
Lymphoma & related disorders
Mature T/NK cell disorders
Aggressive NK/T cell disorders
EBV+ nodal T and NK cell lymphoma
Editorial Board Member: Roberto N. Miranda, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 4 January 2024
Last staff update: 4 January 2024
Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed search: EBV+ nodal T and NK cell lymphoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Stone M, Bladek P, Murga-Zamalloa CA. EBV+ nodal T and NK cell lymphoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaEBVposnodalTNKcell.html. Accessed April 2nd, 2025.
Definition / general
- Primary nodal lymphomas composed of NK or mature T cells with EBV infection in immunocompetent individuals
Essential features
- Primary nodal T cell lymphoma with EBV positive tumor cells in immunocompetent patients
- Tumor cells have high grade morphology and frequently show large cells with vesicular nuclei
- These cases largely represent neoplastic expansions of EBV positive cytotoxic T cell lymphocytes (usually CD8+ with coexpression of TIA1 and granzyme B)
- The majority of cases have been reported in Asia, are usually diagnosed at an advanced stage and feature a poor median survival time of 3 - 8 months
Terminology
- EBV positive nodal T or NK cell lymphoma
- Epstein-Barr virus associated primary nodal T / NK cell lymphoma
ICD coding
Epidemiology
- Active EBV infection in the neoplastic T or NK cells
- Immunocompetent individuals
- Most cases reported are in East Asia
- M:F = 1.5 - 4:1
- More common in older adults (median age: 59 - 64)
- References: Haematologica 2018;103:278, Am J Surg Pathol 2015;39:462, Haematologica 2022;107:1864, Hum Pathol 2015;46:981
Sites
- By definition, this is a primary nodal disease; concomitant extranodal involvement may occur in the bone marrow, spleen and liver (Hum Pathol 2015;46:981, Am J Surg Pathol 2015;39:462, Int J Hematol 2016;104:591, Histopathology 2012;61:186, J Clin Exp Hematop 2020;60:30)
Pathophysiology
- Most of the cases derive from cytotoxic T cell lymphocytes
Etiology
- Epstein-Barr virus is essential (Best Pract Res Clin Haematol 2013;26:15, J Clin Exp Hematop 2020;60:30)
Clinical features
- Splenomegaly
- B symptoms
- Thrombocytopenia
- Pleural effusion or ascites
- Lymphadenopathy
- References: Hum Pathol 2015;46:981, Am J Surg Pathol 2015;39:462, J Clin Exp Hematop 2020;60:30
Diagnosis
- Histological and immunohistochemical examination of lymph node biopsies
Laboratory
- Thrombocytopenia
- Elevated serum lactate dehydrogenase
- Anemia
- References: Am J Surg Pathol 2015;39:462, Hum Pathol 2015;46:981, Histopathology 2012;61:186
Prognostic factors
- Poor prognosis, with a median survival of 2.5 - 8 months (Hum Pathol 2015;46:981, Haematologica 2018;103:278, Haematologica 2022;107:1864, Am J Surg Pathol 2015;39:462, J Clin Exp Hematop 2020;60:30)
Case reports
- 56 year old man with a single enlarged lymph node (Int J Lab Hematol 2022;44:232)
- 69 year old woman with stage IIIb disease involving multiple lymph nodes (Front Oncol 2021:11:706865)
Treatment
- Limited data with no standardized treatment
- No apparent benefit with use of etoposide or anthracycline based chemotherapy approaches
- Poor response to chemotherapy (Hum Pathol 2015;46:981)
Microscopic (histologic) description
- Diffuse proliferation of atypical lymphocytes with effacement of the nodal architecture
- Generally, without conspicuous coagulative necrosis and angioinvasion
- Neoplastic cells are generally pleomorphic, medium to large and a subset of the tumor cells feature anaplastic morphology
- References: Am J Surg Pathol 2015;39:462, Hum Pathol 2015;46:981
Microscopic (histologic) images
Contributed by Carlos A. Murga-Zamalloa, M.D.

Diffuse atypical infiltrate

Morphological atypia

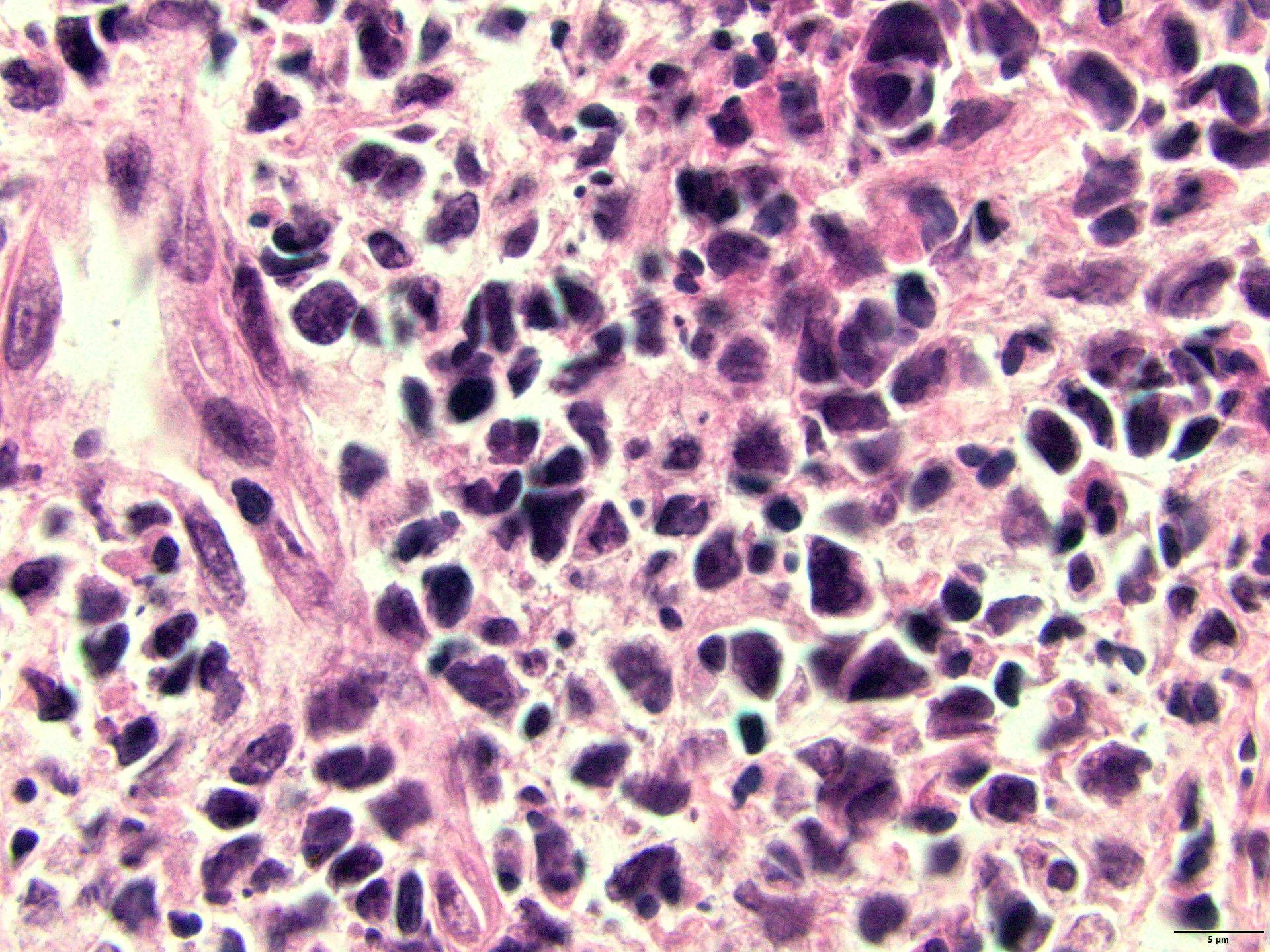
Pleomorphic infiltrate
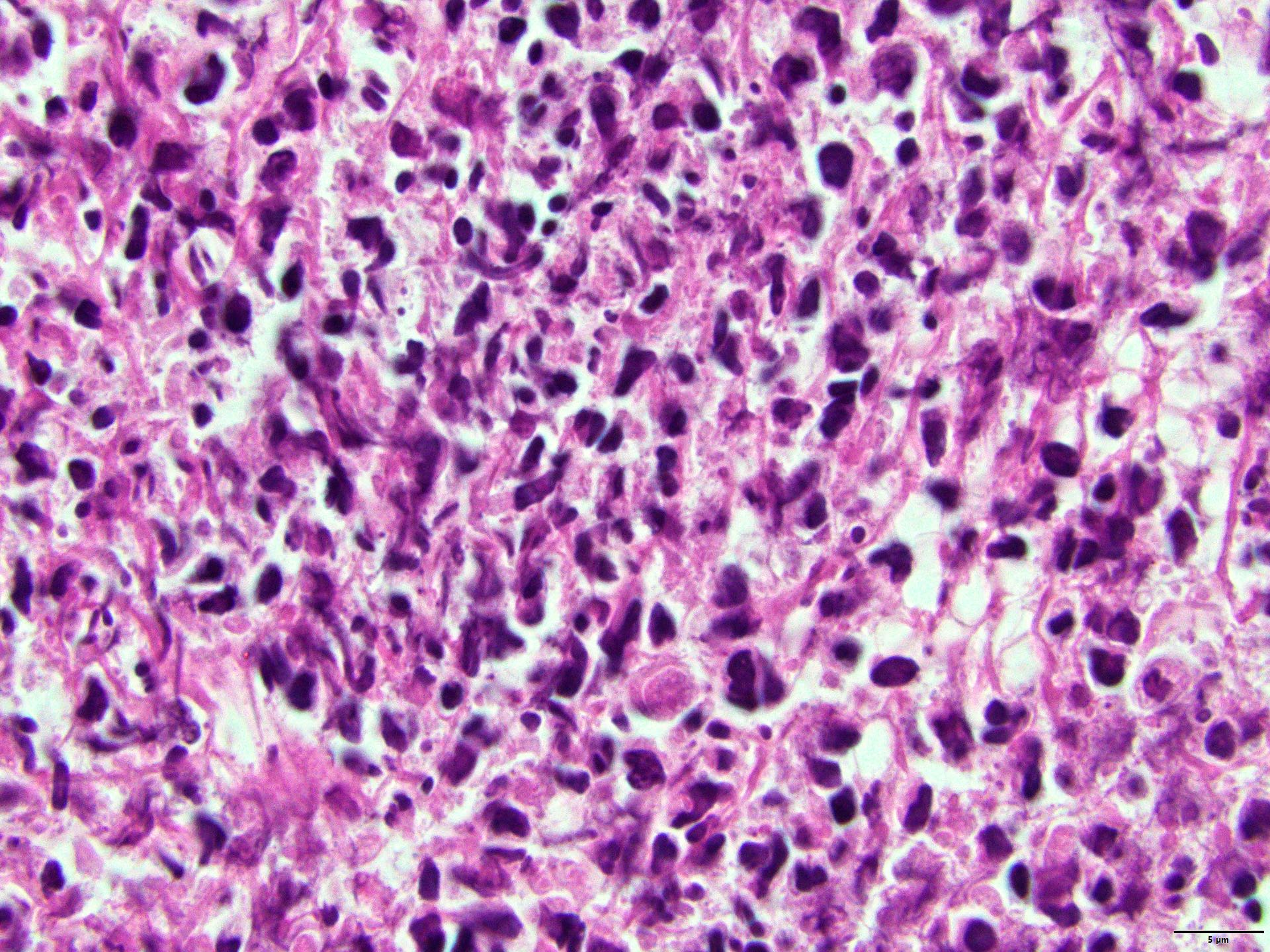
Pleomorphism and marked cellular atypia

EBV positive lymphocytes (EBER in situ hybridization)
Positive stains
- ~90% of the cases reported are CD3+ / CD8+; cases composed of double CD4 / CD8 negative T cells account for ~5 - 10% of the reported cases and those composed by CD4+ / CD8- T cells represent < 5% of the reported cases
- EBV expression (detected by EBER in situ hybridization) is present in at least 30% of the tumor cells
- Cytotoxic markers: TIA1, granzyme B
- TCR alpha / beta (46 - 53% of the cases) > TCR gamma / delta (0 - 13% of the cases)
- CD30 expression can be detected in a small subset of the tumor cells in 20 - 35% of the reported cases
- References: Int J Hematol 2016;104:591, Am J Surg Pathol 2015;39:462, Hum Pathol 2015;46:981, Histopathology 2012;61:186, Pathol Res Pract 2013;209:448
Negative stains
- B cell antigens (CD20, PAX5, CD79a)
- CD4 and CD5 are frequently negative (antigen loss)
- CD56 is negative in most reported cases (90 - 95%)
- Perforin is negative in 80 - 90% of cases
- References: Int J Hematol 2016;104:591, Am J Surg Pathol 2015;39:462, Hum Pathol 2015;46:981, Histopathology 2012;61:186, Pathol Res Pract 2013;209:448
Molecular / cytogenetics description
- Clonal TCR gene rearrangements are detected by PCR testing in 75 - 85% of cases
- Cytogenetic aberrancies include loss of 14q11.2, loss of 13q14.3, loss of 1q32.1 and Xp22.33
- References: Am J Surg Pathol 2015;39:462, Haematologica 2018;103:278
Sample pathology report
- Right axillary lymph node, excisional biopsy:
- Involved by nodal EBV positive NK / T cell lymphoma (see comment)
- Comment: In situ hybridization for EBV (EBER) shows reactivity in > 30% of the atypical cells.
- The neoplastic cells feature a cytotoxic immunophenotype (TIA1 / CD8 positive)
- The overall findings are consistent with EBV+ nodal NK / T cell lymphoma
Differential diagnosis
- Extranodal NK / T cell lymphoma (Am J Surg Pathol 2015;39:462, Haematologica 2018;103:278):
- Primarily involves extranodal sites; most commonly the nasal cavity, nasopharynx, oropharynx, Waldeyer ring and epiglottis
- Often shows conspicuous coagulative necrosis and angioinvasion
- Commonly CD56 positive
- Aggressive NK cell leukemia (Cancers (Basel) 2020;12:2900, Blood Cancer J 2017;7:660):
- Angioimmunoblastic T cell lymphoma (Hum Pathol 2020:102:104):
- Systemic EBV positive T cell lymphoma (SETBL) of childhood (Pathol Int 2022;72:376, Am J Hematol 2002;70:31):
- Affects mainly pediatric populations or young adults and usually develops following a primary EBV infection
- Primarily involves the bone marrow, liver and spleen; secondary involvement of lymph nodes can be present
- Morphologically, SETBL may feature small to medium size lymphocytes with no to mild cytological atypia; however, most cases show medium to large atypical lymphocytes
- Neoplastic lymphocytes are positive for EBV and usually feature a cytotoxic immunophenotype
Additional references
Board review style question #1
The image depicts EBER in situ hybridization in a lymph node. Which of the following is true regarding EBV+ nodal T and NK cell lymphoma?
- EBV is positive in background nonneoplastic B cells
- Expression of the cytotoxic marker TIA1 and granzyme B is usually absent
- Most cases are CD3 / CD4 positive, while CD3 / CD8 positive cases are infrequent
- TCR alpha / beta is more common than TCR gamma / delta expression
- Usually features a good prognosis with response to anthracycline based chemotherapy
Board review style answer #1
D. TCR alpha / beta is more common than TCR gamma / delta expression. More cases feature TCR alpha / beta expression (~50%) rather than TCR gamma / delta (5%). Answer A is incorrect because in contrast to angioimmunoblastic T cell lymphoma, EBV infection drives the oncogenic process and is positive in the neoplastic T cells and not in the background B cell lymphocytes. Answer B is incorrect because this subtype of T cell lymphoma is characterized by the expansion of cytotoxic T cell lymphocytes with frequent expression of TIA1 and granzyme B. Answer C is incorrect because most cases reported feature neoplastic T cells that are CD3 / CD8 positive; < 5% reported feature CD3 / CD4 positive neoplastic T cells. Answer E is incorrect because patients with a diagnosis of EBV+ nodal T and NK cell lymphoma have poor response to standard chemotherapeutic agents and a median survival of 3 - 8 months.
Comment Here
Reference: EBV+ nodal T and NK cell lymphoma
Comment Here
Reference: EBV+ nodal T and NK cell lymphoma
Board review style question #2
The image depicts EBER in situ hybridization in a lymph node. Which of the following is true regarding EBV+ nodal T / NK cell lymphoma?
- By definition, > 80% EBER positivity of the tumor cells are required for the diagnosis of EBV+ nodal T / NK cell lymphoma
- Expression of CD30 is detected in most cases
- Mutations in the RHOA gene are frequently detected in this lymphoma
- There is an overlap in immunophenotypic features with systemic EBV positive T cell lymphoma (SETBL) of childhood; however, EBV+ nodal T / NK lymphoma is predominantly detected in adult populations with primarily nodal disease
- This group of T cell lymphomas is clinically characterized by primary orofacial involvement with secondary nodal disease
Board review style answer #2
D. There is an overlap in immunophenotypic features with systemic EBV positive T cell lymphoma (SETBL) of childhood; however, EBV+ nodal T / NK lymphoma is predominantly detected in adult populations with primarily nodal disease. SETBL and EBV+ nodal T / NK lymphoma constitute neoplastic proliferations of cytotoxic T cell lymphocytes; however, SETBL is diagnosed in pediatric populations and EBV+ nodal T / NK lymphoma is predominantly detected in adult populations. Answer A is incorrect because there are no established criteria regarding the percentage of neoplastic T cells for diagnosis; however, many reports included cases with 30% of neoplastic tumor cells positive for EBV by EBER in situ hybridization. Answer B is incorrect because expression of CD30 can be detected in ~20% of the cases and when positive, only a limited number of neoplastic T cells are positive. Answer C is incorrect because mutations in RHOA are predominantly detected in peripheral T cell lymphomas of the T follicular helper type (TFH type), not in EBV+ nodal T / NK lymphomas. Answer E is incorrect because in contrast to extranodal T / NK nasal type lymphoma, EBV+ nodal T / NK lymphoma is primarily nodal without involvement of extranodal sites in the nasal cavity, nasopharynx, oropharynx, Waldeyer ring and epiglottis.
Comment Here
Reference: EBV+ nodal T and NK cell lymphoma
Comment Here
Reference: EBV+ nodal T and NK cell lymphoma
