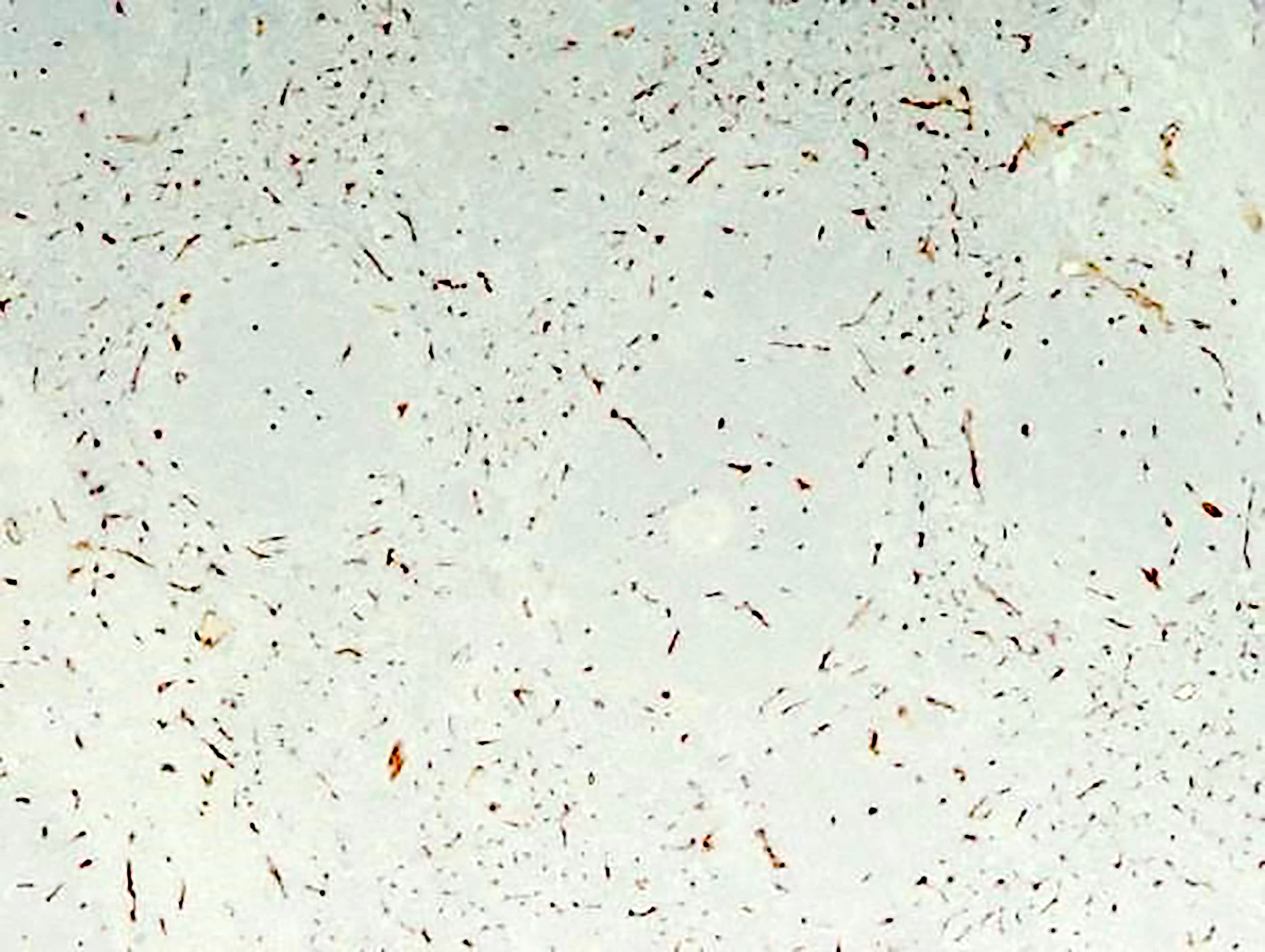
Increased proliferation in interfollicular areas, Ki67
Contributed by Genevieve M. Crane, M.D., Ph.D.

Hyaline vascular Castleman

HHV8+ multicentric Castleman
Images hosted on other servers:

HVCD
- HVCD (Surg Pathol Clin 2019;12:849)
- PCCD (Histopathology 1989;14:333)
- Clusters of plasma cells in the interfollicular areas: CD138, polytypic light chains
- HHV8 MCD (Hum Pathol 2001;32:95, PLoS Pathog 2018;14:e1006967)
- HHV8-LANA1, viral IL6, lambda light chain, cytoplasmic IgM, OCT2, BLIMP1 and IRF4 / MUM1
- Serum concentrations of IL2, IL4, IL6, IL10, TNFα and IFNγ cytokines can be evaluated by flow cytometry (J Med Virol 2021;93:4033)
- HVCD
- Subset of cases shows clonal cytogenetic abnormalities: t(1;16)(p11;p11), t(1;22)(p22;q13) and t(7;8)(qter;q12) (Am J Surg Pathol 2000;24:882)
- In about 75% of cases studied HUMARA gene assays show monoclonal pattern (loss of heterozygosity) (Mod Pathol 2014;27:823)
- MCD
- Monoclonal IGH rearrangement in subset of cases (more common in HIV positive patients with HHV8 infection) (Am J Pathol 1988;131:84)
- B and T lymphocytes in Castleman disease are usually polyclonal (Histopathology 2006;48:233)
- Lymph node, left axillary, excisional biopsy:
- Kaposi sarcoma and HHV8 positive multicentric Castleman disease (see comment and report)
- Comment: The patient has a history of HIV / AIDS and presents with generalized lymphadenopathy and fever. The lymph node shows morphologic features consistent with plasma cell type Castleman disease and focal involvement by Kaposi sarcoma. Flow cytometry shows no evidence of an immunophenotypically abnormal lymphocyte or plasma cell population and molecular analysis to evaluate presence of clonal B cell population is negative ruling out B cell lymphoma and plasma cell neoplasm.
- Systemic lupus erythematosus:
- Follicular hyperplasia, interfollicular expansion of lymphocytes and immunoblasts, and numerous plasma cells within germinal centers and medullary cords
- Coagulative necrosis with abundant karyorrhectic debris and histiocytes
- Hematoxylin bodies
- Serological diagnosis of systemic lupus erythematosus
- Rheumatoid arthritis:
- Can resemble HVCD or PCCD
- Follicular hyperplasia, interfollicular and intrafollicular plasmacytosis and neutrophils within sinuses
- Lacks thickened mantle zones, twinning of germinal centers and piercing vessels
- Clinical and serological diagnosis of autoimmune disease
- Hemophagocytic lymphohistiocytosis:
- Proliferation of benign histiocytes in the sinuses
- Lymphocyte depletion may be seen
- Phagocytosed red cells or white cells
- Adult onset Still disease (Medicine (Baltimore) 2015;94:e787):
- Paracortical hyperplasia or mixed follicular and paracortical hyperplasia
- Vascular proliferation and immunoblasts
- Pericapsular endarteritis
- Clinical and serologic diagnosis of adult onset Still disease
- IgG4 disease (Semin Diagn Pathol 2012;29:226):
- Fibroinflammatory disorder with dense lymphoplasmacytic infiltrates containing numerous IgG4+ plasma cells
- 5 different histological patterns - type resemble MCD
- Hyperplastic and regressed follicles, some with penetrating vessels
- Interfollicular areas with numerous plasma cells
- Serological diagnosis
- Follicular dendritic cell sarcoma:
- Plasma cell neoplasm:
- Monoclonal plasma cells
- HIV associated lymphadenitis:
- Clinical and serological diagnosis of HIV infection
- Angioimmunoblastic T cell lymphoma, early stages:
- Follicular lymphoma:
- Mantle cell lymphoma:
- Reactive lymph node enlargement:
- Lack characteristic histological features of CD
- Can show different histological patterns: follicular hyperplasia, sinus histiocytosis, interfollicular / mixed and diffuse patterns
What is the histopathological feature seen in this lymph node?
- Dysplastic dendritic cells
- Immunoblasts
- Plasma cell infiltrates
- Twinning of germinal centers
Comment Here
Reference: Castleman disease
- Burkitt lymphoma
- EBV positive diffuse large B cell lymphoma, NOS
- Follicular lymphoma
- HHV8 positive large B cell lymphoma
Comment Here
Reference: Castleman disease
