
Liver & intrahepatic bile ducts
Liver transplantation
Early onset graft injury
Transplantation - surgical / vascular complications
Editorial Board Members: Monika Vyas, M.D., Kimberley J. Evason, M.D., Ph.D.

Last author update: 4 October 2023
Last staff update: 4 October 2023
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Liver transplantation complications


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Oliveira RC. Transplantation - surgical / vascular complications. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertransplantcomplications.html. Accessed April 3rd, 2025.
Definition / general
- Complications after liver transplantation
- Biliary and vascular complications are common
- Important cause of posttransplant morbidity
Essential features
- Biliary and vascular complications are common events after liver transplantation
- These events have implication on overall survival and quality of life of patients
- Retransplantation may be necessary
Terminology
- Post liver transplantation biliary complications include:
- Anastomotic strictures
- Nonanastomotic strictures
- Bile leaks
- Bile duct stones
- Bilomas
- Sphincter of Oddi dysfunction
- Ischemic cholangiopathy
- Thrombosis
- Ischemia reperfusion injury
- Lipopeliosis
ICD coding
- ICD-10: T86.4 - complications of liver transplant
Epidemiology
- A major complication in patients submitted to liver transplantation (GE Port J Gastroenterol 2018;25:1)
- Biliary complications arise in 10 to 15% of patients (BMJ Open Gastroenterol 2022;9:e000778)
- Risk of biliary complications is higher in living donor transplantation, up to 30% (Clin Liver Dis (Hoboken) 2017;10:63)
- Biliary complications are associated with 13% of retransplantation and 19% of mortality (Clin Transplant 2004;18:647)
- Number of arterial anastomoses, low donor weight and previous history of abdominal surgeries are risk factors for hepatic artery thrombosis (Liver Transpl 2014;20:713)
Sites
- Liver
- Bile ducts
- Hepatic artery
- Portal vein
Pathophysiology
- Bile duct injury is the result of a multifactorial process
- Cold / warm ischemia, perfusion injury, bile salt toxicity and immune mediated lesions have been described as causative factors, especially for nonanastomotic strictures (Virchows Arch 2012;461:41)
- Lesions of the peribiliary vascular plexus and deep biliary glands are thought to be the main cause of nonanastomotic strictures (J Hepatol 2014;60:1172)
- Graft injury, especially with prolonged cold (> 12 hours) and warm (> 90 minutes) ischemia time, is prone to induce biliary injury (Clin Liver Dis (Hoboken) 2016;7:73)
- Donor graft quality: donors with older age with steatosis > 30% and hypotension are described as smaller for size allograft (Clin Liver Dis (Hoboken) 2016;7:73)
Etiology
- Ischemia
- Inflammation
- Infection
- Surgery complications
- Rejection
Clinical features
- If thrombosis
- Abdominal pain
- Fever (if infection)
- If biliary complications
- Jaundice
- Fecal acholia
- Brown urine
- Ischemia reperfusion injury
- Fatigue
- Jaundice
Diagnosis
- Usually by a combination of clinical, laboratory and radiologic findings
Laboratory
- If biliary complications
- Alkaline phosphatase, gamma glutamyl transferase, total bilirubin and conjugated bilirubin increase
- Nonspecific changes (Ann Hepatobiliary Pancreat Surg 2022;26:76)
- Liver enzyme increase, namely aspartate aminotransferase (AST)
- International normalized ratio (INR) increase
- Acidosis
Radiology description
- If biliary complications
- Extravasation of contrast material in the region of the anastomosis on endoscopic retrograde cholangiopancreatography (Clin Liver Dis (Hoboken) 2016;7:73)
- Cholangiography is able to detect strictures in the bile ducts (Clin Liver Dis (Hoboken) 2016;7:73)
- If thrombosis
- Contrast enhanced ultrasound shows an absence of Doppler flow in the hepatic artery proper and the intrahepatic branches; it has a sensitivity of nearly 100% (Clin Radiol 2020;75:845, Radiographics 2022;42:702)
Radiology images
Contributed by Ricardo Martins, M.D.
Portal vein thrombosis
Hepatic artery thrombosis
Acute portal vein thrombosis
Nonanastomotic strictures
Prognostic factors
- Early elevation of laboratory values after liver transplantation is associated with biliary stenosis (Ann Hepatobiliary Pancreat Surg 2022;26:76)
- Severe liver injury is defined by AST > 3,000 and INR ≥ 2.5, or acidosis (arterial pH ≤ 7.3 or venous pH ≤ 7.25 or lactate ≥ 4 mmol/L) (Clin Liver Dis (Hoboken) 2016;7:73)
- Encephalopathy is a factor of worse prognosis
Case reports
- 30 year old woman with acute portal vein thrombosis after liver transplant (World J Hepatol 2019;11:234)
- 51 year old man with recurrent hepatic artery thrombosis following living donor liver transplant (SN Compr Clin Med 2021;3:2629)
- 60 year old man with an accidentally ligated and subsequently completely unflushed common bile duct (Int J Surg Case Rep 2017;41:200)
Treatment
- If biliary complications
- Endoscopic retrograde cholangiopancreatography (ERCP) with balloon dilation or stenting
- ERCP with sphincterotomy
- Endoscopic ultrasound drainage
- If thrombosis
- Thrombolysis
- Ischemia reperfusion injury
- Shorter ischemia times (cold or warm)
- Use of machine reperfusion on liver graft
- In cases of disease progression / therapeutic failure
- Retransplant
- References: World J Hepatol 2016;8:36, World J Hepatol 2021;13:66, World J Hepatol 2015;7:2890, Visc Med 2022;38:243, Hepatobiliary Surg Nutr 2019;8:490
Gross description
- Biliary complications
- Liver explant with biliary obstruction / fibrosis of the bile duct; on cut section, the liver shows mild to moderate fibrosis with bile casts and green tone
- Vascular complications
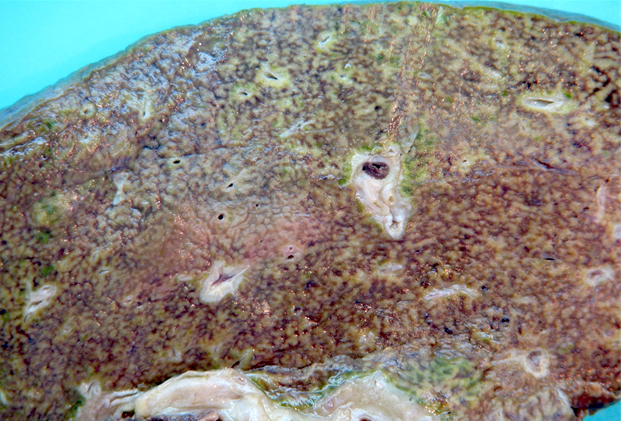
- Liver explant with hepatic artery / portal vein thrombosis, with complete / partial occlusion of vessel(s); on cut section, the liver is hemorrhagic and congestive
Gross images
Contributed by Rui Caetano Oliveira, M.D., Ph.D.
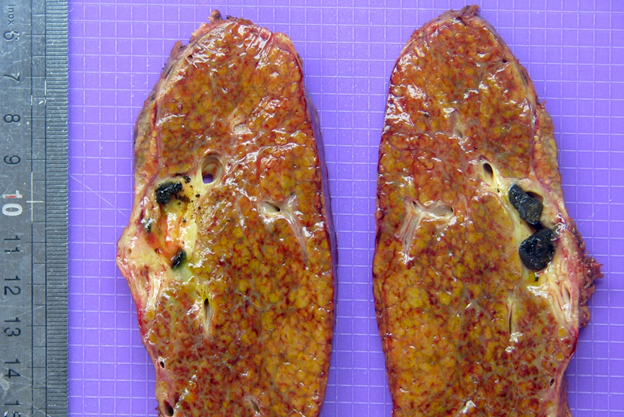
Bile casts in ischemic cholangiopathy

Liver necrosis

Liver necrosis cut section

Liver necrosis cut section
Liver thrombosis
Microscopic (histologic) description
- Ischemia reperfusion injury appears as perivenular ballooning and cholestasis, neutrophilic infiltrate or hepatocyte necrosis in centrolobular regions (in the more severe lesions)
- Lipopeliosis corresponds to the release of fat from ischemia reperfusion hepatocytes in to the extracellular space, inducing sinusoidal compression, blood flow obstruction and ischemic necrosis
- Biliary pattern of fibrosis is common in ischemic cholangiopathy
- Ductular reaction and hepatocyte biliary metaplasia in cases of bile duct obstruction, associated with portal tract edema
- Sinusoidal dilation and congestion are common in venous drainage complications
- Ischemic necrosis is common in thrombosis
- Reference: Diagn Histopathol 2018;24:508
Microscopic (histologic) images
Contributed by Rui Caetano Oliveira, M.D., Ph.D. and @RaulSGonzalezMD on Twitter
Ischemic cholangiopathy
Sinusoidal dilation
Hemorrhage
Foci of necrosis
Severe necrosis
Extensive necrosis
Extensive liver necrosis
Venous portal tract thrombosis
Major portal branch thrombosis
Bile duct ulceration
Extensive ulceration
Bile duct necrosis
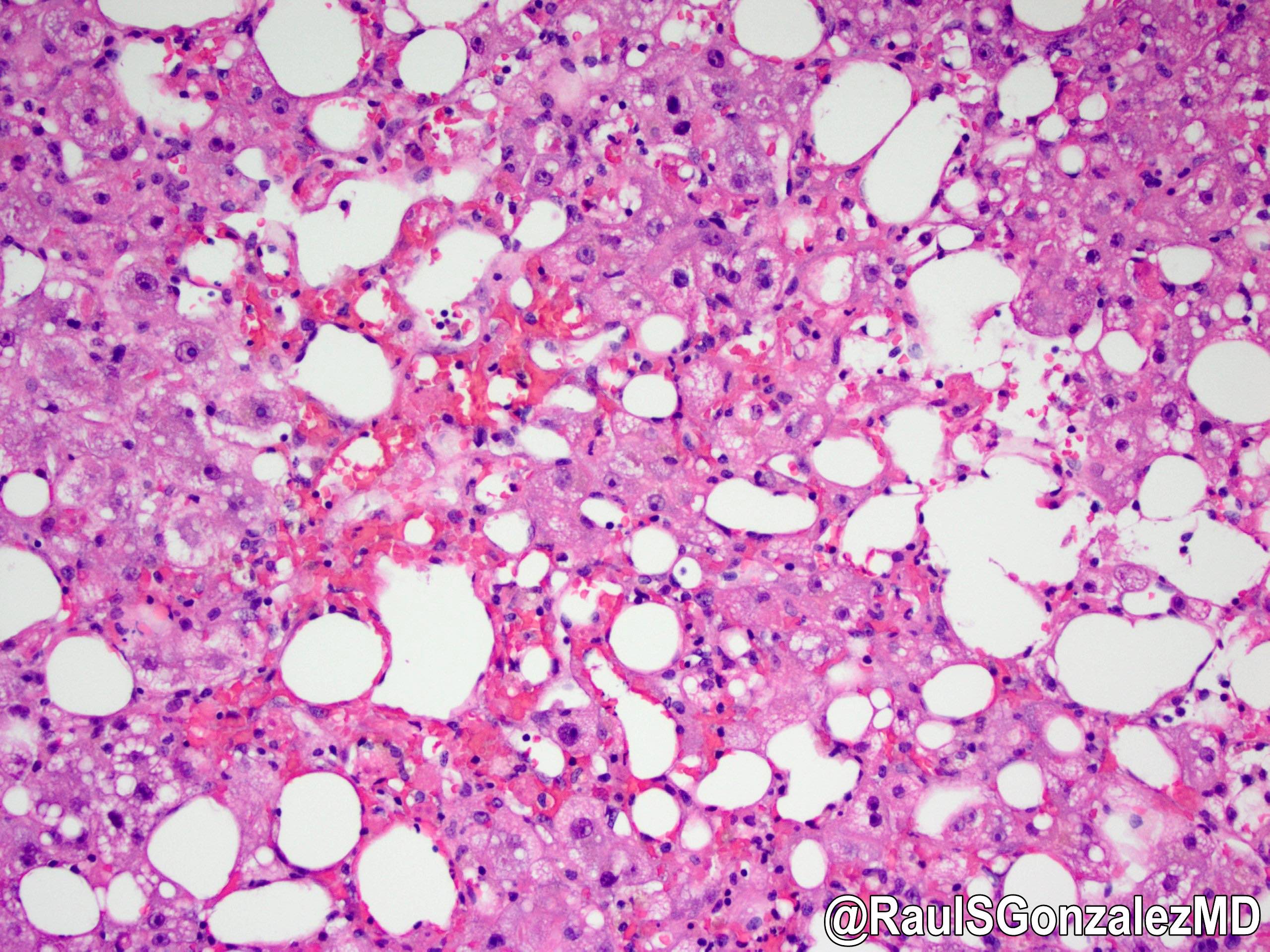
Lipopeliosis following liver transplantation
Biliary cirrhosis
Ductular reaction and biliary metaplasia
Copper accumulation
Positive stains
- CK7 may be useful in demonstrating ductular reaction and hepatocyte biliary metaplasia in cases of biliary obstruction
- Rhodanine stain usually demonstrates copper deposits in periportal hepatocyte in cases of chronic biliary obstruction
Sample pathology report
- Liver, retransplant:
- Biliary cirrhosis due to ischemic cholangiopathy (see comment)
- Comment: There is ulceration of the right biliary duct, with severe inflammation consisting of neutrophils and foamy histiocytes. Hepatic parenchyma exhibits architectural changes, with bridge forming cirrhosis in a jigsaw pattern. CK7 demonstrates a ductular reaction and there is copper accumulation in the periseptal hepatocytes.
Differential diagnosis
- Biliary complications:
- T cell mediated rejection (the major differential diagnosis) (Hepatology 2022;75:1014):
- Portal tract inflammation with eosinophils
- Endotheliitis
- Bile duct damage
- Chronic ductopenic rejection (Hepatology 2022;75:1014):
- Atrophic appearing duct with damaged and attenuated epithelium
- Bile duct absent in portal tract
- Recurrent primary sclerosing cholangitis (PSC):
- Recurs in ~20 - 30% of patients by 5 years of transplantation
- Strictures are more common in patients transplanted for PSC than in those transplanted for other diseases
- Typical histological features include ductular reaction, mixed inflammation, lobular cholestasis, periductal fibrosis and bile infarcts
- Requires clinical history of liver transplantation due to PSC, since histological features are very similar to biliary obstruction (Transpl Int 2010;23:971)
- T cell mediated rejection (the major differential diagnosis) (Hepatology 2022;75:1014):
- Vascular complications:
- Paracetamol overload (Vet World 2019;12:1682):
- Clinical information of paracetamol intake
- Necrosis in acinar zone 3, or zone 2 or 3
- Sepsis (World J Gastroenterol 2008;14:1389):
- Inflammation with variable degrees of polymorphonuclear leukocyte infiltration, cholestasis and steatosis
- Liver architecture is preserved
- Intrahepatocytic or canalicular cholestasis may be found
- Hyperacute rejection:
- Occurs a few hours after liver transplantation
- Histological features include hemorrhagic necrosis, vascular thrombi and neutrophilic infiltrate
- Paracetamol overload (Vet World 2019;12:1682):
Board review style question #1
Liver retransplantation is performed and the image above shows the gross examination. Which of the following is the probable cause?
- Acute rejection
- Biliary complications
- Portal thrombosis
- Primary non function
Board review style answer #1
B. Biliary complications. The evidence of bile casts and biliary dilation in the context of liver transplantation is highly suggestive of ischemic cholangiopathy.
Comment Here
Reference: Transplantation - surgical / vascular complications
Comment Here
Reference: Transplantation - surgical / vascular complications
Board review style question #2
Which of the following is thought to be the main cause of nonanastomotic strictures following liver transplantation?
- Cytomegalovirus infection
- Lesions of the peribiliary vascular plexus and deep biliary glands
- Liver size
- Rejection
Board review style answer #2
B. Lesions of the peribiliary vascular plexus and deep biliary glands. Nonanastomotic strictures are usually associated with vascular injury of the peribiliary vascular plexus, inducing a hypoxia environment. The lesion of the deep biliary glands, a niche for stem cells, is also associated with the impairment of tissue repair.
Comment Here
Reference: Transplantation - surgical / vascular complications
Comment Here
Reference: Transplantation - surgical / vascular complications
