
Bone & joints
Other tumors
Erdheim-Chester disease
Authors: Aishwarya Ravindran, M.D., Karen L. Rech, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 21 April 2020
Last staff update: 27 August 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed search: Erdheim-Chester disease [title] pathology review[ptyp]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ravindran A, Rech KL. Erdheim-Chester disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneerdheim.html. Accessed April 2nd, 2025.
Definition / general
- Rare, clonal histiocytosis with frequent multiorgan involvement
- First described in 1930 by William Chester and Jakob Erdheim
- Previously thought to be an inflammatory disorder, recognized as a neoplasm in WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues in 2016 (Swerdlow: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Edition, 2017)
Essential features
- Correlation of clinical features, histology and radiological findings are essential for diagnosis (Blood 2016;127:2672)
- Systemic disease with frequent involvement of bone, retroperitoneum (hairy kidney, coated aorta), CNS and lung (Blood 2016;127:2672)
- Clinical features and disease outcomes depend on the site(s) involved
- BRAF V600E mutation in > 50% of cases (Blood 2012;120:2700)
Terminology
- Previous known as lipoid (cholesterol) granulomatosis
- Also known as polyostotic sclerosing histiocytosis
- Classified in the ‘L’ group under the revised classification of histiocytic disorders (Blood 2016;127:2672)
ICD coding
- ICD-10: E88.89 - Erdheim-Chester disease
Epidemiology
- Median age at diagnosis: 57 years (range 16 - 80) (Blood 2011;117:2778)
- Rare in children and adolescents (Ped Hem Onc 2017;2:59)
- M:F = 3:1
Sites
- Skeletal involvement in almost all (> 95%) cases, most often in the long bones of the lower extremities
- Extraskeletal disease frequent (50 - 60%) in the retroperitoneum, kidneys, cardiovascular system, lung (Blood 2016;127:2672)
- Central nervous system and pituitary involvement (20 - 30%) (Blood 2016;127:2672)
- Cutaneous involvement in 25%, orbit and testis involvement are rare (Br J Dermatol 2020;182:405)
Etiology
- Activating mutations of the mitogen activated kinase (MAPK) pathway leads to tissue accumulation of histiocytes with increased expression of cytokines (Blood 2014;124:483, Arthritis Rheum 2006;54:4018, Rheumatology (Oxford) 2010;49:1203)
- Sera of Erdheim-Chester disease patients demonstrate a unique inflammatory cytokine signature with elevated levels of interferon (IFN)-α, interleukin (IL)-12, monocyte chemotactic protein-1 and decreased IL-4 and IL-7, suggestive of a Th-1-mediated systemic immune response (Blood 2011;117:2783)
- Increased prevalence of myeloid neoplasms among Erdheim-Chester disease patients that may be clonally related, suggestive of a clonal hematopoietic precursor (Br J Hematol 2019;187:e51, Hematologica 2020;105:e84)
Clinical features
- Heterogeneous clinical course ranging from asymptomatic to progressive, lethal disease (Blood 2016;127:2672)
- Skeletal involvement presents with bone pain predominantly in the distal extremities
- Cardiovascular involvement is usually asymptomatic, diagnosed only on imaging (Arch Pathol Lab Med 2004; 128:682)
- Retroperitoneal fibrosis may be complicated by bilateral hydronephrosis with sparing of the pelvic ureters and inferior vena cava (Rheum Dis Clin North Am 2013; 39:299)
- Pulmonary involvement is often asymptomatic but may present with cough or dyspnea
- Pituitary involvement most often presents with central diabetes insipidus and may predate diagnosis by a decade or more
- Central nervous system involvement predominantly manifests as cerebellar and pyramidal syndromes (J Neurol 2006. 253:1267)
- Cutaneous involvement may present with perioibital xanthelasma-like lesions (Br J Dermatol 2020;182:405)
- Orbital involvement may produce pain, blindness, exophthalmos and oculomotor nerve dysfunction
Diagnosis
- Correlation of clinical and histopathologic features along with radiologic and molecular findings are essential for diagnosis; see associated sections (Blood 2020 Mar 18 [Epub ahead of print], Mayo Clin Proc 2019; 94:2054)
- Erdheim-Chester disease may be associated with other histiocytic neoplasms, including Langerhans cell hisitocytosis and Rosai-Dorfman disease which should be confirmed by biopsy in the setting of atypical clinical manifestations (Blood 2020 Mar 18 [Epub ahead of print], Blood 2014;124:1119, Hematologica 2020;105:e5)
Radiology description
- Bilateral and symmetrical cortical osteosclerosis of the diaphyseal and metaphyseal parts of the long bones, predominantly the distal femur and proximal tibia (Rheum Dis Clin North Am 2013; 39:299)
- Symmetrical and abnormally intense labelling of the long bones of the legs and rarely arms on 99Tc bone scintigraphy (Rheum Dis Clin North Am 2013; 39:299)
- PET-CT findings
- Retroperitoneal involvement with perinephric soft tissue thickening producing the characteristic hairy kidney appearance
- Cardiovascular involvement may be characterized by circumferential soft tissue thickening of the vasculature including the thoracic and abdominal aorta (coated aorta), infiltrating right atrium and atrioventricular groove (Rheum Dis Clin North Am 2013; 39:299)
- Chest CT in pulmonary involvement demonstrates smooth interlobular septal thickening, micronodules, ground glass opacities, thickening of interlobular fissures and parenchymal condensation (Arthritis Rheum 2010;62:3504)
- Cardiac and brain MRI may be useful in initial assessment in suspected Erdheim-Chester disease cases to capture asymptomatic lesions (Mayo Clin Proc 2019; 94:2054)
Radiology images
Images hosted on other servers:

Skeletal and lung involvement

Peirenal soft tissue thickening
Prognostic factors
- Chronic disease with variable prognosis depending on the site(s) involved
- 5 year overall survival of 68% among those treated with interferon therapy (Blood 2011;117:2778)
- With targeted therapies, the 5 year overall survival has increased to 83% (Am J Hematol 2018;93:E114)
- CNS involvement is an independent major prognostic factor and independent predictor of death in survival analysis (Blood 2011;117: 2783, Blood 2014;124:483)
Case reports
- 3 year old boy with osteolytic lesions of skull, diabetes insipidus and bilateral proptosis (Ped Hem Onc 2017;2:59)
- 3.5 year old boy with generalized skin lesions and bone pain (Br J Dermatol 2018;178:261)
- 30 year old man with diffuse bone and articular pain (Medicine (Baltimore) 2016; 95:e5167)
- 53 year old man with headache and double vision for 12 months (Radiology 2017; 284:910)
- 64 year old woman presented with diabetes insipidus and cerebellar ataxia (Pan Afr Med J 2019;33:293)
- 68 year old man with history of controlled hypertension presented with diffuse abdominal pain, pericardial effusion (Circ Cardiovasc Imaging 2018;11:e008531)
Treatment
- Vemurafenib is FDA approved for patients with BRAF V600E mutation (Rheum Dis Clin North Am 2013; 39:299)
- MEK inhibitors such as trametinib or cobimetinib may be a valuable therapeutic option in patients with other MAPK pathway mutations (Blood 2020 Mar 18 [Epub ahead of print], Ann Rheum Dis 2019 Dec 9 [Epub ahead of print])
- If targeted therapy is not available or not well tolerated, cladribine has been reported to be moderately efficacious (JAMA Oncol 2017;3:1253)
- Interferon-α, pegylated interferon-α, anticytokine directed therapy (anakinra, infliximab, tocilizumab) have been shown to decrease lesional burden (Blood 2014;124:483)
Microscopic (histologic) description
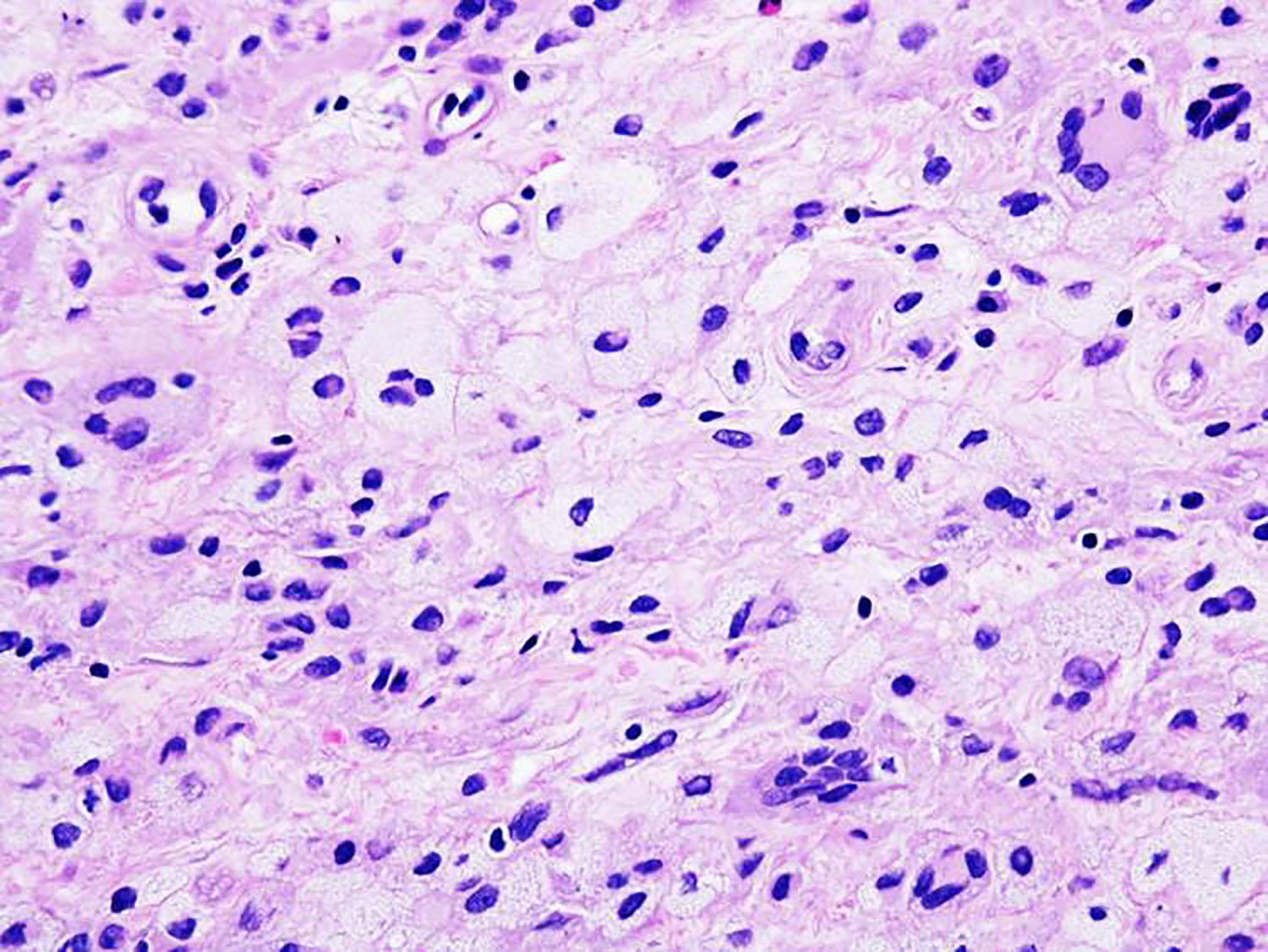
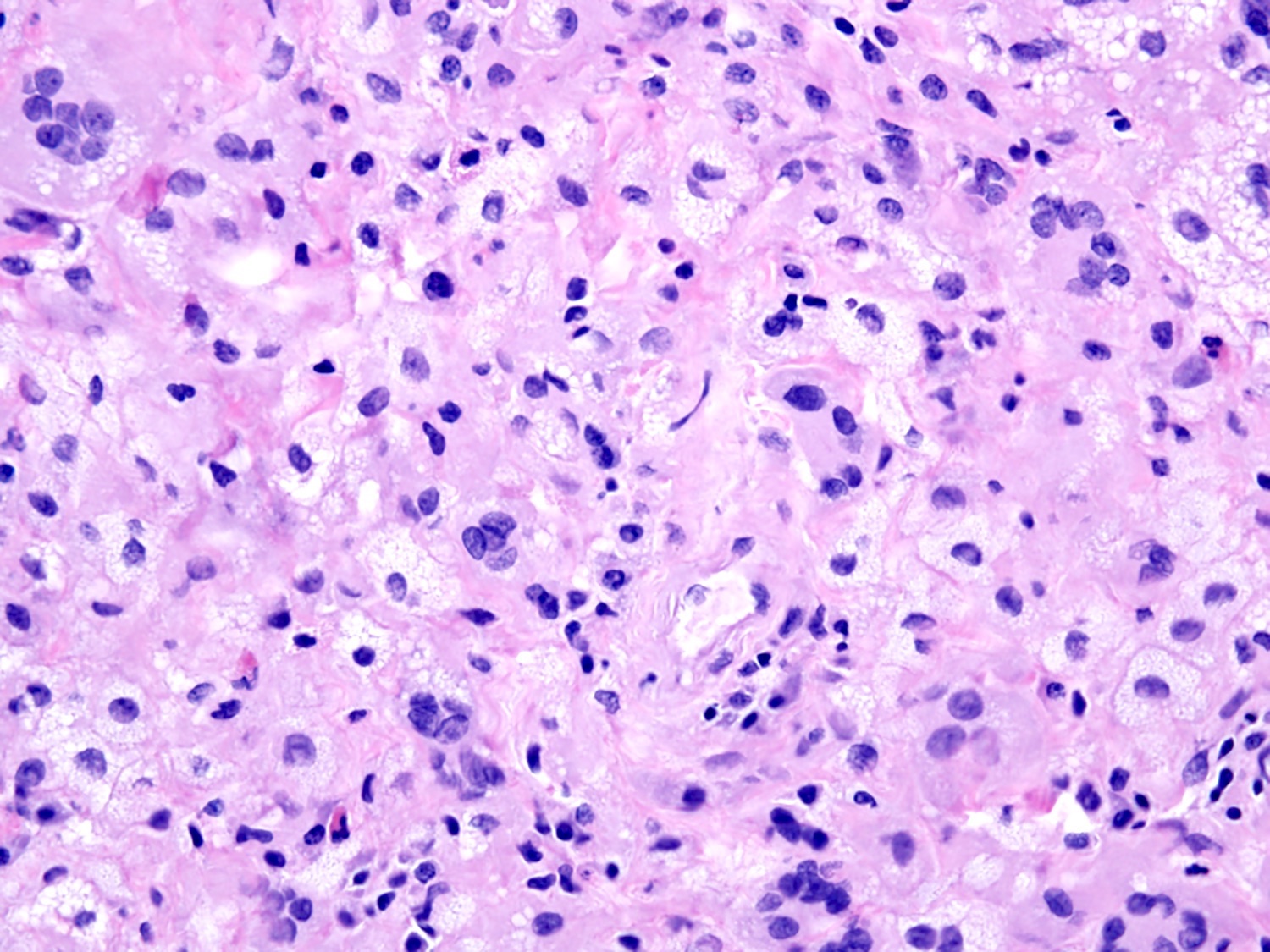
- Soft tissue infiltrate of bland appearing histiocytes characterized by abundant foamy (xanthomatous) cytoplasm with surrounding fibrosis (Mod Pathol 2018;31:581)
- Touton giant cells are frequently present
- Associated lymphoplasmacytic infiltrate is sparse
- Erdheim-Chester disease may be a component of mixed histiocytosis with Langerhans cell histiocytosis or Rosai-Dorfman disease (Blood 2014;124:1119, Hematologica 2020;105:e5)
Microscopic (histologic) images
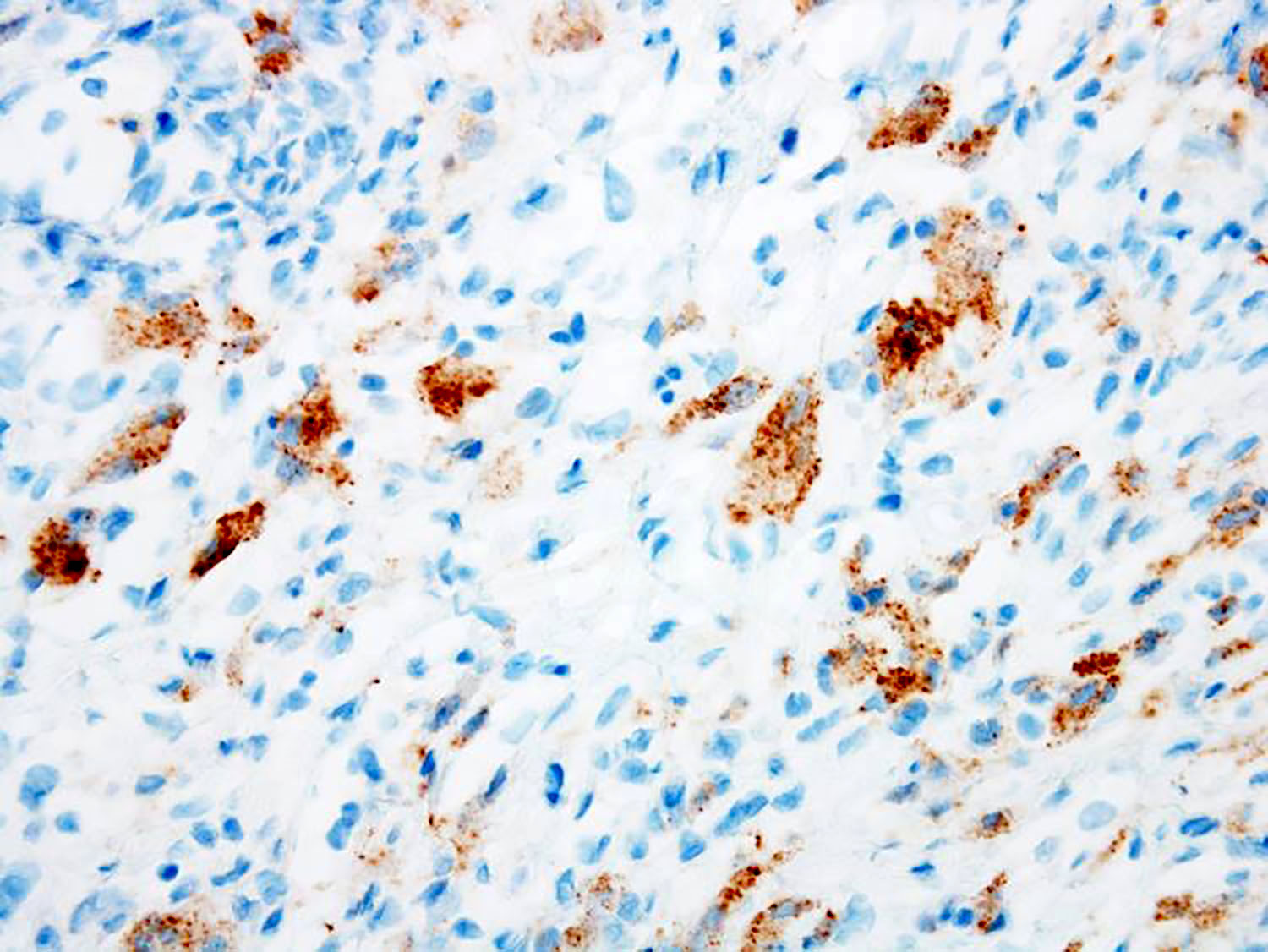
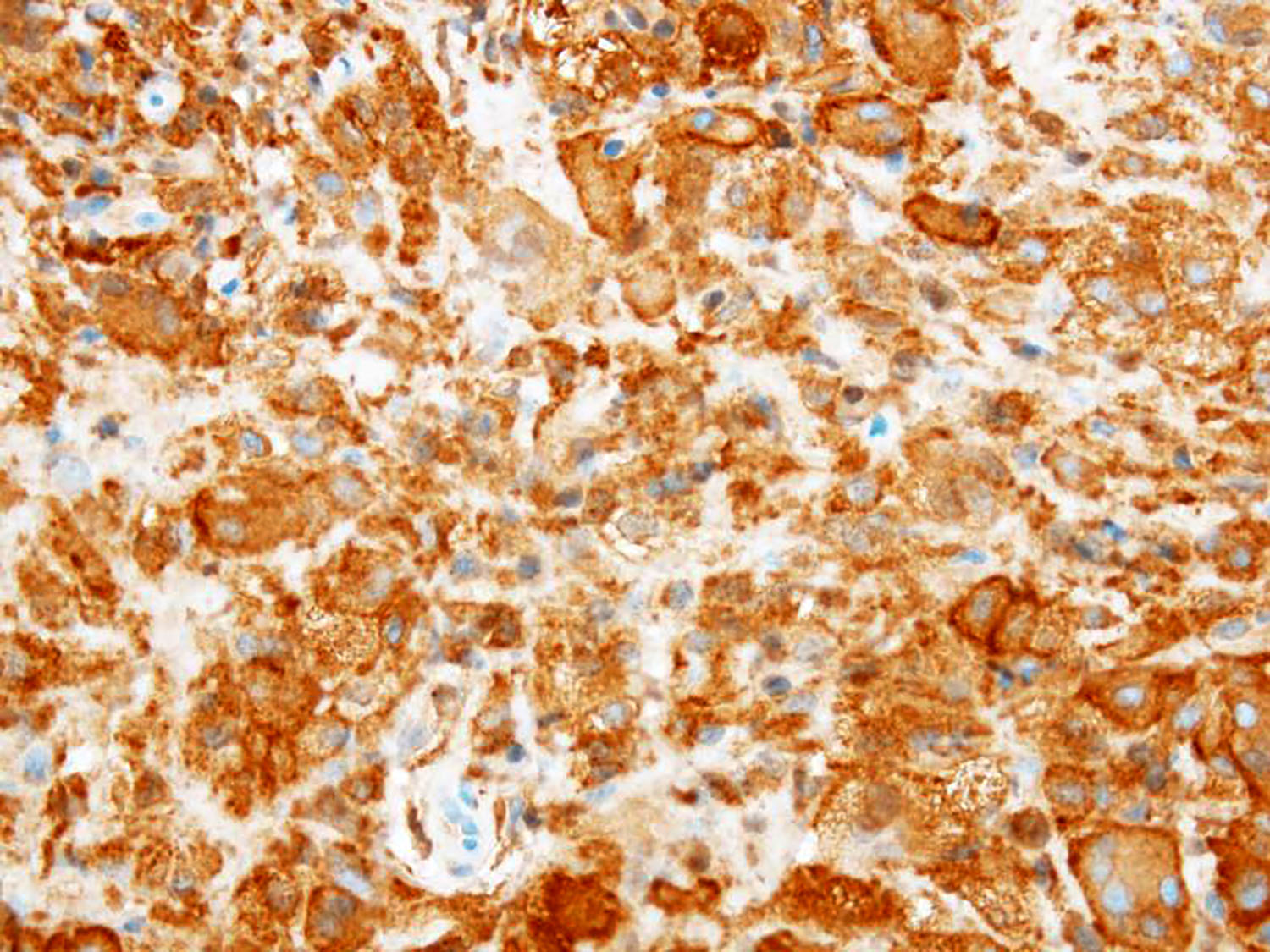
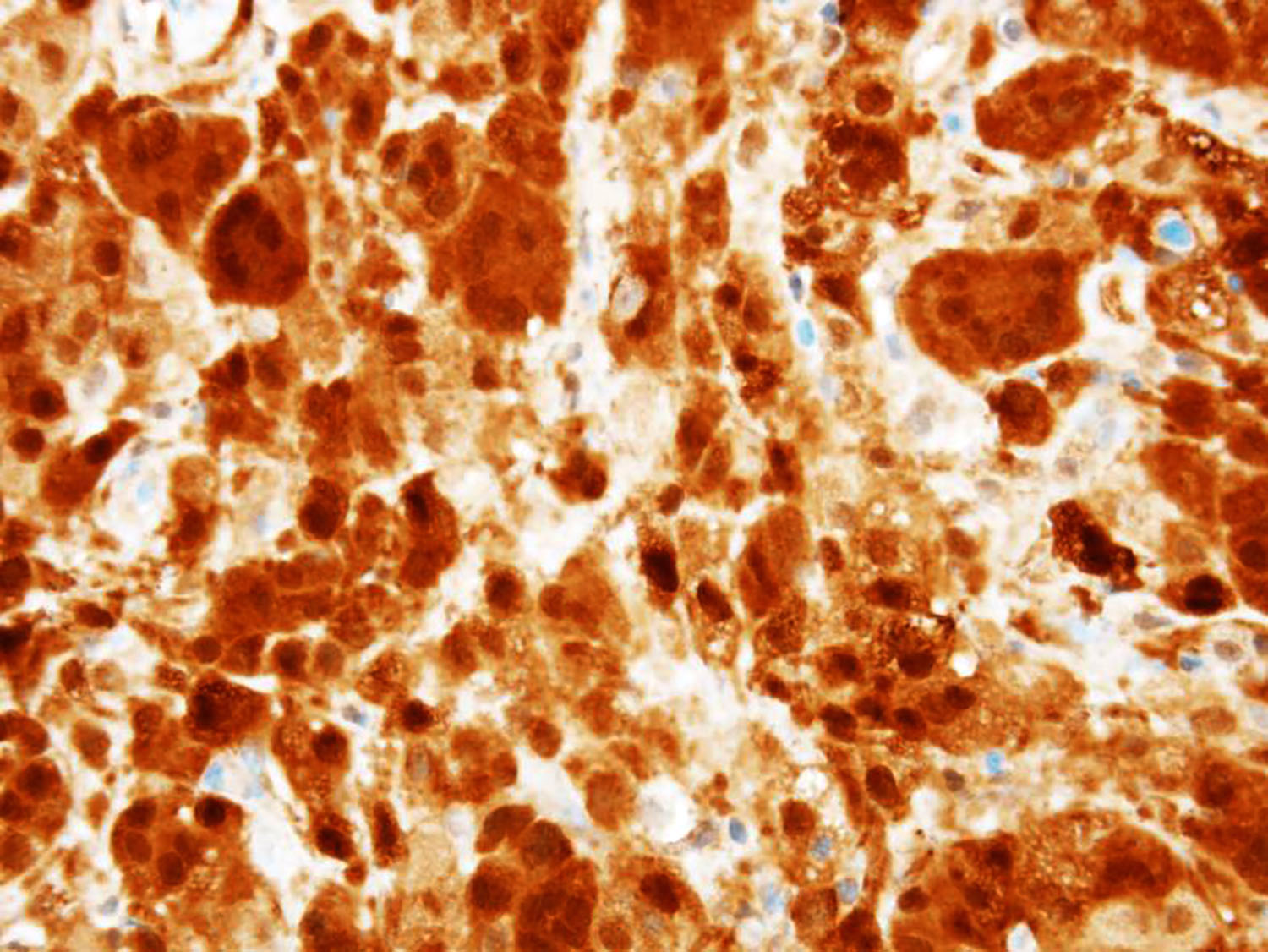
Contributed by Aishwarya Ravindran, M.B.B.S. and Karen L. Rech, M.D.
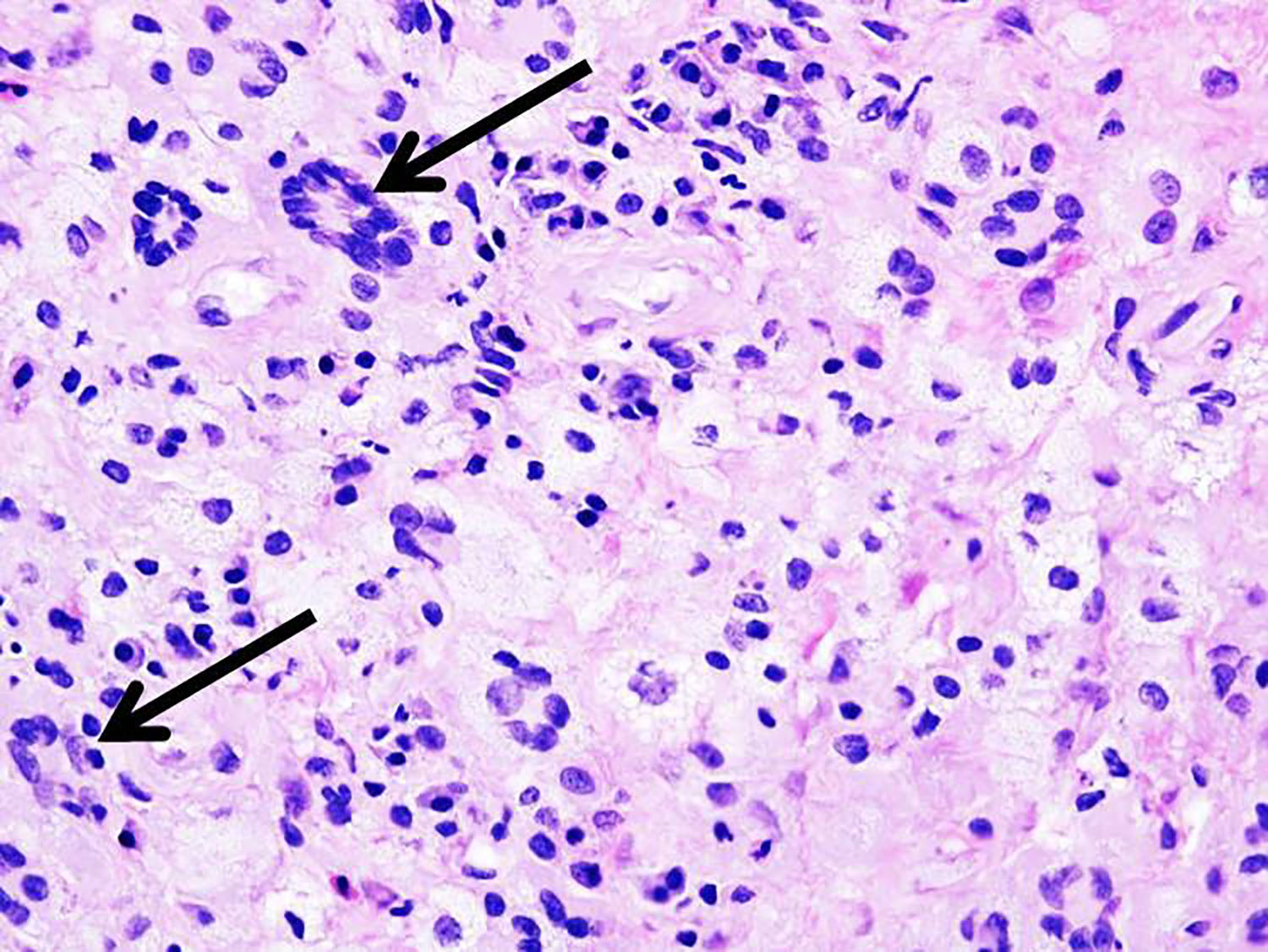
Excisional biopsy of perinephric soft tissue mass
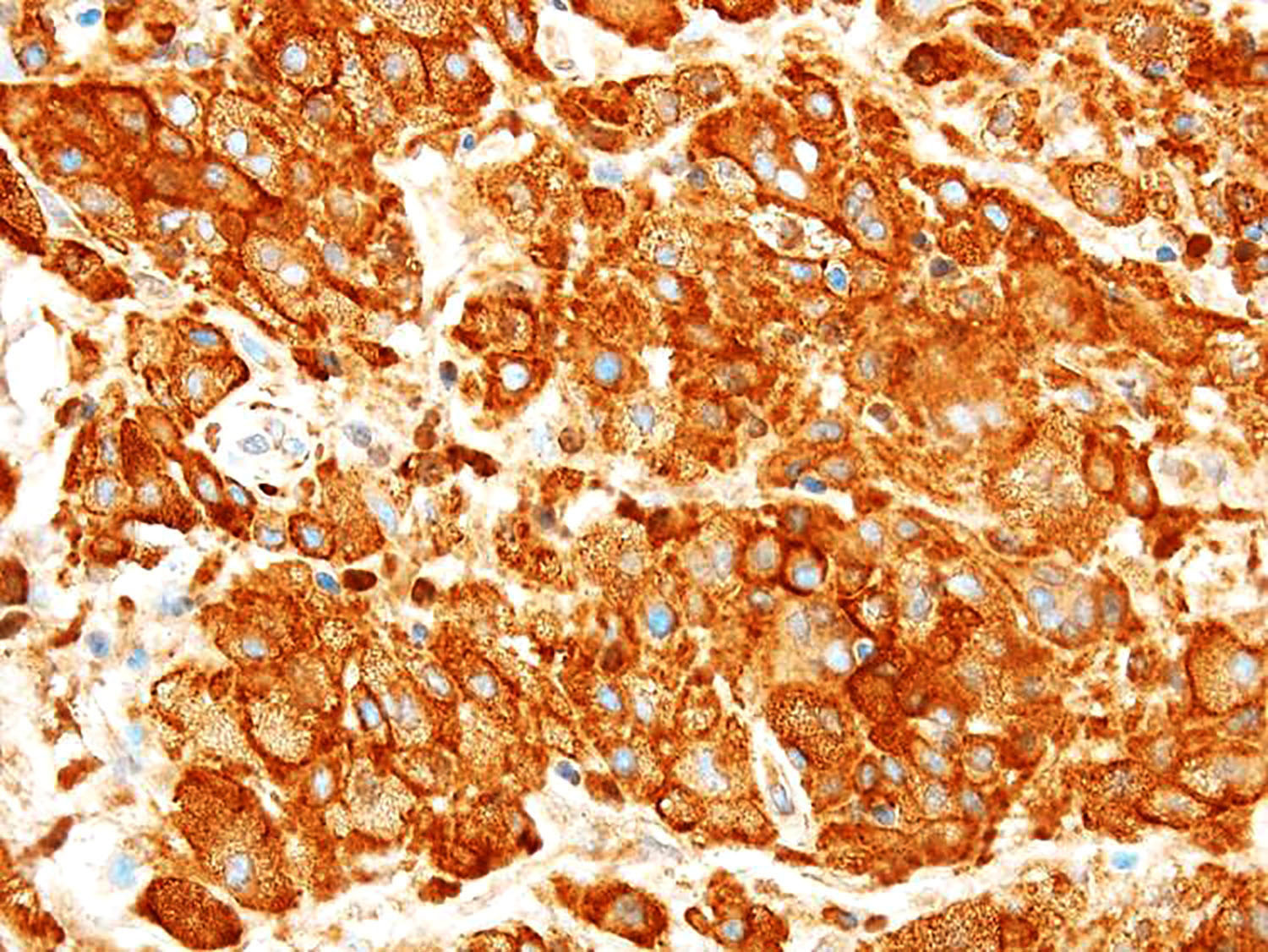
CD163
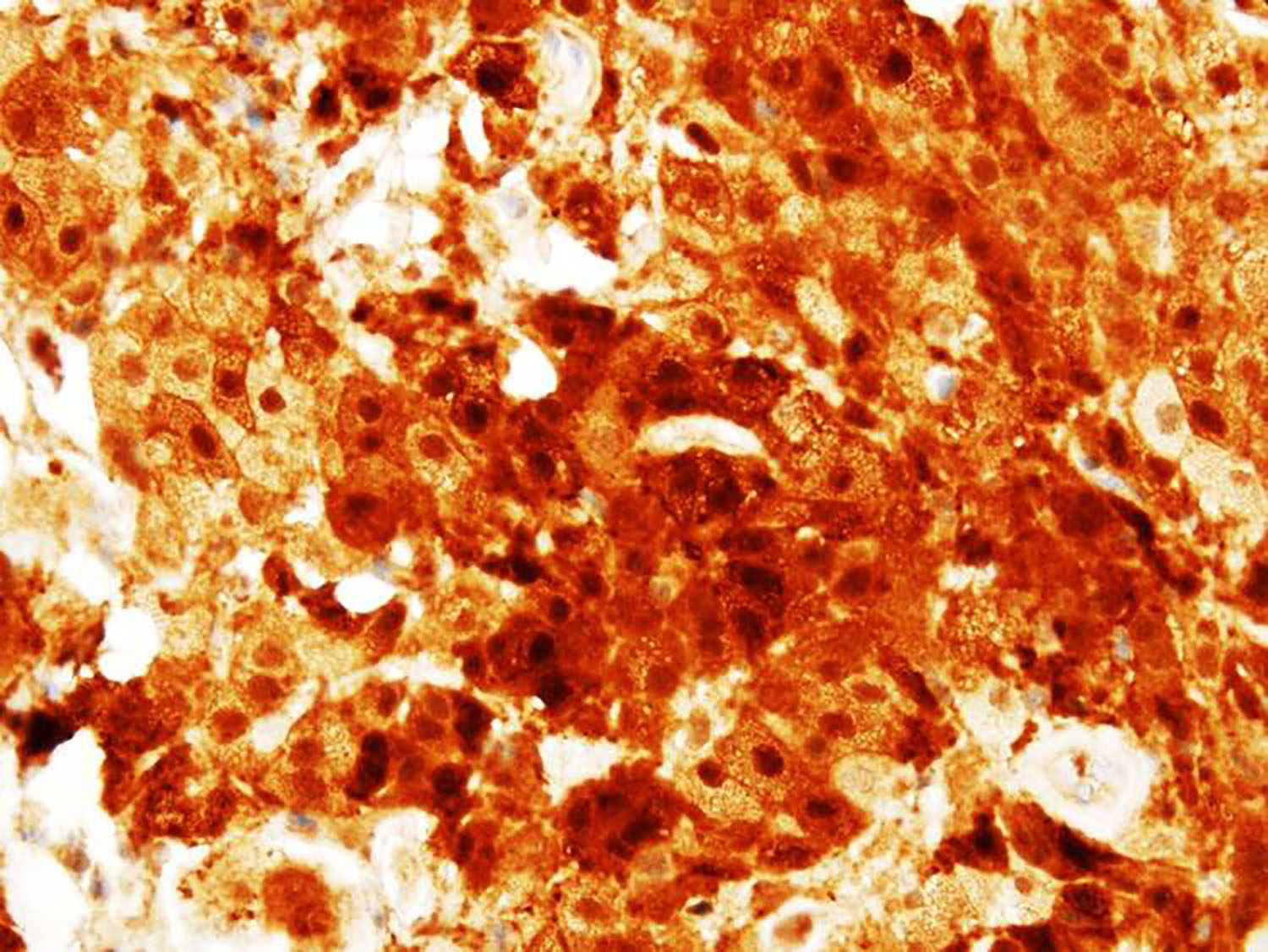
Factor XIIIa

Core biopsy of soft tissue (buttock) mass
Positive stains
- Histiocytic markers: CD14, CD68 and CD163
- Factor XIIIa (strong and diffuse staining)
- BRAF V600E in ~50% cases
- Reference: Mod Pathol 2018;31:581
Negative stains
Molecular / cytogenetics description
- Over 90% harbor mutations in the mitogen activated protein kinase (MAPK) pathway
- Most common mutation is BRAF V600E (reported in >50% cases) (Blood 2012;120:2700)
- Other somatic mutations include MAP2K1, ARAF, MAP2K2, KRAS, NRAS (Mod Pathol 2018;31:581)
Sample pathology report
- Soft tissue, perinephric, biopsy:
- Histiocytic neoplasm with BRAF V600E mutation by immunohistochemistry, consistent with Erdheim-Chester disease in the appropriate clinical context (see comment)
- Comment: The histologic sections demonstrate adipose tissue with an infiltrate of foamy histiocytes admixed with scattered Touton giant cells. There is extensive fibrosis present. Immunoperoxidase studies were performed on paraffin embedded sections using antibodies directed against the following antigens: CD1a, CD68, CD163, Factor XIIIa, IgG, IgG4, langerin, S100 and BRAF V600E. The foamy histiocytes are positive for CD68, CD163 and Factor 13a and are negative for S100, CD1a and langerin. The lesional histiocytes are positive for BRAF V600E mutation by immunohistochemistry. There is no increase in number of IgG4 positive plasma cells or an abnormal IgG4/IgG ratio.
Differential diagnosis
- Reactive histiocytic proliferations, such as those seen in fat necrosis and post chemotherapy:
- Histologically may be indistinguishable
- Clinical features important in distinguishing from histiocytic neoplasm
- Immunostains for Factor XIIIa and BRAF V600E may be helpful
- Langerhans cell histiocytosis:
- Juvenile xanthogranuloma:
- Usually in infants and children
- Histologically and phenotypically similar to Erdheim-Chester disease
- Absence of BRAF or other MAPK pathway mutations
- Rosai-Dorfman disease:
- Lesional histiocytes are characterized by enlarged round nuclei with small distinct nucleoli, abundant cytoplasm and emperipolesis
- More prominent plasma cell infiltrate and lymphoid aggregates
- Positive for S100
Board review style question #1
H&E
CD163
Factor XIIIA
- A 37 year old man presented with abdominal pain. PET CT demonstrated soft tissue thickening around the kidneys with perinephric fat stranding, along with FDG avid metaphyseal lesions bilaterally in the distal femur and proximal tibia. Core biopsy of the perinephric soft tissue demonstrated the staining shown above. In conjunction with the histopathology and radiology, which of the following would be the best diagnosis?
- Erdheim-Chester disease
- Follicular dendritic cell sarcoma
- Juvenile xanthogranuloma
- Langerhans cell histiocytosis
- Reactive process
Board review style answer #1
Board review style question #2
- Which of the following genetic mutations is most commonly associated with Erdheim-Chester disease?
- APC
- BRAF V600E
- KIT D816V
- MET exon 14
- PTEN
Board review style answer #2
