

Bone marrow neoplastic
Bone marrow - neoplastic myeloid
AML with recurrent genetic abnormalities
AML with t(8;21)(q22;q22); RUNX1::RUNX1T1
Authors: Sean Gu, M.D., Ph.D., Alexa J. Siddon, M.D.
Editorial Board Member: Elizabeth Courville, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 12 April 2021
Last staff update: 21 September 2023
Copyright: 2001-2024, PathologyOutlines.com, Inc.
PubMed Search: AML with t(8;21) [TIAB] pathology

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Flow cytometry description | Flow cytometry images | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gu S, Siddon AJ. AML with t(8;21)(q22;q22); RUNX1::RUNX1T1. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/leukemiaAMLwitht821q22q22.html. Accessed December 25th, 2024.
Definition / general
- AML with t(8;21)(q22;q22.1) is defined by a genetic rearrangement that results in the fusion of RUNX1 and RUNX1T1, has characteristic morphologic and immunophenotypic features and is associated with a generally favorable prognosis
Essential features
- AML with t(8;21)(q22;q22.1) is classified in the category of AML with recurrent genetic abnormalities and is diagnostic of AML regardless of blast count
- t(8;21)(q22;q22.1) is a balanced translocation that results in the fusion of RUNX1 and RUNX1T1
- Blasts have distinct morphologic and immunophenotypic features, including abundant basophilic cytoplasm containing azurophilic granules with occasional Auer rods and frequent aberrant expression of B cell markers, such as CD19
- Diagnosis is established by detection of t(8;21) by real time PCR or cytogenetics
- Prognosis is generally favorable, while coexisting KIT mutations adversely affect outcomes
Terminology
- AML with RUNX1-RUNX1T1
- AML with AML1-ETO
- Usually classified as AML M2 subtype in the previous French American British (FAB) classification system
ICD coding
- ICD-10: C92.00 - Acute myeloblastic leukemia, not having achieved remission
Epidemiology
- Typically occurs in younger patients and comprises approximately 1 - 5% of all AML cases
Sites
- Peripheral blood
- Bone marrow
- Myeloid sarcoma soft tissue / organs
Pathophysiology
- t(8;21)(q22;q22.1) results in fusion of the RUNX1 gene on chromosome 21q22.1 with RUNX1T1 gene on chromosome 8q22
- RUNX1 is a member of the core binding factor family of transcription factors, which is critical for the establishment of normal hematopoiesis (Blood 2017;129:2070)
- t(8;21), RUNX1-RUNX1T1 fusion gene expresses a chimeric protein that disrupts the normal function of the core binding factor and predisposes to acute myeloid leukemia (Cell Rep 2013;4:1131)
- Most cases show additional chromosomal abnormalities and cooperating driver mutations that promote transformation to acute myeloid leukemia (Blood 2012;119:e67)
Diagnosis
- Established by detection of t(8;21) by real time PCR or cytogenetics
Prognostic factors
- AML with t(8;21)(q22;q22.1) has a relatively favorable outcome and is associated with high rate of complete remission
- Presence of KIT mutations adversely affects prognosis (J Clin Oncol 2006;24:3904)
Case reports
- 28 year old man with headache was found to have intracranial myeloid sarcoma (Onco Targets Ther 2020;13:237)
- 65 year old woman with epistaxis (Case Rep Hematol 2019;2019:1312630)
- 2 patients with AML also found to have associated systemic mastocytosis (Exp Mol Pathol 2019;108:131)
Treatment
- Typically chemotherapy with induction, followed by intensive cytarabine consolidation
Microscopic (histologic) description
- Blast cells characteristically have slightly basophilic cytoplasm containing abundant azurophilic granules and perinuclear hofs
- Occasionally, large pseudo Chediak-Higashi granules and thin Auer rods may be seen; Auer rods may be seen in neutrophils
- Mature eosinophils that are morphologically normal are often increased in number in the bone marrow
- Mature granulocytes may show dysplastic changes with pseudo Pelger-Huet anomaly
- Generally no dysplasia in the erythroid and megakarocytic lineages
Microscopic (histologic) images
Contributed by Sean Gu, M.D., Ph.D., Alexa J. Siddon, M.D. and AFIP images
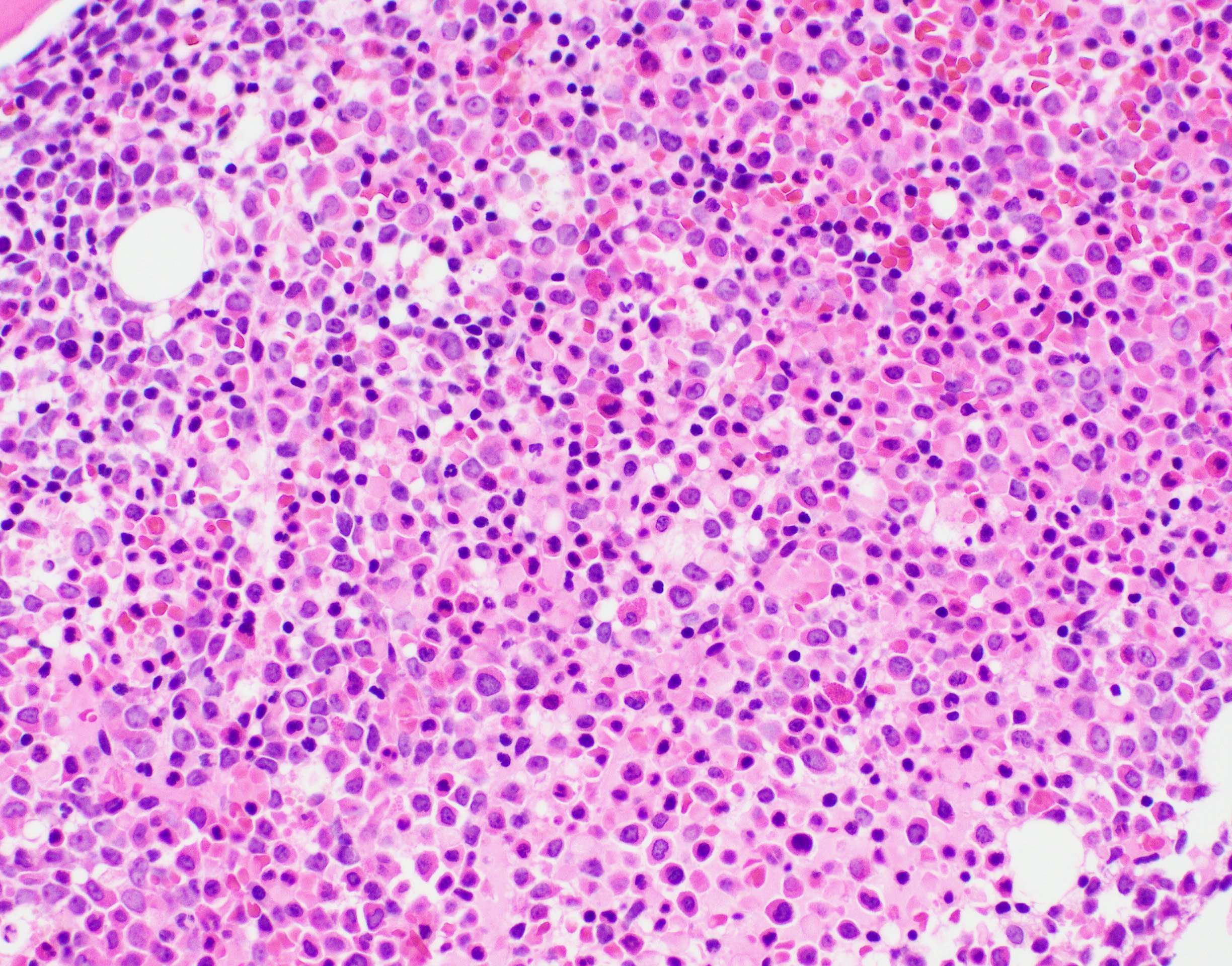
Left shift
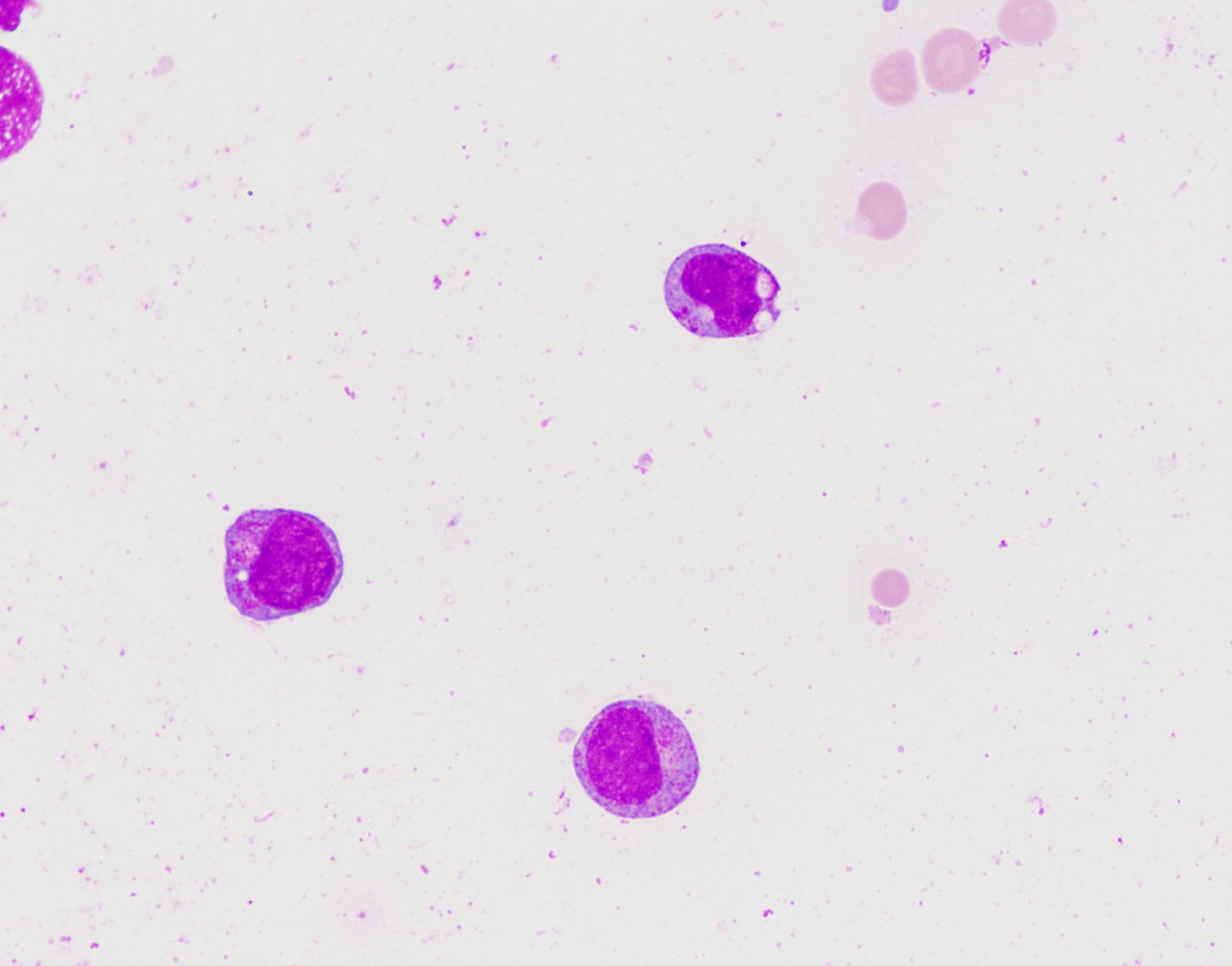
Blasts
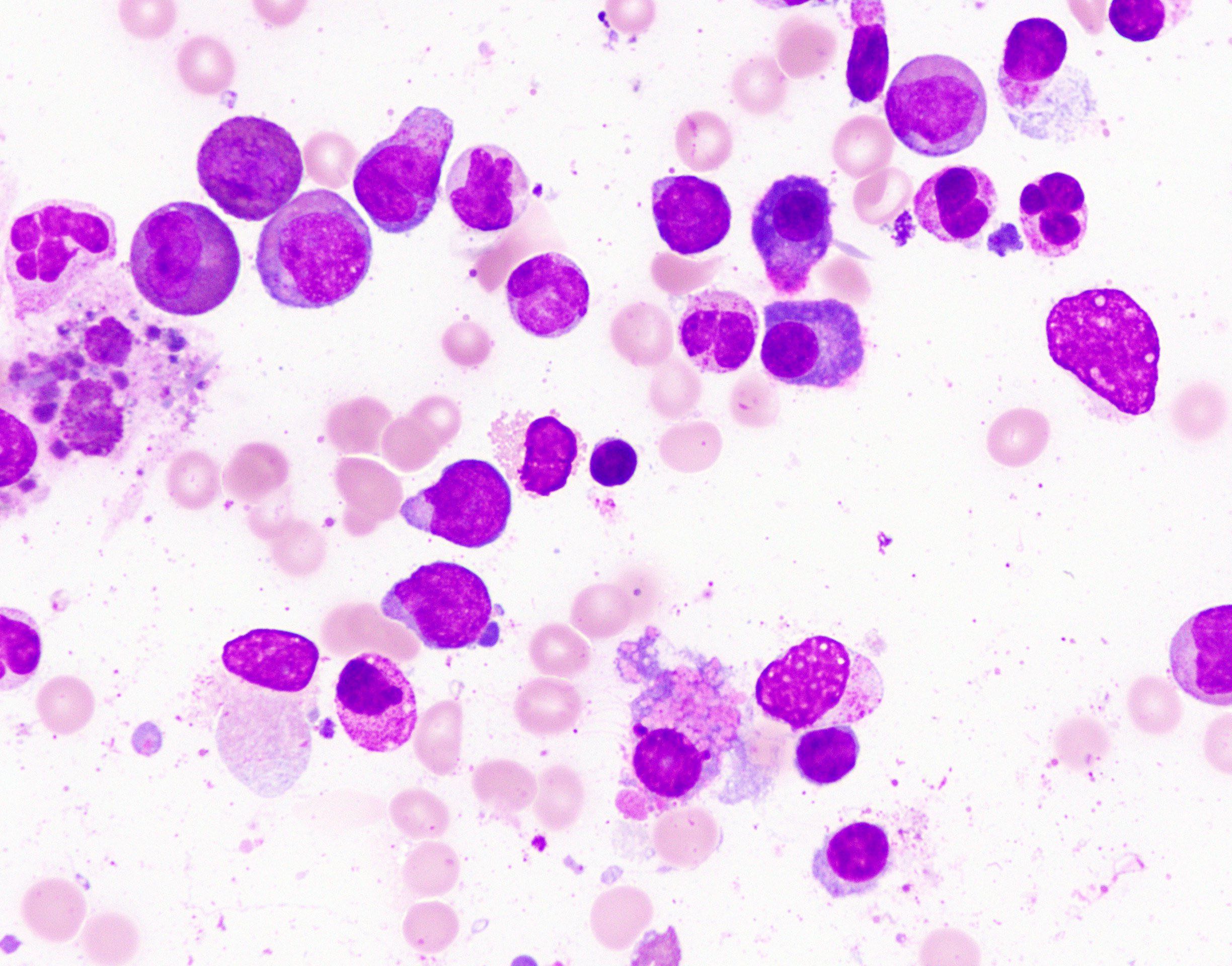
Aspirate morphology
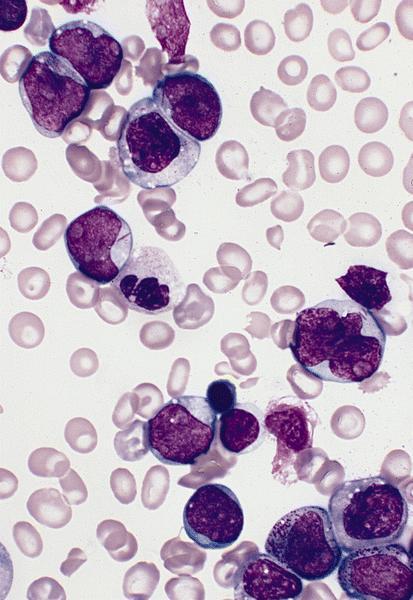
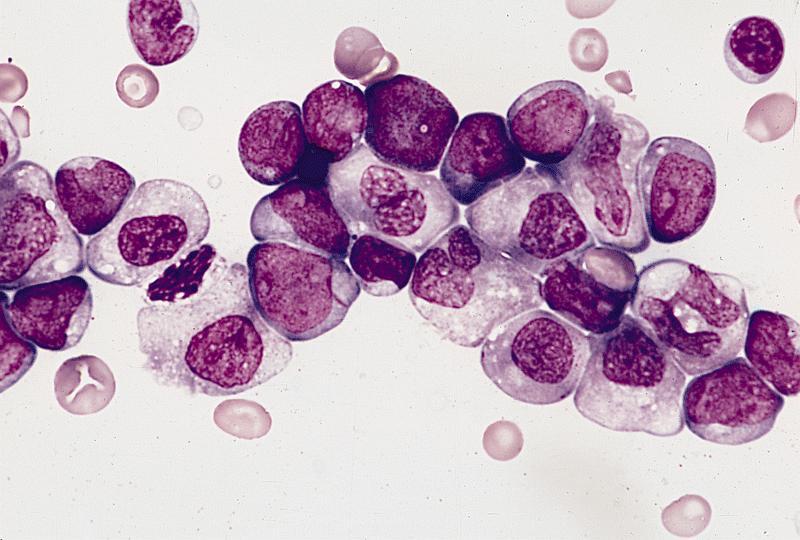
Bone marrow smear (Wright-Giemsa)
Images hosted on other servers:

Myeloblast in AML with t(8;21)
Positive stains
Negative stains
Flow cytometry description
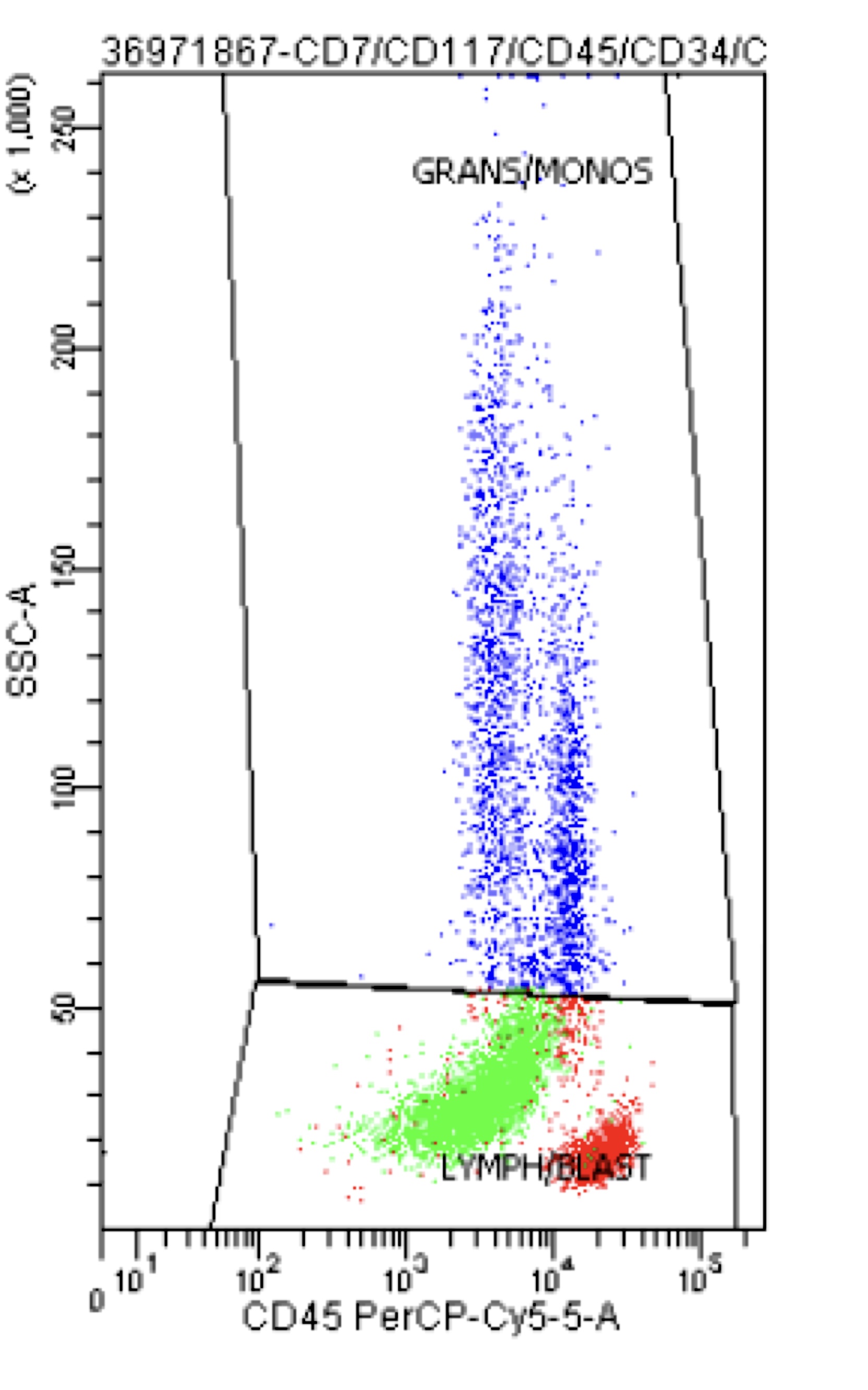
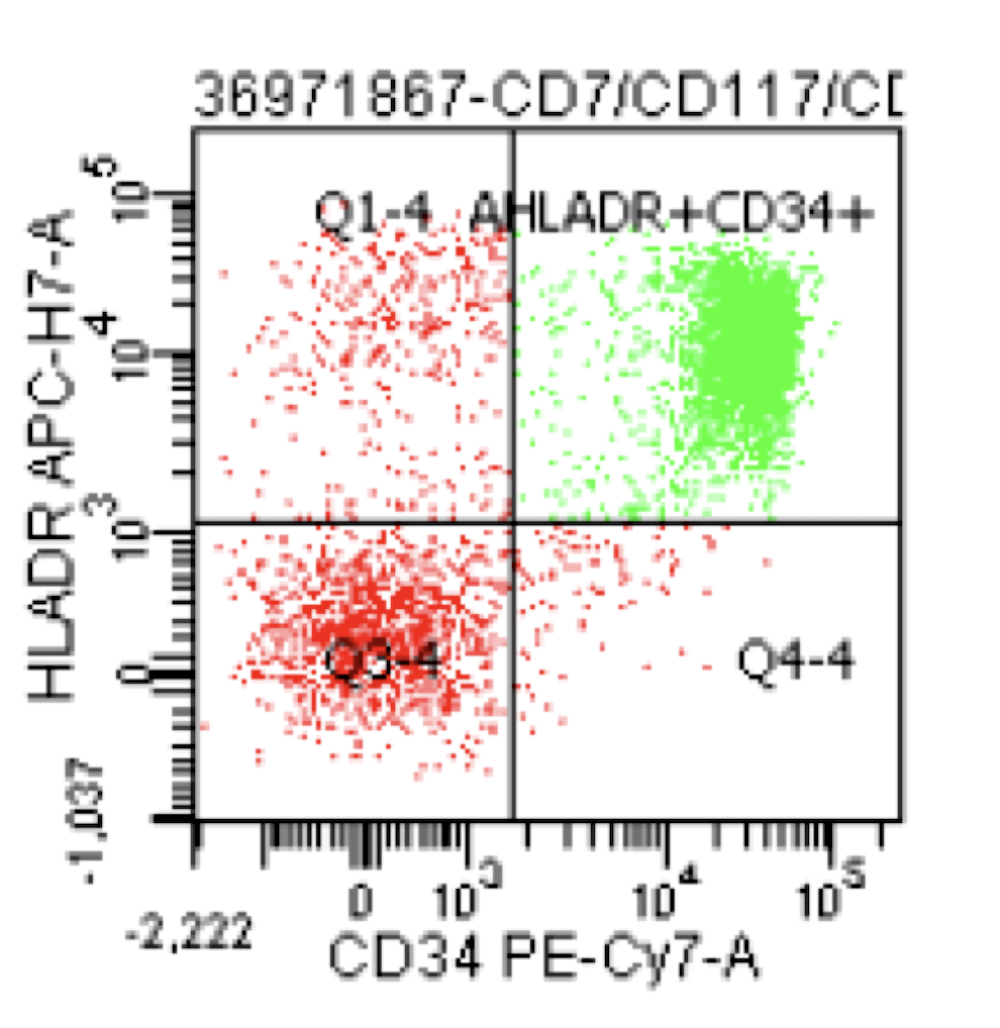
- High levels of CD34, CD13, HLA-DR and myeloperoxidase and weak CD33 expression
- Frequent aberrant expression of B cell markers CD19 and PAX5 (Blood 1992;80:470, Am J Clin Pathol 2006;126:235)
- Expression of CD56 is associated with concomitant KIT mutations and worse prognosis (Blood 1997;90:1643)
Flow cytometry images
Contributed by Genevieve M. Crane, M.D., Ph.D.
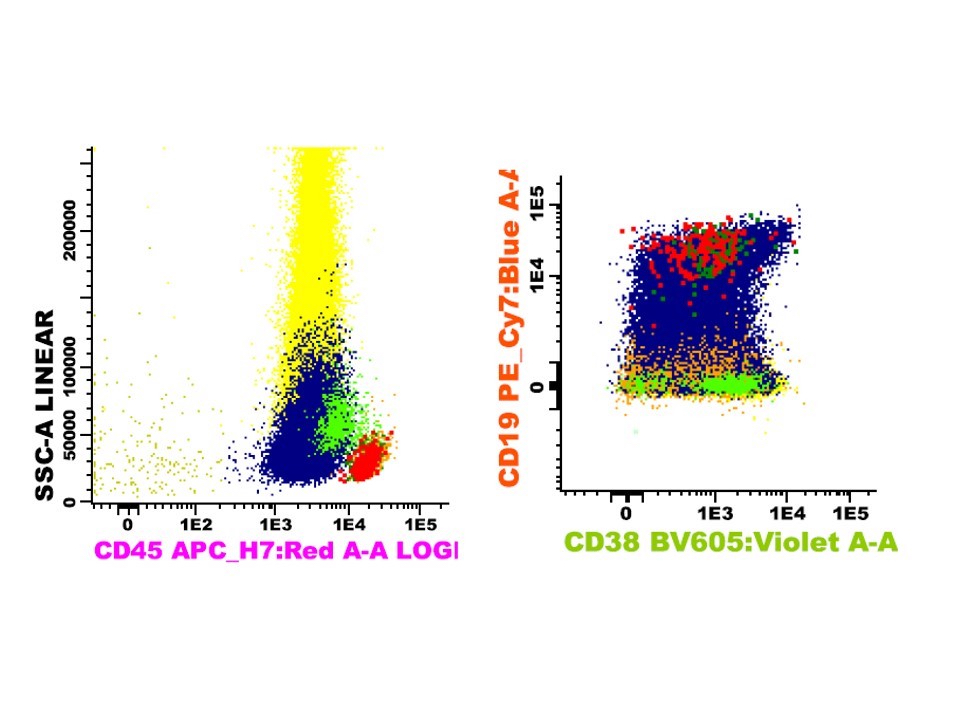
Partial CD19 expression in AML with t(8;21)
Molecular / cytogenetics description
- Demonstration of t(8;21) by real time PCR or cytogenetics
Molecular / cytogenetics images
AFIP images
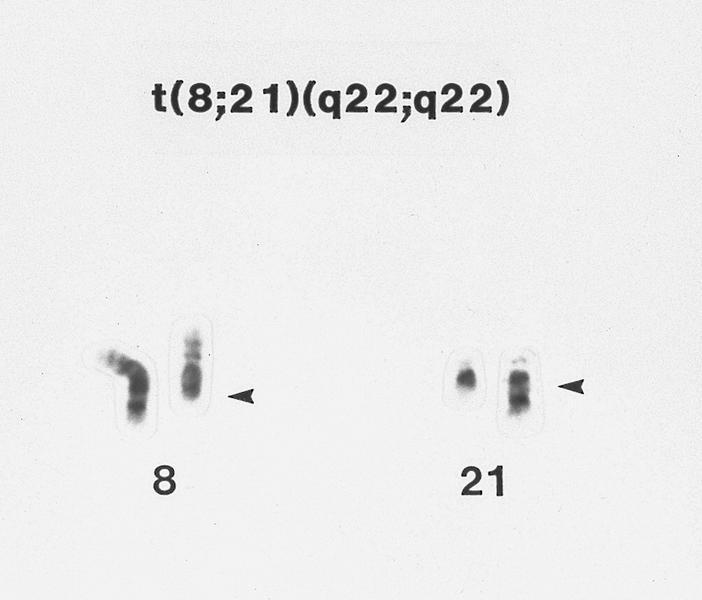
t(8;21) with abnormal chromosomes
Images hosted on other servers:

FISH probes showing
2 abnormal yellow
fusions made of red
and green probes
Sample pathology report
- Left posterior iliac crest, core biopsy and aspirate smear:
- Acute myeloid leukemia with t(8;21)(q22;q22.1); RUNX1-RUNX1T1 (see comment)
- Comment: The bone core biopsy demonstrates an increase in blasts, which are noted to have prominent eosinophilic granules on the aspirate. The presence of t(8;21) by PCR confirms the diagnosis.
Differential diagnosis
- Other AML with recurrent cytogenetic abnormalities:
- AML with t(15;17) may morphologically resemble AML with t(8;21) but would have different flow and molecular findings
- AML with myelodysplasia related changes:
- Lacks t(8;21), often has complex karyotype
- AML with maturation:
- Lacks t(8;21)
- Myelodysplastic syndromes:
- If there are < 20% blasts and no t(8;21), the findings including dysplasia and Auer rods would be compatible with a myelodystplastic syndrome
Additional references
Board review style question #1
Which of the following is true about AML with t(8;21)?
- AML with t(8;21) generally has a poor prognosis
- AML with t(8;21) frequently aberrantly expresses the lymphoid markers CD19 and PAX5
- Auer rods are rare in AML with t(8;21)
- Presence of a concomitant KIT mutation is a good prognostic finding
- Translocation is best identified by microarray
Board review style answer #1
B. AML with t(8;21) frequently aberrantly expresses the lymphoid markers CD19 and PAX5
Comment Here
Reference: AML with t(8;21)(q22;q22)
Comment Here
Reference: AML with t(8;21)(q22;q22)
Board review style question #2
A 26 year old woman is referred to the emergency department when she is noted to have 32% blasts in peripheral blood. Her smear shows large basophilic blasts with prominent eosinophilic granules and rare Auer rods. What will the flow cytometry immunophenotype likely show?
- CD34-, CD117+, HLADR-, MPO++, CD33,
- CD34+, CD33dim+, MPO+, CD71-, CD19dim+
- CD34-, CD13+, CD11b+, CD14+, CD64+, HLA-DR+
- CD34+, CD117+, CD33+, CD19-, CD3-, MPO-
- CD34+, CD19+, CD20-, CD10+, TdT+
Board review style answer #2

