

Liver & intrahepatic bile ducts
Hepatocellular carcinoma
HCC - scirrhous type
Editorial Board Members: Monika Vyas, M.D., Wei Chen, M.D., Ph.D.


Last author update: 20 October 2022
Last staff update: 20 October 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Scirrhous hepatocellular carcinoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Fels Elliott DR, Gill RM. HCC - scirrhous type. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorscirrhousHCC.html. Accessed January 2nd, 2025.
Definition / general
- Subtype of hepatocellular carcinoma (HCC) designated by the WHO, with abundant fibrous stroma separating nests and trabecula of tumor cells
Essential features
- Unencapsulated, often subcapsular location, may have satellite lesions
- Abundant fibrous stroma (> 50% of tumor) but lacks central scar or radiating fibrous bands
- May mimic intrahepatic cholangiocarcinoma on imaging and gross evaluation
Terminology
- Also called sclerosing variant of HCC
ICD coding
- ICD-10: C22.7 - other specified carcinomas of liver
Epidemiology
- Incidence ranges from 0.2 - 4.6% of all HCC (J Gastroenterol Hepatol 2006;21:1470)
Sites
- Liver, often subcapsular
Pathophysiology
- Molecular alterations: TSC1 / TSC2 mutations (J Hepatol 2017;67:727)
- Associated with expression of transforming growth factor beta (TGFβ), epithelial - mesenchymal transition (EMT) and stem cell / progenitor related genes (J Hepatol 2017;67:727, Hepatology 2012;55:1776)
Etiology
- Similar etiologic factors to classic HCC
- May arise in cirrhotic and noncirrhotic liver (Dig Dis Sci 2012;57:1698)
Clinical features
- No differences in patient demographics, presence of cirrhosis or serum alpha fetoprotein (AFP) levels, in comparison with classic HCC (Surg Pathol Clin 2013;6:367)
- Association with hypercalcemia and hypophosphatemia has been described (Liver 1981;1:33)
Diagnosis
- Imaging modalities for diagnosis of HCC: multiphasic computed tomography (CT) or magnetic resonance imaging (MRI)
- Tissue biopsy is indicated if imaging not diagnostic of HCC
Laboratory
- Elevation in serum alpha fetoprotein (AFP)
Radiology description
- Radiographic appearance may be similar to intrahepatic cholangiocarcinoma
- Contrast enhanced CT scan shows peripheral ring enhancement in arterial phase and delayed central enhancement in venous phase (Eur J Radiol 2009;69:123)
Radiology images
Images hosted on other servers:


CT scans
Prognostic factors
- Comparison of prognosis with classic HCC shows conflicting results (Surg Pathol Clin 2013;6:367)
- Prognostic factors for HCC: stage (TNM), single lesion versus multifocal, size, vascular invasion, portal vein thrombosis, severity of underlying liver disease (Liver Int 2009;29:502, J Surg Oncol 2018;117:644)
Case reports
- 60 year old man with cirrhosis and a 1.5 cm liver nodule (World J Gastroenterol 2009;15:2296)
- 67 year old woman with epigastric pain (Clin Gastroenterol Hepatol 2009;7:A28)
- 68 year old man with hereditary hemochromatosis (Semin Diagn Pathol 2017;34:126)
Treatment
- Surgical resection
- Radiofrequency ablation
- Transarterial chemoembolization (TACE)
- Transplantation (e.g., Milan criteria, modified by some institutions) (Nat Rev Gastroenterol Hepatol 2017;14:203)
Gross description
- Unencapsulated, gray-white, firm, lobulated mass, often with serrated border
- Often subcapsular, may have satellite nodules
- More extensive fibrosis than fibrolamellar variant; no radiating fibrous bands, no central scar
- Gross appearance may be similar to intrahepatic cholangiocarcinoma
- Reference: Surg Pathol Clin 2013;6:367
Gross images
Images hosted on other servers:

Firm, whitish tumor
Microscopic (histologic) description
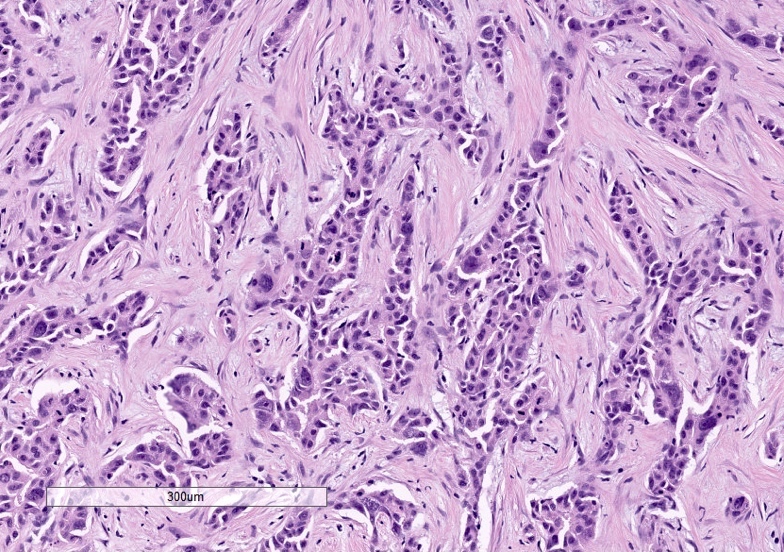
- Abundant fibrous stroma separating nests / trabeculae of tumor cells
- Criteria for amount of intratumoral fibrosis is > 50% (Gastroenterol Clin North Am 2017;46:365)
- Absence of fibrous capsule, no necrosis or hemorrhage, may contain intratumoral portal tracts and prominent tumor infiltrating lymphocytes (Pathol Int 2005;55:724, Hepatogastroenterology 2009;56:1086)
- Clear cell change, steatotic change and hyaline bodies may be present (J Gastroenterol Hepatol 2006;21:1470, Hum Pathol 2019;86:222)
- Less frequently poorly differentiated and more likely to have steatosis than nonscirrhous HCC (Hum Pathol 2019;86:222)
Microscopic (histologic) images
Contributed by Ryan M. Gill, M.D., Ph.D. and Maura F. O’Neil, M.D.
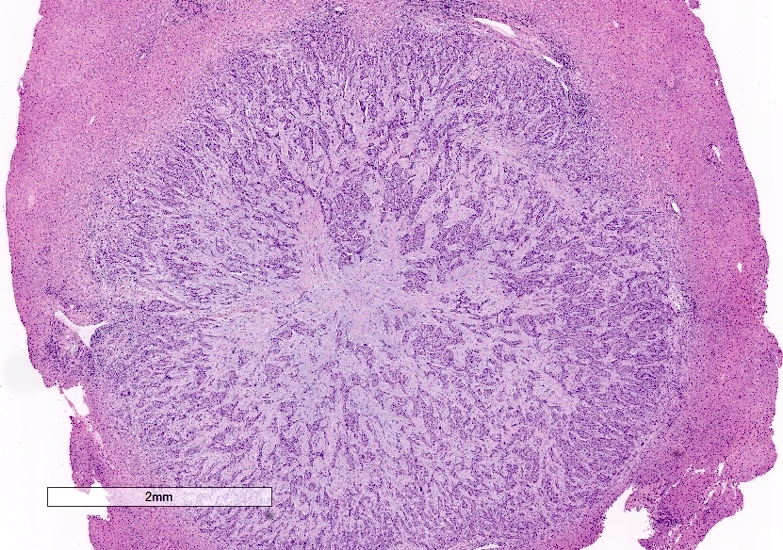
Unencapsulated

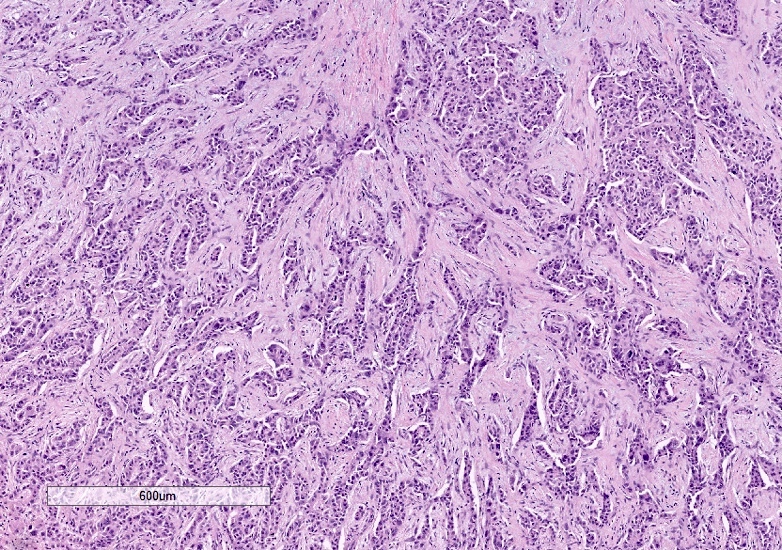
Fibrous stroma
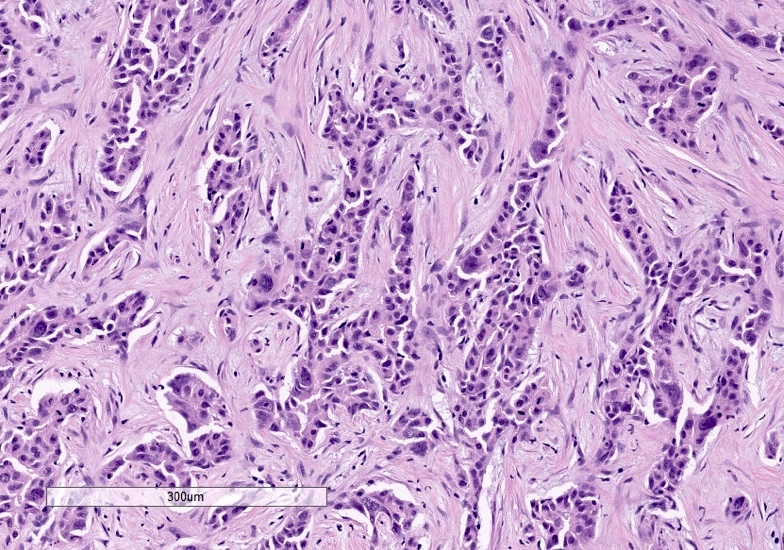
Cytologic features
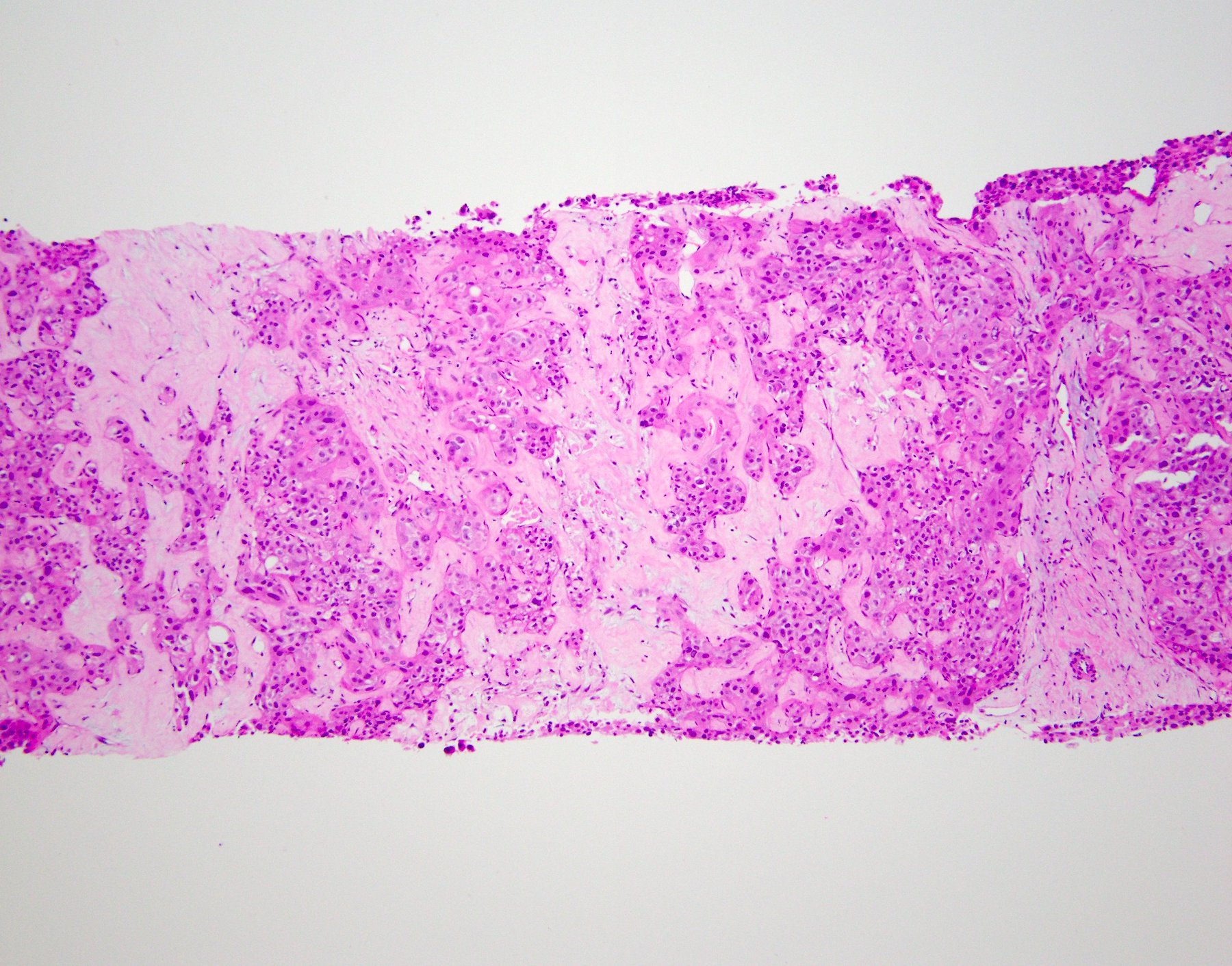
Core biopsy
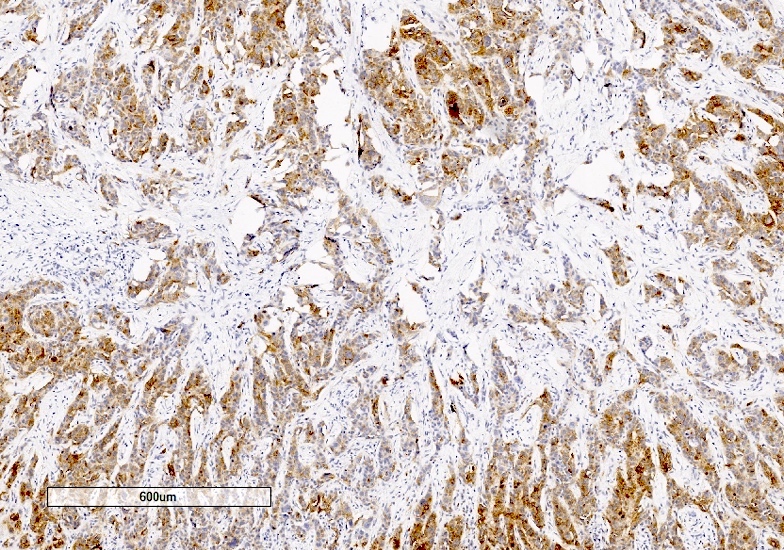
CK7
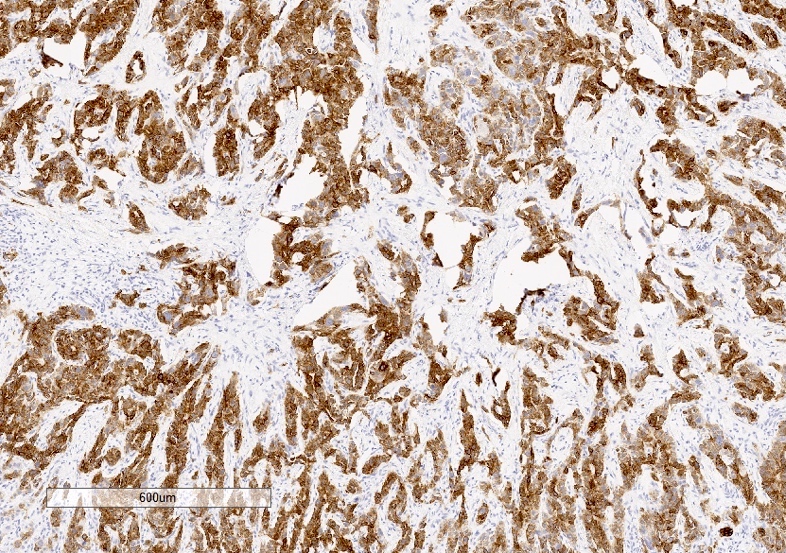
Glypican 3

HepPar1
Cytology description
- Cells are polygonal with distinct cell membranes, high N:C ratio and round nuclei and may have prominent nucleoli (similar to moderately differentiated HCC)
Positive stains
- Glypican 3 and arginase1 in 90% of cases (Mod Pathol 2013;26:782)
- CK7, CK19 and EpCAM in majority of cases (Histopathology 2005;47:382)
Negative stains
- HepPar1 and polyclonal CEA in > 50% (Surg Pathol Clin 2013;6:367)
- Mucin (e.g., mucicarmine)
Molecular / cytogenetics description
- Associated with TSC1 / TSC2 mutations (J Hepatol 2017;67:727)
Sample pathology report
- Liver, mass, partial hepatectomy:
- Scirrhous hepatocellular carcinoma (see comment)
- Comment: This tumor shows histologic features of scirrhous hepatocellular carcinoma with nests and trabecula of hepatoid cells within a dense fibrous stroma. The tumor cells show positive staining for glypican 3, arginase1 and CK7, as is typical for this variant.
Differential diagnosis
- Fibrolamellar variant:
- Intrahepatic cholangiocarcinoma:
- Metastatic carcinoma of pancreas:
- May form glands / tubules with cytoplasmic or intraluminal mucin
- Glypican 3-, arginase1-, albumin ISH-
- Epithelioid hemangioendothelioma:
- Myxoid stroma, blister cells with red blood cells in lumens or vacuoles
- CD34+, ERG+, CD31+, FLI1+, mucicarmine-, variable pankeratin, CAMTA1+, TFE3+ (subset) (Arch Pathol Lab Med 2009;133:967)
- Hepatocellular carcinoma with therapy induced fibrosis:
- May be difficult or impossible to distinguish from scirrhous HCC
- Check treatment history; look for other evidence of injury (e.g., necrosis, embolization beads)
Additional references
Board review style question #1
Which of the following is true regarding this variant of hepatocellular carcinoma?
- Abundant eosinophilic cytoplasm
- Abundant fibrous stroma
- Central scar
- Lamellar fibrous bands
- Prominent nucleoli
Board review style answer #1
Board review style question #2
Which of the following is true regarding the scirrhous variant of hepatocellular carcinoma?
- Association with hypocalcemia has been described
- CK7 and CK19 are often negative
- It is associated with TSC1 / TSC2 mutations
- There is often necrosis or hemorrhage
Board review style answer #2

