Lung
Infectious
Viral
Adenovirus
Author: Elliot Weisenberg, M.D.

Last author update: 1 August 2011
Last staff update: 21 July 2020
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed search: adenovirus pneumonia lungs

Table of Contents
Definition / general | Epidemiology | Sites | Clinical features | Prognostic factors | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Weisenberg E. Adenovirus. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumoradenovirus.html. Accessed April 2nd, 2025.
Definition / general
- Lung disease caused by infection with adenovirus, a nonenveloped, lytic, double stranded DNA virus
Epidemiology
- At least 51 serotypes of adenovirus have been associated with clinical syndromes; not well understood why specific sterotypes are associated with specific syndromes, but differences in mode of transmission and virus tropism are likely to play a role
- Seven species are known (groups A - G); respiratory disease is caused by groups C, E and some members of group B
- Infection is ubiquitous; most individuals have had several infections during childhood
Sites
- In addition to lung, also occurs in the upper respiratory tract (tonsils, adenoids), liver, GI tract, CNS, heart, kidneys, urinary bladder, ear, eyes
Clinical features
- Half of infections are subclinical
- Represent 5% - 10% of febrile illness in infants and young children
- Transmission is through respiratory droplets, fomites, or fecal-oral
- In children, causes 5% of upper respiratory tract infections and 10% of cases of pneumonia; adult infection is less common
- Can persist as a latent infection for years after primary disease; tonsils and adenoids are likely reservoirs
- Outbreaks among military recruits have caused epidemics of serious disease at military training centers
- Certain subgroups are associated with severe pneumonia, especially young children
- Virulent strains have led to fatalities in previously healthy young adults (Clin Infect Dis 2003;37:e142)
- Serious disease has occurred in immunocompromised hosts, especially patients with solid organ and hematopoietic stem cell transplants, although infection may be associated only with asymptomatic shedding
- Adenovirus infections are only rare causes of significant disease in AIDS patients
- When symptomatic, upper respiratory tract infection causes fever, sore throat, cough, hoarseness, rhinorrhea
- Disease may mimic tonsillitis with group A streptococcal infection, due to exudative pharyngitis and enlarged cervical lymph nodes
- Otitis media may occur children under age 1 year
- Upper respiratory tract infection may progress to involve lower respiratory tract with cough and shortness of breath; often with systemic symptoms of fever, headache, myalgias; abdominal pain may occur
- May cause a pertussis-like syndrome
- Chest Xray: bilateral, patchy, ground glass opacities consistent with viral pneumonia
- In hematopoietic stem cell transplants, the GI tract is more commonly affected than lungs; cold agglutinins are present in 20% of patients with adenovirus pneumonia
- In solid organ transplants, usually the transplanted organ affected is by adenovirus
- In lung transplant patients, disease usually occurs in early post-transplant period and is associated with graft failure, bronchiolitis obliterans, and often death
- Disease in transplant patients may be due to primary infection or reactivation
- Diagnosis: rountine tissue culture, PCR, serology, or antigen specific assays; in tissue samples, use immunostains
Prognostic factors
- In transplant patients, increasing viral load by PCR and greater immunosuppression increases the risk of serious disease
- Other risk factors are young patient age, graft vs. host disease, unrelated stem cell donor, T cell depletion of graft, cord stem cell transplant, low T cell counts post transplant, total body irradiation, use of antilymphocyte antibodies
Treatment
- Only supportive care is known to be effective
- Some studies have shown benefit of ribavirin therapy, but this is not universal
- Immunotherapy is being investigated
- Appropriate hand hygiene can reduce transmission
- In the United States, military recruits formerly received vaccinations against some strains of adenovirus; production of this vaccine stopped, however, efforts to resume production are ongoing
Microscopic (histologic) description
- Epithelial cells contain smudged nuclei with brick-like, intranuclear inclusions; start as small, eosinophilic inclusions, then briefly appear as basophilic inclusions with a thin halo; then enlarge to obscure the nuclear membrane to take on the typical smudgy appearance
- Two patterns of disease are commonly encountered that may occur concurrently: diffuse alveolar damage like pattern with interstitial edema, mononuclear cell infiltrates and exudative fluid accumulation in alveoli with hyaline membranes; second pattern is necrosis of bronchi, bronchioles, and alveoli with neutrophilic and histiocytic infiltrates, with interstitial fibrosis and obliterative bronchiolitis as potential sequelae
Microscopic (histologic) images
Contributed by Elliot Weisenberg, M.D.
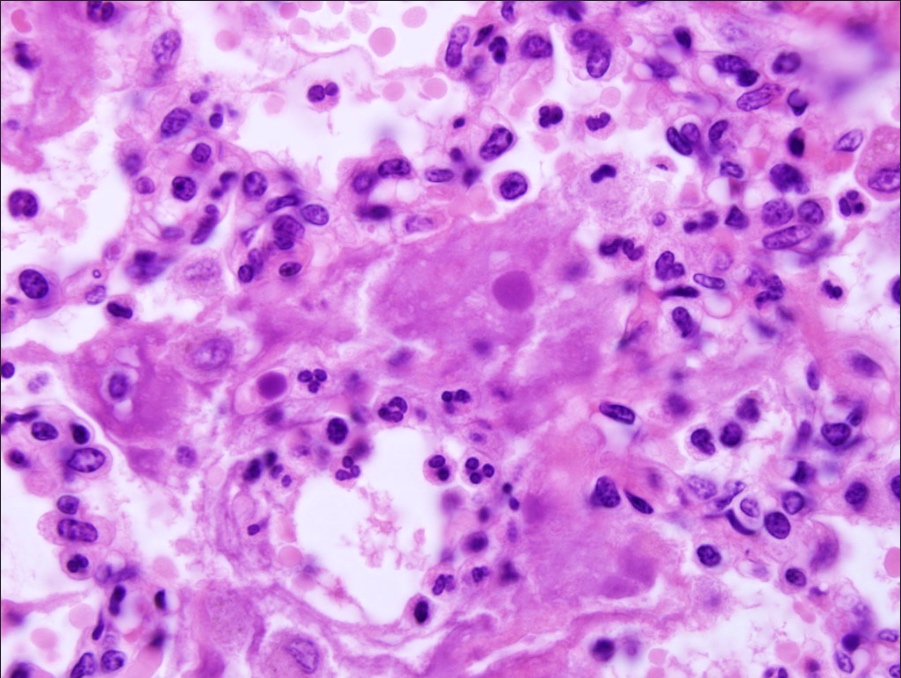
Adenovirus inclusions
in lung from an infant
chimpanzee
Images hosted on other servers:

Interstitial inflammation (no inclusions identifiable)

Various images
Positive stains
- Adenovirus immunohistochemistry
Electron microscopy description
- 60 - 90 nm, icosahedral particles in crystalline array
Differential diagnosis
- The diagnosis can be made by rountine tissue culture, PCR, serology, or antigen specific assays
- In tissue samples, immunohistochemistry can confirm the diagnosis
Additional references
