

Liver & intrahepatic bile ducts
Other malignancies
Neuroendocrine carcinoma
Author: Whayoung Lee, M.D.
Editorial Board Member: Kimberley J. Evason, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.

Last author update: 9 September 2024
Last staff update: 9 September 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Neuroendocrine carcinoma liver

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Lee W. Neuroendocrine carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorNEcarcinoma.html. Accessed January 4th, 2025.
Definition / general
- Poorly differentiated neuroendocrine carcinomas are high grade, primary malignant epithelial neoplasms of liver or intrahepatic bile ducts with neuroendocrine differentiation
- Divided into small cell carcinoma (SCNET) and large cell carcinoma (LCNEC)
Essential features
- Exceedingly rare, virtually a diagnosis of exclusion after ruling out the possibility of metastasis
- Can be a component of mixed neuroendocrine - nonneuroendocrine neoplasm (MiNEN) with hepatocellular carcinoma or cholangiocarcinoma
- Ki67 proliferation index > 20% (typically > 50%) with abundant apoptosis and necrosis
Terminology
- Poorly differentiated neuroendocrine carcinoma, including small cell carcinoma (SCNEC) and large cell carcinoma (LCNEC)
- Mixed neuroendocrine - nonneuroendocrine neoplasm (MiNEN)
- Not recommended: carcinoid tumor of the liver, atypical carcinoid tumor of the liver
ICD coding
Epidemiology
- Exceedingly rare (0.3% of neuroendocrine neoplasms, < 0.5% of primary hepatic malignancies, < 100 cases reported) (Endocrine 2017;58:368, Endocr Relat Cancer 2010;17:909, Case Rep Oncol 2023;16:681)
- Usually not associated with chronic liver disease / cirrhosis
Sites
- Liver and intrahepatic bile ducts
Pathophysiology
- Not known; 2 hypotheses (Case Rep Oncol 2023;16:681)
- Originated from neuroendocrine cells in the intrahepatic bile duct epithelium
- Dedifferentiated from other malignant cells (malignant hepatocytes)
Etiology
- Not known
Clinical features
- Not well known due to rarity
- It is extremely important to rule out metastatic disease from other organs (e.g., gastrointestinal [GI] tract, pancreas and lung) by clinical workup (e.g., endoscopy, colonoscopy) and imaging study (e.g., gallium 68 dotatate scan and positron emission tomography / computed tomography [PET / CT])
Diagnosis
- Diagnosis of exclusion after ruling out metastasis (fluorodeoxyglucose [FDG] PET scan can be helpful)
- Due to its rarity and lack of characteristic imaging appearance, diagnosis is made by cytology / fine needle biopsy or on surgical specimens
Radiology description
- Large solitary mass with necrosis
- Hyperenhancement in the arterial phase and washout in the portal venous phase due to rich blood supply (similar to hepatocellular carcinoma [HCC]) (Case Rep Oncol 2023;16:681)
- Gallium 68 dotatate PET / computed tomography (CT) scan may show uptake in the lesion and can be used to rule out metastasis
Radiology images
Images hosted on other servers:

Large solitary mass
Prognostic factors
- Not known; generally considered poor prognosis
Case reports
- 22 year old woman with primary hepatic NEC (Case Rep Oncol 2023;16:681)
- 39 year old man with mixed NEC and HCC (Front Surg 2021;8:678853)
- 76 year old man with poorly differentiated HCC and NEC (Am Surg 2016;82:1121)
- 84 year old woman with mixed NEC and HCC (World J Surg Oncol 2021;19:78)
Treatment
- Surgical resection
- Chemotherapy: platinum based regimen (not established)
Gross description
- Typically large solitary mass with areas of hemorrhage and necrosis; may be cystic
Frozen section description
- High grade malignant neoplasm with necrosis, apoptosis and mitotic activity
Microscopic (histologic) description
- Similar histomorphology of poorly differentiated neuroendocrine carcinoma of anywhere in the body
- Solid sheet-like proliferation of the tumor cells with geographic area of necrosis, high mitotic figures and abundant apoptosis (Front Oncol 2013;3:2)
- Small cell NEC: cellular pleomorphism with high N:C ratio, nuclear atypia, hyperchromasia, nuclear molding and frequent mitotic figures
- Large cell NEC: more rounded, marked nuclear pleomorphism with prominent nucleoli
- May have signet ring cell morphology with intracytoplasmic vacuoles negative for mucin but positive for neuroendocrine markers (Semin Liver Dis 2010;30:422)
- If mixed neuroendocrine - nonneuroendocrine neoplasm (MiNEN), 2 types have been reported (J Chin Med Assoc 2009;72:430)
- Collision type tumor: 2 simultaneous but histologically distinct tumors without histologic admixture
- Combined type tumor: both components intermingle with each other and cannot be separated in the transitional area
Microscopic (histologic) images
Contributed by Whayoung Lee, M.D.
Nested growth

Cytologic atypia

Synaptophysin positivity

Chromogranin positivity

Ki67 proliferation
Cytology description
- High N:C ratio with nuclear molding, dark chromatin with inconspicuous nucleoli, background necrosis and typical crush artifact / nuclear streaming
Cytology images
Contributed by Whayoung Lee, M.D.

Diff-Quik stain

Pap stain
Positive stains
- Cytokeratins (CK AE1 / AE3, CAM5.2, CK8 / CK18): may show perinuclear dot-like staining pattern
- Synaptophysin: usually positive; rarely weak or focal
- Chromogranin: usually positive; can be weak and patchy or can be almost absent
- INSM1: new marker of neuroendocrine differentiation; may have better sensitivity in neuroendocrine carcinoma (Am J Pathol 2015;185:3164)
- p53: aberrant expression, either overexpression or null type expression (PLoS One 2017;12:e0187667)
- No site specific IHC stain for hepatic NEC: panel still can be used to exclude metastasis (Torbenson: Tumors of the Liver (AFIP Atlas of Tumor Pathology), 4th Edition, 2018)
- Caveat
- Occasional HCCs can show aberrant staining for synaptophysin or CD56, which does not qualify as the combined HCC - NEC (Torbenson: Biopsy Interpretation of the Liver, 4th Edition, 2021)
- Neuroendocrine tumor can show focal arginase, HepPar1, glypican 3 and AFP staining (Torbenson: Biopsy Interpretation of the Liver, 4th Edition, 2021, Torbenson: Tumors of the Liver (AFIP Atlas of Tumor Pathology), 4th Edition, 2018)
- TTF1 can be positive in NEC regardless of the site of origin (Mod Pathol 2000;13:238)
Negative stains
- RB1: loss of Rb stain (Cancer Discov 2022;12:692)
- Hepatocellular markers: HepPar, arginase1, glypican 3, unless mixed tumor (can show patchy positivity) (Torbenson: Biopsy Interpretation of the Liver, 4th Edition, 2021, Torbenson: Tumors of the Liver (AFIP Atlas of Tumor Pathology), 4th Edition, 2018)
- Beta catenin (J Hepatocell Carcinoma 2018;5:61)
Sample pathology report
- Liver, mass biopsy:
- Involved by poorly differentiated neuroendocrine carcinoma, consistent with small cell carcinoma (see comment)
- Comment: Primary neuroendocrine tumor of the liver is exceedingly rare. Radiologic and clinical correlation is recommended to exclude the possibility of metastatic disease.
Differential diagnosis
- Metastatic neuroendocrine carcinoma from other sites:
- Well differentiated neuroendocrine tumor (WDNET), grade 3:
- Organoid architecture
- Presence of low grade areas (tumor heterogeneity) favors WDNET
- Poorly differentiated hepatocellular carcinoma:
- Positive for hepatocellular markers
- Hepatoblastoma:
- Positive for beta catenin and hepatocellular markers
- Lymphoma:
- Negative for cytokeratin and neuroendocrine markers
- Melanoma:
- Positive for SOX10, HMB45, MelanA, PRAME
- Negative for cytokeratin and neuroendocrine markers
- Metastatic small round blue cell tumors: Ewing sarcoma, desmoplastic small round blue cell tumor, alveolar rhabdomyosarcoma, etc.:
- Negative for cytokeratin and neuroendocrine markers
Additional references
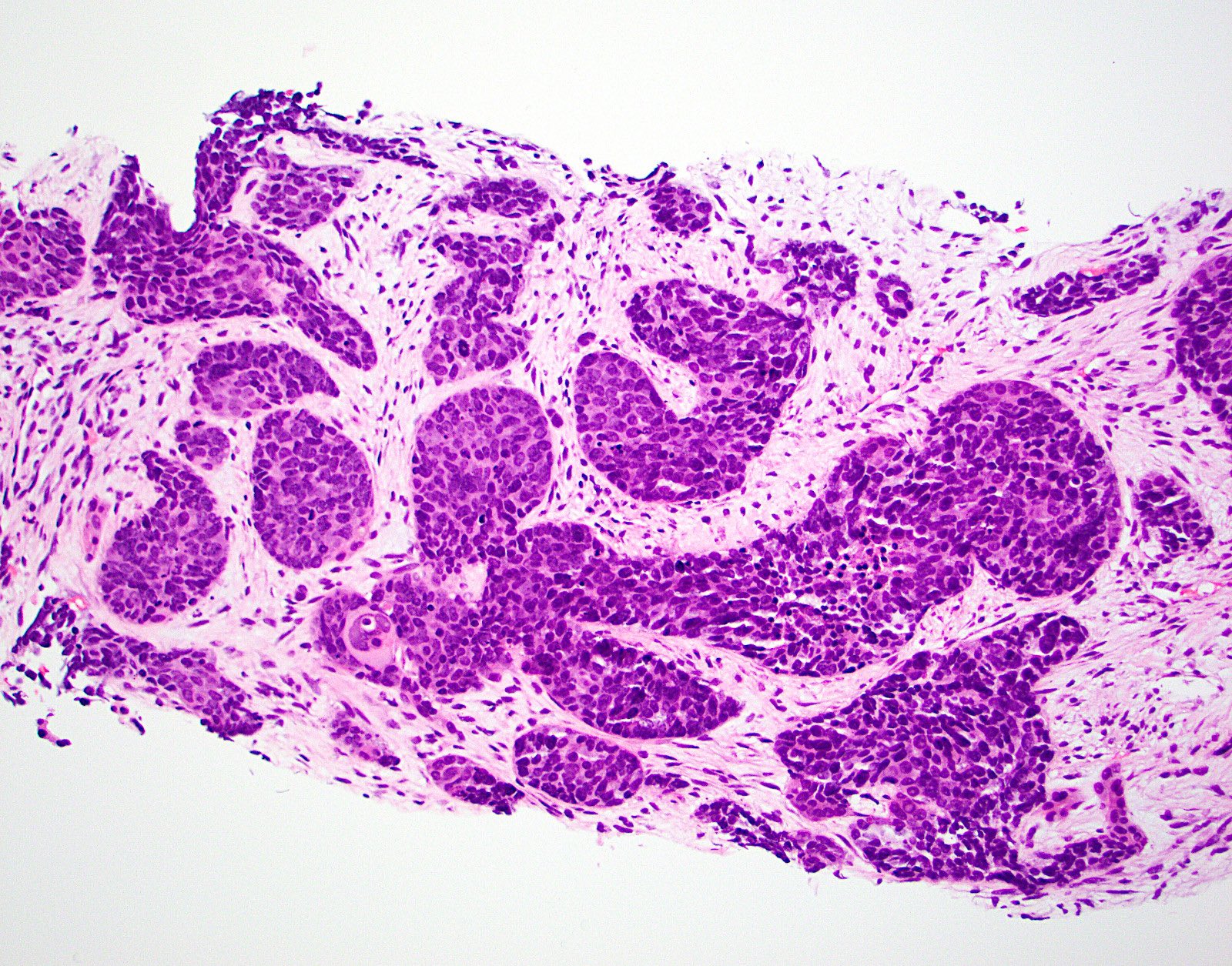
Board review style question #1
A large hepatic mass, shown in the image above, is biopsied. The tumor cells are positive for cytokeratin, synaptophysin and chromogranin. The Ki67 proliferative index is increased to more than 80%. Which of the following is characteristic of neuroendocrine carcinoma of the liver?
- Hepatic primary is more common than metastasis
- It can be seen as a component of hepatocellular carcinoma or cholangiocarcinoma
- It is a well differentiated neuroendocrine tumor
- It usually arises in the background of a cirrhotic liver
- Tumor cells are typically positive for arginase, HepPar1 or glypican 3
Board review style answer #1
B. It can be seen as a component of hepatocellular carcinoma or cholangiocarcinoma. This tumor is a high grade neuroendocrine carcinoma. Primary hepatic neuroendocrine carcinoma is exceedingly rare and the diagnosis should be made after carefully excluding possible metastatic disease. It can be a component of mixed neuroendocrine - nonneuroendocrine neoplasm (MiNEN) with hepatocellular carcinoma or cholangiocarcinoma.
Answer A is incorrect because metastatic lesions in the liver are more common than hepatic primary. Answer C is incorrect because it is a poorly differentiated neuroendocrine carcinoma (PDNEC). Answer D is incorrect because neither primary hepatic PDNEC nor metastatic neuroendocrine neoplasms are usually found in the noncirrhotic background. Answer E is incorrect because hepatic PDNEC does not typically express hepatocellular markers unless it is mixed HCC - PDNEC.
Comment Here
Reference: Neuroendocrine carcinoma
Comment Here
Reference: Neuroendocrine carcinoma

