
Liver & intrahepatic bile ducts
Dysplasia
High grade dysplastic nodule
Last author update: 27 January 2021
Last staff update: 17 March 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed search: High grade "dysplastic nodule" liver




Table of Contents
Definition / general | Essential features | Terminology | Clinical features | Radiology description | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Assarzadegan N, Gonzalez RS. High grade dysplastic nodule. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorhighgradedysplasticnod.html. Accessed April 2nd, 2025.
Definition / general
- Discrete nodules in cirrhotic livers, containing high grade architectural and cytologic changes insufficient for a diagnosis of carcinoma (Hepatology 2009;49:658)
Essential features
- Dysplastic nodules (both low grade and high grade) are associated with higher risk of development of hepatocellular carcinoma
- High grade dysplastic nodules have a higher risk of transformation into hepatocellular carcinoma than low grade nodules and themselves show molecular changes similar to carcinoma (J Hepatol 2003;39:208)
Terminology
- Also called borderline nodule, macroregenerative nodule type II, atypical macroregenerative nodule, atypical adenomatous hyperplasia
Clinical features
- Considered a precursor to hepatocellular carcinoma
- Usually increase in size over time and do not regress
Radiology description
- Reduced portal blood flow in the nodule on computed tomography is an important predictor for development of hepatocellular carcinoma (Cancer 2006;106:636)
- Usually isovascular or hypovascular compared to surrounding parenchyma, whereas hepatocellular carcinoma appears hypervascular
Treatment
- Ablation or resection should be strongly considered
Gross description
- Often vaguely nodular; can be a distinct nodule often in the background of cirrhosis
- Lack a true capsule
- Typically about 1 cm; can be single or multiple
Microscopic (histologic) description
- Increased cellularity (more than 2 times higher than the adjacent nontumoral liver), often with an irregular trabecular pattern
- Cytologic atypia is usually small cell change; large cell change may or may not be seen (Arch Pathol Lab Med 2011;135:704)
- Portal tracts can be present within the nodules
- Unpaired arteries can be present but not in great numbers (Dig Liver Dis 2011;43:S361)
- "Nodule in nodule" appearance may be seen, where the larger nodule is a high grade dysplastic nodule and the inside subnodule is usually a well differentiated hepatocellular carcinoma
Microscopic (histologic) images
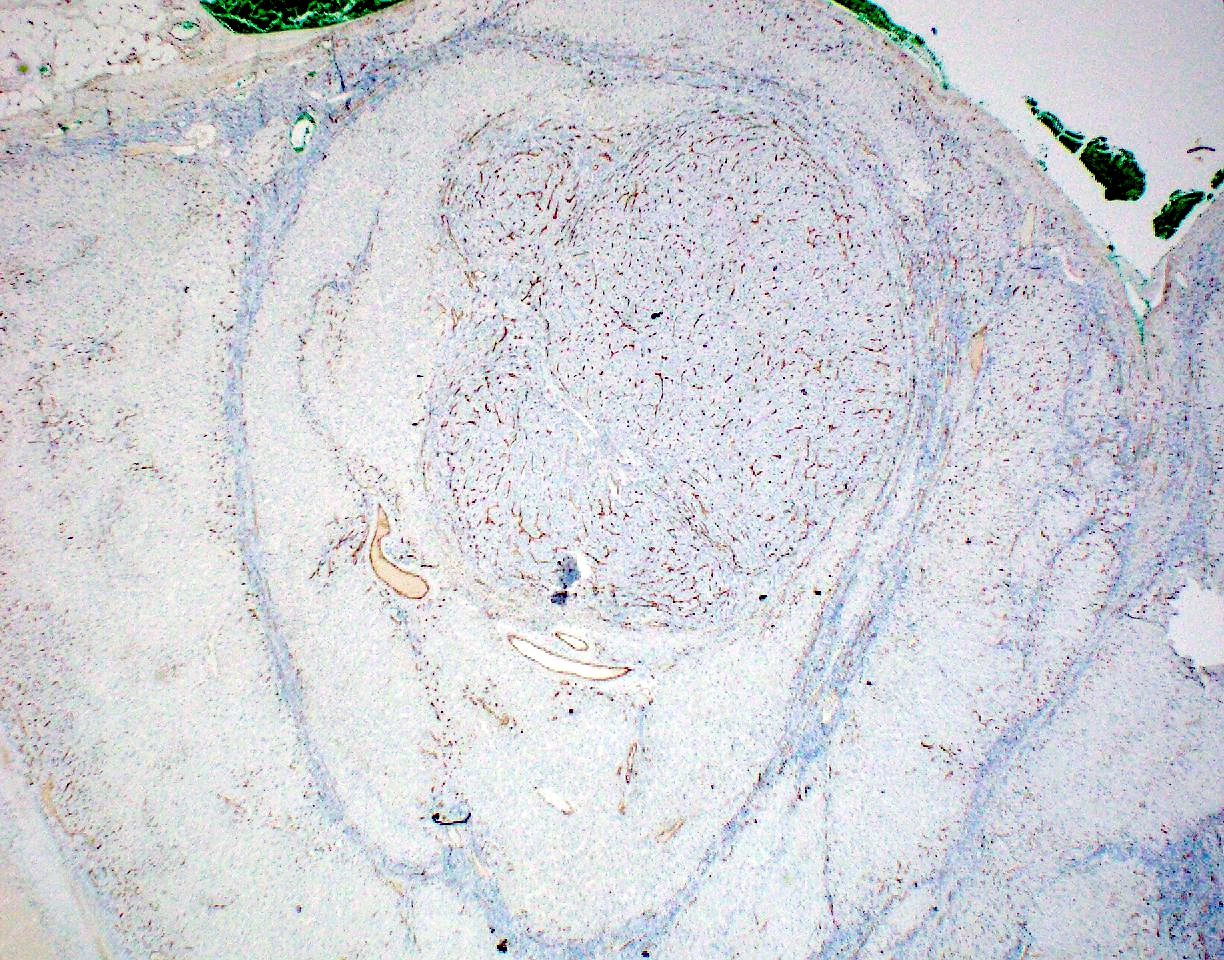
Contributed by Raul S. Gonzalez, M.D.
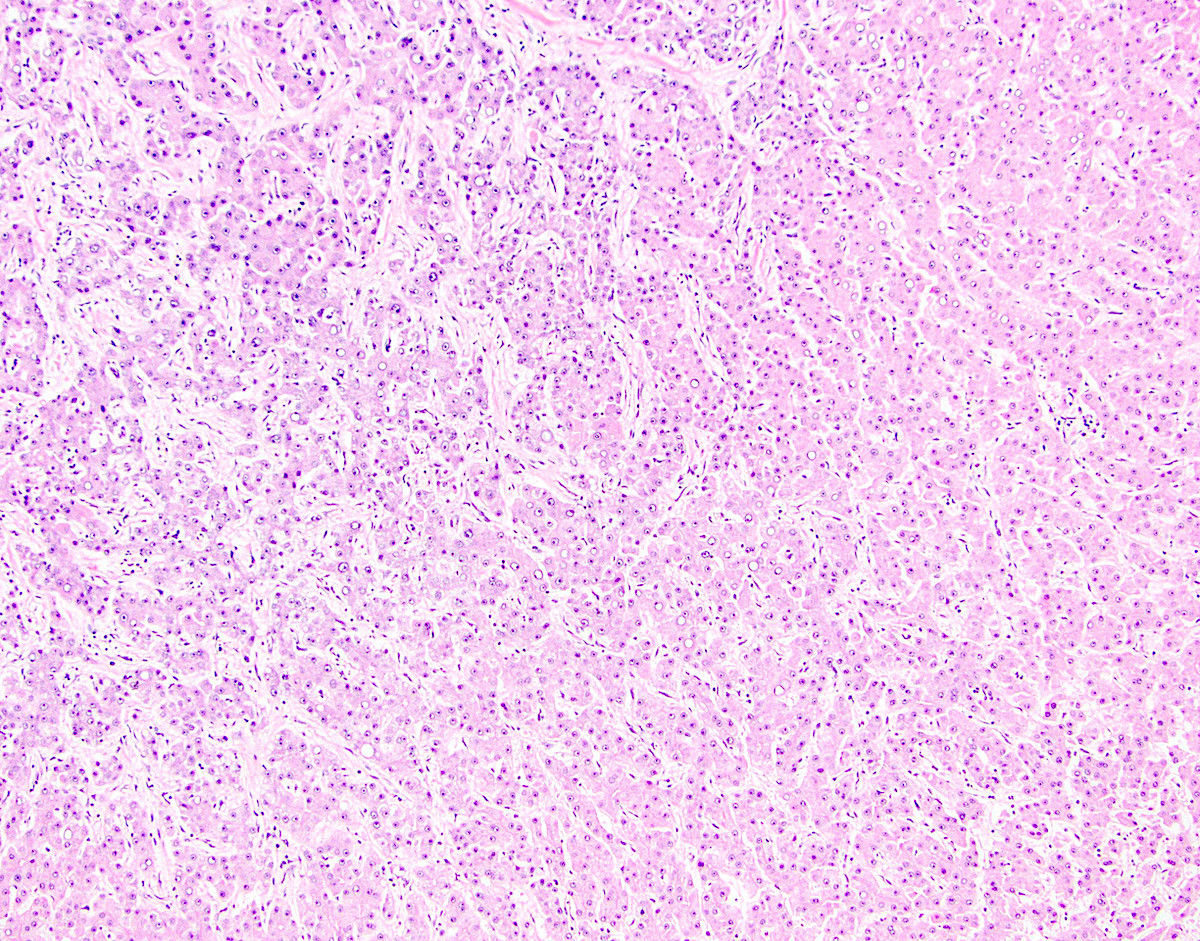
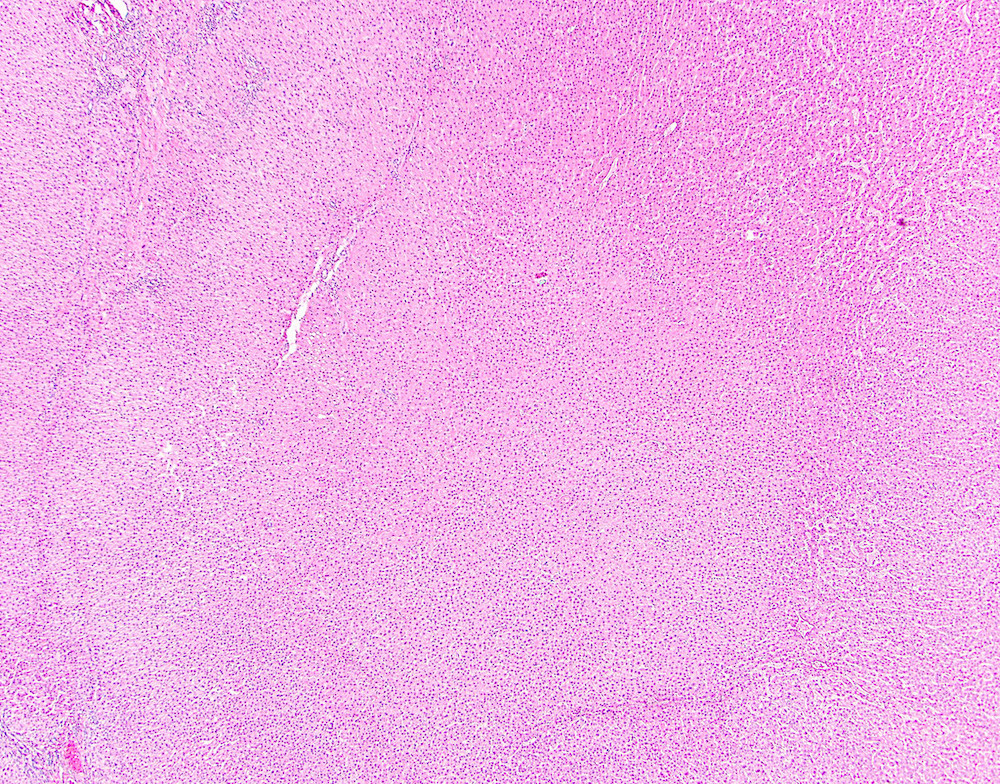

High grade dysplastic nodule

Images hosted on other servers:

Increased cellularity and unpaired arteries
Molecular / cytogenetics description
- Telomere shortening, increased telomerase activity and strong expression of hTERT mRNA at levels similar to hepatocellular carcinoma (Hepatology 2014;60:1983)
- Inactivation of p21 in contrast to cirrhotic nodules, which show activation (Mod Pathol 2009;22:1121)
Sample pathology report
- Liver, native, orthotopic transplantation:
- Cirrhosis with mild chronic inflammation and two high grade dysplastic nodules (see comment)
- Negative for malignancy.
- Margins of resection unremarkable.
- Comment: The findings are consistent with the patient’s reported history of chronic hepatitis B infection. A trichrome stain confirms cirrhosis. An iron stain is unremarkable.
Differential diagnosis
- Dysplastic focus:
- Typically less than 0.1 cm and not nodular
- Hepatocellular carcinoma:
- Distinction can be difficult
- Carcinoma can be positive for glypican 3, heat shock protein 70 or glutamine synthetase and lacks ductular reaction (Hepatology 2007;45:725)
- Low grade dysplastic nodule:
- Less likely to be nodular
- Atypia and cellular are less severe
Board review style question #1
Which of the following is true about high grade dysplastic nodules of the liver?
- They arise in noncirrhotic livers
- They may contain unpaired arteries
- Their molecular profile is the same as that of normal hepatocytes
- They usually measure several centimeters
Board review style answer #1
