
Lung
Cystic disease / congenital anomalies
Sequestrations
Editorial Board Member: Jefree J. Schulte, M.D.


Last author update: 11 October 2022
Last staff update: 20 January 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Sequestrations

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Nelson ND, Pogoriler J. Sequestrations. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumorsequestrations.html. Accessed December 4th, 2024.
Definition / general
- Congenital lung malformation that is defined by an anomalous systemic vascular supply and sequestration from the tracheobronchial tree
Essential features
- Systemic feeding vessel is usually identified radiographically, documented in the surgical note and identifiable in intact gross specimens
- Extralobar bronchopulmonary sequestrations are outside the normal pleural investment and can be associated with other congenital anomalies
- Intralobar bronchopulmonary sequestrations are found within the normal pleura and are associated with an increased risk of infection
- Sequestrations may rarely have an aberrant airway connection to the GI tract but usually the main airway ends blindly in the parenchyma at the site of the feeding vessel (Pediatr Dev Pathol 2007;10:75)
Terminology
- Also called pulmonary sequestration, intralobar sequestration (ILS), extralobar sequestration (ELS)
- Hybrid lesion is a bronchopulmonary sequestration with cystic parenchymal changes similar to a type 2 congenital pulmonary airway malformation (CPAM)
ICD coding
- ICD-10: Q33.9 - congenital malformation of lung, unspecified
Epidemiology
- Congenital lung lesion
- Intralobar sequestrations are the most common (Thorax 1979;34:96, Eur J Cardiothorac Surg 2001;19:388)
- Most lesions are asymptomatic at birth
- Clinical course is dependent upon the size and location of the lesion
Sites
- Intralobar bronchopulmonary sequestrations are invested within the normal pleura and are almost always found in the lower lobes of the lung (Thorax 1979;34:96, J Pediatr Surg 2019;54:1286)
- Systemic blood supply is most often from the thoracic aorta
- Venous return is typically via the pulmonary veins
- Extralobar bronchopulmonary sequestrations are distinct from the lung and outside the normal pleural investment
- Most commonly found within the thorax but can also be seen within the abdomen, diaphragm, retroperitoneum and neck (J Pediatr Surg 2019;54:1286)
- Systemic blood supply is most often from the thoracic or abdominal aorta
- May rarely communicate with the gastrointestinal tract
Etiology
- Numerous hypotheses have been proposed
- Development from an aberrant accessory lung bud (N Engl J Med 1968;278:1413)
- Embryonal injury to the tip of a developing bronchovascular bundle with the blood supply maintained by a persistent embryonic vascular network (Thorax 1987;42:401)
- Traction caused by an aberrant systemic artery pulling a portion of the lung out of place (J Pathol Bacteriol 1946;58:457)
Diagrams / tables
Images hosted on other servers:

ILS as seen at surgery
Clinical features
- Among historic symptomatic cases, ~40 - 60% of patients with extralobar bronchopulmonary sequestrations have other congenital anomalies, including congenital diaphragmatic hernia and congenital heart disease (Thorax 1979;34:96)
- Incidence of associated anomalies is lower with asymptomatic cases identified by prenatal ultrasound (Am J Surg Pathol 2019;43:47)
- Intralobar bronchopulmonary sequestrations are most often isolated anomalies but can be associated with other findings in ~15% of symptomatic patients (Thorax 1979;34:96)
- Intralobar sequestrations that are not diagnosed prenatally may present with recurrent infection
Diagnosis
- Often diagnosed on prenatal ultrasound but may not be detected until later in life
- Can be an incidental finding
Radiology description
- Xray: homogenous opacity in the lung base; may have air fluid levels (AJR Am J Roentgenol 2000;175:1005)
- Ultrasound: homogenous, echogenic solid mass with an aberrant systemic artery (J Ultrasound Med 2018;37:371)
- CT: solid mass with emphysematous changes at the margins; may or may not have associated cystic changes and air fluid levels
Radiology images
Images hosted on other servers:

Xray

Ultrasound

CT scan
Prognostic factors
- Intralobar sequestrations are prone to repeat infections (Eur J Cardiothorac Surg 1999;15:11, Eur J Cardiothorac Surg 2001;19:388, J Pediatr Surg 2019;54:1286)
- Extralobar sequestrations may have a mass effect depending on their site and the size of the lesion
- Less likely to predispose to infection as they are distinct from the lungs
- May regress during development; thought to occur via an ischemic mechanism due to twisting of vascular pedicle
Case reports
- Fetal lung mass (Obstet Gynecol Sci 2020;63:529)
- 13 year old girl with an extralobar bronchopulmonary sequestration and associated congenital diaphragmatic hernia (J Chest Surg 2021;54:224)
- 17 year old boy with chest pain and posterior mediastinal mass (Ann Transl Med 2020;8:969)
Treatment
- Surgical resection is curative and routinely performed for symptomatic lesions
- Asymptomatic lesions are often prophylactically resected to prevent subsequent infections and respiratory symptoms (Semin Pediatr Surg 2015;24:187)
Gross description
- Intralobar bronchopulmonary sequestration (Semin Pediatr Surg 2015;24:176)
- Aberrant systemic feeding vessel is often apparent as a tied / stapled vascular margin that is distinct from the hilar structures
- Variable parenchymal findings, ranging from grossly unremarkable lung to cysts measuring up to 2.5 cm in greatest dimension
- May have a mucocele
- Extralobar bronchopulmonary sequestration (Semin Pediatr Surg 2015;24:176)
- Irregularly shaped portion of lung entirely invested by pleura with a vascular pedicle
- Variable parenchymal findings, ranging from grossly unremarkable lung to cysts measuring up to 2.5 cm in greatest dimension
- May have a mucocele
- May have prominent fine lymphatics underlying the pleural surface
Gross images
Contributed by Jennifer Pogoriler, M.D., Ph.D.

ILS with systemic vessel
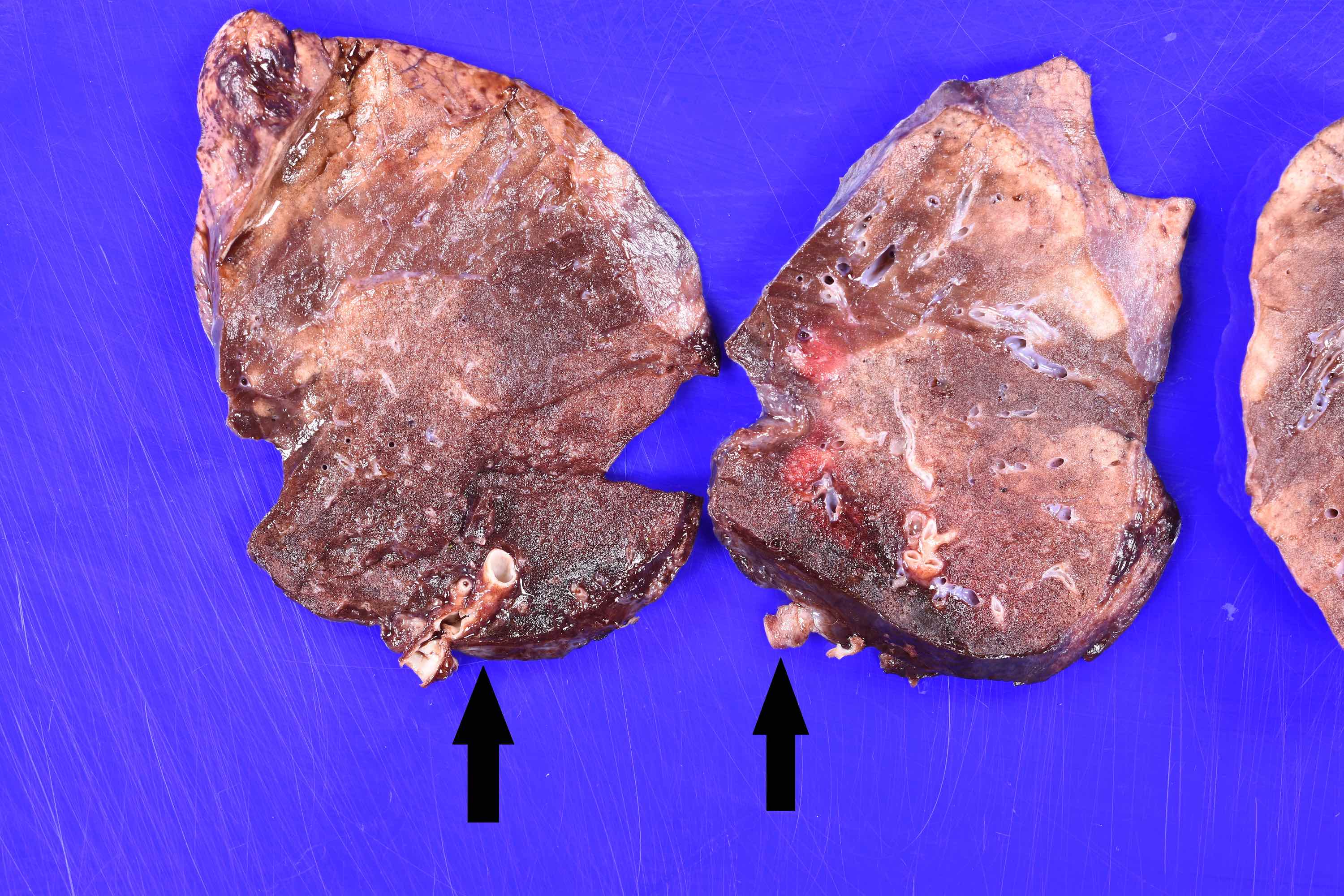
Cut surface ILS with systemic vessel
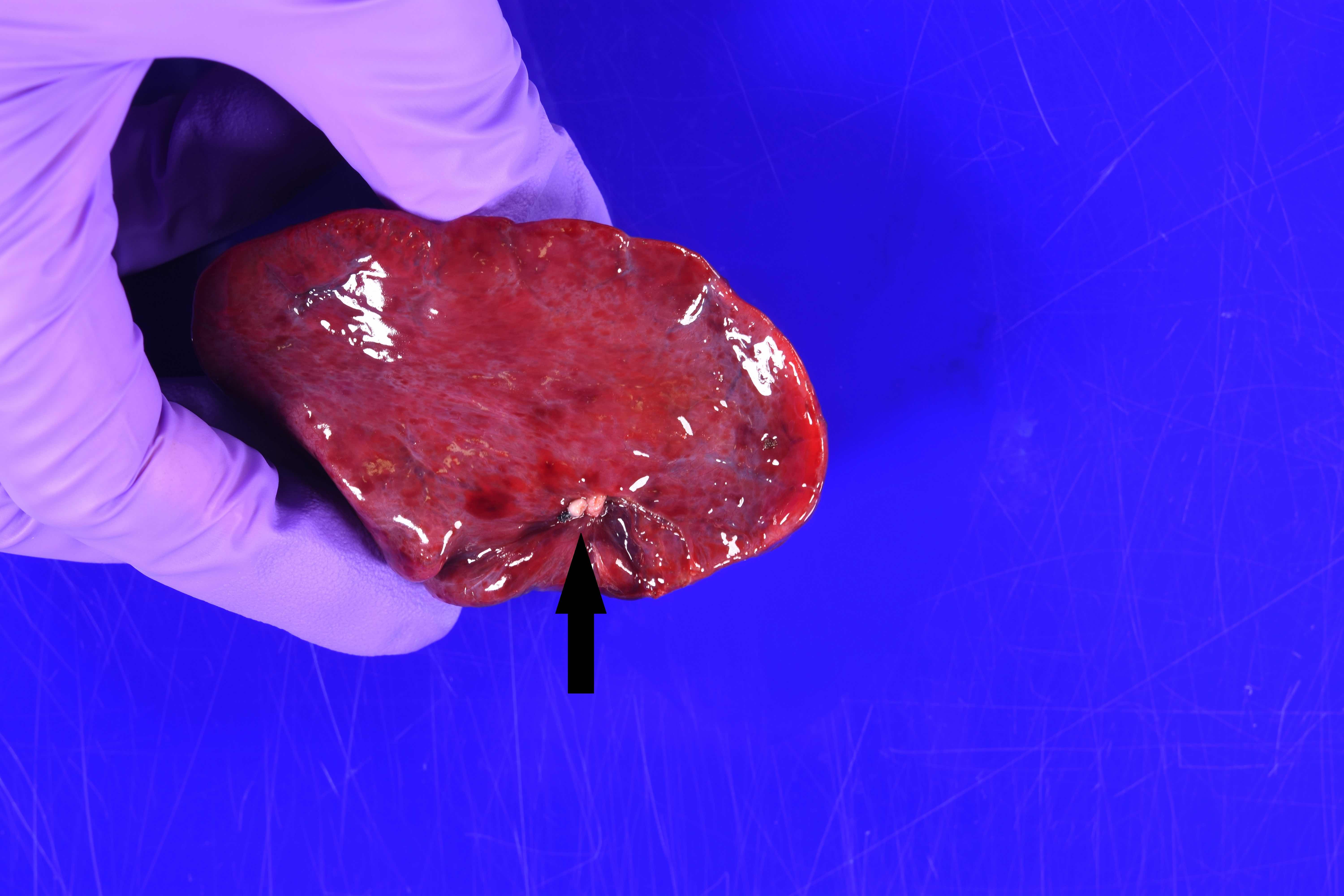
ELS and feeding vessel

Cut surface of ELS
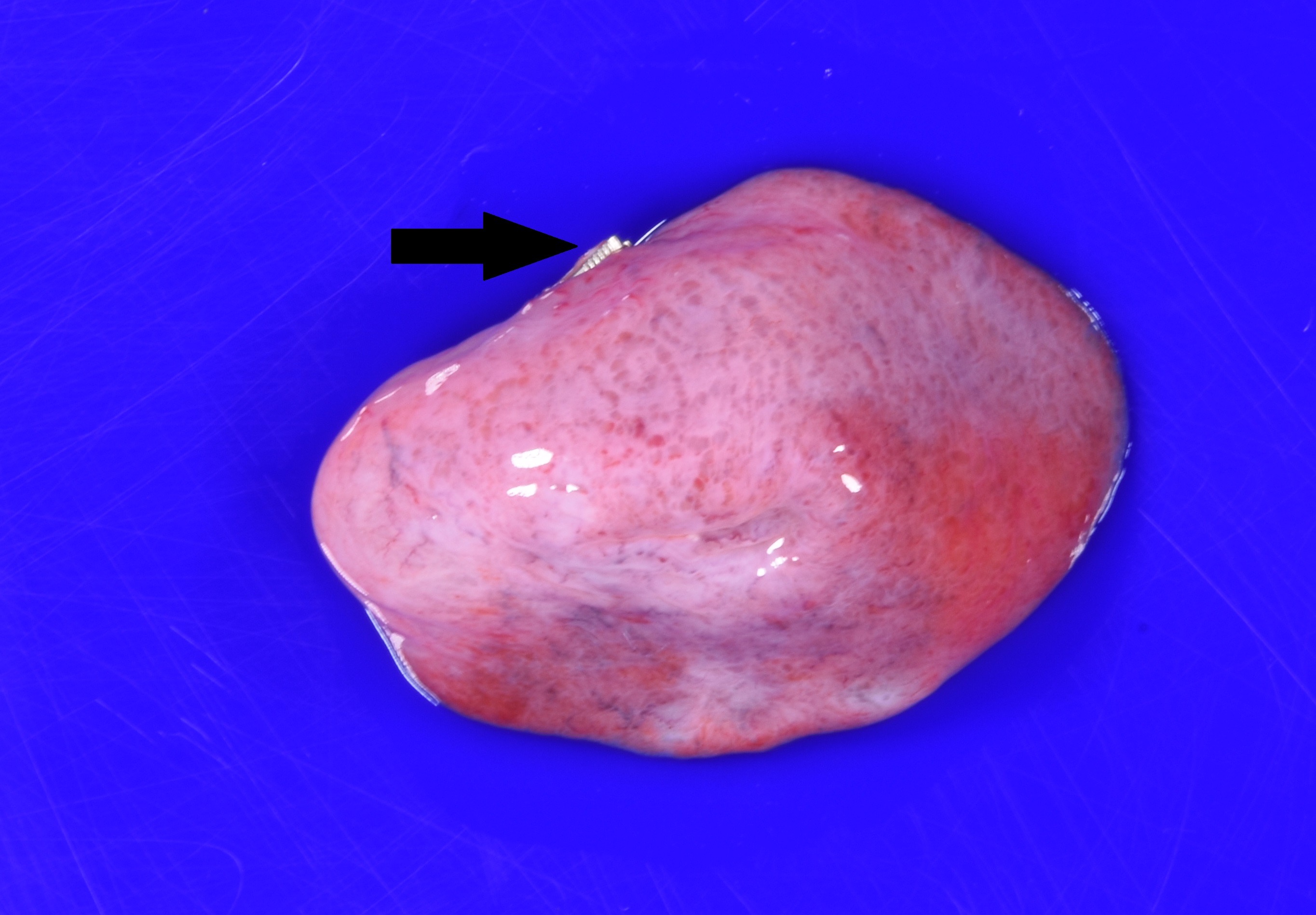
ELS with prominent lymphatics

ELS with cystic changes
Microscopic (histologic) description
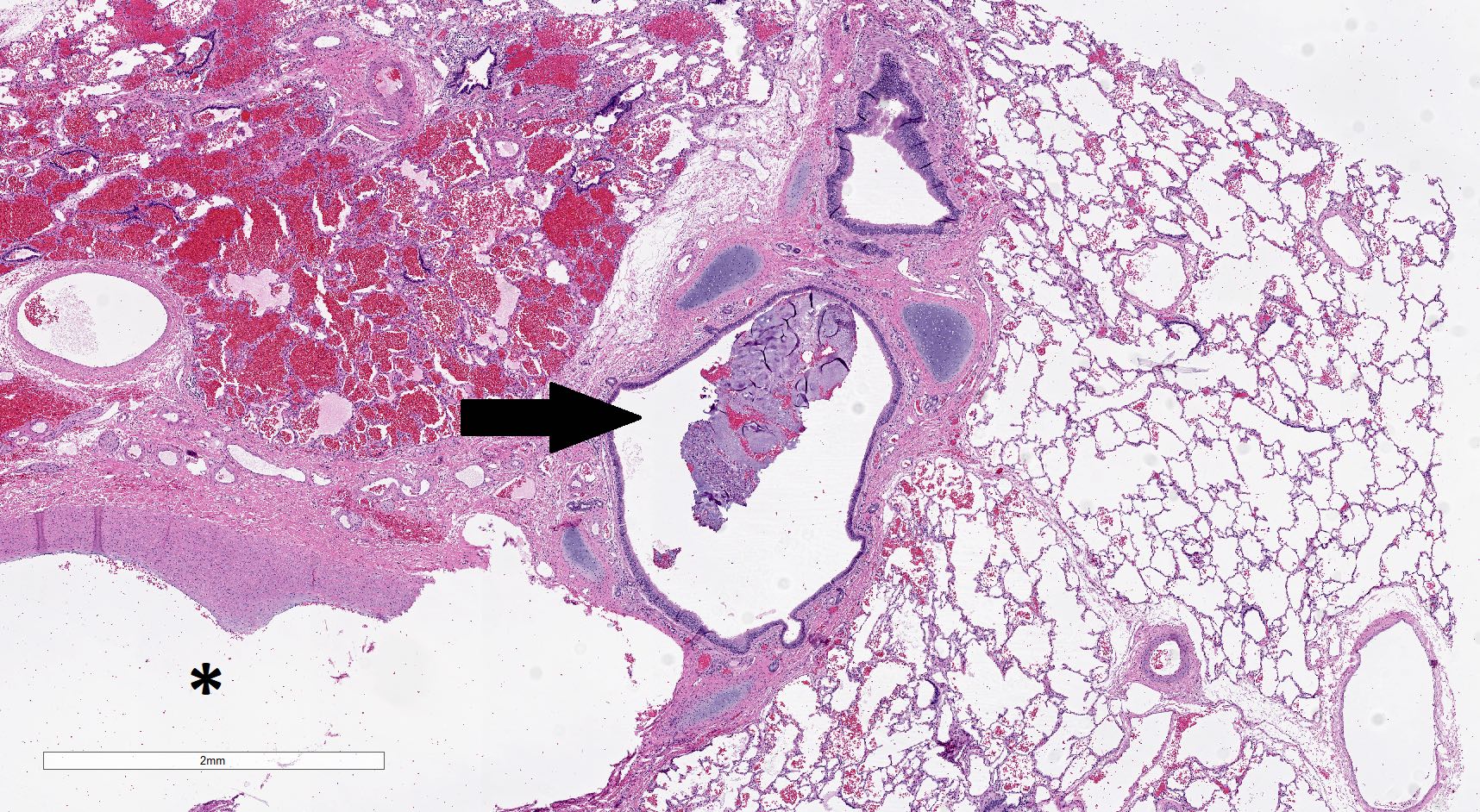
- Systemic feeding vessel is often accompanied by hilar type structures, including an airway, nerves, and lymph nodes (Pediatr Dev Pathol 2007;10:75)
- Systemic artery branches within the lesion are often somewhat thicker than normal pulmonary arteries and may show pulmonary hypertension-like changes in older patients (Histopathology 2010;57:121)
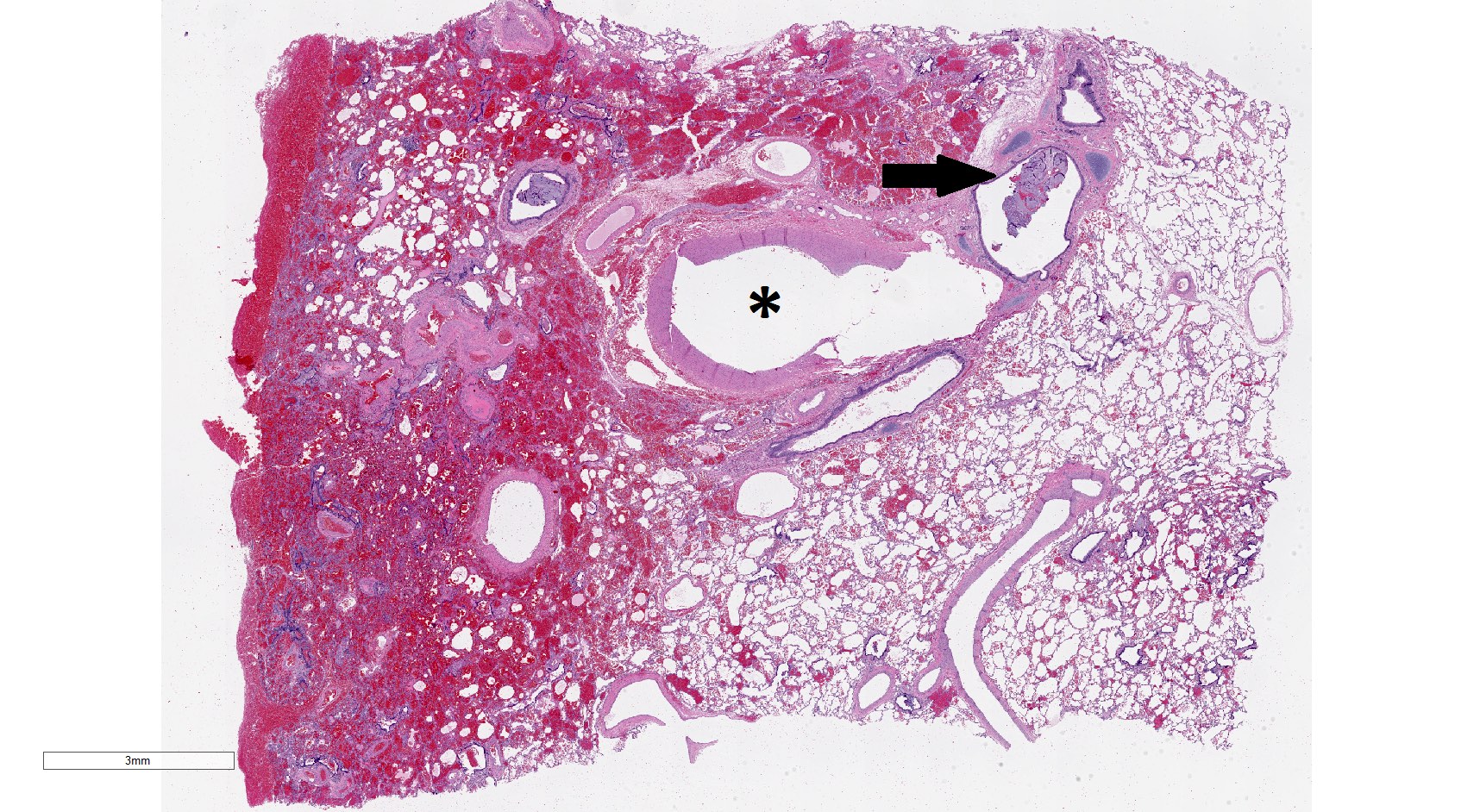
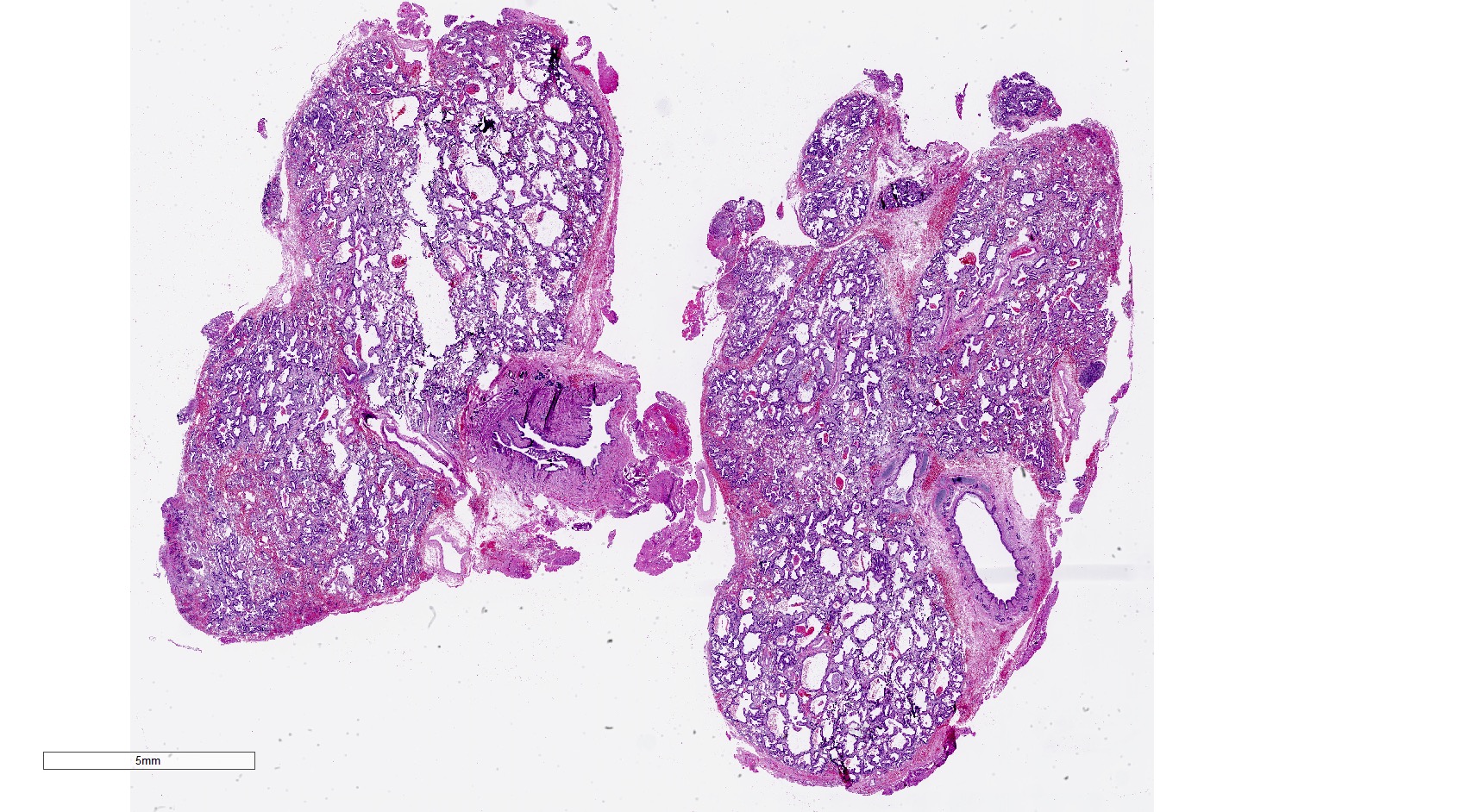
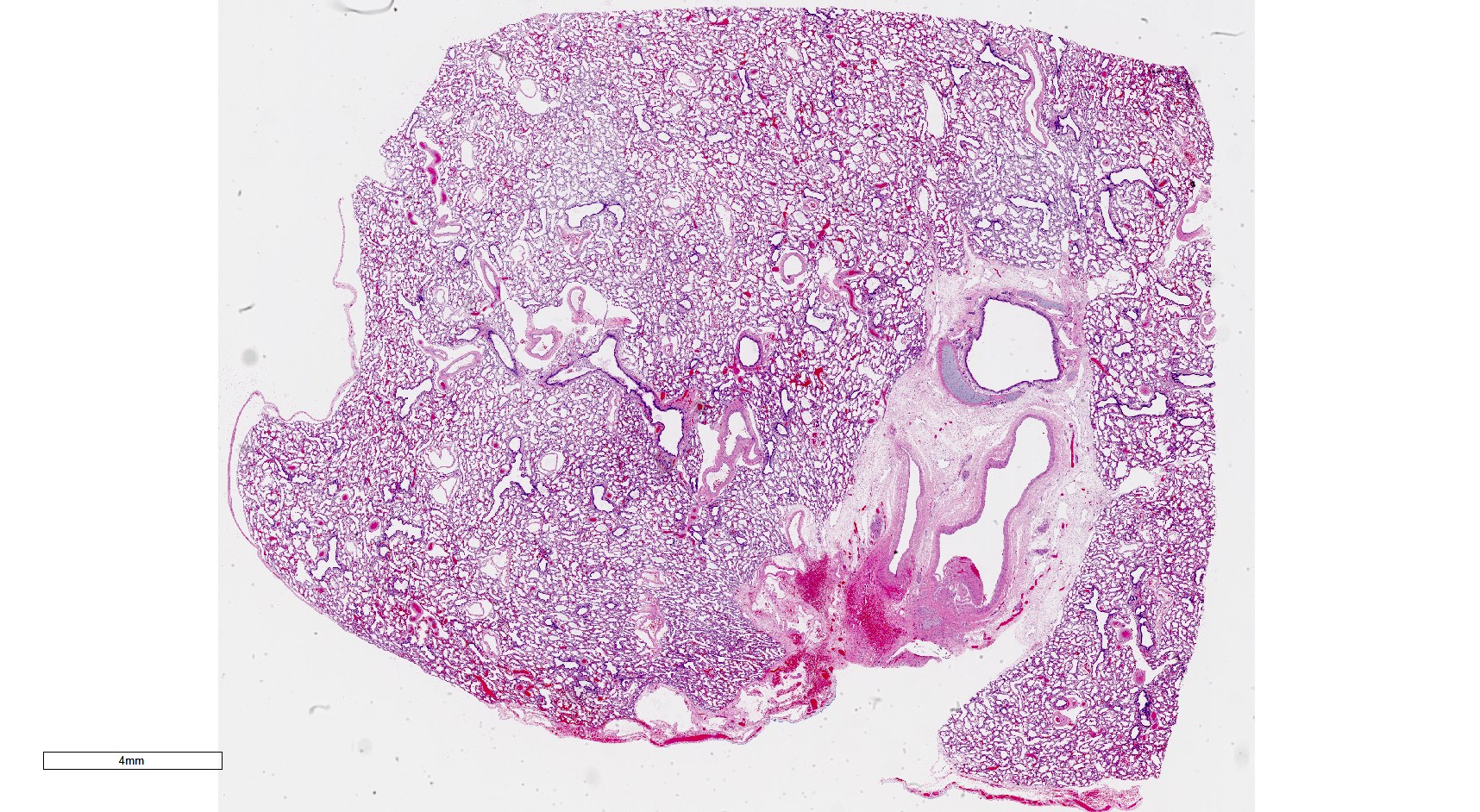
- Cases universally have at least mild parenchymal maldevelopment with enlarged and simplified alveoli
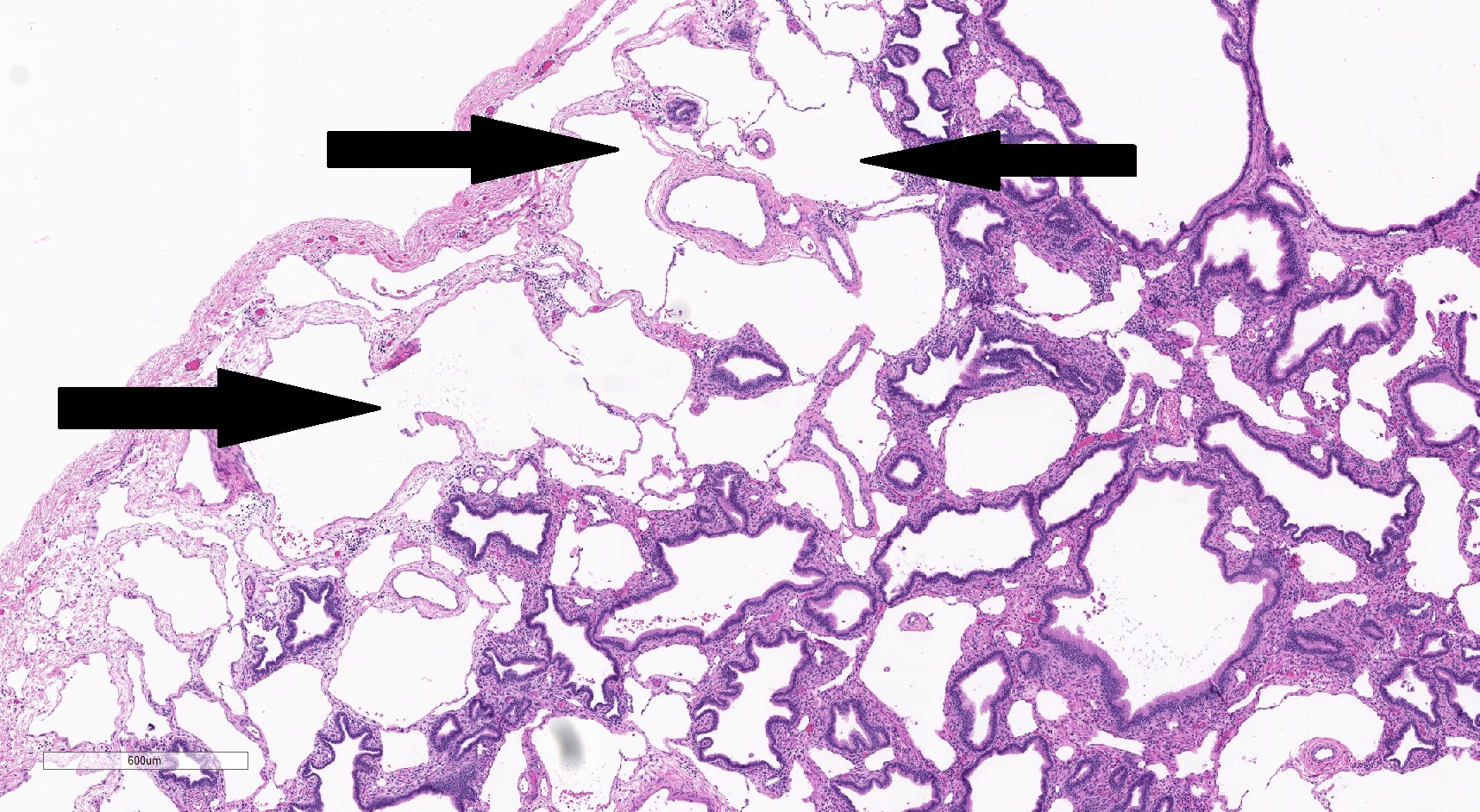
- ~50% of cases also have cystic parenchymal maldevelopment
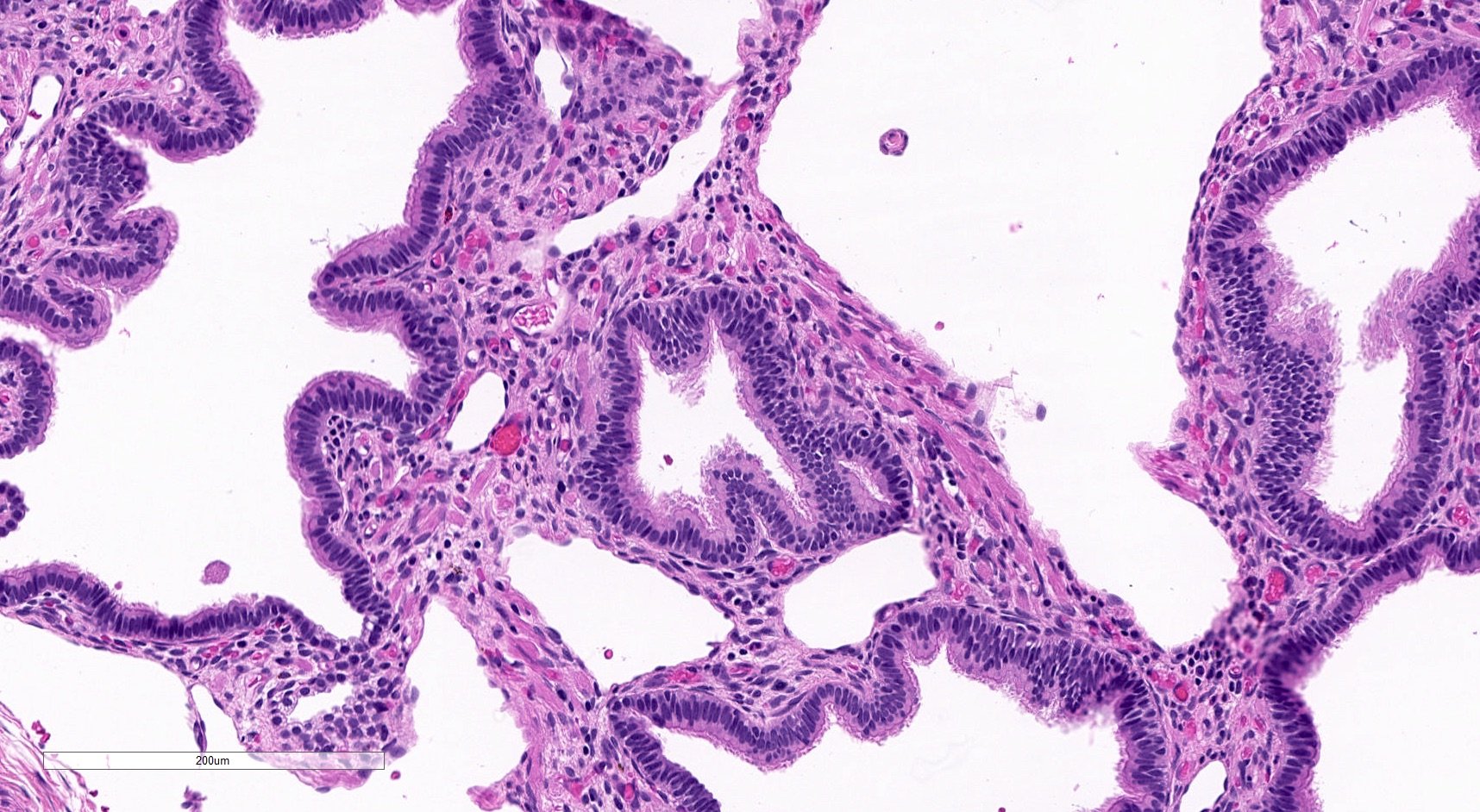
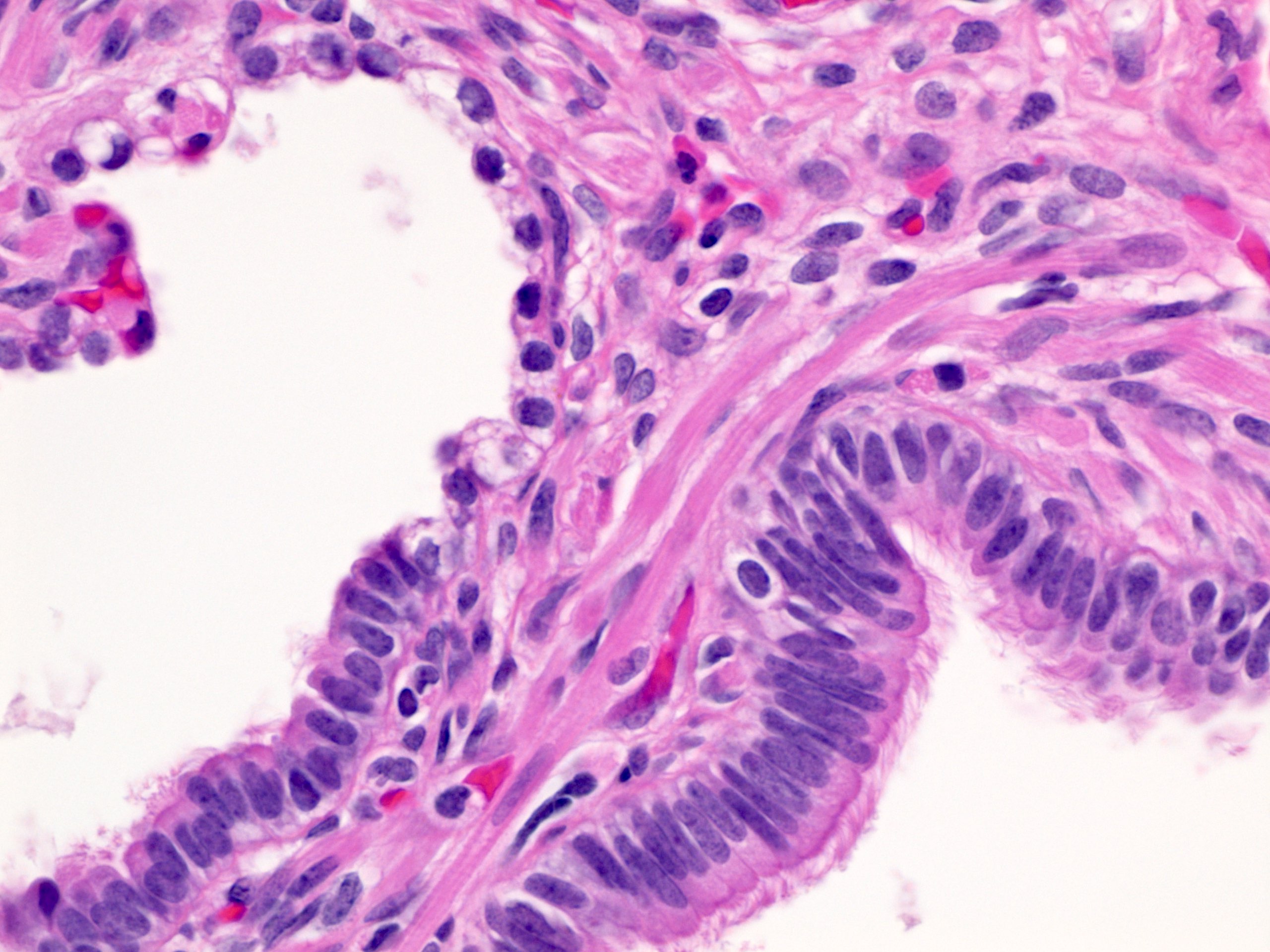
- Cysts are typically round and lined by ciliated columnar epithelium; epithelial complexity is rare
- Histologically similar to a type 2 CPAM
- Sequestrations with cystic parenchymal maldevelopment are often referred to as a hybrid lesion (Pediatr Dev Pathol 1999;2:454, J Pediatr Surg 1997;32:986)
- Often have prominent evidence of mucostasis, including pools of mucin and foamy intra-alveolar macrophages (Am J Surg Pathol 2019;43:47)
- May have foci of skeletal muscle within septa between larger cysts
- Prominent lymphangiectasia is seen in a subset of extralobar bronchopulmonary sequestrations
Microscopic (histologic) images
Contributed by Jennifer Pogoriler, M.D., Ph.D.
ILS aberrant hilum
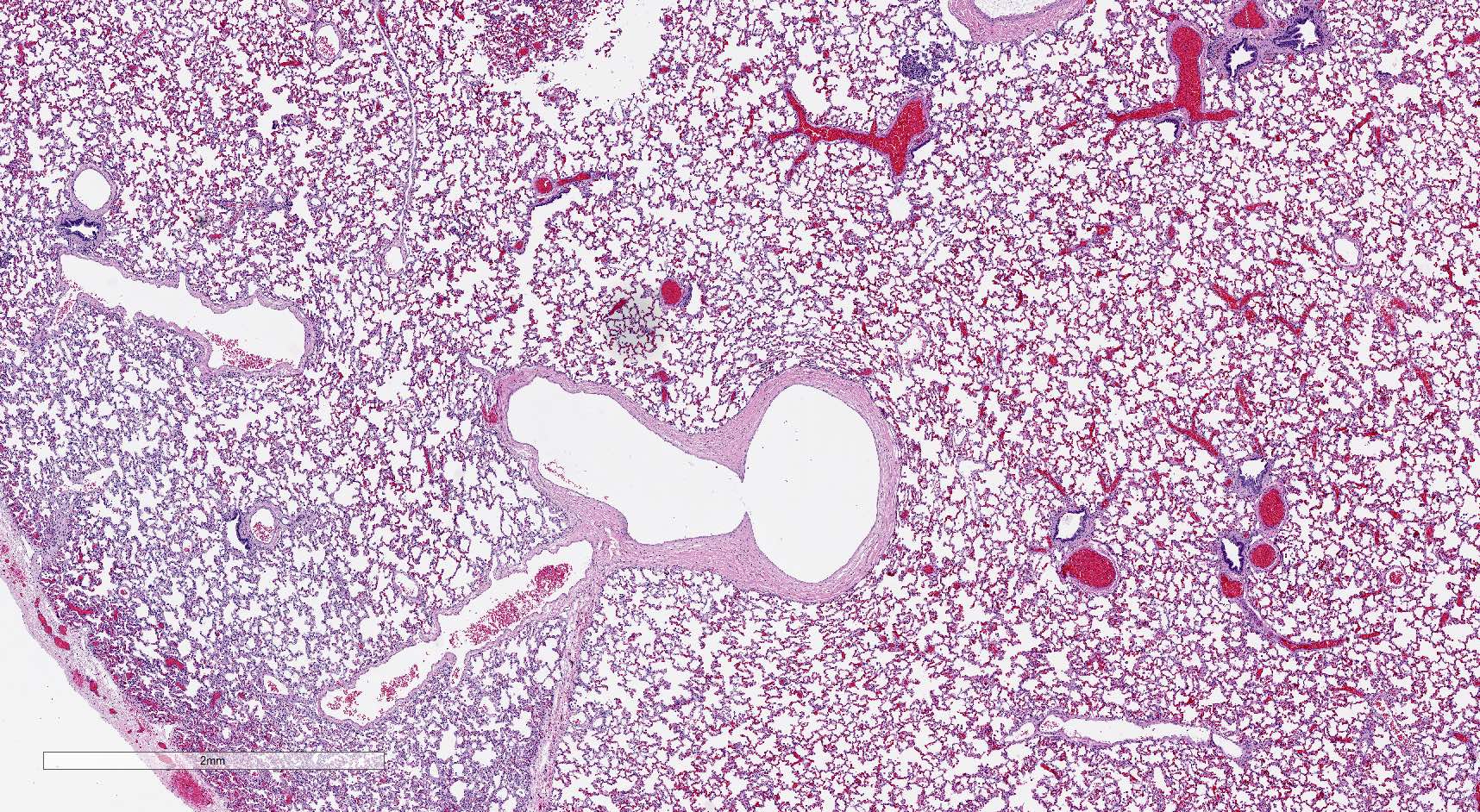
Normal lung adjacent to ILS
ILS with parenchymal maldevelopment
Cystic changes in ELS
ELS with prominent lymphangiectasia
Skeletal muscle in septa
High power skeletal muscle
Sample pathology report
- Lung, left lower lobe, lobectomy:
- Intralobar bronchopulmonary sequestration with associated cystic parenchymal maldevelopment (see comment)
- Comment: These features have been referred to as hybrid lesion.
Differential diagnosis
- Type 1 CPAM:
- No systemic feeding vessel or aberrant hilum
- Gross: readily identifiable cysts
- Variably sized cystic spaces with epithelial complexity
- Mucinous cell clusters seen in ~75%
- Mucostasis is rare
- Type 2 CPAM:
- No systemic feeding vessel or aberrant hilum
- Morcellated specimens may require correlation with operative note
- Gross: may have cysts measuring up to 2.5 cm
- Spectrum of histologic changes from mild parenchymal maldevelopment to simple round cystic spaces, similar to bronchopulmonary sequestrations
- Prominent mucostasis
- No systemic feeding vessel or aberrant hilum
- Intrapulmonary bronchogenic cyst:
- No systemic feeding vessel or aberrant hilum
- Gross: single, thick walled cyst
- May also have cystic changes in the adjacent parenchyma
Board review style question #1
Diagnosis of a bronchopulmonary sequestration requires which of the following?
- Cystic parenchymal changes
- Epithelial complexity
- Prominent lymphangiectasia
- Systemic feeding vessel
Board review style answer #1
D. Systemic feeding vessel. A sequestration should be sequestered from both the normal pulmonary arterial circulation as well as from the tracheobronchial tree. Although the parenchyma is maldeveloped, frank cystic change is seen only in a subset of cases. Epithelial complexity is rarely seen. This is a feature more typical of type 1 congenital pulmonary airway malformation. Lymphangiectasia may be present in a subset of extralobar sequestrations but is not a required feature.
Comment Here
Reference: Sequestrations
Comment Here
Reference: Sequestrations
Board review style question #2
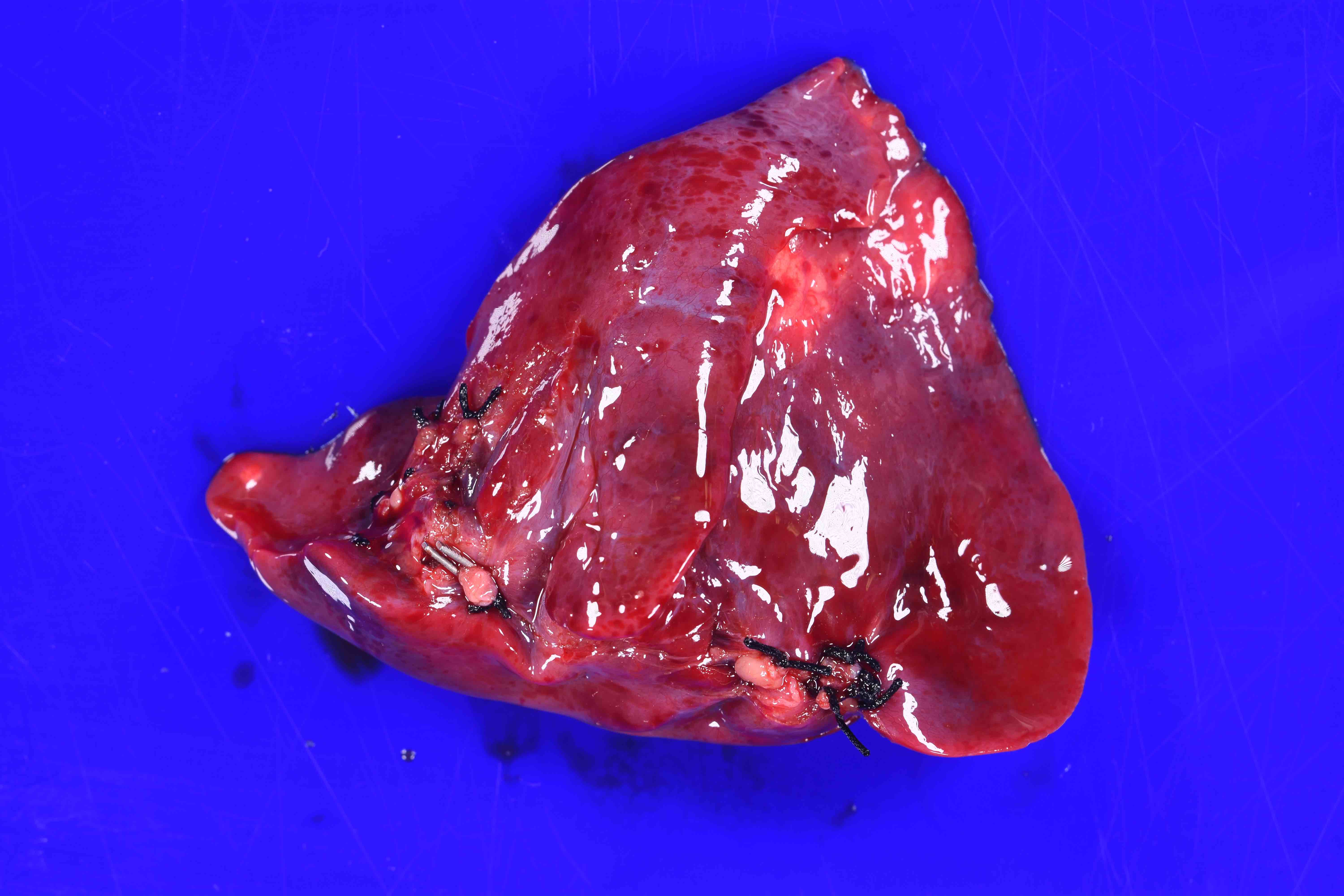
Gross examination of the lobectomy specimen shown above reveals a sutured vessel along the periphery of the lobe that is distinct from the hilum. What is the best diagnosis?
- Bronchogenic cyst
- Extralobar bronchopulmonary sequestration
- Intralobar bronchopulmonary sequestration
- Type 2 congenital pulmonary airway malformation
- Type 3 congenital pulmonary airway malformation
Board review style answer #2
C. Intralobar bronchopulmonary sequestration. This image shows a systemic feeding vessel associated with a lower lobe (note diaphragmatic surface). This is an intralobar sequestration. An extralobar sequestration does not share pleura with the normal lung. Congenital pulmonary airway malformations and intrapulmonary bronchogenic cysts do not have a systemic feeding vessel.
Comment Here
Reference: Sequestrations
Comment Here
Reference: Sequestrations

