Lung
Salivary gland type tumors
Pleomorphic adenoma
Author: Roseann I. Wu, M.D., M.P.H.
Last author update: 1 May 2016
Last staff update: 7 June 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Pleomorphic adenoma lung [title]

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Differential diagnosis | Additional referencesCite this page: Wu R. Pleomorphic adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumoradenoma.html. Accessed April 1st, 2025.
Definition / general
- Pulmonary adenoma includes bronchial adenoma, alveolar adenoma, papillary adenoma
- Pleomorphic adenoma could be considered a type of bronchial adenoma
- Benign tumor with biphasic growth, resembling counterpart in salivary glands; need to exclude metastasis from salivary glands
- Related entities:
- Alveolar adenoma:
- Benign tumor in asymptomatic patients
- Presents as coin lesion, usually in peripheral lung, consisting of small cystic spaces lined by type II pneumocytes and containing fluid
- Interstitial cellular component consists of epithelioid and spindle shaped cells
- Bronchial gland adenoma:
- Includes oncocytoma and mucus gland adenoma, a rare, solitary, benign, well circumscribed, multicystic, predominately exophytic bronchial tumor
- Carcinoma ex pleomorphic adenoma:
- Malignant cases arising from pleomorphic adenoma (Am J Clin Pathol 2011;136:793)
- Intracapsular carcinoma ex pleomorphic adenoma:
- Malignant component does not breach the capsule of the parent tumor, no metastatic potential
- Papillary adenoma:
- Arises in peripheral lung, composed of type II pneumocytes (club cells), TTF1+
- Rarely has infiltrative features (Virchows Arch 2000;436:289)
- Alveolar adenoma:
Essential features
- Primary pulmonary pleomorphic adenoma is a very rare benign tumor that tends to arise in the large airways
- Tumors tend to show small, branching, double layered ductules rather than ducts and less cartilaginous stroma as compared to pleomorphic adenomas arising in the salivary gland
- Keratin and vimentin staining of the epithelial component supports diagnosis of primary pulmonary tumor as opposed to only keratin staining in salivary gland tumors (Arch Pathol Lab Med 2003;127:621)
- Prognosis is generally good, but cases of carcinoma ex pleomorphic adenom have been reported
Terminology
- Pleomorphic adenoma is also known as mixed tumor
- Overlaps with “myoepithelioma”, which could be used for lesions with less cartilaginous and ductal differentiation
Epidemiology
- Very rare (< 40 cases reported), predominantly in young adults, age range 8 - 74 years
- Possibly shows slight F > M
Sites
- Usually in trachea and major bronchi, rarely in distal bronchi
Etiology
- Controversial, possibly from tracheal and bronchial submucosal glands or primitive stem cells
Clinical features
- Frequently asymptomatic but can present with dyspnea, hemoptysis, fever, weight loss or effusion
- Depending on location, may cause obstruction of airway
Diagnosis
- Broader differential diagnosis on biopsy specimens but generally straightforward on resection specimen
Radiology images
Images hosted on other servers:

Enhanced and nonenhanced CT scan
Prognostic factors
- Generally indolent; no features to predict rare cases of metastasis
Case reports
- 8 year old boy with severe respiratory distress and tracheal mass (J Pediatr Surg 2006;41:e23)
- 34 year old woman with dyspnea on exertion and mainstem bronchus mass (Gen Thorac Cardiovasc Surg 2009;57:43)
- 56 year old woman with incidental lesion (Arch Pathol Lab Med 2003;127:621)
- 65 year old man with stridor and mainstem bronchus mass (Ann Thorac Surg 2008;86:1025)
Treatment
- Complete conservative surgical excision, but may recur many years later
- Endobronchial resection may be an option in some cases (Intern Med 2008;47:1117)
Gross description
- Bronchial lesions are typically polypoid
- Peripheral lesions are usually attached to bronchi, well circumscribed, no capsule, 1 - 16 cm, gray - white, soft, rubbery with chondroid cut surface, may have tumor tongues outside circumscribed margin
Gross images
Images hosted on other servers:

Cut surface shows a well defined
mass, whitish to yellowish,
partly myxoid, solid and cystic
Microscopic (histologic) description
- Generally less cartilaginous stroma than salivary gland counterpart, with small branching ductules rather than ducts
- Nests, tubules, trabeculae
- Mixture of round or oval epithelial cells and myoepithelial cells in chondromyxoid or fibromyxoid stroma with focal hyalinization
- Generally nuclear atypia / necrosis / hemorrhage / mitoses, occasional multinucleated giant cells
- May show myoepitheliomatous, plasmacytoid, squamous features
- Lumina may contain PAS+ eosinophilic secretions
Microscopic (histologic) images
Contributed by Roseann Wu, M.D., M.P.H.
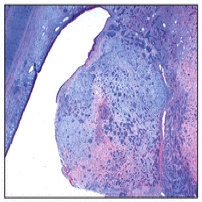
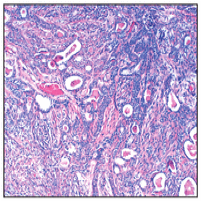
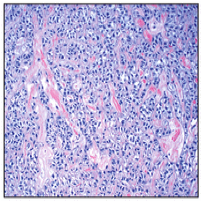
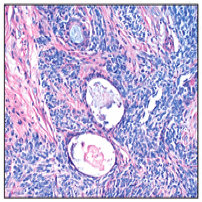
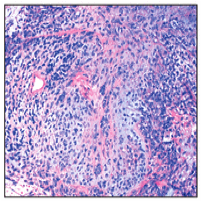

Various images
Images hosted on other servers:

Metastasizing tumor with benign features
Cytology description
- Fibrillary stroma mixed with bland basaloid epithelial cells
Positive stains
Negative stains
Differential diagnosis
- Primary salivary gland tumors: have ducts with single layer of cells, no PAS+ material in lumens, no S100+ / vimentin+ myoepithelial layer
- In biopsy specimens: hamartoma / chondroma, squamous cell carcinoma (in cases of pleomorphic adenoma with squamous metaplasia), or biphasic malignancies could be considered
Additional references
