
Lung
Adenocarcinoma
Enteric
Authors: Sevilay Özmen, M.D., Pembe Oltulu, M.D.
Editorial Board Member: Jefree J. Schulte, M.D.


Last author update: 21 March 2023
Last staff update: 21 March 2023
Copyright: 2022-2024, PathologyOutlines.com, Inc.
PubMed Search: Enteric adenocarcinoma lung

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Özmen S, Oltulu P. Enteric. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumoradenoenteric.html. Accessed December 25th, 2024.
Definition / general
- Pulmonary enteric adenocarcinoma (PEAC) is an extremely rare subtype of non-small cell lung cancer that is characterized by pathological features similar to those of colorectal adenocarcinoma
Essential features
- Morphologically similar to colorectal adenocarcinoma
- Enteric pattern may coexist with other adenocarcinoma patterns
- Diagnosis of enteric adenocarcinoma should be made when the enteric component is > 50% of the tumor (Medicine (Baltimore) 2017;96:e8153, Int J Clin Exp Pathol 2014;7:1266)
Terminology
- Adenocarcinoma, enteric type
- Primary lung enteric adenocarcinoma
- Pulmonary intestinal type adenocarcinoma (not recommended)
- Pulmonary adenocarcinomas showing enteric differentiation (not recommended)
ICD coding
- ICD-O: 8144/3 - adenocarcinoma, intestinal type
- ICD-10: C34 - malignant neoplasm of bronchus and lung
- ICD-11: 2C25.0 & XH0349 - adenocarcinoma of bronchus or lung & adenocarcinoma, intestinal type
Epidemiology
- Overall prevalence in non-small cell lung carcinoma and primary pulmonary adenocarcinoma is 0.5% and 0.68%, respectively (Transl Oncol 2021;14:101123)
- Large proportion of patients are elderly (Oncotarget 2017;8:63442, J Transl Med 2018;16:81)
- Youngest patients in the literature are a 24 year old man and 26 year old woman (Case Rep Pulmonol 2014;2014:282196)
- Recent epidemiological studies have revealed that it usually occurs in ex smokers or nonsmokers; in previous studies, 45.6% of patients with PEAC reported smoking (Transl Oncol 2021;14:101123)
- M:F = 4:5 (Int J Clin Exp Pathol 2014;7:1266)
Sites
- Generally located in the right upper lobe (Transl Oncol 2021;14:101123, Int J Clin Exp Pathol 2014;7:1266)
- PEAC is mostly located peripherally (Medicine (Baltimore) 2017;96:e8153)
Pathophysiology
- High ERBB2, MMR and KRAS mutation rates; low EGFR and BRAF mutation rates (Transl Oncol 2021;14:101123)
Etiology
- Many studies have reported that 45.6% of patients with PEAC are smokers (Transl Oncol 2021;14:101123)
Clinical features
- Clinical features are not substantially different from those of other lung adenocarcinomas
- Most patients are elderly men and smokers with advanced stage disease (Hum Pathol 2017;64:179, Exp Ther Med 2016;11:201, Medicine (Baltimore) 2017;96:e8153)
- Nonproductive cough and chest pain, fever, hemoptysis (Int J Clin Exp Pathol 2014;7:1266)
- Compared with primary pulmonary invasive adenocarcinoma, patients with PEAC are older and have larger lesions at more advanced stages (Medicine (Baltimore) 2017;96:e8153)
- Coughing is the most common but nonspecific symptom (Chin Med J (Engl) 2019;132:1368, Oncol Lett 2017;13:4651)
- Other symptoms include expectoration, hemoptysis, chest tightness, chest pain, shortness of breath, fever, night sweats, throat discomfort, headache, fatigue and enlarged cervical lymph nodes (Chin Med J (Engl) 2019;132:1368)
- lt is crucial to exclude metastatic colorectal carcinoma, which is more common than primary enteric type adenocarcinoma in the lung, by careful clinical evaluation (Am J Surg Pathol 2005;29:660)
- No gastrointestinal symptoms (e.g., hematochezia, nonproductive abdominal pain, diarrhea and ventosity) (Transl Oncol 2021;14:101123, ScienceDirect: Gastrointestinal Distress [Accessed 21 March 2023], ScienceDirect: Rectal Bleeding [Accessed 21 March 2023])
Diagnosis
- Tumor with enteric morphology and expression of intestinal markers (CDX2, CK20, HNF4a or MUC2) and coexpression of TTF1 or CK7
- Considering the common clinical features with other adenocarcinomas, a combination of clinical signs, histopathology, IHC and molecular features is required for a definitive diagnosis
- Colorectal adenocarcinoma should be ruled out by endoscopy and radiology, even if the pathological results correspond to primary enteric adenocarcinoma of the lung
- Pathology and immunohistochemistry results are mostly used in the diagnosis of PEAC (World J Clin Cases 2021;9:9236)
- The patient can finally be diagnosed with PEAC when primary PEAC consists mainly of tissue with > 50% intestinal differentiation, tumor cells are positive for at least 1 immunohistochemical marker associated with colorectal cancer (e.g., CK20, CDX2, MUC2, villin, etc.) and tumors of gastrointestinal origin are excluded
- CK7 is important for pulmonary origin
Laboratory
- Consistent overexpression of CEA and CA199 appears to be closely associated with advanced pathological stage in primary PEAC (J Transl Med 2018;16:81, World J Clin Cases 2021;9:9236)
Radiology description
- Solid nodules (Medicine (Baltimore) 2017;96:e8153)
- On CT, patients with PEAC had larger lesions than patients with primary pulmonary invasive adenocarcinoma (Medicine (Baltimore) 2017;96:e8153)
Radiology images
Images hosted on other servers:

Right upper lobe
and mediastinal
lymph node
metastasis

Tumor in the lower lobe of the left lung
Prognostic factors
- Aggressive cancer characterized by rapid growth and early metastatic behavior (Oncol Lett 2017;13:4651)
Case reports
- 24 year old man and 26 year old woman with enteric type lung adenocarcinoma in resected lung mass (Case Rep Pulmonol 2014;2014:282196)
- 53 year old woman presented with a mass around the right sternoclavicular joint and cough (Exp Ther Med 2016;11:201)
- 62 year old man with pancreatic metastases (Oncol Lett 2017;13:4651)
Treatment
- Current treatment strategy is the same as for primary adenocarcinoma
- A comprehensive treatment supported by surgical treatment, chemotherapy, radiotherapy or targeted therapy is selected according to clinical stage (Transl Oncol 2021;14:101123, World J Clin Cases 2021;9:9236)
- Patients may benefit from anti-HER2 therapy and immune checkpoint inhibitors (Transl Oncol 2021;14:101123)
- EGFR tyrosine kinase inhibitor in PEAC is unreasonable and inefficient (J Transl Med 2018;16:81)
- Patients may be more likely to benefit from checkpoint blocking immunotherapy (J Transl Med 2018;16:81)
- Although only limited data are available, alterations eligible for tyrosine kinase inhibitor therapy seem to be less common than in other non-small cell lung cancer subtypes (Mod Pathol 2019;32:855)
Gross description
- Enteric type adenocarcinomas are well circumscribed tumors; section surface may include areas of focal bleeding and necrosis (Int J Clin Exp Pathol 2014;7:1266)
- Often includes geographic necrosis (Transl Oncol 2021;14:101123)
- Tumors are ~10 - 115 mm (Transl Oncol 2021;14:101123)
- Cross sectional surface is gray-white or gray-yellow; some tumors contain hard or necrotic areas (Transl Oncol 2021;14:101123)
Frozen section description
- An adenocarcinoma with enteric morphology may be said to be present on frozen sections but without immunohistochemical study and radiological and clinical correlation, it cannot be determined whether the malignancy in the lung is primary or secondary
Microscopic (histologic) description
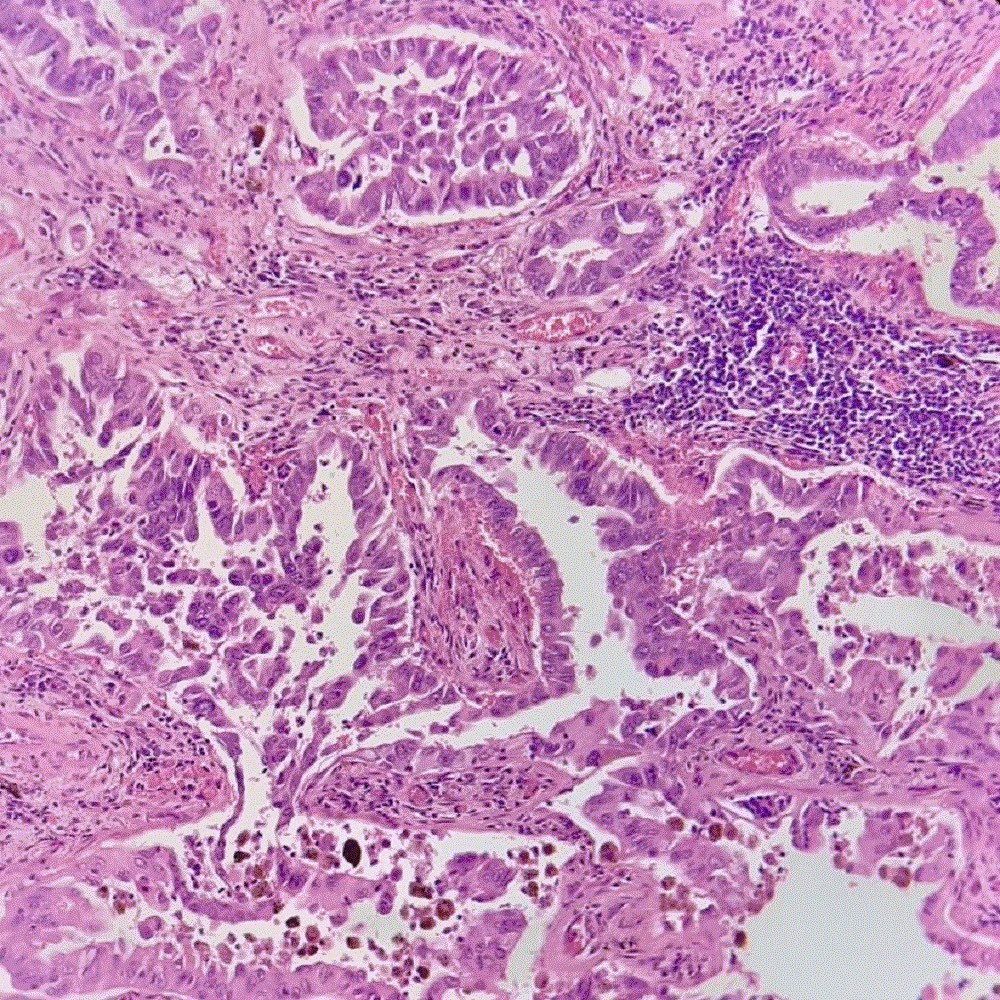
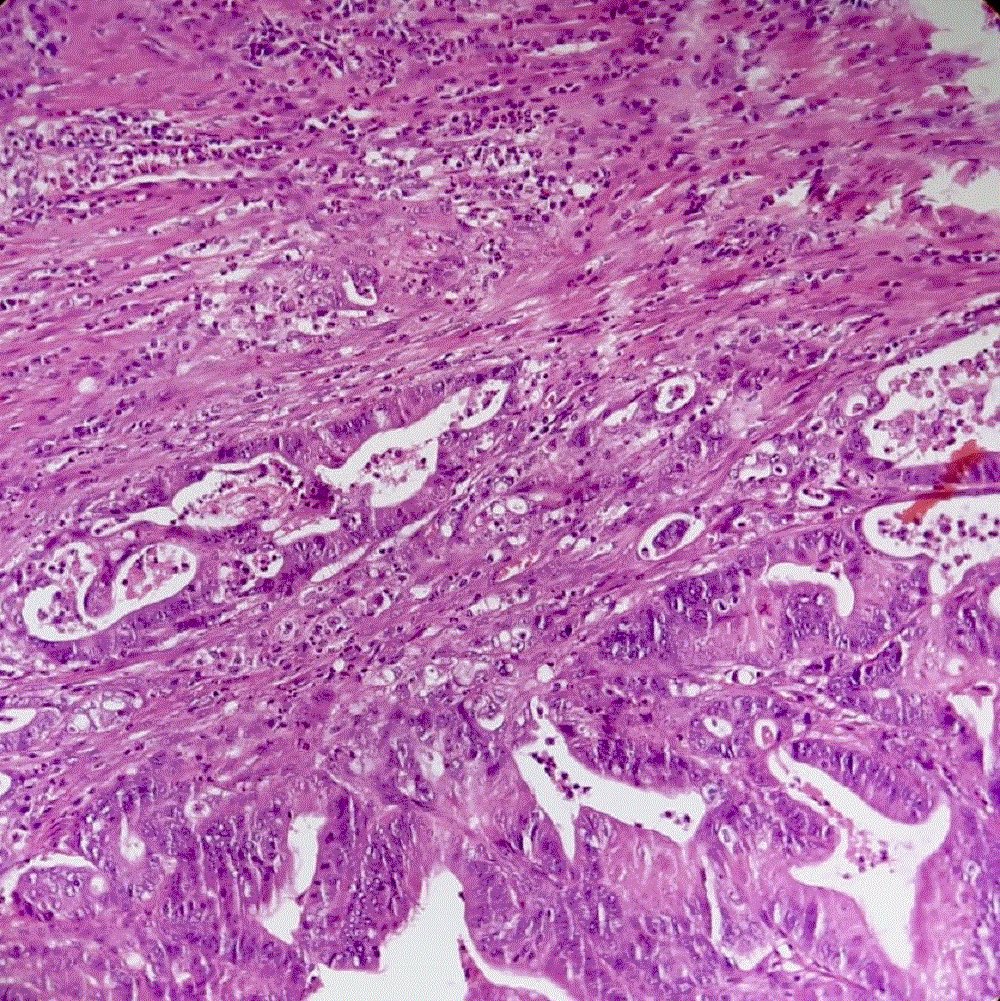
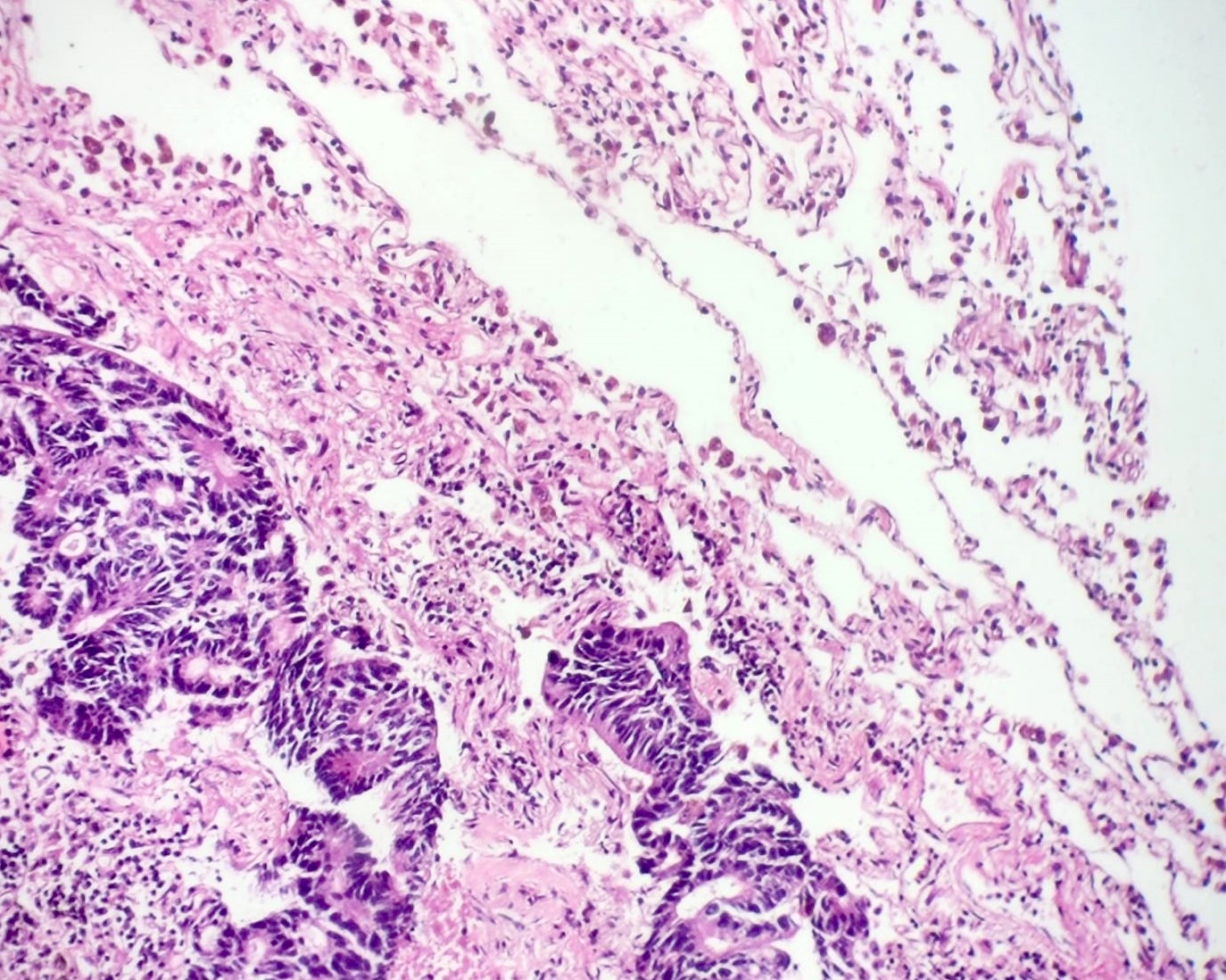
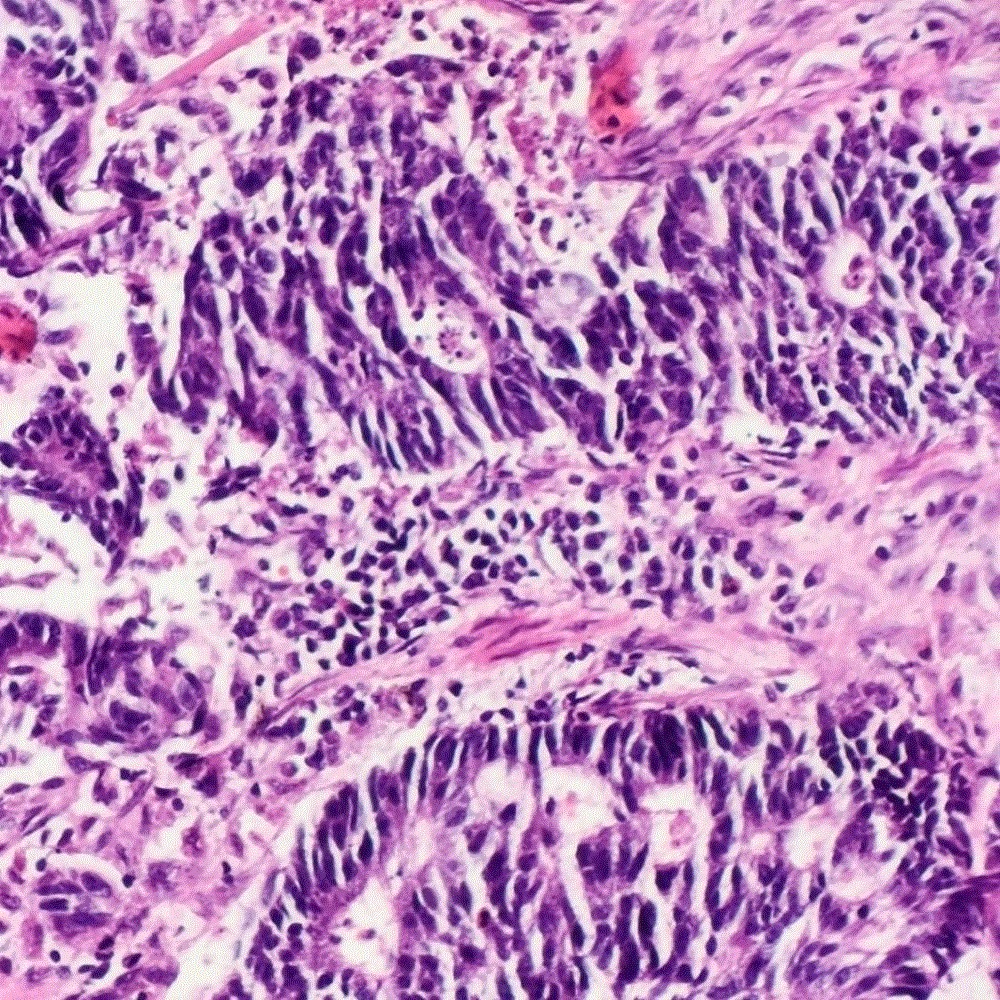
- Enteric pattern exhibits the features of colorectal adenocarcinoma, which has glandular, papillary or cribriform structures with luminal necrosis, tall columnar cells with pseudostratified and atypical nuclei, and eosinophilic cytoplasm (Oncol Lett 2017;13:4651, Int J Clin Exp Pathol 2014;7:1266)
- Enteric pattern can be admixed with other patterns of adenocarcinoma
- Mitotic figures are often found
- Stroma is often desmoplastic and associated with prominent inflammatory cell infiltrates
- Histologically, PEAC has features of intermediate differentiation and sometimes forms a cribriform pattern with tall columnar cells arranged in irregular acini or with extensive central necrosis (Oncotarget 2017;8:63442)
Microscopic (histologic) images
Contributed by Sevilay Özmen, M.D. and Pembe Oltulu, M.D.
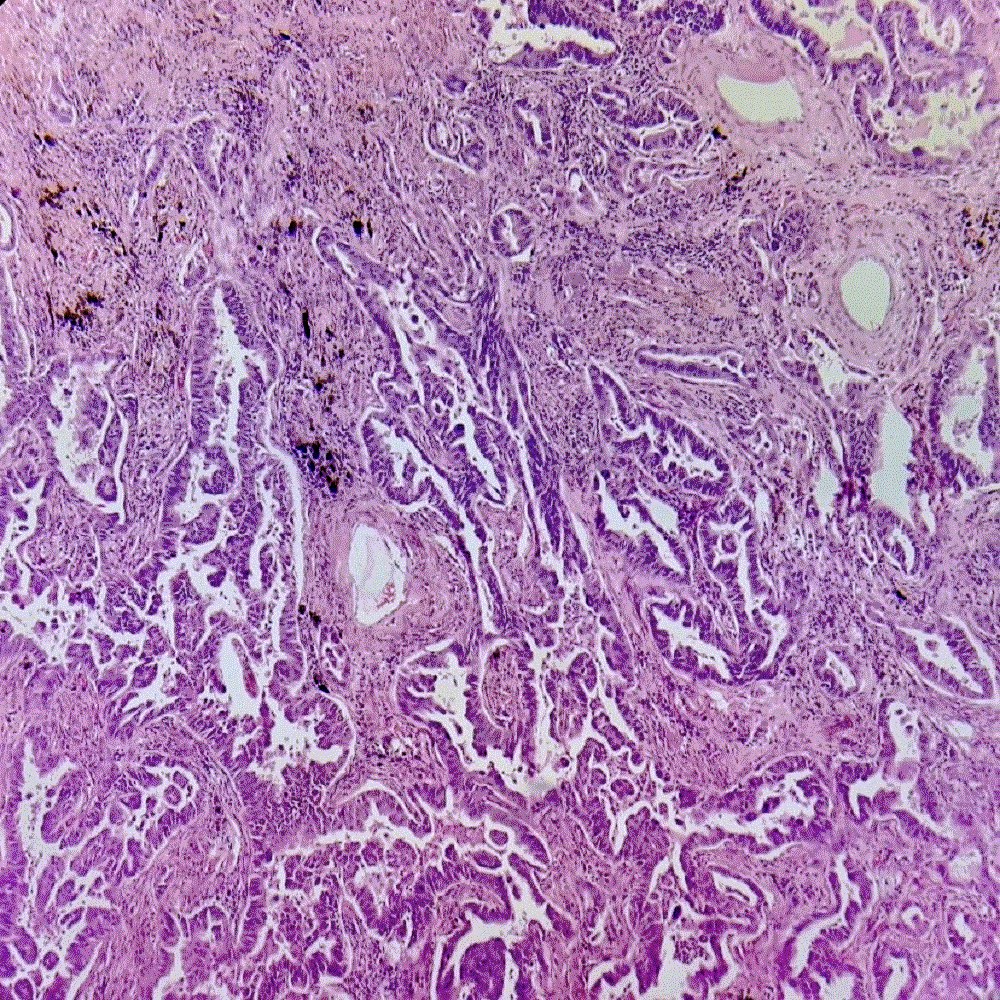
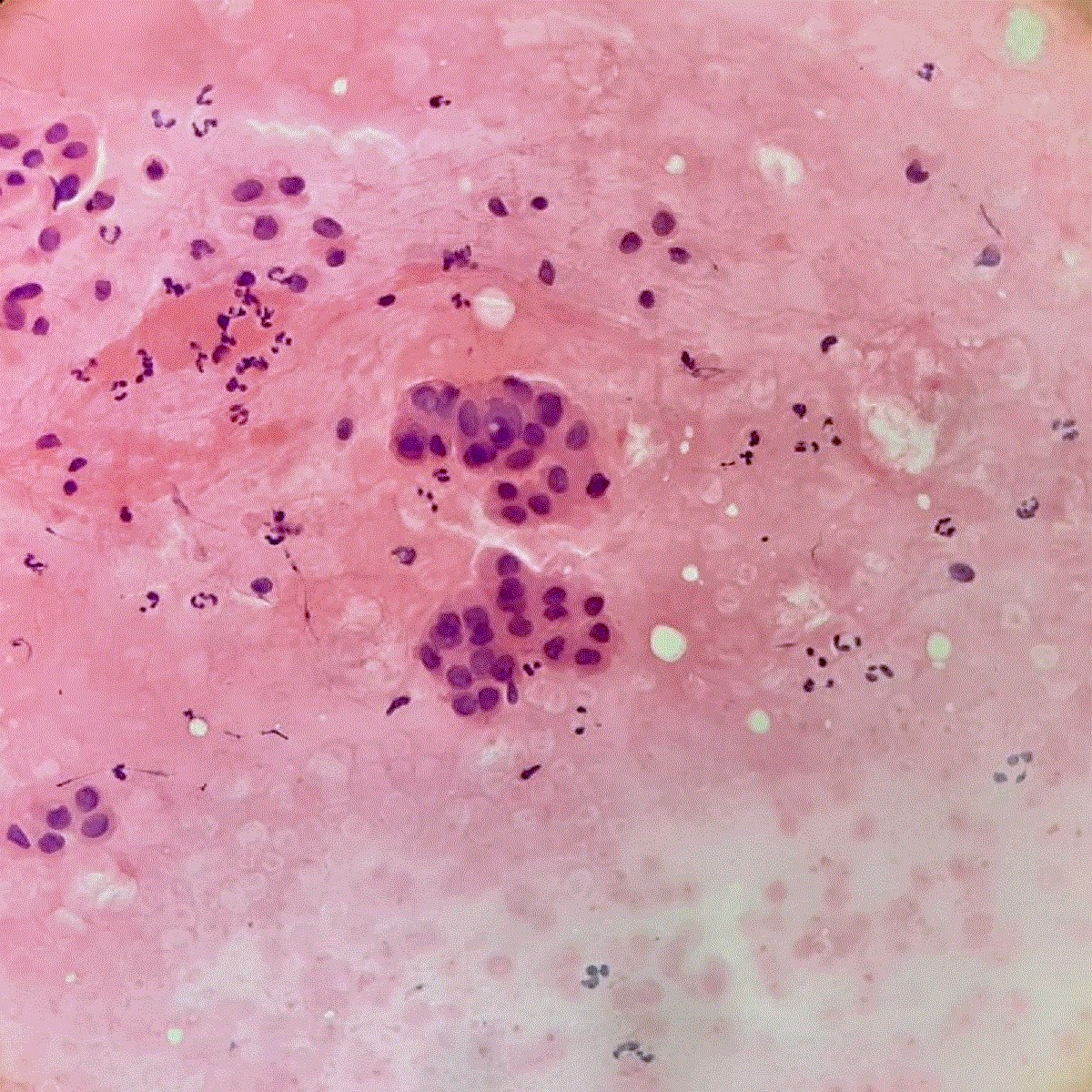
Moderately differentiated glands with necrotic debris
Cribriform and acinar growth pattern
Glands filled with necrotic debris
Cribriform growth pattern
Glands filled with necrotic debris

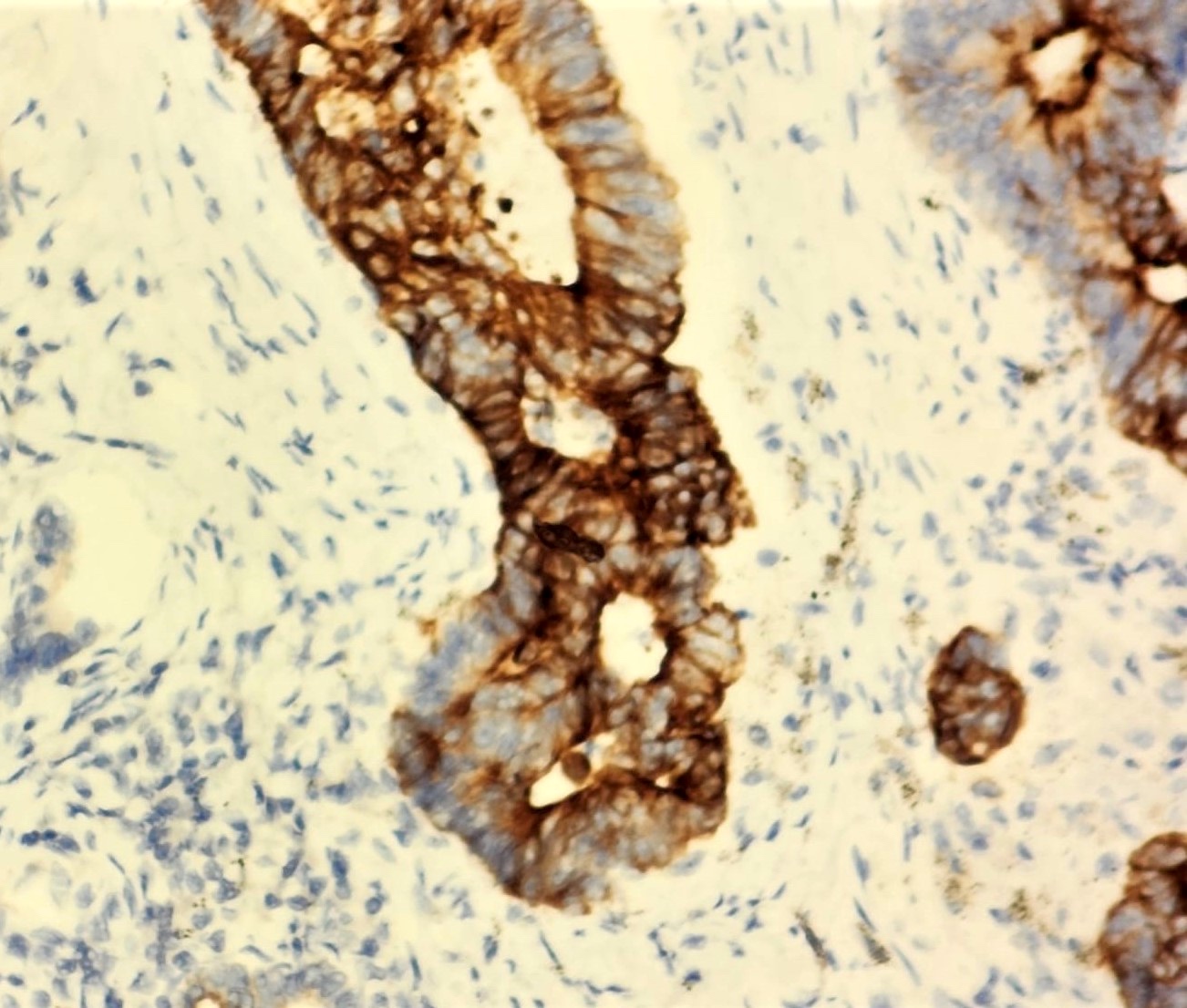
CK7 positivity
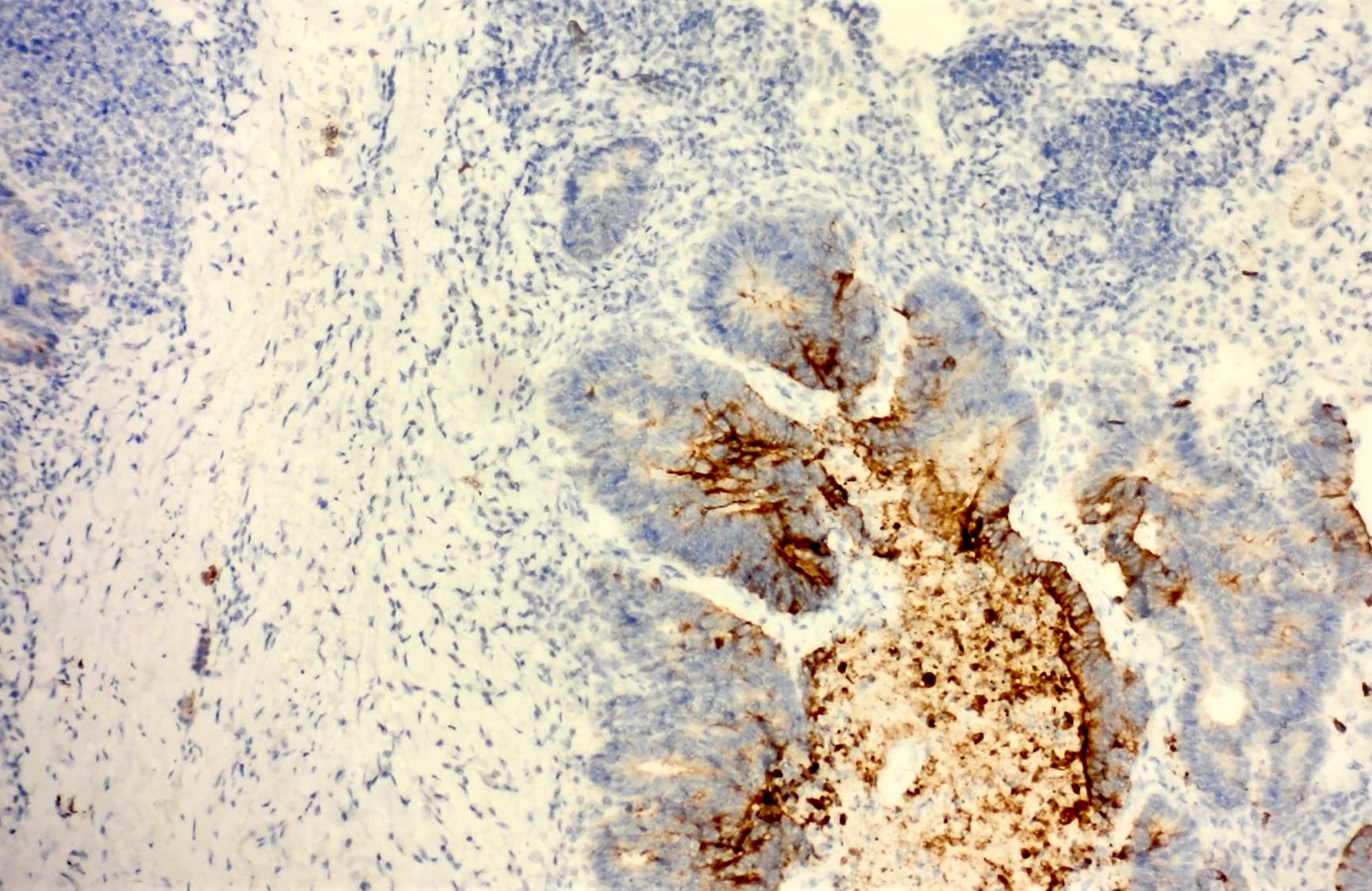
CK20 positivity
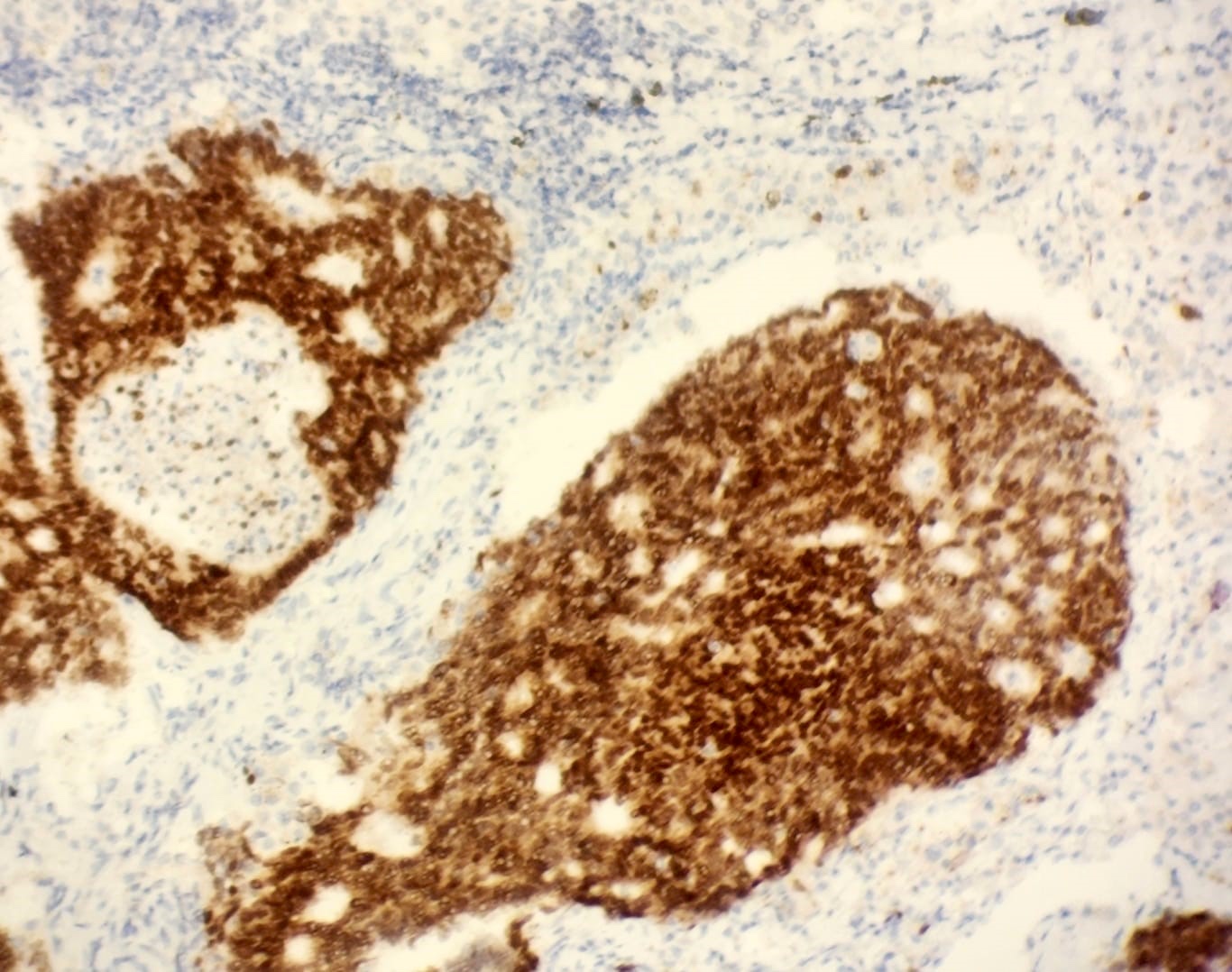
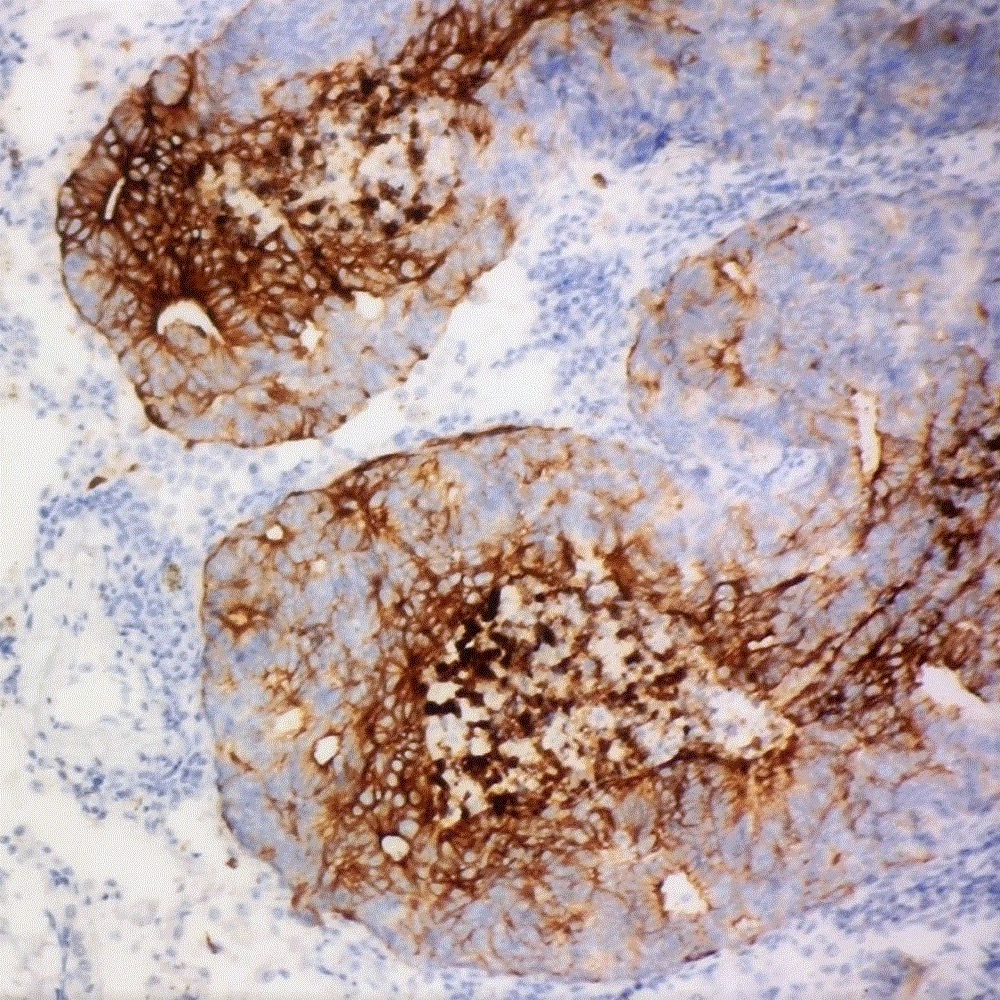
CDX2 positivity
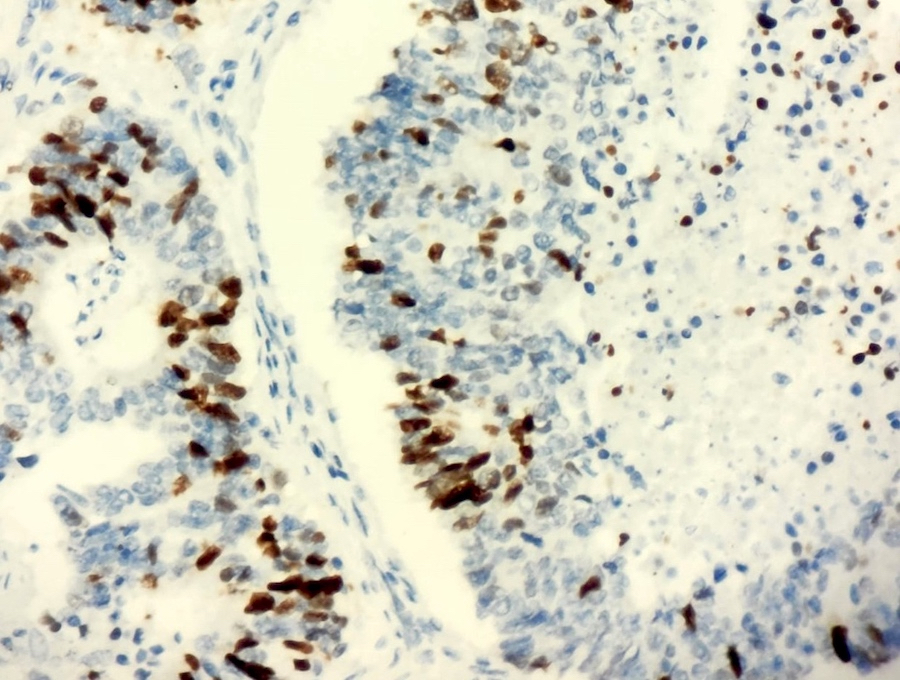
TTF1 positivity
Cytology description
- Sheets or papillary clusters of high columnar cells
- Intracytoplasmic mucin
Cytology images
Contributed by Sevilay Özmen, M.D.
Small clumps of tumor cells
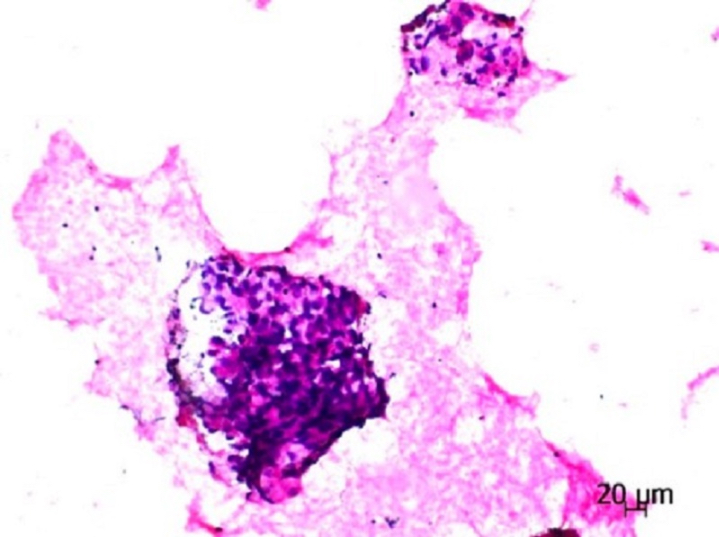
Cluster of tumor cells
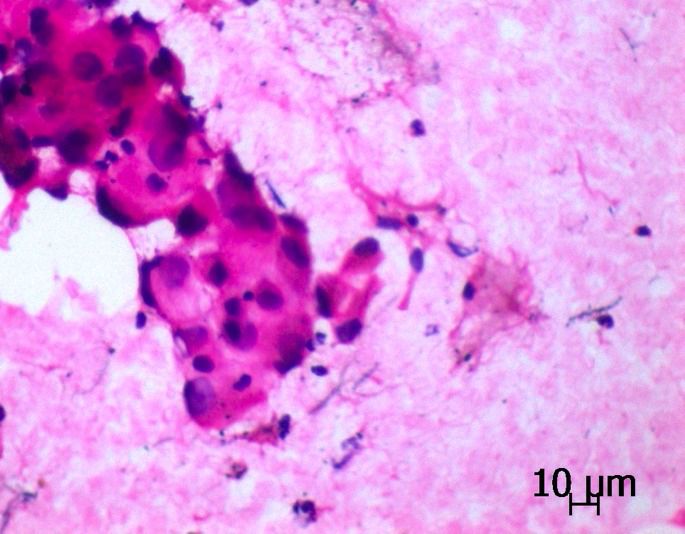
Papillary cluster
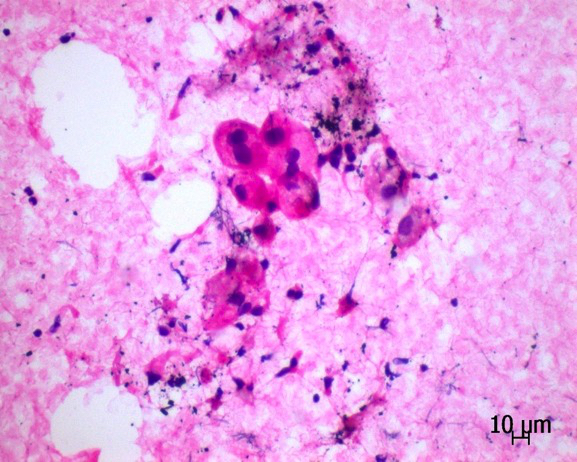
Acinar cluster
Positive stains
- CK7 / CK20 (J Transl Med 2018;16:81)
- CK7 expression in > 80% of tumor cells helps differential diagnosis from colorectal adenocarcinoma
- CDX2 (J Transl Med 2018;16:81, Chin Med J (Engl) 2019;132:1368, Front Oncol 2022;12:988625, Medicine (Baltimore) 2017;96:e8153)
- MUC2 positive in pulmonary intestinal type adenocarcinoma (J Transl Med 2018;16:81)
- Villin (Chin Med J (Engl) 2019;132:1368, Transl Oncol 2021;14:101123)
- HNF4a (Cancer Sci 2017;108:1888)
- TTF1, Napsin A: can be very weakly or focally positive (Mod Pathol 2019;32:855)
- MUC1 (Masui 1992;41:369)
Negative stains
- CDH17, only very rare expression (Mod Pathol 2008;21:1379, Adv Anat Pathol 2014;21:131, Am J Clin Pathol 2012;138:211, J Transl Med 2018;16:81, Oncotarget 2017;8:63442)
- SATB2, only very rare expression (Hum Pathol 2017;64:179, J Transl Med 2018;16:81, Oncotarget 2017;8:63442)
- Beta catenin (Hum Pathol 2017;64:179)
Molecular / cytogenetics description
- KRAS mutations are more frequent in enteric adenocarcinoma than in nonenteric pulmonary adenocarcinoma (J Transl Med 2018;16:81, Mod Pathol 2019;32:855)
- Higher nonsynonymous tumor mutation burden and more frequent MMR mutation (J Transl Med 2018;16:81)
- ERBB2 (HER2) amplification / mutation and MMR gene mutation can also occur (J Transl Med 2018;16:81)
- PIK3CA mutations and ALK rearrangement can also occur
- KRAS, HER2, MMR mutation rates are higher while EGFR is much lower (Transl Oncol 2021;14:101123)
- No ALK, MET, EGFR or ROS1 alterations (Mod Pathol 2019;32:855)
- EGFR mutation is common in primary lung adenocarcinoma but is rarely reported in PEAC (Front Oncol 2022;12:988625)
- Comutations of EGFR, KRAS and TP53 are possible (Front Oncol 2022;12:988625)
Sample pathology report
- Lung, right upper lobe, resection:
- Pulmonary enteric adenocarcinoma (see synoptic report)
- Lung, biopsy:
- Adenocarcinoma with enteric differentiation (see comment)
- Comment: In the case where malignancy in the gastrointestinal tract was excluded, the findings are consistent with enteric differentiated adenocarcinoma of the lung.
Differential diagnosis
- Metastatic colorectal adenocarcinoma:
Board review style question #1
What gene mutation is most commonly associated with enteric adenocarcinoma?
- BRCA
- EGFR
- KRAS
- NRAS
- PIK3CA
Board review style answer #1
C. KRAS. The KRAS gene in pulmonary enteric adenocarcinoma has a high mutation rate of ~40 - 50%.
Comment Here
Reference: Enteric adenocarcinoma
Comment Here
Reference: Enteric adenocarcinoma
Board review style question #2
A 60 year old man presented with complaints of cough, chest tightness and shortness of breath. He was a former smoker with 20 pack years. Chest tomography showed a 6 cm mass in the periphery of the lung. A biopsy was performed. Tumor cells immunohistochemically express CK7, CK20, CDX2 and TTF1 and the patient does not show malignancy in the gastrointestinal tract. According to the image above, what is the pathological diagnosis?
- Adenocarcinoma with enteric differentiation
- Invasive mucinous adenocarcinoma of the lung
- Large cell carcinoma of the lung
- Small cell lung cancer
- Squamous cell lung cancer
Board review style answer #2

