
Lung
Neuroendocrine tumors
Carcinoid tumorlet
Editorial Board Member: Carolyn Glass, M.D., Ph.D.


Last author update: 30 November 2021
Last staff update: 3 May 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Tumorlet[TIAB] lung

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gagné A, Joubert P. Carcinoid tumorlet. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumortumorlet.html. Accessed January 4th, 2025.
Definition / general
- Tumor of neuroendocrine differentiation, defined by size < 5 mm in diameter, mitotic count < 2 mitoses/2 mm² and absence of necrosis
Essential features
- Can be found incidentally in lung resections but can arise in the context of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH)
- Defined as a proliferation of neuroendocrine cells < 5 mm in diameter that extend through the bronchial basement membrane with < 2 mitoses/2 mm² and no necrosis
- Progression to typical carcinoid tumors is possible
ICD coding
Epidemiology
- Typically affects middle aged women (Ann Oncol 2010;21:vii65, Chest 2007;131:1635):
- Frequent incidental finding in lung resection specimens or can be found in the context of DIPNECH
- Real incidence and prevalence unknown:
- Often missed on imaging and can be easily overlooked during grossing because of their small size (J Thorac Oncol 2009;4:383, Med Sci Monit 2020;26:e926014)
- Can be found in lung specimens resected for typical (8%) or atypical (4.3%) carcinoids (J Thorac Oncol 2009;4:383)
- Can be found in patients with multiple endocrine neoplasia type 1 (MEN1) (Neuroendocrinology 2016;103:240)
Sites
- Tumorlets are located in the same region as inflammatory or fibrous lung disease (AJR Am J Roentgenol 2004;183:293)
- When arising in the context of DIPNECH, they are typically located in the terminal bronchioles
Pathophysiology
- Not well described
- Incidental finding in lung resection specimens, accompanying inflammatory or fibrous conditions (J Thorac Dis 2012;4:655, Med Sci Monit 2020;26:e926014, Int J Surg Pathol 2018;26:660, Respirol Case Rep 2018;6:e00373t)
- Presence of multiple carcinoids more likely to be part of DIPNECH
- It is believed that some tumorlets may progress into carcinoid tumors, mostly typical carcinoids (AJR Am J Roentgenol 2010;195:661)
Etiology
- Unknown
Clinical features
- Frequently asymptomatic, as it can be an incidental finding (AJR Am J Roentgenol 2010;195:661)
- Clinical features of DIPNECH can be seen in patients with tumorlets arising in this context
Diagnosis
- See DIPNECH for details on diagnosis for tumorlets arising in this setting
Radiology description
- CT scan: can present as a bronchial wall thickening that can appear nodular or show multiple peribronchiolar spherical to ovoid solid or ground glass nodules (Clin Radiol 2015;70:317)
- Images are similar to the ones for DIPNECH when arising in this context
- When tumorlets arise in a context of chronic pulmonary lung disease, they can be subtle and masked by the underlying process (Med Sci Monit 2020;26:e926014)
Radiology images
Contributed by Andréanne Gagné, M.D., M.Sc. and Philippe Joubert, M.D., Ph.D.
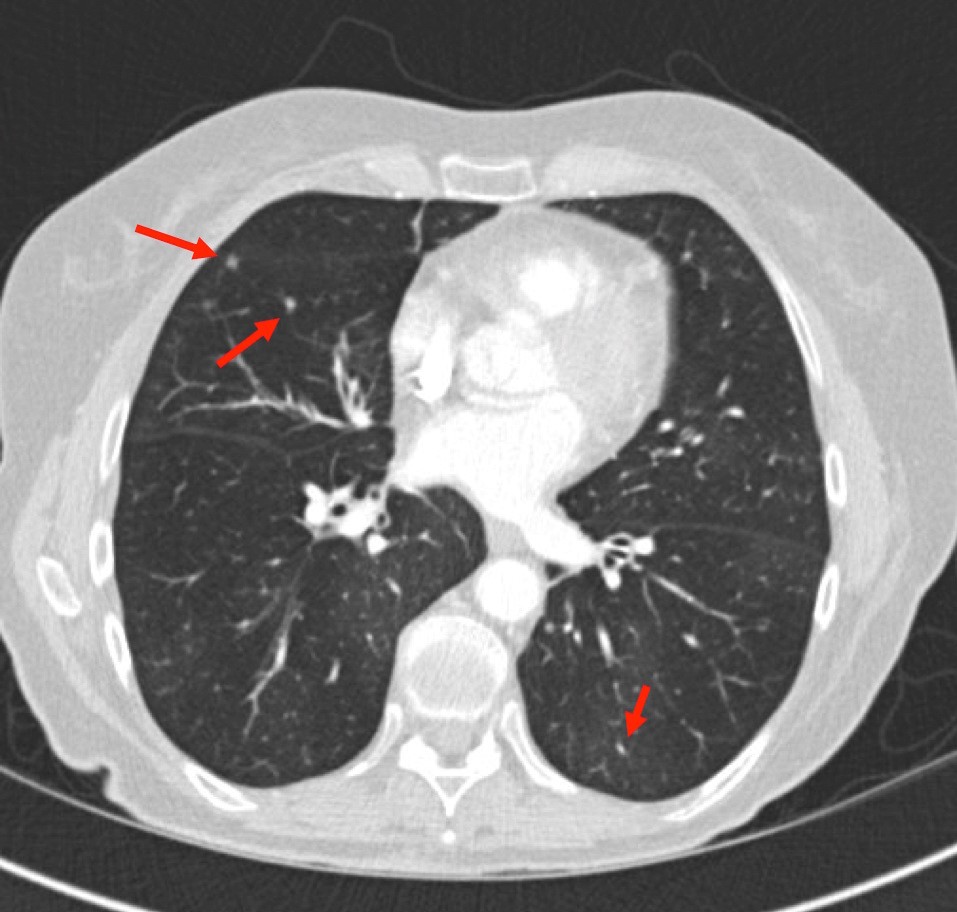
CT scan: nodules
Images hosted on other servers:

Peribronchiolar nodules

Multiple nodules

Nodules and air trapping (DIPNECH)
Prognostic factors
- Most tumorlets are benign incidental findings for which surgical resection is curative and prognosis is excellent (Chest 2007;131:1635)
- See DIPNECH for details on prognosis of tumorlets arising in this setting
Case reports
- 18 year old man with multiple sclerosing pneumocytomas and carcinoid tumorlets (J Endocr Soc 2019;3:937)
- 73 year old woman with pulmonary hypoplasia and carcinoid tumorlets (Respirol Case Rep 2018;6:e00373t)
- 73 year old woman with a lung fungus and a carcinoid tumorlet (Intern Med 2018;57:3485)
Treatment
- See DIPNECH for details on tumorlets arising in this setting
Gross description
- Difficult to identify but when visible, they are seen as small gray-white nodules < 5 mm in diameter, intimately associated with bronchioles
Frozen section description
Microscopic (histologic) description
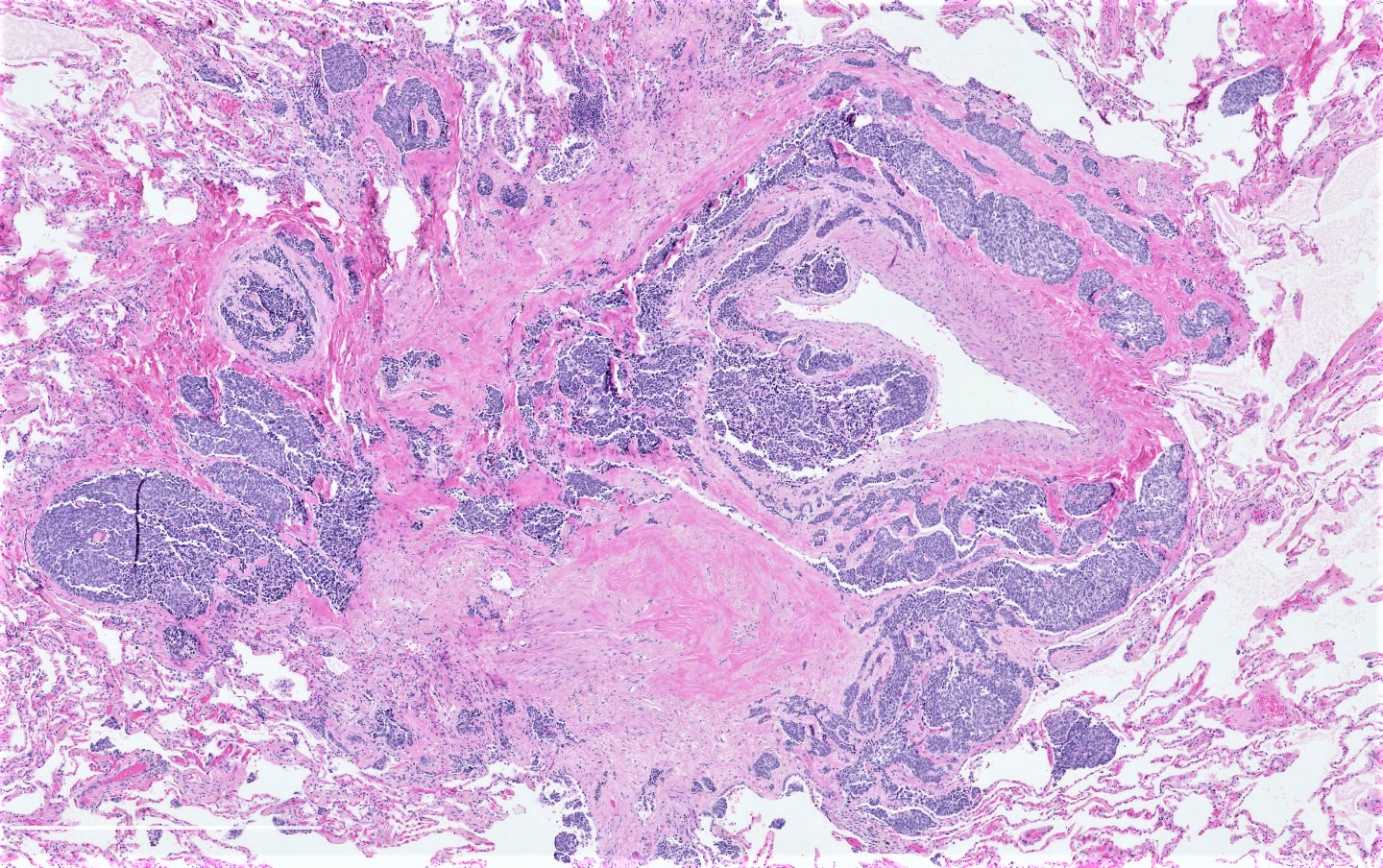
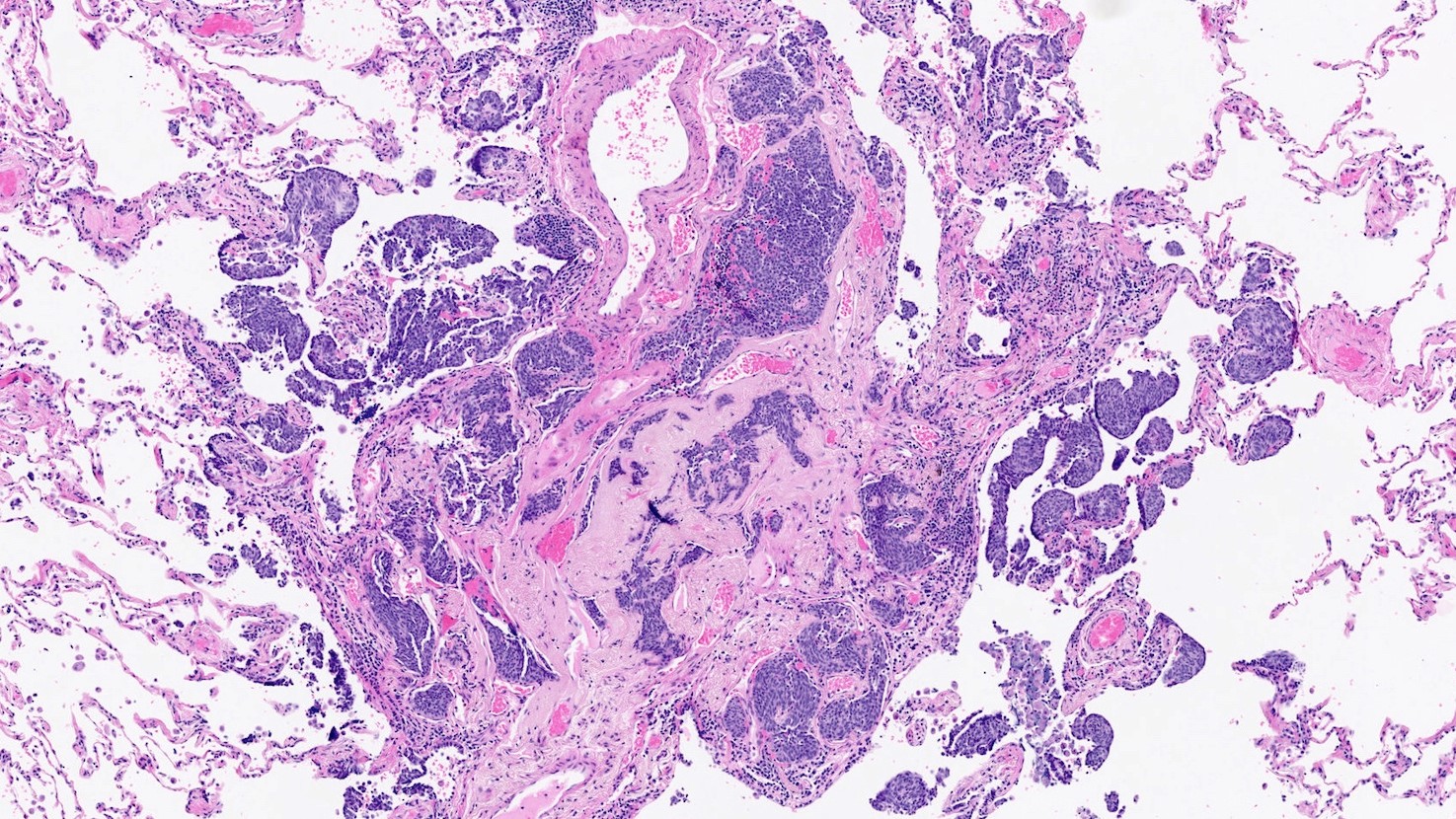
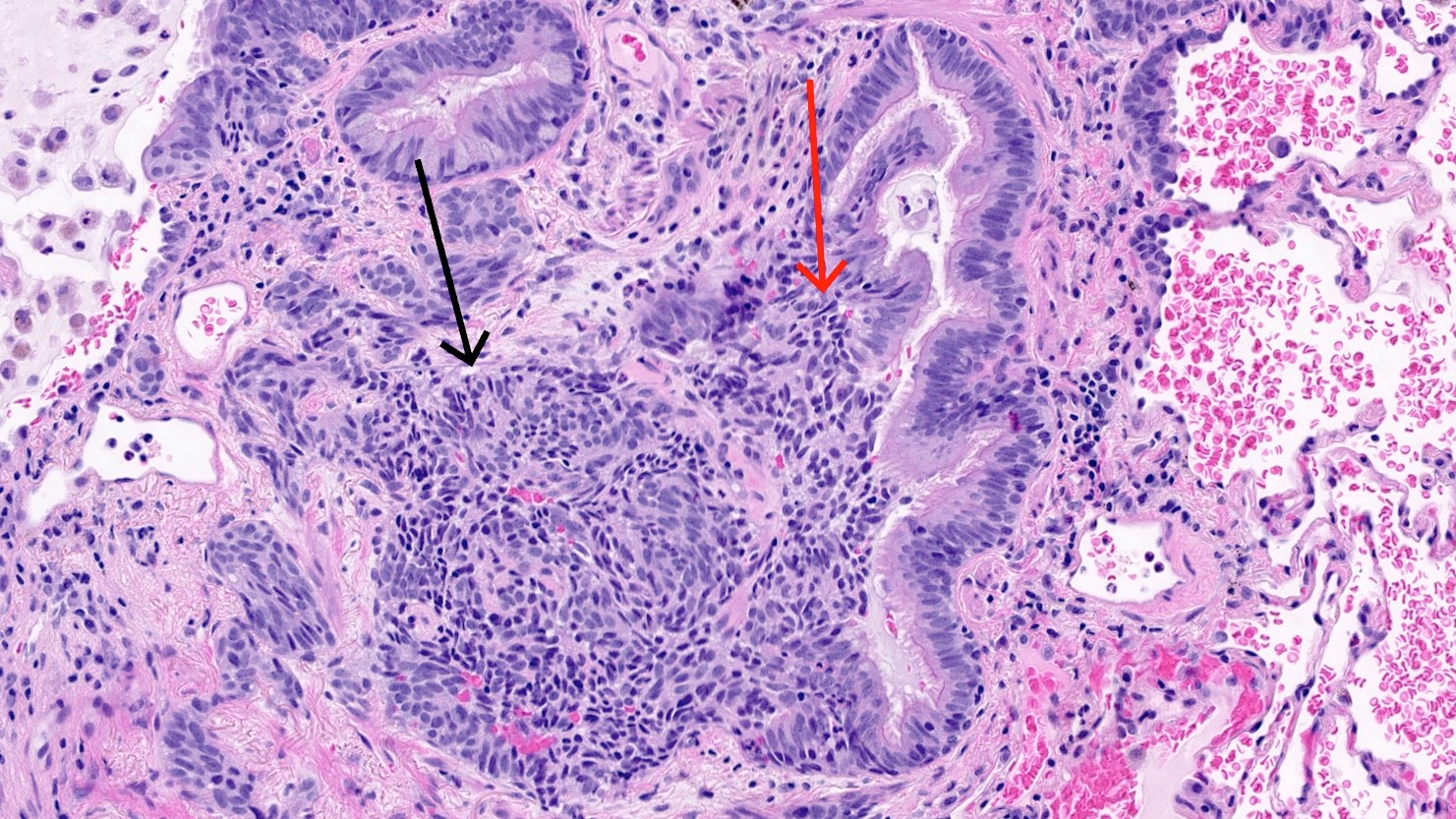
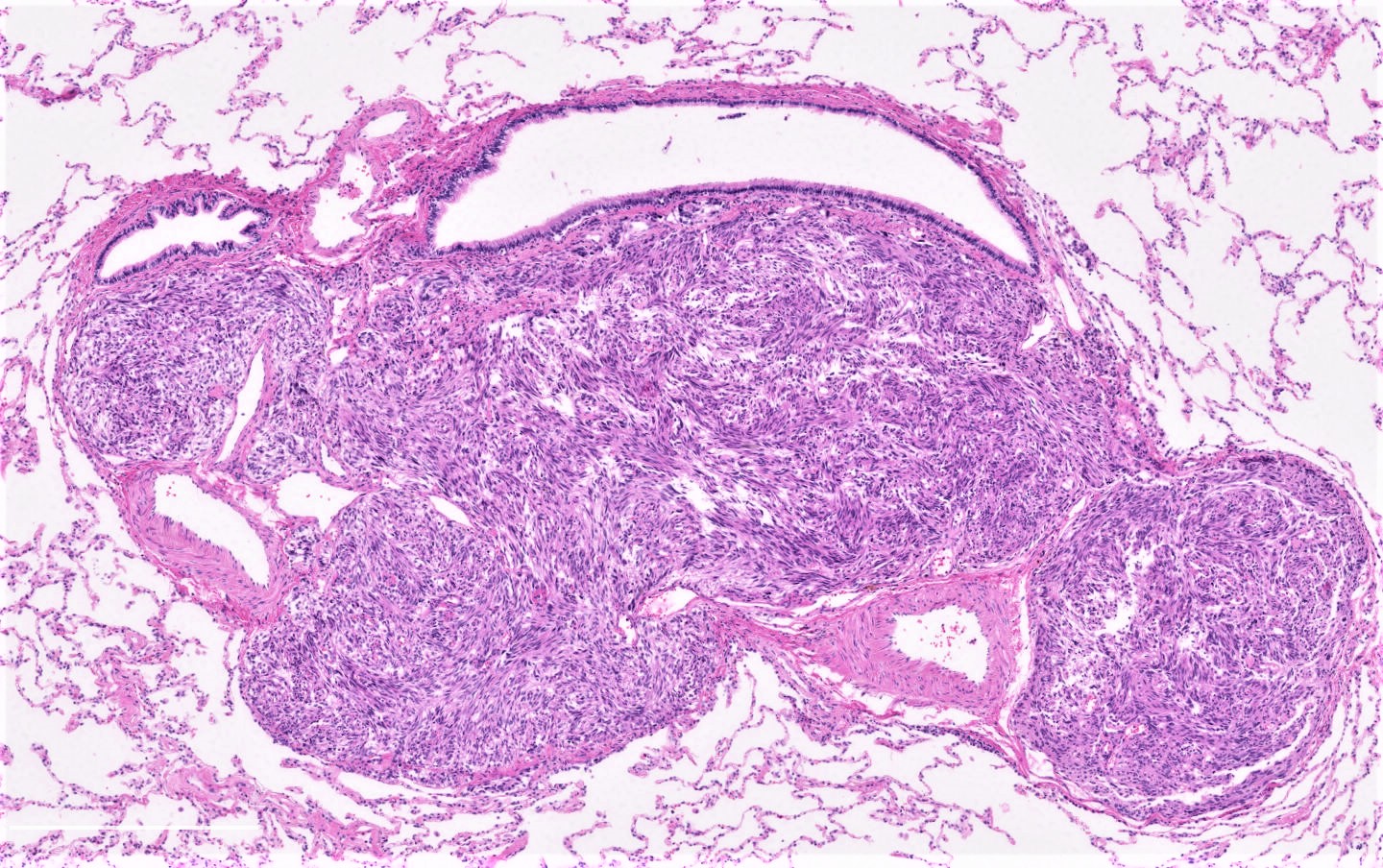
- Poorly defined nodule of neuroendocrine cells that cross the mucosal basal membrane in a fibrotic stroma:
- Size < 5 mm with < 2 mitoses/2 mm² and absence of necrosis
- Usually found in association with an airway
- Composed of neuroendocrine cells that are oval to round or spindle shaped; cells have round to oval nuclei with salt and pepper chromatin and a moderate amount of eosinophilic cytoplasm
- Complete features of DIPNECH or an underlying lung disease can be seen
Microscopic (histologic) images
Contributed by Andréanne Gagné, M.D., M.Sc. and Philippe Joubert, M.D., Ph.D.
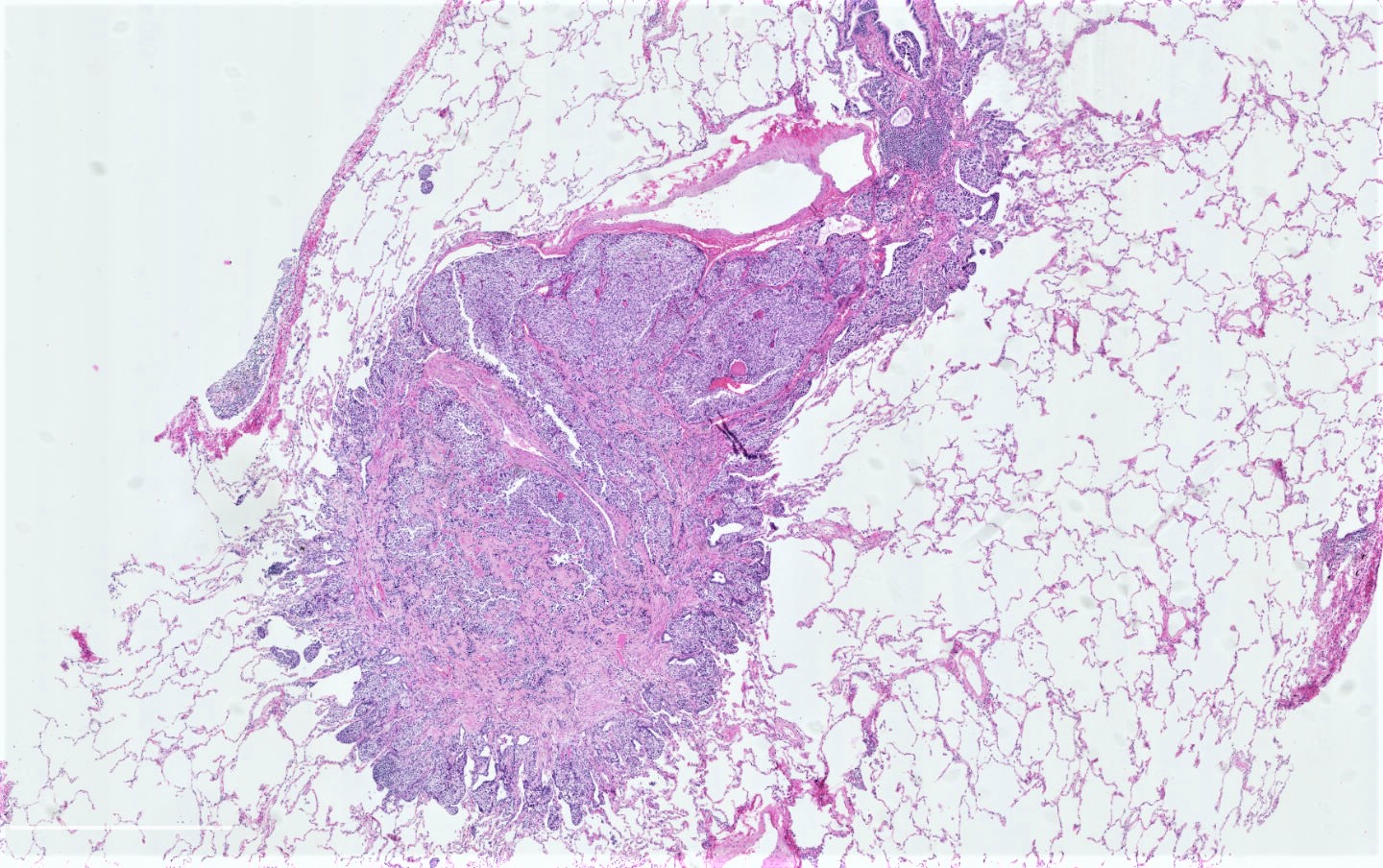
Peripheral nodule
Poorly delineated nodule
Tumorlet
Tumorlet arising in DIPNECH
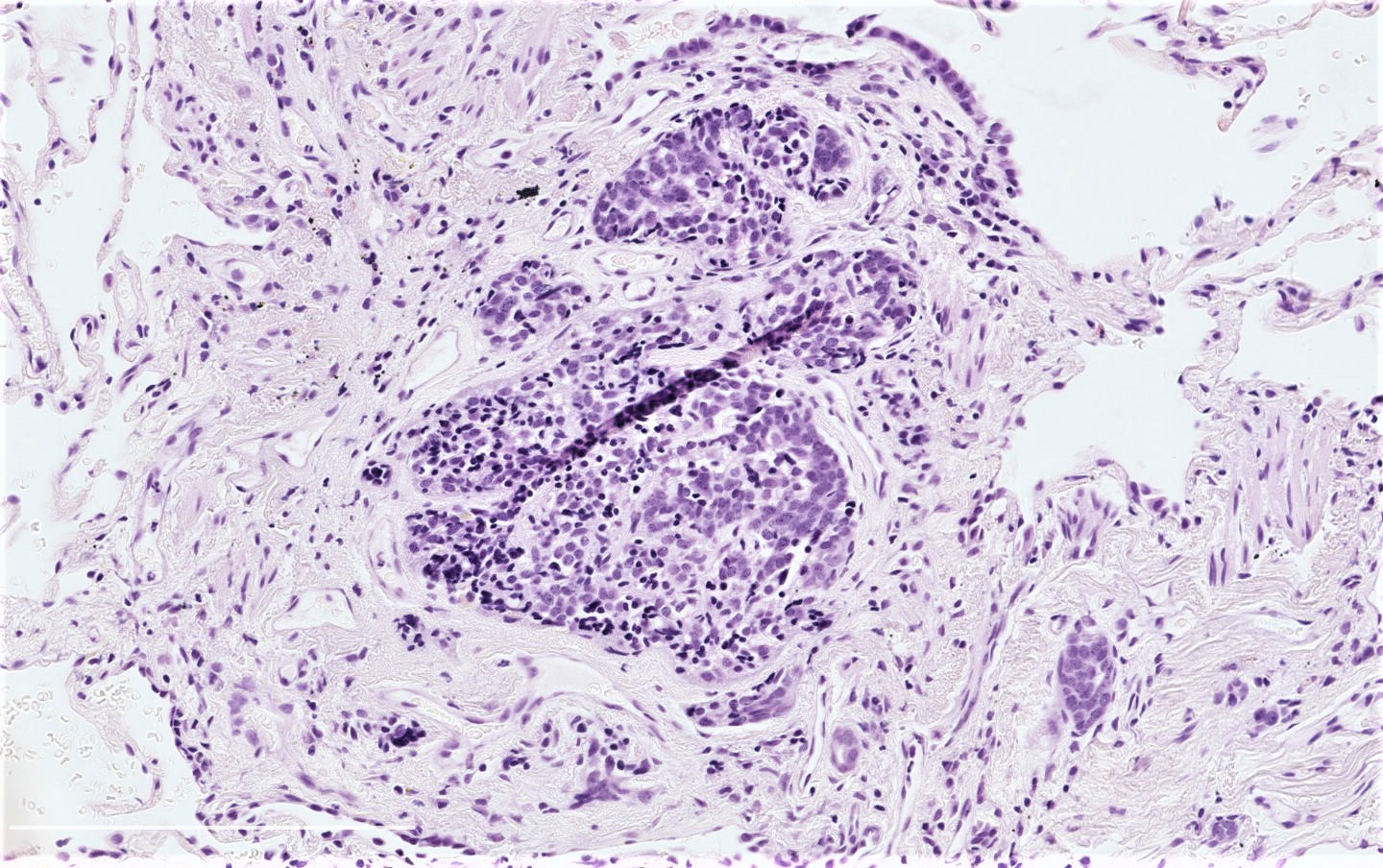
Small tumorlet

Clear cell features
Spindle cell features

Salt and pepper chromatin
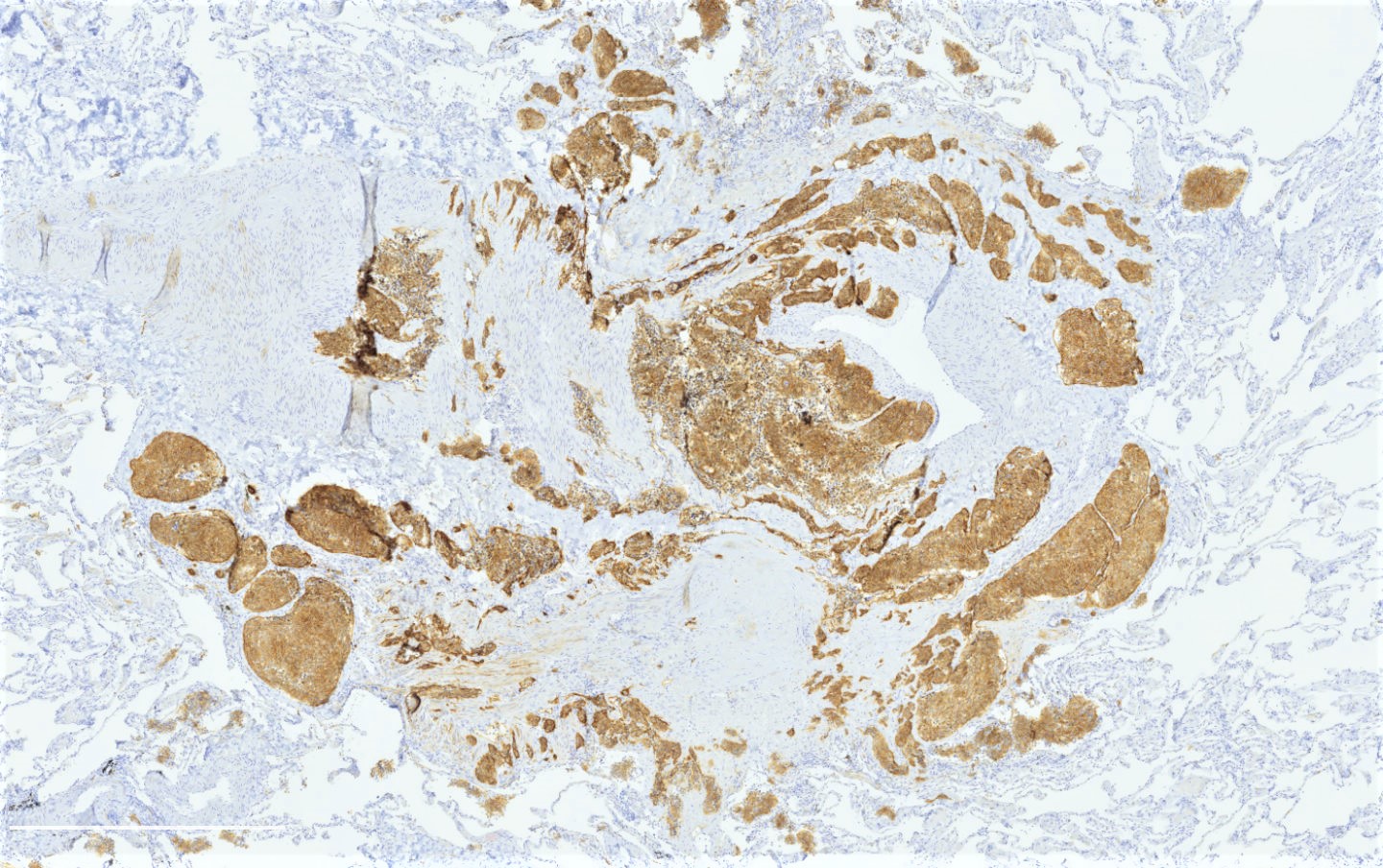
CD56
Cytology description
Positive stains
- Neuroendocrine markers: chromogranin A, synaptophysin, CD56, INSM1 (Chest 2007;131:1635, Histopathology 2018;72:1067)
- TTF1: 70% of cases (Chest 2007;131:1635)
Negative stains
Molecular / cytogenetics description
- To date, molecular alterations of tumorlets are poorly described
Sample pathology report
- See DIPNECH for an example of a report when tumorlets arise in this setting
Differential diagnosis
- Minute pulmonary meningothelial-like nodules:
- Randomly distributed nodules in the lung that are positive for EMA and CD56, negative for other neuroendocrine markers (chromogranin, synaptophysin and INSM1) and pankeratin (Histopathology 2018;72:1067, Am J Surg Pathol 2009;33:487)
- Typical carcinoid:
- Tumor size ≥ 5 mm with < 2 mitoses/2 mm² and absence of necrosis
- Atypical carcinoid:
- > 2 mitoses/2 mm² or presence of necrosis
Additional references
Board review style question #1
Regarding the lung nodule (tumor size < 5 mm without necrosis and mitoses) presented in the image, which of the following is true?
- EMA and CD56 stains are positive
- Many of them have EGFR mutations
- Their prognosis is poor
- They can be seen in the context of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH)
Board review style answer #1
D. They can be seen in the context of DIPNECH. A lung tumorlet is depicted in the image. While CD56 is positive in those tumors, EMA is negative and can help to differentiate with minute pulmonary meningothelial-like nodules (A). To date, molecular alterations of tumorlets are poorly described (B). Whether they occur in association with DIPNECH or with an underlying lung process, tumorlets have a good prognosis (C).
Comment Here
Reference: Carcinoid tumorlet
Comment Here
Reference: Carcinoid tumorlet
Board review style question #2
Which of the following is true about lung tumorlets?
- More than 2 mitoses/2 mm² can be seen
- Rare tumorlets of more than 1 cm have been reported
- They are confined to bronchial mucosa, without crossing the bronchial basal membrane
- They are frequently found in association with an airway
Board review style answer #2
D. They are frequently found in association with an airway. Tumorlets, by definition, have a size < 5 mm and < 2 mitoses/2 mm² with absence of necrosis (A and B). Statement C refers to diffuse idiopathic pulmonary neuroendocrine cell hyperplasia.
Comment Here
Reference: Carcinoid tumorlet
Comment Here
Reference: Carcinoid tumorlet

