

Liver & intrahepatic bile ducts
Infectious nonviral
Fasciola hepatica
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 19 August 2022
Last staff update: 26 August 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Fasciola hepatica


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Samdanci ET, Ozcan M. Fasciola hepatica. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverfasciolahepatica.html. Accessed January 19th, 2025.
Definition / general
- Parasitic infection of liver and biliary tract; parasitic flatworm included in the trematode group; infects hepatobiliary system of various mammals, including humans (Mahmud: Medical Parasitology, 1st Edition, 2017)
Essential features
- Presentation with tumor-like masses
- Tract shaped granulomas contain necrotic material in their lumens with increased eosinophils
- Numerous Charcot-Leyden crystals may be seen in necrosis
Terminology
- Liver fluke or sheep liver fluke
ICD coding
- ICD-10: B66.3 - fascioliasis
Epidemiology
- Human infections are distributed globally, mainly in sheep rearing countries
Sites
- Mostly liver, bile ducts and gallbladder
Pathophysiology
- Parasite penetrates liver capsule, migrates into bile ducts, to large bile ducts and gallbladder (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
Etiology
- Transmitted to humans from watercress or other freshwater plants containing metacercariae (Mahmud: Medical Parasitology, 1st Edition, 2017, Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
Diagrams / tables
Images hosted on other servers:


Life cycle
Clinical features
- Presentation changes according to phase of illness
- Invasion phase: fever, hepatomegaly, upper abdominal pain, ascending bacterial cholangitis, obstructive jaundice, blood eosinophilia
- Biliary phase: hepatomegaly, right upper quadrant pain, fever and blood eosinophilia, biliary colic, epigastric pain, fatty food intolerance, nausea, jaundice and pruritus (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- Mass may present incidentally at radiologic imaging
- Rare signs / symptoms include acute pancreatitis and involvement of the pancreas or kidney; anaphylaxis has not been described (Turk J Gastroenterol 2010;21:183, BMC Gastroenterol 2004;4:15)
Diagnosis
- Demonstration of eggs in feces or aspirated bile (Mahmud: Medical Parasitology, 1st Edition, 2017)
- Histologically, the organism can be seen in the bile ducts in the mass removed due to the tumor (Turk Patoloji Derg 2019;35:58)
Laboratory
- Eosinophilia reaching 30% or more of the total white blood cell (WBC) count (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
Radiology description
- Ultrasound: hepatic parenchymal heterogeneity, dilatation of the bile duct with wall thickening, peripheral hypoechoic nodular lesions (Clin Microbiol Infect 2005;11:859)
- CT / MRI: multiple, small, hypodense lesions 2 - 10 mm in diameter and microabscesses arranged in a tunnel-like branching pattern (tortuous tracts), with frequent subcapsular locations of the lesions
- In rare instances, abscess-like lesions 7 - 10 cm in diameter can be seen and may be mistakenly considered a tumor
- Liver capsular thickening and subcapsular hemorrhage can also be detected (Clin Imaging 2016;40:251)
Radiology images
Images hosted on other servers:

CT

PET scan

MRI
Prognostic factors
- Capsular invasion can cause subcapsular hematomas
- Choledochal obstruction can cause cholangitis (Res Rep Trop Med 2020;11:149)
- Resection is mostly curative
Case reports
- 9 year old girl with liver abscess (APSP J Case Rep 2015;6:27)
- 26 and 52 year old women with fascioliasis cases mimicking liver tumors (Turk Patoloji Derg 2019;35:58)
- 48 year old woman with abdominal distension (Am J Trop Med Hyg 2013;89:1212)
- 48 year old woman with Fasciola hepatica mimicking sepsis without eosinophilia (Turkiye Parazitol Derg 2014;38:131)
- 63 year old man with Fasciola hepatica in FNA of a liver mass (Cytopathology 2015;26:259)
- 65 year old woman with right upper quadrant discomfort (J Radiol Case Rep 2010;4:13)
- 87 year old man with Fasciola hepatica infection mimicking cholangiocarcinoma (Korean J Parasitol 2014;52:193)
- 4 fascioliasis cases occurring in the same family (Korean J Parasitol 2017;55:55)
Treatment
- Triclabendazole is the treatment of choice; bithionol is an alternative drug (Mahmud: Medical Parasitology, 1st Edition, 2017)
Clinical images
Images hosted on other servers:

Living fasciola


Endoscopic view
Gross description
- Solitary or multiple solid to cystic nodules with necrosis that may resemble metastases
Gross images
Images hosted on other servers:

Formalin fixed tissue

Fresh tissue
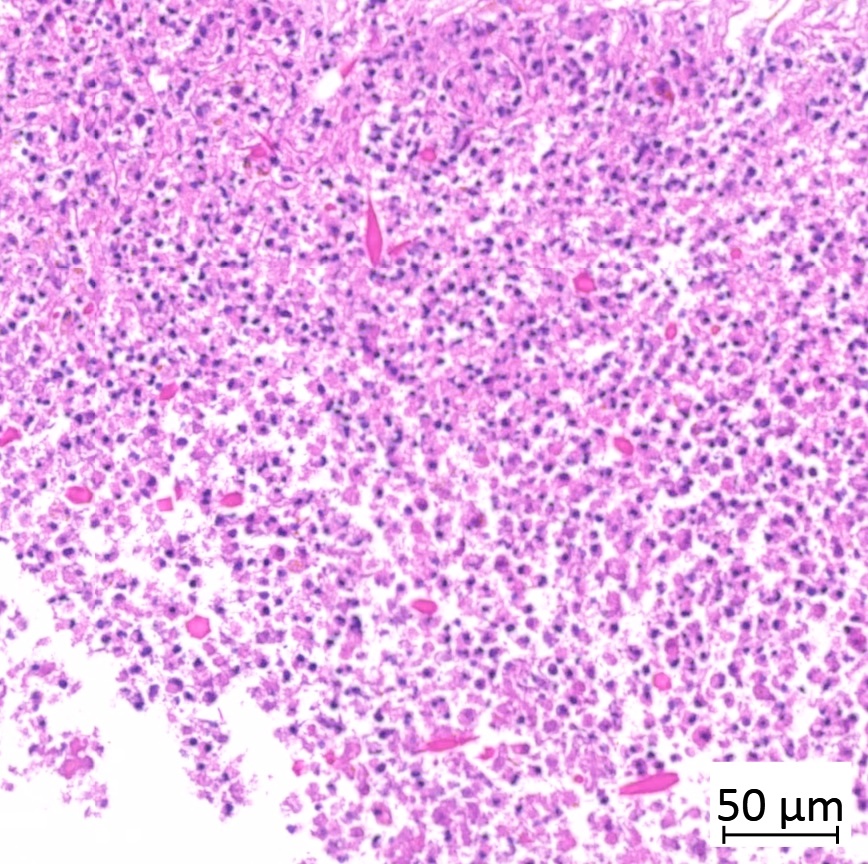
Microscopic (histologic) description
- Dilated intrahepatic bile ducts may contain adult flukes
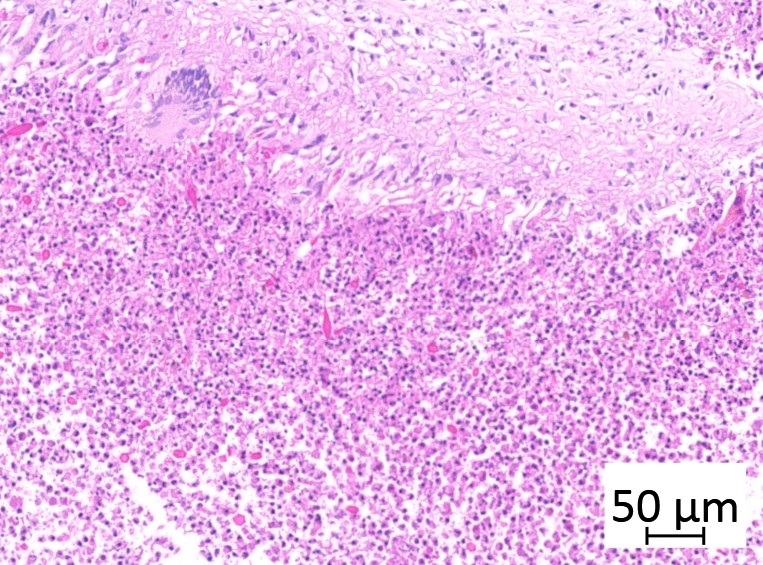
- Tract shaped necrotic debris
- Eosinophils
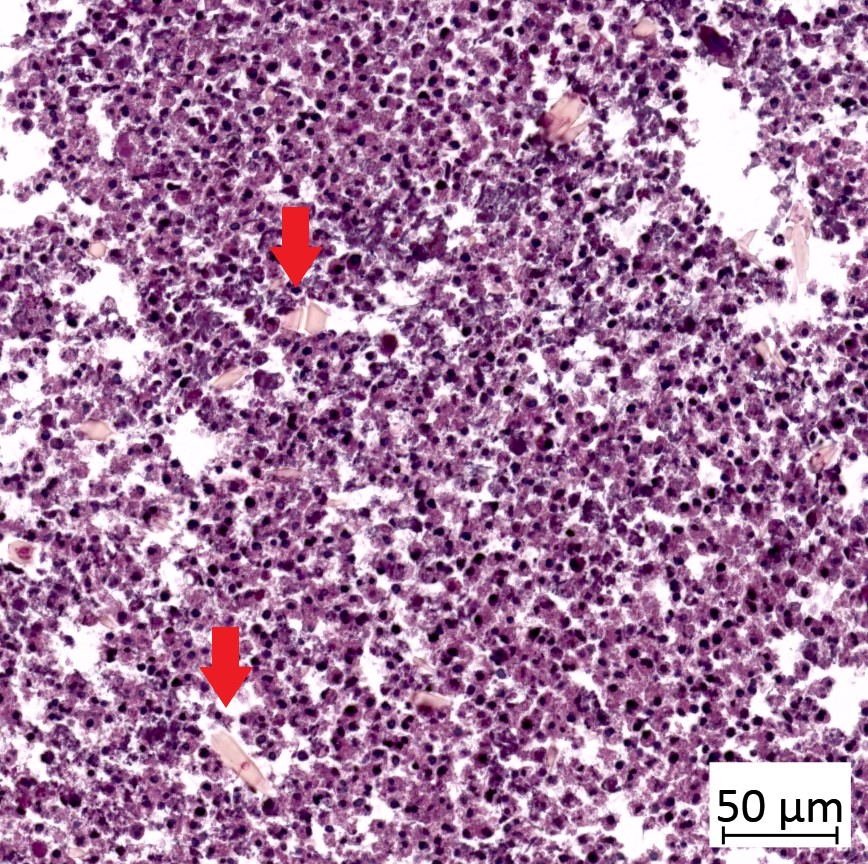
- Charcot-Leyden crystals (Turk Patoloji Derg 2019;35:58)
- Eosinophilic granulomas: center of dense inflammatory cells composed predominantly of eosinophils with scattered Charcot-Leyden crystals surrounded by a palisade of granulomatous (histiocytic) response (Am J Surg Pathol 2001;25:1316)
- Histiocytes
- Rarely, eggs (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
Microscopic (histologic) images
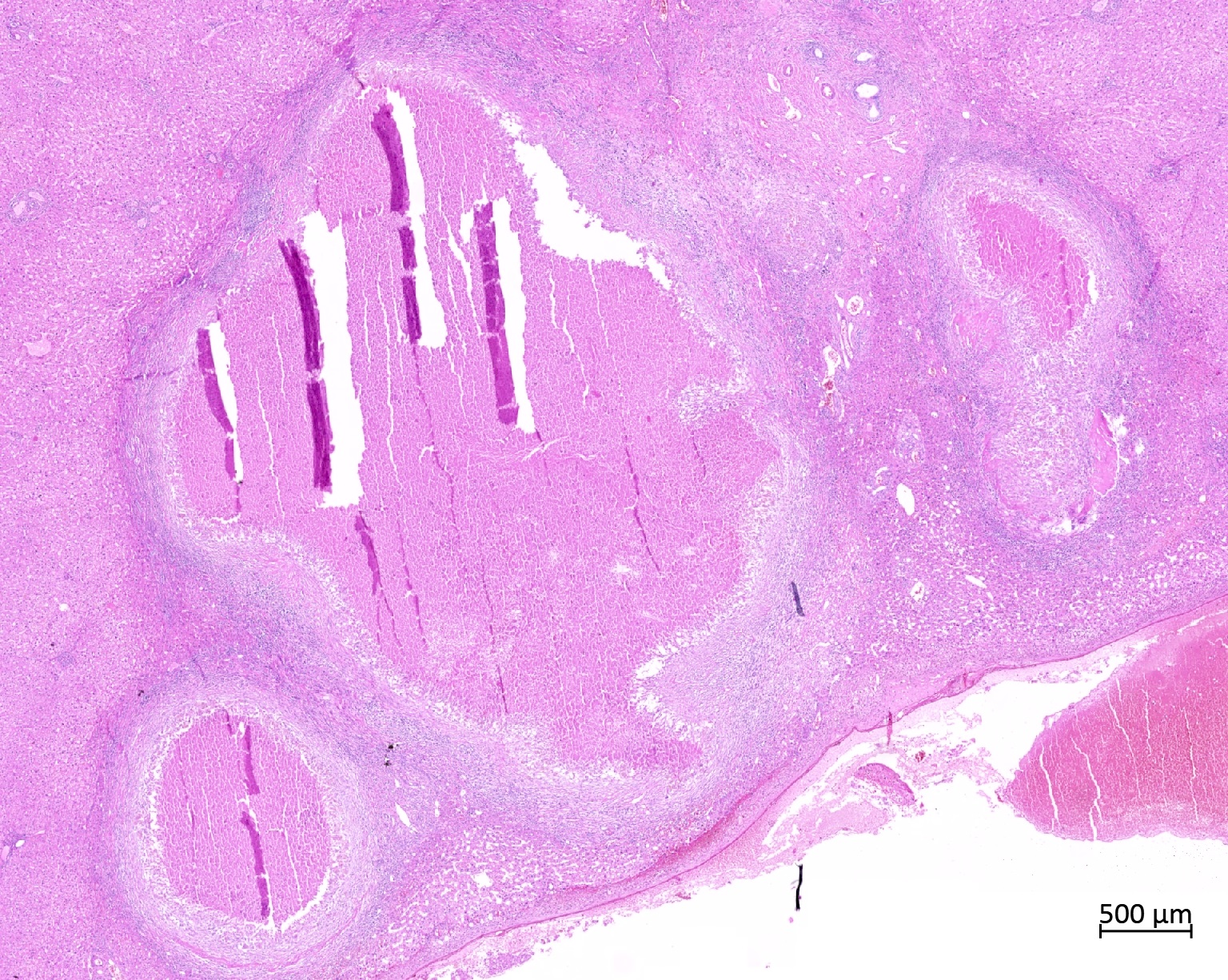
Contributed by Emine Turkmen Samdanci, M.D. and Mehmet Ozcan, M.D.
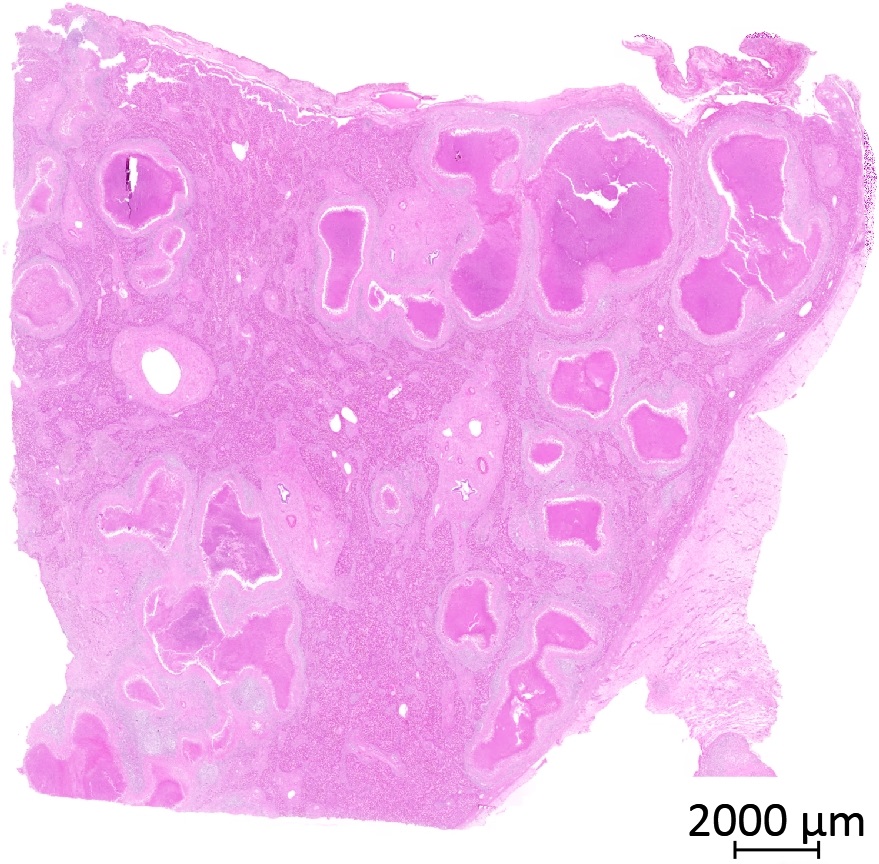
Necrotic lesions
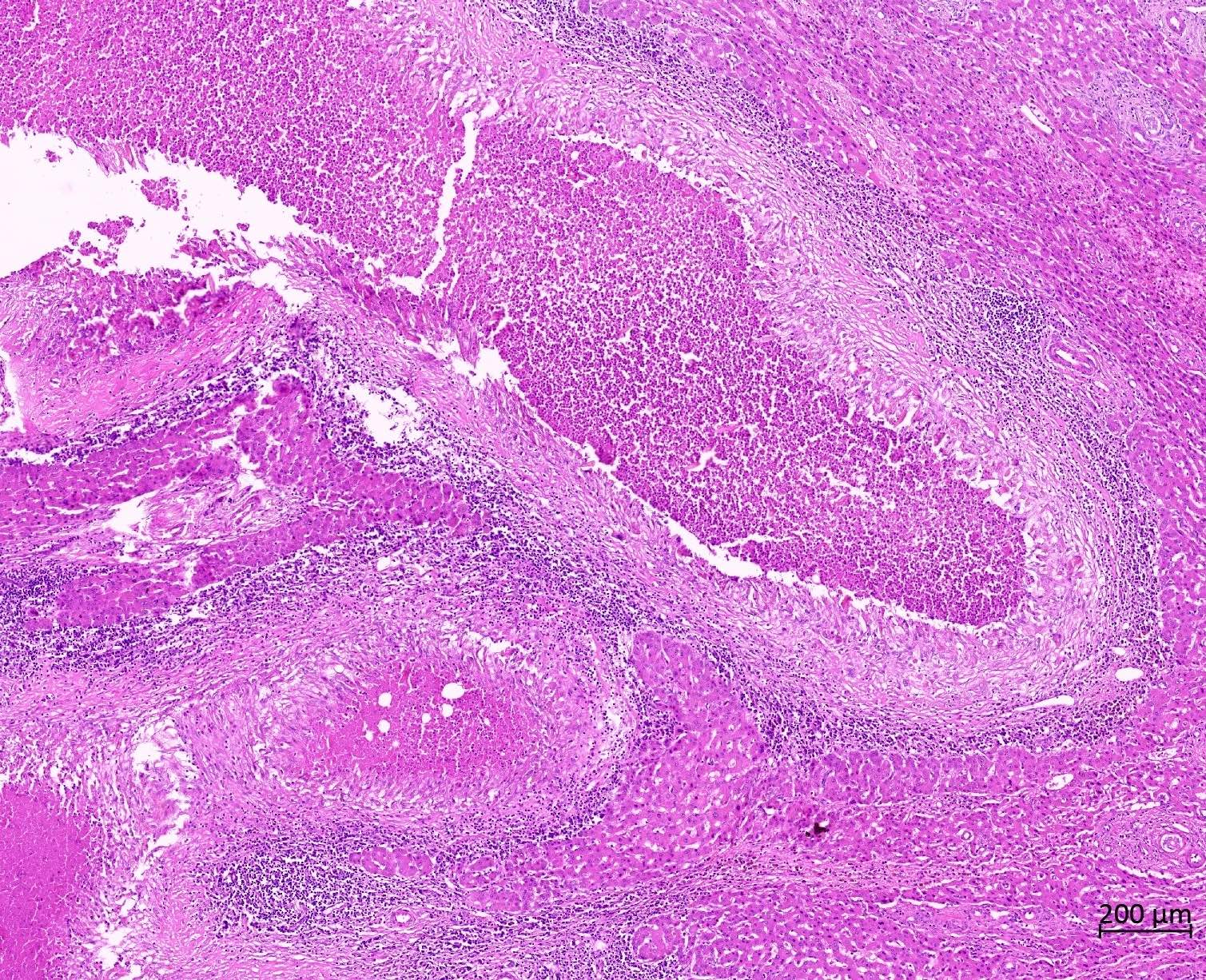
Tract shaped granulomas
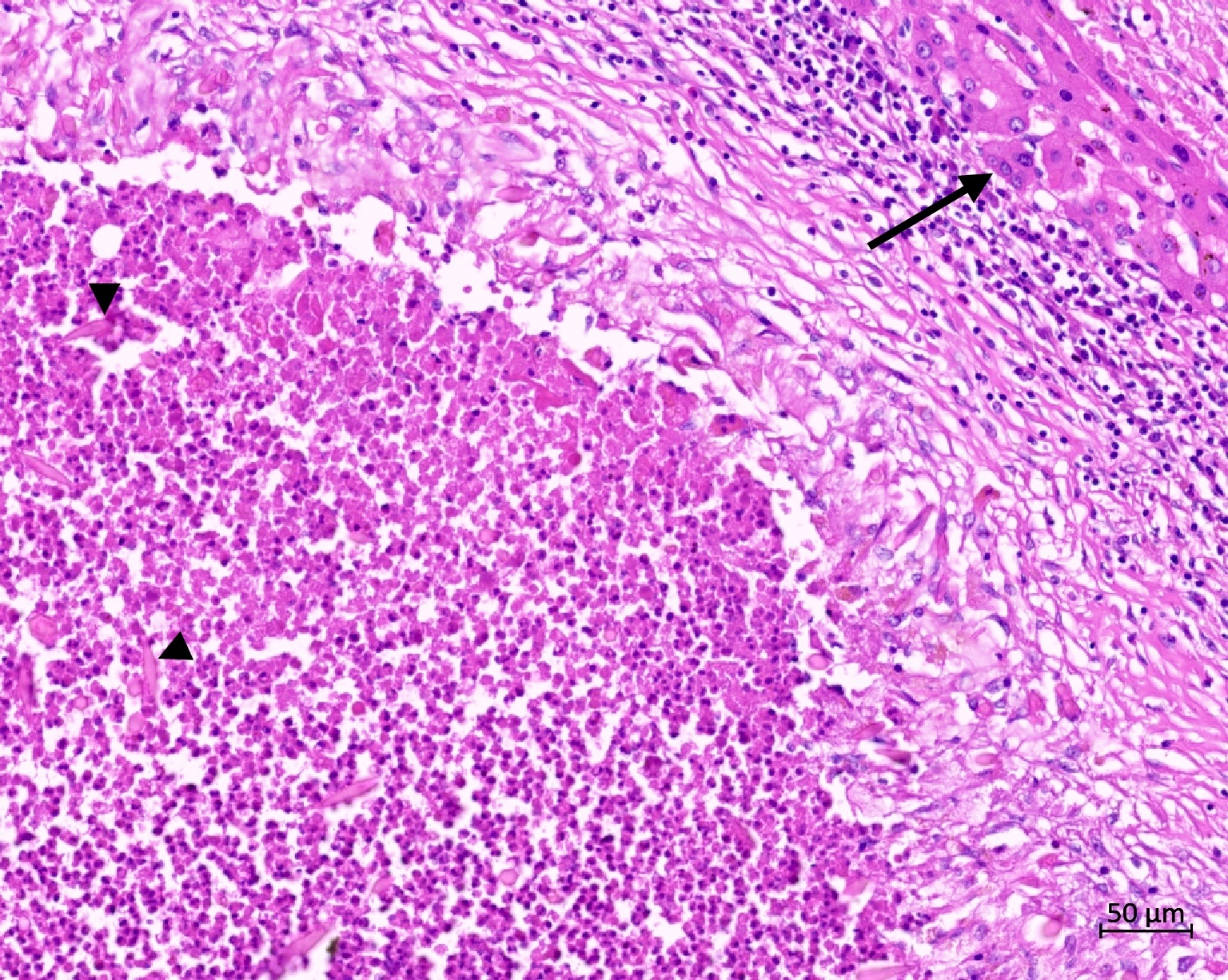
Charcot-Leyden crystals
Crystals in necrotic debris
Masson trichrome stain
Cytology description
- Cohesive clusters of epithelioid histiocytes representing granulomas
- Eosinophils
- Charcot-Leyden crystals (Cytopathology 2015;26:259)
Videos
Fascioliasis caused by Fasciola hepatica
Sample pathology report
- Liver, right hepatectomy:
- Fascioliasis / massive necrosis (see comment)
- Comment: When clinical, histopathological and laboratory findings are evaluated together, the case can be accepted as fascioliasis. Clinicopathological correlation is recommended.
Differential diagnosis
- Any tumor:
- Necrosis can be seen but eosinophils and Charcot-Leyden crystals are typically absent
- Histologic identification of neoplastic cells
- Echinococcus granulosus:
- PASD / PAS positive acellular lamellar membrane and scolices
- Echinococcus alveolaris / multilocularis:
- Macroscopically seems more invasive, PASD / PAS positive membranes
- Can be invasive or metastatic
- Toxocara species:
- Similar clinical, radiologic and histologic findings
- Presence of pets in the history may be meaningful for Toxocara
- Antigen tests can differentiate
- Granulomatous infections, such as M. tuberculosis:
- Inflammation does not contain eosinophils
Board review style question #1
Which of the following findings of Fasciola hepatica is a common presenting symptom?
- Abdominal pain
- Acute pancreatitis
- Anaphylactic reaction
- Splenomegaly
Board review style answer #1
A. Abdominal pain and fever are common findings. Acute pancreatitis and other organ involvement are uncommon and anaphylaxis has not been described.
Comment Here
Reference: Fasciola hepatica
Comment Here
Reference: Fasciola hepatica
Board review style question #2

A 25 year old man presents with a liver mass, which is suspicious for malignancy on imaging. PET scan shows little uptake. There is no history of malignancy and the patient denies taking any medication. A Trucut biopsy is done (shown above) and shows necrosis, which includes eosinophils and Charcot-Leyden crystals. There are a few hepatocytes in the biopsy, which show mostly reactive changes. What is the most likely diagnosis and appropriate next step?
- Drug reaction, recommend discontinuation of drugs
- Parasite, consistent with Fasciola hepatica
- Tumor, biopsy must be done again to see tumor cells
- Echinococcus granulosus
Board review style answer #2
B. Parasite, consistent with Fasciola hepatica. Charcot-Leyden crystals and eosinophils suggest Fasciola hepatica and not a drug reaction. No tumor cells are identified. There is no suggestion of an acellular lamellar membrane or scolices associated with Echinococcus.
Comment Here
Reference: Fasciola hepatica
Comment Here
Reference: Fasciola hepatica

