Lung
Neuroendocrine tumors
Small cell carcinoma
Editorial Board Members: Debra L. Zynger, M.D., Jefree J. Schulte, M.D.


Last author update: 20 September 2022
Last staff update: 6 February 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Small cell neuroendocrine carcinoma lung

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Electron microscopy description | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Mullins CI, Glass C. Small cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorsmallcell.html. Accessed March 31st, 2025.
Definition / general
- High grade neuroendocrine tumor that arises in the hilum of smokers, with a poor prognosis and no current targeted therapy
Essential features
- High grade, usually advanced at diagnosis
- Almost exclusively associated with smoking / tobacco exposure
- Positive for at least one neuroendocrine marker
ICD coding
- ICD-10: C34.90 - malignant neoplasm of unspecified part of unspecified bronchus or lung
Epidemiology
- 10 - 15% of lung cancer cases (J Clin Oncol 2006;24:4539, Cell Biol Int 2020;44:1564)
- M = F
- 70% have metastasis at time of diagnosis (Cancer Treat Res 2016;170:301)
Sites
- Lung: central / bronchial / hilar; rarely a peripheral nodule
- Submucosal growth
- Metastasis to liver, adrenals, bone, bone marrow, brain; often widespread
Pathophysiology
- Arises from neuroendocrine cells of basal bronchial epithelium
Etiology
- Smoking (rare in nonsmokers)
Clinical features
- Cough, dyspnea, weight loss
- Paraneoplastic syndromes (World J Clin Oncol 2014;5:197)
- Adrenocorticotropic hormone (ACTH) production → Cushing syndrome
- Antidiuretic hormone (ADH) → syndrome of inappropriate antidiuretic hormone secretion (SIADH) → hyponatremia
- Lambert-Eaton
- Limbic encephalitis
- Superior vena cava syndrome
- Staging (Cancer Treat Res 2016;170:301)
- Limited: ipsilateral hemithorax and regional lymph nodes
- Extensive: contralateral thorax and lymph nodes, metastasis or malignant effusions
- TNM staging less useful
Diagnosis
- Biopsy: based on hematoxylin and eosin morphology
Laboratory
- No diagnostic labs but can have associated abnormalities (see Clinical features and Prognostic factors)
Radiology description
- More useful as staging tool; often not visible on chest Xray due to central location (Cancer Treat Res 2016;170:301)
- Imaging for staging includes chest CT, brain MRI or CT, bone scans (technetium or PET) (Radiographics 2006;26:41)
Radiology images
Images hosted on other servers:

Right hilar mass

Left hilar mass
Prognostic factors
- Adverse (Cancer Treat Res 2016;170:301)
- Continued smoking → chemotherapy resistance
- Labs: elevated lactate dehydrogenase (LDH), alkaline phosphatase, albumin
- Metastasis to the liver, bone marrow and brain
- Presence of paraneoplastic syndromes
- Favorable (Lung Cancer 2019;130:216)
- Women
Case reports
- 53 year old man, a smoker, presenting acutely with malignant tension hydrothorax (Respirol Case Rep 2019;7:e00420)
- 62 year old man with pituitary gland metastasis (Am J Case Rep 2019;20:207)
- 64 year old man with inappropriate antidiuretic hormone paraneoplastic syndrome (BMC Pulm Med 2018;18:169)
- 76 year old man with 2 morphologically distinct patterns of small cell lung carcinoma (Pathol Int 2018;68:618)
- Septuagenarian man with back spasms presenting with tumor lysis syndrome (BMJ Case Rep 2018;2018:bcr2018224512)
Treatment
- Combined chemotherapy (platinum based) and radiation (Cancer Treat Res 2016;170:301, Lung Cancer 2019;130:216, Cell Biol Int 2020;44:1564, Cancer Cell 2021;39:297)
- No targeted immunotherapy available
- Median survival time
- 15 - 20 months (limited disease)
- 8 - 13 months (extensive disease)
- 5 year survival rate: 10 - 13 % (limited), 1 - 2% (extensive)
Gross description
- Central or hilar mass
- White-tan, soft, friable, necrotic (Am J Surg Pathol 2002;26:1184)
- Peripheral nodules: circumscribed, with fleshy cut surface
Gross images
Contributed by Carolyn Glass, M.D.

Central tumor with bronchial spread
Images hosted on other servers:

Hilar mass

Central tumor

Spreading along bronchi
Frozen section description
- Rarely seen at frozen section due to being diagnosed on cytology and usually treated nonoperatively
Microscopic (histologic) description
- Round / oval blue cells with minimal cytoplasm; usually small to medium sized
- Nuclear features: finely dispersed chromatin, no distinct nucleoli, molding, smudging, high mitotic rate
- Stroma: thin, delicate, scant, fibrovascular
- Necrosis and apoptosis of individual cells common
- Patterns: sheets, clusters, ribbons, rosettes, peripheral palisading
- Other / rarer features (Surg Oncol Clin N Am 2016;25:447)
- Azzopardi phenomena: basophilic nuclear material lining blood vessel walls
- Metastatic cells usually have more cytoplasm
- Scattered giant cells
Microscopic (histologic) images
Contributed by Carolyn Glass, M.D.
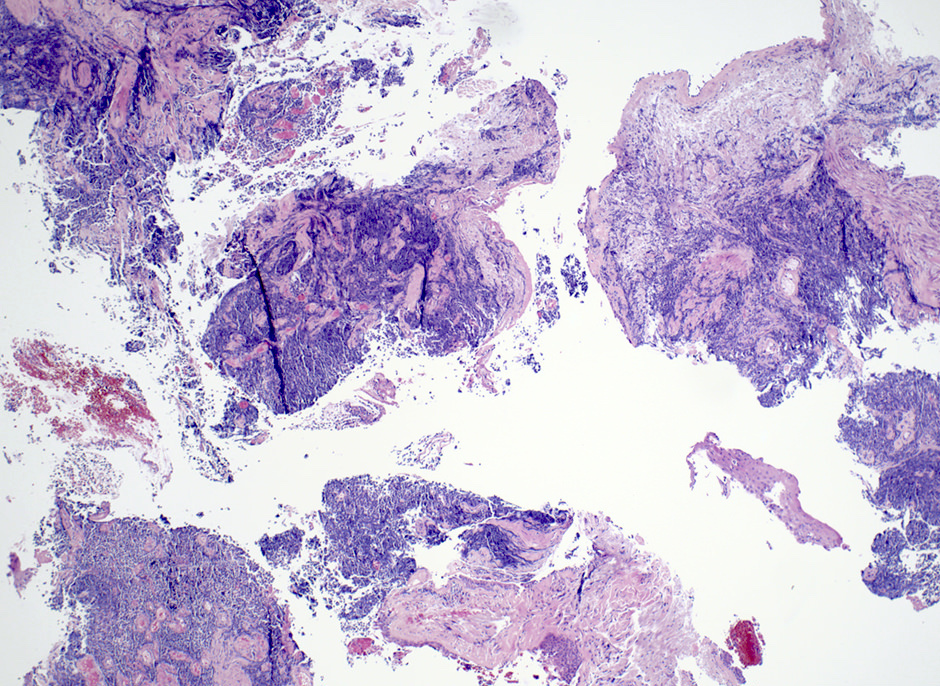
Sheets of tumor cells
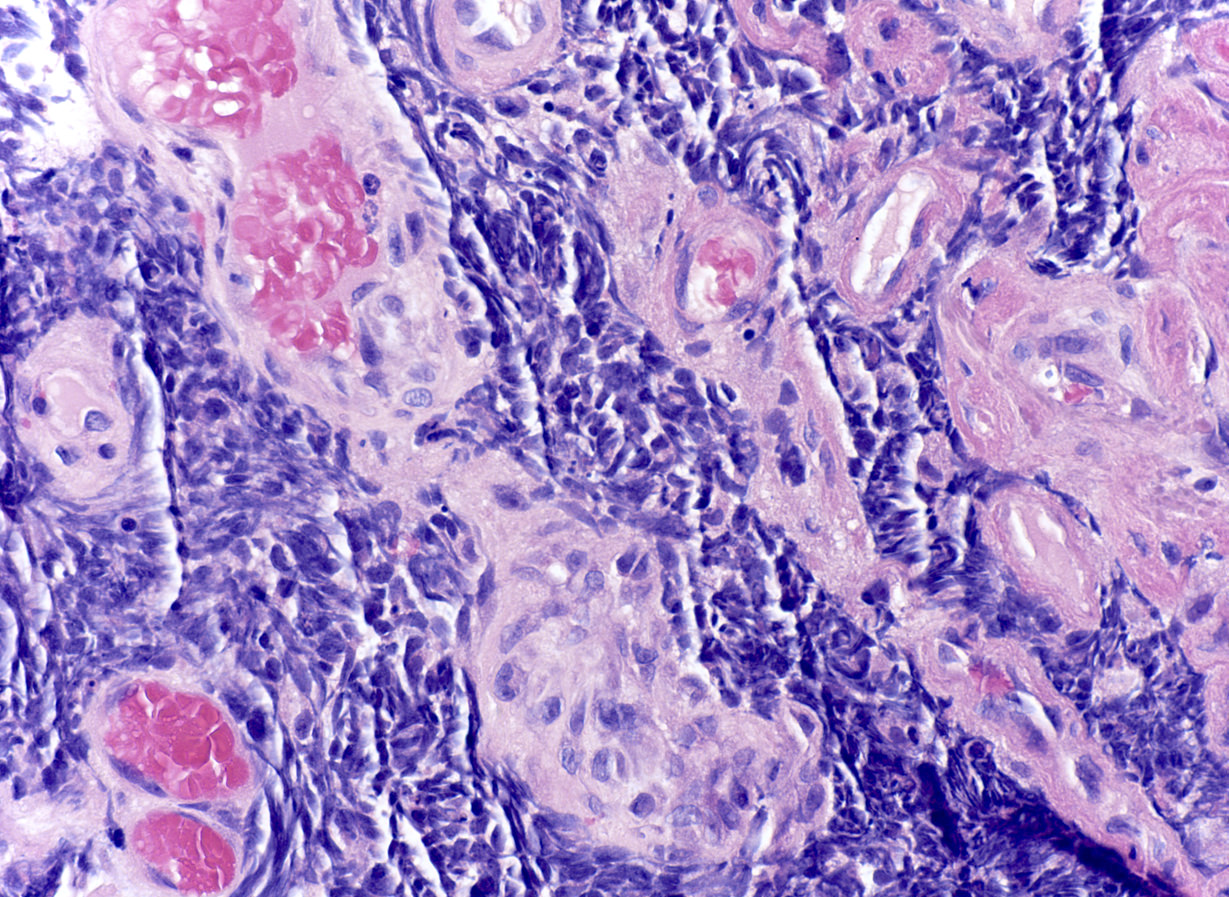
Crushed blue cells
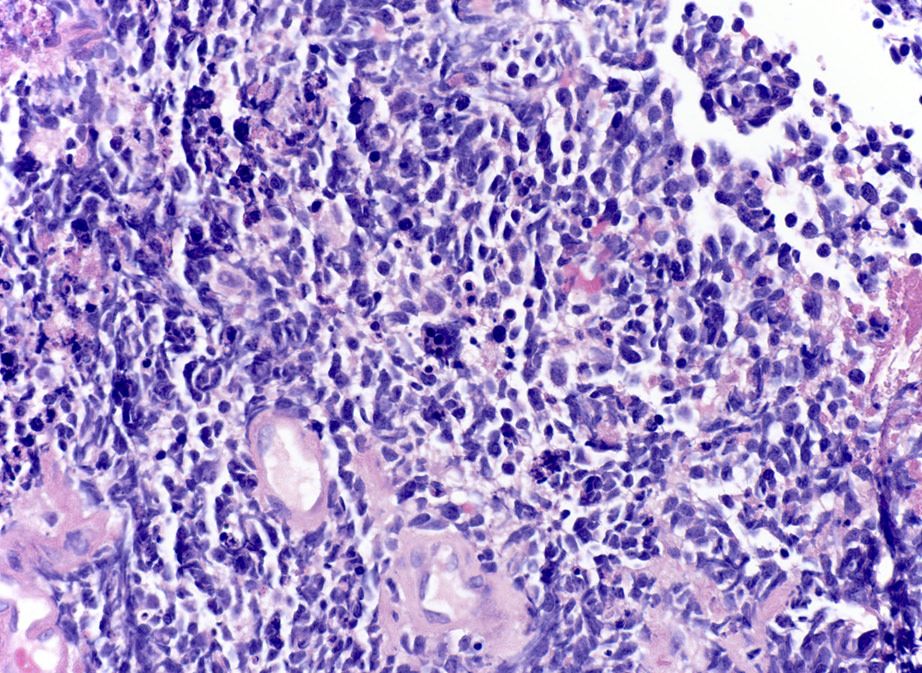
Cellular morphology
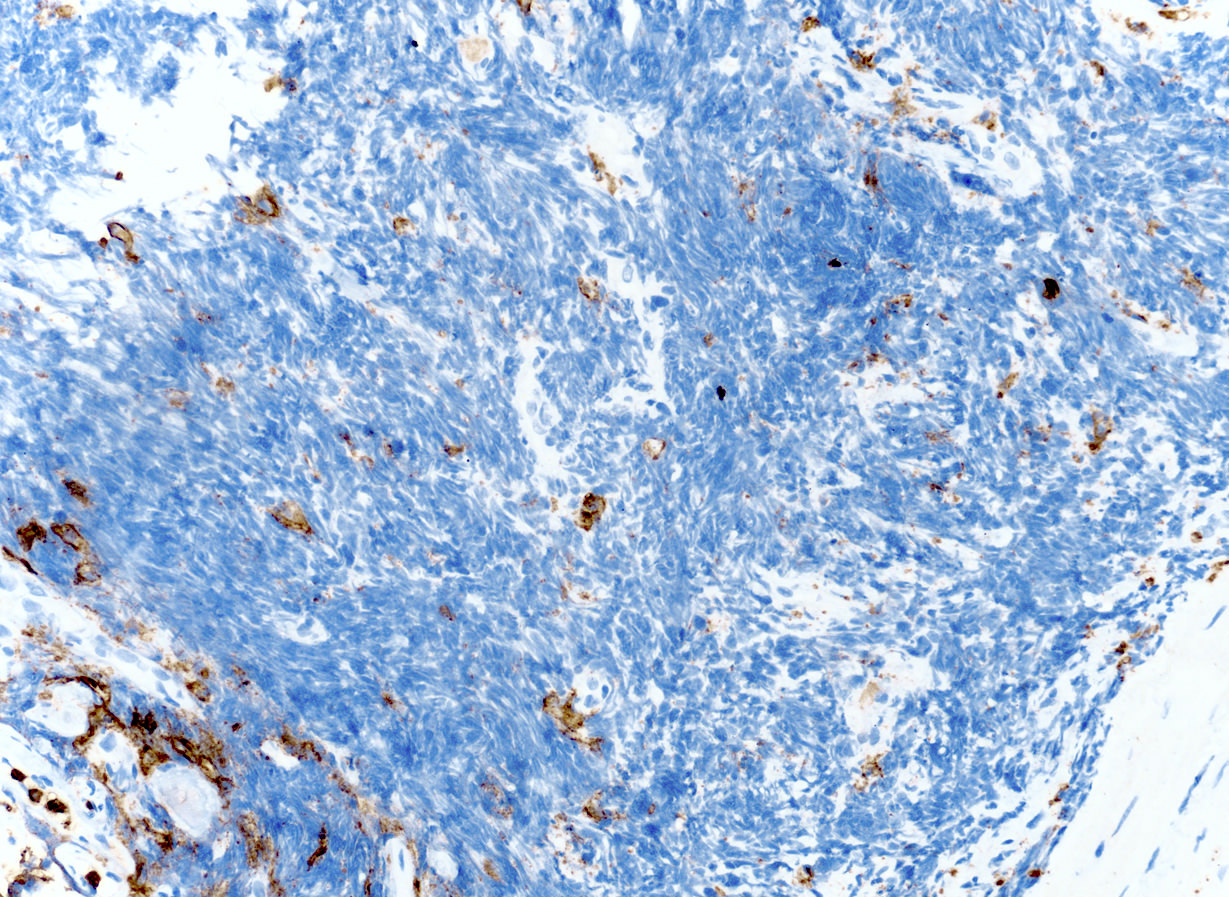
CK7

TTF1
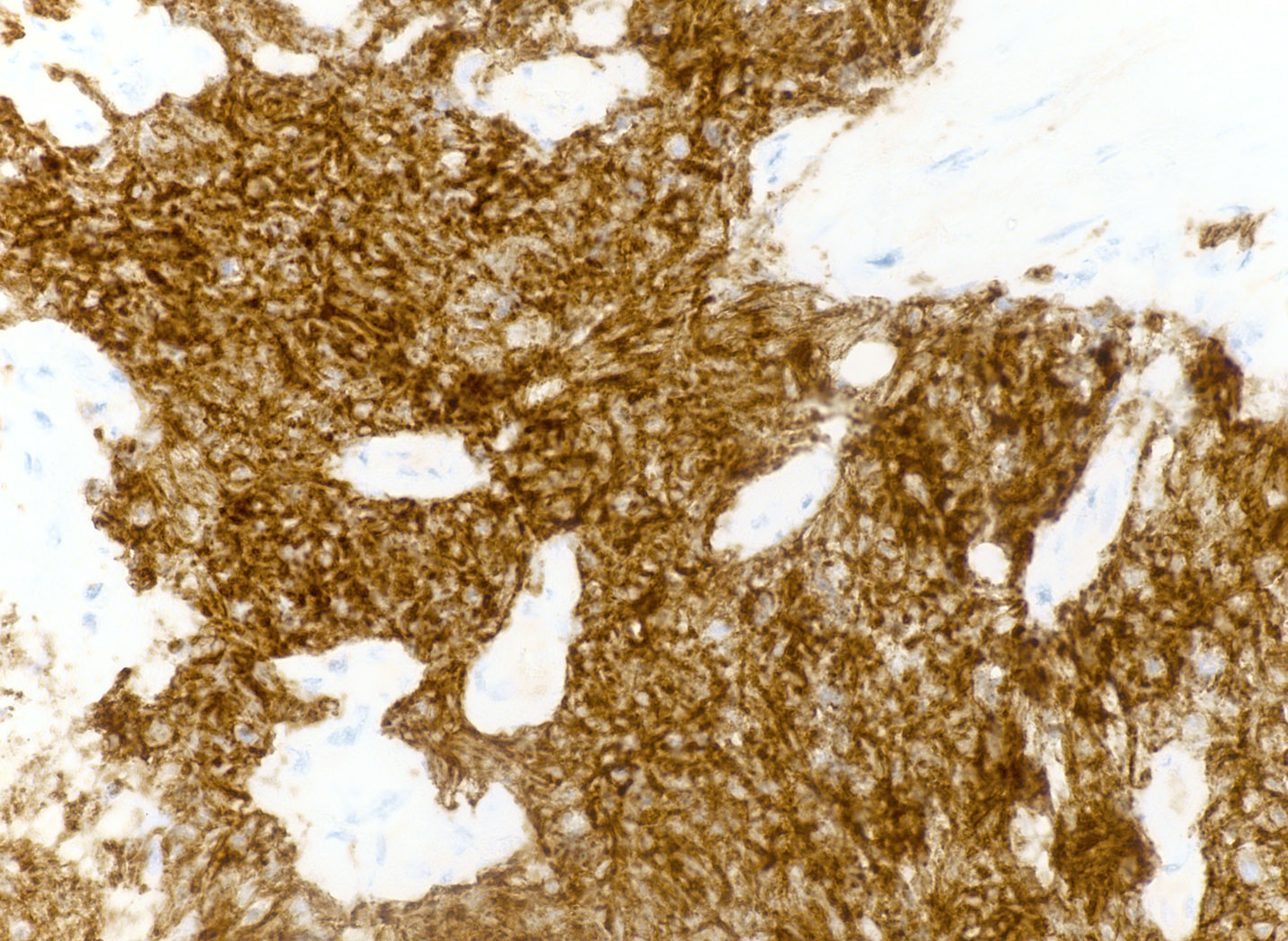
CD56
Virtual slides
Images hosted on other servers:

Small cell lung carcinoma
Cytology description
- Nuclei: oval / elongated, hyperchromatic, absent nucleoli, granular cytoplasm, smooth membrane
- Scant cytoplasm
- Pattern: molding, individual cells or loose clusters, crush artifact
- Necrosis and apoptosis of individual cells and tumor background
- Hypercellular (Int J Clin Exp Pathol 2010;3:367)
Positive stains
- Synaptophysin, chromogranin A, INSM1 (90 - 100% specificity, low sensitivity), CD56
- TTF1 (negative in 15 - 20%)
- CK7 (punctate, not strong / diffuse)
- p16, SOX2, CD117, PAX5, p53, calretinin (48%), CK8
- Ki67: will show a high proliferation index useful for differentiating between low and high grade neuroendocrine carcinomas
Electron microscopy description
- Neurosecretory granules - dense in central cytoplasm with peripheral halo (Oncotarget 2017;8:73745)
Electron microscopy description
Images hosted on other servers:

Dense core granules
Molecular / cytogenetics description
- Deletion of 3p → loss of MLH1, VHL (Nat Commun 2018;9:3114, Genes Chromosomes Cancer 1991;3:283, Biochim Biophys Acta 2012;1826:255, Semin Oncol 2001;28:3)
- p53 mutations due to deletion at 17p (90%) (Nat Commun 2018;9:3114, Biochim Biophys Acta 2012;1826:255, Semin Oncol 2001;28:3)
- RB1 loss of function at 13q14 (80 - 100%) (Nat Commun 2018;9:3114, Biochim Biophys Acta 2012;1826:255, Semin Oncol 2001;28:3)
- PTEN mutation (15 - 20%) (Nat Commun 2018;9:3114)
- Wild type c-KIT upregulation (80 - 90%) (Nat Commun 2018;9:3114)
- MYC (MYC, MYCL1 or MYCN) amplification (20%) (Nat Commun 2018;9:3114, Semin Oncol 2001;28:3)
- Telomerase activation (90%) (Nat Commun 2018;9:3114, Semin Oncol 2001;28:3)
- Rare EGFR mutations and ALK rearrangements (Nat Commun 2018;9:3114)
Sample pathology report
- Lung, left upper lobe, endobronchial biopsy:
- Small cell carcinoma (see comment)
- Comment: Positive immunoreactivity for keratin, CD56 and TTF1 with negative staining for CD45 supports the diagnosis of small cell carcinoma.
Differential diagnosis
- Basaloid variant of squamous cell carcinoma:
- Positive for p40 and high molecular weight keratins, negative neuroendocrine markers (CD56, synaptophysin, chromogranin)
- Lung adenocarcinoma, poorly differentiated:
- Negative for neuroendocrine markers, diffuse / strong CK7
- Atypical carcinoid tumor:
- More prominent nucleoli, organoid growth pattern
- Large cell neuroendocrine carcinoma:
- Larger cells with more cytoplasm and prominent nucleoli
- Usually peripherally located
Board review style question #1
A 65 year old man presents to the clinic with generalized fatigue for 6 months. He says he has been feeling very down lately and that his mood has had a negative impact on his relationship with his wife of 30 years. He also reports recent acne flares, which he says he has not struggled with since college. He is a 25 pack per year smoker and has hypertension, previously well controlled on his current regimen. Vitals taken today show a BP of 155/95. Physical exam reveals an adipose deposit on the dorsal upper thorax and abdominal striae. A chest Xray reveals a hilar lung mass. Which of the following tumors most commonly produces the paraneoplastic syndrome seen in this patient?
- Adenocarcinoma of the lung
- Large cell carcinoma of the lung
- Small cell lung cancer
- Squamous cell lung cancer
Board review style answer #1
C. Small cell lung cancer is associated with paraneoplastic syndromes and one of the most common is Cushing syndrome, as in this patient. This is caused by increased production of adrenocorticotropic hormone by the small cell tumor. Symptoms include weight gain, fatigue, glucose intolerance, moon face, buffalo hump, muscular weakness, skin manifestations (thinning, acne, abdominal striae), psychological symptoms (depression, anxiety, decreased libido), hypertension, increased risk of bone fracture and reproductive symptoms (irregular or absent menstruation in females and erectile dysfunction in males). Other paraneoplastic syndromes associated with small cell lung carcinoma include syndrome of inappropriate antidiuretic hormone secretion and Lambert-Eaton.
Comment Here
Reference: Small cell carcinoma
Comment Here
Reference: Small cell carcinoma
Board review style question #2
A 59 year old female smoker with no significant past medical history comes to the clinic complaining of dyspnea. She states that a month ago, she began experiencing shortness of breath during her morning 2 mile walk, which she had previously enjoyed without difficulty. Over the last week, she has started becoming short of breath throughout the day and complains of headaches that are not relieved with ibuprofen. When asked about her diet, she says she has decreased her salt intake, as she thinks her face has become swollen. On physical exam, you note edema of the right arm and distention of right sided neck veins. Xray of the chest shows a right sided lung mass at the hilum. Fine needle aspiration of this mass would most likely reveal which of the following?
- Granulomas with central necrosis and giant cells
- Islands of large eosinophilic cells containing keratin
- Nests of cells with large irregular shaped nuclei that are forming glands
- Sheets of small round blue cells with finely dispersed chromatin
Board review style answer #2
D. Sheets of small round blue cells with finely dispersed chromatin. Small cell lung cancer is histologically described as small round / oval cells with high nuclear to cytoplasmic ratio. The nuclei have finely dispersed or salt and pepper chromatin and absent nucleoli. Small cell lung cancer is most often located at the hilum and grows along the bronchi. Growth of the tumor can cause compression of the superior vena cava leading to superior vena cava syndrome, characterized by swelling of the face and upper limbs, cough and distention of the neck veins, as venous blood flow is obstructed.
Comment Here
Reference: Small cell carcinoma
Comment Here
Reference: Small cell carcinoma
Board review style question #3
A patient undergoes a biopsy of a lung mass with the histology shown in the image. Which of the following immunohistochemical results would be most typical of the lesion?
- INSM1+, chromogranin+, CK7+ diffuse, p40+, Ki67 low
- INSM1+, chromogranin-, CK7+ diffuse, p40+, Ki67 high
- INSM1-, chromogranin+, CK7- punctate, p40+, Ki67 high
- INSM1+, chromogranin+, CK7- punctate, p40-, Ki67 high
- INSM1-, chromogranin-, CK7- punctate, p40-, Ki67 low
Board review style answer #3
D. INSM1+, chromogranin+, CK7- punctate, p40-, Ki67 high. The tumor shown is small cell carcinoma of the lung. Of the choices listed, INSM1+, chromogranin+, CK7- punctate, p40-, Ki67 high (answer D) is the most likely immunoprofile.
Comment Here
Reference: Small cell carcinoma
Comment Here
Reference: Small cell carcinoma
