
Liver & intrahepatic bile ducts
Biliary tract disease
Primary sclerosing cholangitis
Author: Raul S. Gonzalez, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 15 February 2022
Last staff update: 5 August 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Primary sclerosing cholangitis[TI] liver[TI] pathology full text[sb]


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gonzalez RS. Primary sclerosing cholangitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverpsc.html. Accessed April 3rd, 2025.
Definition / general
- Primary sclerosing cholangitis (PSC) is a biliary disease causing progressive stricturing of the biliary tree, leading to cirrhosis and possibly cholangiocarcinoma
Essential features
- Etiology unclear
- Patients are at increased risk of developing ulcerative colitis and cholangiocarcinoma
- Liver biopsy rarely samples the classic "onion skin" periductal fibrosis, meaning typical imaging findings are more reliable for establishing the diagnosis
ICD coding
- ICD-10: K83.01 - primary sclerosing cholangitis
Epidemiology
- Incidence of roughly 1 per 100,000 person years (Hepatology 2011;53:1590)
- Rates may be lower in developing countries, though reliable data are lacking
Sites
- Large intrahepatic and extrahepatic biliary tree affected, including gallbladder (J Hepatol 2008;48:598)
Etiology
- Possibly autoimmune, though etiology uncertain overall
- Gut microbiome has been suggested to play a role (Ann Transl Med 2016;4:512, World J Gastroenterol 2020;26:2768)
- Siblings of primary sclerosing cholangitis patients more likely to develop primary sclerosing cholangitis, suggesting a genetic component (Clin Gastroenterol Hepatol 2008;6:939)
Diagrams / tables
Images hosted on other servers:

Algorithm for the management of suspected PSC
Clinical features
- M:F = 2:1
- Usually age 30 - 50; can occur in children (Hepatology 2017;66:518)
- Half asymptomatic at diagnosis
- Symptoms: fatigue, pruritus, jaundice, right upper quadrant pain / tenderness
- Increased risk for bacterial cholangitis and cholangiocarcinoma (Clin Liver Dis 2016;20:67)
- Up to 70% also have inflammatory bowel disease (particularly ulcerative colitis, although fewer than 10% with ulcerative colitis have primary sclerosing cholangitis) (Gut Liver 2018;12:17)
- Patients may also have an overlap syndrome with autoimmune hepatitis (J Hepatol 2011;54:374)
Diagnosis
- Firm diagnostic criteria do not exist
- British Society of Gastroenterology recently offered extensive PSC diagnosis guidelines (Gut 2019;68:1356)
- Diagnosis generally established by cholestatic lab findings combined with bile duct stricturing on imaging (Lancet 2018;391:2547)
- Liver biopsy useful to rule out other possibilities but generally cannot establish the diagnosis
Laboratory
- Elevated alkaline phosphatase; variable bilirubin
- Many patients are pANCA positive, though this is nonspecific and serology is not helpful in general (World J Gastroenterol 2008;14:3781)
- Usually negative antimitochondrial antibody
Radiology description
- Multifocal bile duct strictures causing a "beads on a string" appearance on magnetic resonance cholangiography and endoscopic retrograde cholangiopancreatography (J Hepatol 2017;66:1265)
- Patients without such imaging findings who otherwise appear to have primary sclerosing cholangitis may have small duct primary sclerosing cholangitis (Gastroenterology 2008;134:975)
Radiology images
Images hosted on other servers:

Diffuse intrahepatic bile duct stricture

Prominent irregular hepatic ducts
Prognostic factors
- Small duct primary sclerosing cholangitis has a better outcome than typical primary sclerosing cholangitis (Gut 2002;51:731)
- Anti-GP2 IgA autoantibodies reportedly indicate poor prognosis (Gut 2017;66:137)
Case reports
- 26 year old man with primary sclerosing cholangitis and ulcerative colitis with low grade dysplasia (J Crohns Colitis 2013;7:e61)
- 33 year old man with primary sclerosing cholangitis and Crohn's disease (Intern Med 2012;51:2077)
- 84 year old woman with primary sclerosing cholangitis and CREST syndrome (J Med Case Rep 2015;9:272)
- 2 patients with overlap between primary sclerosing cholangitis and primary biliary cholangitis (Dig Liver Dis 2015;47:432)
Treatment
- Ursodeoxycholic acid can improve lab values but does not halt disease progression (Lancet Gastroenterol Hepatol 2016;1:68)
- Obeticholic acid also emerging as a treatment (J Hepatol 2020;73:94)
- Only truly effective treatment is liver transplantation, though disease recurs in 33% of patients (Hum Pathol 2003;34:1127)
Gross description
- Alternating fibrosis / stenosis and ectasia of bile ducts, with bile sludge and calculi
- Liver may be distorted or cirrhotic
Gross images
Contributed by Raul S. Gonzalez, M.D.
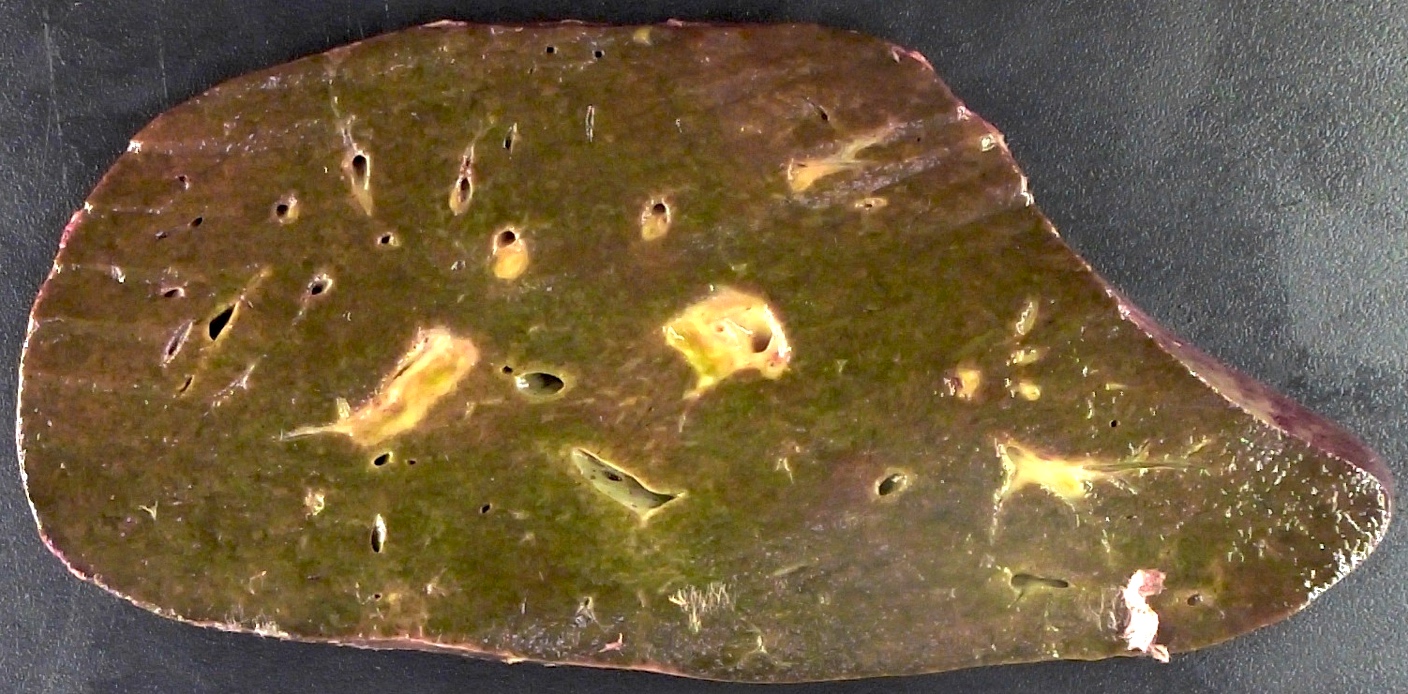
Periductal fibrosis
Microscopic (histologic) description
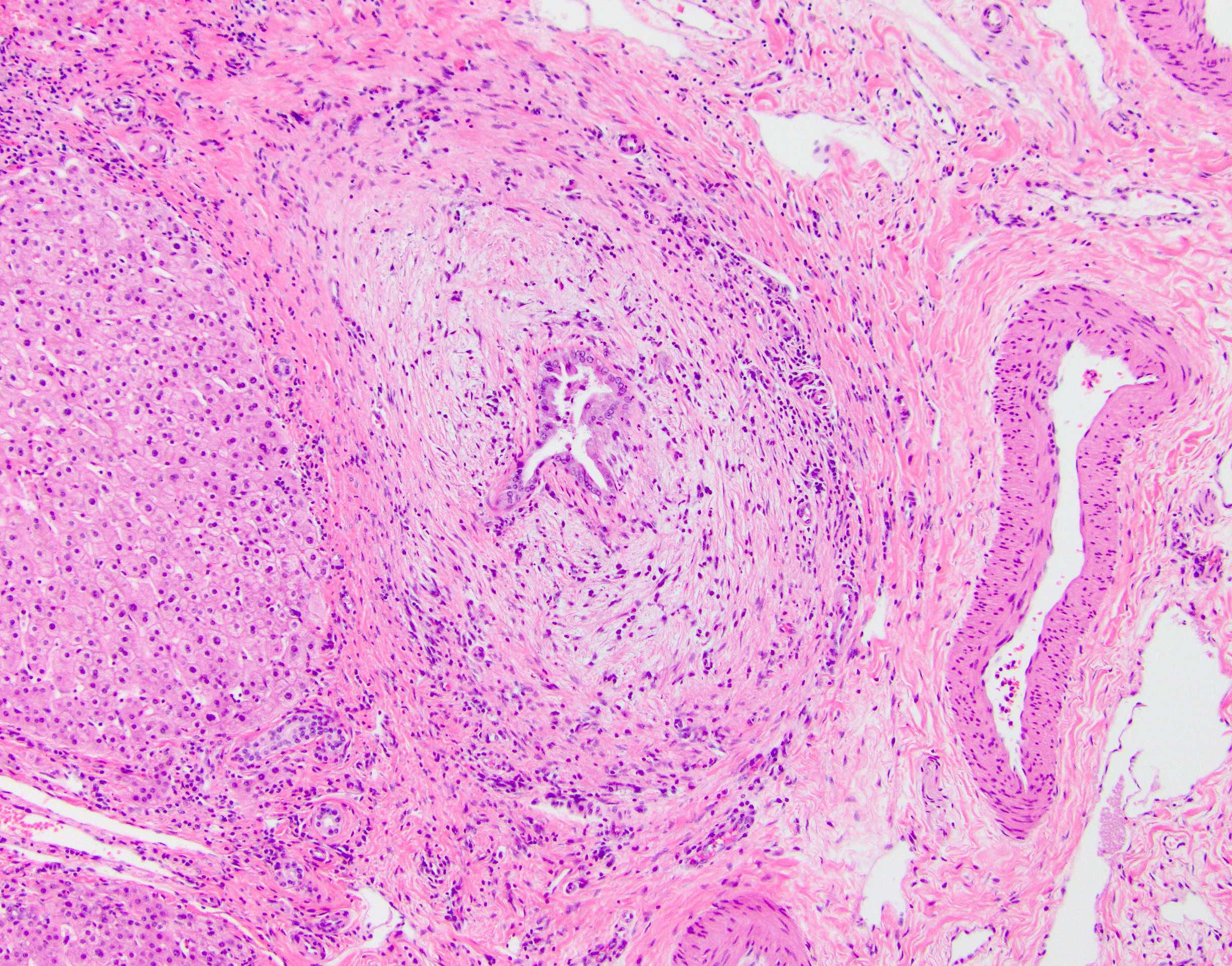
- Classic finding is "onion skin" fibrosis around affected medium sized bile ducts; smaller ducts rarely affected (except in small duct primary sclerosing cholangitis), meaning biopsy sampling rarely demonstrates this finding
- Progressive atrophy of bile duct epithelium and obliteration of the lumen, leaving a fibrous scar
- Ductular reaction and cholestasis may occur
- Inflammatory infiltrate is typically mild and limited to biliary epithelium and portal tracts, though largest ducts may show increased infiltrate
- Extravasated bile may elicit xanthomatous or granulomatous response
- Portal edema and fibrosis may be seen secondary to obstruction of larger ducts
- Primary sclerosing cholangitis cirrhosis shows the typical biliary jigsaw pattern
- Cholangiocarcinoma may occur in primary sclerosing cholangitis, preceded by intestinal metaplasia and biliary intraepithelial neoplasia (Am J Surg Pathol 2010;34:27)
- Several staging systems exist, with the Ludwig system the most commonly used (Hepatology 2017;65:907):
- Cholangitis / portal hepatitis
- Periportal fibrosis or periportal hepatitis
- Bridging fibrosis or necrosis
- Cirrhosis
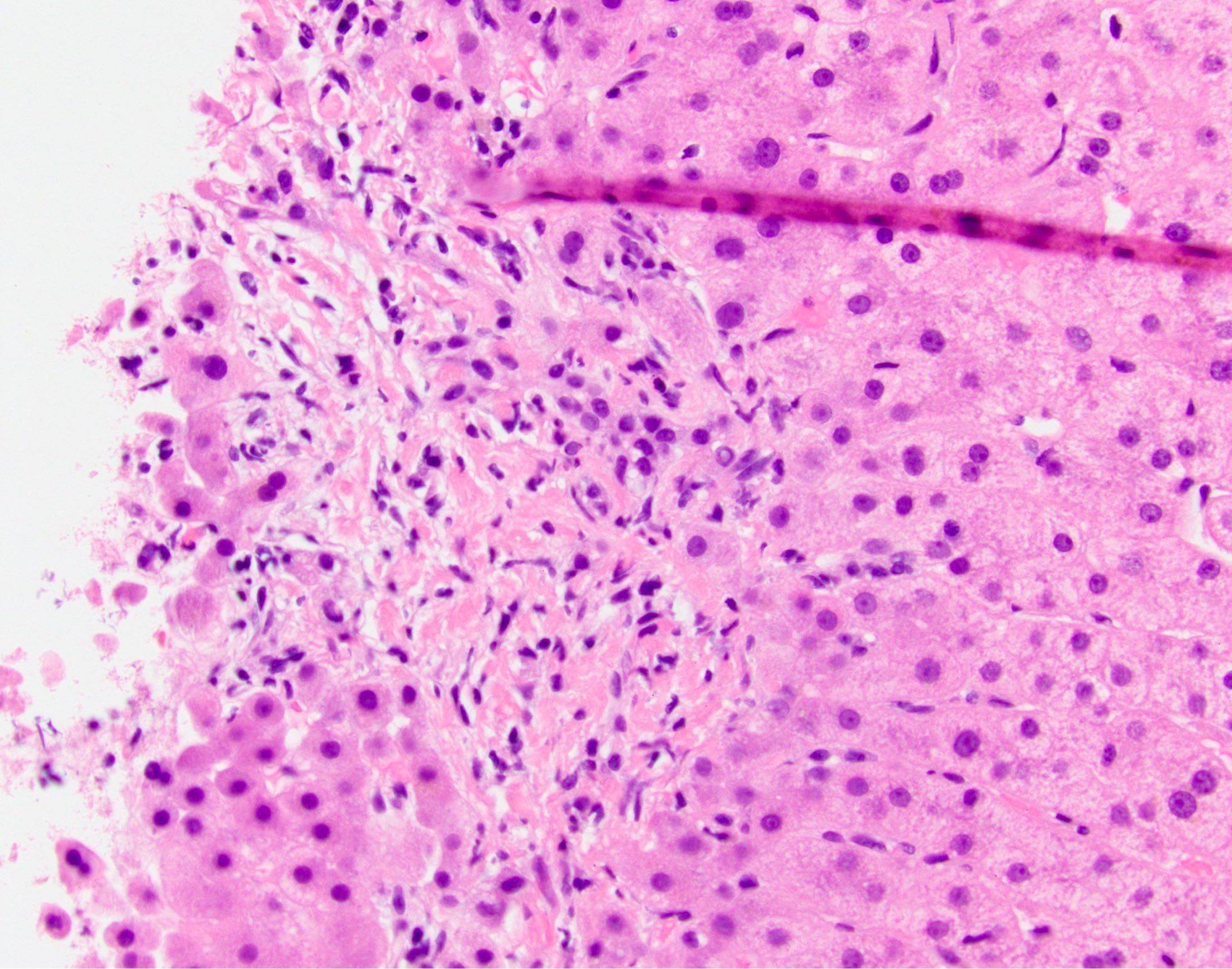
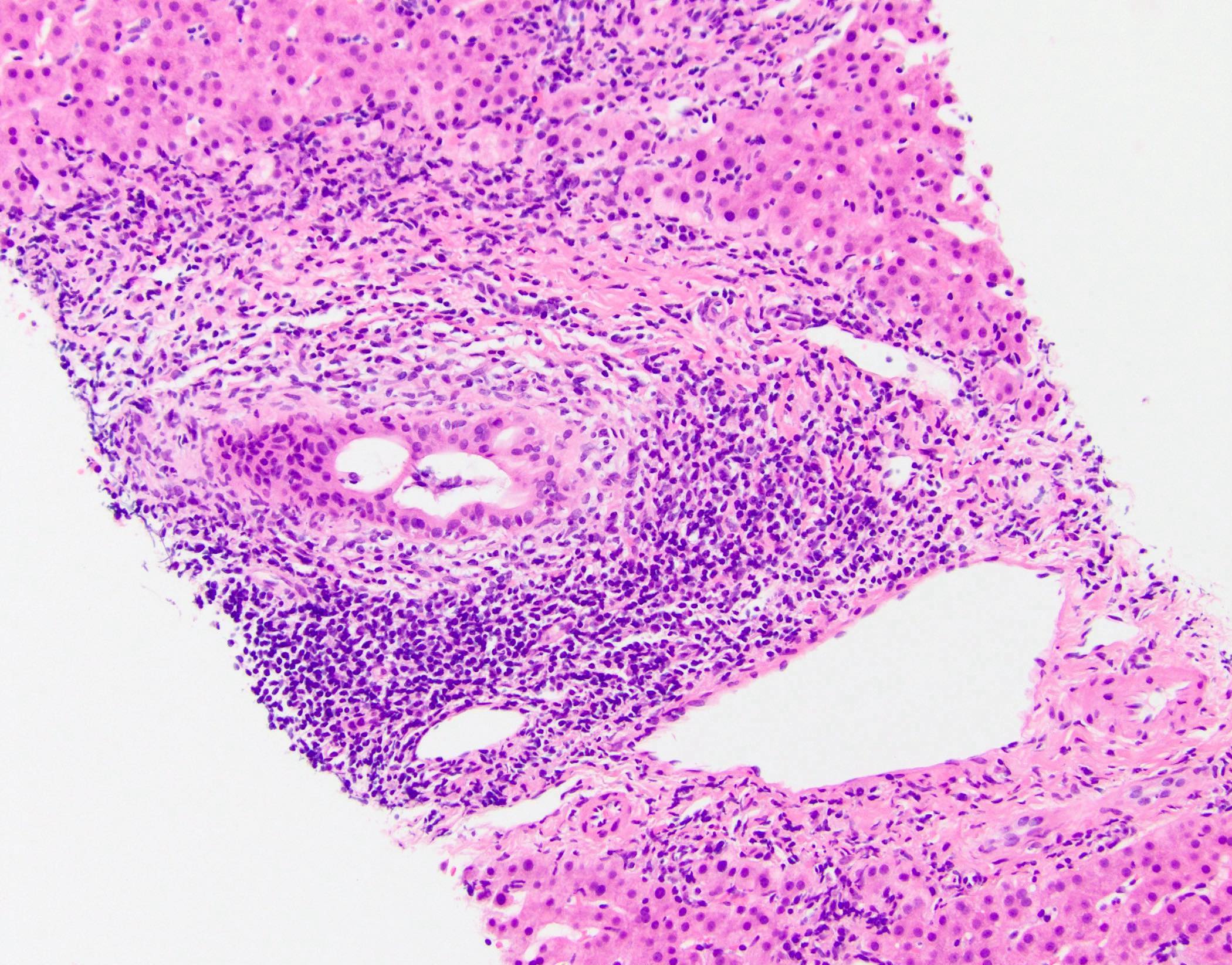
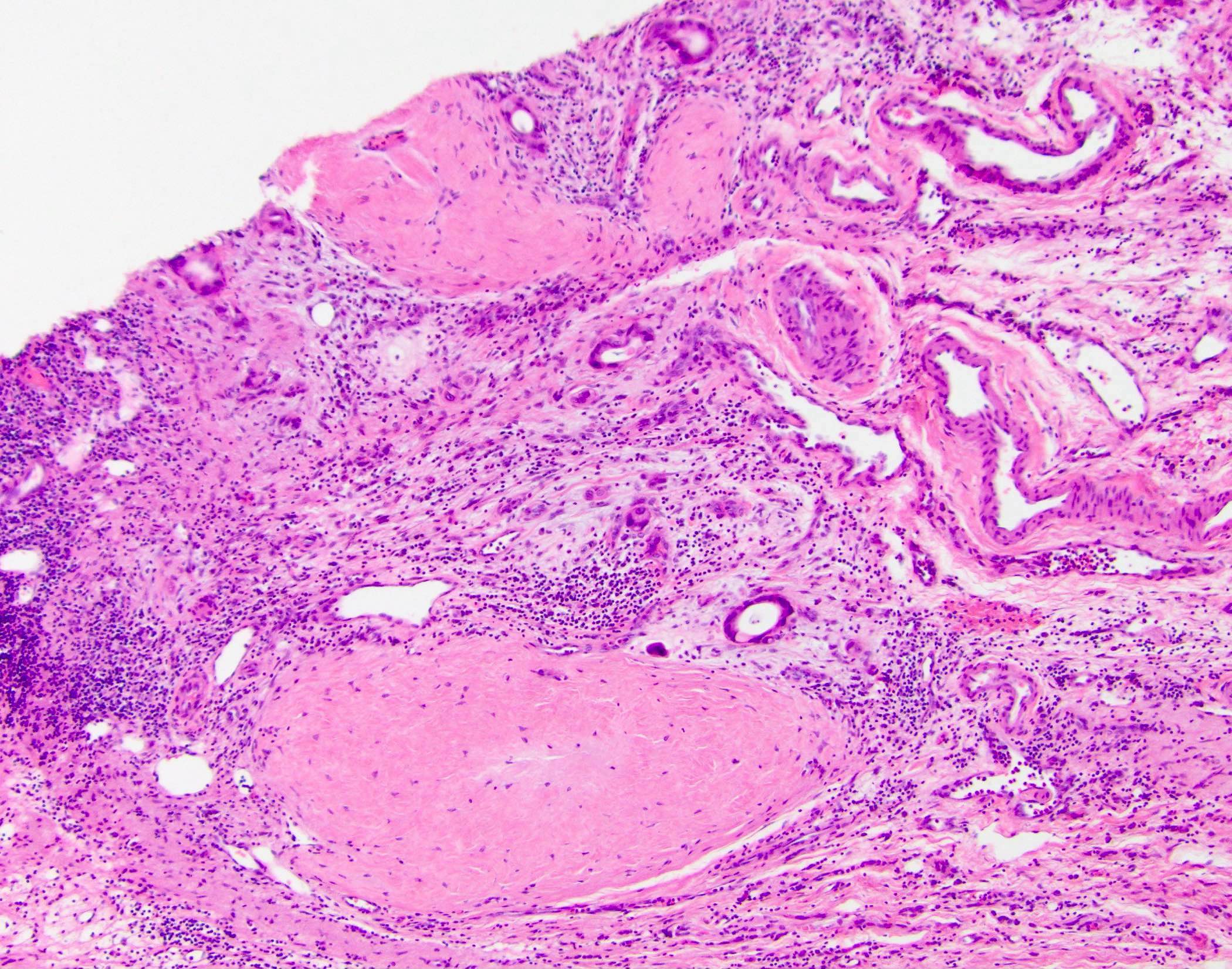
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
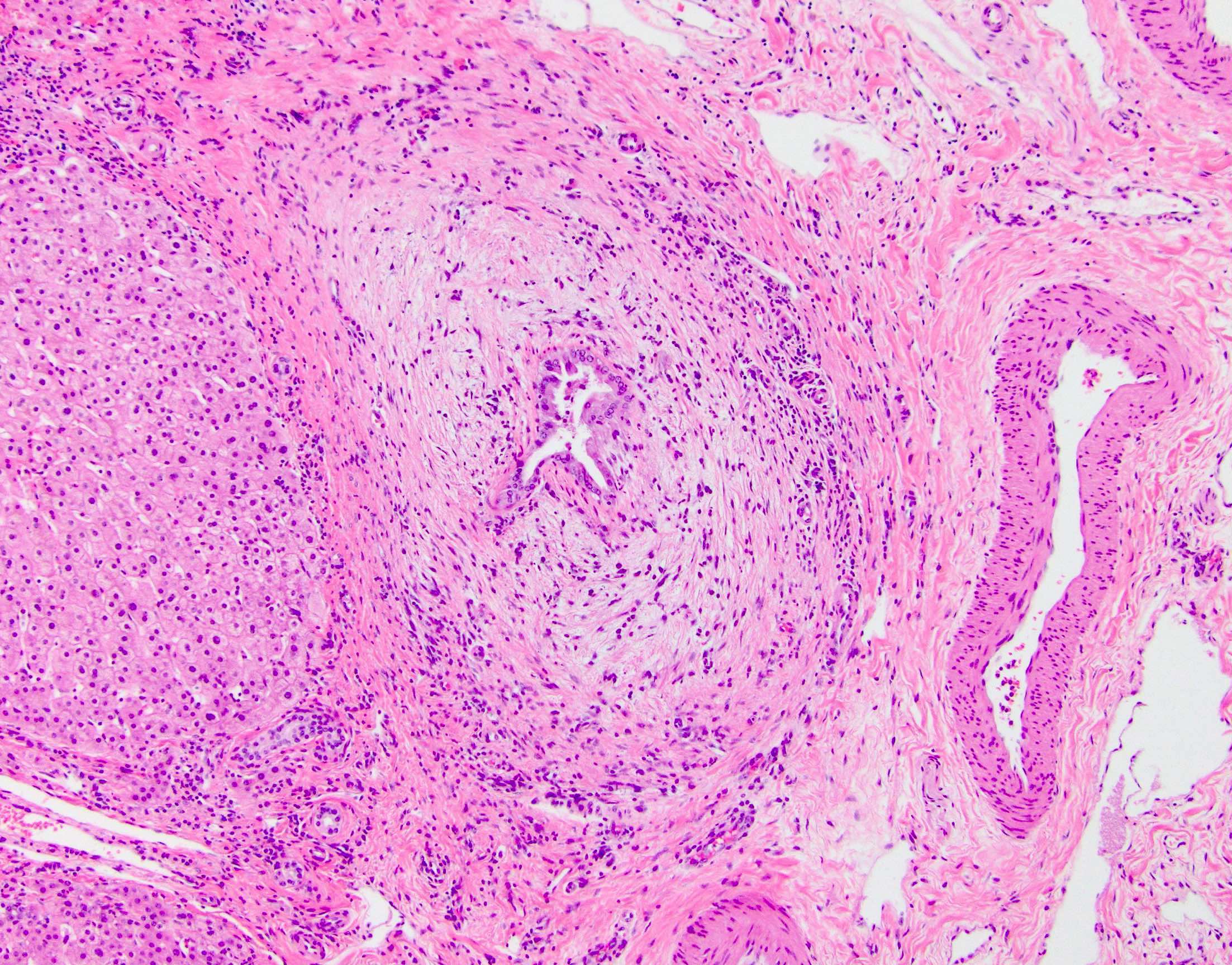
"Onion skin" fibrosis
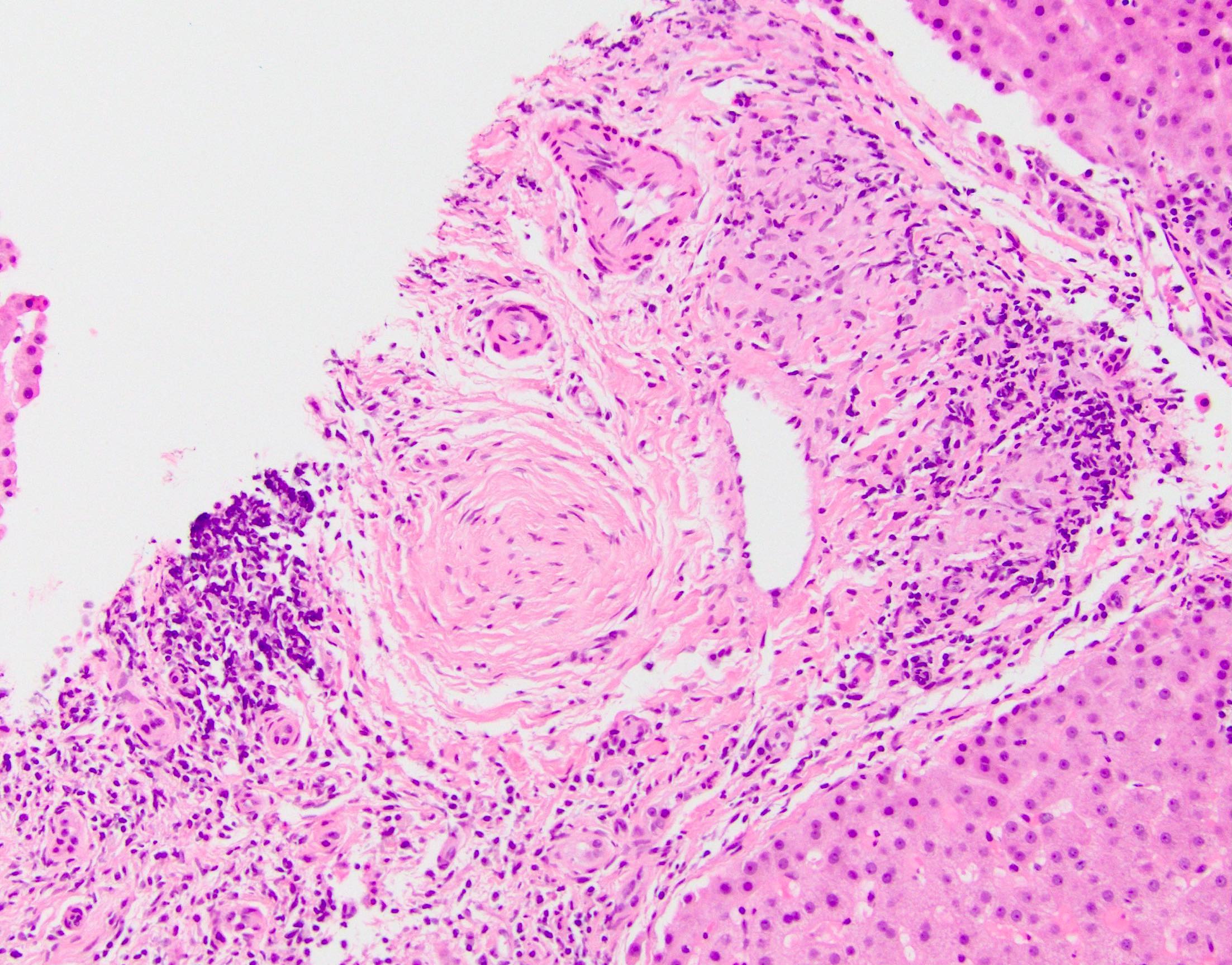
Scar replacing duct
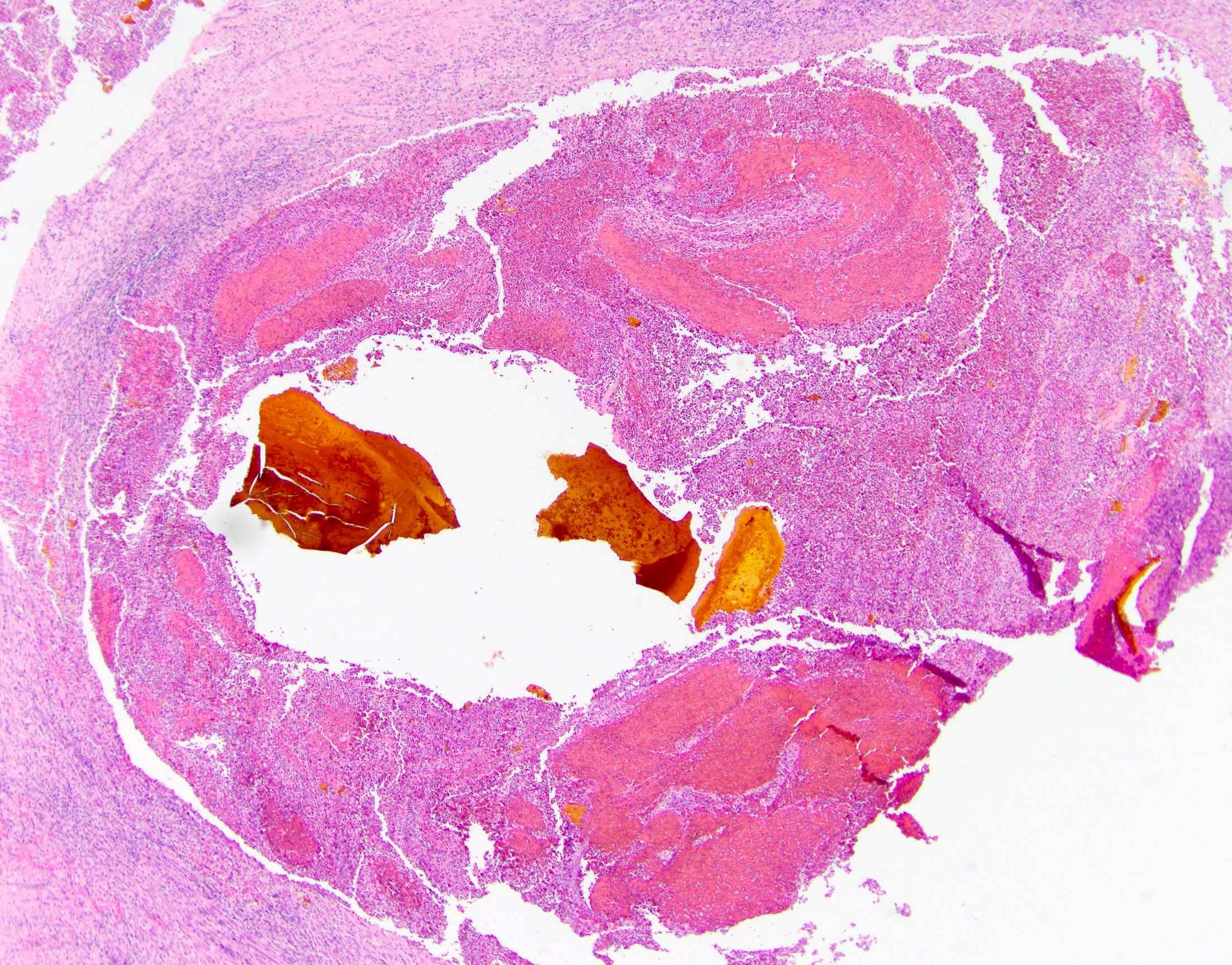
Large duct rupture

Ductular reaction
Duct injury
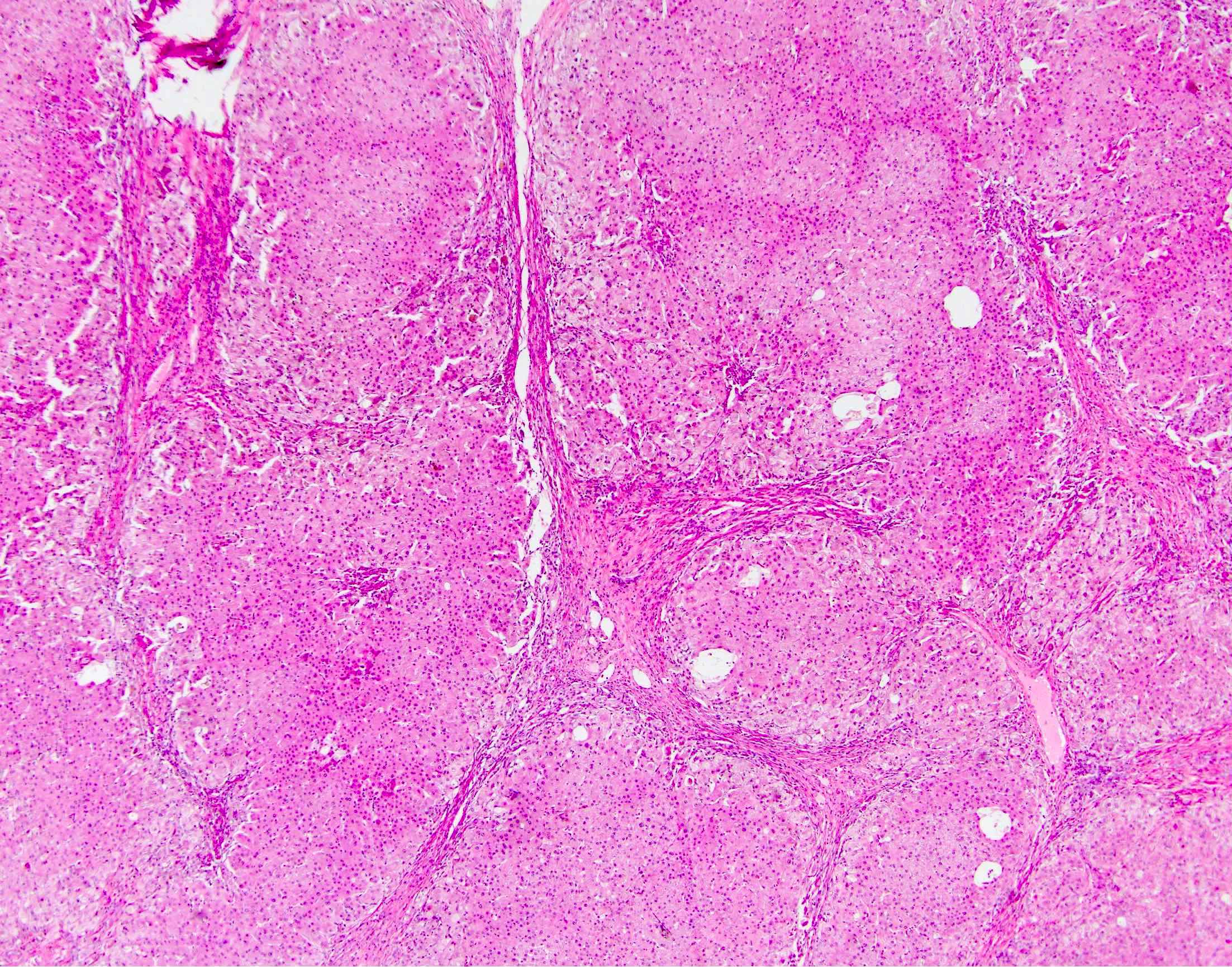
Biliary type cirrhosis
PSC autoimmune hepatitis overlap
PSC with
cholangiocarcinoma
Sample pathology report
- Liver, biopsy:
- Liver parenchyma with ductular reaction, bile duct distortion with focal inflammation and minimal portal chronic inflammation (see comment)
- Comment: The reported finding of bile duct stricturing on magnetic resonance cholangiopancreatography is noted. While the histologic findings are not specific, they are compatible with primary sclerosing cholangitis. A trichrome stain shows no significant fibrosis.
Differential diagnosis
- Cholangiocarcinoma:
- May have similar radiologic findings
- Primary biliary cholangitis:
- Florid duct lesions, more prominent inflammation
- Secondary sclerosing cholangitis:
- Due to stones, prior surgery
- "Onion skin" fibrosis and inflammation often more diffuse
- Duct obstruction:
- May occur due to primary sclerosing cholangitis or other causes
- Pure duct obstruction often has early cholestasis
- IgG4 related sclerosing cholangitis:
- More prominent inflammation, with numerous IgG4 positive plasma cells by IHC
- Disease has more aggressive clinical course (shorter time to transplant, higher likelihood of recurrence) (Am J Surg Pathol 2010;34:88, World J Gastroenterol 2013;19:7661)
Additional references
Board review style question #1
Which of the following modalities is most useful for establishing a diagnosis of primary sclerosing cholangitis?
- Liver biopsy
- Liver enzymes
- Magnetic resonance cholangiography
- Serology
Board review style answer #1
Board review style question #2
A 60 year old man presents with signs and symptoms of liver failure. He discloses a long history of abdominal pain and intermittent jaundice but chose not to visit a doctor previously. He is found to have cirrhosis and ultimately undergoes liver transplantation. Histologic examination shows the following
Which of the following is true about this patient?
Which of the following is true about this patient?
- He is at increased risk of developing Crohn's disease but not ulcerative colitis
- He appears to have the small duct variant of this disease
- Serologic testing would demonstrate positive antimitochondrial antibodies
- The liver explant should be carefully examined to rule out cholangiocarcinoma
Board review style answer #2
D. The liver explant should be carefully examined to rule out cholangiocarcinoma
Comment Here
Reference: Primary sclerosing cholangitis
Comment Here
Reference: Primary sclerosing cholangitis
