
Liver & intrahepatic bile ducts
Benign / nonneoplastic
Segmental atrophy
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 15 March 2022
Last staff update: 15 March 2022
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Segmental atrophy liver[TI]


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Daniels E, Assarzadegan N. Segmental atrophy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorsegmentalatrophy.html. Accessed April 2nd, 2025.
Definition / general
- Rare, underrecognized benign entity, which can present as a mass lesion (pseudotumor)
- Typical features of segmental atrophy include loss of hepatic parenchyma, mild inflammation, abnormal vessels, bile ductular proliferation, biliary retention cysts and early fibrotic and elastotic changes
Essential features
- Unifocal, benign mass lesion
- Pathophysiology involves a possible vascular injury and ischemia with subsequent elastin remodeling by liver myofibroblasts
- Histologically, the lesions display extinction of hepatocytes with elastin deposition, thick walled blood vessels and biliary duct cystic changes
Terminology
- Nodular elastosis of the liver
- Hepatic segmental atrophy
- Hepatic pseudotumor
ICD coding
Epidemiology
- Variable age range (3 - 91 years old) with the majority presenting in the fifth to sixth decades of life
- Female predominance
- Seen in association with cardiovascular disease and connective tissue disorders
- Reference: USCAP: Abstracts - Liver Pathology [Accessed 20 January 2022]
Sites
- Liver; usually subcapsular but can involve any part of the liver parenchyma
- No predilection for specific lobes or segments
Pathophysiology
- Elastic fibers composed of elastin and microfibrils are present in portal tracts, walls of large vessels and central veins in the normal liver
- Ischemic injury to the liver results in disorganized, excessive elastin deposition by hepatic myofibroblasts, chronic inflammation and vascular fibrosis
- Damaged bile ducts can leak bile into surrounding parenchyma causing further damage with fibrotic change
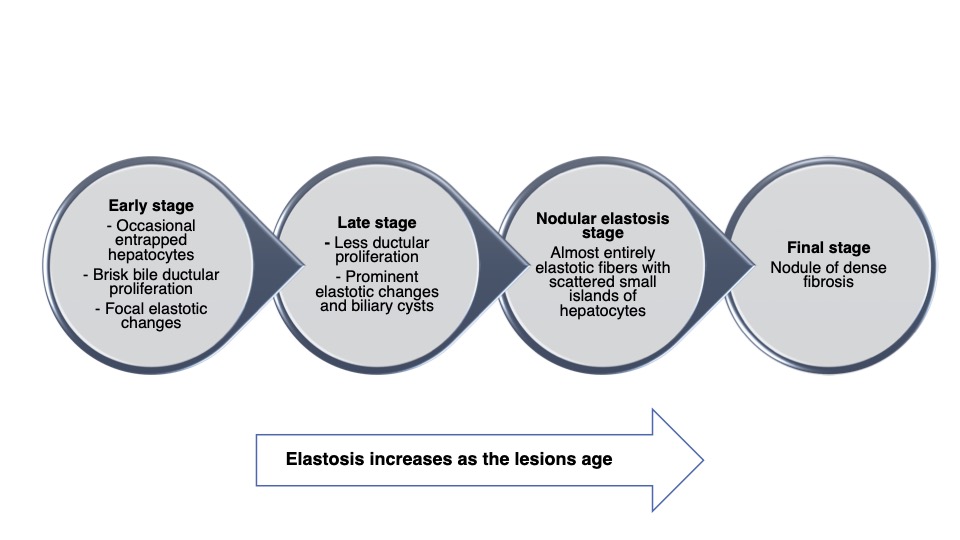
- Occurs in a stepwise fashion, with progressive elastosis and eventual fibrosis in the final stages (see Diagrams / tables and Microscopic [histologic] description) (Am J Surg Pathol 2011;35:364)
Etiology
- Not precisely known
- Possible vascular injury and subsequent ischemia leading to parenchymal extinction (Am J Surg Pathol 2011;35:364)
Clinical features
- Can present with right upper quadrant pain, ascites or a palpable abdominal mass or it may be discovered incidentally in an asymptomatic patient
Diagnosis
- Imaging, such as ultrasound, CT or MRI
- Requires tissue confirmation due to similar radiographic appearance to many malignant lesions
Laboratory
- No specific diagnostic laboratory tests
- Liver transaminases and bilirubin studies are usually within normal limits
- Alpha fetoprotein levels are not elevated (as seen with hepatocellular carcinoma)
Radiology description
- Iso or hypoechoic on ultrasound with ill defined margins and no Doppler flow
- Can resemble malignant neoplasm
- Well circumscribed, hypodense, noncontrast enhancing mass on CT
- May be partially calcified
- Hypointense on T1 weighted MRI due to edema, arterioportal shunting and fibrosis
- Iso to hyperintense on T2 weighted MRI and diffusion weighted images (DWI)
- May be hyperdense if adjacent to fatty changes of the liver
- Isometabolic to background hepatic parenchyma on PET / CT
- PET / CT or serial imaging can be used to help differentiate from malignant process
- Reference: Abdom Radiol (NY) 2017;42:2447
Radiology images
Contributed by Naziheh Assarzadegan, M.D.
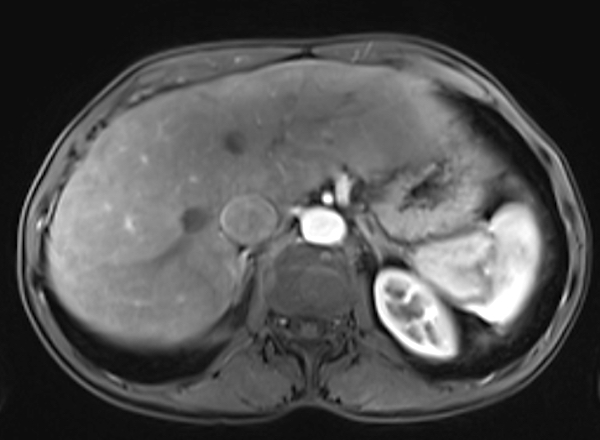
Mass,
concerning for
cholangiocarcinoma
Prognostic factors
- Benign condition with favorable prognosis
Case reports
- 4 year old girl with a 2 year history of abdominal pain (S Afr J Child Health 2019;13:100)
- 45 year old woman with incidental liver lesion on routine ultrasound (Surgery 2015;157:826)
- 73 year old man with an unusual whitish nodule found during laparoscopy (Dig Dis Sci 2014;59:3122)
- 73 year old man who had a questionable liver lesion in the setting of pancreatic adenocarcinoma (Dig Dis Sci 2014;59:3122)
- 74 year old man with a suspected cholangiocarcinoma (Dig Dis Sci 2014;59:3122)
Treatment
- Complete excision of the lesion
Gross description
- Often presents as a unifocal, yellow-white, ill defined or well circumscribed mass that can involve any part of the liver
- Varies in size (1.8 - 10.0 cm) and is typically subcapsular
- Cut surface is ill defined and variegated with tan-white coloration and areas of hemorrhage (Dig Dis Sci 2014;59:3122)
- Can have a nodular appearance in later stages due to dense elastosis and fibrosis
- May have grossly apparent biliary duct dilation with bile duct cysts, resembling a biliary cystic neoplasm
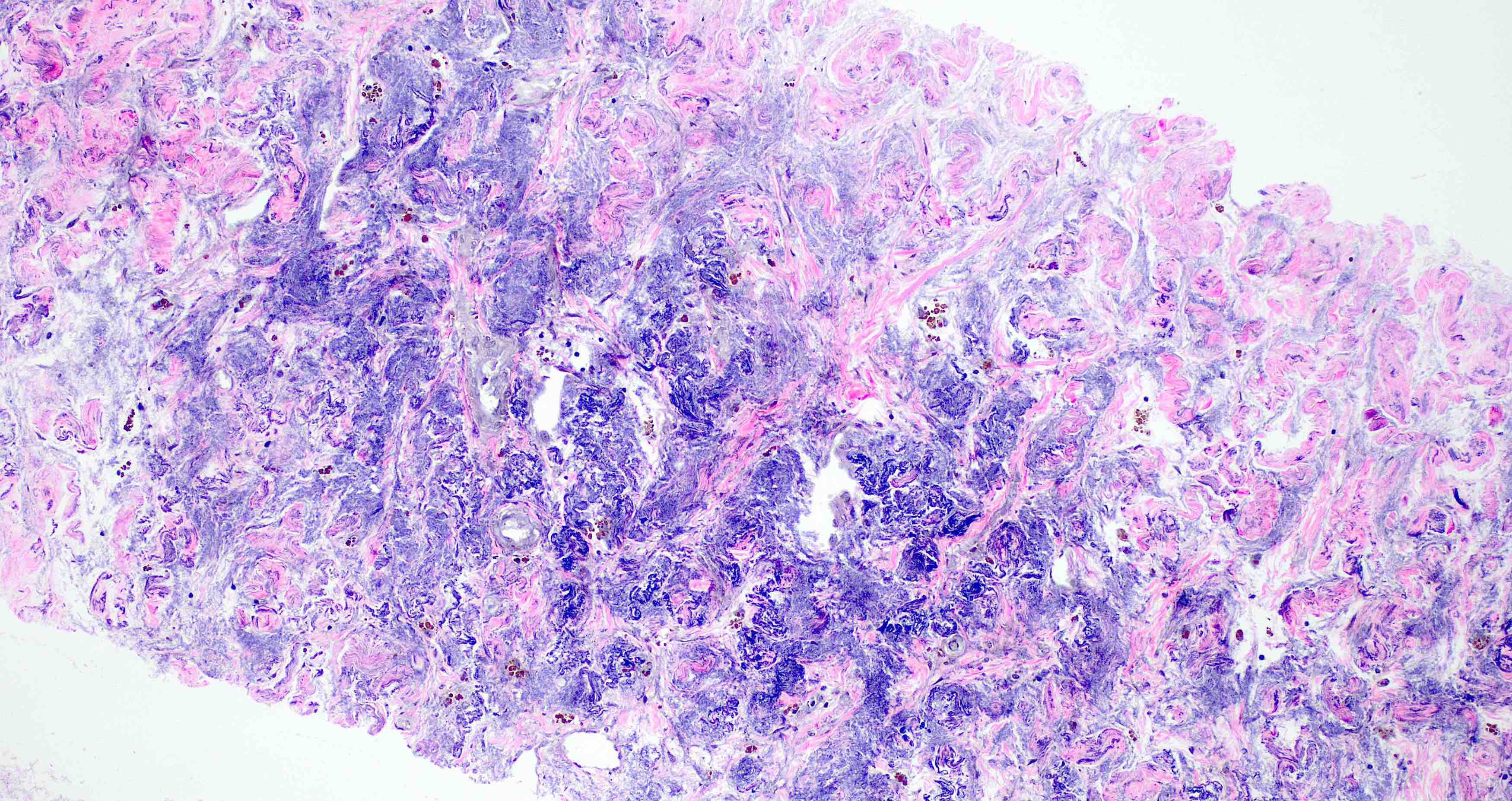
Microscopic (histologic) description
- Demonstrates a spectrum of elastotic change (Am J Surg Pathol 2011;35:364):
- Early stage:
- Collapsed hepatic parenchyma with islands of residual hepatocytes
- Chronic inflammation
- Prominent bile duct proliferation
- Mild elastosis
- Stage 2:
- Decreased inflammation compared to early stage
- Little to no ductular proliferation
- Varying degrees of elastosis
- Stage 3:
- Nodular elastosis with marked elastin deposition
- Entrapped portal tracts and central veins
- Mild cellularity with small bland cells
- No atypia or mitoses
- Stage 4:
- Nodular elastosis with dense fibrosis
- Small, scattered islands of hepatocytes
- Residual portal tracts
- Variably sized biliary cysts usually at the edges of the lesion
- Thick walled, thrombosed vessels with fibrotic change and recanalization
- Early stage:
- Involves only a few hepatic lobules; does not usually involve entire segments
Microscopic (histologic) images
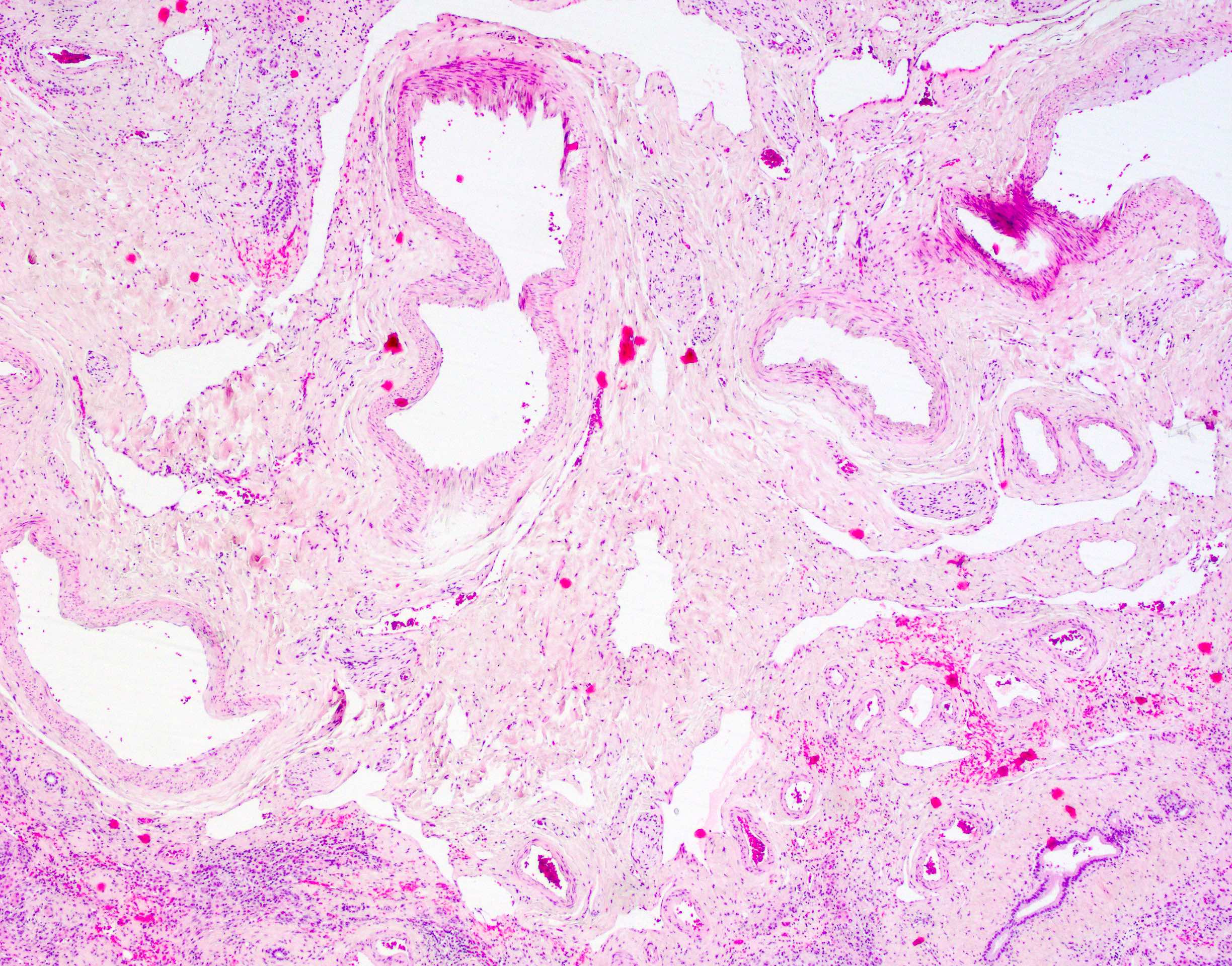
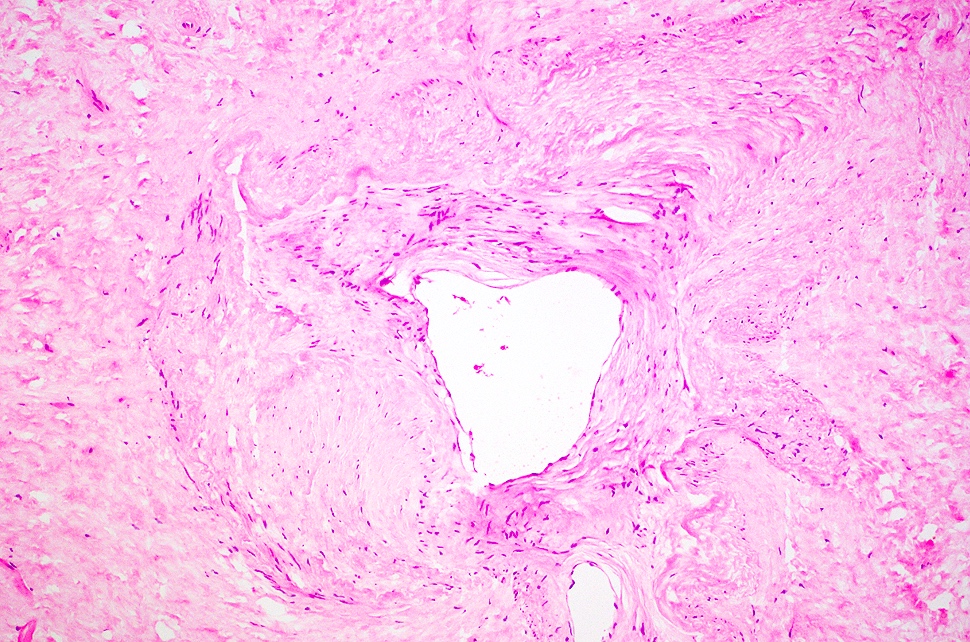
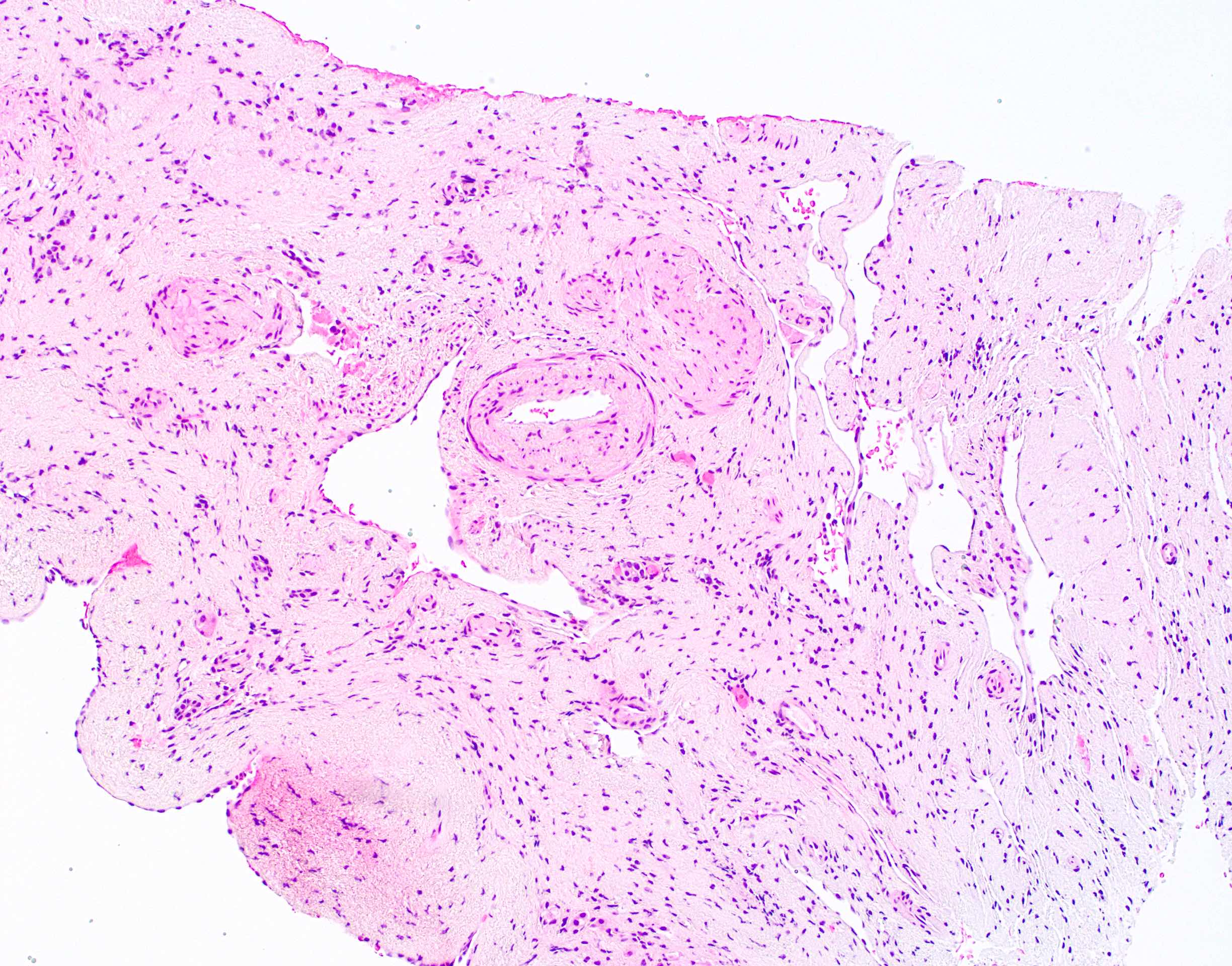
Contributed by Naziheh Assarzadegan, M.D.
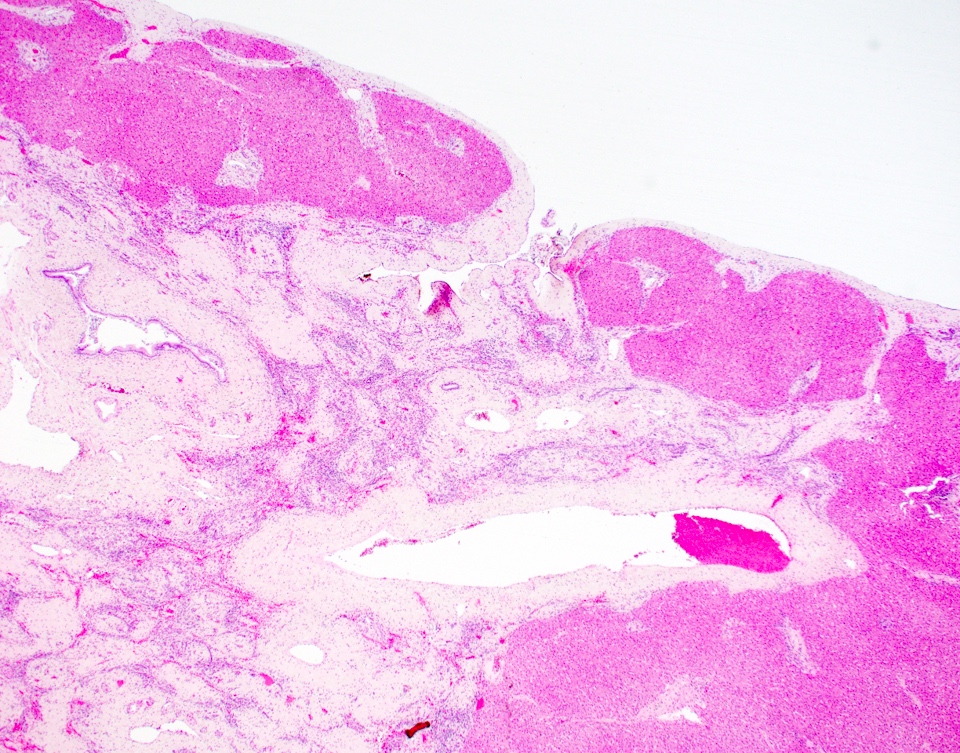
Subcapsular lesion
Abnormal thick walled blood vessels
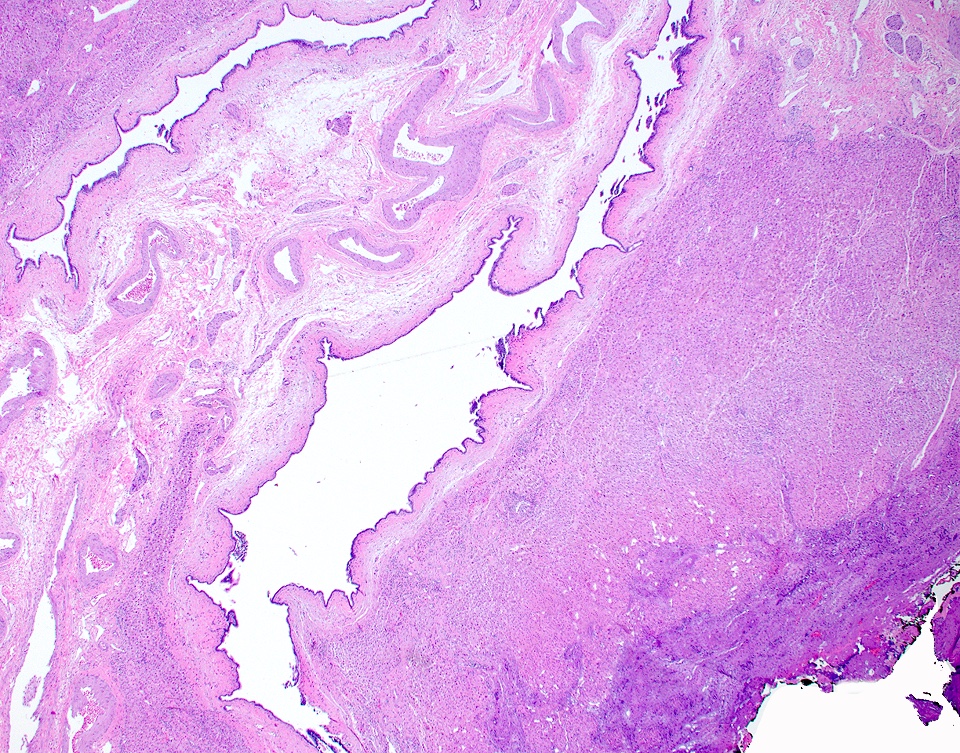

Biliary cyst
Positive stains
- Verhoeff van-Gieson: stains elastin fibers black; identifies presence and extent of elastin deposition
- Reticulin: highlights reticular fibers
- Movat pentachrome: stains diffuse elastic fibers black and intersecting reticular fibers yellow
- Reference: Am J Surg Pathol 2011;35:364
Negative stains
- Congo red: positive in amyloidosis
Sample pathology report
- Liver, wedge biopsy:
- Segmental atrophy of the liver; no malignancy identified (see comment)
- Comment: The patient's history of a 5.9 cm partially exophytic, solid lesion in the right hepatic dome is noted. The lesion shows predominant sclerosis with abnormal thick walled blood vessels, entrapped hepatocytes and focal bile ductular proliferation at the periphery of the lesion. The elastic stains show focal dense network of elastic fibers in the stroma of the lesional tissue. The features taken together, including the degree of elastosis and presence of other salient features of segmental atrophy (abnormal thick walled blood vessels and focal bile ductular proliferation), are part of a spectrum of histologic features described in later stages of segmental atrophy (Am J Surg Pathol 2011;35:364).
Differential diagnosis
- Simple hepatic cyst or solitary bile duct cyst:
- Usually diffuse and is associated with renal cysts
- Regenerative hepatic pseudotumor (RHP) (Hum Pathol 2020;99:43)
- Recently described pseudotumor
- Caused by vascular flow changes
- Reactive parenchyma changes, sinusoidal dilatation, vascular thrombosis, patchy bile ductular proliferation and portal vein abnormalities
- Elastosis is absent or only focally present
- Mucinous cystic neoplasm:
- Ovarian type stroma
- Intraductal papillary neoplasm of the bile duct (IPNB):
- Papillary projections with complex tubulovillous or micropapillary architecture
- Caroli disease (pediatric):
- Segmental (saccular) dilatation of large intrahepatic bile ducts
- Most commonly involves the left lobe
- Typically associated with congenital hepatic fibrosis
- Dilated ducts without abnormal vessels
- Amyloid deposition:
- Amyloid will demonstrate apple green birefringence with Congo red stain
- Epithelioid hemangioendothelioma:
- Resembles nodular elastosis due to amphophilic tumor matrix and similar cellularity
- Nuclear pleomorphism and mitosis present (will not see in nodular elastosis)
- Hepatic sclerosing cavernous hemangioma (Histopathology 2019;75:876):
- Less elastin deposition
- Greater density of vasculature with thin walled vessels (CD34 staining can be helpful in highlighting the vessels)
- Cancer associated elastosis:
- Can see elastosis associated with cholangiocarcinoma or metastatic carcinoma
- Would see glands; segmental atrophy does not have a significant glandular component
Board review style question #1
A 45 year old woman with history of diabetes and hypertension presents with abdominal pain and a 4.5 cm mass in the right lobe of the liver. The mass is biopsied and shows the above. What is the best diagnosis?
- Amyloidosis
- Benign biliary cyst
- Sclerosed hemangioma
- Segmental atrophy
Board review style answer #1
D. Segmental atrophy. The image shows lesional tissue composed of predominantly sclerosed parenchyma with abnormal thick walled blood vessels. Elastin stain highlights the increased elastic fibers.
Comment Here
Reference: Segmental atrophy
Comment Here
Reference: Segmental atrophy
Board review style question #2
What stain would be the most helpful in diagnosing segmental atrophy of the liver?
- CD34
- Congo red
- Elastin stain
- Trichrome
Board review style answer #2
C. Elastin stain is helpful in identifying the elastic fibers and excluding other differentials.
Comment Here
Reference: Segmental atrophy
Comment Here
Reference: Segmental atrophy
