

Liver & intrahepatic bile ducts
Infectious nonviral
Schistosomiasis
Editorial Board Member: Claudio Luchini, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 4 September 2024
Last staff update: 4 September 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Schistosomiasis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Abdalla AM, Gonzalez RS. Schistosomiasis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverschisto.html. Accessed November 28th, 2024.
Definition / general
- Schistosomiasis is a parasitic disease caused by Schistosoma blood flukes
- Liver infection results in fibrosis and obstruction
Essential features
- Most common cause of portal hypertension worldwide
- Adult worms settle in the portal vein and produce thousands of eggs, which leads to inflammation and subsequent periportal fibrosis and portal hypertension (Pathology 2008;40:161)
- Portal fibrosis in schistosomiasis forms thick collagen bundles scattered among fibroblasts
Terminology
- Also known as bilharziasis (first described in 1852 by Theodor Bilharz) and snail fever
ICD coding
- ICD-10: B56.1 - schistosomiasis due to Schistosoma mansoni
Epidemiology
- Schistosomiasis is the second most common human parasitic infection, affecting almost 240 million people worldwide; more than 700 million people live in high risk areas (World Health Organization: Schistosomiasis (Bilharzia) [Accessed 7 August 2024])
- Risk factors include travel to endemic areas and exposure to contaminated freshwater with poor sanitation
- Schistosoma mansoni: Southern and Subsaharan Africa, Nile River Valley in Sudan and Egypt, South America (Brazil, Suriname, Venezuela) and Caribbean
- Schistosoma japonicum: Southeast Asia and China
- Schistosoma mekongi: Cambodia and Laos
- Children are more exposed as they swim in water contaminated with the infectious cercariae
Pathophysiology
- After being excreted in feces into fresh water, Schistosoma eggs hatch and gives rise to ciliated and motile miracidia that penetrate the intermediate host, a snail known as Biomphalaria
- Within the snail, the life cycle progresses through asexual multiplication and the release of cercariae (the infectious forms for humans) into water
- Cercariae penetrate the skin of humans and migrate to the lungs and then the mesenteric veins (J Clin Transl Hepatol 2014;2:212)
- Female worms release eggs, which can travel by portal blood into the liver (Nature 1978;273:609)
- Tissue injury in chronic schistosomiasis is mediated by egg induced granulomas; in the liver, this leads to portal fibrosis (Mem Inst Oswaldo Cruz 2004;99:51)
- Schistosome eggs also release specific substances that directly trigger the production of osteopontin in liver cells
- This protein is known to promote liver fibrosis by activating hepatic stellate cells, causing them to transform into myofibroblasts (Clin Sci (Lond) 2015;129:875)
Diagrams / tables
Images hosted on other servers:

Schistosoma life cycle

Geographic distribution of schistosomiasis
Clinical features
- Schistosomiasis is the most common cause of portal hypertension worldwide and does not cause cirrhosis
- Within 24 hours after penetration of cercariae, a pruritic rash (swimmer's itch) occurs for 2 - 5 days
- Acute manifestations typically diminish; however, the infection progresses to a chronic phase
- 2 - 8% of patients with heavy chronic infection develop periportal fibrosis (Symmers pipestem fibrosis) and can present with hepatosplenomegaly and esophageal varices, which can lead to gastrointestinal hemorrhage (Int J Parasitol 2014;44:1055)
- Hepatic function is usually preserved
Diagnosis
- Definite diagnosis of schistosomiasis requires identification of schistosome eggs in feces or via tissue sampling
- Stool examination is typically performed with concentration methods (Kato-Katz technique)
- Ultrasound helps determine stage of liver fibrosis (Radiology 1984;153:777)
- Periportal fibrosis appears as an echogenic band surrounding portal vessels extending from the hilum to the periphery of the liver
- In advanced cases, the liver surface may appear nodular
- MRI can also be used (Radiol Case Rep 2016;11:152)
Laboratory
- Direct antigen assay in stool, urine or blood (circulating anodic antigen [CAA] and circulating cathodic antigen [CCA]) (Lancet 2006;368:1106)
- Indirect antibody assay by serology
- Liver function tests are usually normal
Radiology description
- Irregular hepatic surface and septal fibrosis
- Mosaic pattern: echogenic septa outlining polygonal areas of relatively normal liver parenchyma
- Grading of periportal fibrosis thickness on ultrasonography is as follows (Am J Trop Med Hyg 1992;46:403)
- Grade 1: thickness ranges from 3 to 5 mm
- Grade 2: thickness ranges from 5 to 7 mm
- Grade 3: thickness above 7 mm
- S. mansoni usually exhibits portal vein wall thickening with increased echogenicity (bullseye appearance)
Radiology images
Images hosted on other servers:


Hyperechoic pipestem fibrosis

Periportal fibrosis
Prognostic factors
- Patients with coexisting hepatitis B virus (HBV), hepatitis C virus (HCV), HIV or malaria infections have worse prognoses (Liver 2000;20:281)
- Portal fibrosis may completely regress following curative treatment of the parasites (Mem Inst Oswaldo Cruz 1992;87:129, Am J Trop Med Hyg 1991;44:444)
Case reports
- 26 year old man with massive splenomegaly (Acta Gastroenterol Belg 2018;81:93)
- 38 year old woman with jaundice and a history of tuberculosis (Cureus 2023;15:e35169)
- 39 year old woman with 1 month history of fever and fatigue (Intern Med 2019;58:2495)
- 40 year old woman with intestinal and hepatic schistosomiasis (IDCases 2022;27:e01383)
- 47 year old man with abnormal liver enzymes and ultrasound (Clin Case Rep 2020;8:1522)
Treatment
- Praziquantel is the treatment of choice for all species of schistosomiasis
Gross description
- Liver appears enlarged and nodular but with normal acinar architecture still preserved (Acta Trop 2008;108:79)
- On cut surface, periportal fibrosis (pipestem fibrosis) forms large plaques of hard white fibrous tissue against a background of normal parenchyma
- Portal tract enlargement and a stellate appearance may be observed
Gross images
Images hosted on other servers:

Enlarged and nodular liver
Microscopic (histologic) description
- Early stages show portal inflammation with eosinophils, Kupffer cell hyperplasia and focal hepatocyte necrosis; ova are usually absent
- In chronic disease, there is a granulomatous reaction to the eggs, which may be associated with portal inflammation and giant cells
- Portal tracts become enlarged and densely sclerotic, forming fibrous septa and sometimes sinusoidal fibrosis but cirrhosis does not occur
- Portal veins are obstructed and destroyed, with proliferation of hepatic artery branches
- Fragmentation of muscle fibers of the media of portal veins, most evident on Masson trichrome stain, is a useful indicator for S. mansoni
- Ova may be sparse, rendering their detection difficult; cutting multiple additional tissue sections can assist
- S. mansoni eggs measure 60 x 140 μm and have a lateral spine
- S. japonicum eggs are 70 - 100 μm long and have a minute lateral spine
- Hemozoin pigment (like that in malaria) may be present, particularly in worms within portal veins but also sometimes in macrophages (Burt: MacSween's Pathology of the Liver, 8th Edition, 2023)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D. and Keloth Pradeep, M.D.
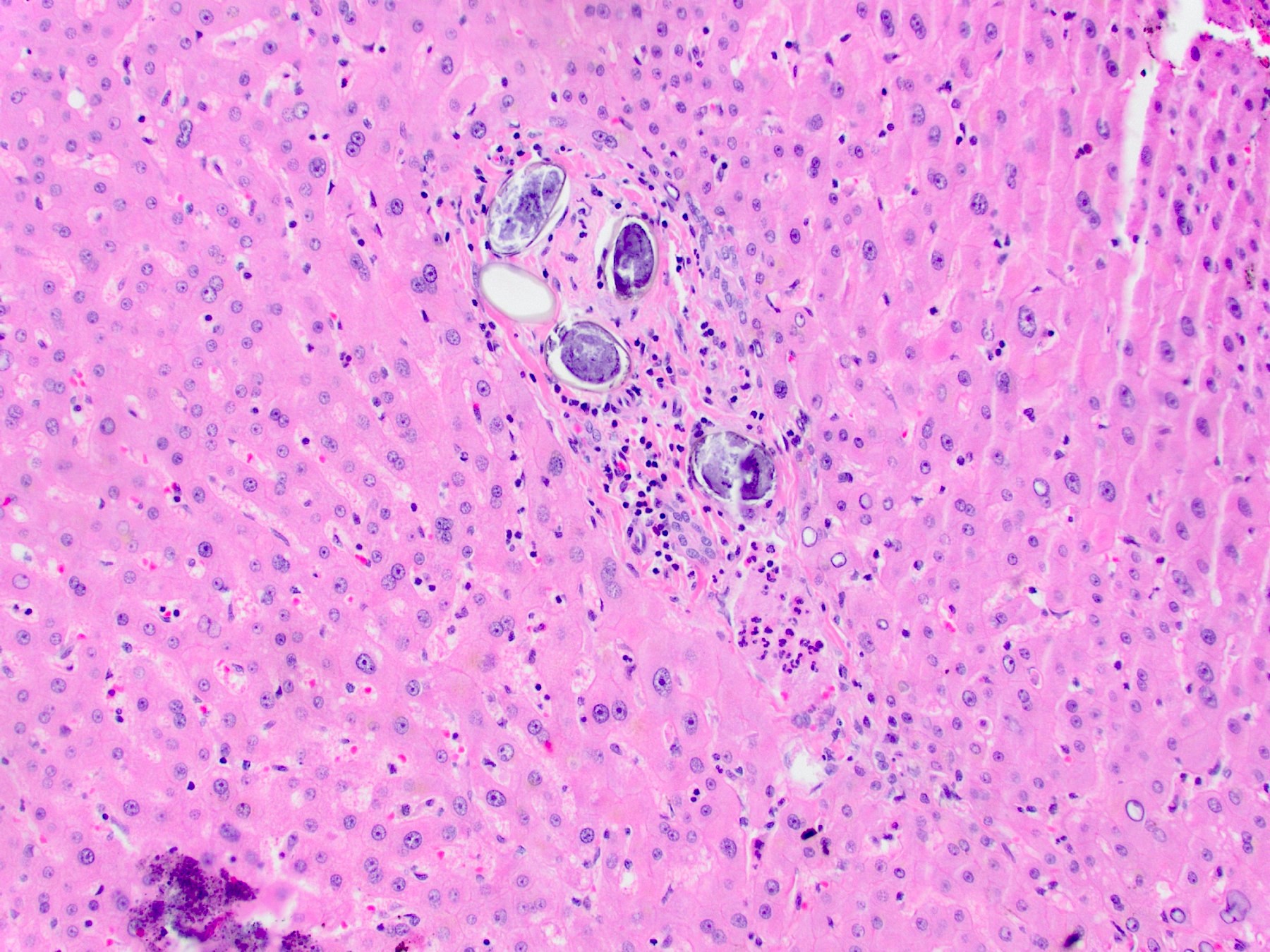
Portal tract eggs
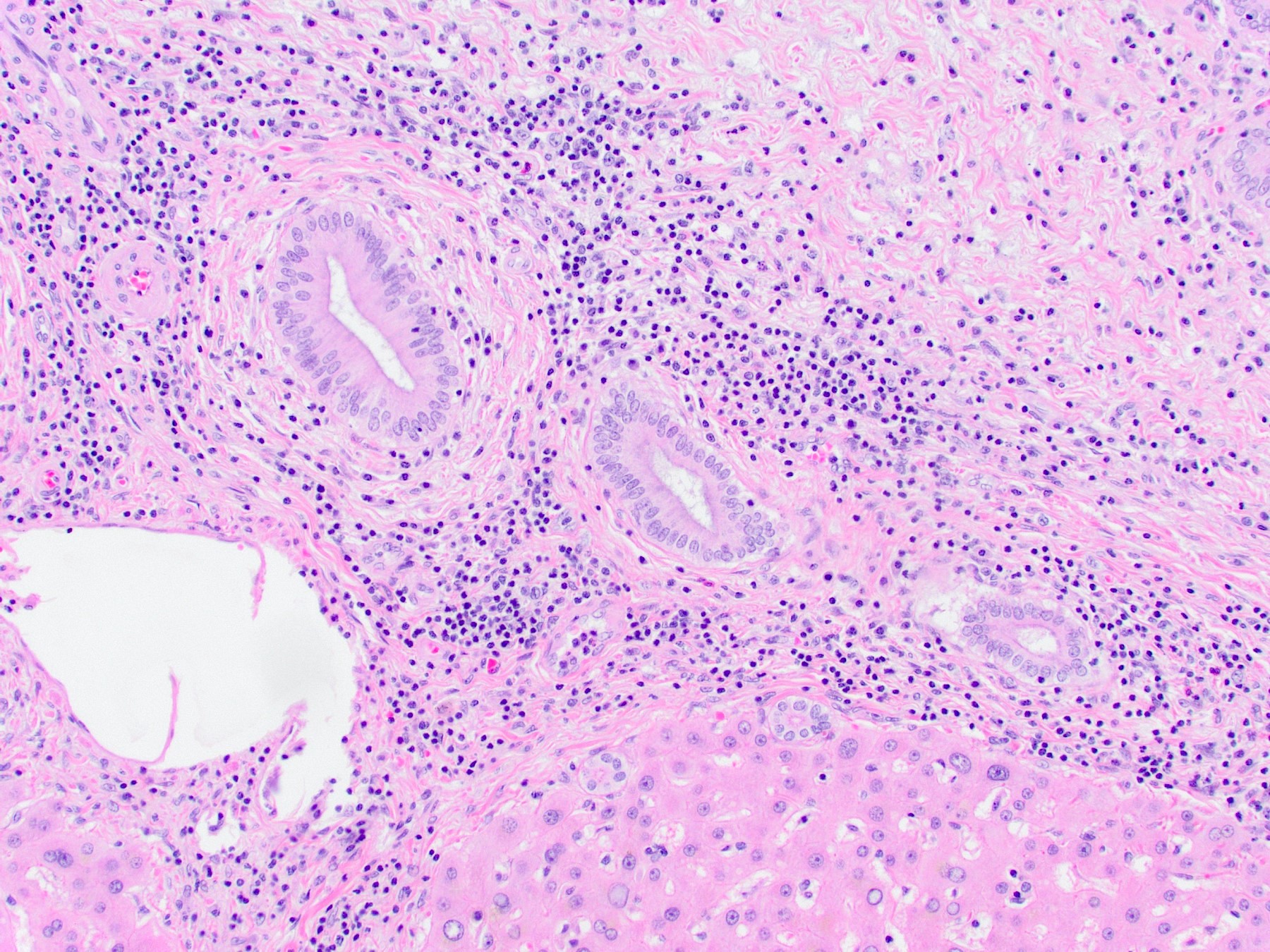
Background portal inflammation

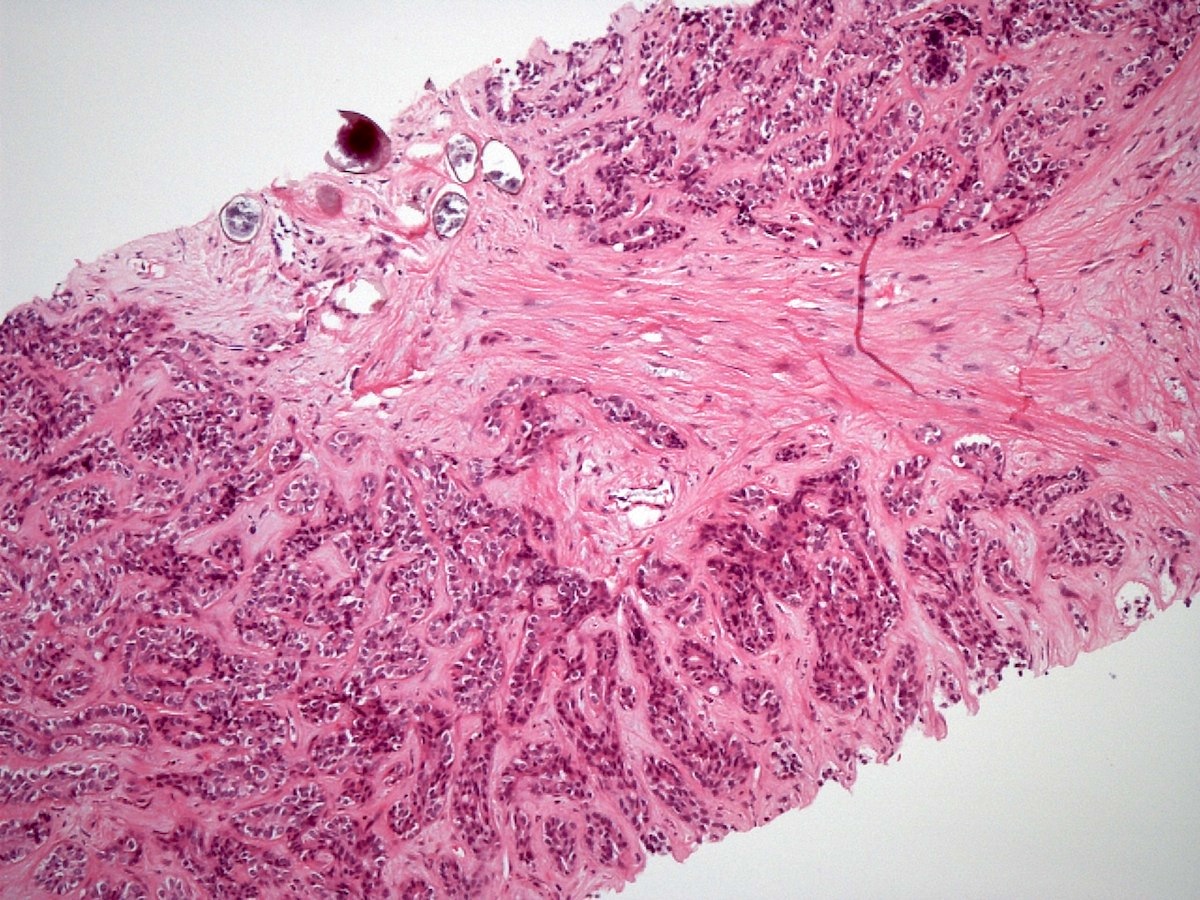
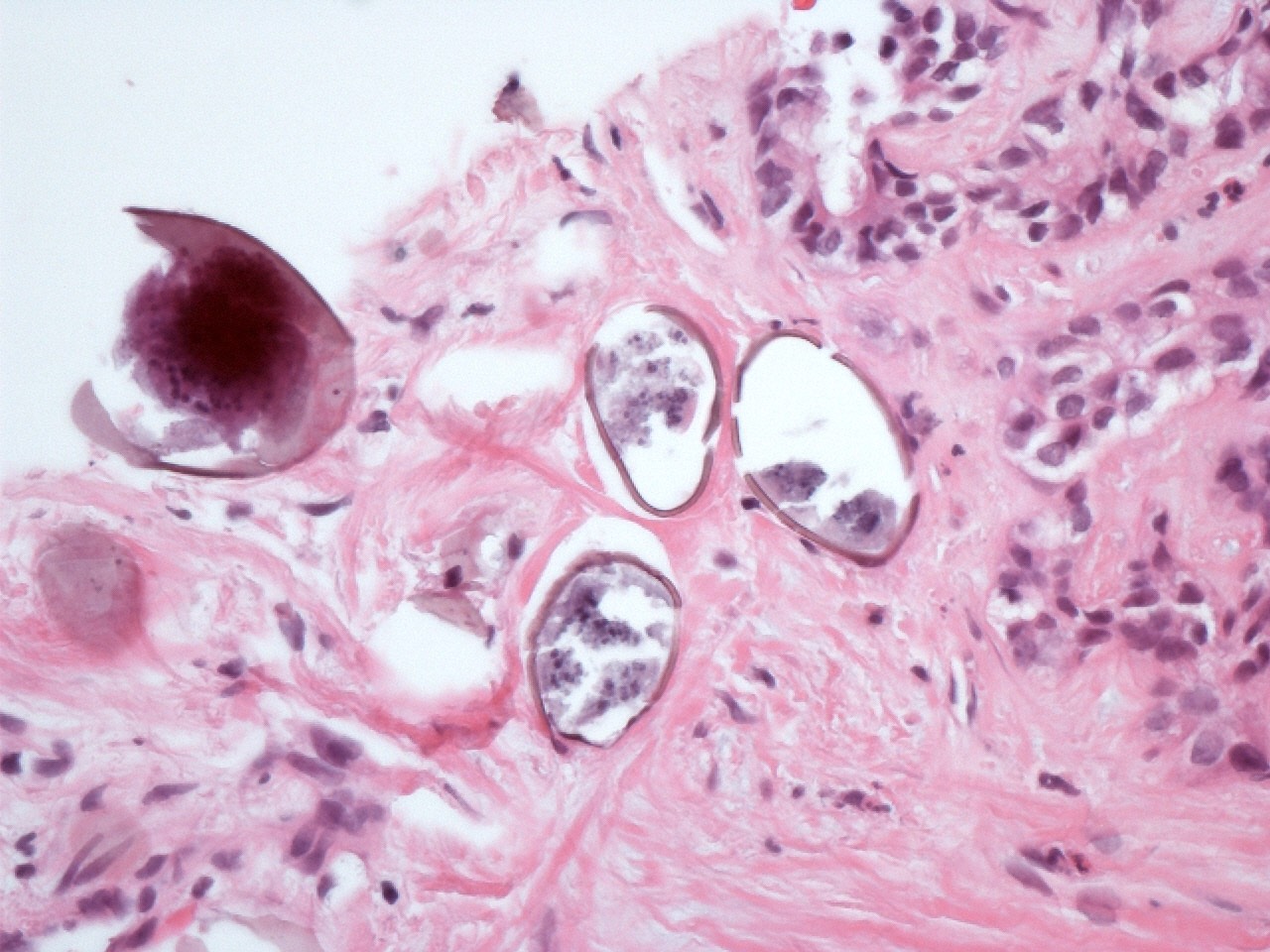
Schistosoma ova and metastatic adenocarcinoma in liver
Positive stains
- S. mansoni eggs stain positive for acid fast stain Ziehl-Neelsen (Am J Trop Med Hyg 1954;3:1066)
Negative stains
Videos
Schistosomiasis in liver
Sample pathology report
- Liver, orthotopic transplantation:
- Liver with dense portal / periportal fibrosis and rare Schistosoma eggs with associated inflammatory reaction (see comment)
- Negative for malignancy
- Comment: The patient's reported history of noncirrhotic portal hypertension is noted. The findings indicate schistosomiasis as the cause.
Differential diagnosis
- Cirrhosis:
- Patients have portal hypertension clinically and abnormal liver findings on imaging
- Cirrhotic livers demonstrate nodular architecture due to extensive fibrous septa, whereas schistosomiasis does not cause this degree of fibrosis
- Ova are not present
- Hepatoportal sclerosis:
- Patients have portal hypertension
- Portal vein intimal fibrosis and delicate septa with phlebosclerosis and atrophic liver parenchyma
- Ova are not present
- Malaria:
- Hemozoin pigment can be seen in macrophages in malaria infection as well as schistosomiasis
- Ova are not present
- Other trematodes may infect the liver and biliary tract, including Clonorchis sinensis, Opisthorchis species and Fasciola hepatica
- These all have their own distinctive appearance on H&E
Board review style question #1
Which of the following statements is true regarding the microscopic description of liver schistosomiasis?
- Granulomatous inflammation and periportal fibrosis are commonly seen
- It is characterized by the presence of atypical hepatocytes
- It shows diffuse fatty infiltration of hepatocytes
- There is loss of the hepatic lobular architecture
Board review style answer #1
A. Granulomatous inflammation and periportal fibrosis are commonly seen. Liver schistosomiasis is characterized by granulomatous inflammation around the trapped schistosome eggs and periportal fibrosis. Answer B is incorrect because hepatocyte atypia does not occur. Answer C is incorrect because hepatocyte steatosis does not occur. Answer D is incorrect because the hepatic lobular architecture remains intact in this condition.
Comment Here
Reference: Schistosomiasis
Comment Here
Reference: Schistosomiasis
Board review style question #2
Hepatic schistosomiasis is the most common cause worldwide of which of the following clinical findings?
- Abnormal liver appearance on ultrasound
- Excretion of ova
- Gastrointestinal hemorrhage
- Portal hypertension
Board review style answer #2
D. Portal hypertension. Liver schistosomiasis is the most common cause of portal hypertension worldwide, despite not causing cirrhosis. Answers A, B and C are incorrect because while these symptoms can occur in patients with hepatic schistosomiasis, it is not the most common cause for them.
Comment Here
Reference: Schistosomiasis
Comment Here
Reference: Schistosomiasis

