
Liver & intrahepatic bile ducts
Hepatocellular carcinoma
HCC - cytology


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Hepatocellular carcinoma cytology


- Most common primary malignancy of the liver
- Hepatocytic differentiation
- Fine needle aspiration is a useful tool in the diagnosis of hepatocellular carcinoma (HCC)
- 70 - 90% arise in cirrhotic patients
- Elevated alpha fetoprotein (AFP)
- Accuracy of cytopathologic diagnosis of HCC is high (> 90%) (J Surg Oncol 1991;48:246, Diagn Cytopathol 2002;26:283, Acta Cytol 2013;57:332)
- Common pitfalls:
- False negative: well differentiated HCC mistaken as benign lesion or nonneoplastic liver (false nondiagnostic)
- False positive: dysplastic nodules and benign hepatic tumors mistaken for well differentiated HCC
- Misdiagnosis: poorly differentiated HCC mistaken for metastatic carcinoma
- Cell blocks are useful to confirm hepatocellular differentiation with immunohistochemical stains (arginase1, HepPar1, glypican 3)
- Liver
- Common metastatic sites: lymph nodes and lungs
- Less common metastatic sites: adrenal glands, bone, kidney, spleen and ovary
- Elevated alpha fetoprotein (AFP)
- Ultrasound typically shows a distinct hepatic nodule; when a nodule is detected through ultrasound, diagnosis is complemented by CT and MRI (Eur J Radiol 2018;101:72)
- Dynamic CT or MRI (contrast enhanced imaging) shows a typical pattern of intense enhancement during arterial phase when compared to surrounding parenchyma and progressive decrease during venous phases (wash out) (Eur J Radiol 2018;101:72)
- When the typical findings are present, a biopsy is not always mandatory for the diagnosis of HCC (Eur J Radiol 2018;101:72)
- Liver Imaging Reporting and Data System (LI-RADS) classifies liver nodules detected on dynamic CT / MRI into categories depending on the risk of malignancy (Eur J Radiol 2018;101:72, Radiology 2018;289:816):
- LI-RAD 1: definitely benign
- LI-RAD 2: probably benign
- LI-RAD 3: intermediate probability of malignancy
- LI-RAD 4: probably HCC
- LI-RAD 5: definitely HCC
Contributed by Lawrence Hsu Lin, M.D., Ph.D. and Tamar C. Brandler, M.D., M.S.
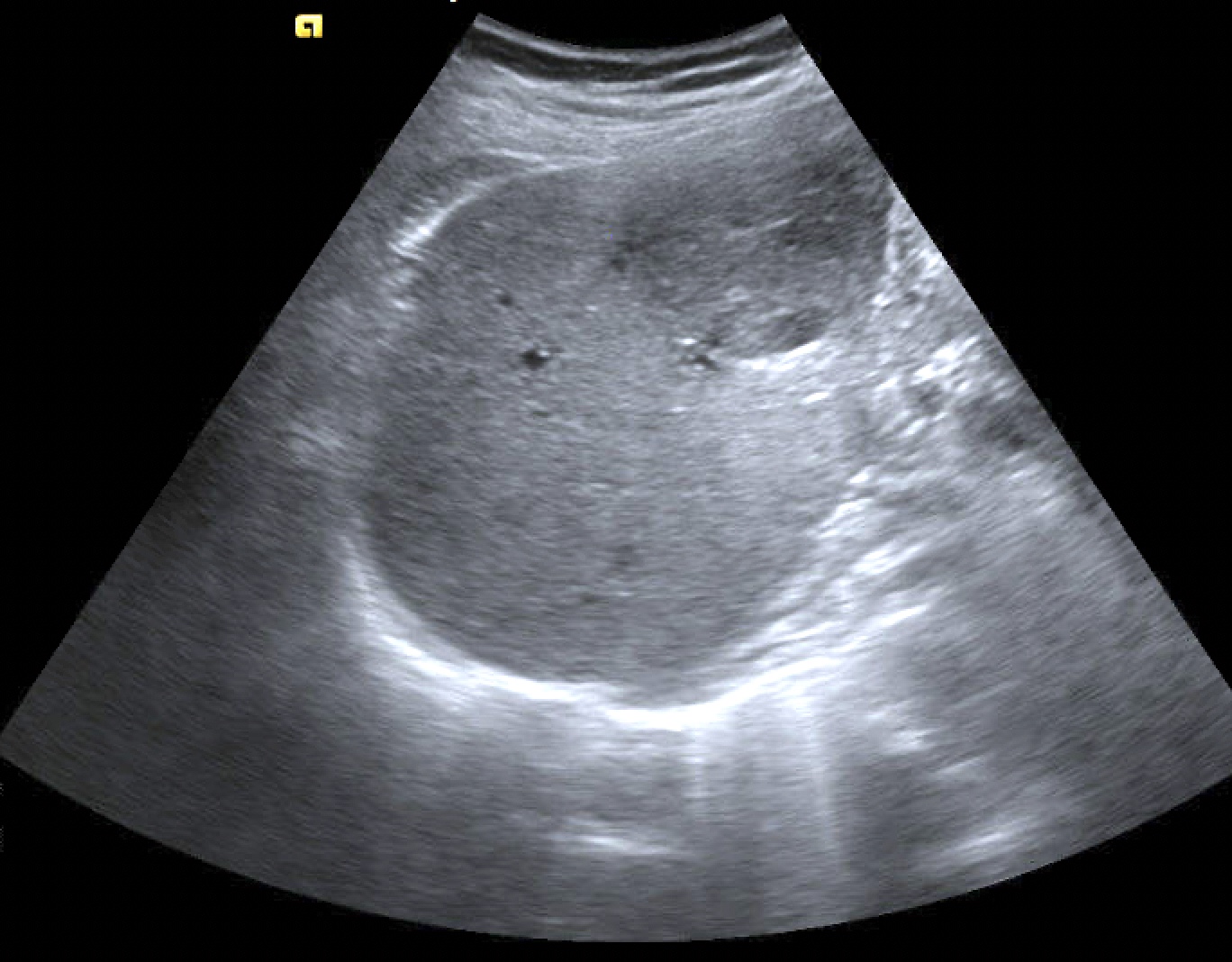
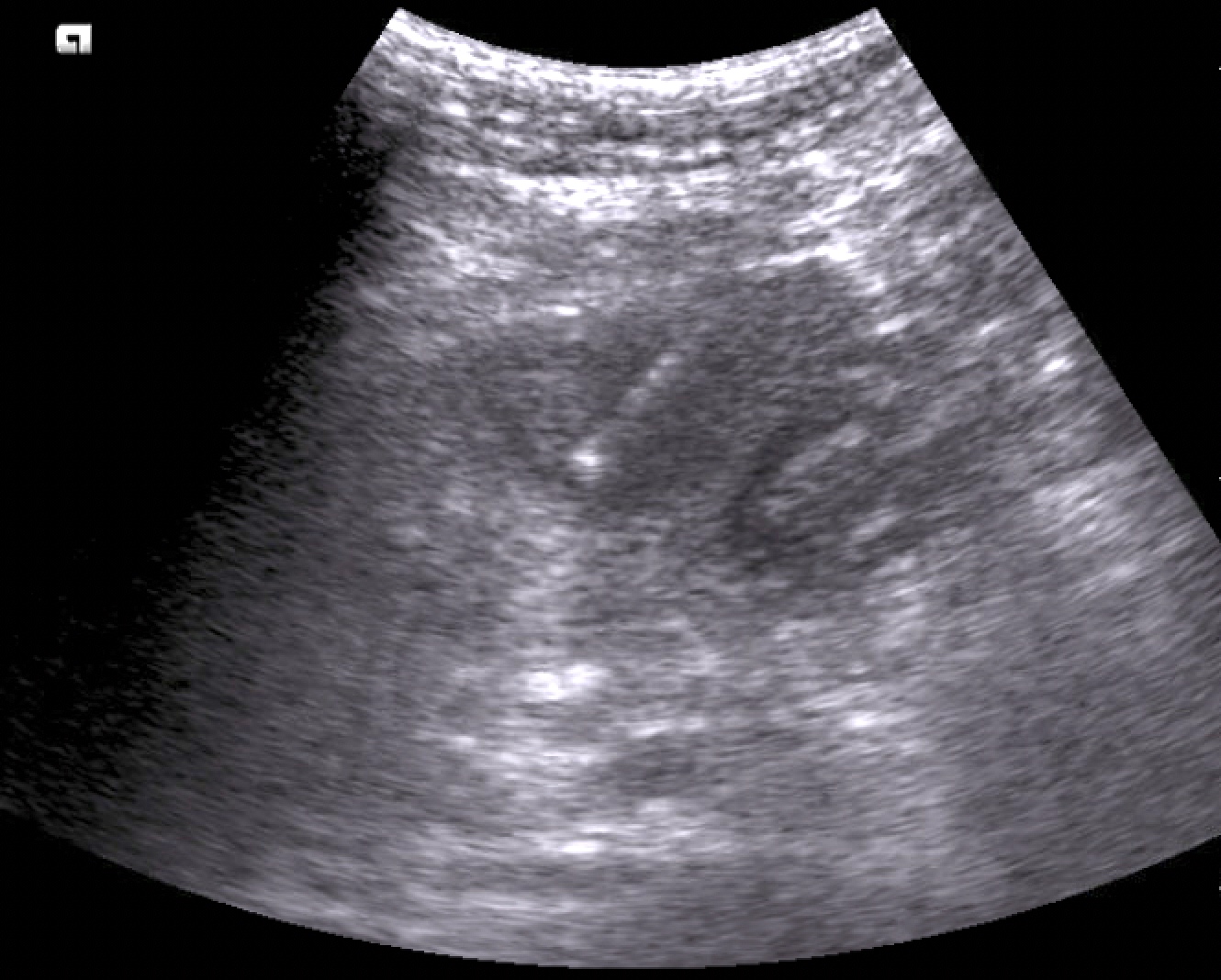
Rounded mass (ultrasound)
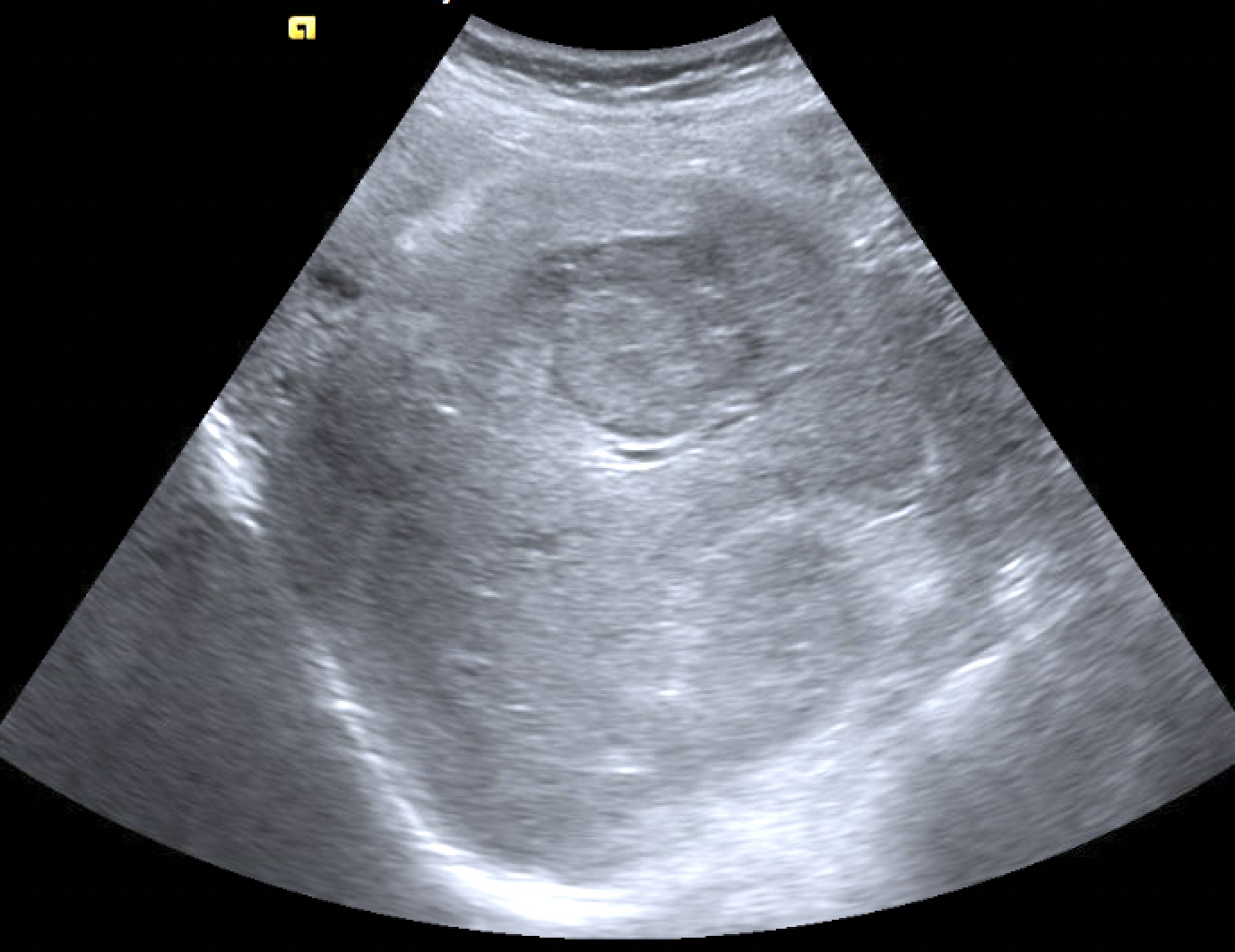
Lobulated mass (ultrasound)
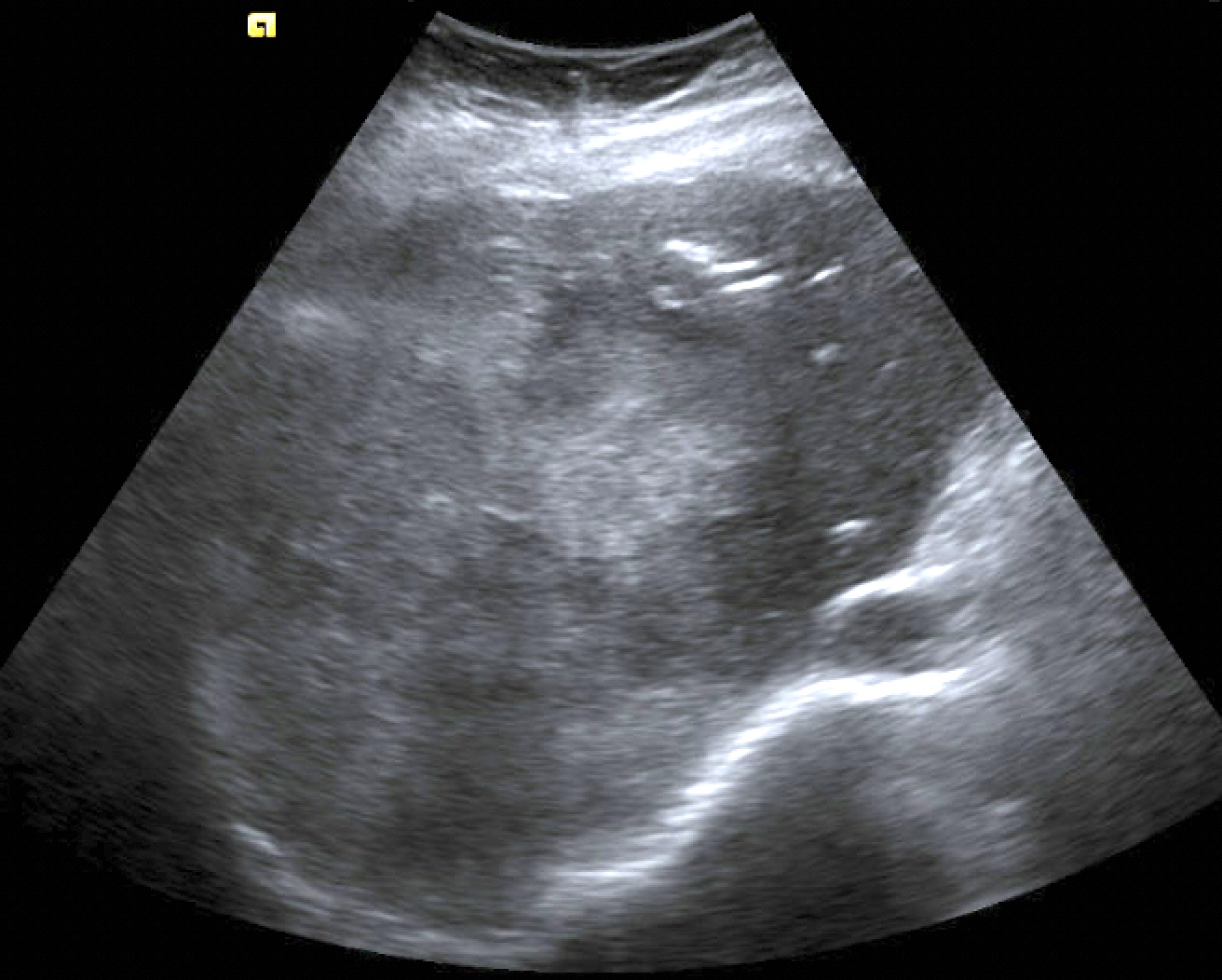
Heterogeneous echotexture (ultrasound)
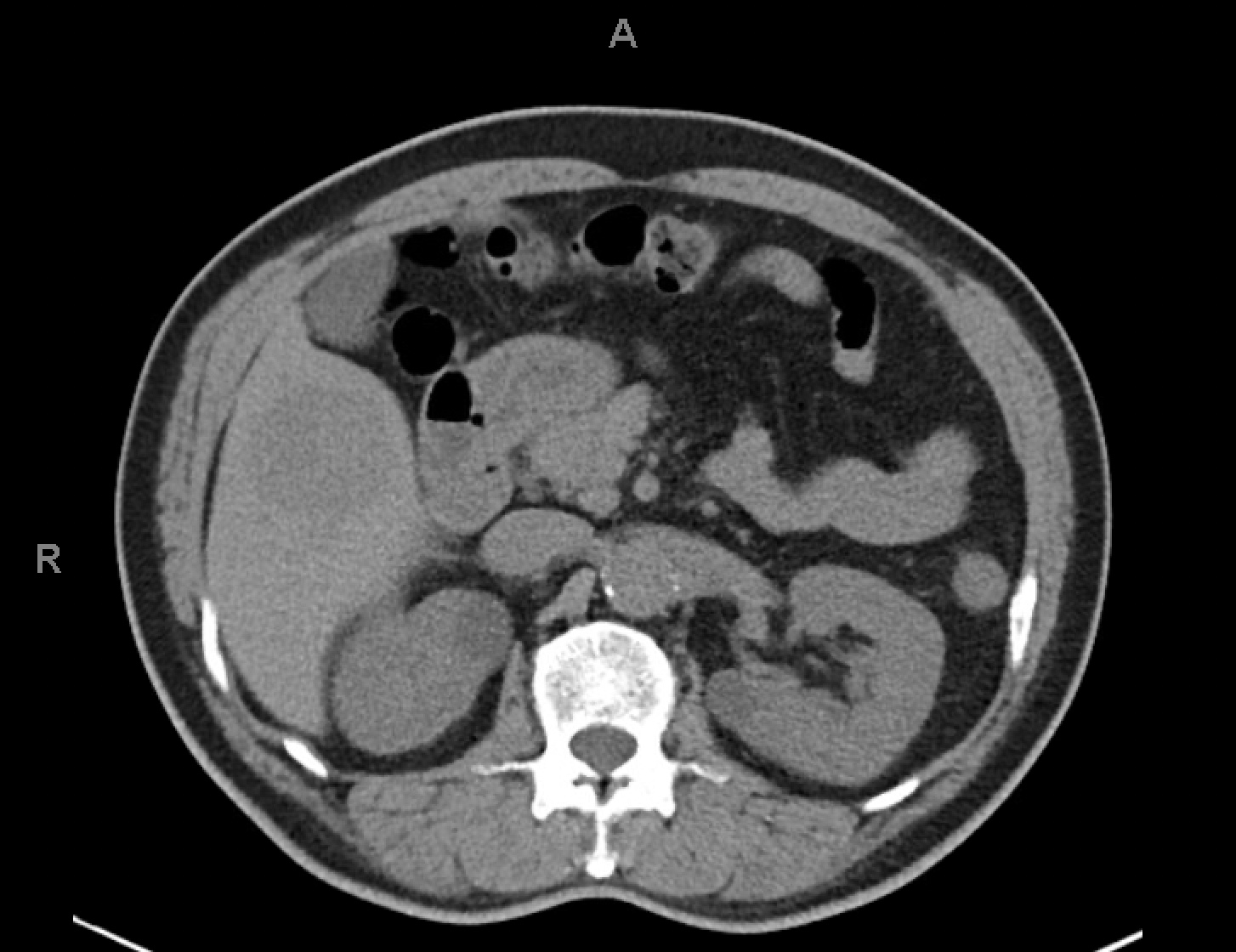
Hypodense mass (CT)

Ill defined area (CT)
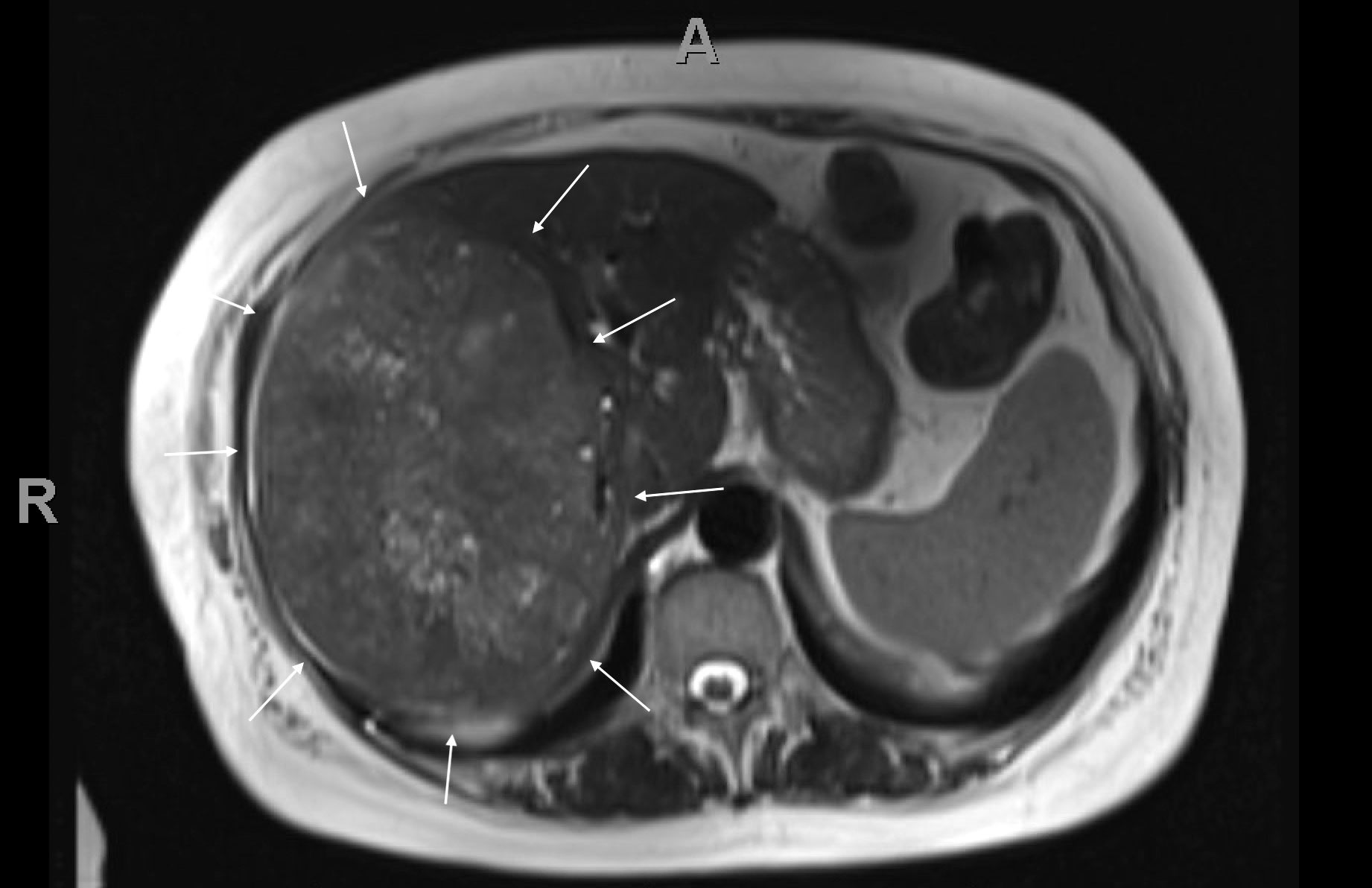
Large hepatic mass (MRI)
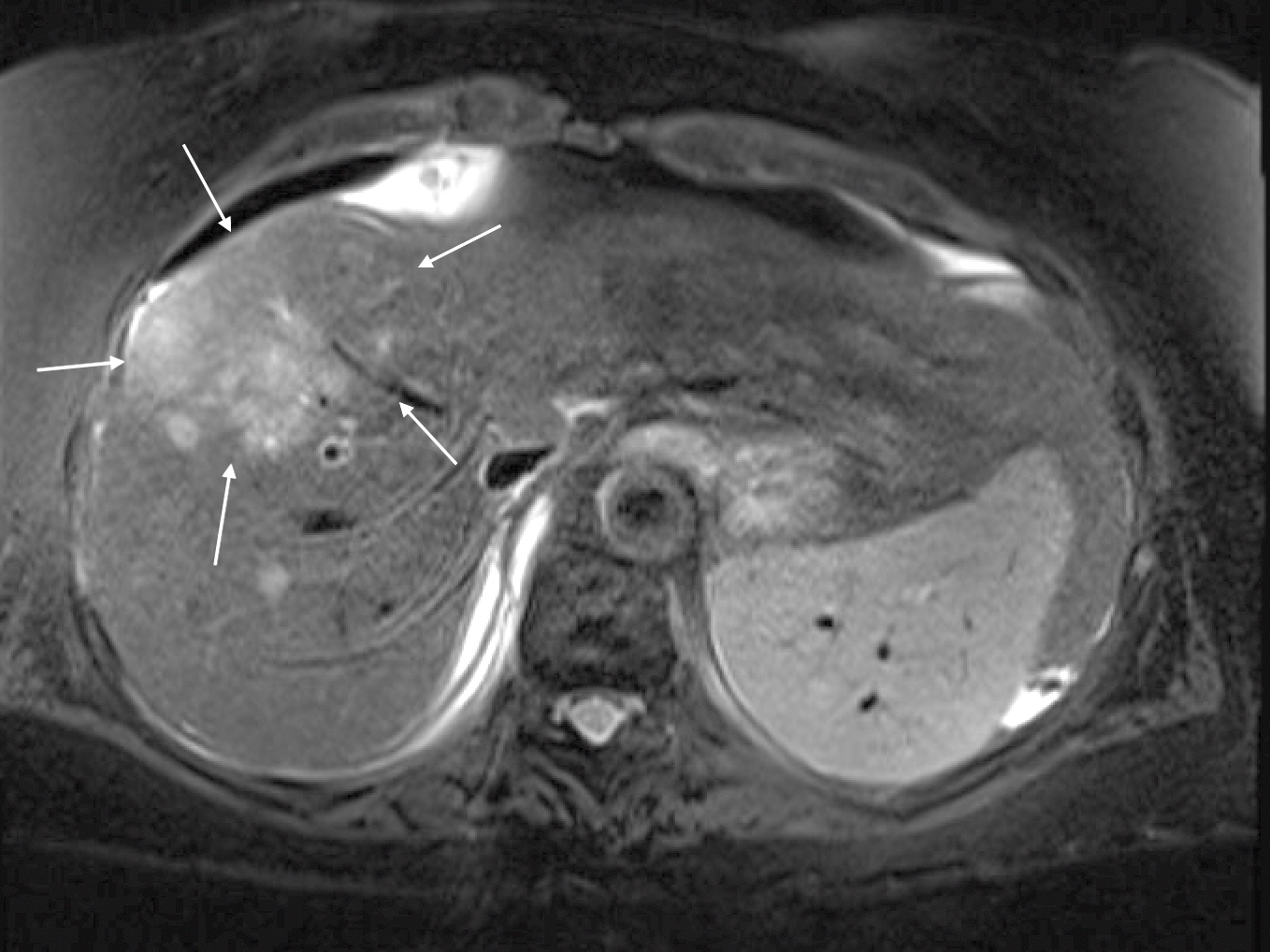
Poorly defined mass (MRI)
Ultrasound guided biopsy

CT guided biopsy
- 20 year old woman with lung mass (Int J Clin Exp Pathol 2013;6:1942)
- 32 year old woman with mediastinal lymphadenopathy (Cytojournal 2011;8:2)
- 36 year old man with neck mass (Int J Surg Case Rep 2013;4:76)
- 56 year old man with breast mass (Cytojournal 2012;9:21)
- 64 year old man with hilar lymphadenopathy (Respirol Case Rep 2021;9:e00792)
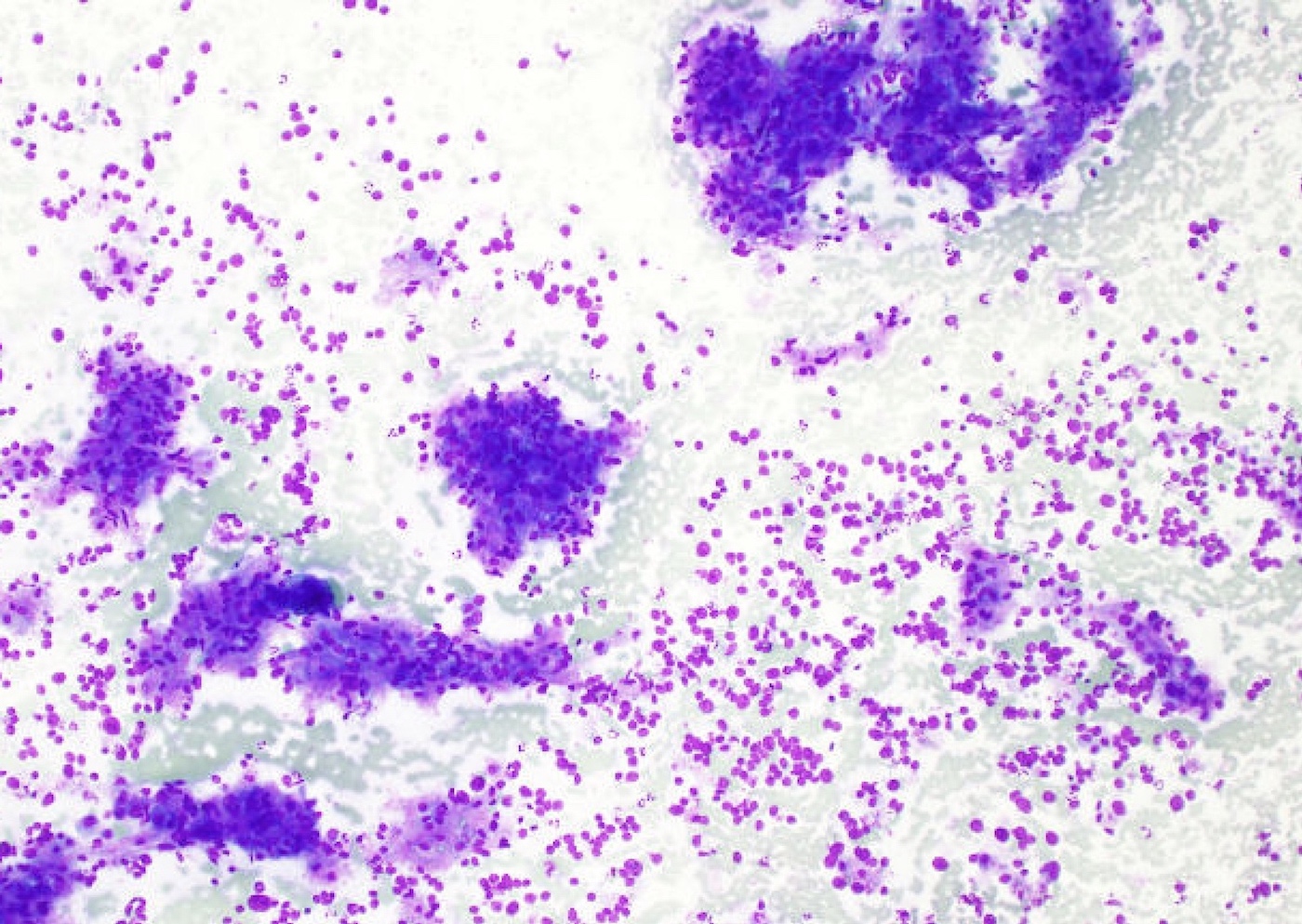
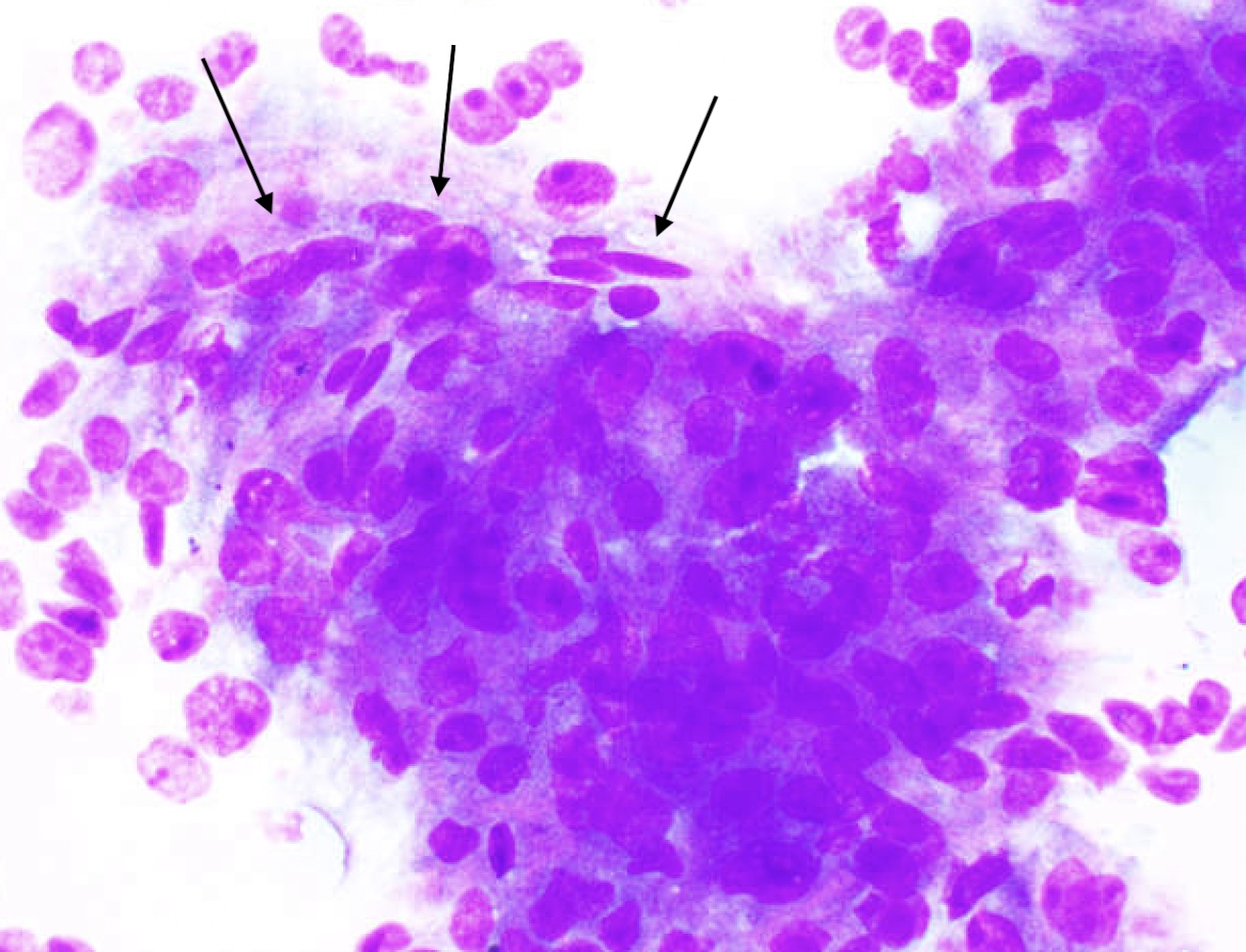
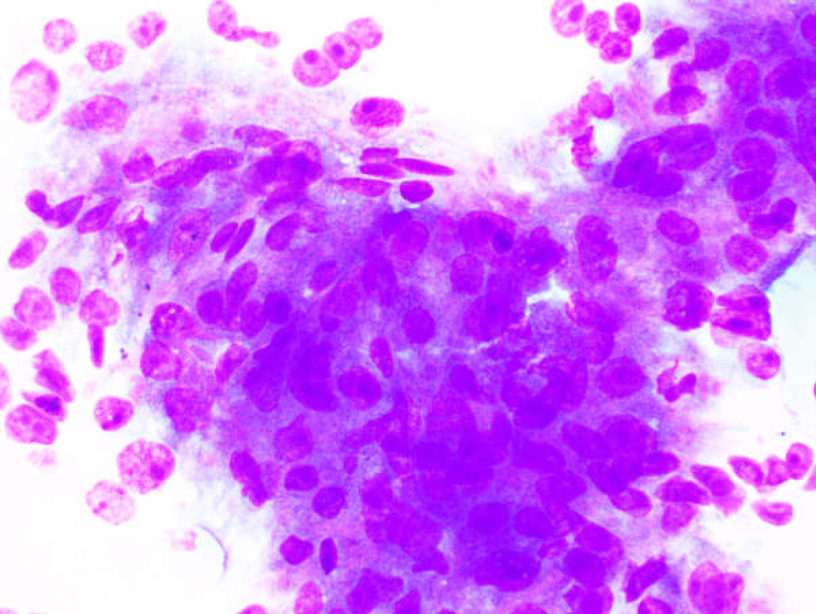
- Highly cellular smears
- Cytologic features of the neoplastic cells depend on the level of differentiation of HCC
- Well and moderately differentiated show resemblance to normal hepatocytes with:
- Polygonal monotonous cells
- Granular cytoplasm
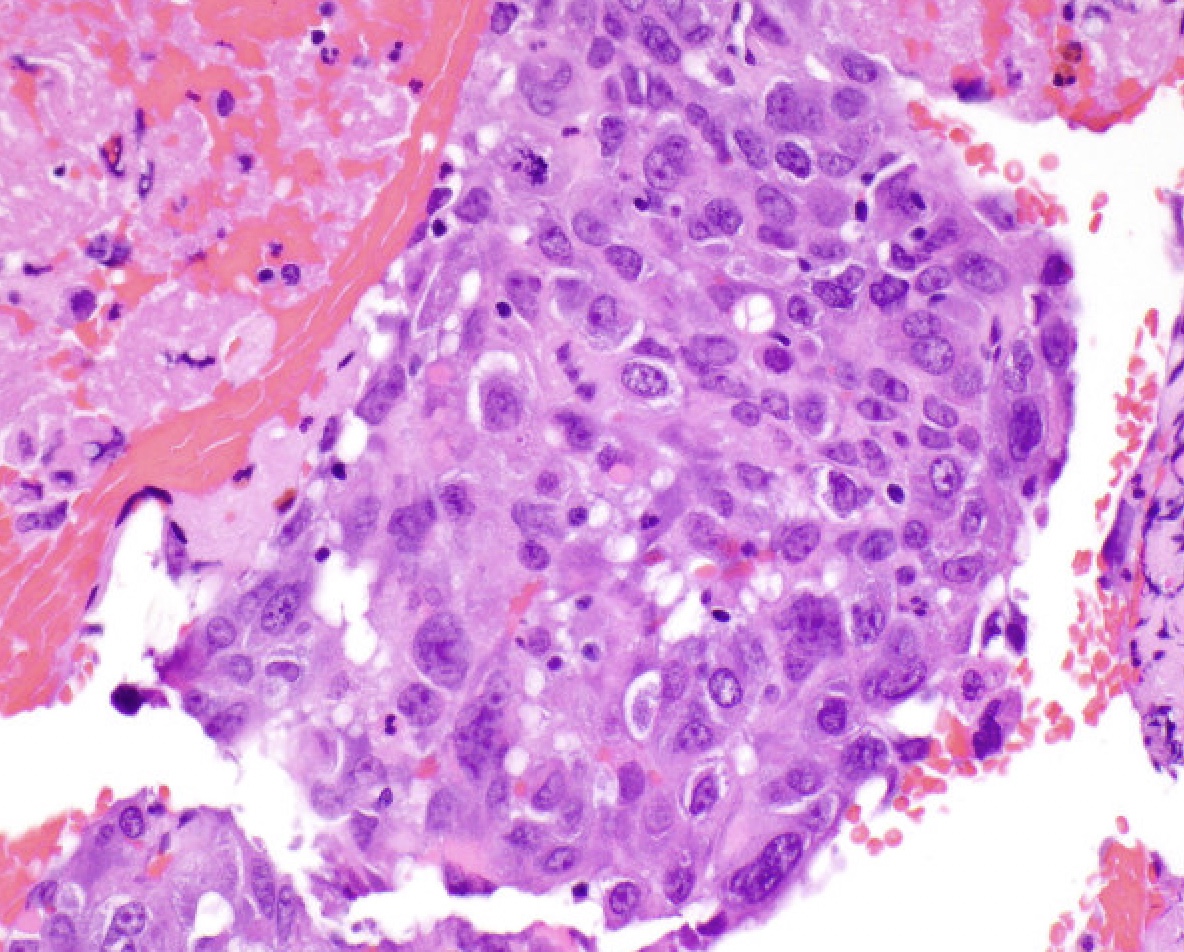
- Enlarged nuclei
- Increased nuclear to cytoplasmic ratio
- Nuclear membrane irregularity
- Coarse chromatin
- Prominent macronucleoli
- Bile may be present in cytoplasm
- Cytoplasmic inclusions (Mallory-Denk bodies, hyaline inclusions, ground glass) may be present
- Nuclear pseudoinclusions
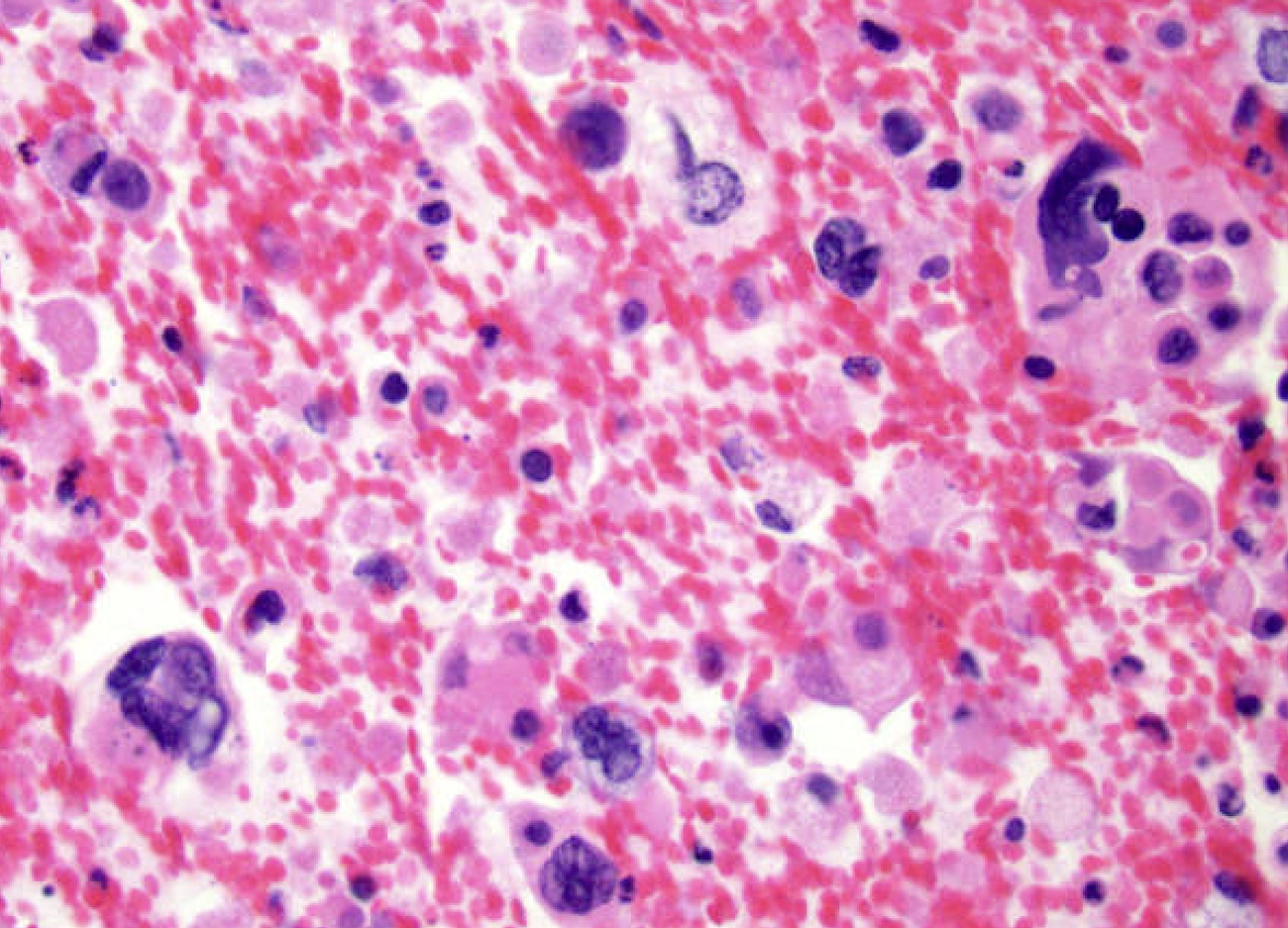
- Poorly differentiated HCC shows no resemblance to hepatocytes:
- Marked nuclear pleomorphism
- Multinucleated tumor cells
- Spindle cells
- Atypical mitosis
- Necrosis
- Well and moderately differentiated show resemblance to normal hepatocytes with:
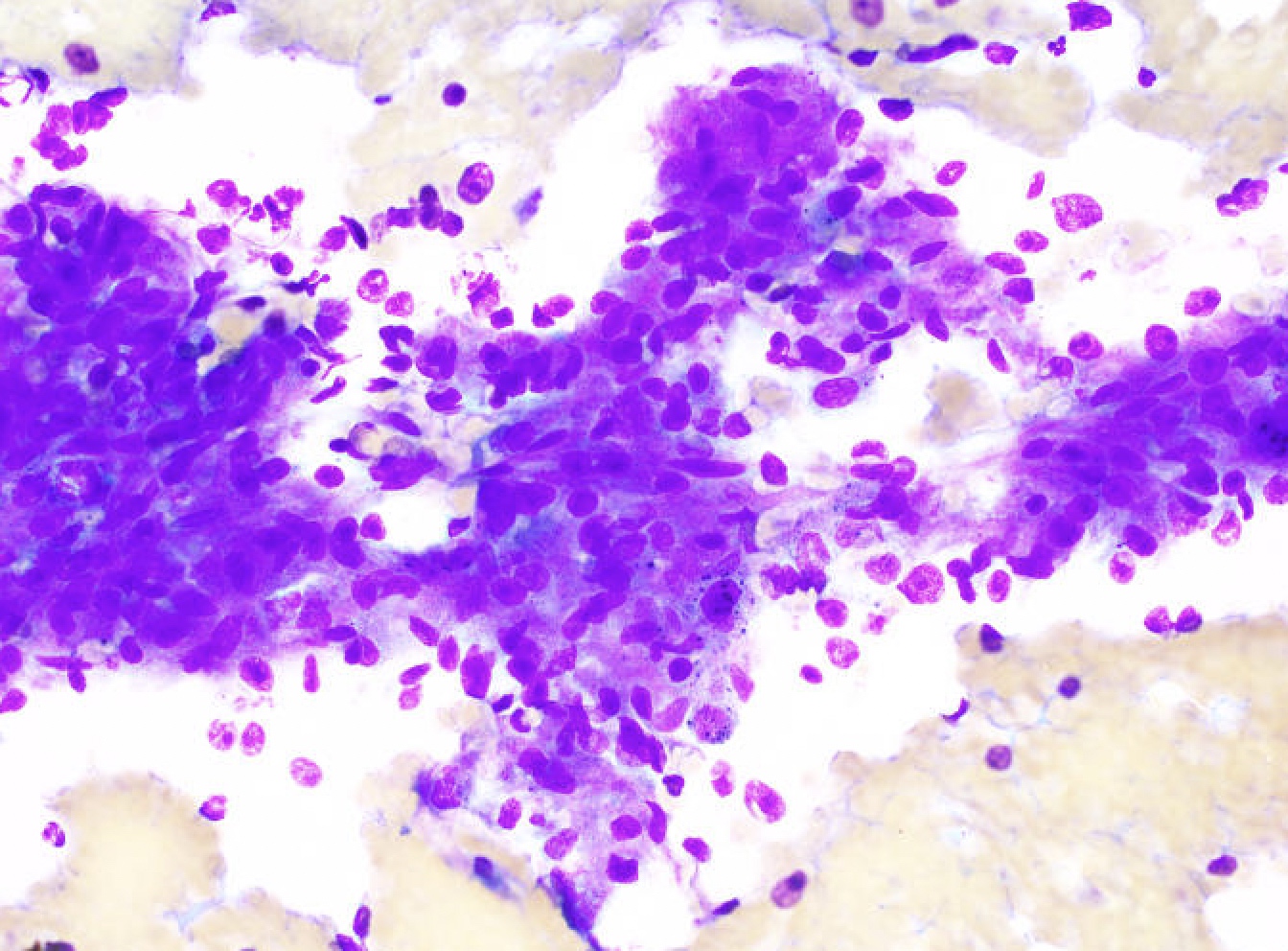
- Numerous isolated cells and large naked nuclei
- Nuclear crowding and overlapping cells
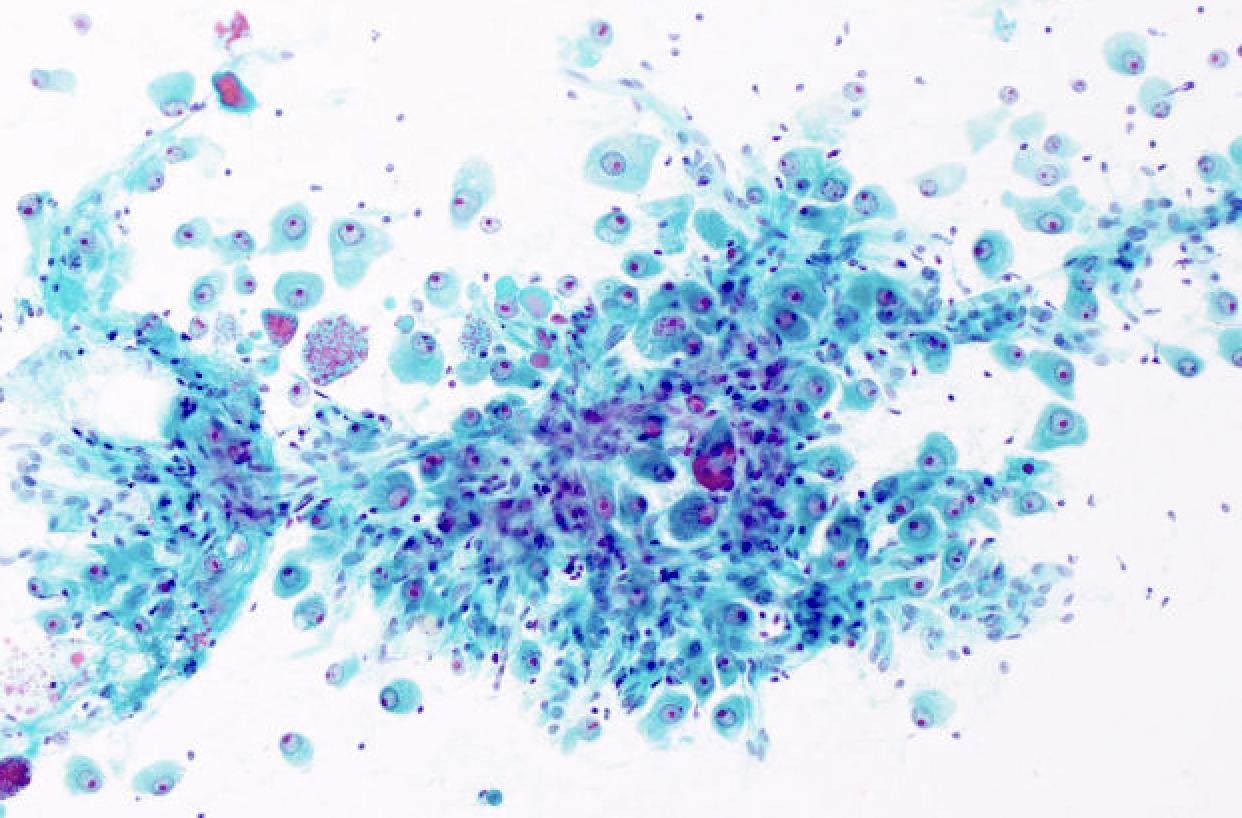
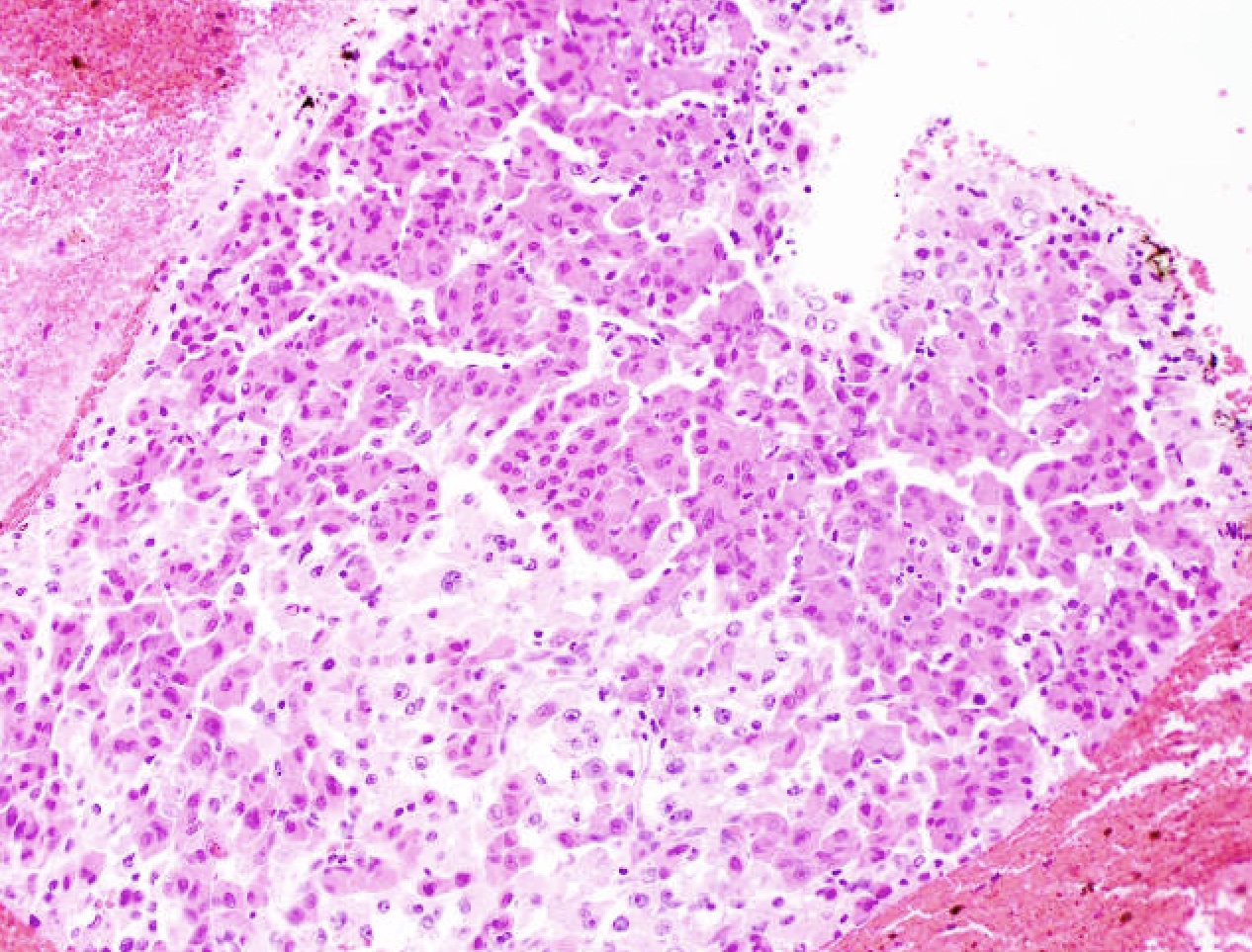
- Thickened cell cords (trabeculae) with endothelial wrapping, sometimes better appreciated on cell block
- Pseudoglandular structures (pseudoacinar pattern), sometimes better appreciated on cell block
- Peripheral endothelial cells (endothelial wrapping around neoplastic cells)
- Transgressing vessels (vessels transversing neoplastic tissue)
- Cytologic features of fibrolamellar subtype of HCC
- Larger neoplastic cells than in ordinary HCC
- Lower nuclear to cytoplasmic ratio than in ordinary HCC
- Fibrous stroma fragments
- Specific cytologic features may suggest subtypes of HCC
- Clear cells: clear cell HCC (Diagn Cytopathol 1997;17:306, Acta Cytol 1991;35:671)
- Spindle cells: sarcomatoid HCC
- Immunohistochemistry and special stains
- Reticulin: highlights the thickened trabeculae (> 3 cells) (Mod Pathol 1997;10:1258)
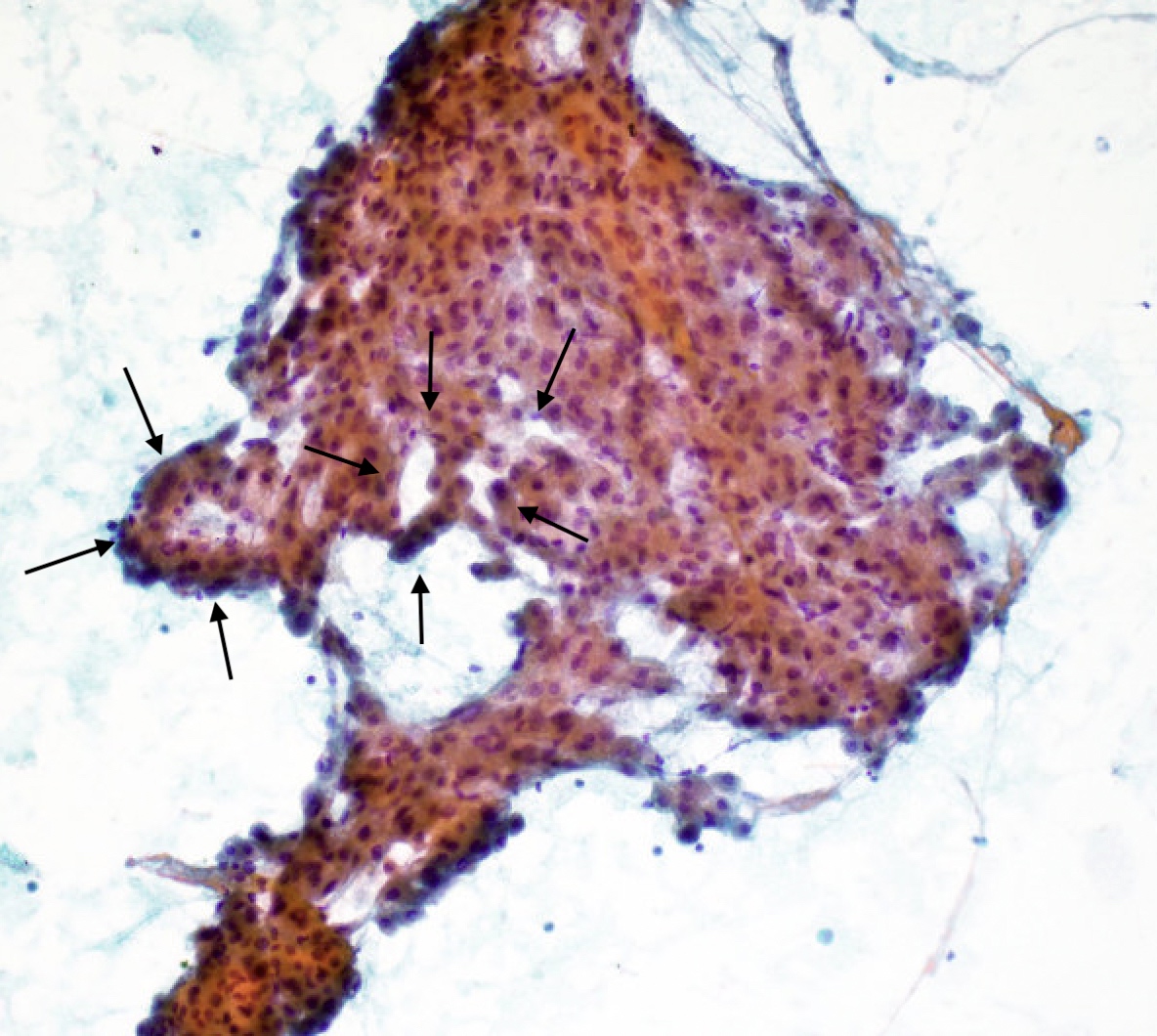
- Arginase1 (ARG1): cytoplasmic and nuclear; highly sensitive and specific (Cancer Cytopathol 2012;120:230, Cancer Cytopathol 2012;120:223)
- HepPar1 (hepatocyte paraffin 1): cytoplasmic and granular; highly sensitive, expressed in 50% of poorly differentiated HCC (Am J Surg Pathol 2002;26:978, Pathol Oncol Res 2015;21:379, Diagn Cytopathol 2004;30:1)
- Glypican 3 (GPC3): cytoplasmic; high sensitivity in poorly differentiated and scirrhous hepatocellular carcinoma, low sensitivity in well differentiated hepatocellular carcinoma, negative in benign and nonneoplastic liver (Diagn Cytopathol 2009;37:629, Pathol Oncol Res 2015;21:379)
- Alpha fetoprotein (AFP): cytoplasmic; highly specific but low sensitivity (Am J Surg Pathol 2002;26:978)
- Polyclonal CEA: canalicular pattern; limited sensitivity in poorly differentiated HCC (Acta Cytol 1997;41:1147, Diagn Cytopathol 2004;30:1)
- TTF1: cytoplasmic; positivity is highly variable and clone dependent (Am J Clin Pathol 2006;125:519, Am J Clin Pathol 2004;121:343)
- CD34: highlights endothelial cells wrapping around thickened trabeculae (Diagn Cytopathol 2004;30:1)
- CAM5.2: positive (Hum Pathol 2002;33:1175, Am J Clin Pathol 1993;99:551)
- CK7, CK19, CK20: usually negative but can be positive in a few cases (Hum Pathol 2002;33:1175)
Contributed by Lawrence Hsu Lin, M.D., Ph.D. and Tamar C. Brandler, M.D., M.S.
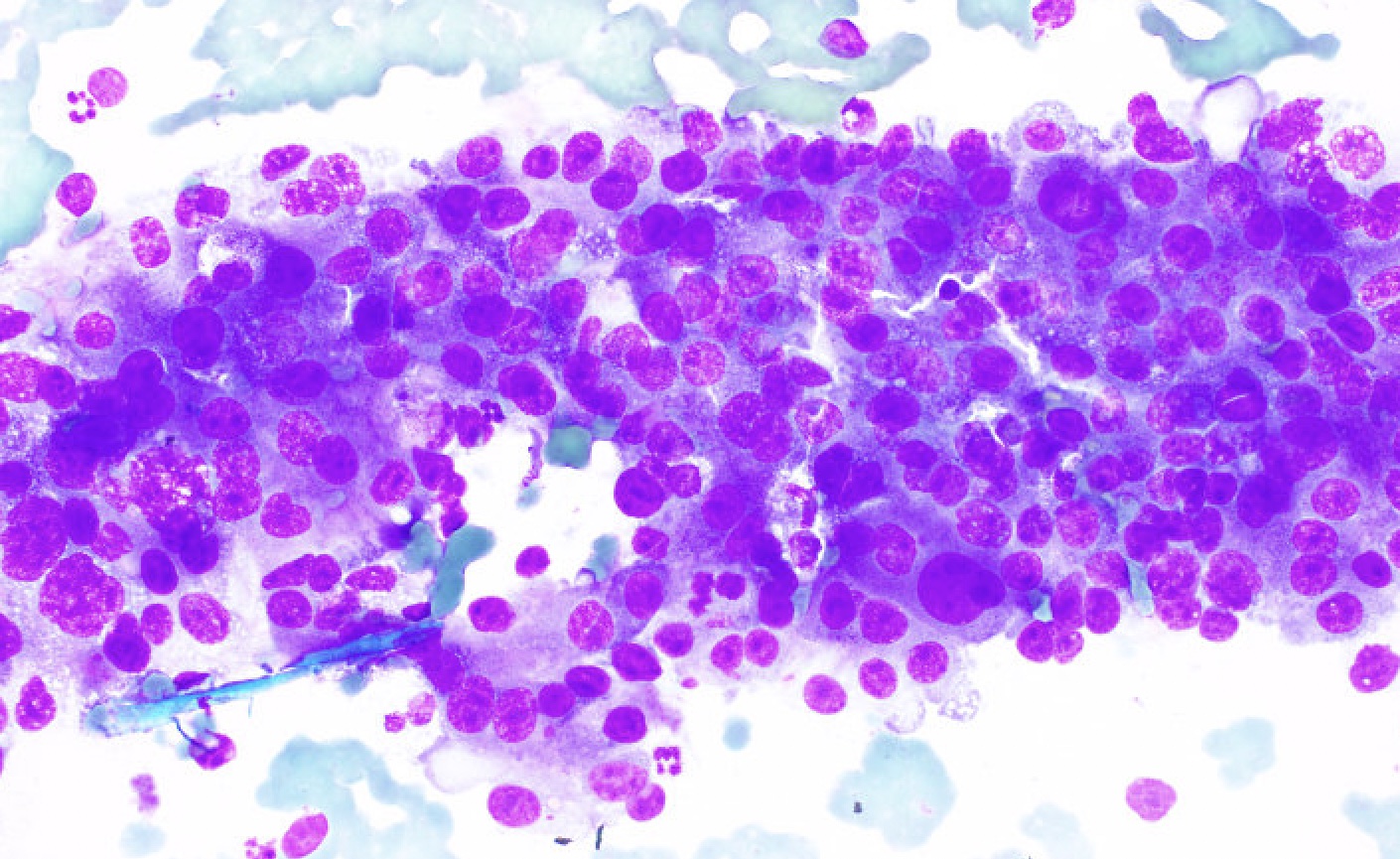
High cellularity with bare nuclei
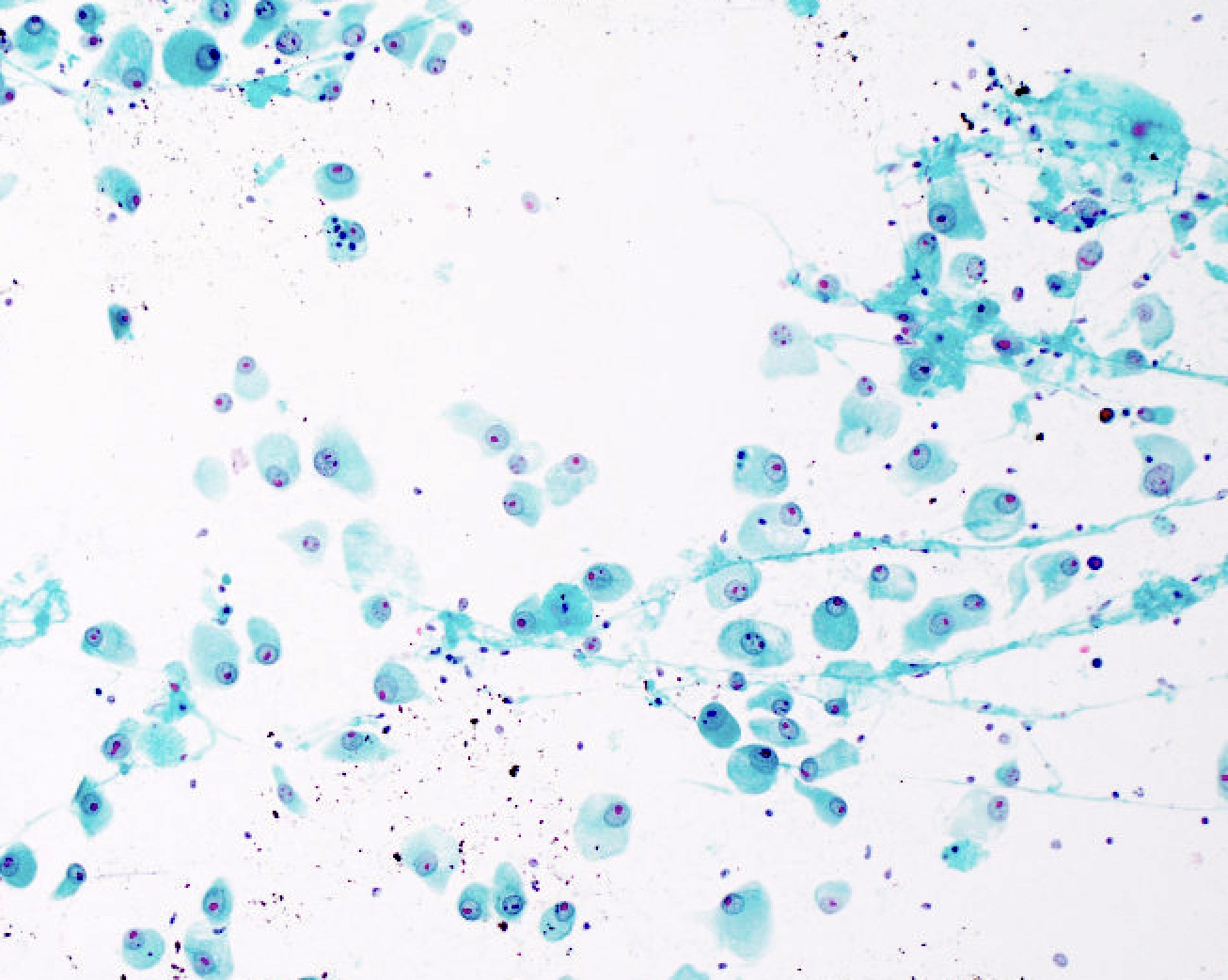
High cellularity and normal appearing hepatocytes
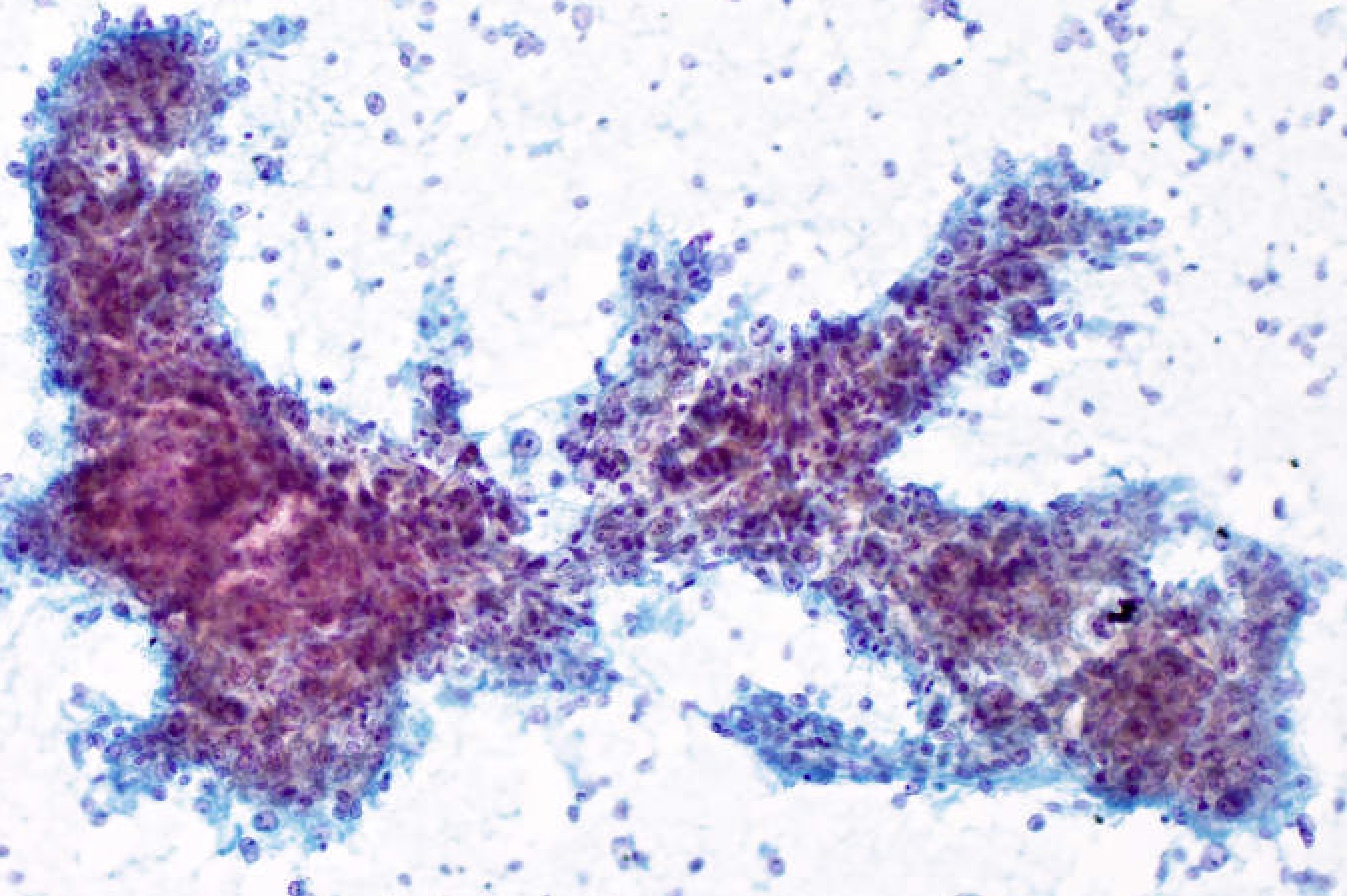
Thickened trabeculae
Pseudoglandular structures
Endothelial wrapping
Transgressing vessel
Transversing vessel
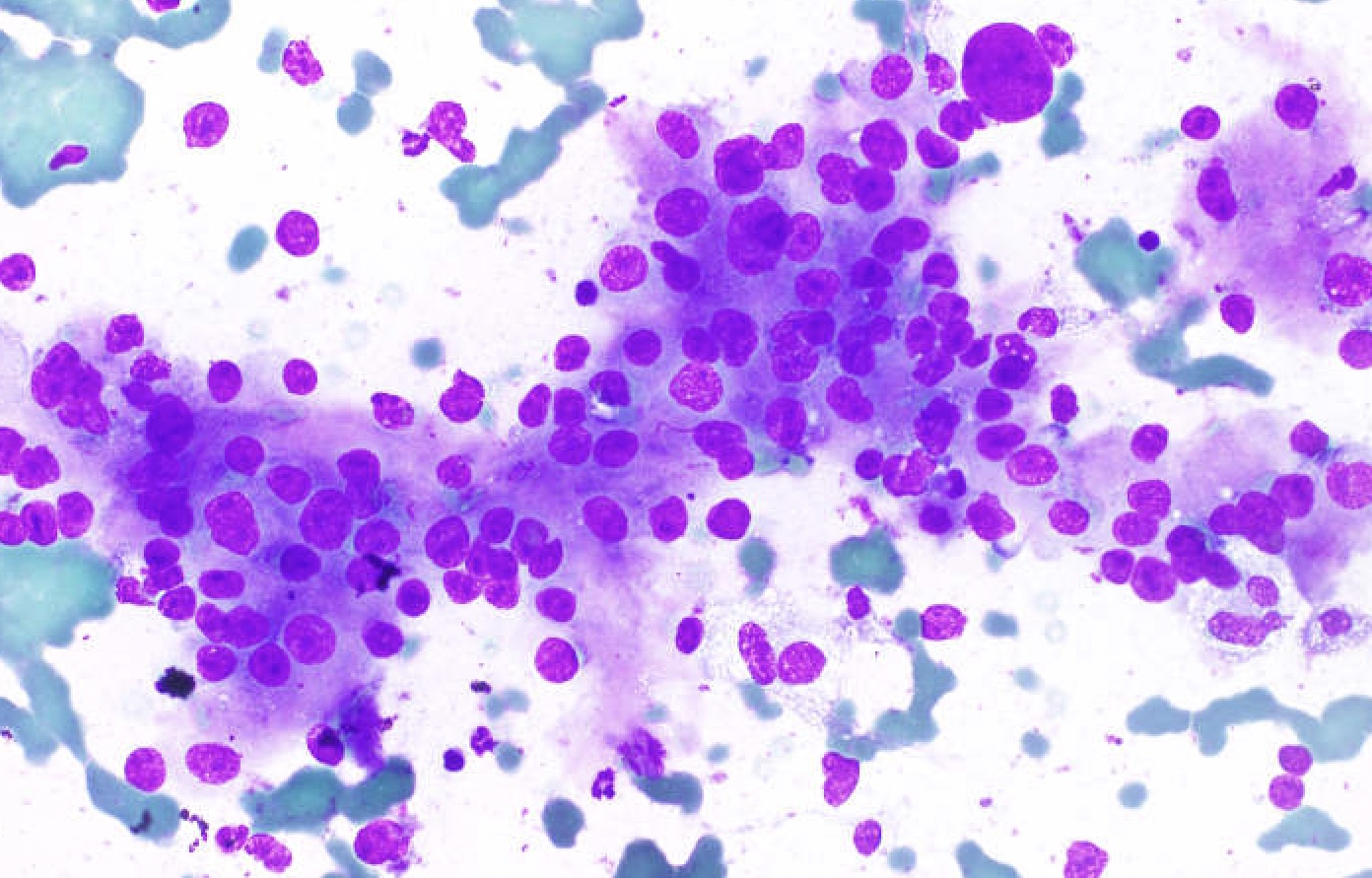
Enlarged nuclei and increased N/C ratio
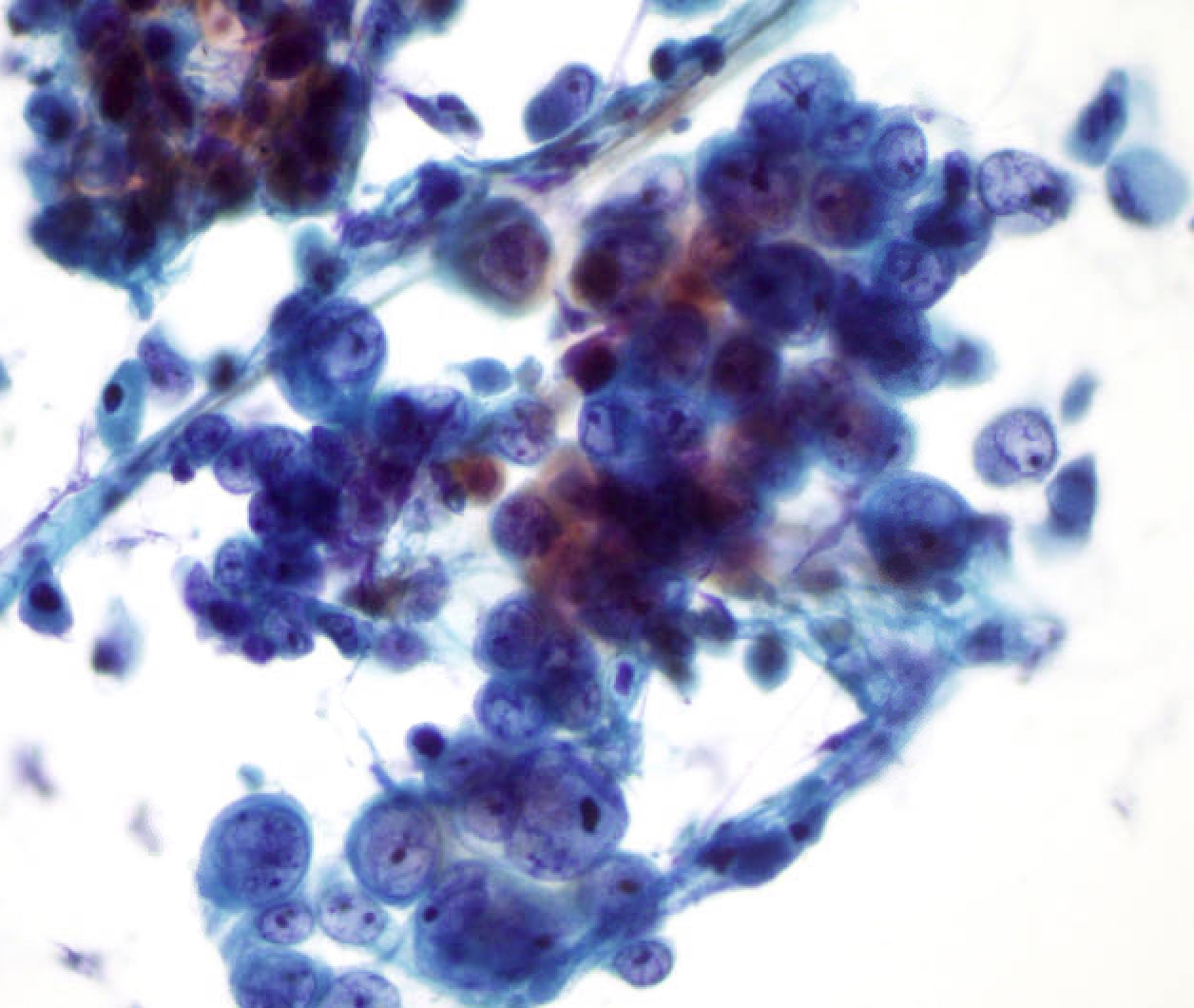
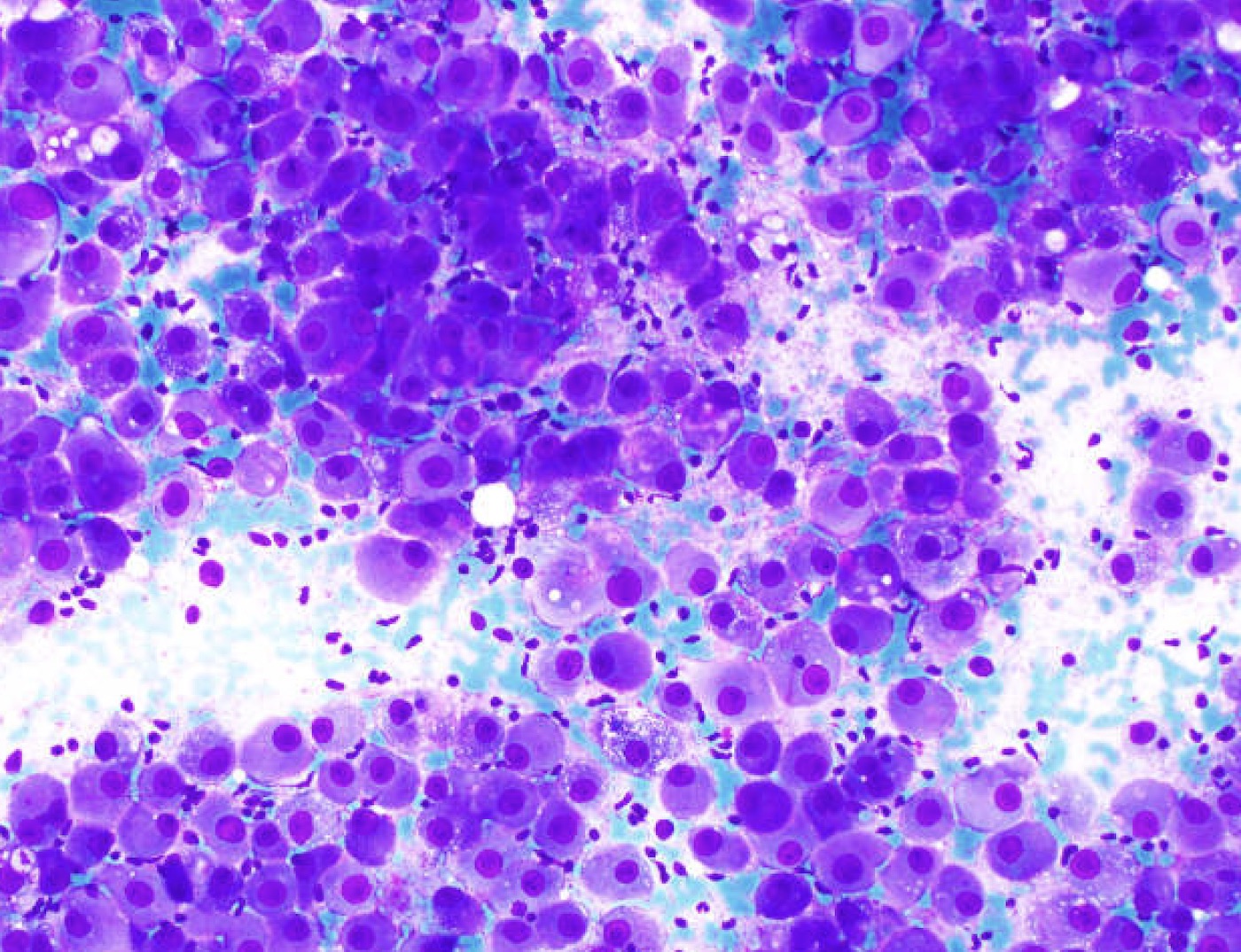
Enlarged nuclei and prominent nucleoli
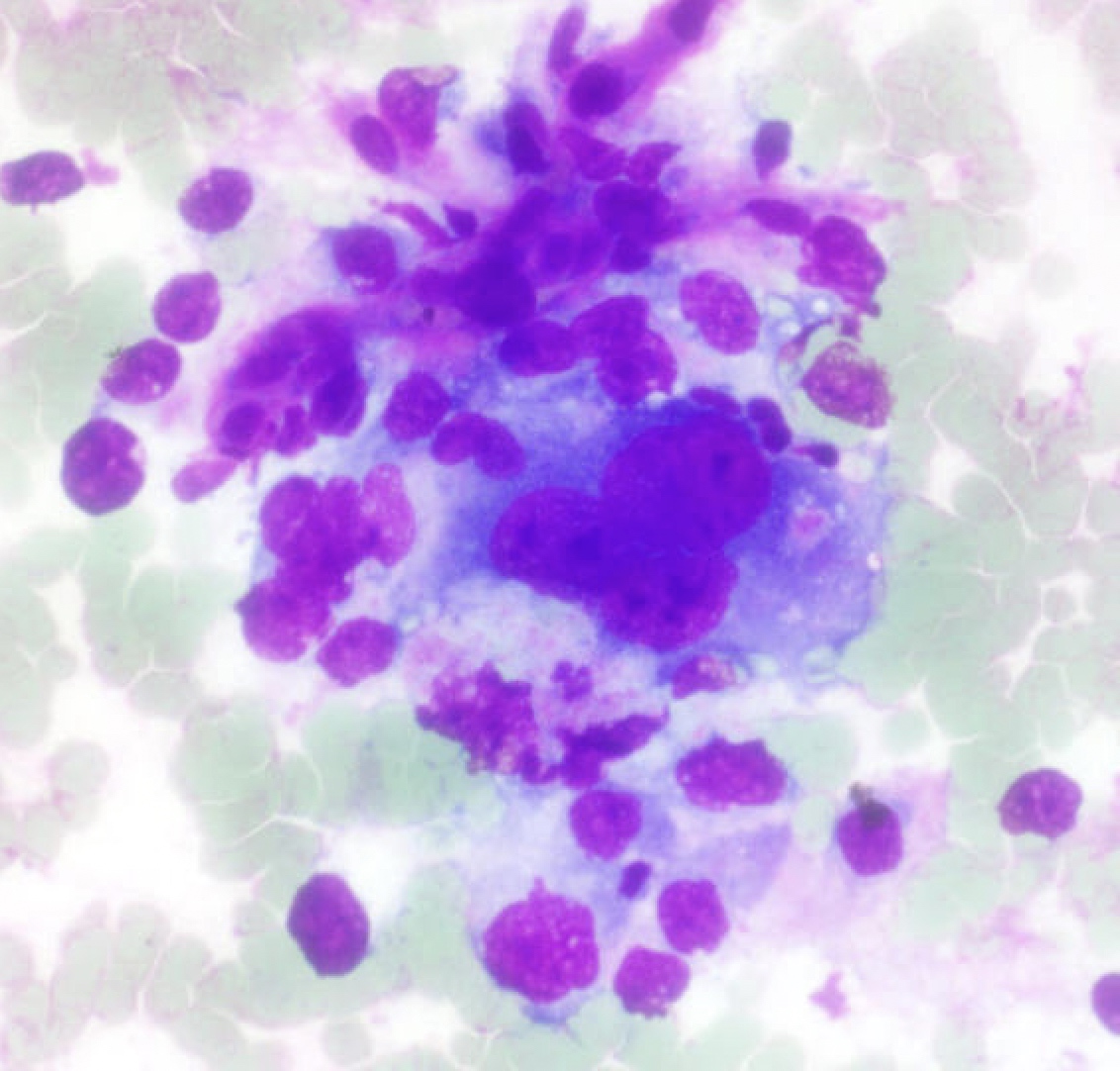
Multinucleated tumor cells
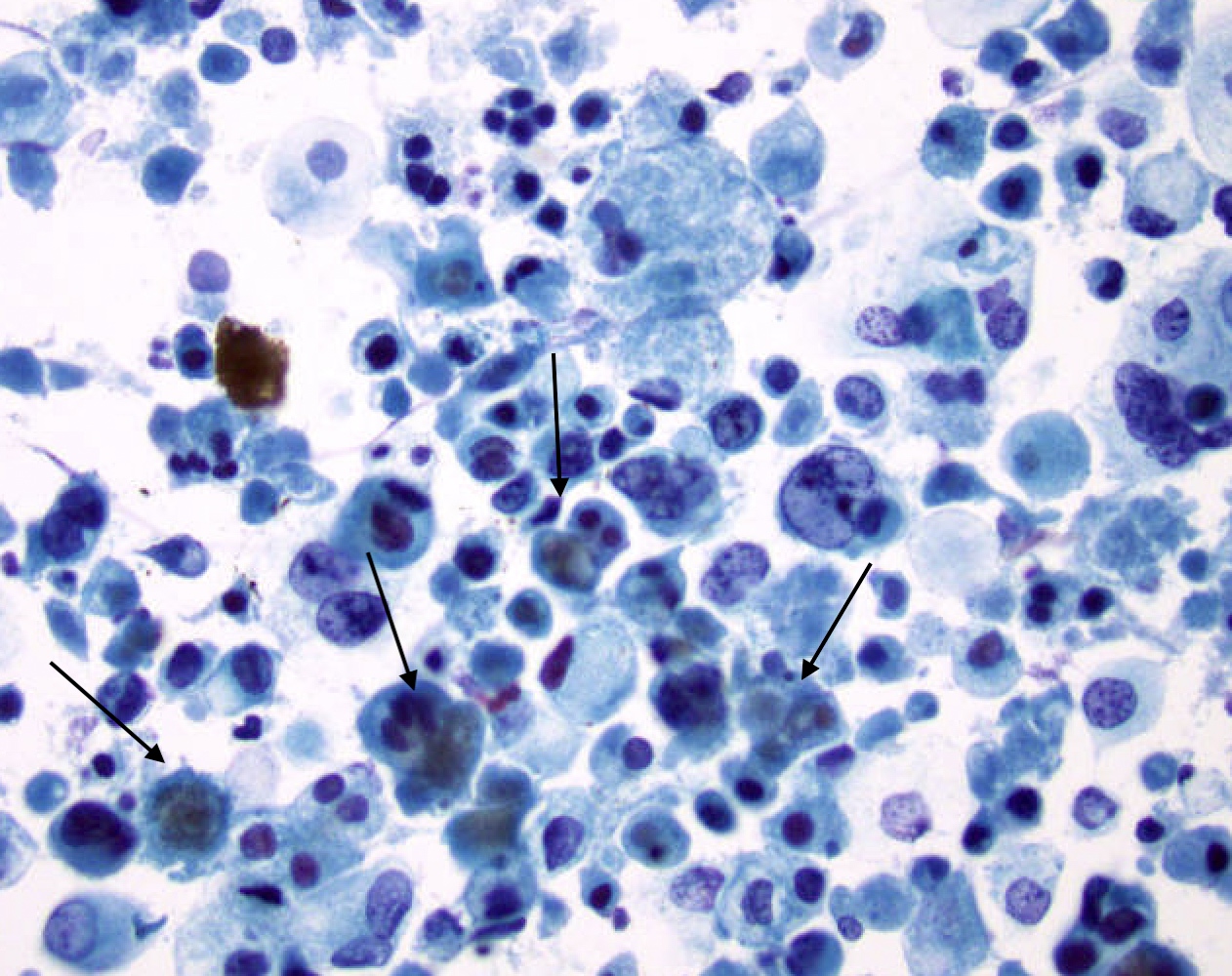
Bile production
Cell block - well differentiated HCC
Cell block - poorly differentiated HCC
Cell block - multinucleated tumor cells
Images hosted on other servers:

Well differentiated neoplasm

Moderately differentiated neoplasm


Poorly differentiated neoplasm (marked nuclear pleomorphism)

Trabecular and pseudoacinar patterns

Pseudoacinar pattern


Fatty change

Mallory hyaline

Fibrolamellar variant

Sarcomatoid change

HepPar1, CEA and CD31 IHC

Reticulin stain
- Liver, mass, ultrasound guided aspiration biopsy (smears and cell block):
- Moderately differentiated hepatocellular carcinoma, positive for malignancy (see comment)
- Comment: Cellular sample showing atypical monotonous cells with enlarged nuclei, abundant granular cytoplasm arranged in trabecular and pseudoglandular patterns with transgressing vessels. Single bare nuclei are present in the background. Immunohistochemical stains show that the neoplastic cells are reactive for HepPar1, arginase1, glypican 3. Polyclonal CEA stain shows a canalicular pattern. Immunohistochemical stains for CK7 and CK20 are nonreactive. The morphologic and immunohistochemical profile supports the diagnosis of moderately differentiated hepatocellular carcinoma.
- Normal liver:
- Presence of normal appearing hepatocytes may represent a sampling error, hepatic adenoma, focal nodular hyperplasia or regenerative nodule; therefore, correlation with imaging is needed to establish if there was a sampling issue
- Features of normal appearing hepatocytes:
- Low nuclear to cytoplasmic ratio
- No nuclear atypia
- No prominent nucleoli
- Hepatic adenoma:
- Normal appearing hepatocytes
- Normal trabeculae (1 - 3 cells thick)
- No transgressing vessels
- Intact reticulin and glypican 3 negative
- Focal nodular hyperplasia:
- Normal appearing hepatocytes
- Normal trabeculae (1 - 3 cells thick)
- No transgressing vessels
- Bile duct cells
- Fragments of fibrous stroma
- Intact reticulin and glypican 3 negative
- Regenerative nodule:
- Normal appearing hepatocytes
- Normal trabeculae (1 - 3 cells thick)
- Intact reticulin
- Dysplastic nodule:
- Cytologic atypia
- Normal trabeculae (1 - 3 cells thick)
- Intact reticulin
- Well differentiated neuroendocrine tumor:
- Salt and pepper chromatin, rosette formation
- Synaptophysin+, chromogranin+, CD56+, INSM1+
- Angiomyolipoma:
- Intrahepatic cholangiocarcinoma:
- Intracytoplasmic mucin
- Glandular architecture
- Positive for mucicarmine
- Immunohistochemistry: positive for CK7, CK19, MOC31; negative for hepatocytic markers
- Combined hepatocellular / cholangiocarcinoma:
- Challenging diagnosis
- Dual population with HCC features and adenocarcinoma morphologic and immunohistochemical profile (Acta Cytol 1997;41:1269)
- Diagnostic pitfall if one of the components is not sampled
- Metastatic neoplasms:
- Metastatic neoplasms are the most common malignancy in the liver
- History of other primary neoplasm
- Often no evidence of cirrhosis in background liver
- Negative for hepatocytic immunohistochemical stains
- Specific morphologic and immunohistochemical features can indicate primary site
- Gastric adenocarcinoma:
- Intracellular mucin, glandular architecture, signet ring cell morphology
- Colon adenocarcinoma:
- Gastrointestinal stromal tumor:
- Spindle morphology
- c-KIT / CD117+, DOG1+
- Breast carcinoma:
- Ductal carcinomas show larger cluster of neoplastic cells, whereas lobular carcinoma can have bland appearance with discohesive pattern and signet ring cell morphology
- GATA3+, mammaglobin+, ER / PR variable, p40-, CK7+, CK20-
- Lung adenocarcinoma:
- Thyroid carcinoma:
- Renal cell carcinoma (clear cell):
- Urothelial carcinoma:
- Prostate adenocarcinoma:
- Neuroendocrine neoplasms:
- Salt and pepper chromatin, rosette formation
- Synaptophysin+, chromogranin+, CD56+, INSM1+
- Small cell carcinoma:
- Small cells with hyperchromatic nuclei and nuclear molding
- Synaptophysin+, chromogranin+, CD56+, INSM1+
- Squamous cell carcinoma:
- Melanoma:
- Sarcomas:
- Spindled, round or pleomorphic cells
- Gastric adenocarcinoma:
Which of the following serum markers has the highest diagnostic accuracy for the condition shown in the above smear obtained from a liver fine needle aspiration?
- AFP
- CA125
- CA19-9
- CEA
- PSA
- Cholangiocarcinoma
- Hepatocellular adenoma
- Hepatocellular carcinoma
- Lymphoma
- Metastatic carcinoma
