
Lymphoma & related disorders
HHV8 associated lymphoproliferative disorders
HHV8 positive DLBCL, NOS
Editorial Board Member: Roberto N. Miranda, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.

Last author update: 6 September 2022
Last staff update: 2 January 2025
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: HHV8 related diffuse large B cell lymphoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Saksena A, Jaffe ES. HHV8 positive DLBCL, NOS. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaHHV8DLBCL.html. Accessed April 3rd, 2025.
Definition / general
- HHV8 related diffuse large B cell lymphoma (DLBCL) is a neoplasm characterized by a monoclonal proliferation of HHV8 infected lymphoid cells that resemble plasmablasts and express IgM lambda
- Neoplastic cell corresponds to a naïve IgM producing B cell without immunoglobulin somatic hypermutations
Essential features
- Usually arises in association with multicentric Castleman disease (MCD) and HIV infection
- Morphologically similar to plasmablasts but correspond to naïve IgM producing B cell without somatic hypermutations
- Sheets of HHV8 latency associated nuclear antigen (LANA1) positive plasmablasts efface lymph node architecture
- Atypical cells are strongly positive for cytoplasmic IgM with lambda light chain restriction and negative for EBV encoded small RNA (EBER)
Terminology
- HHV8+ large B cell lymphoma arising in multicentric Castleman disease (obsolete)
- HHV8 positive plasmablastic lymphoma (obsolete)
- HHV8+ diffuse large B cell lymphoma, not otherwise specified
ICD coding
- ICD-O: 9738/3 - large B cell lymphoma arising in HHV8 associated multicentric Castleman disease
- ICD-10:
- C83.3 - diffuse large B cell lymphoma
- C83.30 - diffuse large B cell lymphoma, unspecified site
- C83.31 - diffuse large B cell lymphoma, lymph nodes of head, face and neck
- C83.32 - diffuse large B cell lymphoma, intrathoracic lymph nodes
- C83.33 - diffuse large B cell lymphoma, intra-abdominal lymph nodes
- C83.34 - diffuse large B cell lymphoma, lymph nodes of axilla and upper limb
- C83.35 - diffuse large B cell lymphoma, lymph nodes of inguinal region and lower limb
- C83.36 - diffuse large B cell lymphoma, intrapelvic lymph nodes
- C83.37 - diffuse large B cell lymphoma, spleen
- C83.38 - diffuse large B cell lymphoma, lymph nodes of multiple sites
- C83.39 - diffuse large B cell lymphoma, extranodal and solid organ sites
- ICD-11: 2A81.Y - other specified diffuse large B cell lymphomas (large B cell lymphoma arising in HHV8 associated multicentric Castleman disease)
Epidemiology
- Rare disease with overall frequency of 0.1% (Leuk Lymphoma 2018;59:1375)
- Median age is 47 years (range 39 - 66); M:F = 3.3:1 (Pathology 2020;52:53)
- Usually arises in association with HHV8 positive multicentric Castleman disease (MCD) and HIV (15 times higher risk) (Blood 2002;99:2331)
Sites
- Characteristically involves lymph nodes or spleen
- Can disseminate to other viscera including liver, lungs and gastrointestinal tract
- Can also manifest as a leukemia with involvement of peripheral blood (Blood 2002;99:2331)
Pathophysiology
- HHV8 infects singly scattered cells that are morphologically similar to plasmablasts with abundant cytoplasmic immunoglobulin but are, in fact, naïve IgM producing B cells that lack IG somatic hypermutations and are polyclonal at the molecular level
- HHV8 positive plasmablasts form aggregates (microlymphomas), which can be polyclonal or monoclonal (Am J Clin Pathol 2017;147:171)
- HHV8 positive aggregates rarely can expand to HHV8 positive large B cell lymphoma, which is monoclonal
Etiology
- By definition, the large plasmablastic cells in all cases are positive for HHV8
- Molecular mechanism is similar to other HHV8 positive entities (Blood 2004;104:3349)
Clinical features
- Usually manifests with profound immunodeficiency, enlarging lymph nodes and massive splenomegaly
- There may be manifestations of Kaposi sarcoma (Blood 2002;99:2331)
- Rarely, may arise in absence of MCD (Mod Pathol 2017;30:745)
Diagnosis
- Biopsy of involved lymph node with immunohistochemistry
- Effacement of lymph node architecture by sheets of HHV8 positive, LANA1 positive and EBER negative plasmablasts (Am J Clin Pathol 2017;147:171)
Laboratory
- Rarely, there is involvement of bone marrow and peripheral blood by HHV8 positive IgM lambda plasmablasts (Eur J Haematol 2013;91:497)
Prognostic factors
- Extremely aggressive clinical course and poor prognosis
Case reports
- 37 and 42 year old men with multifocal hepatic Kaposi sarcoma and intravascular HHV8 positive (EBV negative) systemic DLBCL, NOS (Autops Case Rep 2020;10:e2020206)
- 56 year old man with an unusual EBV associated HHV8 positive large B cell lymphoma (Clin Case Rep 2019;7:587)
- 59 year old woman with hemoglobin sickle cell disease and sequential development of HHV8 positive DLBCL and chronic myelomonocytic leukemia (Pathol Res Pract 2019;215:152704)
Treatment
- No definite treatment guidelines
- Can be treated with the same regimens described for patients with HIV associated DLBCL
Gross description
- Involved lymph node is enlarged
- Firm, fleshy mass
Microscopic (histologic) description
- Effacement of lymph node / splenic architecture by confluent sheets of large plasmablastic cells
- Large plasmablastic cells have amphophilic cytoplasm and vesicular, often eccentrically placed nuclei containing 1 or 2 prominent nucleoli (Am J Clin Pathol 2017;147:171)
- High mitotic activity
Microscopic (histologic) images
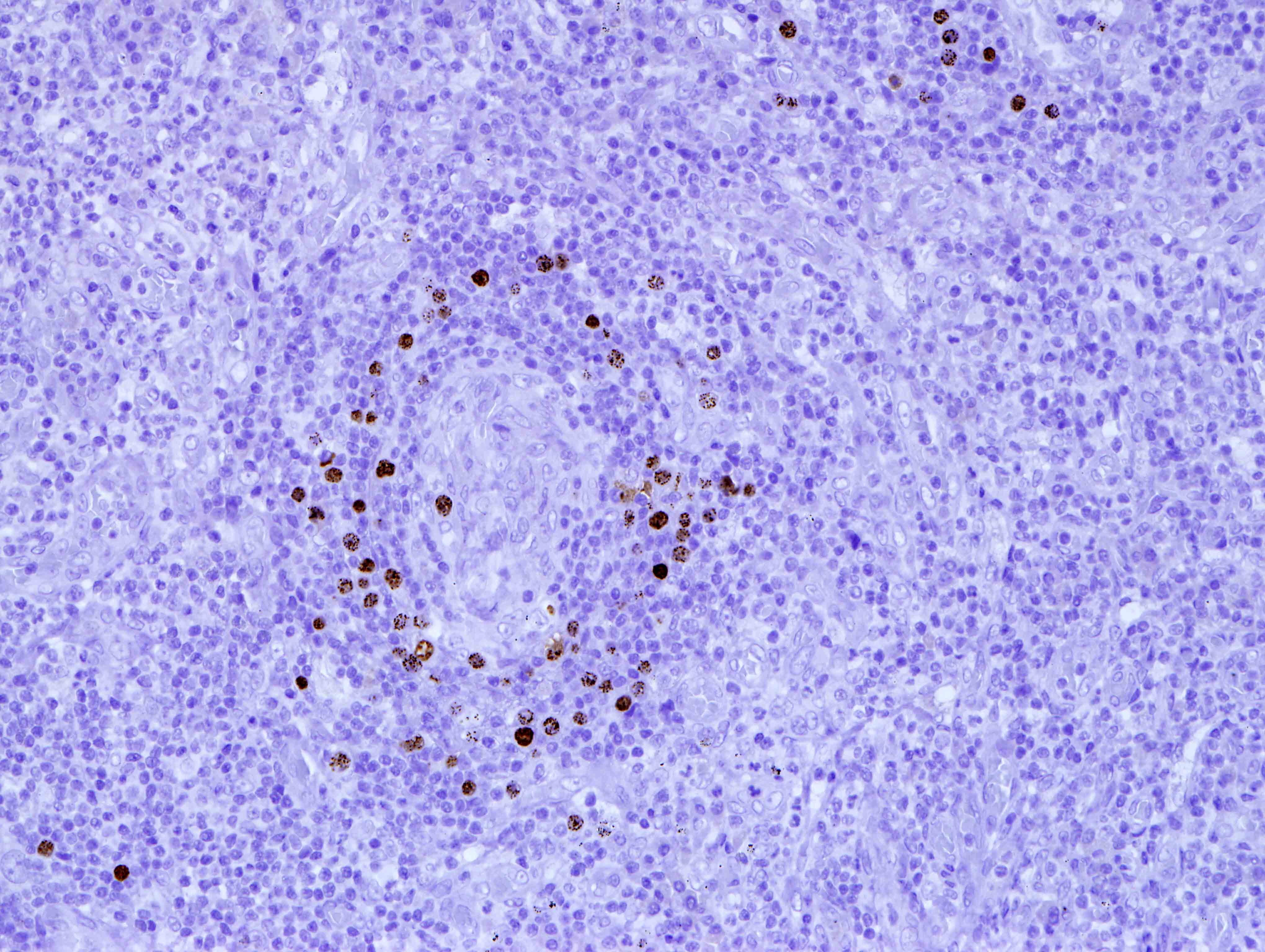
Contributed by Annapurna Saksena, M.B.B.S, M.D. and Elaine S. Jaffe, M.D.
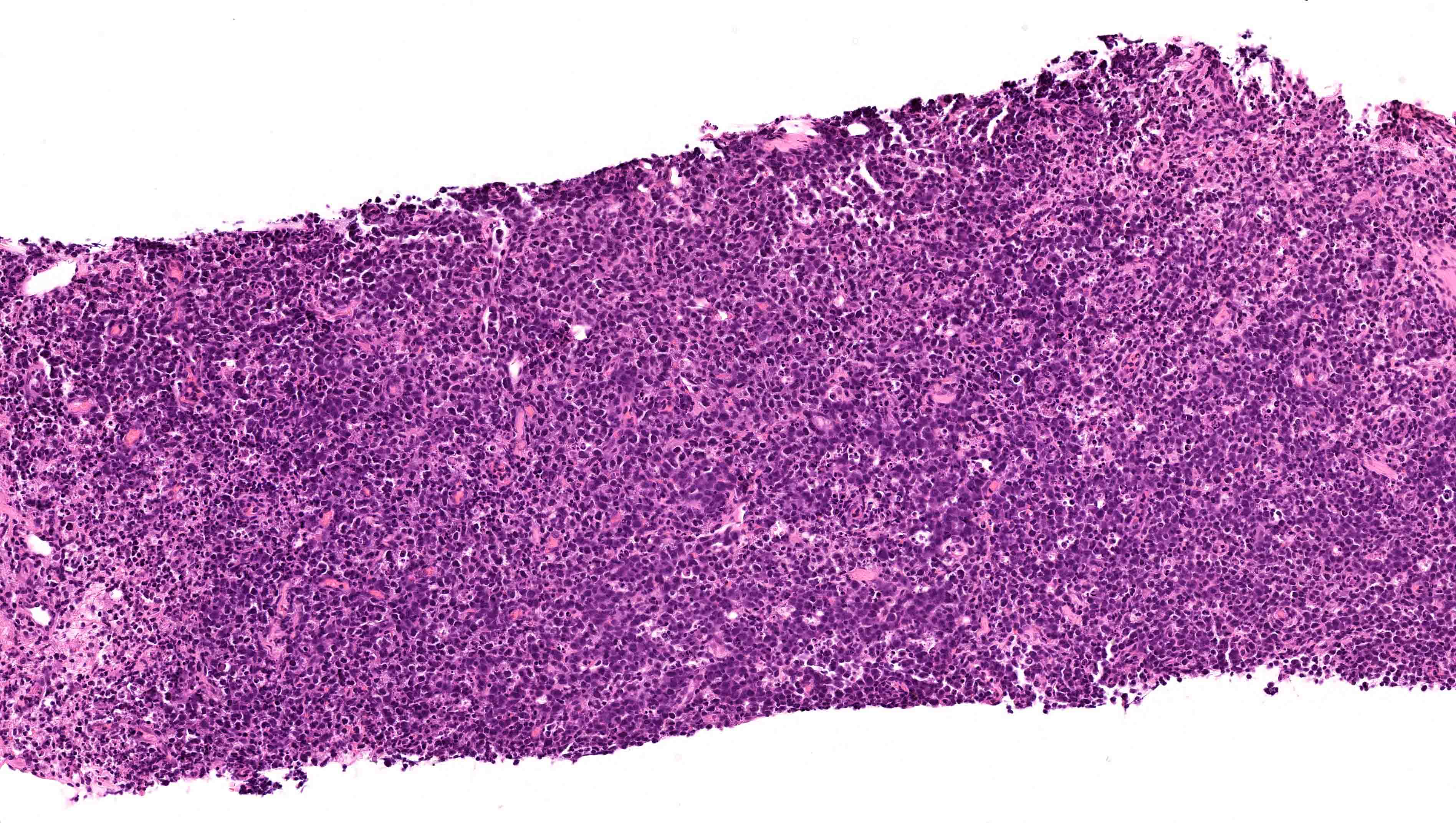
Diffuse growth pattern

Atypical large lymphoid cells
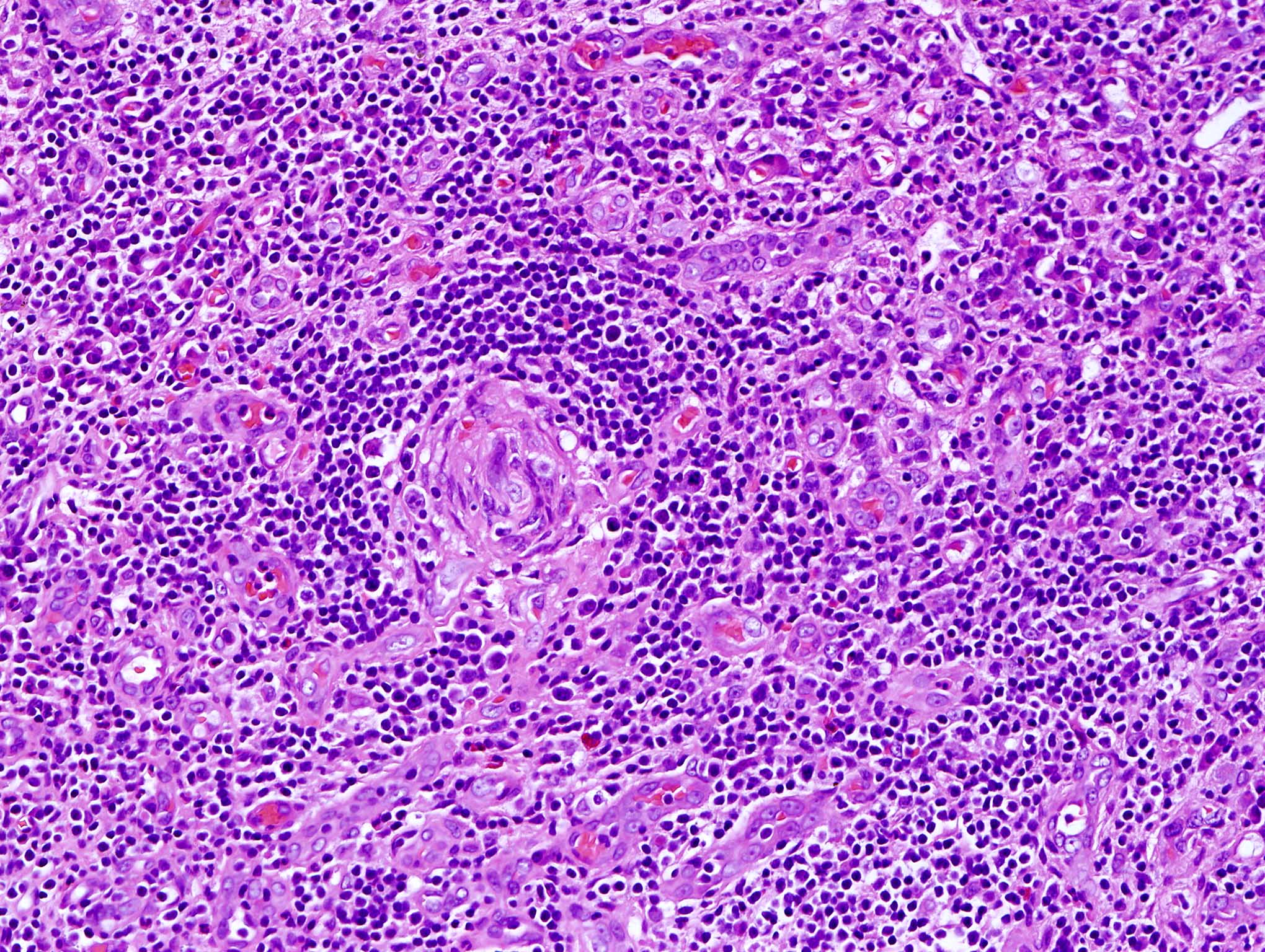
Multicentric Castleman disease
Multicentric Castleman disease, HHV8
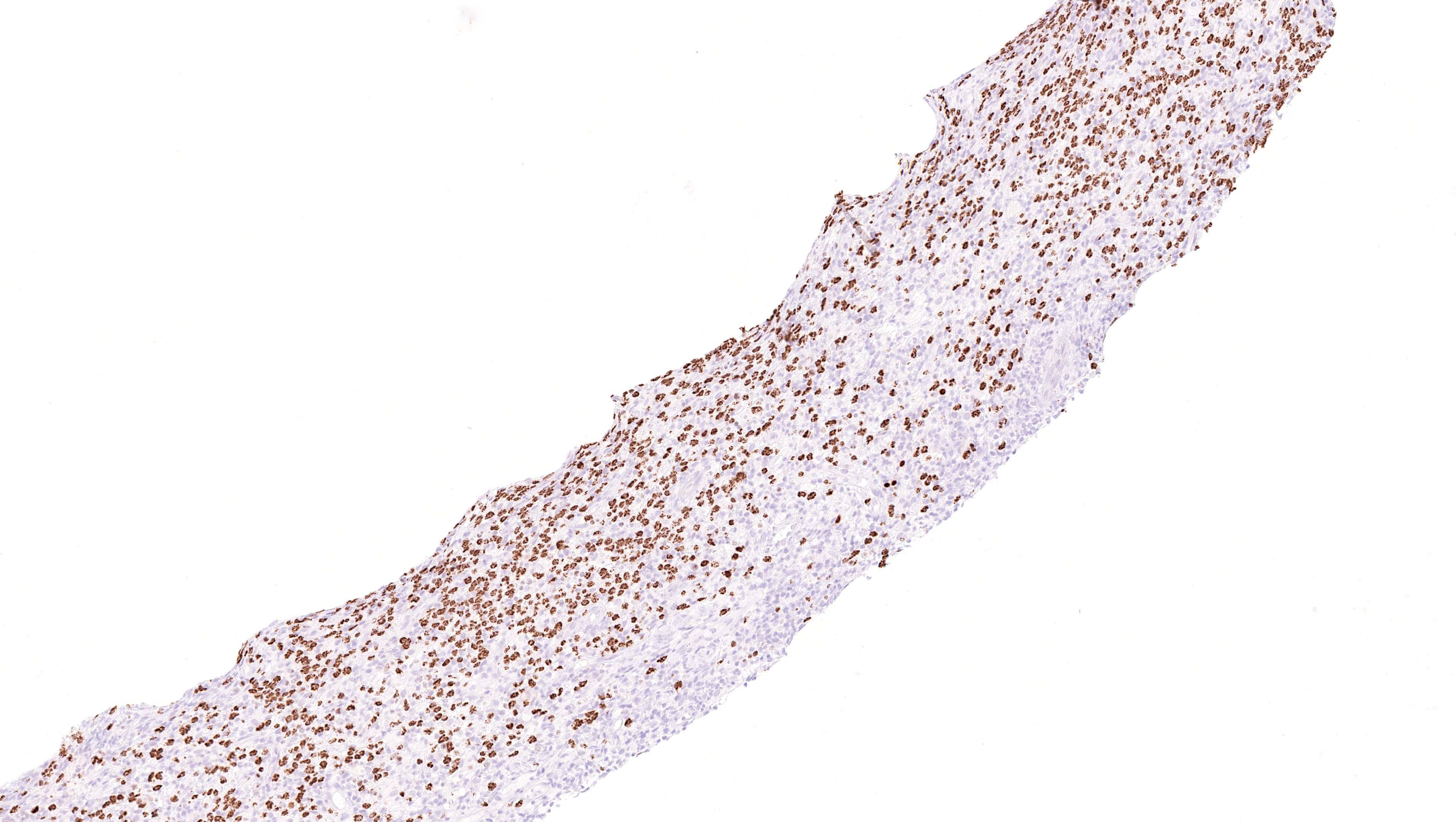
HHV8 LANA positive atypical cells
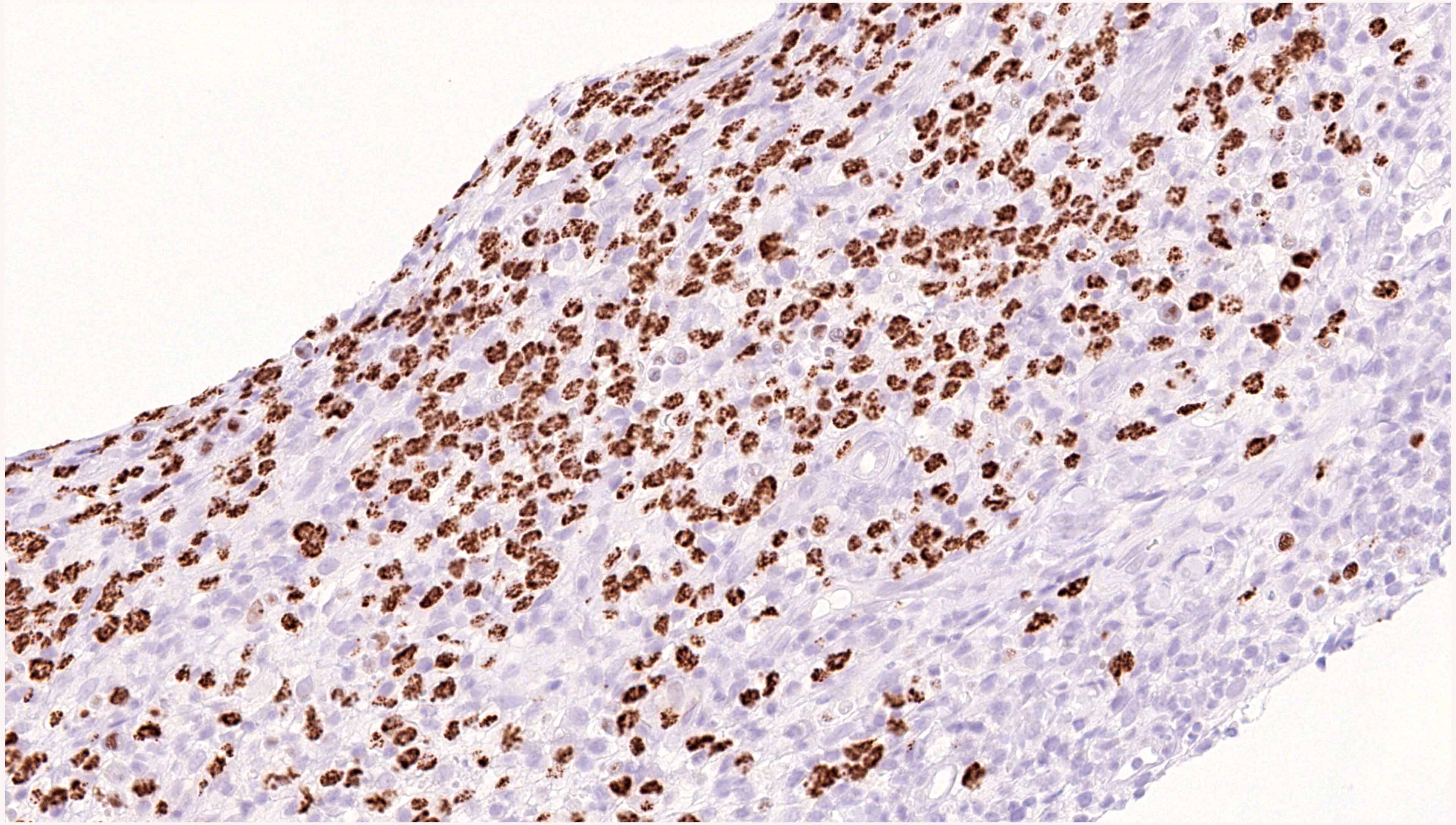
HHV8 LANA nuclear staining
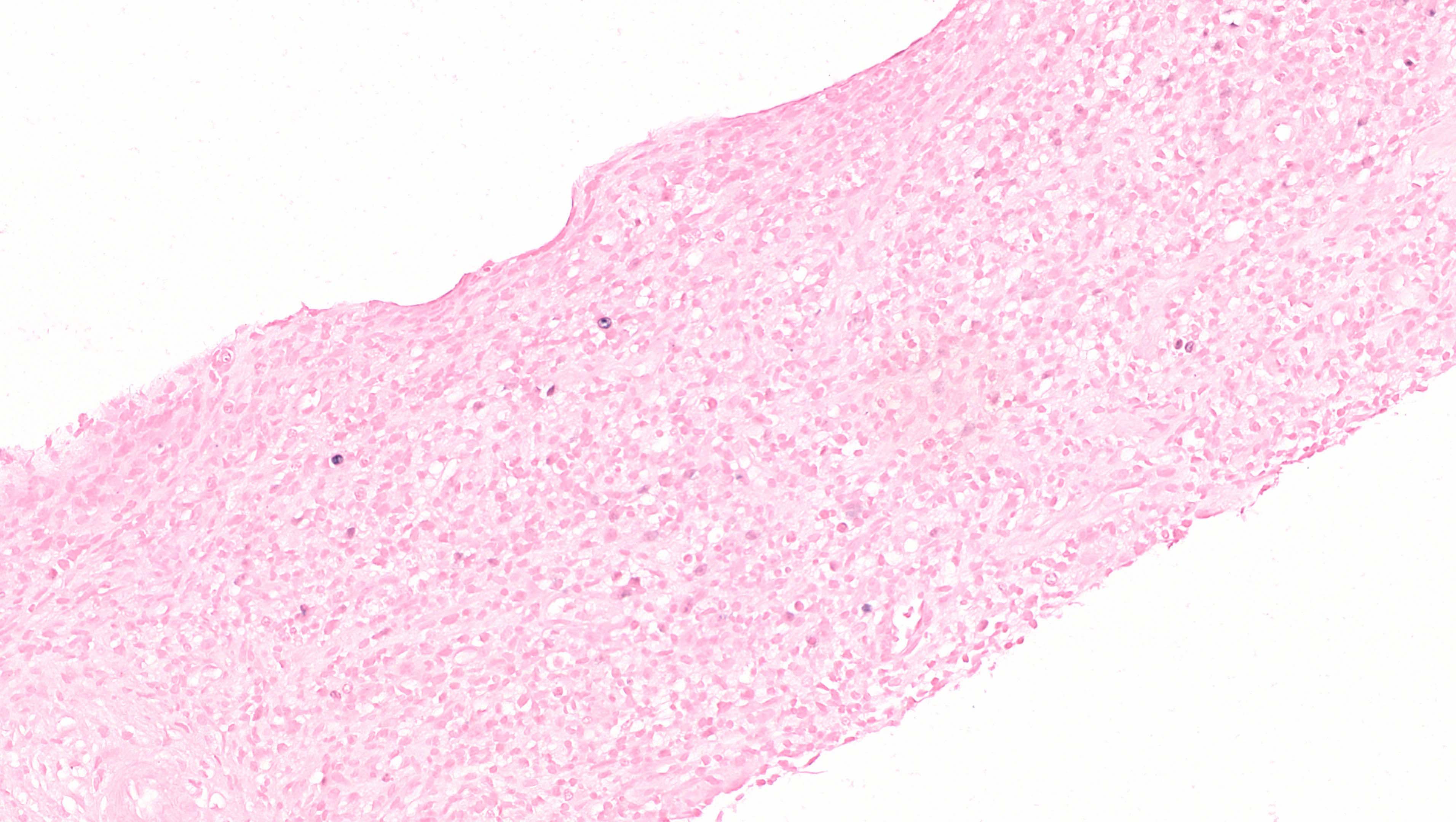
EBER ISH negative atypical cells
Positive stains
- Stippled nuclear staining for HHV8 (LANA1) in large plasmablasts in all cases
- Strongly express cytoplasmic IgM with lambda light chain restriction (Blood 2002;99:2331)
- MUM1
- CD20 and CD38 may be positive
Negative stains
Molecular / cytogenetics description
- PCR reveals a monoclonal B cell population
- Immunoglobulin (IG) genes are unmutated, lacking somatic hypermutation
Sample pathology report
- Lymph node, right cervical, excision:
- Diffuse large B cell lymphoma, HHV8 positive, NOS
Differential diagnosis
- Extracavitary primary effusion lymphoma (Am J Surg Pathol 2004;28:1401):
- HHV8+ multicentric Castleman disease (MCD) (Blood 2014;123:2924, Blood 2001;97:2130):
- Often presents with generalized lymphadenopathy and constitutional symptoms
- Abnormal follicles with varied degree of hyalinization and involution of germinal centers
- Widened concentric rings of mantle zones (onion skinning) and prominent penetrating venules
- Interfollicular plasma cell hyperplasia
- Plasmablasts predominantly in mantle zones and lambda light chain restricted
- Polyclonal pattern of IG rearrangement
- HHV8 related germinotropic lymphoproliferative disorder (Blood 2002;100:3415, Ann Pathol 2014;34:373):
- Occurs in immunocompetent patients
- HIV-
- Localized or sometimes multifocal lymph node involvement
- Retention of lymph node architecture with HHV8+ plasmablasts involving or replacing germinal centers
- EBER+, CD38+, kappa or lambda light chain restriction
- Polyclonal or oligoclonal pattern of IGH rearrangement
- Favorable response to chemotherapy or radiation
- Plasmablastic lymphoma (Histopathology 2012;61:1183, Am J Surg Pathol 2010;34:1686):
- Often presents in oral cavity or extranodal sites
- Association with immunodeficiency or HIV
- EBER+, HHV8-
- Usually expresses a plasma cell phenotype (CD38+, CD138+, MUM1+)
- Cytoplasmic immunoglobulin positive (mostly IgG and kappa / lambda)
- Frequently class switched and hypermutated IG genes
- MYC translocation in approximately 50% of cases
Additional references
Board review style question #1
What pattern on HHV8 staining (shown above) is considered positive in HHV8 related diffuse large B cell lymphoma (DLBCL), NOS?
- Cytoplasmic
- Golgi region
- Homogenous nuclear
- Membranous
- Stippled nuclear
Board review style answer #1
Board review style question #2
Which of the following is true about HHV8 related diffuse large B cell lymphoma (DLBCL), NOS?
- Clonal rearrangement pattern with somatic hypermutation of IG genes
- Clonal rearrangement pattern without somatic hypermutation of IG genes
- Polyclonal rearrangement pattern with somatic hypermutation of IG genes
- Polyclonal rearrangement pattern without somatic hypermutation of IG genes
Board review style answer #2
B. Clonal rearrangement pattern without somatic hypermutation of IG genes
Comment Here
Reference: HHV8 related DLBCL, NOS
Comment Here
Reference: HHV8 related DLBCL, NOS
