
Lymph nodes & spleen, nonlymphoma
Lymph node-nonspecific findings
Reactive lymphadenopathy
Author: Jayalakshmi Balakrishna, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.
Editor-in-Chief: Patricia Tsang, M.D., M.B.A.

Last author update: 17 February 2025
Last staff update: 17 February 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed search: Reactive lymphadenopathy

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Peripheral smear description | Peripheral smear images | Positive stains | Negative stains | Flow cytometry description | Flow cytometry images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Balakrishna J. Reactive lymphadenopathy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphnodesreactivegeneral.html. Accessed April 1st, 2025.
Definition / general
- Lymph node enlargement due to proliferation of some or all compartments or cellular components of lymph nodes, reflecting antigenic stimulation
- Can be acute or chronic depending on the pathogenic agents
Essential features
- Lymph node enlargement
- Acute: painful or tender; chronic: nontender
- 4 architectural patterns: follicular hyperplasia, sinus histiocytosis, interfollicular / mixed and diffuse
- Clonal B or T cell proliferations are generally not detected but reactive clonal populations may occur
- Lacks significant cytologic or architectural atypia
Terminology
- Reactive lymphoid hyperplasia
- Reactive follicular hyperplasia
- Diffuse paracortical hyperplasia
- Sinus histiocytosis
- Acute nonspecific lymphadenitis
- Chronic lymphadenitis
ICD coding
- ICD-10: R59.9 - enlarged lymph nodes, unspecified
Epidemiology
- Represents the reaction of lymphoid tissue to intrinsic or environmental antigens
- Most lymph node enlargements are reactive
- Can occur in any age group and gender
- In children, most lymphadenopathies are benign; in adults, chance of malignancy increases with age (Mayo Clin Proc 2000;75:723)
Sites
- Any lymph node group can be affected depending on the etiology and area of drainage (Clin Pediatr (Phila) 2011;50:683)
Pathophysiology
- Lymph nodes filter lymph drained from tributary regions
- Antigenic substances reaching the lymph nodes evoke an immune reaction (Semin Diagn Pathol 2018;35:4)
- Bacteria and fungi cause predominantly inflammatory reactions; viruses and drugs cause predominantly immune reactions
- Acute nonspecific lymphadenitis: acute inflammation of the lymph node due to an infectious or inflammatory etiology
- Chronic nonspecific lymphadenitis: chronic inflammation of the lymph node in response to a pathogen / antigen, known or unknown
Etiology
- Infections: virus, bacteria, fungi and protozoa
- Chemicals: environmental pollution
- Drugs: phenytoin, allopurinol, gold, penicillin, quinidine
- Altered tissue components: inflammation, tissue necrosis
- Inflammatory / autoimmune conditions, such as rheumatoid arthritis
- Other antigens or allergens, including vaccines (Mayo Clin Proc 2000;75:723, Iran J Med Sci 2014;39:158, Pediatr Clin North Am 2002;49:1009)
Clinical features
- Clinical features reflect the underlying cause
- Enlarged lymph nodes (Am Fam Physician 2016;94:896)
- In acute lymphadenitis, can be painful or tender and nodes may be soft or fluctuant, with or without associated fever, weight loss, malaise, loss of appetite and redness of overlying skin
- In chronic lymphadenitis, enlarged lymph nodes are commonly painless (Mayo Clin Proc 2000;75:723)
Diagnosis
- Clinical examination
- Histopathology: biopsy is rarely performed if reactive nature is clinically obvious
- In chronic lymphadenitis, biopsy and histopathology evaluation are necessary
- Exclusion of specific causes: clinical, laboratory and imaging findings
- If suspicious, exclude lymphoid neoplasia by immunohistochemistry, flow cytometry and required genetic studies
Laboratory
- Laboratory findings depend on the etiology and nature of the process (acute versus chronic)
- Complete blood count (CBC) may show leukocytosis with neutrophilia or lymphocytosis and erythrocyte sedimentation rate (ESR) may be elevated
- Confirmatory tests for specific etiologic agents (infectious agents) may be positive
Radiology description
- Enlarged lymph node(s)
- Advanced imaging techniques may help to distinguish reactive lymph node enlargement from tumor metastases or other specific lymph node enlargements (Mol Imaging Biol 2013;15:40, Indian J Gastroenterol 2016;35:55)
Prognostic factors
- Benign, usually self limiting process with good prognosis
- Prognosis depends on the etiology and appropriate and timely management of the cause
Case reports
- 40 year old man who received dasatinib for chronic myeloid leukemia presented with a large axillary mass (Medicine (Baltimore) 2020;99:e22791)
- 41 year old woman with a history of nasopharyngeal carcinoma and enlarged cervical lymph nodes (Clin Nucl Med 2022;47:367)
- 57 year old woman with rheumatoid arthritis and generalized lymphadenopathy (Case Rep Rheumatol 2014;2014:386328)
- 68 year old man with right cheek melanoma and multiple FDG avid lymph nodes in the left axilla (Clin Nucl Med 2021;46:433)
Treatment
- Treat the underlying cause
Gross description
- Enlarged, soft lymph nodes with tan, homogenous cut surfaces
- Acute lymphadenitis: suppuration may lead to necrosis and abscess formation
- Chronic lymphadenitis: thickened capsule and fibrosis may be obvious (Walker: Clinical Methods - The History, Physical, and Laboratory Examinations, 3rd Edition, 1990)
Gross images
Contributed by Kathy Smith, PA

Enlarged lymph node
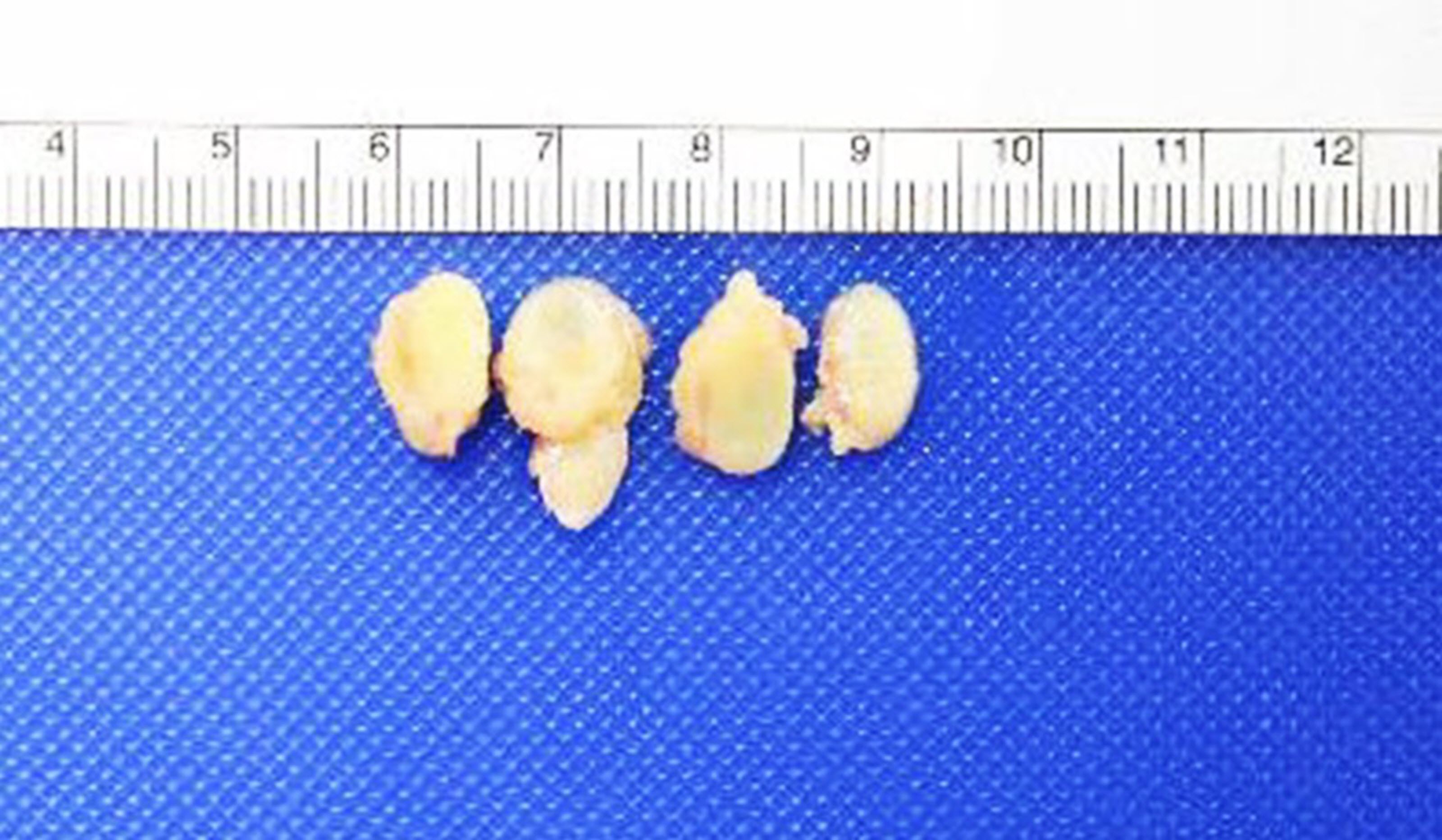
Tan, homogenous appearance
Microscopic (histologic) description
- 4 architectural patterns of reactive hyperplasia are described, depending on the etiology: follicular / nodular, sinus histiocytosis, interfollicular / mixed and diffuse
- Follicular hyperplasia (most common reactive pattern)
- Enlarged follicles, varying in size and shape, may coalesce and display different configurations
- Prominent germinal center and mantle zone
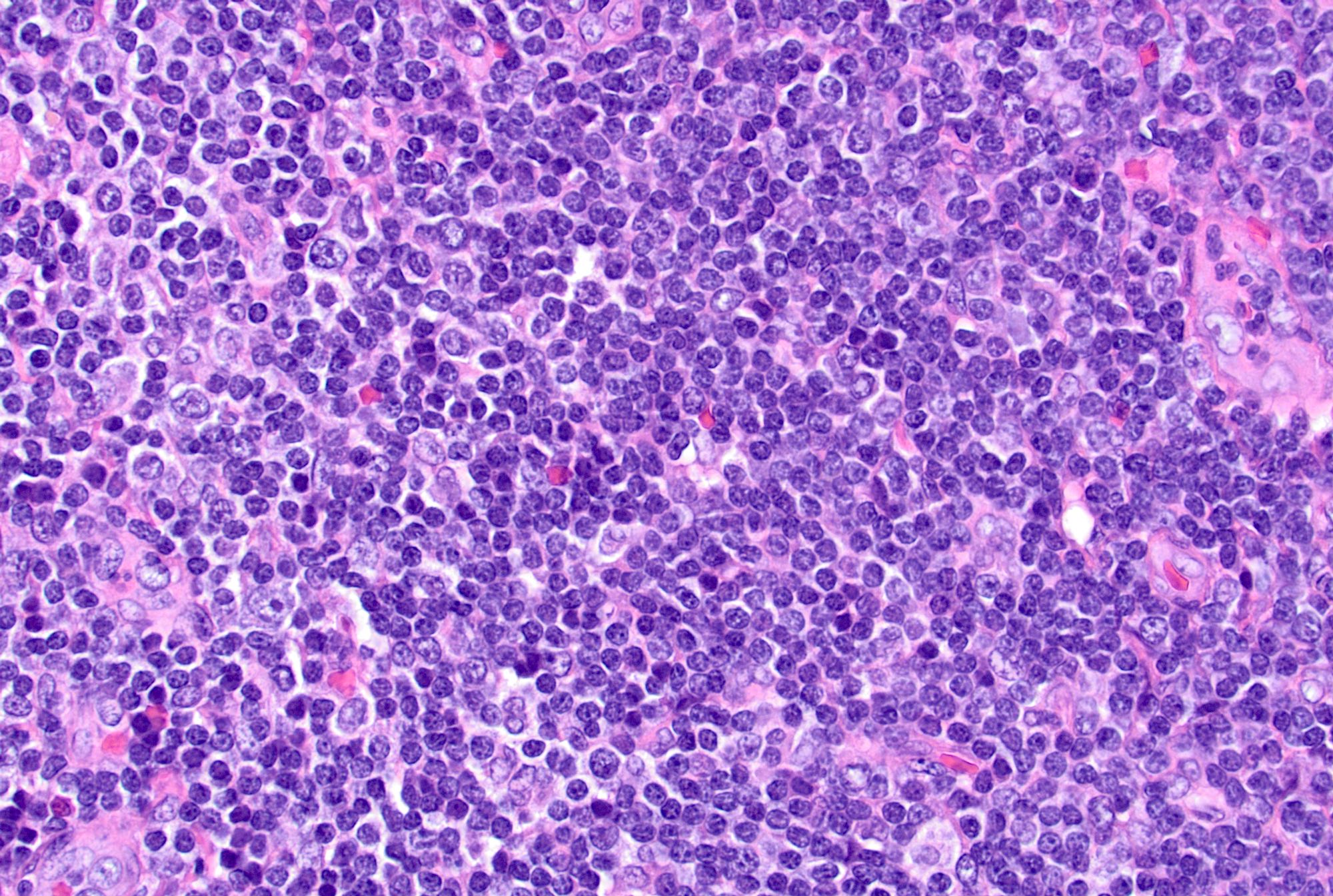
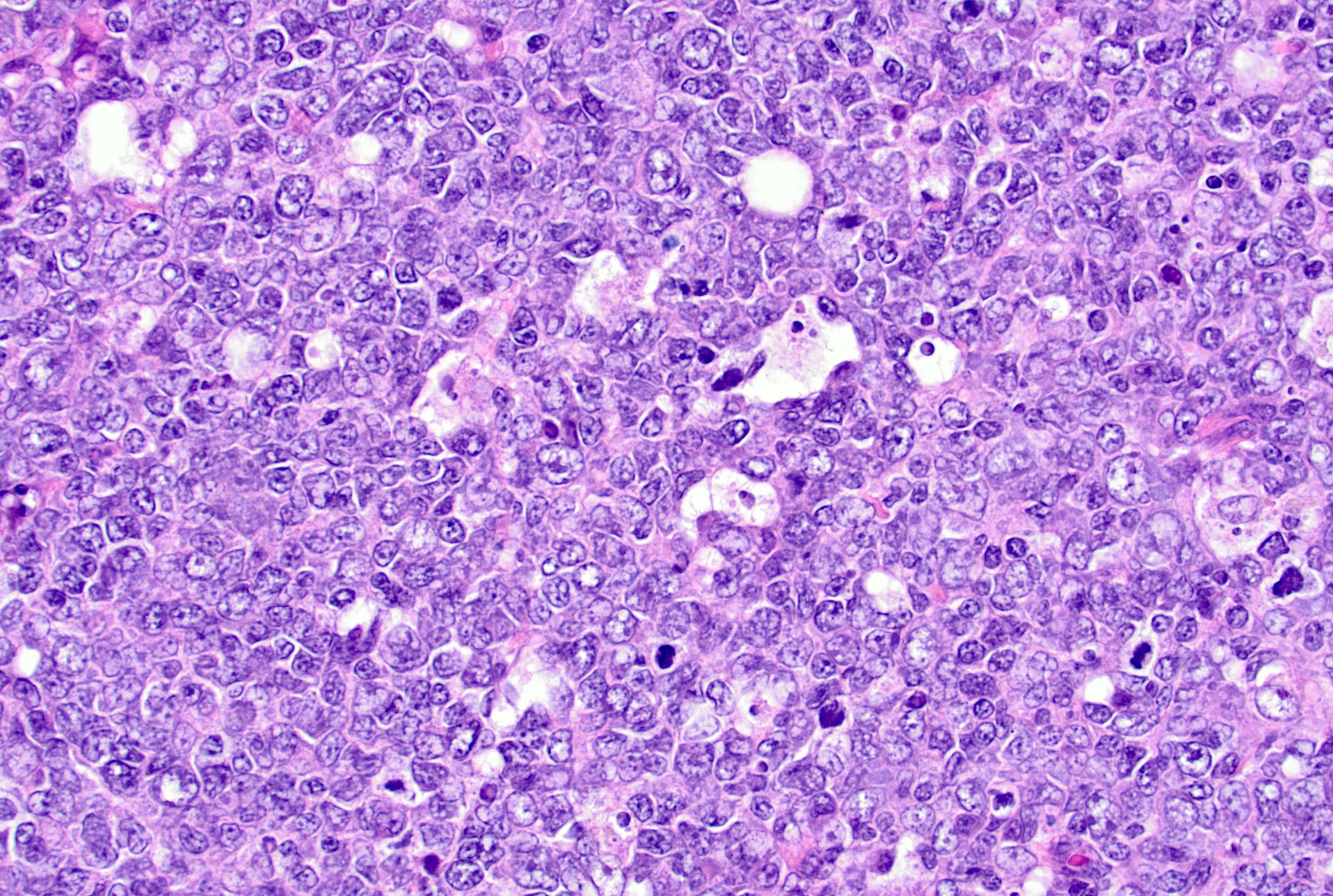
- Germinal centers show mixed small and large lymphocytes, centrocytes and centroblasts
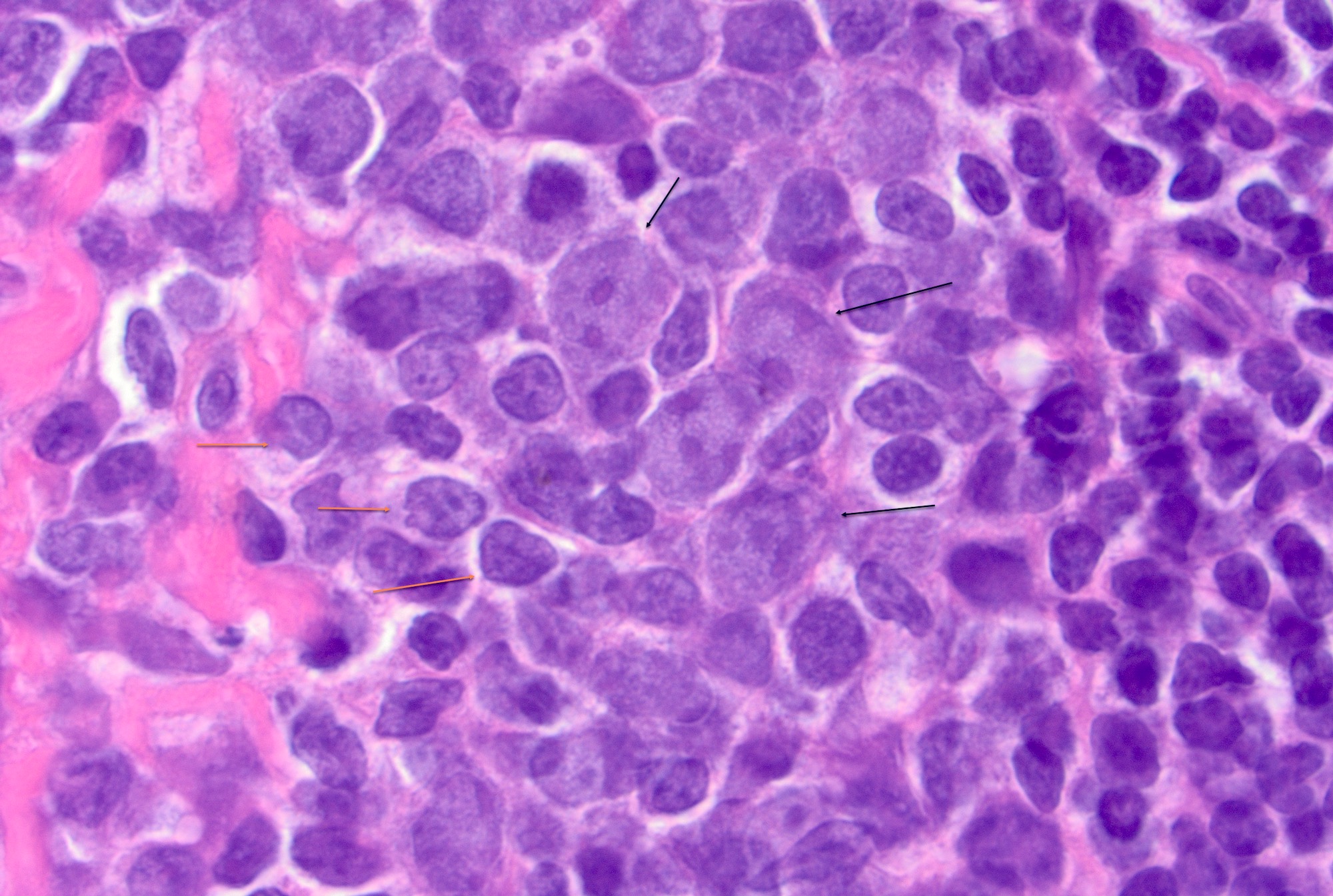
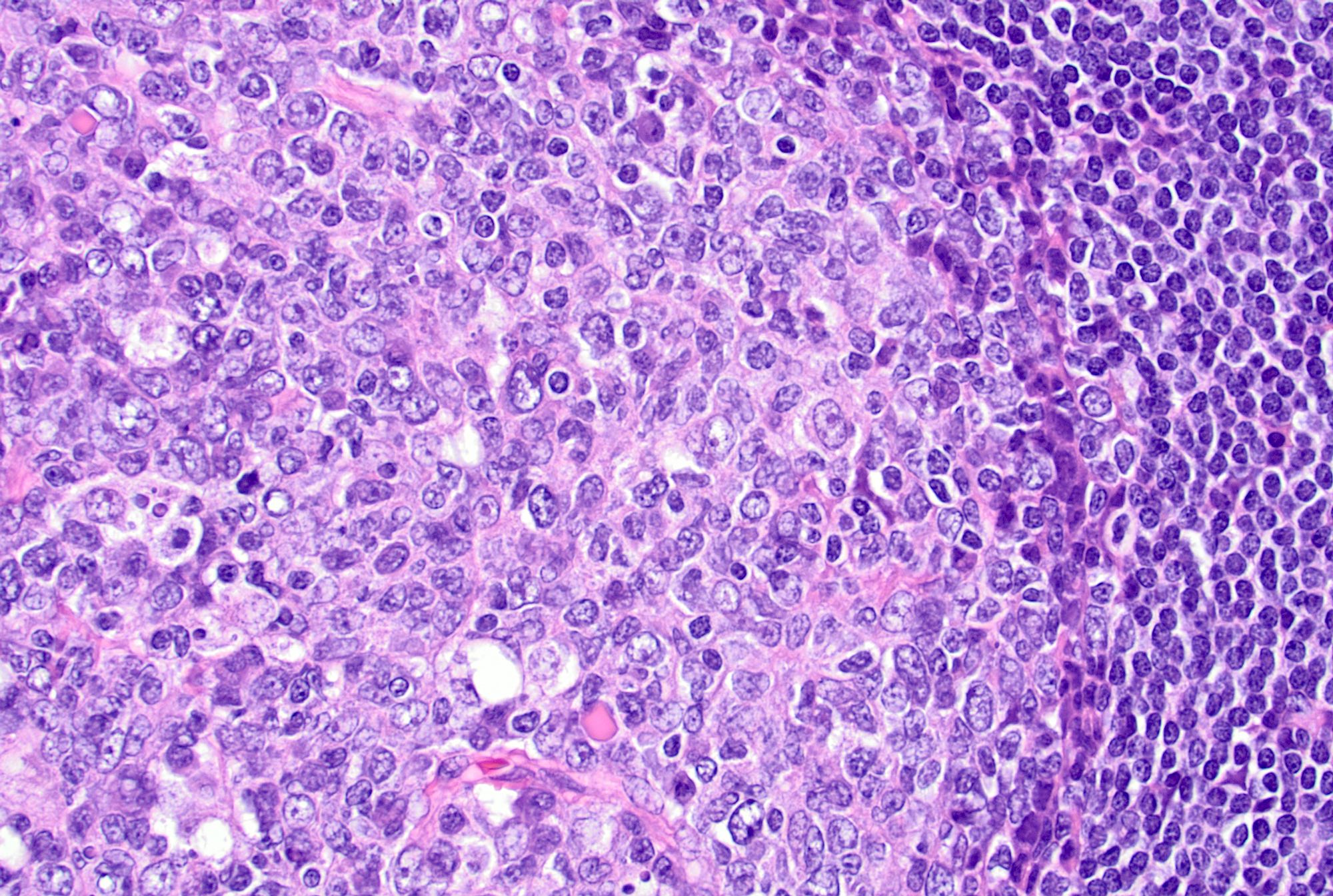
- Centroblasts polarize to the medial pole / medullary side forming the darker zone and centrocytes accumulate at the peripheral pole / capsular side forming the lighter zone (Immunity 2016;45:471)
- Centroblasts are 3 - 4 times larger than the inactivated lymphocytes and show a narrow rim of basophilic cytoplasm and large, round to oval vesicular nuclei with 1 - 3 prominent peripheral nucleoli
- Mitotic figures are frequent
- Centrocytes are smaller lymphocytes with scant cytoplasm, cleaved nuclei, clumped chromatin and small or absent nucleoli
- Numerous tingible body macrophages are a characteristic feature of follicular hyperplasia (Semin Diagn Pathol 2018;35:4, Am J Surg Pathol 1987;11:866)
- Other cells: plasma cells, T cells and follicular dendritic cells
- PD-1+ T cells (T follicular helper cells) are seen predominantly at the periphery of the germinal center (Ann Diagn Pathol 2020;44:151421)
- Mantle zone: around the light zone, small lymphocytes
- Interfollicular areas may show rare transformed cells (immunoblasts), small lymphocytes, plasma cells and high endothelial venules
- Monocytoid B cell proliferation may be seen in follicular hyperplasia around cortical sinuses (Pathol Res Pract 1998;194:559)
- Sinus histiocytosis
- Expansion of sinuses by histiocytes
- Common pattern in lymph nodes draining tumor (Br J Surg 1983;70:317)
- Interfollicular / mixed patterns
- Paracortical hyperplasia: seen usually in viral infections, nodes draining tumors and autoimmune disorders (Pathol Res Pract 2001;197:237, Hum Pathol 1975;6:363, APMIS 2001;109:419)
- Mixed small lymphocytes and immunoblasts, with increased vascularity and interdigitating dendritic cells
- Granulomatous lymphadenitis: necrotizing, nonnecrotizing or suppurative granulomas depending on the etiology (Rev Infect Dis 1986;8:322)
- Diffuse
- Architecture may be effaced
- Diffuse proliferation of mixed small lymphocytes, immunoblasts and plasma cells (APMIS 2001;109:419)
- Immunoblasts may rarely mimic Hodgkin / Reed-Sternberg cells
- Follicular hyperplasia (most common reactive pattern)
- Acute lymphadenitis
- Sinus dilatation followed by accumulation of neutrophils, vascular dilatation and edema of the capsule
- Suppurative or necrotizing inflammation may be seen depending on the etiology (Semin Pediatr Surg 2006;15:99)
- Chronic lymphadenitis
- Follicular hyperplasia, prominence of postcapillary venules, increased number of immunoblasts, fibrosis, plasma cells and histiocytes
- Capsule may be inflamed or fibrotic (Semin Pediatr Surg 2006;15:99)
Microscopic (histologic) images
Contributed by Jayalakshmi Balakrishna, M.D.
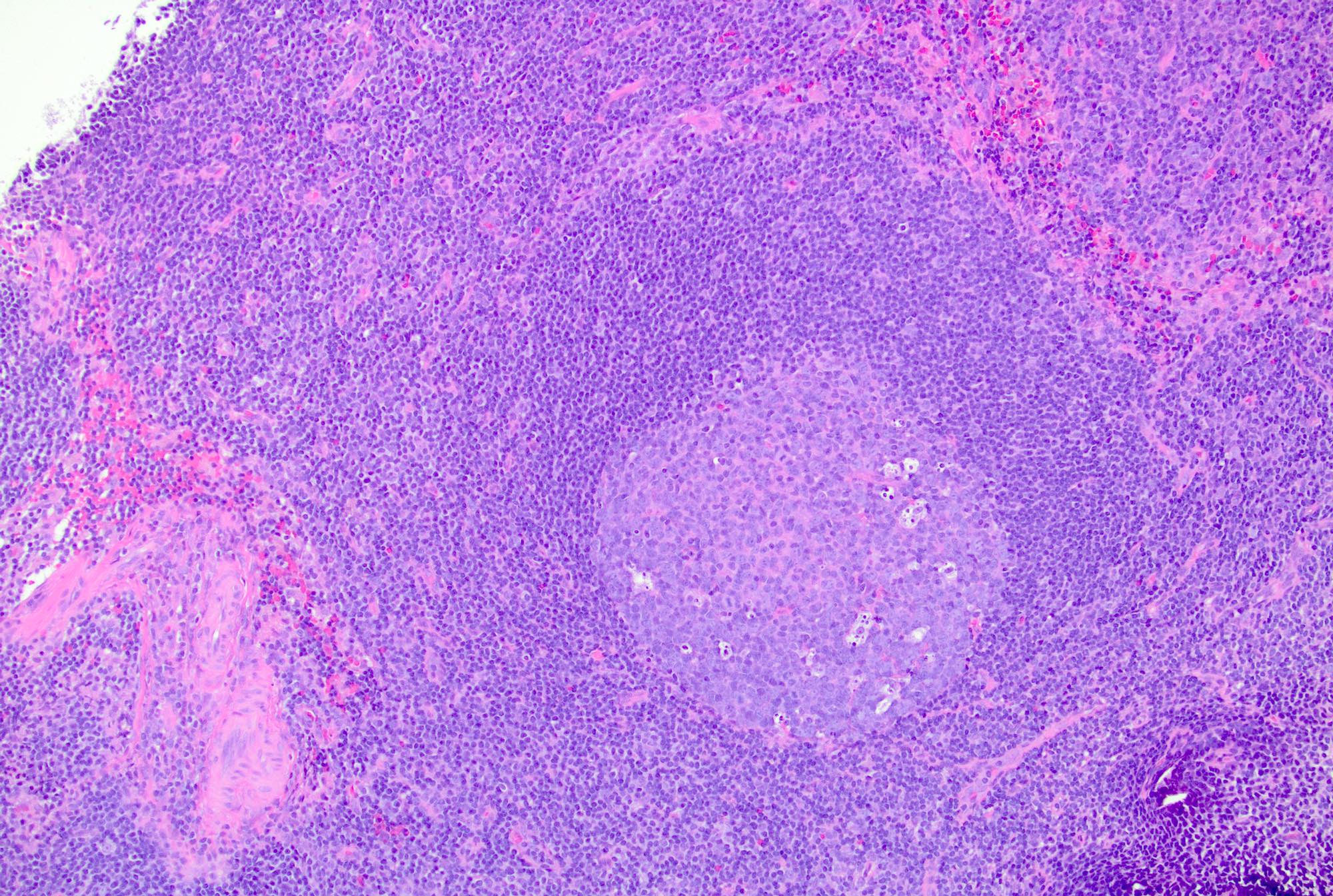
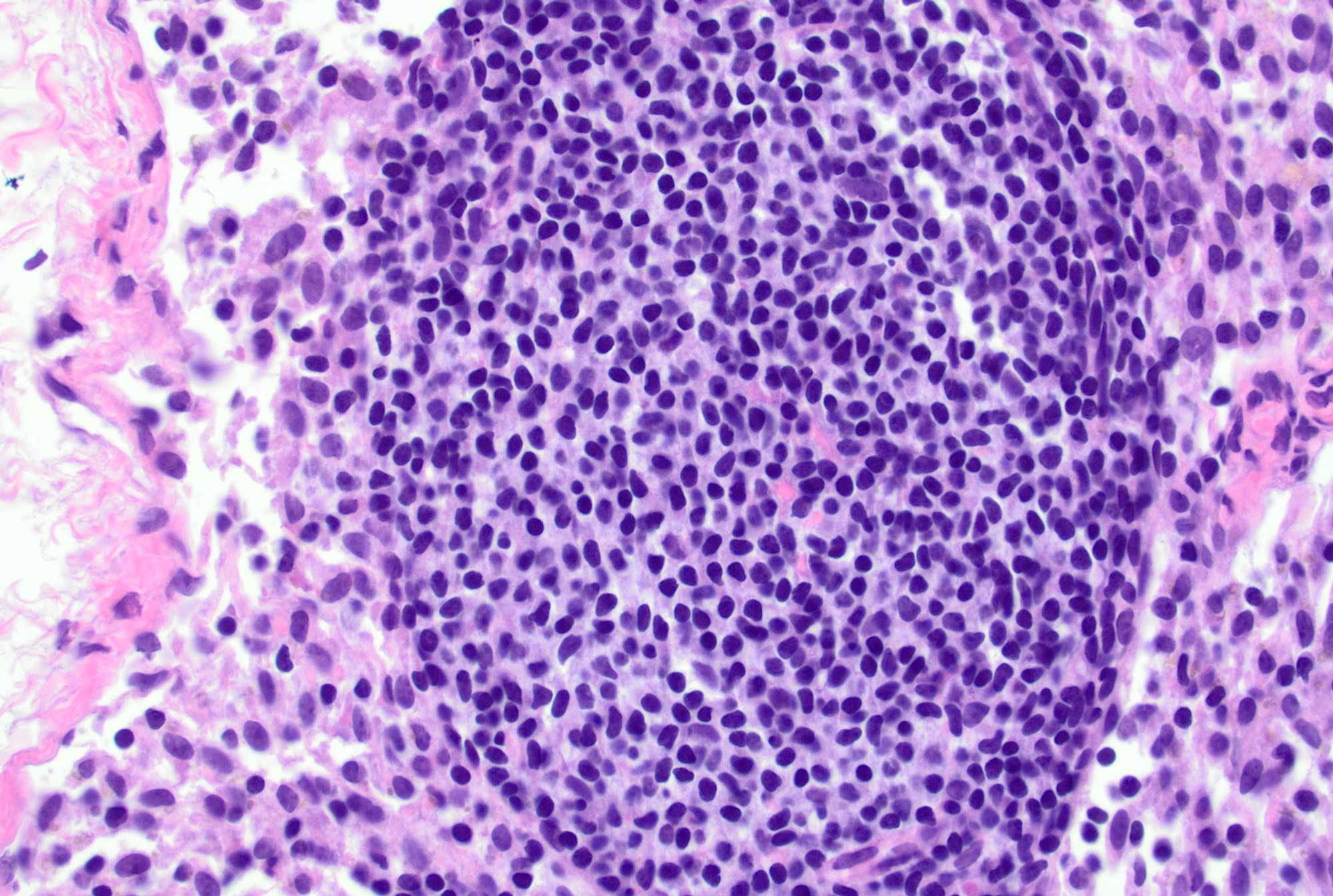
Follicular hyperplasia
Follicular hyperplasia
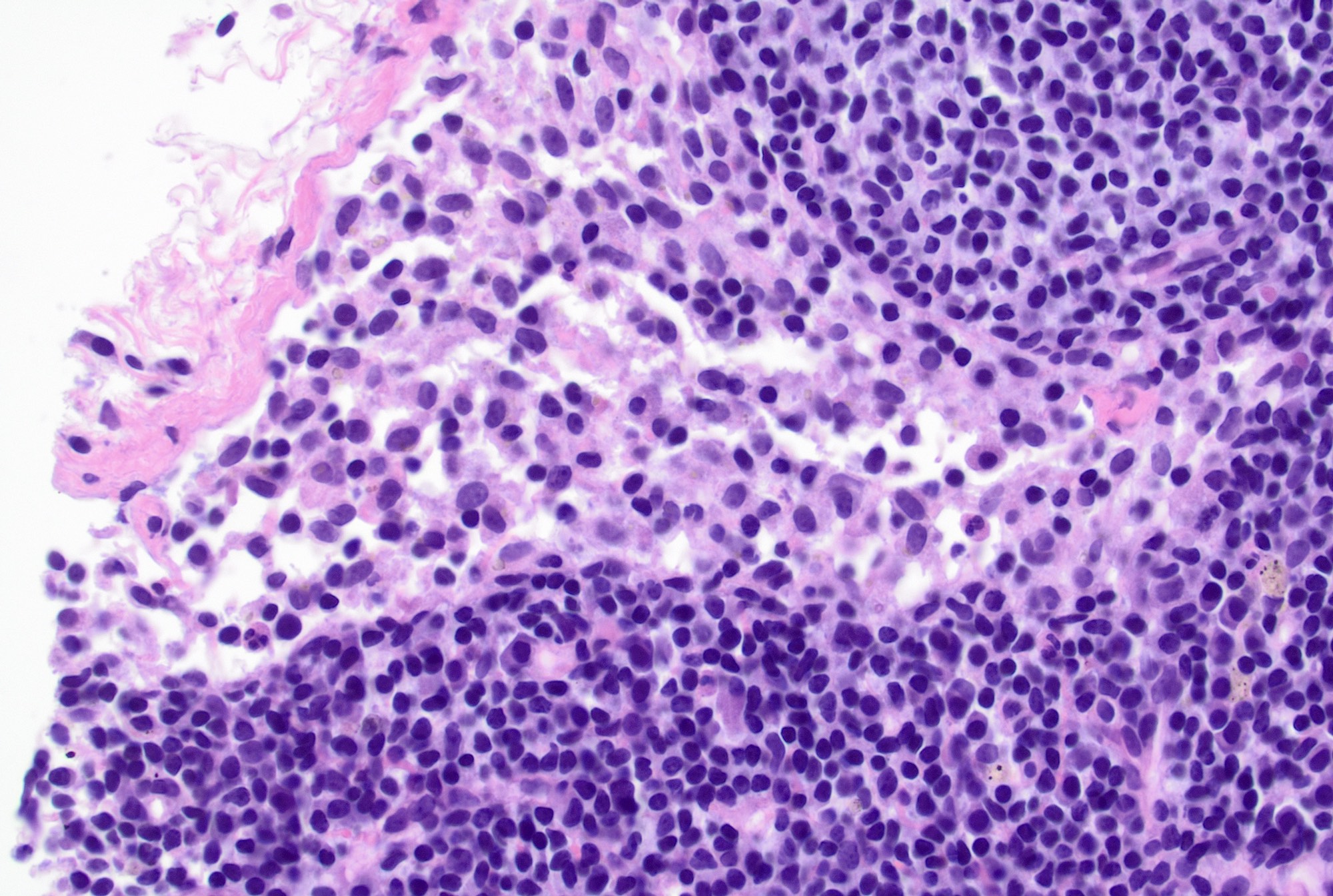
Interfollicular area
Germinal center dark zone
Sinus histiocytosis
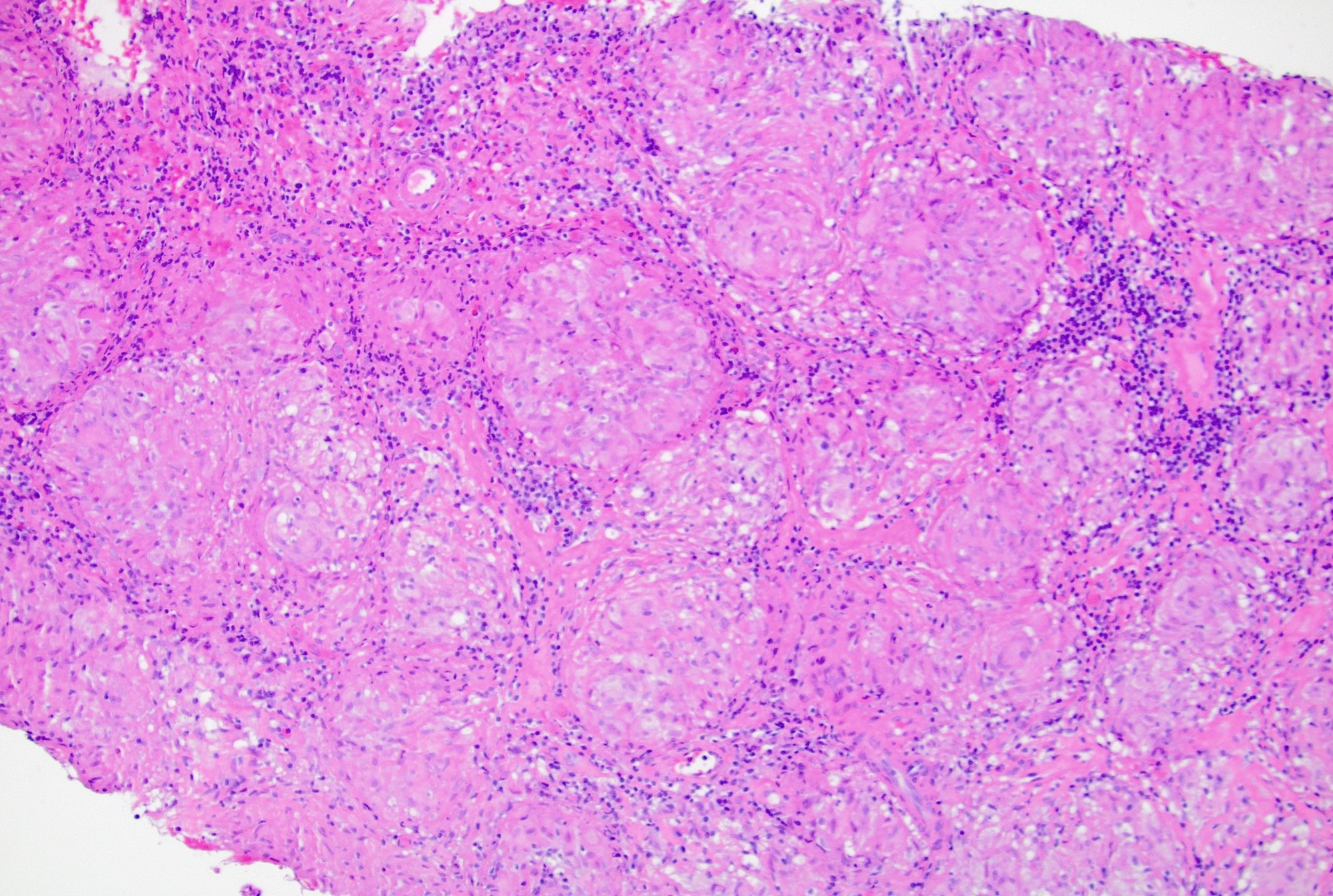
Granulomatous lymphadenitis
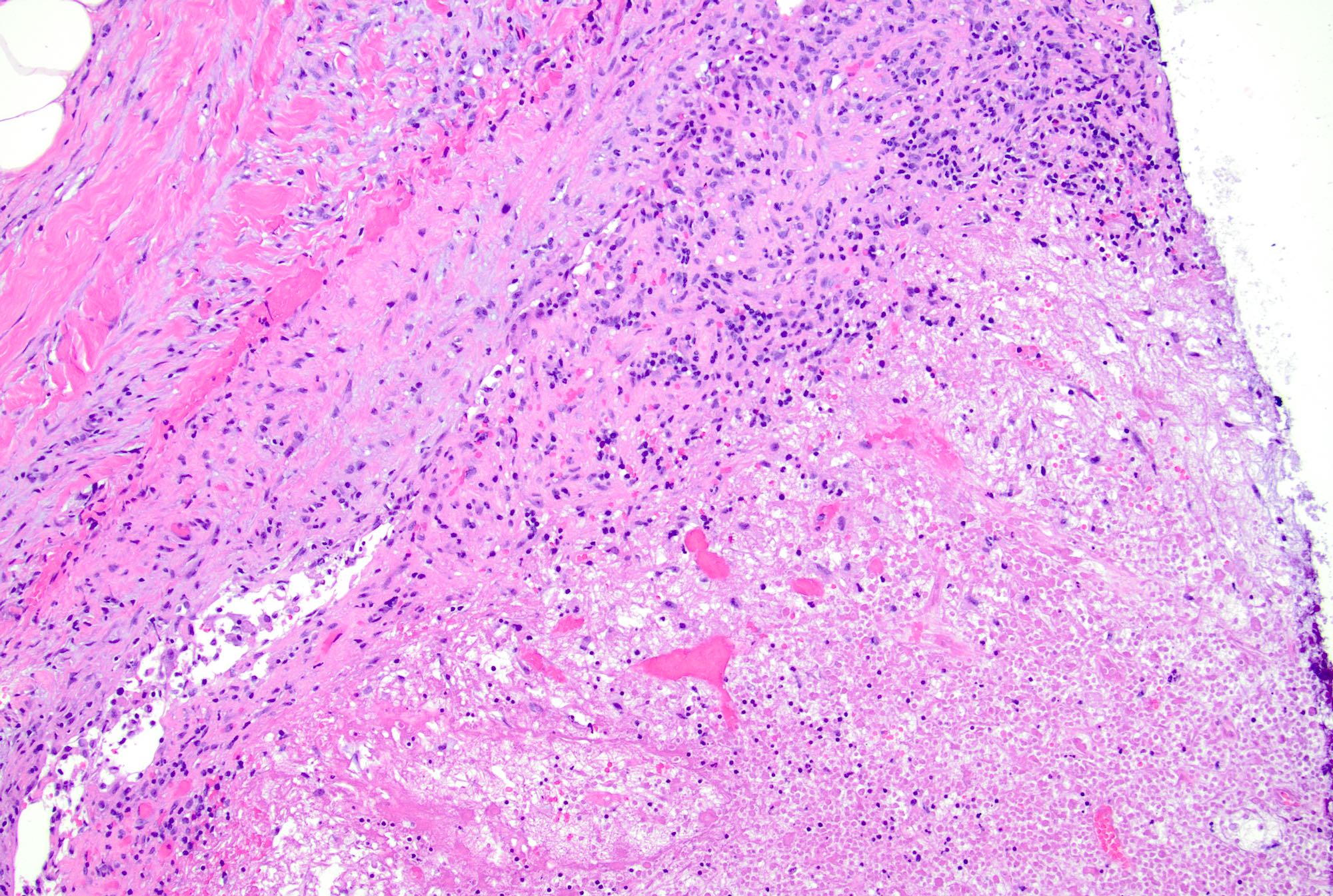
Necrosis
Chronic lymphadenitis
Primary follicle
Primary follicle
Primary follicle
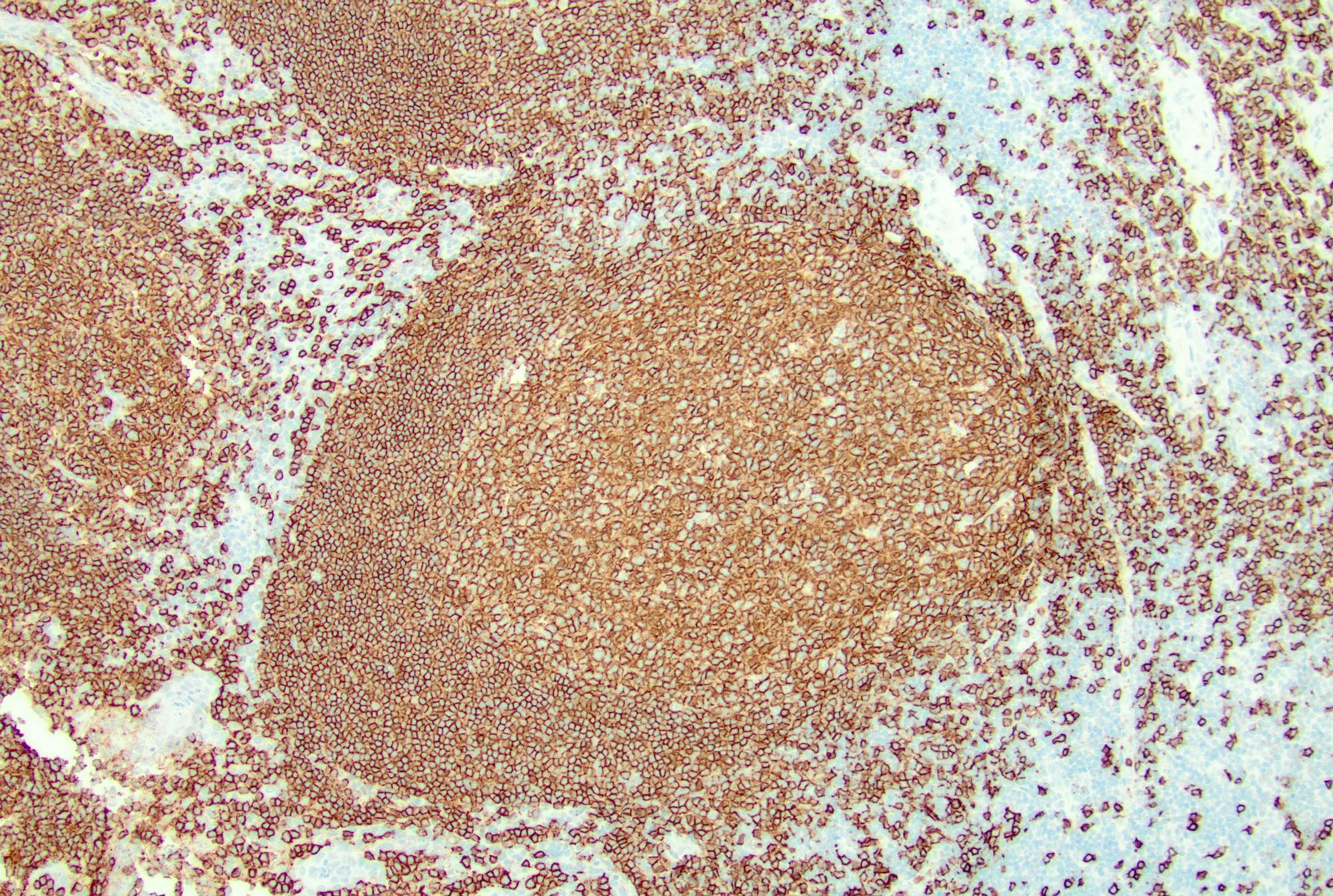
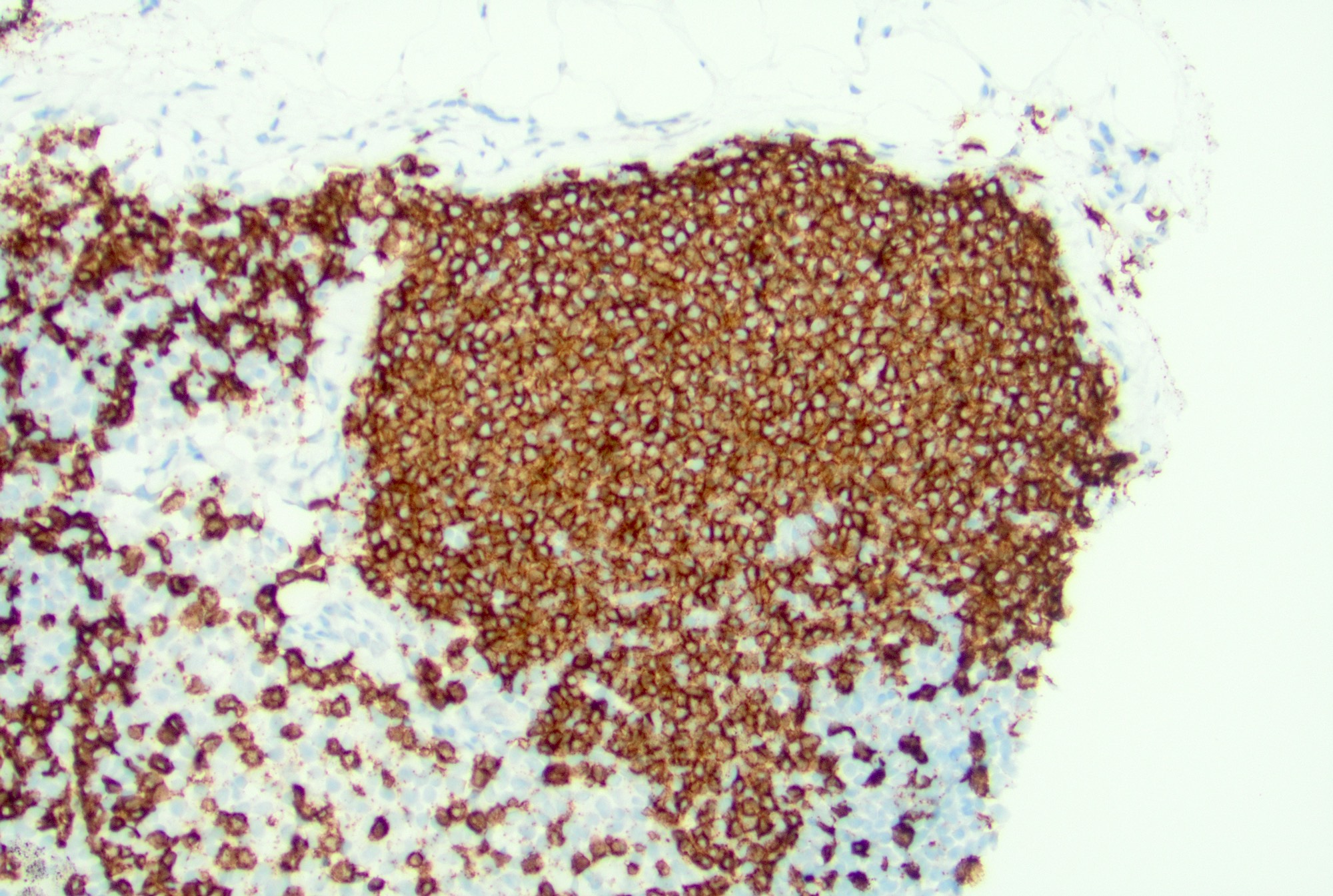
CD20
Germinal center
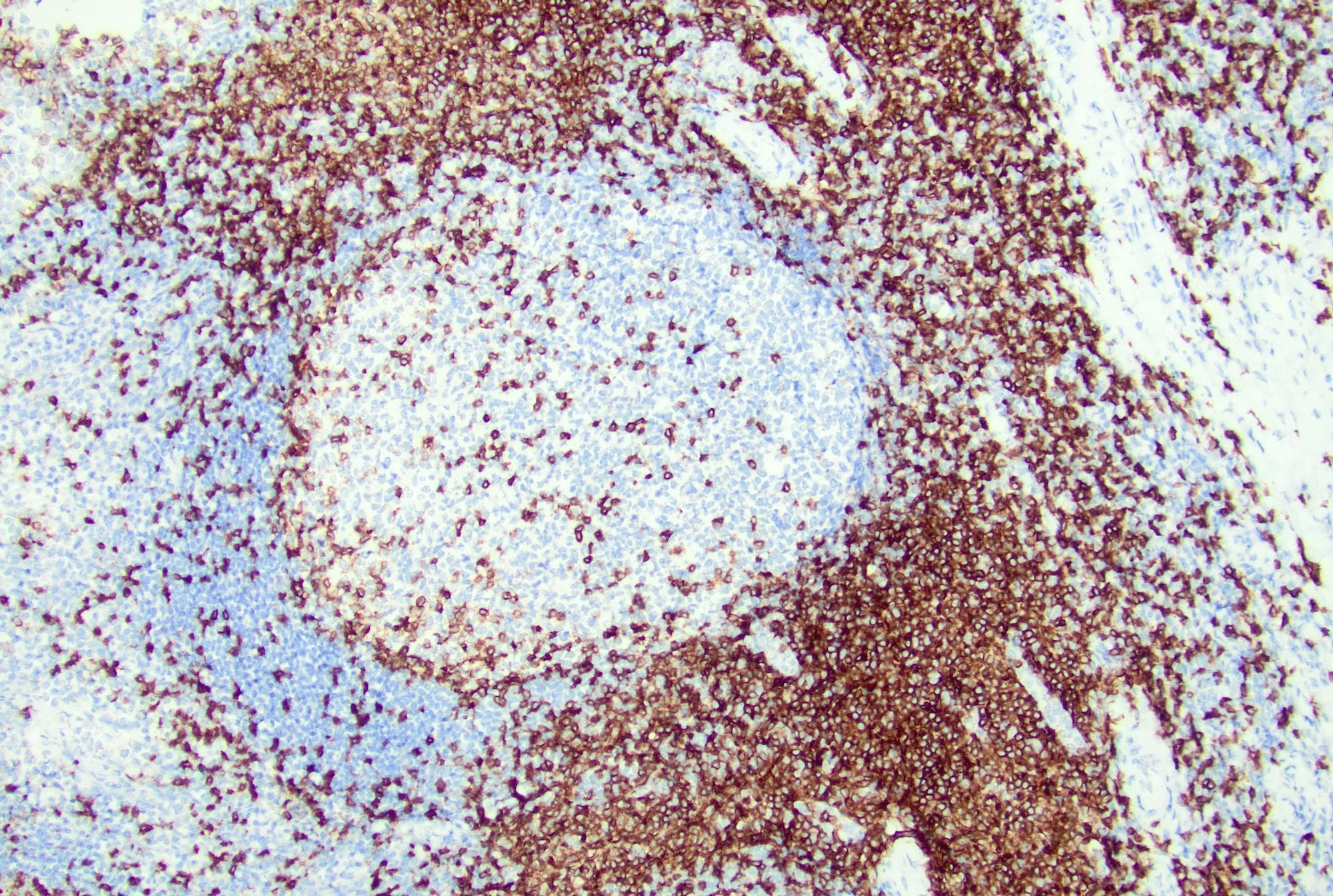
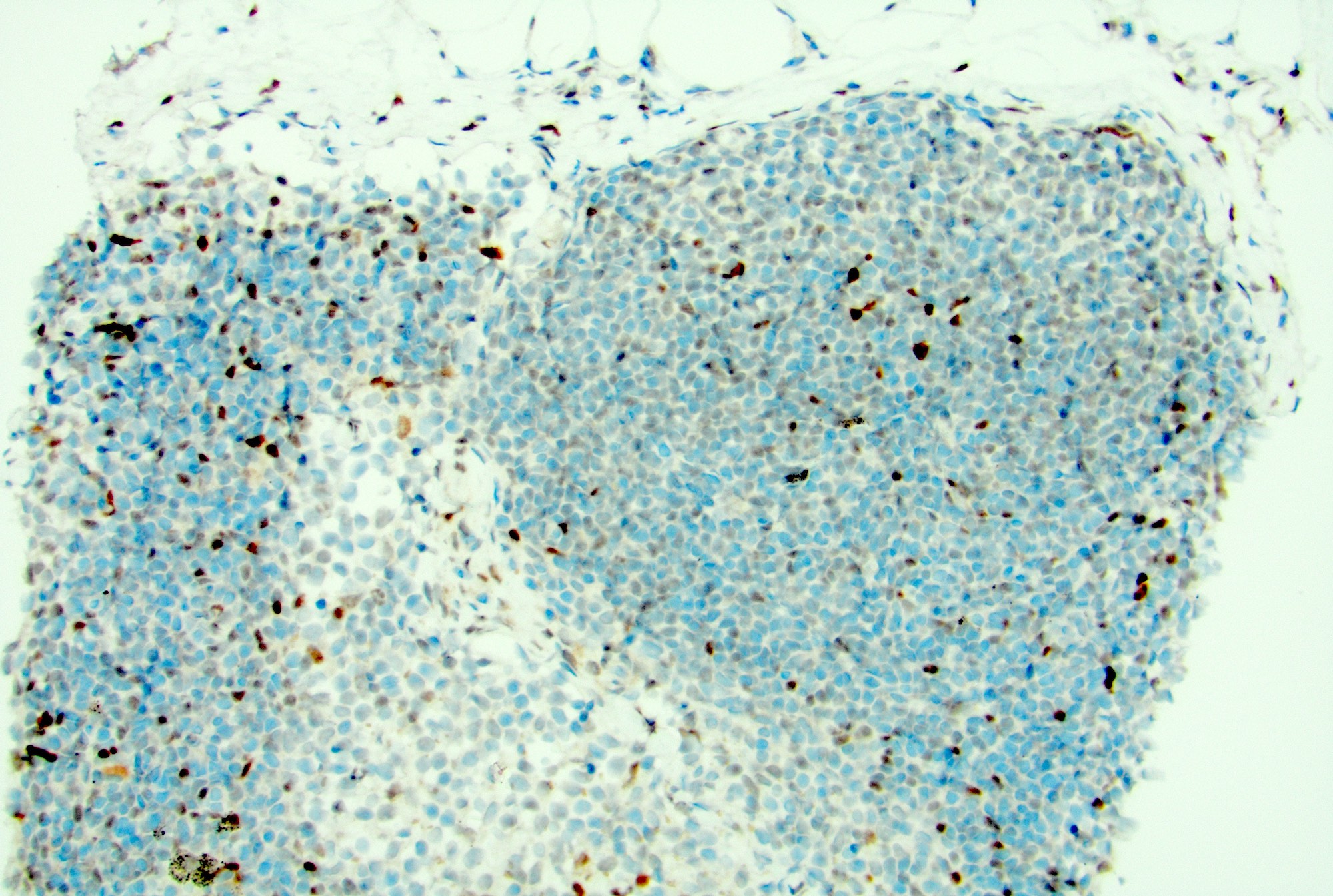
CD3
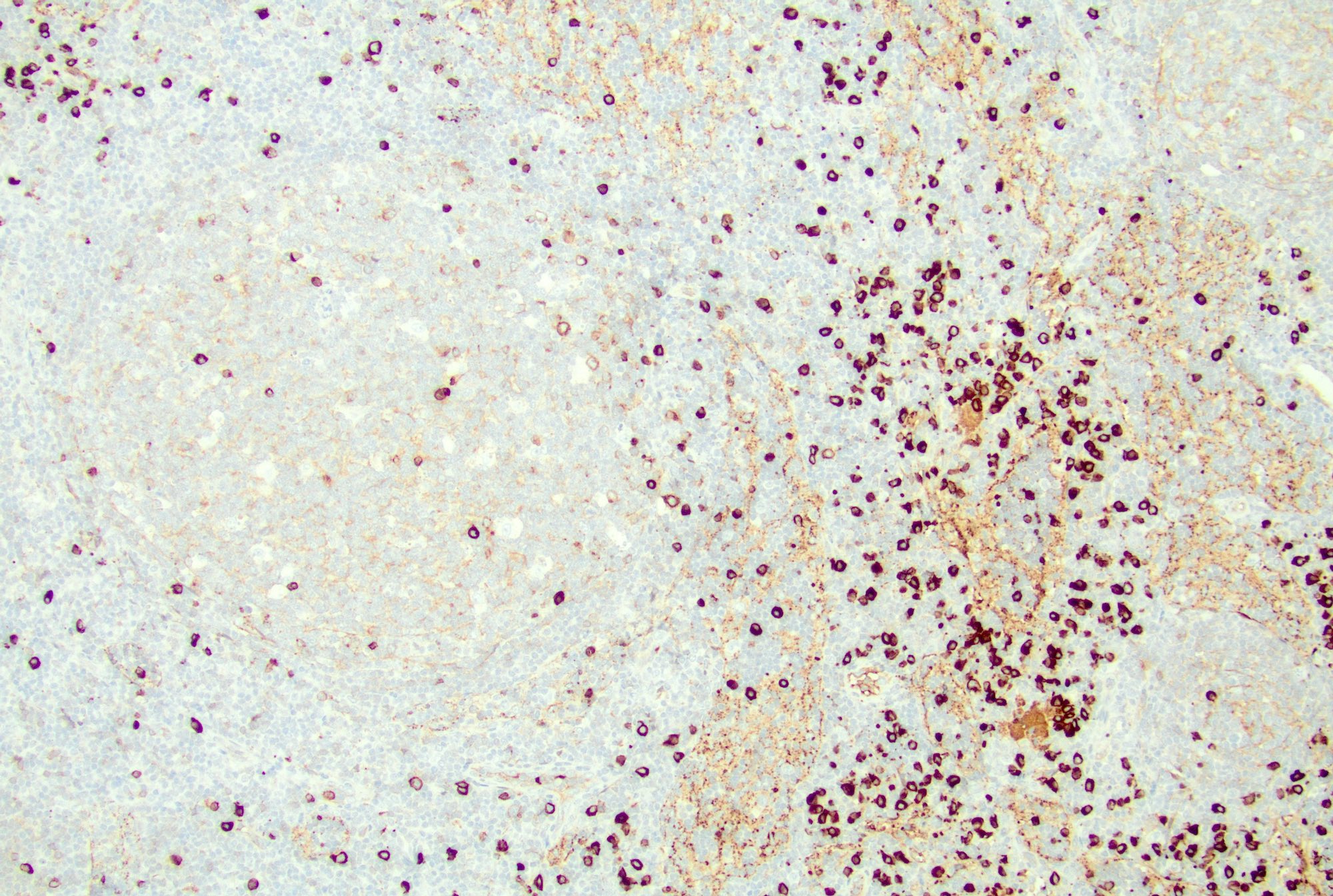
Plasma cells
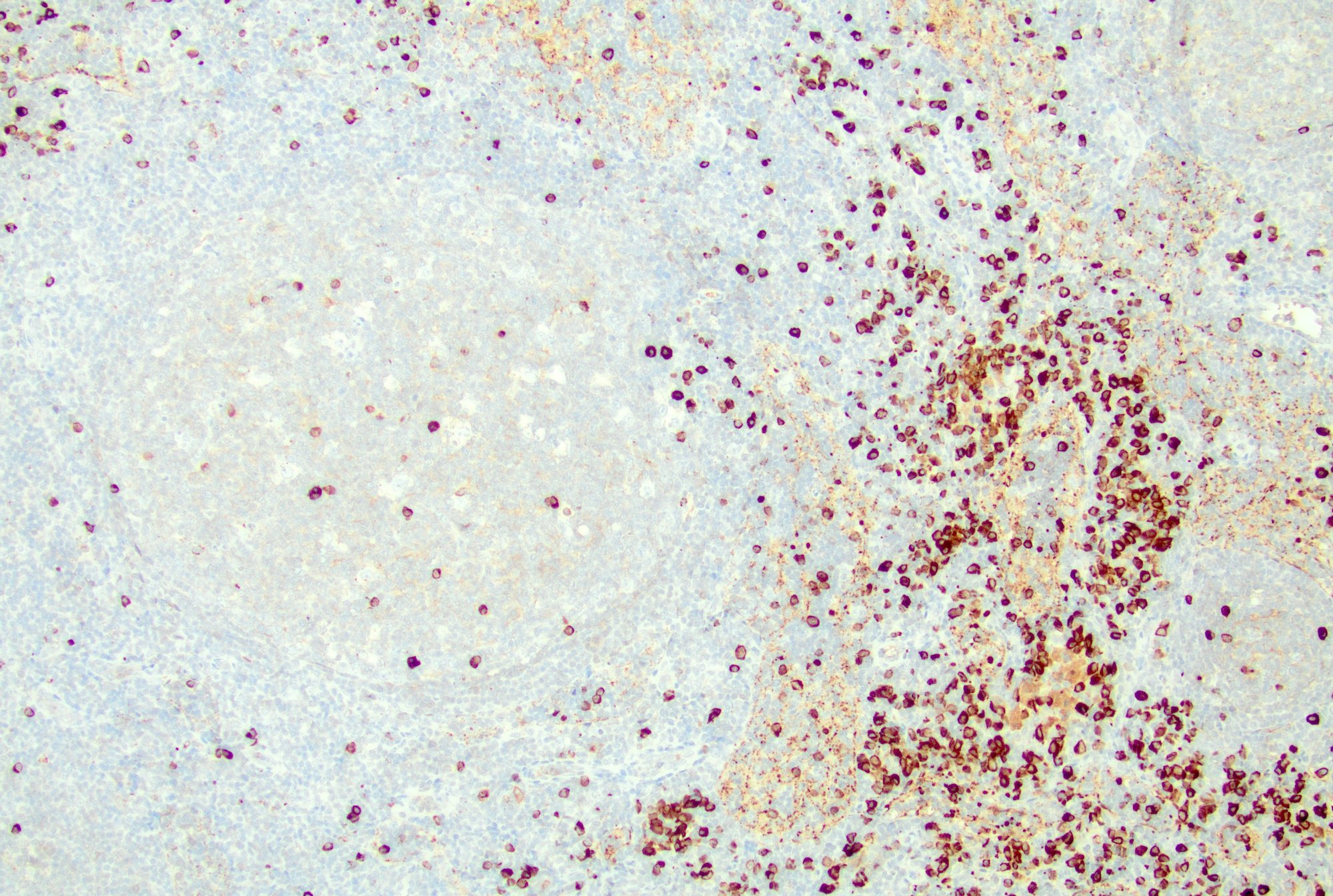
Plasma cells
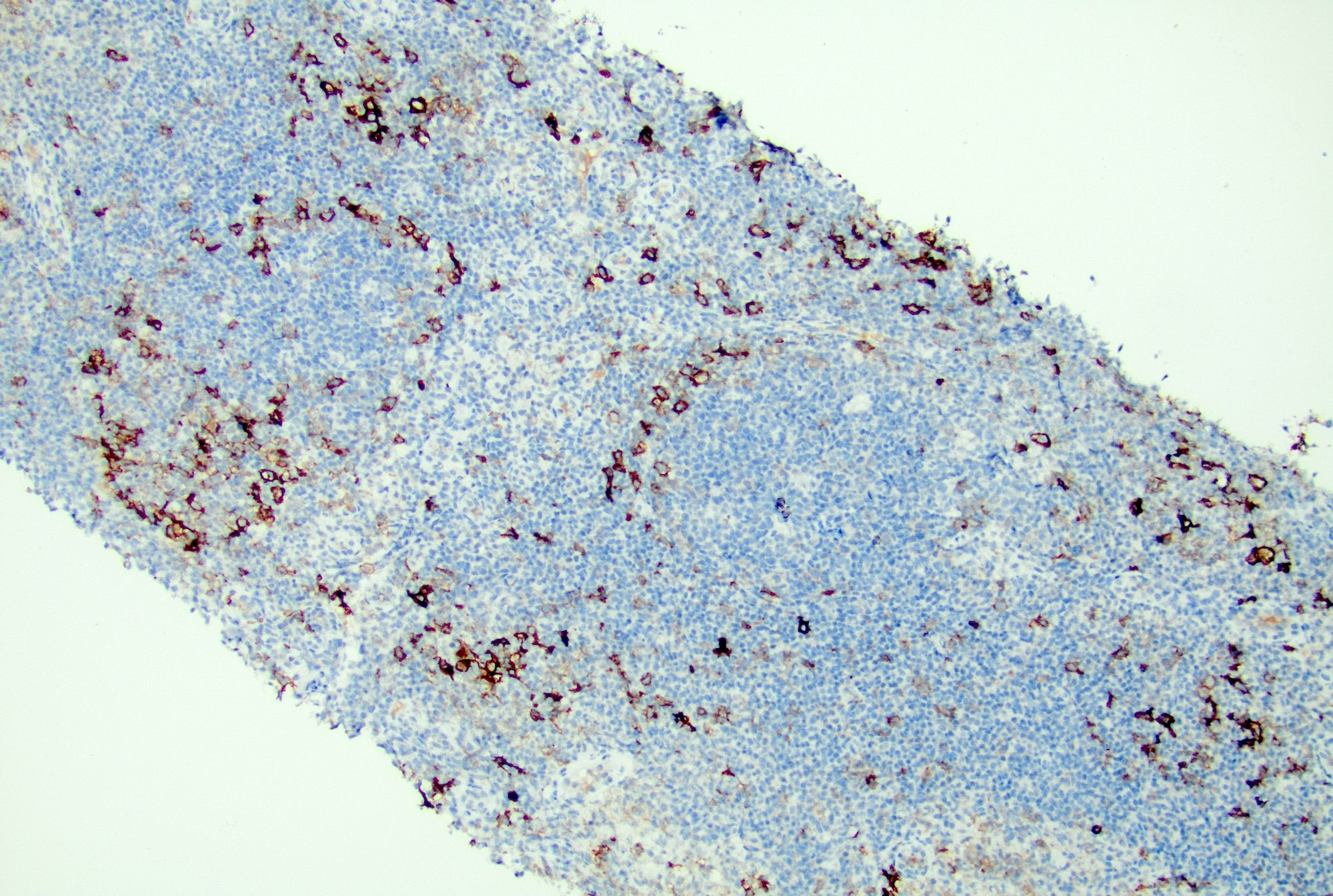
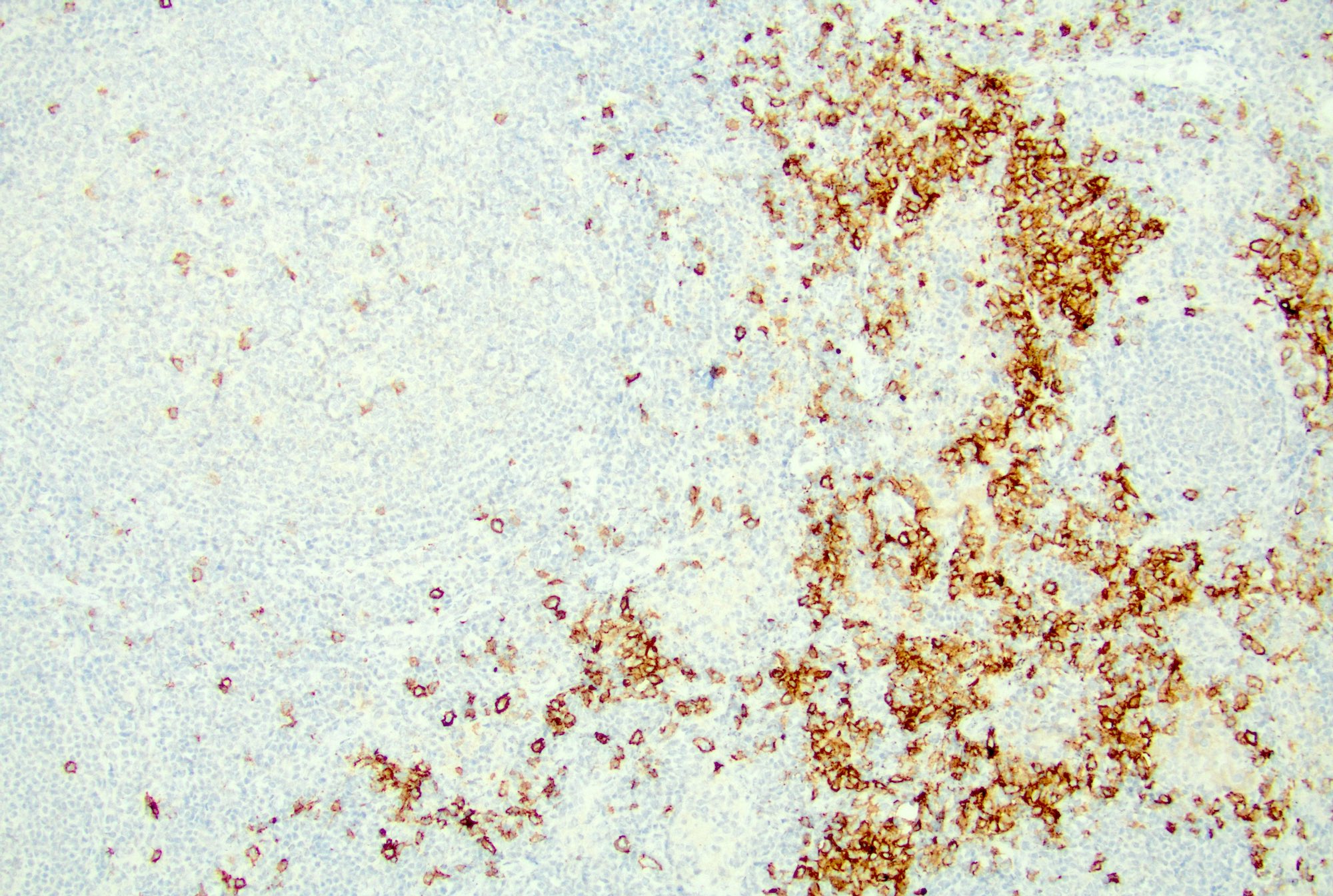
Immunoblasts
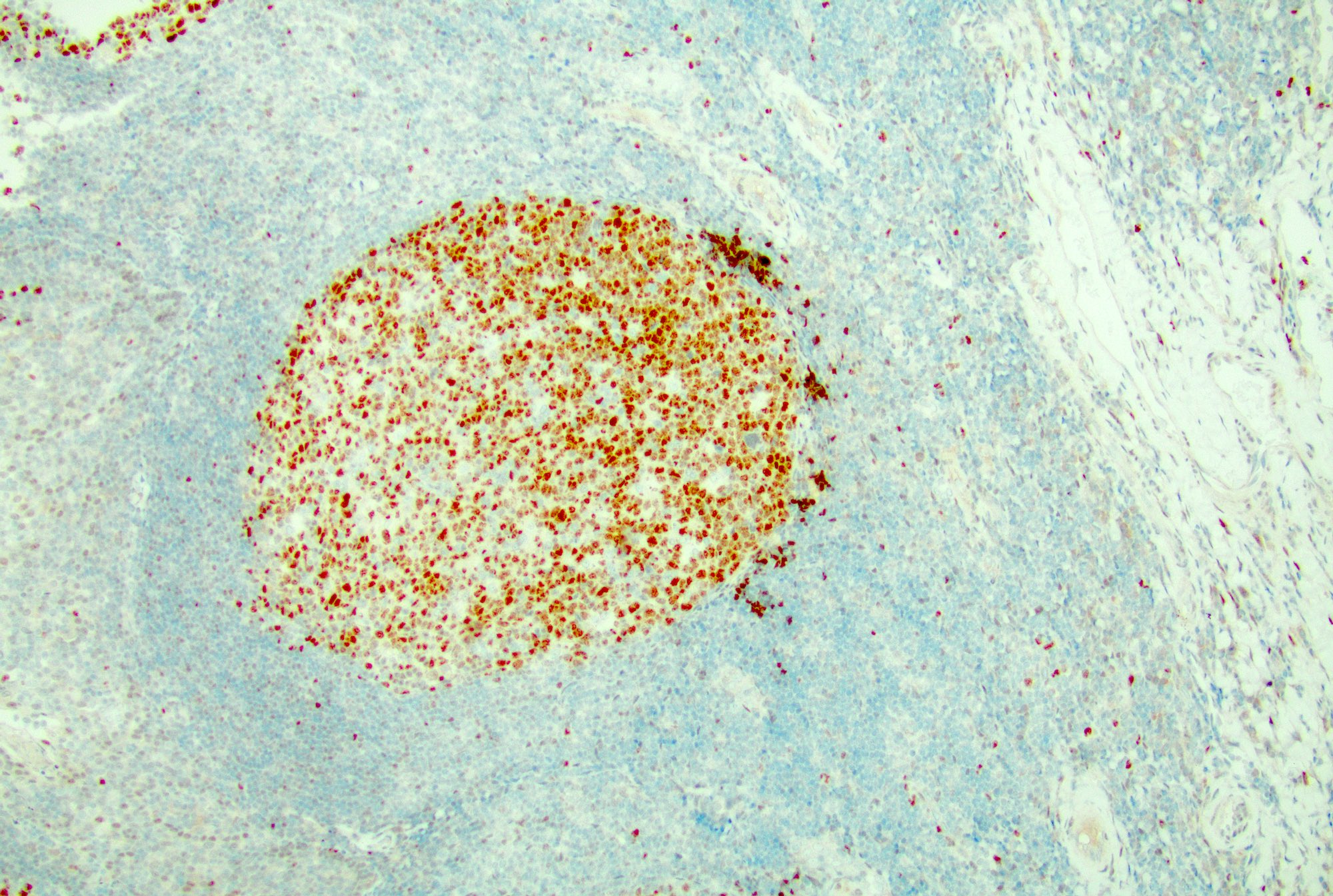
Polarization of germinal center
Reactive germinal center
Cytology description
- Cellular smears with mixed small and large lymphocytes, tingible body macrophages and other cell types including histiocytes and follicular dendritic cells
- In acute lymphadenitis, a prominence of neutrophils may be seen
Peripheral smear description
- In reactive lymphadenopathy, peripheral smears may show leukocytosis with either lymphocytosis or neutrophilia, depending on the underlying cause
Peripheral smear images
Contributed by Jayalakshmi Balakrishna, M.D.
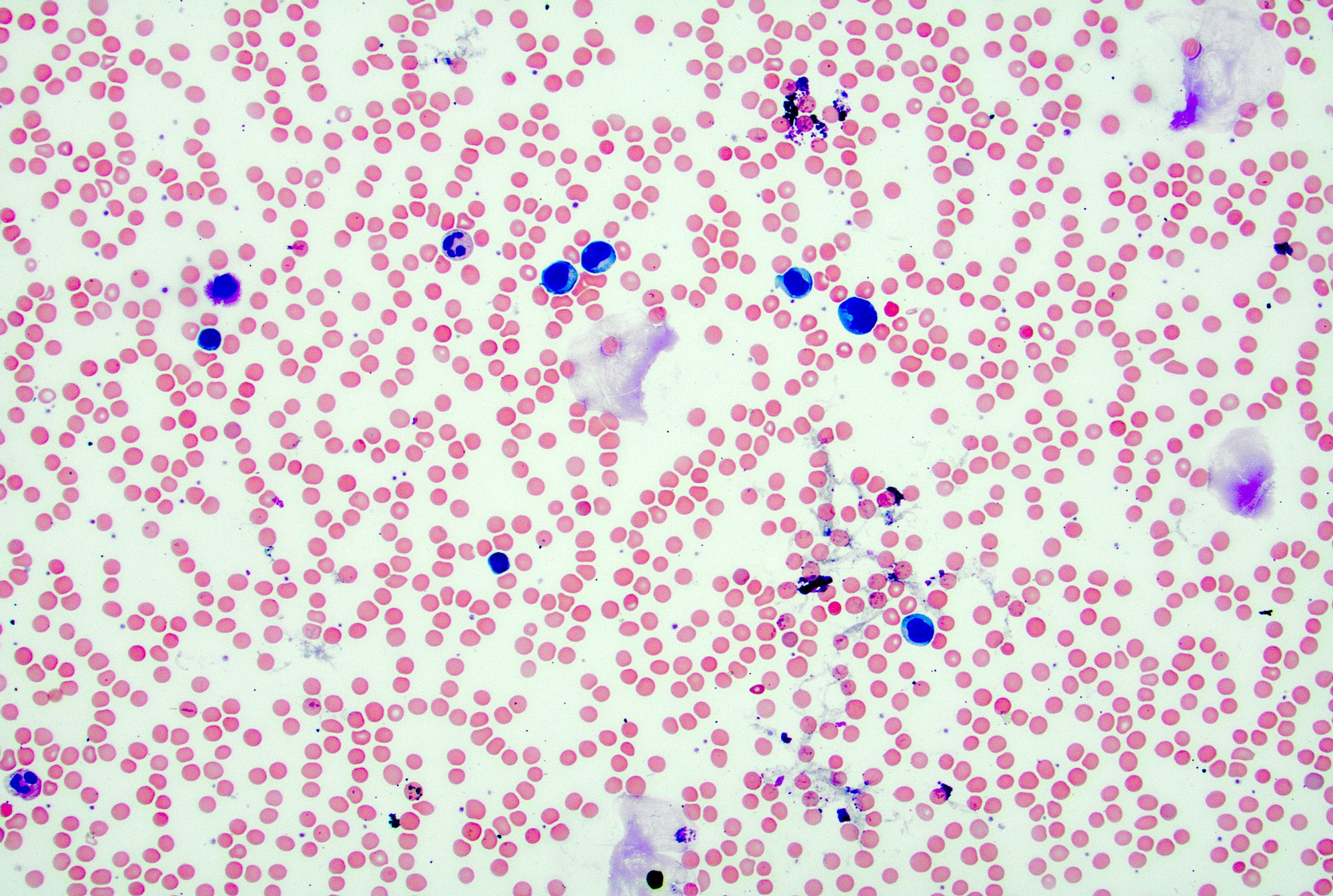
Lymphocytosis
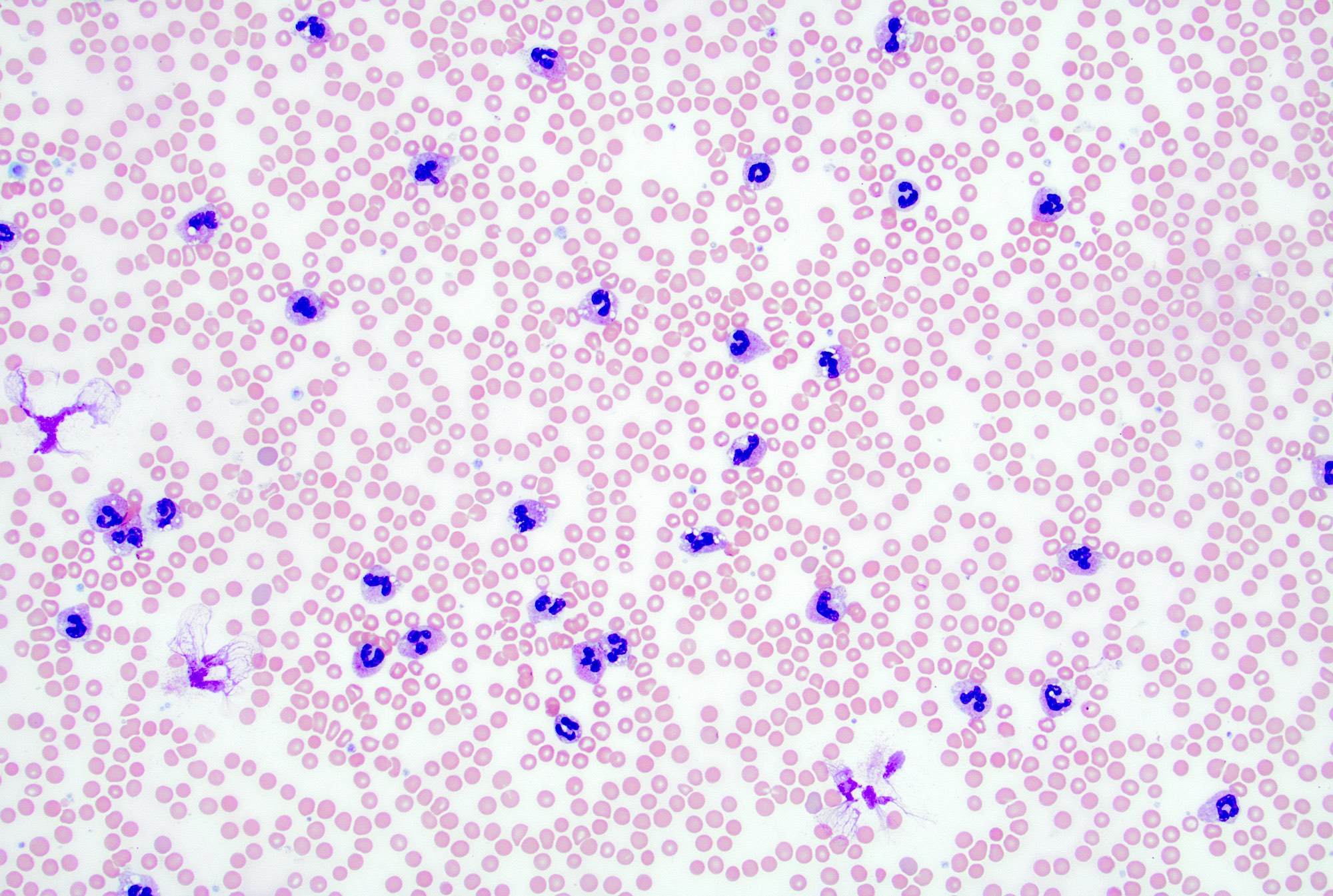
Neutrophilic leukocytosis
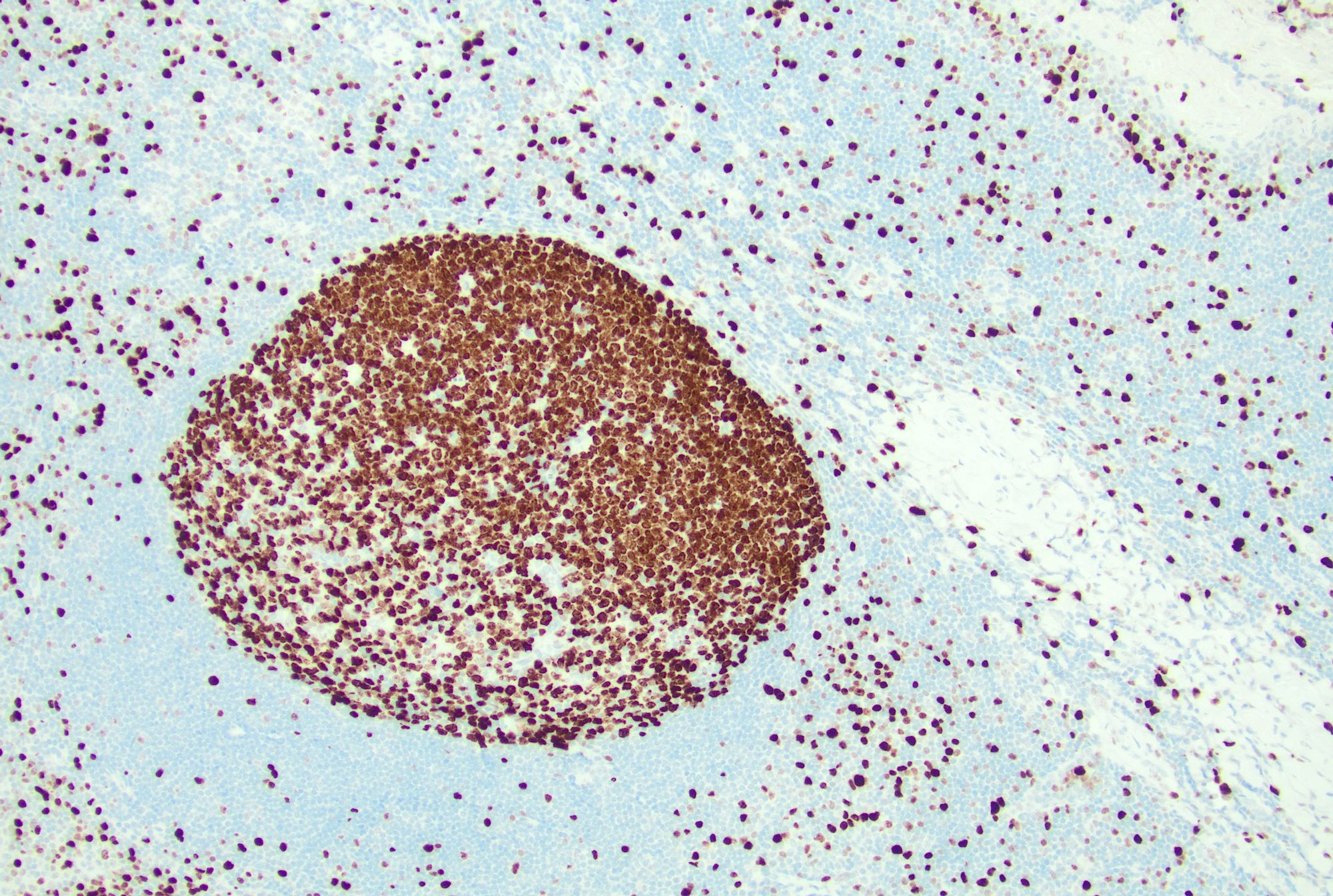
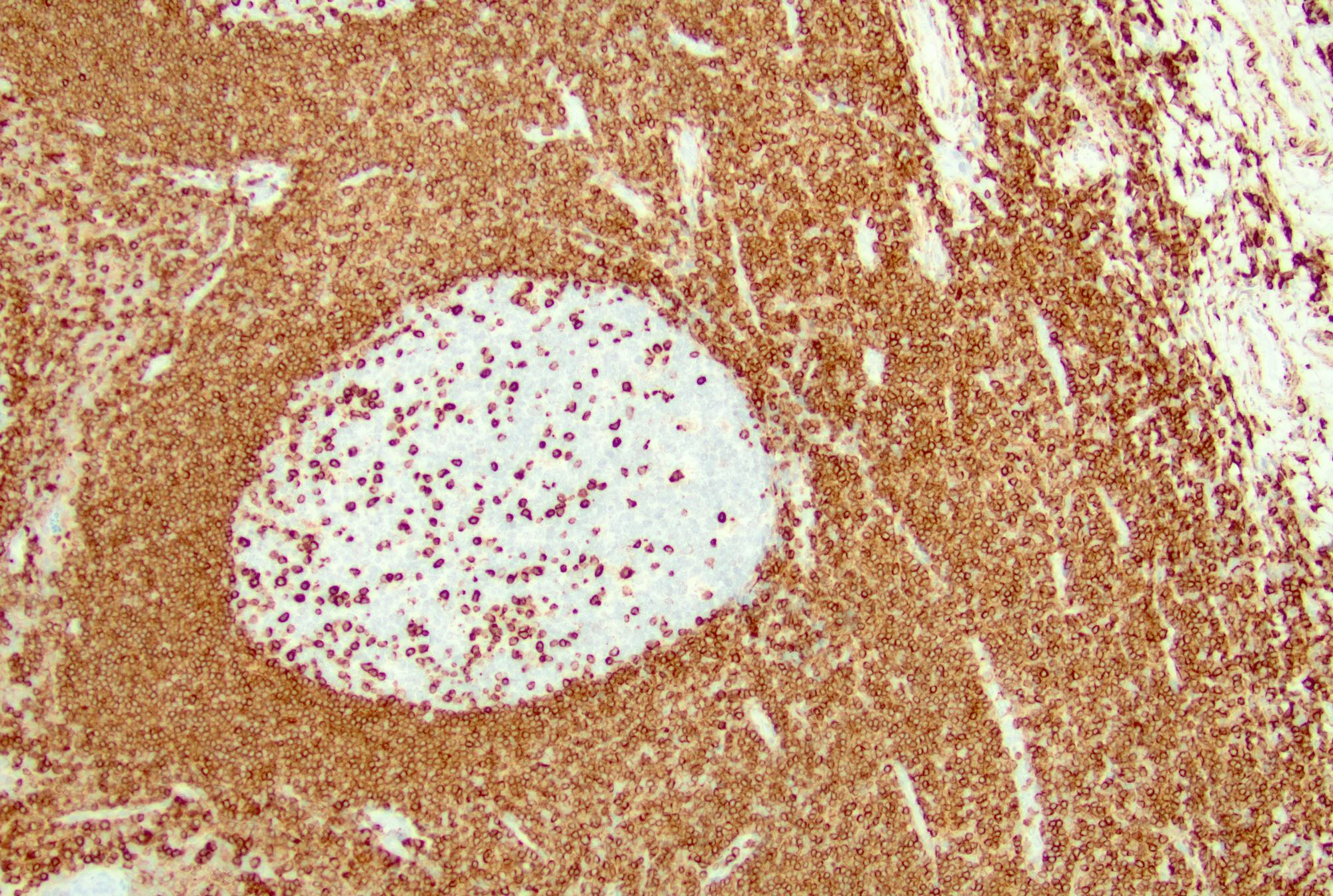
Positive stains
- Follicles: positive for pan-B cell markers, such as CD19, CD20, CD22, CD79a, PAX5
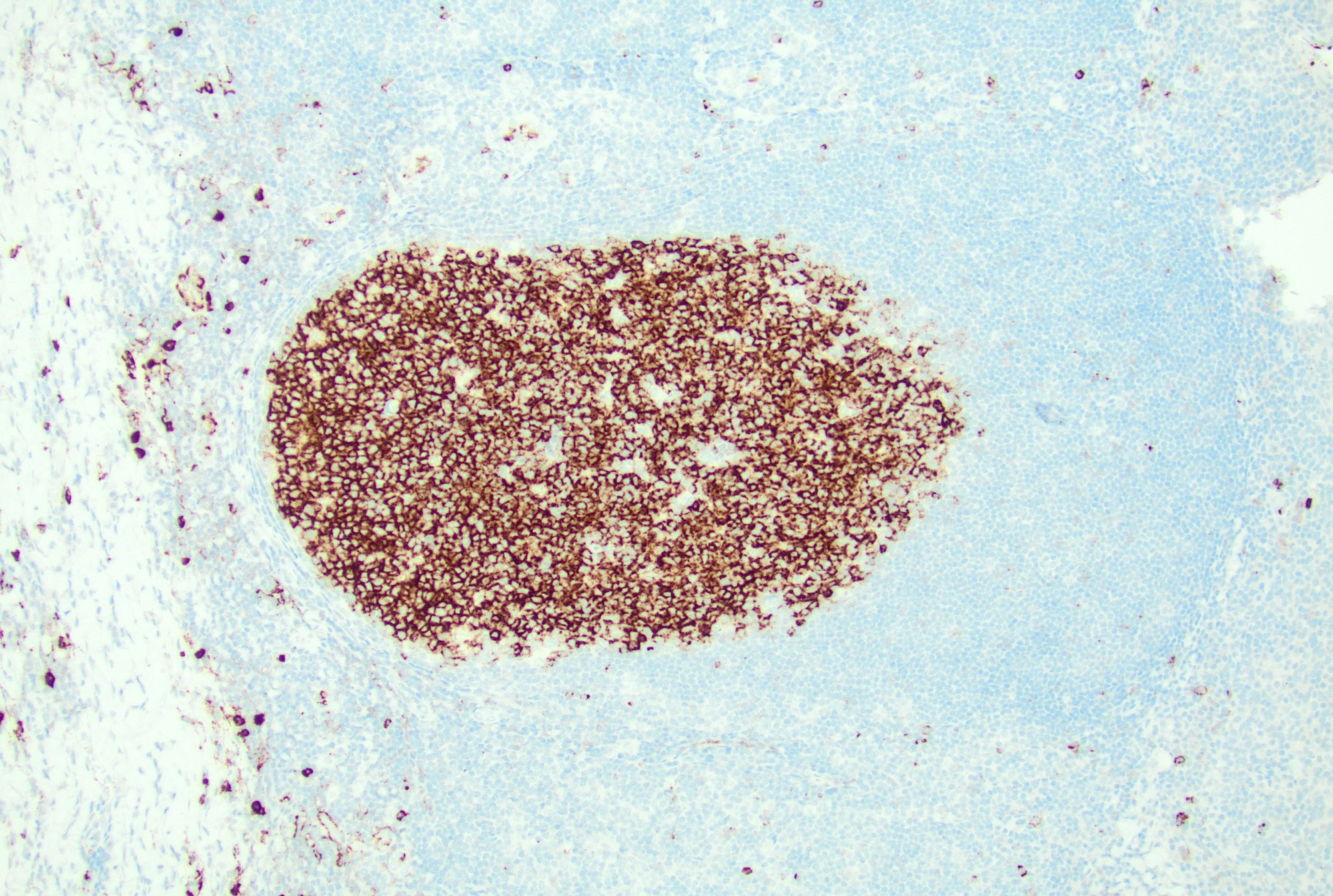
- Germinal centers: positive for germinal center markers, such as CD10 and BCL6
- Follicular dendritic cells: positive for CD21, CD23
- T cells: CD3, CD4, PD-1
- Plasma cells: CD138
- Paracortex (T cells): positive for pan-T cell markers, such as CD3, CD2, CD5 and CD7, mixed CD4 and CD8 positive T cells
- Immunoblasts: positive for CD30 (StatPearls: Histology, Lymph Nodes [Accessed 4 December 2024])
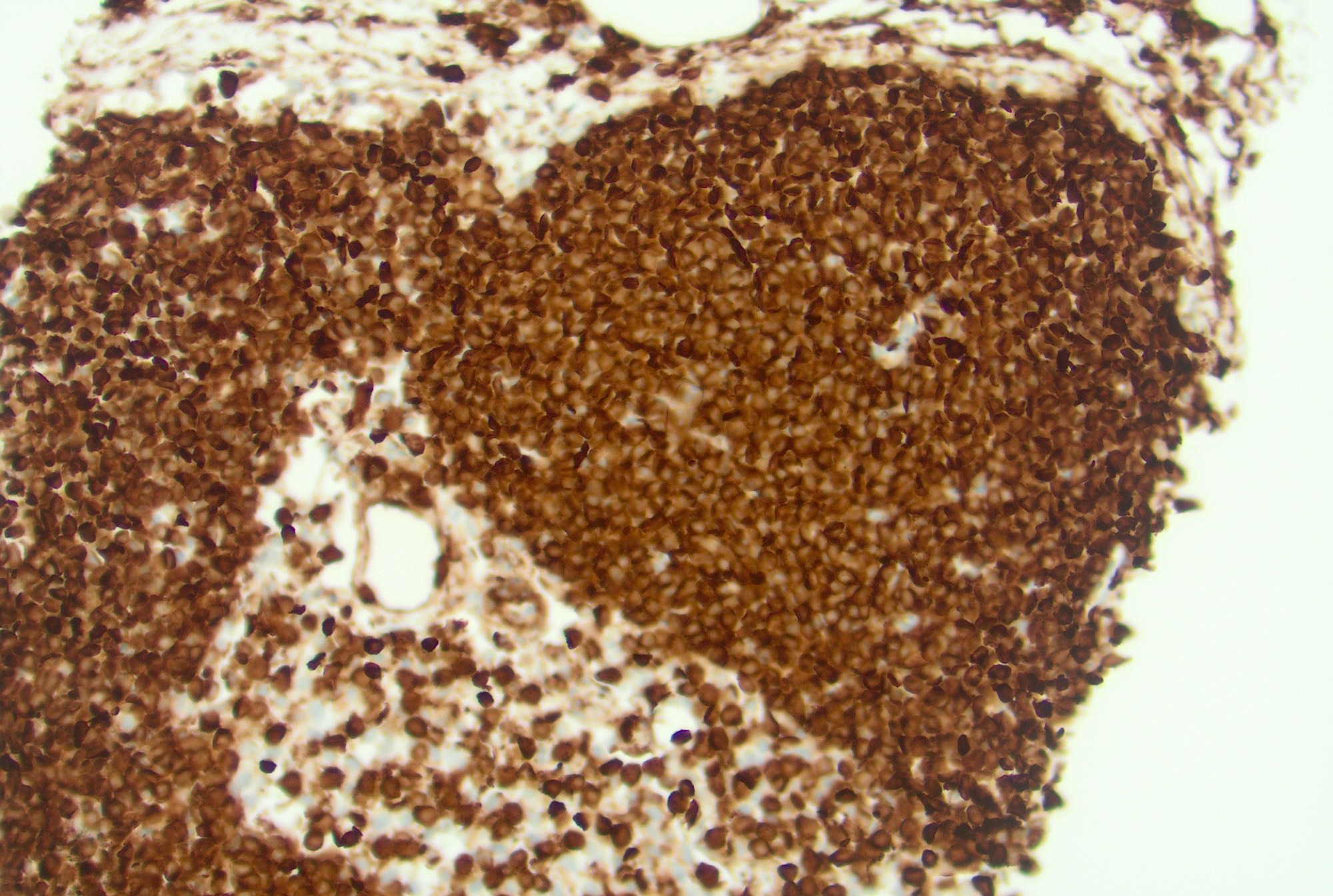
- Ki67: high proliferation rate in the germinal centers with polarization (dark zone with higher rate of proliferation and light zone with lower rate)
Negative stains
- Germinal center B cells: negative for BCL2
Flow cytometry description
- Mixed B and T cell populations
- T cells typically show mixed CD4+ and CD8+ subsets (Cytopathology 2022;33:505, J BUON 2013;18:739)
- Usually no immunophenotypic aberrancies but rarely clonal CD10+ B cell proliferations are detected by flow cytometry (Am J Clin Pathol 2004;121:464)
- B cells polytypic based on light chain pattern (except rare cases as above)
Flow cytometry images
Contributed by Jayalakshmi Balakrishna, M.D.
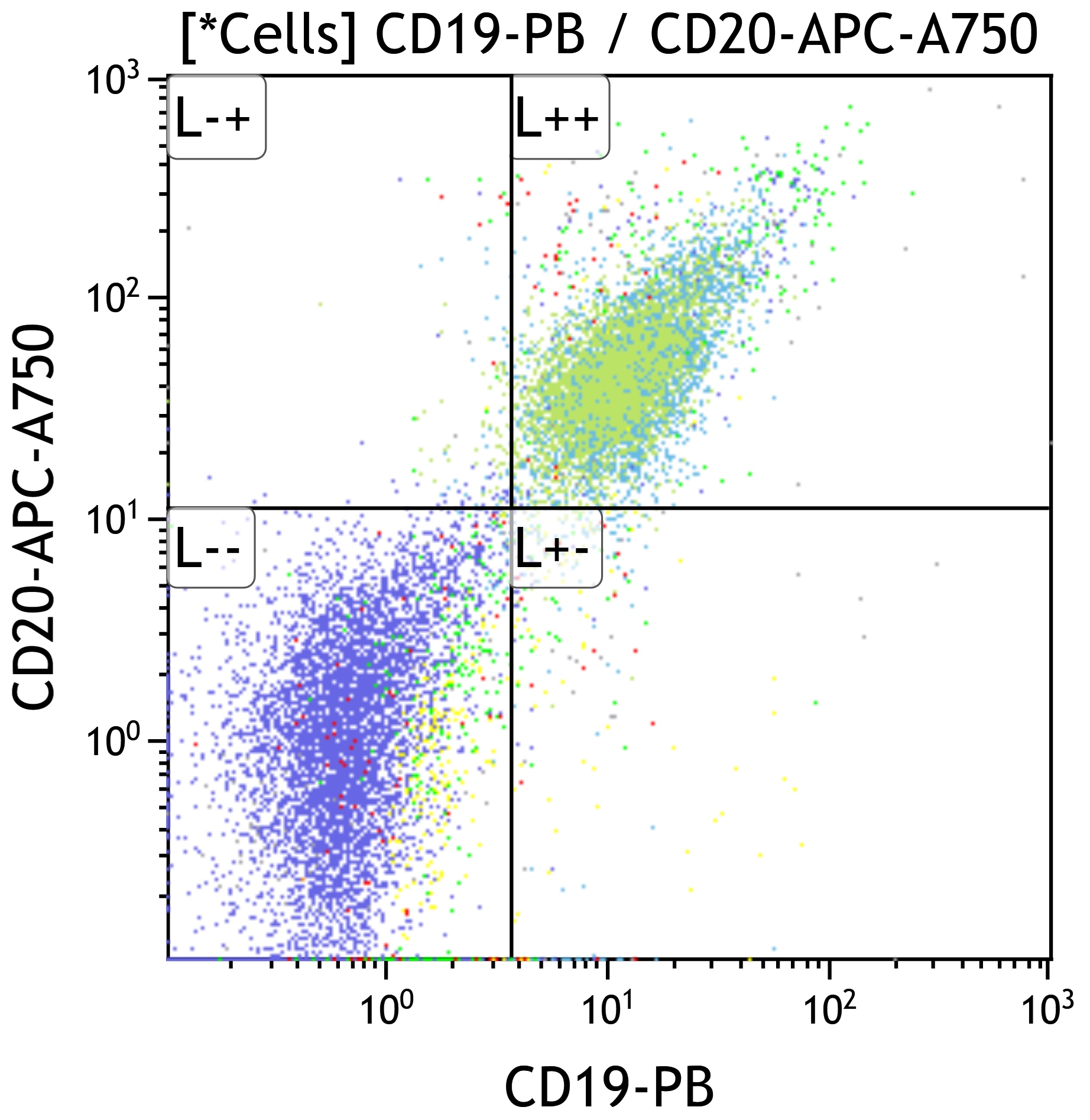
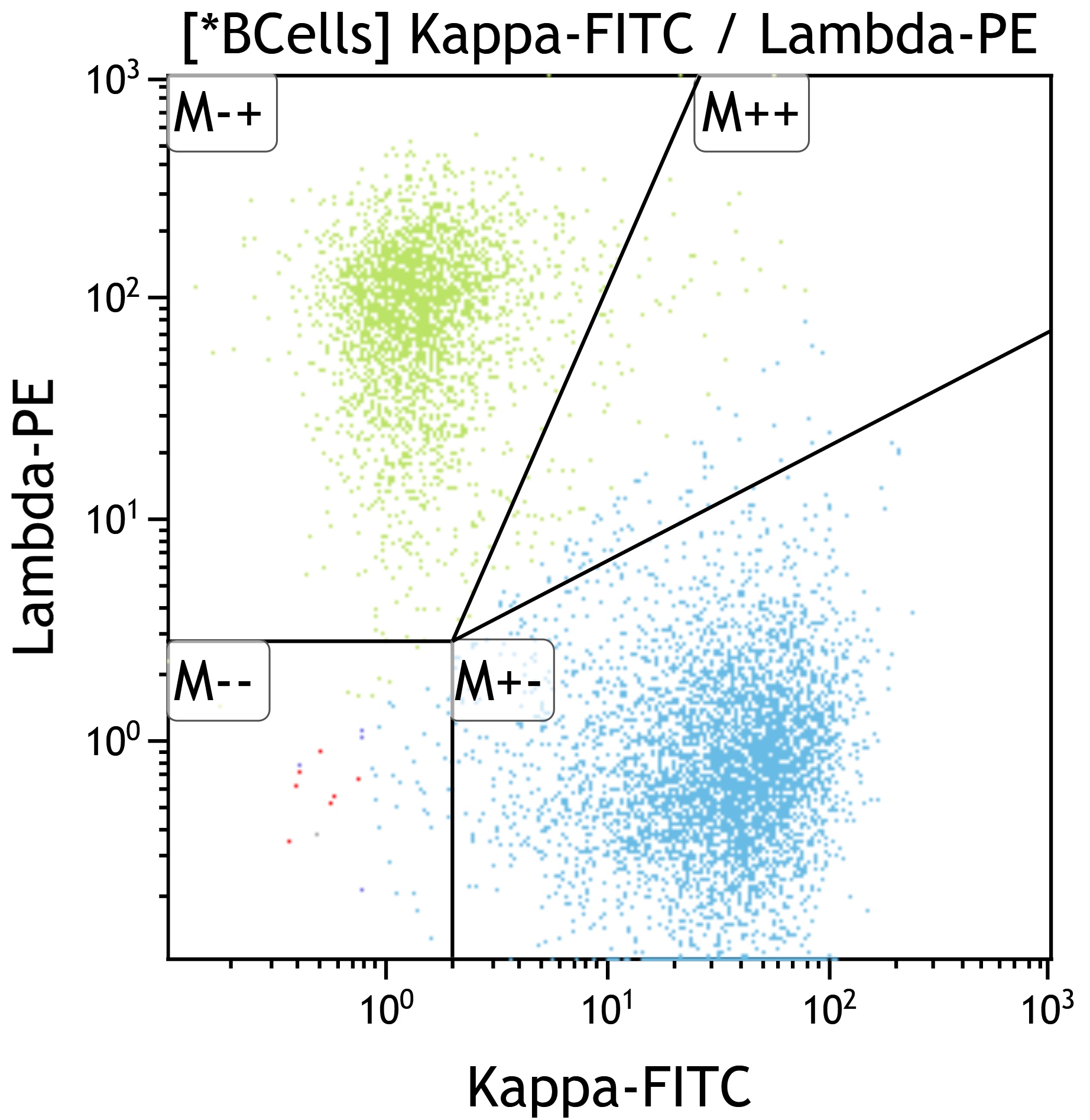
B cells
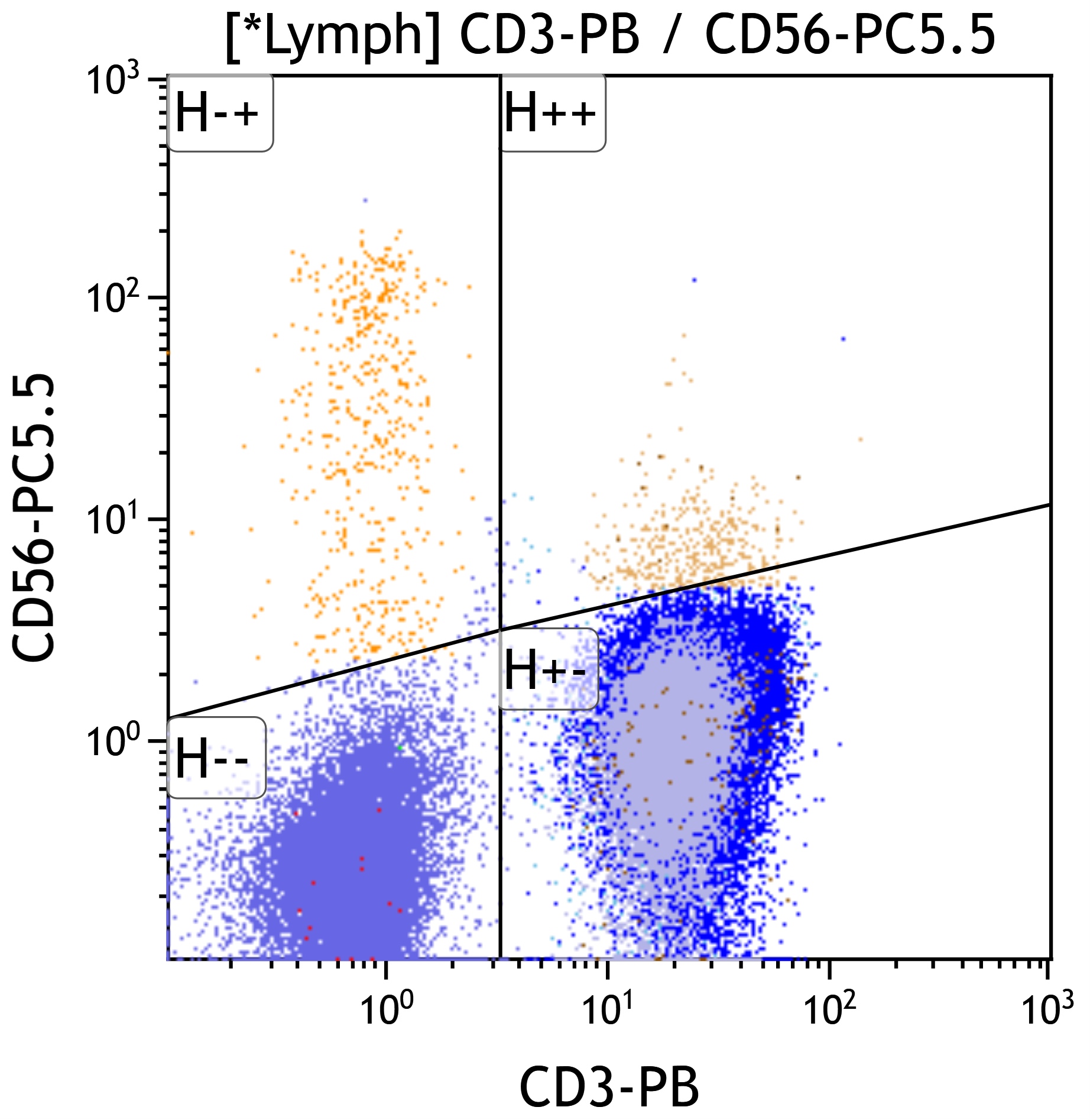
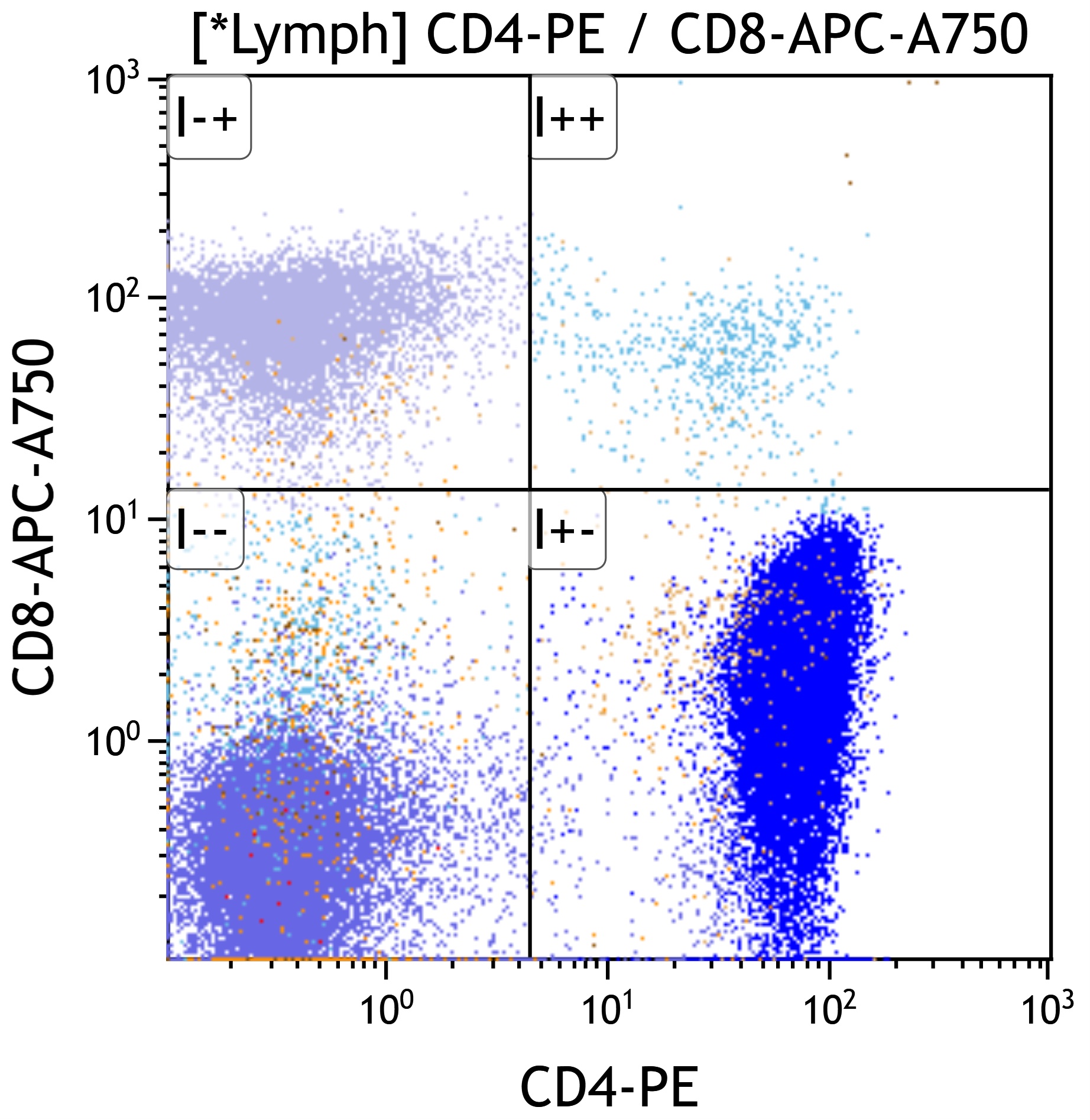
T cells
Molecular / cytogenetics description
- Polyclonal pattern of B and T cell gene rearrangements
- Negative for cytogenetic or molecular abnormalities
Sample pathology report
- Lymph node, left cervical, needle core biopsy:
- Reactive lymphoid hyperplasia and no morphologic or immunophenotypic evidence of a lymphoproliferative disorder
Differential diagnosis
- Follicular hyperplasia
- Classic follicular lymphoma:
- Effaced architecture, back to back follicles, invasion of capsule or adjacent structures, no polarization of the follicle, no tingible body macrophages, no well defined mantle zones
- Positive for CD10, BCL6 and BCL2, monotypic light chain expression, monoclonal B cell gene rearrangement and presence of t(14;18)
- In situ follicular neoplasia:
- No polarization with bright expression of CD10 and BCL2 in involved germinal centers, monotypic light chain expression, monoclonal B cell gene rearrangement and presence of t(14;18)
- Classic follicular lymphoma:
- Sinus histiocytosis
- Expansion of the sinuses with tumor cells
- Melanoma:
- Positive for S100 and melanocytic markers
- Mesothelioma:
- Positive for WT1 and other mesothelial markers
- Anaplastic large cell lymphoma:
- Rosai-Dorfman disease:
- Sinuses with accumulation of histiocytes with enlarged, round to oval hypochromatic nuclei and abundant eosinophilic cytoplasm, often containing engulfed intact inflammatory cells known as emperipolesis (Am J Surg Pathol 2021;45:35)
- Melanoma:
- Expansion of the sinuses with tumor cells
- Classic Hodgkin lymphoma (CHL):
- Architectural effacement with an inflammatory infiltrate containing large atypical cells with complex nuclear features (Hodgkin / Reed-Sternberg cells) in a mixed background of lymphocytes, histiocytes, plasma cells and eosinophils
- Generally morphologically distinct from reactive conditions but cases with partial nodal involvement, primarily interfollicular involvement or more mononuclear Hodgkin / Reed-Sternberg (HRS) forms can create diagnostic challenges
- Prolonged or atypical EBV associated lymphadenitis may develop and be observed on biopsy evaluation (Mod Pathol 2012;25:1149)
- EBV+ CHL can be distinguished based on cytologic atypia; EBER expression should be exclusive to the HRS cells
- Immunosuppression related and EBV associated lymphoproliferations:
- May show greater variation in morphology and marker expression
- Morphology may range from hyperplasias to polymorphic lymphoproliferative disorders to morphologic lymphoma
- Caution is advised in this setting, including correlation with clinical and radiographic status, type of immune suppression and whether the proliferation is viral associated (Leukemia 2022;36:1720)
- Specific causes of lymphadenitis need to be ruled out
- Acute:
- Lymphogranuloma venereum, cat scratch disease, bubonic plague, tularemia, anthrax, typhoid fever, melioidosis
- Chronic:
- Tuberculosis, leprosy, atypical mycobacteria, syphilis, fungal or parasitic infections:
- Special stains for the causative microorganisms will be positive
- Tuberculosis, leprosy, atypical mycobacteria, syphilis, fungal or parasitic infections:
- Acute:
Additional references
Board review style question #1
If a biopsy were performed, which morphologic feature would best differentiate an EBV+ classic Hodgkin lymphoma from an acute EBV lymphadenitis?
- Cytologic atypia in CD30+ cells
- Lack of detection of EBV protein EBNA2
- Paracortical expansion
- Positivity by CISH for EBV encoded RNA (EBER)
Board review style answer #1
A. Cytologic atypia in CD30+ cells. Malignant processes involving the lymph node can best be recognized by architectural distortion and cytologic atypia. Hodgkin / Reed-Sternberg cells in classic Hodgkin lymphoma will show complex nuclear features and express CD30, CD15 (often) and dim PAX5. When EBV associated, they will express EBER and EBV LMP1.
Answer B is incorrect because Hodgkin / Reed-Sternberg cells may express EBER and LMP1 but are always negative for EBNA2. EBNA2 may be expressed in EBV associated lymphadenitis but is not always present.
Answer D is incorrect because EBER can be expressed (although with different patterns) in EBV+ lymphadenitis as well as EBV+ classic Hodgkin lymphoma.
Answer C is incorrect because paracortical expansion can be seen in both reactive conditions and lymphoma. EBV+ lymphadenitis generally shows a paracortical expansion.
Comment Here
Reference: Reactive lymphadenopathy
Comment Here
Reference: Reactive lymphadenopathy
Board review style question #2
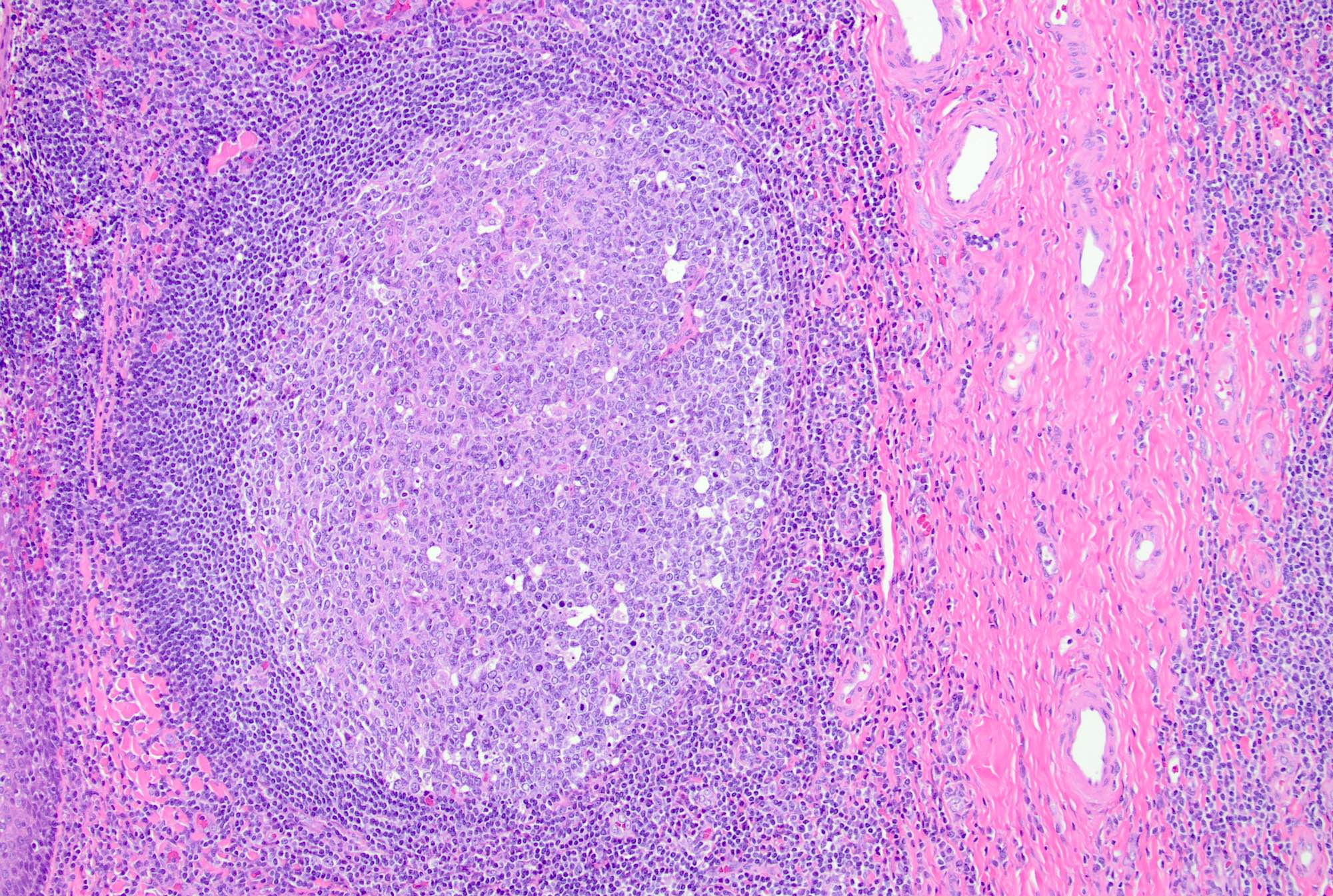
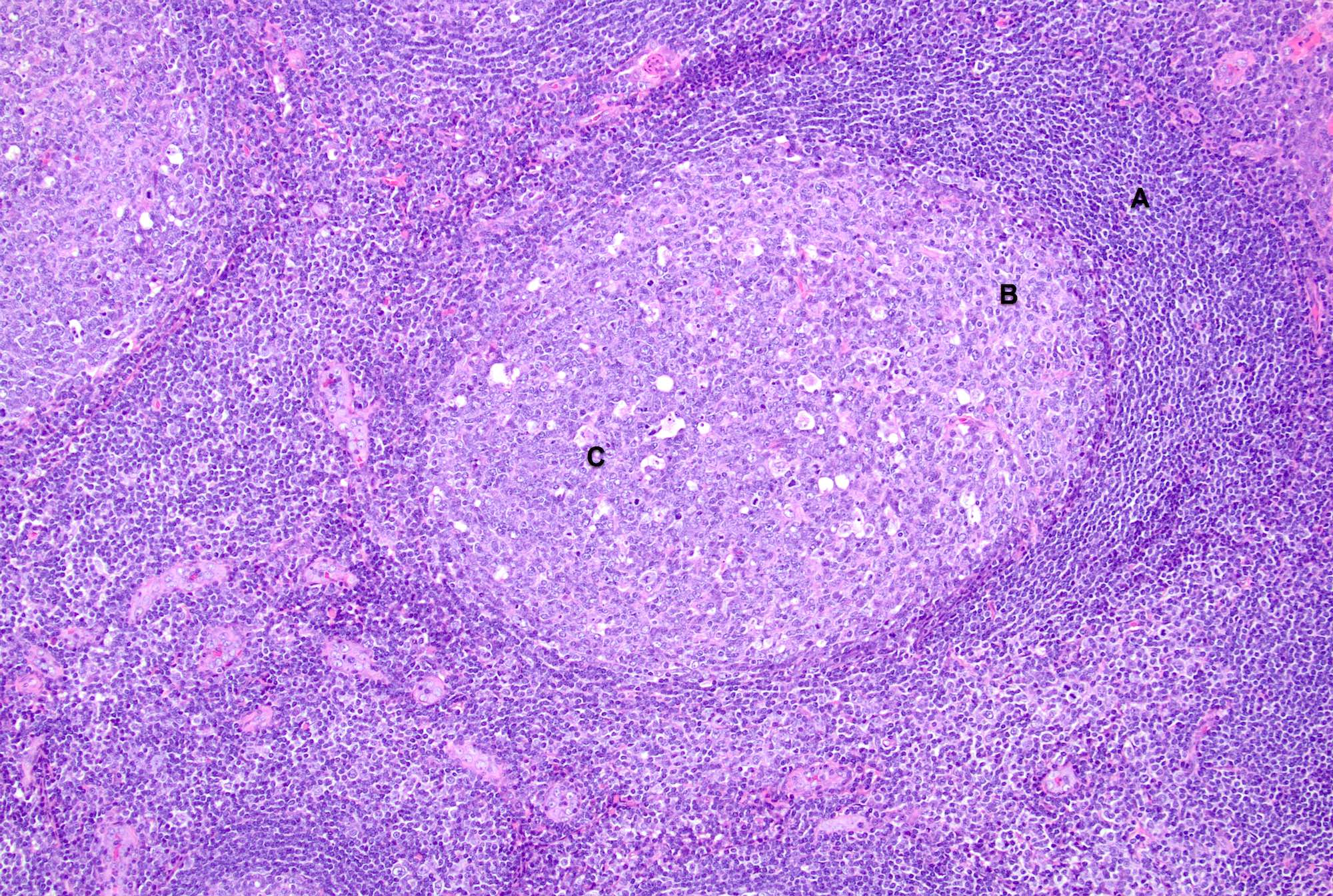
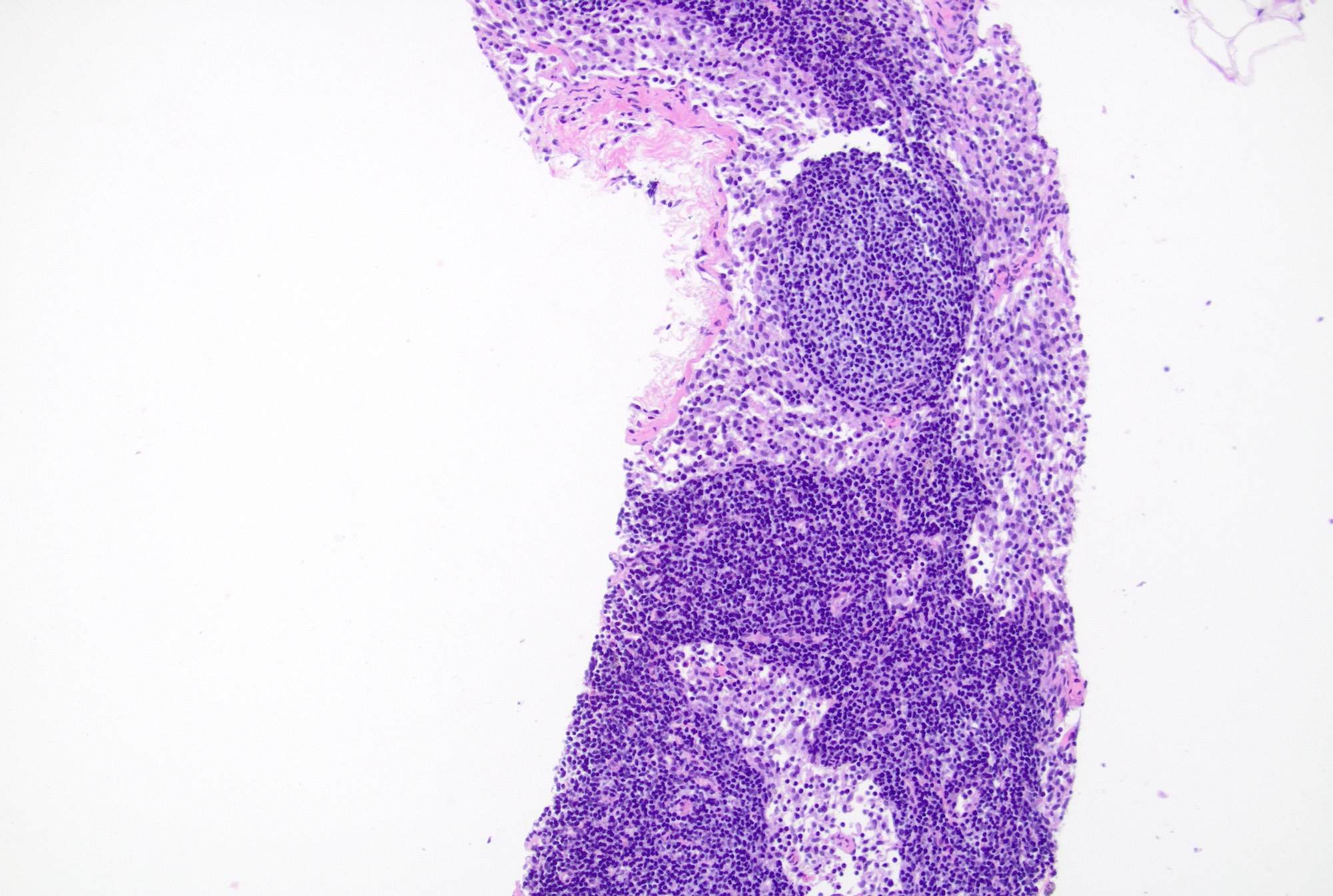
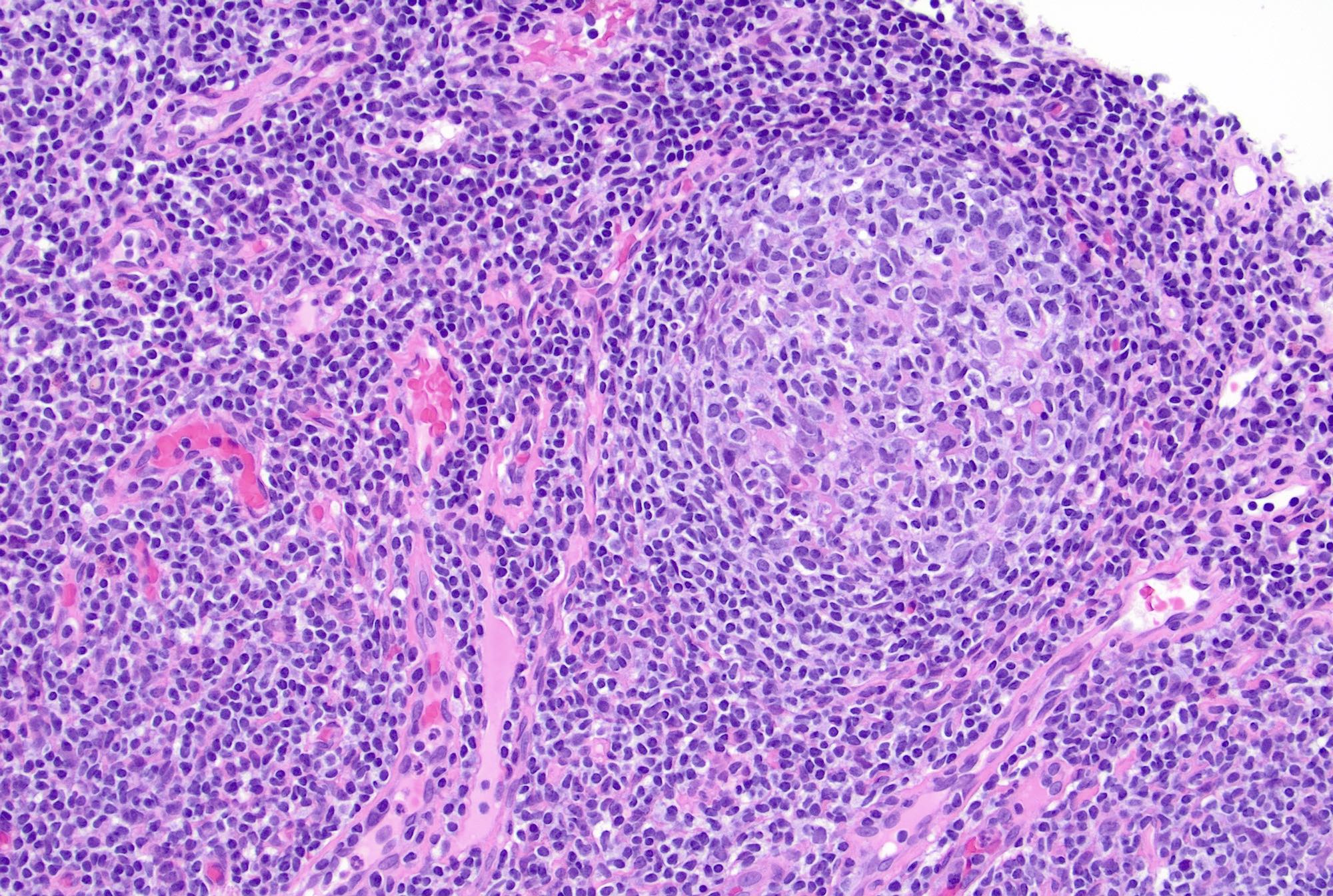
A 10 year old girl presents with bilateral cervical lymph node enlargement. Her parents state that she has had a fever and throat pain for the past few days. On examination, she is found to have multiple enlarged bilateral cervical lymph nodes. The above image shows a low power view of the cervical lymph node biopsy (H&E, 10x). What is the most likely diagnosis based on the H&E image?
- Burkitt lymphoma
- Follicular hyperplasia
- Follicular lymphoma
- Paracortical expansion
Board review style answer #2
B. Follicular hyperplasia. The presence of hyperplastic secondary follicles with prominent germinal centers, which show polarization and tingible body macrophages and mantle zone, is favorable for reactive follicular hyperplasia. Answer C is incorrect because follicular lymphoma shows effaced architecture with back to back follicles, absence of polarization and tingible body macrophages; it also lacks well defined mantle zones. Answer A is incorrect because Burkitt lymphoma is a diffuse proliferation of medium sized atypical lymphoid cells with blastoid morphology and conspicuous 1 - 3 nucleoli. Answer D is incorrect because paracortical hyperplasia is the expansion of interfollicular areas with mixed small lymphocytes, immunoblasts, vessels and interdigitating dendritic cells.
Comment Here
Reference: Reactive lymphadenopathy
Comment Here
Reference: Reactive lymphadenopathy
