
Lung
Adenocarcinoma
Colloid
Editorial Board Member: Matthew J. Cecchini, M.D., Ph.D.


Last author update: 31 August 2023
Last staff update: 31 August 2023
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Colloid adenocarcinoma lung

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Olteanu GE, Mataić A, Brčić L Colloid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorcolloidadeno.html. Accessed January 15th, 2025.
Definition / general
- Colloid adenocarcinoma is a type of invasive lung cancer characterized by extracellular mucin accumulation that distends alveolar spaces and destroys lung tissue
- It is important to differentiate colloid adenocarcinoma from metastases of mucinous carcinoma originating in other organs and from invasive mucinous adenocarcinoma of the lung by identifying key characteristics, such as large pools of mucin destroying alveolar walls, which must be present in at least 50% of the tumor
Essential features
- Invasive adenocarcinoma with extensive extracellular mucin pools distending alveolar spaces and destroying alveolar walls
- Tumor cells are mucin filled, cuboidal to columnar, floating in mucin pools or lining fibrous walls of mucin filled spaces
- Predominantly found in the peripheral lung parenchyma
- Immunohistochemistry: positive for CK7 and CDX2 and CK20; weak or negative for TTF1, napsin A and EMA (MUC1)
- Mostly indolent clinical course with a relatively favorable prognosis after complete surgical resection
Terminology
- Recommended: colloid adenocarcinoma
- Not recommended: mucinous cystadenocarcinoma; mucinous cystic tumor of borderline malignancy
ICD coding
- ICD-O: 8480/3 - colloid adenocarcinoma
- ICD-11: 2C25.Z & XH7GY6 - malignant neoplasms of bronchus or lung, unspecified & adenocarcinoma of lung, mucinous
Epidemiology
- Epidemiology of colloid adenocarcinoma is like that of other lung adenocarcinomas (J Surg Oncol 2016;114:211)
Sites
- Colloid adenocarcinoma typically occurs in the peripheral lung parenchyma (Intern Med 2018;57:3637, J Surg Oncol 2016;114:211)
Pathophysiology
- Pathogenesis of mucinous lung tumors, which may share similarities with mucinous / colloid gastrointestinal adenocarcinomas, could be attributed to gastrointestinal differentiation, as both types of tumors exhibit predominant extracellular accumulation of mucin
- Colloid adenocarcinomas are generally negative for predictive biomarkers such as EGFR mutations and ALK rearrangements, while KRAS mutations are found in ~50% of these tumors
- References: Virchows Arch 2015;467:675, Hum Pathol 2015;46:836
Etiology
- Etiology of colloid adenocarcinoma is like that of other lung adenocarcinomas (J Surg Oncol 2016;114:211)
Clinical features
- In most cases, it is asymptomatic (J Surg Oncol 2016;114:211)
- Incidental findings during routine radiographic evaluation or with no specific symptoms (i.e., cough, shortness of breath and unresolved pneumonia) (Hum Pathol 2015;46:836)
Diagnosis
- Usually diagnosed in light of incidental findings on CT scans (Hum Pathol 2015;46:836)
- Pathological diagnosis following lobectomy or wedge resection (J Surg Oncol 2016;114:211)
Radiology description
- On CT, colloid adenocarcinoma usually presents as an intrapulmonary mass with poor contrast enhancement (Intern Med 2018;57:3637)
- On MRI on T1 weighted imaging (WI), colloid adenocarcinoma is characterized by low intensity and high intensity on T2WI, probably from the mucus component of the tumor (Intern Med 2018;57:3637)
- On 18F fluorodeoxyglucose positron emission tomography (18F FDG PET), the majority of tumors show intense accumulation of 18F FDG (median standardized uptake value of 6.25, ranging from 3.0 to 8.6) (J Surg Oncol 2016;114:211)
Radiology images
Images hosted on other servers:

Radiological evaluation

Radiology and bronchoscopy
Prognostic factors
- Estimated 5 year survival of 51% in patients who benefit from surgical resection (J Thorac Oncol 2011;6:1496)
- Apparent better prognosis for tumors that are CDX2 and MUC2 positive compared with tumors that are CDX2 and MUC2 negative (Am J Surg Pathol 2004;28:442)
- Clinical progression is generally slow; after comprehensive surgical removal, the prognosis is relatively favorable (Am J Surg Pathol 2004;28:442)
- Poorer prognosis, involving recurrence and metastasis, is indicated by the existence of signet ring cells and a noncolloid component (Am J Surg Pathol 2004;28:442)
Case reports
- 66 year old woman with a history of ovarian cancer (Respirol Case Rep 2023;11:e01109)
- 69 year old woman with a giant lung mass detected on chest radiograph (Case Rep Oncol 2020;13:1097)
- 76 year old asymptomatic man with a mass in the right lower lung (Intern Med 2018;57:3637)
Treatment
- Complete surgical resection is the treatment of choice (Respirol Case Rep 2023;11:e01109)
- KRAS mutations are the most common
- Targetable alterations in EGFR and ALK are typically absent in colloid adenocarcinoma (i.e., EGFR mutations and ALK rearrangements) (Hum Pathol 2015;46:836)
Clinical images
Images hosted on other servers:

Intraoperative view
of white mass
with indistinct
margins

Intraoperative
view of giant
cystic colloid
adenocarcinoma
Gross description
- Tumors appear as diverse, nonencapsulated, single, soft, jelly-like nodules with a mucoid appearance and protruding when cut; their sizes range from 5 to 100 mm (Mod Pathol 1992;5:634)
- In rare instances, these tumors may display a notably cystic appearance (Hum Pathol 2015;46:836)
Gross images
Contributed by Matthew J. Cecchini, M.D., Ph.D.
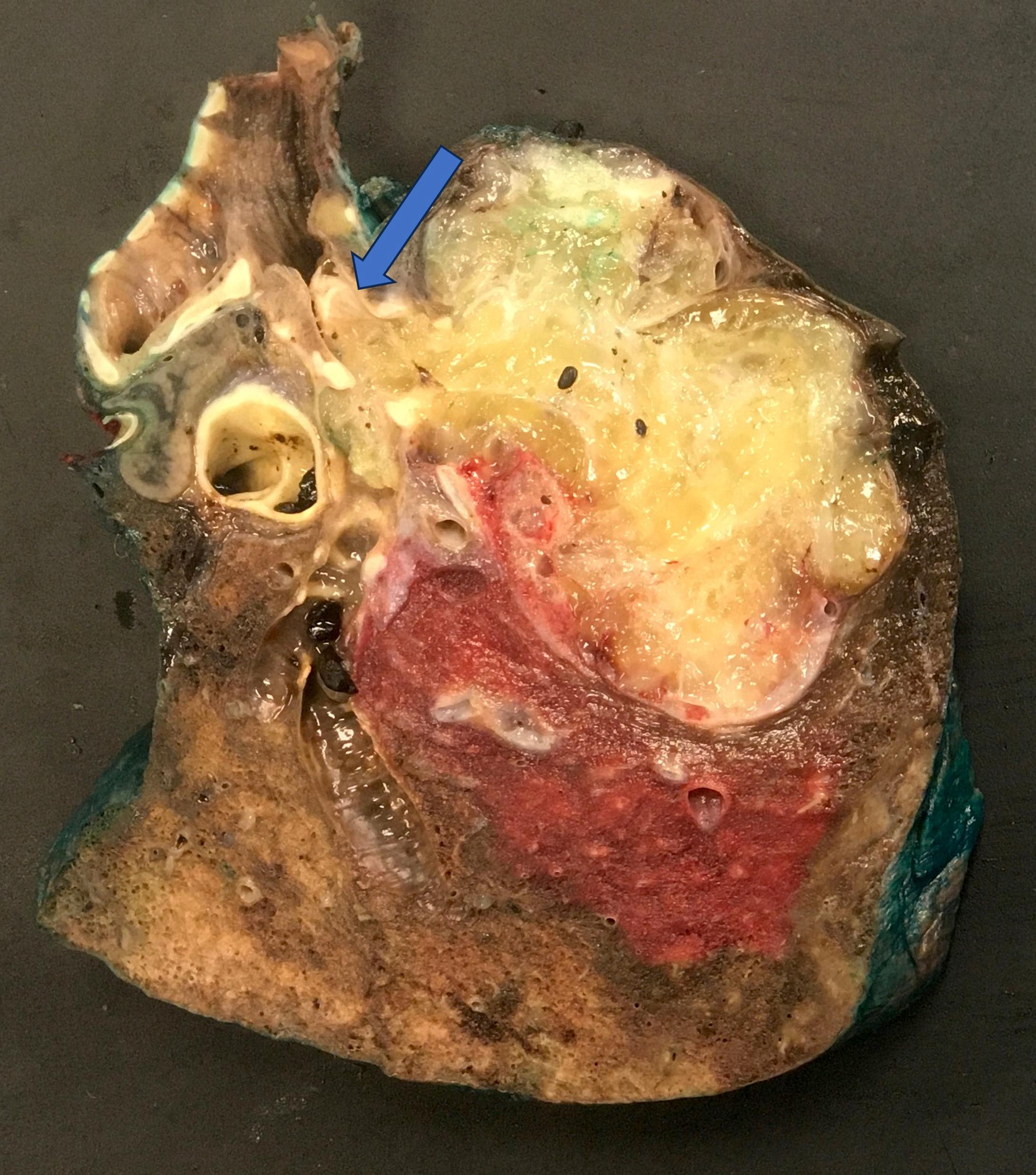
Gross cut surface
Images hosted on other servers:

Gross cut surface

Cystic lesion with mucin pooling
Microscopic (histologic) description
- Abundant extracellular mucin
- Distended and destroyed alveolar spaces
- Invasive growth pattern
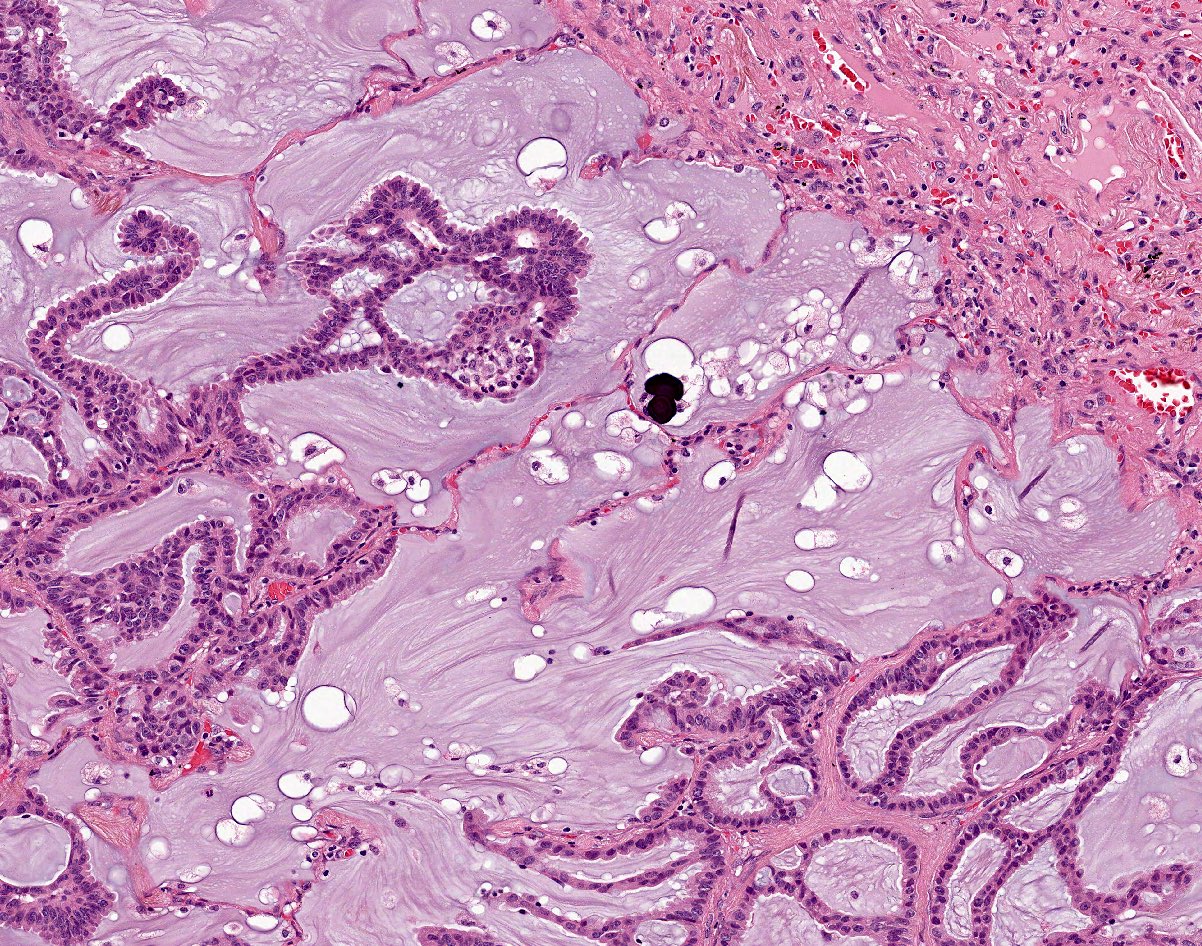
- Mucin laden cuboidal / columnar cells
- Possible signet ring morphology
- Inconspicuous, well differentiated cells
- Low mitotic count, no necrosis
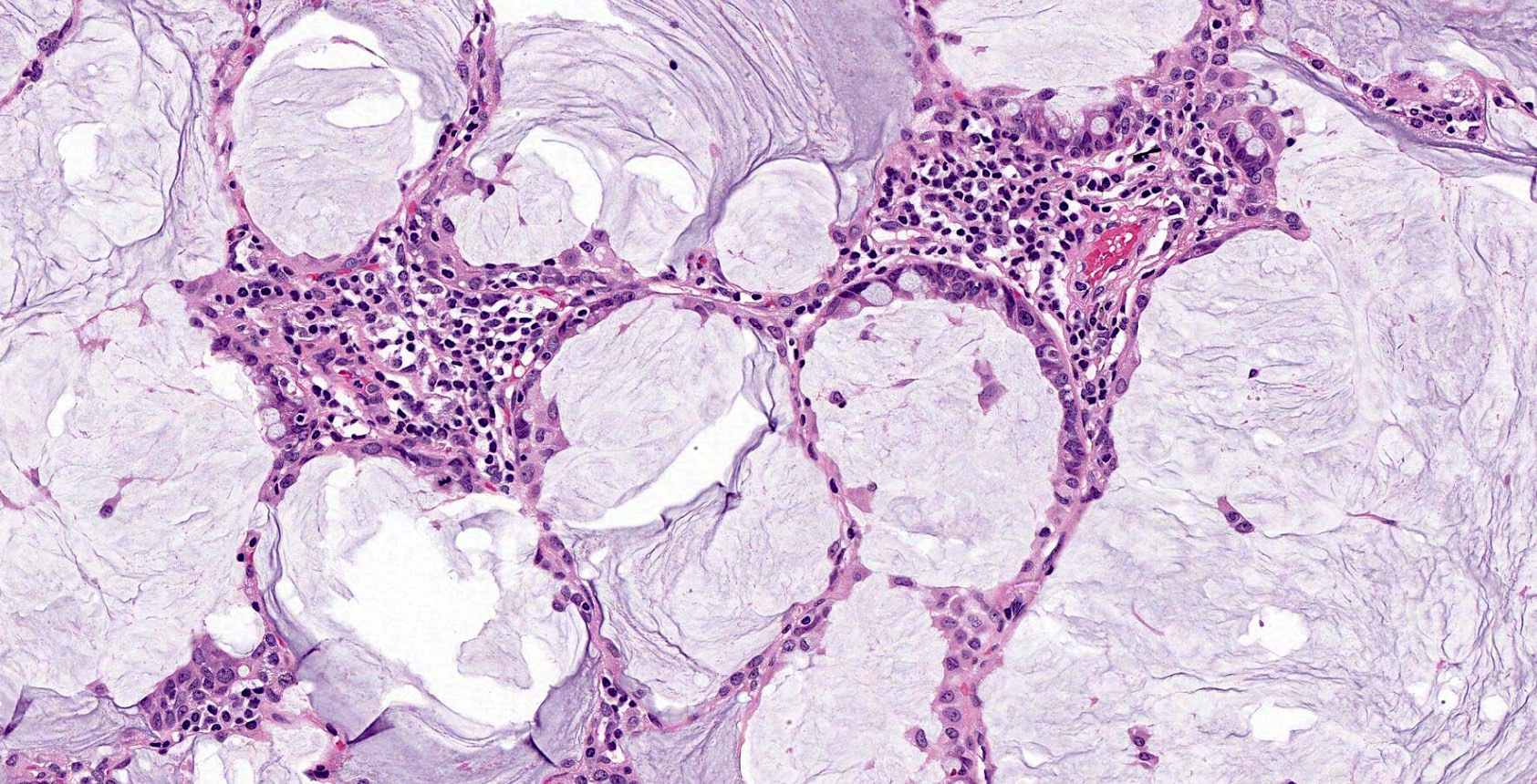
- Inflammatory infiltrate possible
- Reference: Hum Pathol 2015;46:836
Microscopic (histologic) images
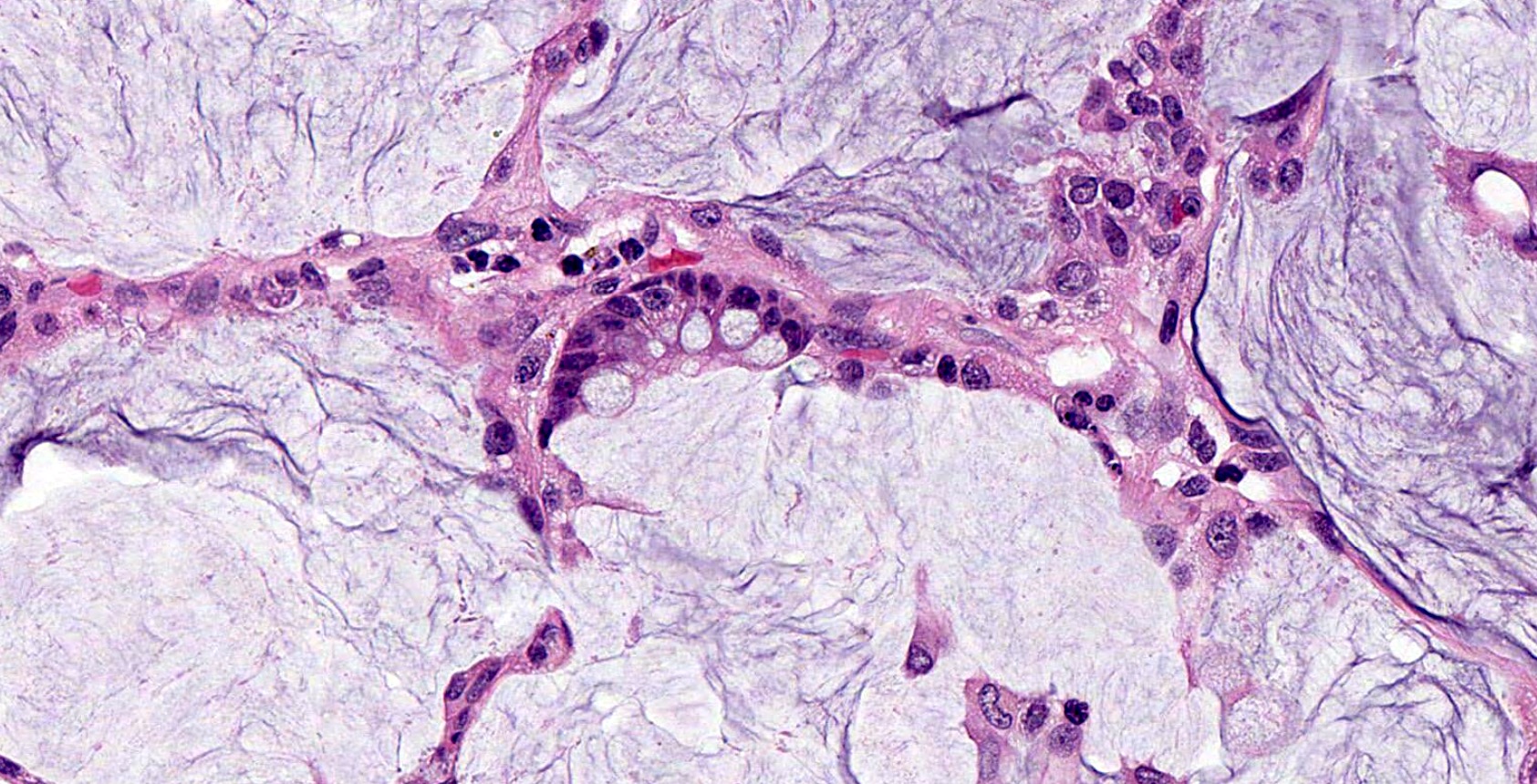
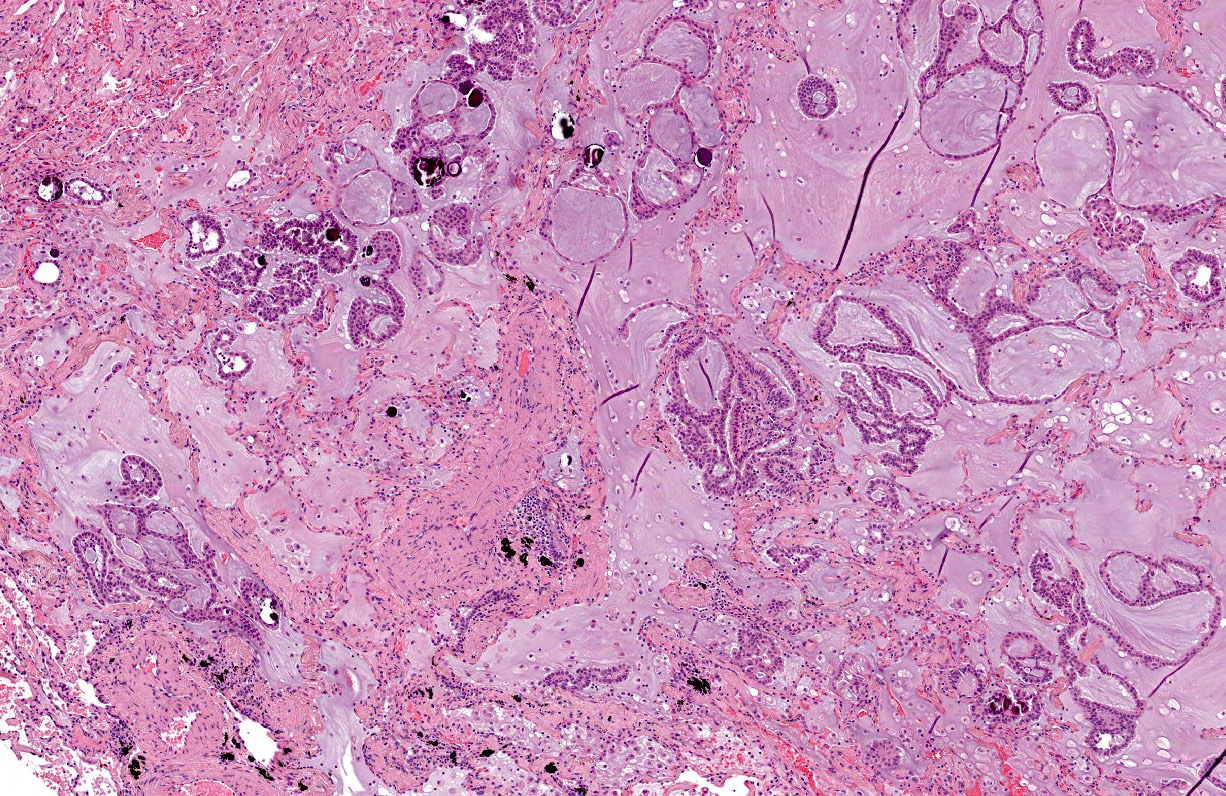
Contributed by Gheorghe-Emilian Olteanu, M.D., Ph.D., Ana Mataić, M.D. and Luka Brčić, M.D., Ph.D.
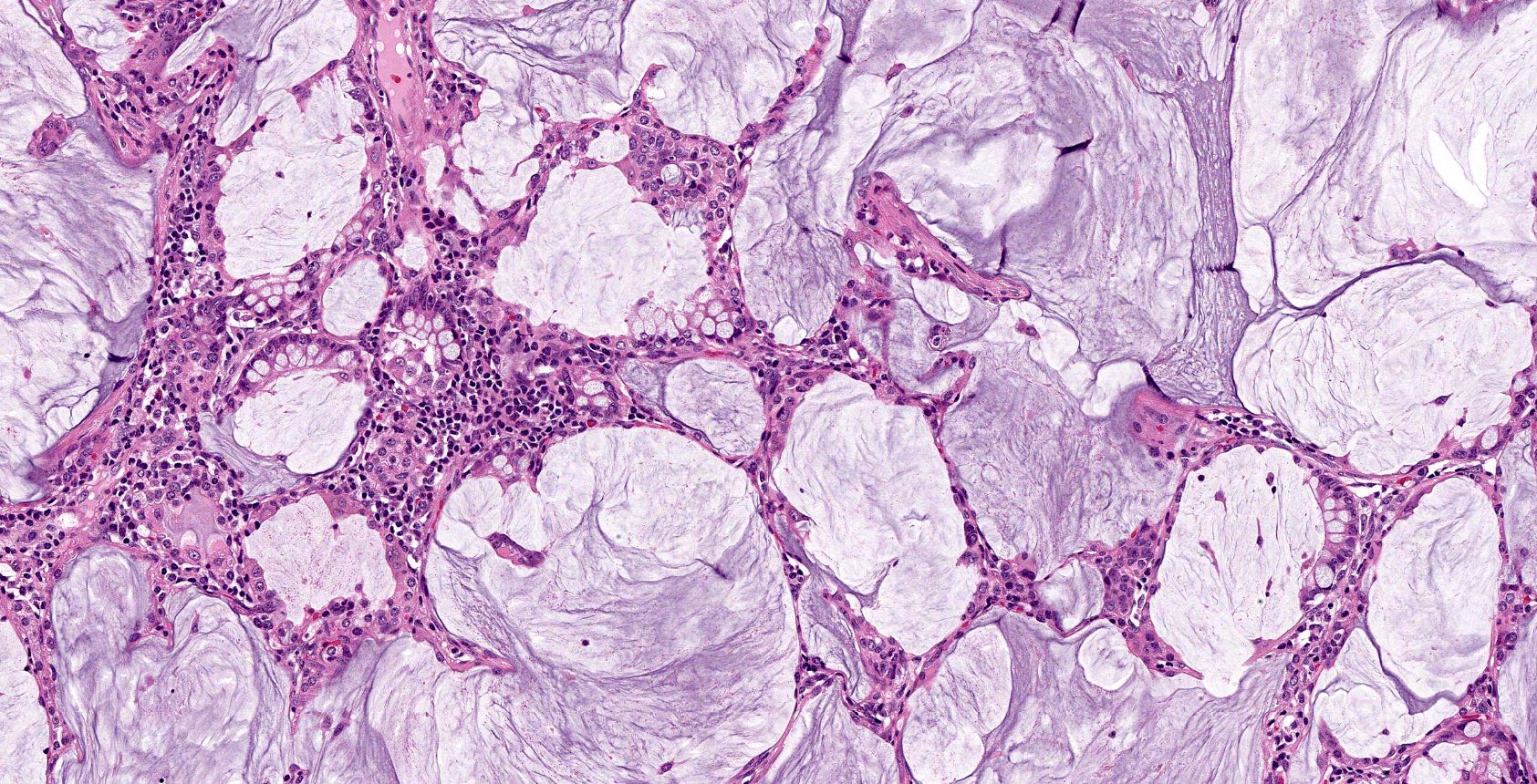
Abundant extracellular mucin
Mucin laden cells
Hypercellularity
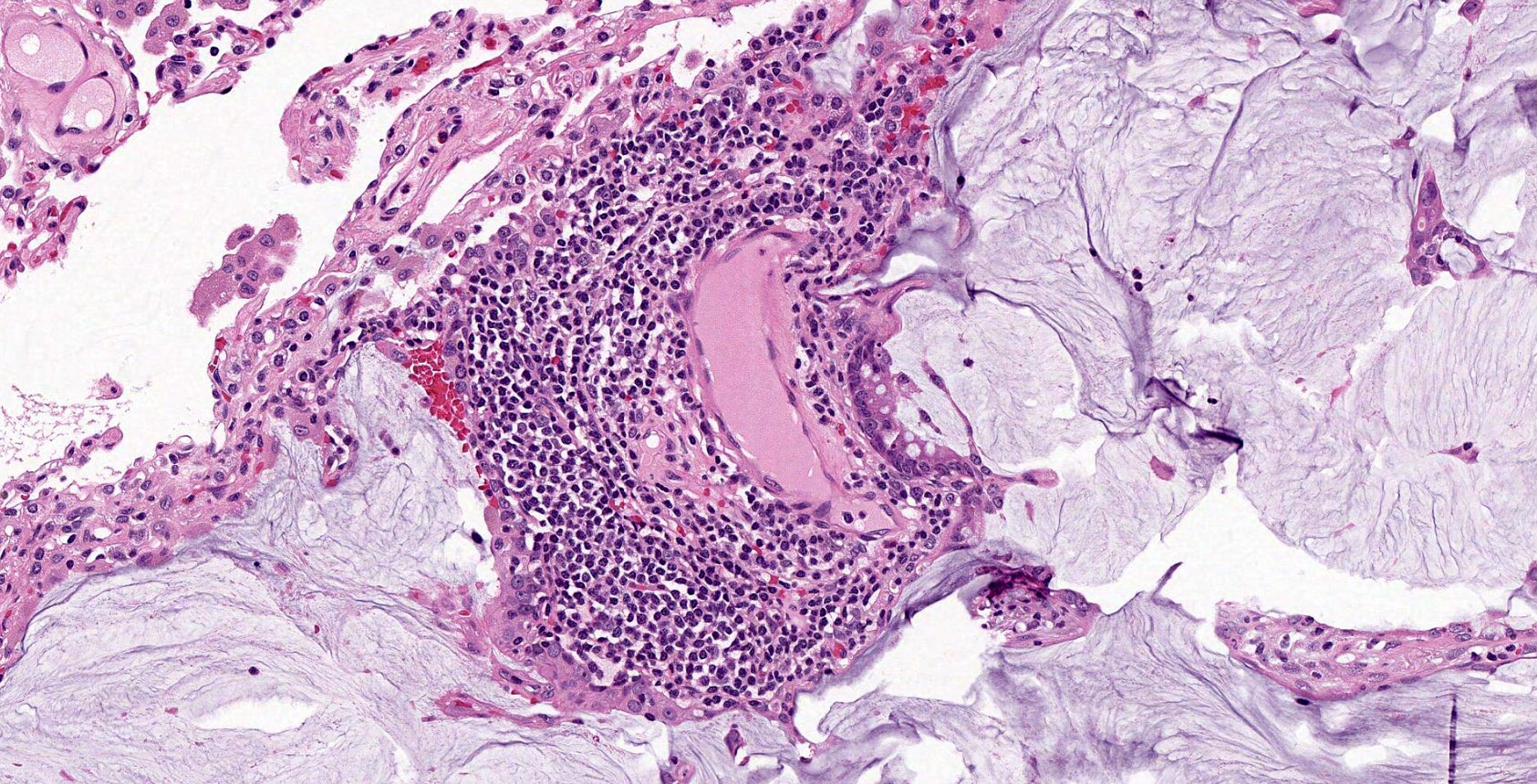
Inflammatory infiltrate
Nuclear and cytoplasm detail
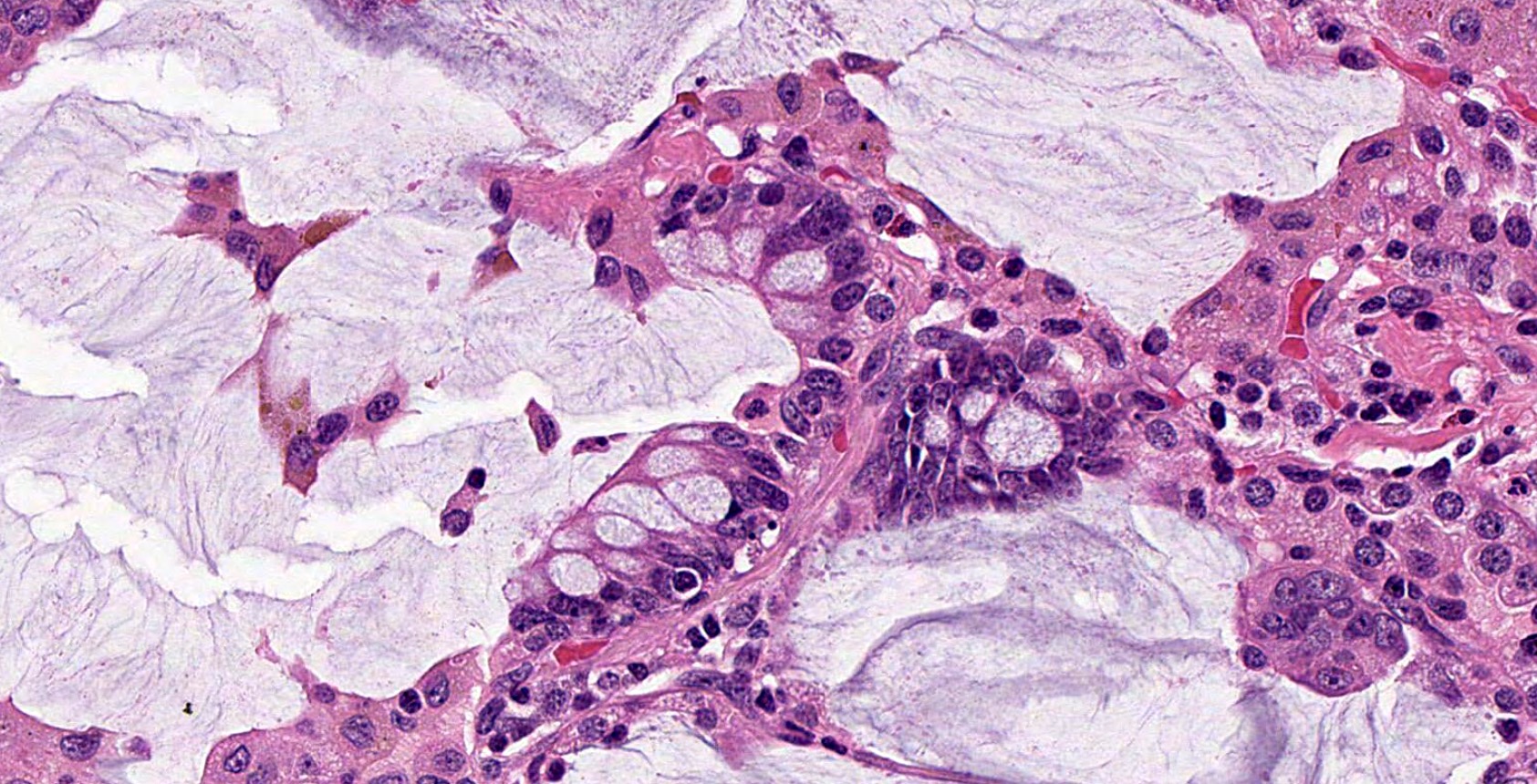
Siderophages and colloid adenocarcinoma cells
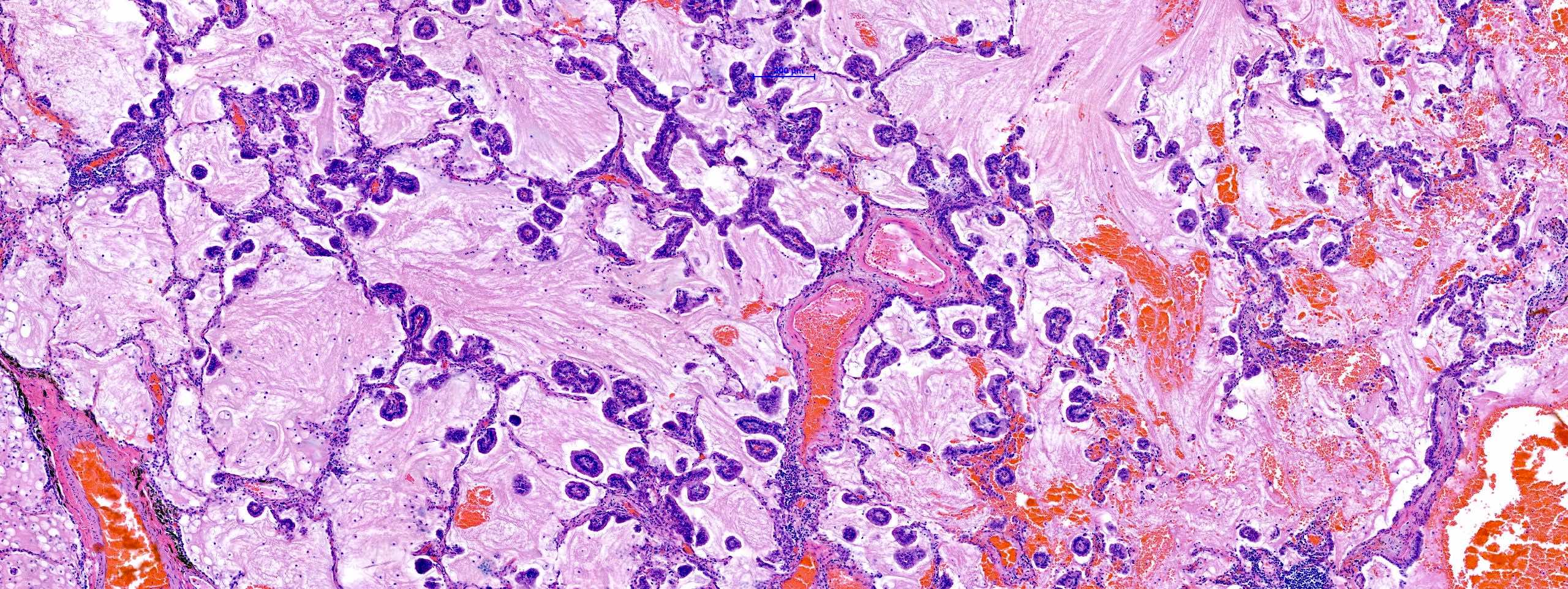
Extensive extracellular mucin
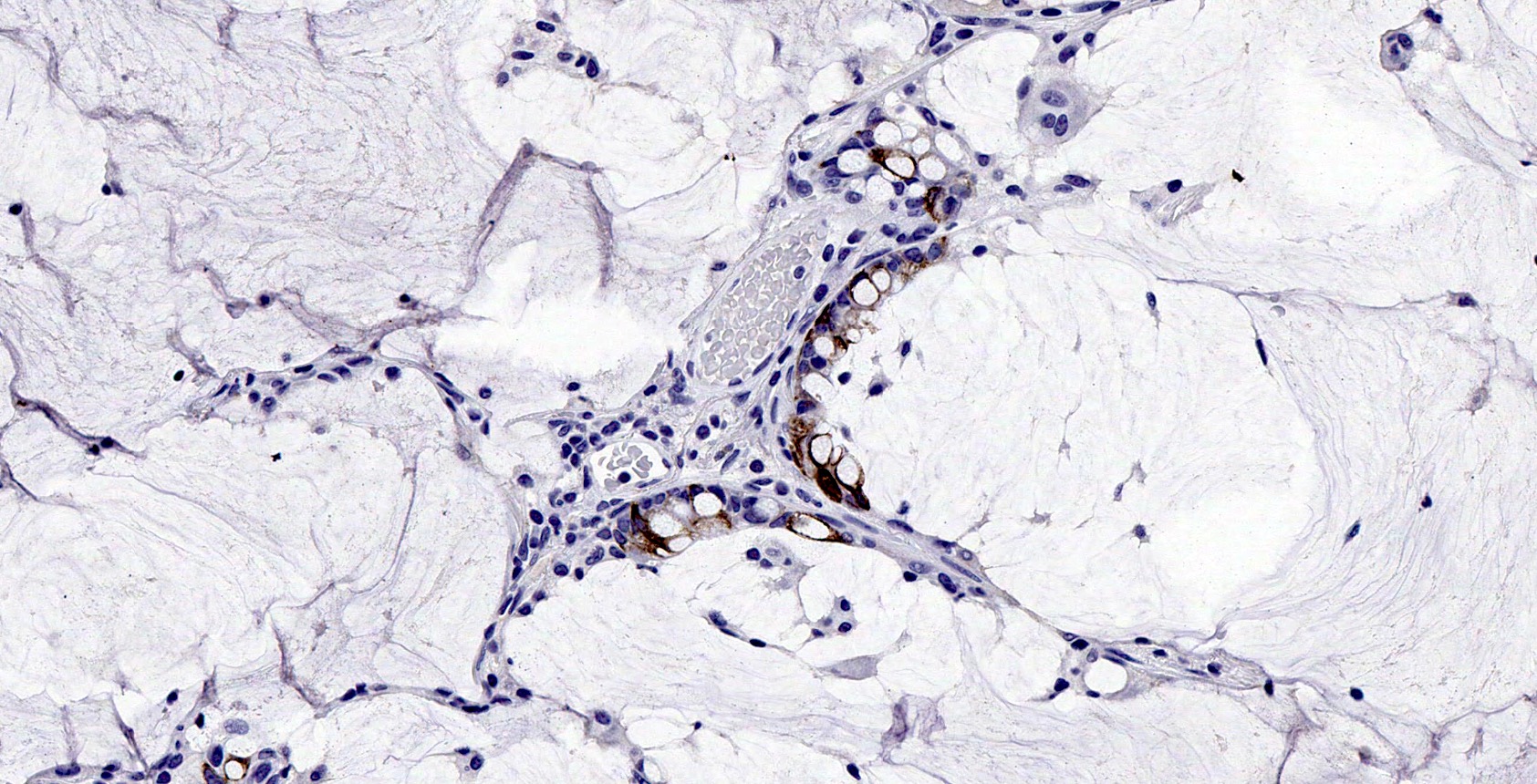
CK20 IHC stain
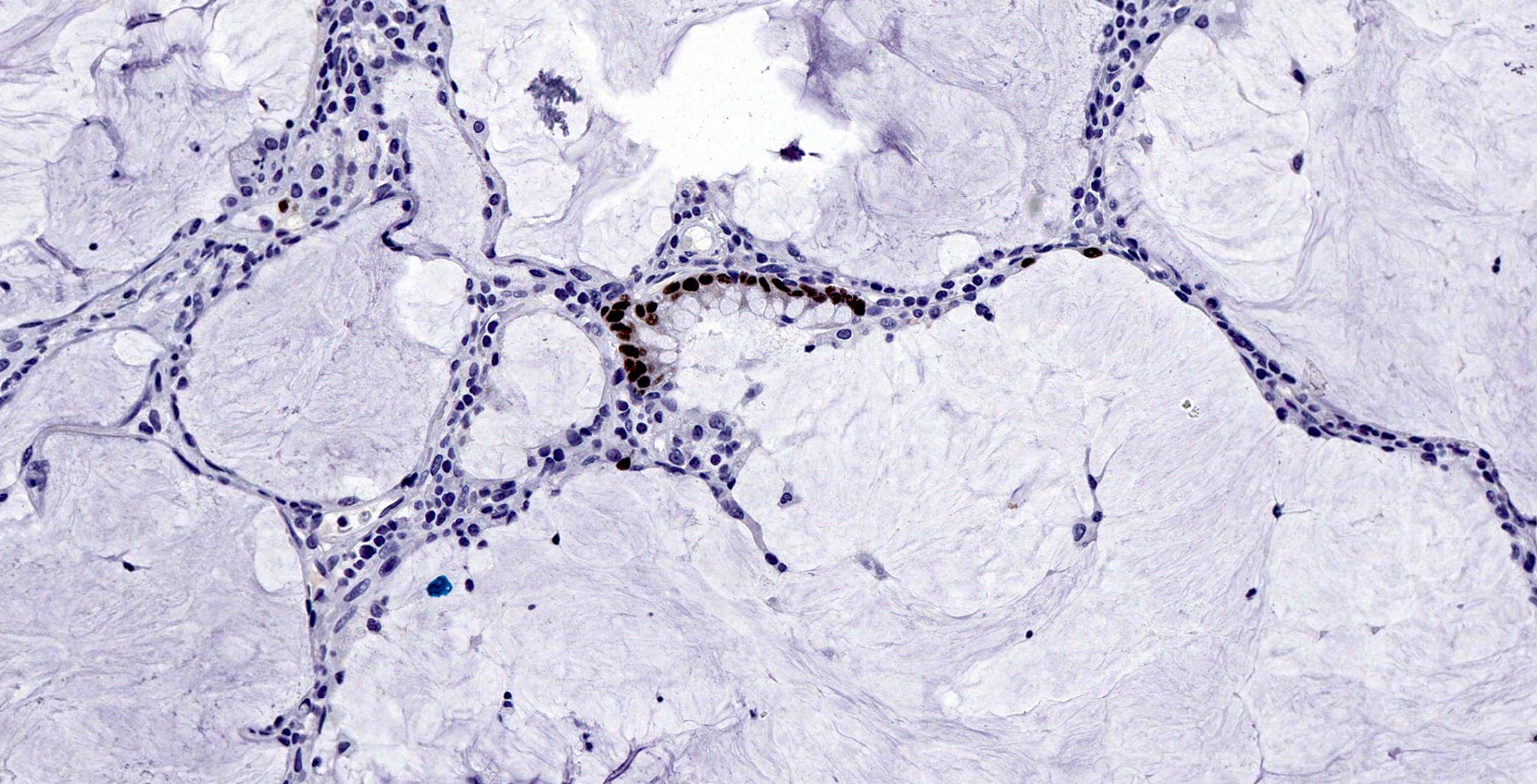
CDX2 IHC stain
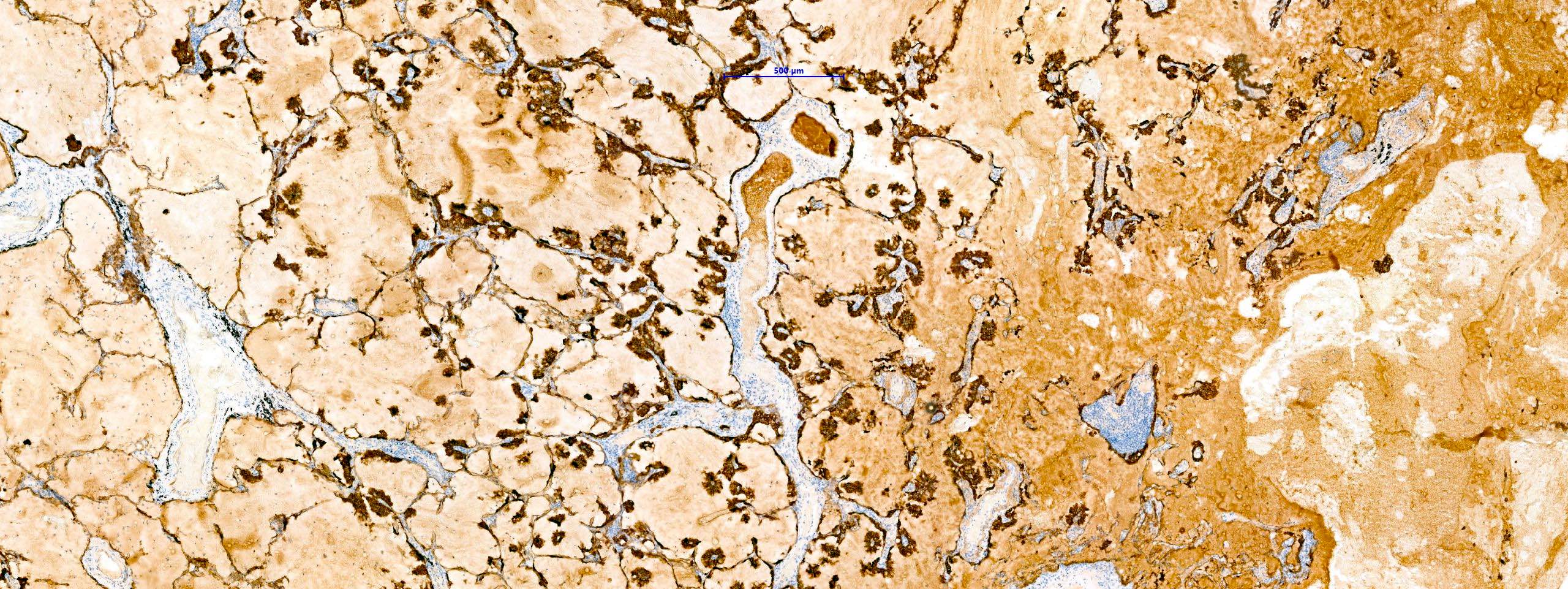
CK7 IHC stain
Virtual slides
Images hosted on other servers:

Well demarcated
colloid adenocarcinoma
with abundant
mucin pools
Cytology description
- Low cellularity
- Tumor cells in tissue fragments
- Single cells resembling histiocytes
- Thick extracellular mucin pools
- Reference: Cancer Cytopathol 2015;123:306
Cytology images
Images hosted on other servers:

Clusters of cells with basally oriented nuclei
Positive stains
- CK7, CK20 and CDX2 are diffusely and strongly positive (Hum Pathol 2015;46:836)
- TTF1 can be focally positive in a percentage of cases (Hum Pathol 2015;46:836)
Negative stains
Molecular / cytogenetics description
- KRAS mutations are more common (mutations in codons 12 and 13 have been seen)
- No EGFR mutations or ALK rearrangements
- Reference: Hum Pathol 2015;46:836
Sample pathology report
- Lung, lobectomy:
- Colloid adenocarcinoma (see comment)
- Comment: Abundant extracellular mucin pools with distended and destroyed alveolar spaces. Tumor cells are bland, mucin laden and cuboidal to columnar. Overall, the tumor has an invasive growth pattern.
Differential diagnosis
- Imaging and history is often needed given the overlapping immunoprofiles of metastatic mucinous adenocarcinomas with colloid adenocarcinoma
- Metastatic carcinoma:
- Positive markers dependent on site of origin (e.g., SATB2 if colorectal, GATA3 if breast, S100P if pancreatic) (Hum Pathol 2015;46:836, Int J Surg Case Rep 2018;42:242, Am J Surg Pathol 2001;25:26, J Cytol 2018;35:247)
Additional references
Board review style question #1
Which of the following uniquely represents invasive colloid adenocarcinoma of the lung, distinguishing it from other subtypes of lung adenocarcinoma?
- Absence of smoking as a risk factor
- Invasive lung cancer characterized by large pools of mucin destroying alveolar walls, with > 50% of the tumor demonstrating these characteristics
- Positive markers for CK7 and CDX2
- Presence of KRAS mutations
Board review style answer #1
B. Invasive lung cancer characterized by large pools of mucin destroying alveolar walls, with > 50% of the tumor demonstrating these characteristics. Invasive colloid adenocarcinoma of the lung is distinctly marked by large pools of mucin that destroy alveolar walls and this feature is present in > 50% of the tumor.
Answer D is incorrect as KRAS mutations are not unique to invasive colloid adenocarcinoma; they are one of the most commonly found mutations in all types of lung adenocarcinomas. Answer C is also incorrect since positive immunohistochemistry for CK7 and CDX2 is not exclusive to invasive colloid adenocarcinoma but is also found in mucinous lung adenocarcinoma and adenocarcinoma with enteric differentiation. Answer A is incorrect because smoking is a risk factor for all lung cancers, including colloid adenocarcinoma, and is not absent as a risk factor.
Comment Here
Reference: Colloid
Answer D is incorrect as KRAS mutations are not unique to invasive colloid adenocarcinoma; they are one of the most commonly found mutations in all types of lung adenocarcinomas. Answer C is also incorrect since positive immunohistochemistry for CK7 and CDX2 is not exclusive to invasive colloid adenocarcinoma but is also found in mucinous lung adenocarcinoma and adenocarcinoma with enteric differentiation. Answer A is incorrect because smoking is a risk factor for all lung cancers, including colloid adenocarcinoma, and is not absent as a risk factor.
Comment Here
Reference: Colloid
Board review style question #2
Which of the following statements about invasive colloid adenocarcinoma is accurate?
- Negative for CK7 and TTF1
- Positive for CDX2 and SATB2
- Positive for CK7 and CDX2
- Typically presents EGFR mutations or ALK rearrangements
Board review style answer #2
C. Positive for CK7 and CDX2. Invasive colloid adenocarcinomas typically test positive for CK7 and CDX2. They usually display weak or negative expressions for TTF1 and are negative for SATB2 (it is important to note that the positivity for CDX2 is a common pitfall in colloid adenocarcinoma). Answer D is incorrect because invasive colloid adenocarcinomas more often have KRAS mutations and generally test negative for predictive biomarkers like EGFR mutations and ALK rearrangements. Answer B is incorrect because these tumors are typically negative for SATB2. Answer A is incorrect because invasive colloid adenocarcinomas are generally positive for CK7, not negative. While they can be weak or negative for TTF1, this statement does not represent the full picture.
Comment Here
Reference: Colloid
Comment Here
Reference: Colloid
Board review style question #3
A 67 year old man presented with difficulty breathing, cough and expectoration. A chest CT reveals a mass in the lower right portion of the lung measuring 53 mm in diameter. A biopsy finds abundant mucin but no atypical cells. Following a lobectomy, immunohistochemistry of tumor cells indicates expression of CK7, CK20 and CDX2 but not TTF1 or SATB2. The patient has no history of previous tumors and no malignancy in the gastrointestinal tract is currently detected. Given the image and the provided information, what is your pathological diagnosis?
- Adenocarcinoma with enteric differentiation
- Invasive colloid adenocarcinoma of the lung
- Invasive mucinous adenocarcinoma of the lung
- Metastatic adenocarcinoma of the gastrointestinal tract
Board review style answer #3
B. Invasive colloid adenocarcinoma of the lung. The patient's immunohistochemistry results and morphological characteristics suggest invasive colloid adenocarcinoma of the lung. Although invasive mucinous adenocarcinomas and enteric type adenocarcinomas are possible considerations based on the immunohistochemistry, the morphology leans towards a diagnosis of colloid lung adenocarcinoma. Answer C is incorrect as the presence of abundant mucin, specific immunohistochemical markers and the lack of atypical cells makes invasive mucinous adenocarcinoma less likely. Answer A is incorrect as adenocarcinoma with enteric differentiation typically expresses SATB2, which is not observed in this case. Answer D is ruled out by the patient's negative history of previous tumors, the absence of current gastrointestinal malignancy and negative SATB2 expression.
Comment Here
Reference: Colloid
Comment Here
Reference: Colloid

