
Larynx, hypopharynx & trachea
Squamous cell carcinoma
Squamous cell carcinoma of larynx
Authors: Jamie Brown, M.D., Ruta Gupta, M.D.
Editorial Board Member: Bin Xu, M.D., Ph.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 27 February 2025
Last staff update: 27 February 2025
Copyright: 2024-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma of larynx

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Brown J, Gupta R. Squamous cell carcinoma of larynx. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/larynxscc.html. Accessed April 2nd, 2025.
Definition / general
- Malignant proliferation of squamous epithelial cells
- Most common primary cancer of the larynx (CA Cancer J Clin 2017;67:31)
Essential features
- Malignant proliferation of squamous epithelial cells
- Most common primary cancer of the larynx (CA Cancer J Clin 2017;67:31)
- Strong association with smoking and alcohol use
- Recognized subtypes are conventional, verrucous, basaloid, papillary, lymphoepithelial, adenosquamous and spindle cell
Terminology
- Squamous cell carcinoma (SCC) of the larynx has several historical names; these are currently not recommended and are included below for historical interest only as these reflect the evolution of surgical pathology
- Epidermoid carcinoma
- Ackerman tumor
- Lane tumor, pseudosarcoma sarcomatoid carcinoma, carcinosarcoma
ICD coding
- Conventional squamous cell carcinoma
- ICD-O
- ICD-11
- 2B6C.0 - squamous cell carcinoma of piriform sinus
- 2B6D.0 - squamous cell carcinoma of hypopharynx and variants
- 2C23.10 - squamous cell carcinoma of larynx, glottis
- 2C23.20 - squamous cell carcinoma of larynx, supraglottis
- 2C23.30 - squamous cell carcinoma of larynx, subglottis
- 2C24.1 - squamous cell carcinoma of trachea
- Nonconventional subtypes
- Adenosquamous carcinoma
- ICD-11
- 2B6C.Y & XH7873 - other specified malignant neoplasms of piriform sinus & adenosquamous carcinoma
- 2B6D.Y & XH7873 - other specified malignant neoplasms of hypopharynx & adenosquamous carcinoma
- 2C23.1Y & XH7873 - other specified malignant neoplasms of larynx, glottis & adenosquamous carcinoma
- 2C23.2Y & XH7873 - other specified malignant neoplasms of larynx, supraglottis & adenosquamous carcinoma
- 2C23.3Y & XH7873 - other specified malignant neoplasms of larynx, subglottis & adenosquamous carcinoma
- 2C24.Y & XH7873 - other specified malignant neoplasms of trachea & adenosquamous carcinoma
- ICD-11
Epidemiology
- Second most common malignancy of the aerodigestive tract after lung cancer
- 200,000 cases globally and 123,000 deaths in 2019 (Lancet Respir Med 2021;9:1030)
- Estimated 12,650 new laryngeal cancer cases in the U.S. in 2024; 3,880 deaths (CA Cancer J Clin 2024;74:12)
- ~80% occur in males; strong male predominance is not explained by other risk factors (CA Cancer J Clin 2024;74:12, Cancer 2022;128:3531)
- Typically presents in the seventh decade
- More common in rural areas than urban, with no difference in staged matched survival (Laryngoscope 2018;128:1874)
- Strong association with smoking and alcohol use, with compounding combined effects
- Gradual decline in incidence corresponds with decreasing smoking rates
Sites
- Classified based on location in relationship to glottis as glottic, subglottic, supraglottic and tracheal
- Most tumors are glottic
- Glottis subsites include true vocal cords, anterior commissure and posterior commissure
- 30% are supraglottic
- Supraglottic subsites include suprahyoid epiglottis, aryepiglottic folds (laryngeal aspect), infrahyoid epiglottis, arytenoids and ventricular bands (or false cords)
- 1.5% are subglottic (JAMA Otolaryngol Head Neck Surg 2023;149:34)
- Primary tracheal SCC is rare
Pathophysiology
- Epithelial dysplasia is accepted as a precursor lesion
- Epithelial dysplasia can be graded using 2 tiered (low grade dysplasia / squamous intraepithelial lesion [SIL] versus high grade dysplasia / squamous intraepithelial lesion) or 3 tiered systems (also includes carcinoma in situ); by definition, the basement membrane is preserved (Head Neck Pathol 2020;14:1046)
- Chromosomal instability in precursor lesions has been associated with a significantly increased rate of progression to invasive cancer (Pathology 2014;46:216)
- Several driver gene mutations have been implicated in oncogenesis, including p53, cyclin D1, p16 (CDKN2a / INK4a, independent of human papillomavirus [HPV]), p14 (ARF), FHIT, RASSF1A, EGFR and RB1 (J Clin Pathol 2006;59:445, N Engl J Med 2007;357:2552)
- Significantly higher rate of smoking related mutations in laryngeal SCC compared to other head and neck SCCs (Sci Rep 2019;9:19256)
Etiology
- Smoking is strongly associated with laryngeal SCC development (Eur Arch Otorhinolaryngol 2017;274:1617)
- Heavy alcohol use is an established risk factor
- Combined smoking and alcohol use have a multiplicative effect on risk
- Gastroesophageal reflux disease (GERD) is a possible risk factor for laryngeal but not hypopharyngeal SCC (Am J Otolaryngol 2020;41:102653)
- HPV is found in a minority of cases, with recent studies finding 11.6% and 13% of cases positive (J Pathol Transl Med 2020;54:411, Oral Oncol 2019;98:20)
- Unlike oropharyngeal SCC, the role of HPV in the carcinogenesis of laryngeal SCC has not been established (Head Neck 2011;33:581, Nat Rev Dis Primers 2020;6:92)
- Unlike lymphoepithelial carcinoma of the nasopharynx, lymphoepithelial carcinoma of the larynx does not appear to be associated with Epstein-Barr virus (EBV) (Mod Pathol 2019;32:621)
Clinical features
- Most common presentation is hoarseness with or without sore throat
- Larger lesions can present with dysphagia or airway obstruction
- Women are more likely to present with supraglottic tumors (Arch Otolaryngol Head Neck Surg 1991;117:774)
- Clinical staging includes endoscopic visualization of the larynx, palpation of cervical nodes, cranial nerve examination and endoscopic assessment of vocal cord mobility (Amin: AJCC Cancer Staging Manual, 8th Edition, 2017)
Diagnosis
- Clinical evaluation of vocal cord mobility / function is crucial for identifying a lesion, staging, prognosis and determining treatment modalities (Oral Oncol 2024;152:106744)
- Diagnosis requires histological assessment, with biopsy during direct laryngoscopy being the most common method to obtain tissue from the primary tumor
- Fine needle aspiration (FNA) cytology of suspected nodal disease is also commonly employed as part of diagnostic workup
Radiology description
- Computed tomography (CT): asymmetrical enhancing tissue mass that may be exophytic or infiltrative
- Magnetic resonance imaging (MRI) is limited by motion artifact and is typically used to assess for cartilage involvement (T4a) when CT is equivocal (Hodler: Diseases of the Brain, Head and Neck, Spine 2020-2023 - Diagnostic Imaging, 1st Edition, 2020)
Prognostic factors
- 5 year survival rate is (Laryngoscope Investig Otolaryngol 2020;5:74)
- 77.4% for localized disease
- 44.7% for patients with regional nodal involvement
- 33.3% for those with distant disease
- Prognosis is dependent on anatomical location and stage
- Glottic tumors tend to present at an earlier stage and have a better prognosis; this is primarily due to poor lymphatic supply and lower incidence of regional node involvement
- Supraglottic tumors are more likely to have nodal disease at presentation (Laryngoscope Investig Otolaryngol 2020;5:74)
- Subglottic tumors have a poor prognosis (Braz J Otorhinolaryngol 2022;88:S70)
- Prognosis depends upon histologic subtypes
- Verrucous carcinoma does not metastasize and has a better prognosis than conventional SCC, with an overall survival rate of 80.3% (Otolaryngol Head Neck Surg 2017;156:38)
- Papillary SCC has a better prognosis than conventional SCC, with a 5 year disease specific survival rate of 83.1% (Otolaryngol Head Neck Surg 2015;153:54)
- Spindle cell SCC has a comparable prognosis to conventional SCC and generally presents at an early stage (Am J Surg Pathol 2002;26:153)
- Overall disease specific 5 year survival rate is 74.1% (Laryngoscope 2015;125:2709)
- Basaloid SCC has traditionally been considered a more aggressive subtype, with a poorer prognosis compared to conventional SCC in the larynx (JAMA Otolaryngol Head Neck Surg 2013;139:1306)
- Adenosquamous carcinoma is considered more aggressive than conventional laryngeal SCC
- Prognosis also depends upon the presence or absence of adverse histopathologic factors
- Japanese study comparing early stage SCC subtypes found equivalent survival rates for conventional, verrucous, papillary and spindle cell, with adenosquamous having a worse prognosis (Acta Otolaryngol 2023;143:70)
- For early stage glottic cancers, positive margins do not affect local control and surgical margins of 1 - 2 mm are considered adequate (Eur Arch Otorhinolaryngol 2018;275:2333, Curr Oncol Rep 2020;22:82)
- Patients with advanced cancers with involved margins have a significantly worse prognosis than those with close or clear margins (Curr Oncol Rep 2020;22:82)
- Proportion of involved nodes is an important prognostic factor (J Otolaryngol Head Neck Surg 2020;49:31)
- HPV status has not been shown to affect prognosis (Cureus 2018;10:e2234)
- Occult metastasis occurs in ~20% of laryngeal SCCs and is more common in supraglottic cases, with a greater risk at advanced stage (Ann Otol Rhinol Laryngol 2021;130:67)
- Staging (see Staging-larynx)
- Specific tumor staging criteria (pT) for each site: supraglottis, glottis and subglottis
- pT stage relates to the extent of involvement of adjacent structures
- pN stage is dependent on the number of involved nodes (single versus multiple), their site (ipsilateral versus contralateral), the size of the deposit (cutoffs 3 cm and 6 cm) and the presence of extranodal extension
Case reports
- 55 year old man with 2 month history of hoarseness (lymphoepithelial carcinoma) (Front Surg 2022;9:851481)
- 65 year old man who presented with hoarseness and dyspnea (Int J Surg Case Rep 2023;111:108791)
- 72 year old man with 2 month history of progressive worsening dysphonia (Rare Tumors 2024;16:20363613241242705)
Treatment
- Treatment goals include local control of cancer and the preservation of laryngeal function
- Surgery, chemotherapy, radiotherapy or a combination of these
- Definitive radiotherapy with or without chemotherapy can be considered for low stage or low volume glottic tumors (Cancer Control 2016;23:208)
- Total laryngectomy is used for definitive treatment and salvage therapy
- Neck dissection is usually carried out with laryngectomy
Gross description
- Conventional SCC is firm, white and presents as exophytic masses or with endophytic growth patterns; ulceration is usually present
- Verrucous SCC is typically exophytic with a hyperkeratotic and friable, ragged surface (Head Neck Pathol 2011;5:23)
- Papillary SCC has a papillary appearance macroscopically and is usually friable and soft, with frond-like extension into the lumen (Head Neck Pathol 2011;5:23)
- Spindle cell SCC is usually a polypoid mass macroscopically
- Basaloid SCC, lymphoepithelial carcinoma and adenosquamous carcinoma have a similar appearance to conventional SCC and may have necrosis
- Higher stage tumors can invade adjacent sites, making classification of primary tumor site or subsite difficult
- References: Goldblum: Rosai and Ackerman's Surgical Pathology, 11th Edition, 2017, Longacre: Mills and Sternberg's Diagnostic Surgical Pathology, 7th Edition, 2022
Gross images
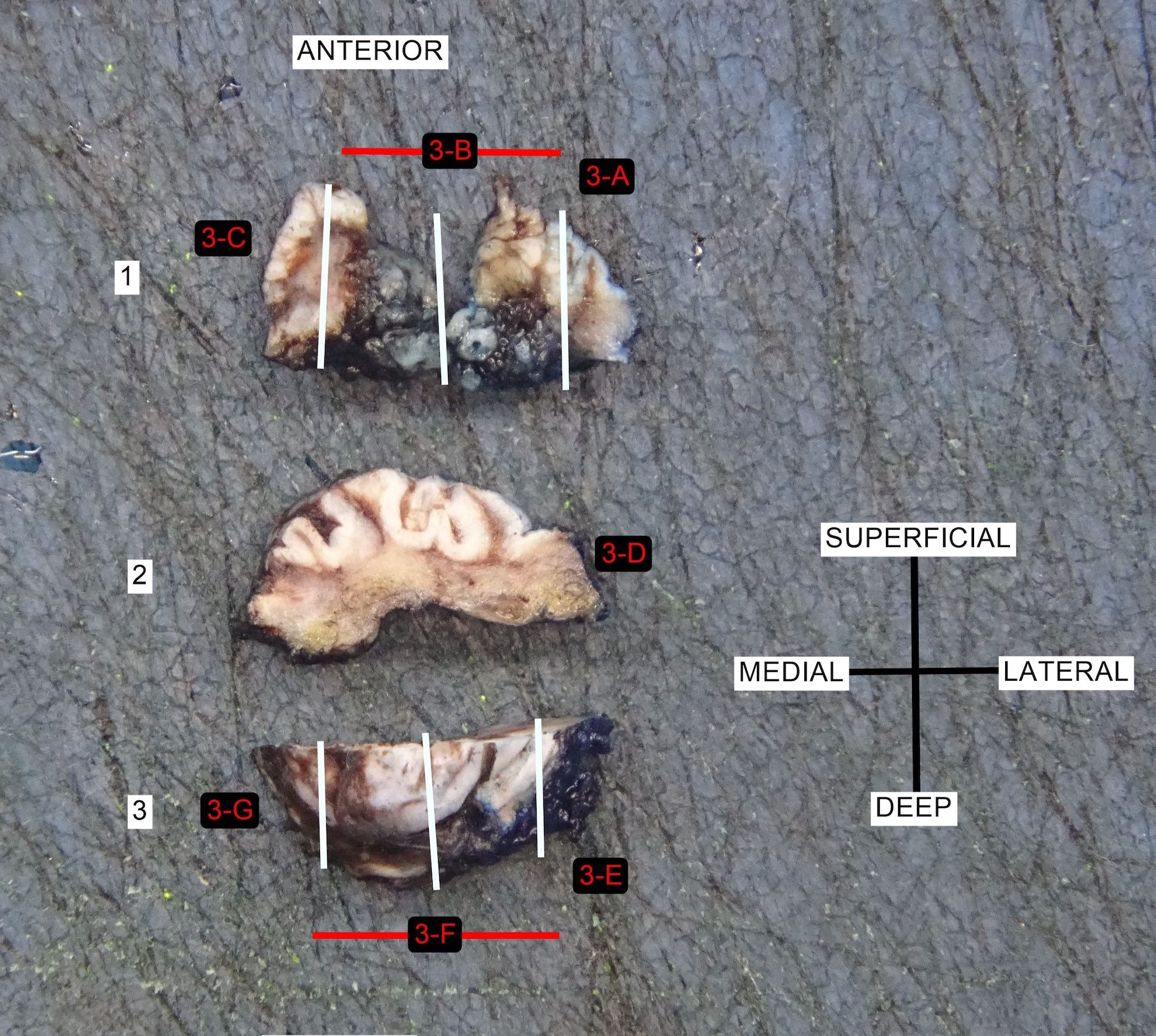
Contributed by Jamie Brown, M.D. and Ruta Gupta, M.D.

Conventional laryngeal SCC
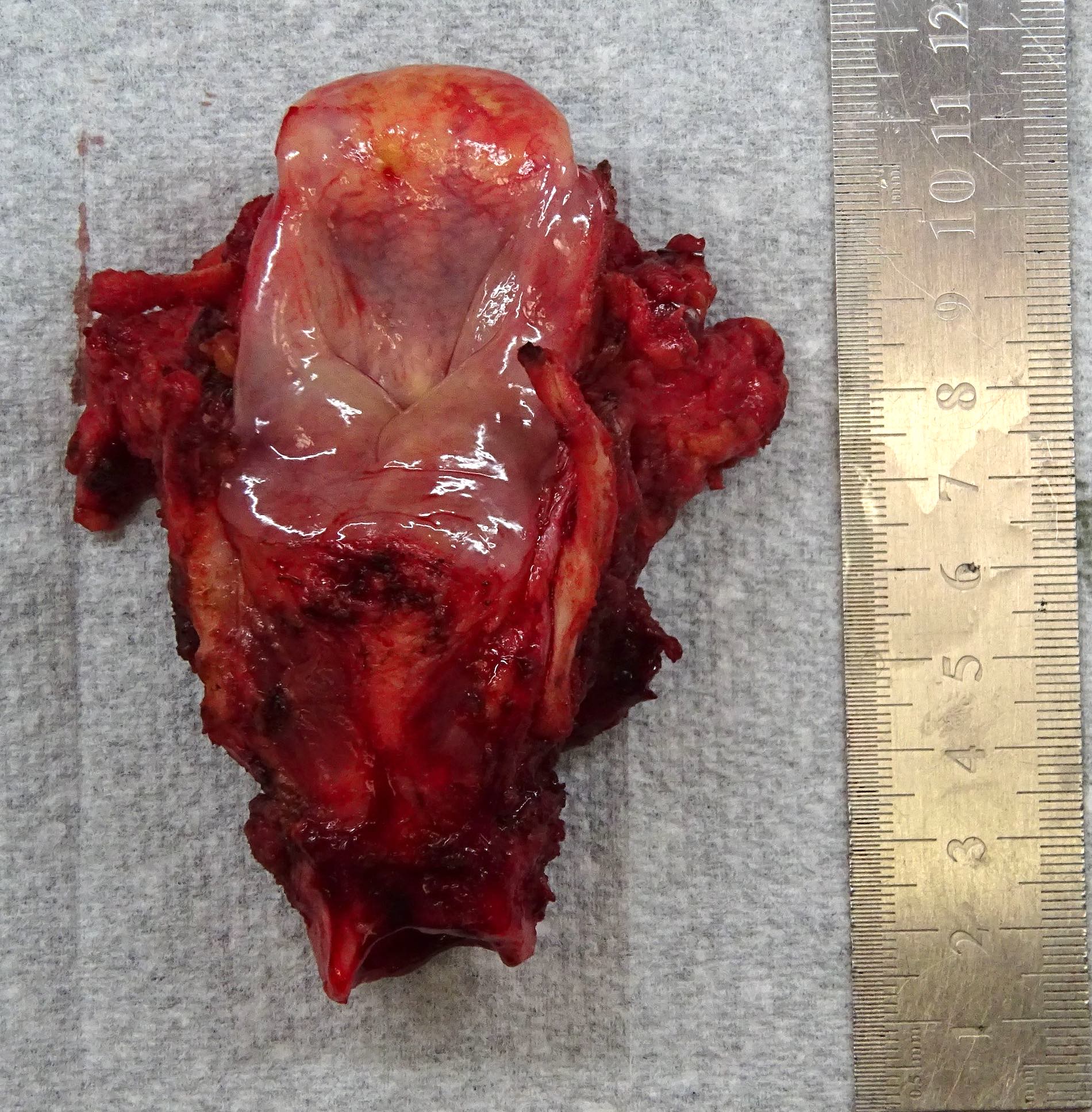
Laryngectomy (fresh)

Laryngectomy specimen (fixed)

Laryngectomy specimen (fixed) and bisected
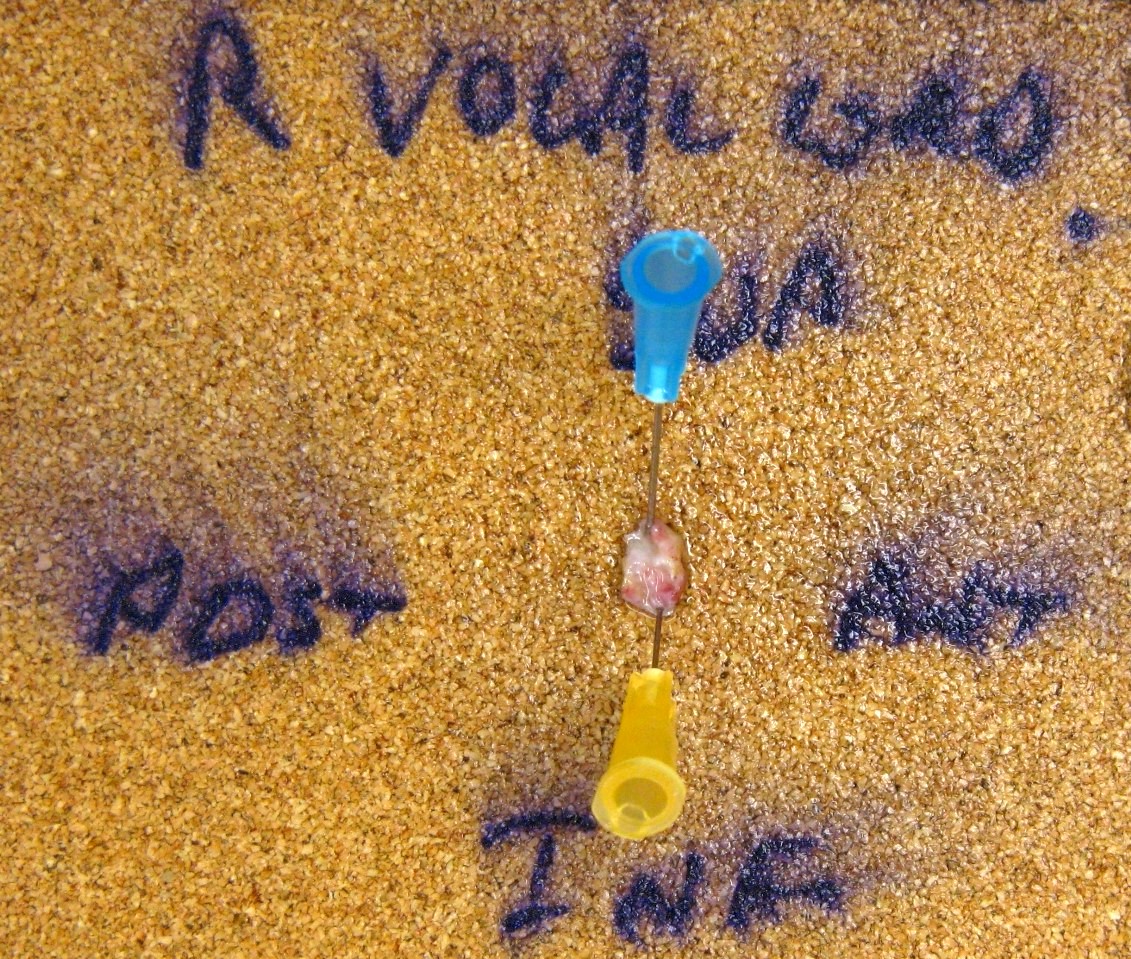
Laser vocal cord resection

Verrucous SCC
Microscopic (histologic) description
- In situ lesions (noninvasive) can be keratinizing or nonkeratinizing
Squamous cell carcinoma
- Conventional SCC
- Histologically, similar to conventional squamous cell carcinoma at other head and neck sites
- Typically consists of nests of squamous cells with or without keratin pearls and intercellular bridges
- Evidence of stromal invasion is required for diagnosis: desmoplastic stromal reaction is usually present
- Tumor grading is based on resemblance to normal squamous epithelium
- WHO diagnostic criteria
- Essential: a malignant epithelial neoplasm with evidence of squamous differentiation and stromal invasion
- Evidence for squamous differentiation: keratinization with keratin pearls or the presence of intercellular bridges; immunohistochemistry may be required for poorly differentiated tumors
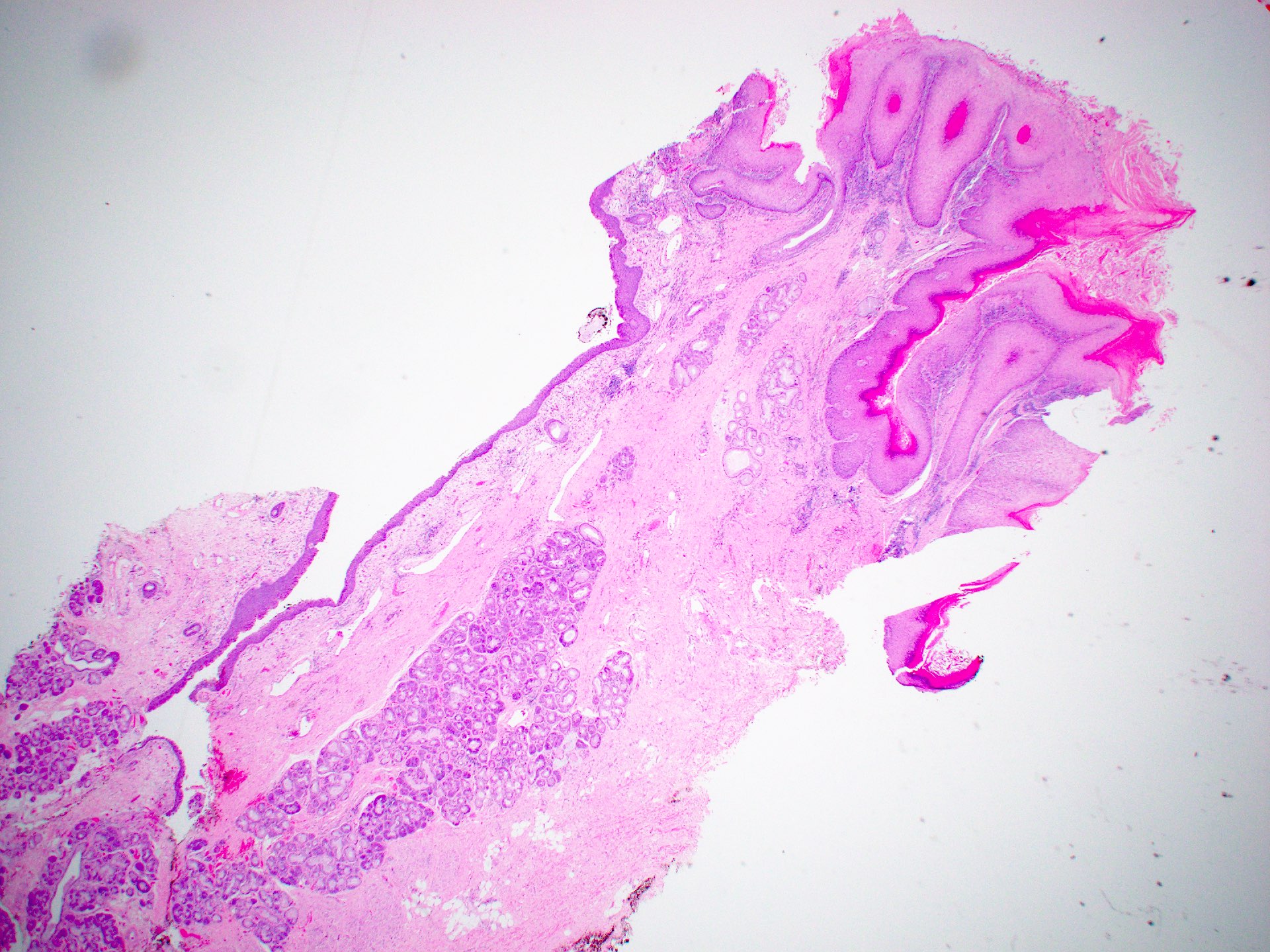
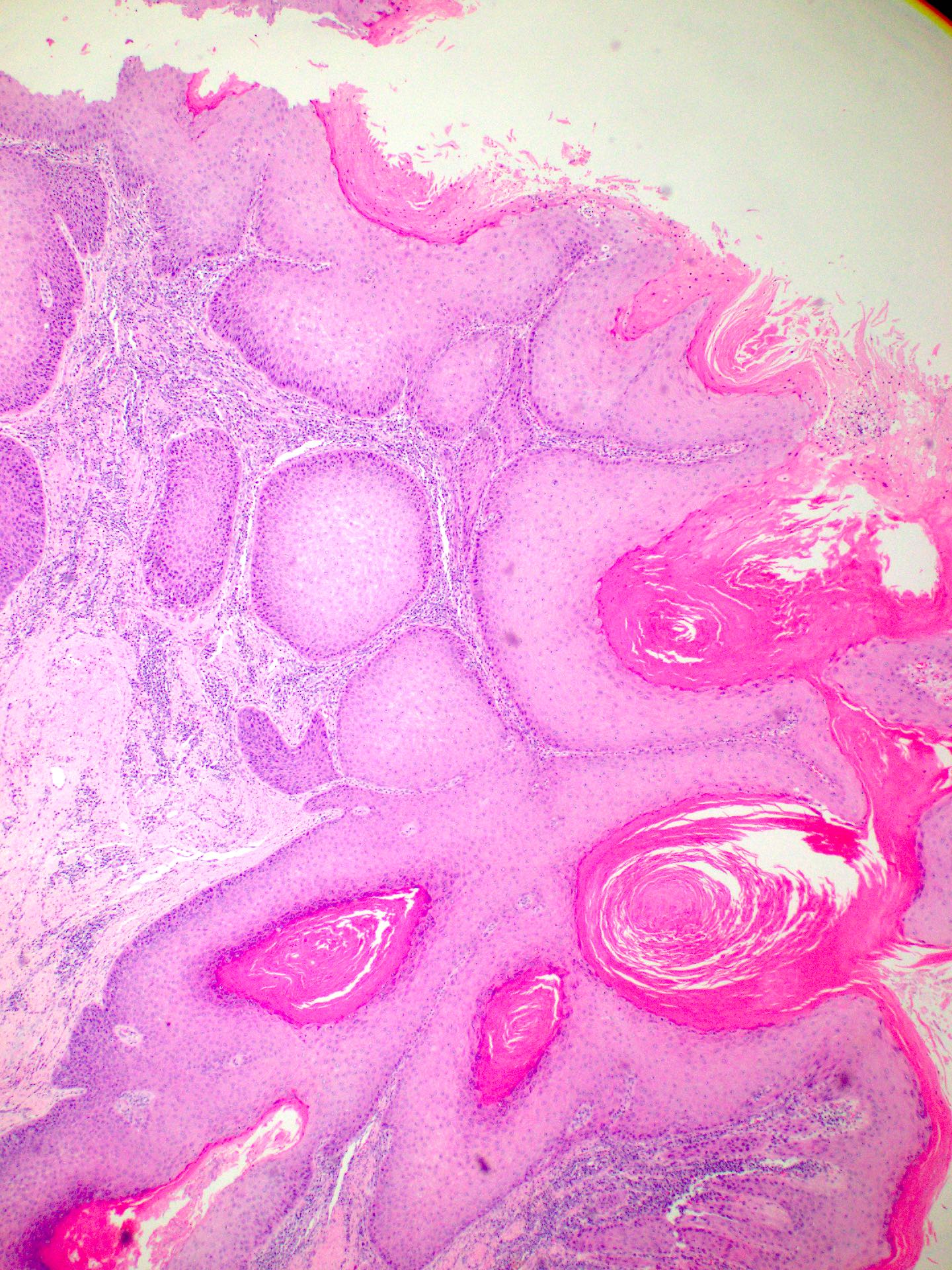
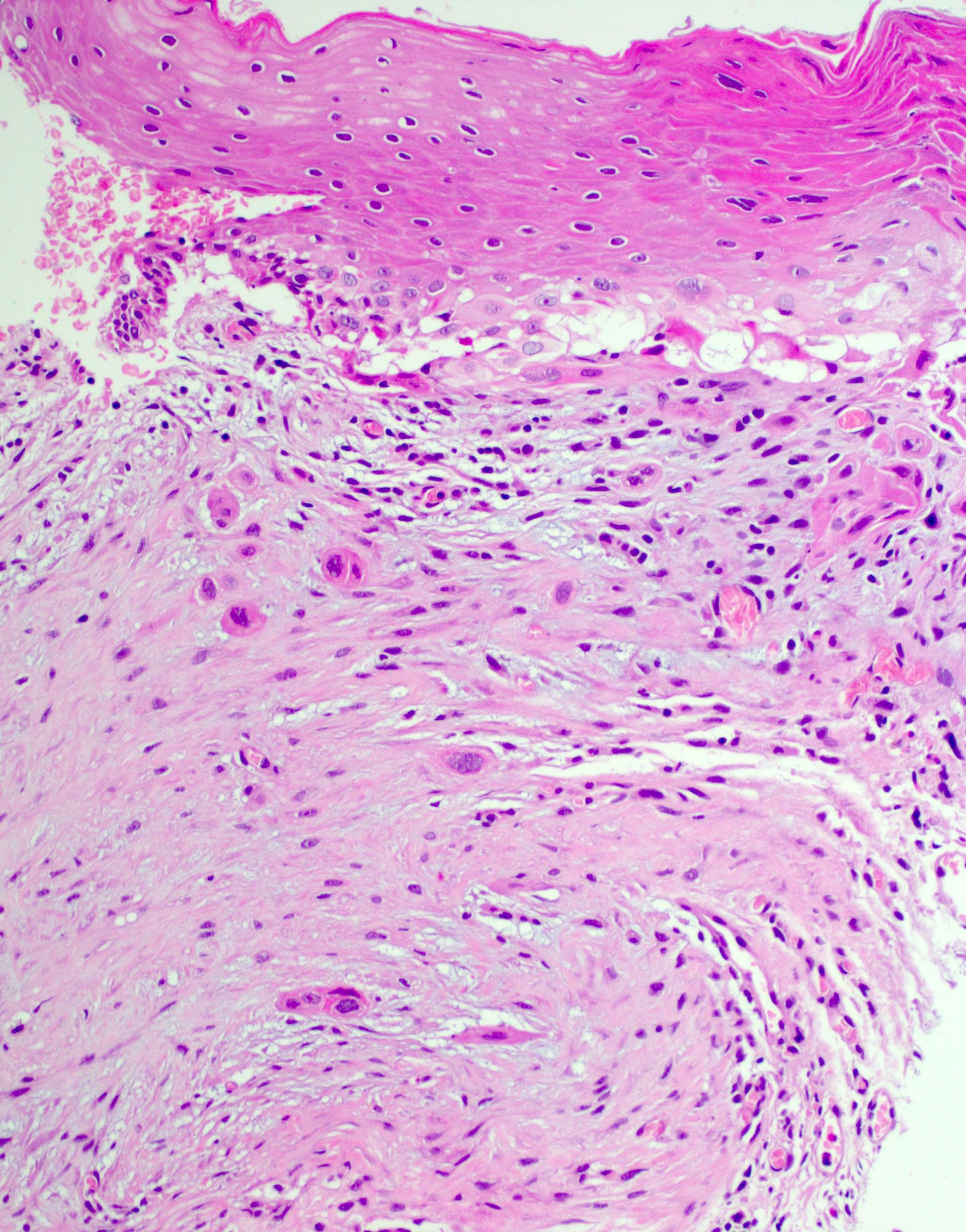
Verrucous (Head Neck Pathol 2011;5:23)
- Infoldings of well differentiated squamous epithelium with abundant surface keratinization
- Densely eosinophilic cytoplasm
- Low mitotic rate
- Pushing borders and generally absent desmoplastic stromal reaction
- Prominent lymphoplasmacytic infiltrate usually present
- Presence of any high grade dysplasia or a minor component of conventional SCC warrants a diagnosis of hybrid verrucous SCC or invasive well differentiated SCC with verrucous features (ICD-O: 8070/3)
- WHO diagnostic criteria
- Essential: acanthotic, hyperkeratotic and undulating squamous epithelium; bulbous keratotic crypts (elephant feet)
- Smooth interface with the stroma with pushing invasion below the level of the surrounding normal epithelium
- Cytologically bland squamous epithelium
- Mitoses limited to basal / parabasal layers
Papillary SCC
- Papillary architecture composed of branching fibrovascular cores lined by stratified squamous epithelium with or without keratinization
- Epithelium lining papillae show marked dysplasia, with little or no maturation and a high N:C ratio (Head Neck Pathol 2011;5:23)
- WHO diagnostic criteria
- Essential: exophytic growth composed predominantly of papillary fronds with fibrovascular cores covered by a nonkeratinizing malignant stratified squamous epithelium or in the keratinizing type, by high grade atypia
- Desirable: stromal infiltration
Basaloid
- Lesional cells resemble the basal layer of stratified squamous epithelium; tumor cells have basophilic chromatin and a high N:C ratio and are usually arranged in nests with peripheral palisading (Head Neck Pathol 2011;5:23)
- Solid and cribriform growth patterns are also common
- Tumors usually have a high mitotic rate and necrosis is frequently seen
- WHO diagnostic criteria
- Essential
- Tumor with prominent basaloid morphology
- Presence of squamous differentiation
- Absence of neuroendocrine or myoepithelial differentiation by histology or immunohistochemistry
- Desirable
- High grade histological features
- Myxoid to hyaline stromal alterations
- Essential
Adenosquamous
- Conventional SCC component and adenocarcinoma; may be juxtaposed or admixed
- Conventional SCC component may show keratinization
- Adenocarcinoma component composed of glands arranged in a tubular of cribriform configuration
- Necrosis is common
- Perineural and lymphovascular space invasion is frequently seen
- Special stains (e.g., PAS, Alcian blue) will highlight mucin in the adenocarcinoma component
- WHO diagnostic criteria
- Essential: biphasic tumor with squamous and glandular components that are distinctly recognized adjacent to each other on H&E examination
- Desirable
- Evidence of origin from surface epithelium (e.g., squamous dysplasia)
- Mucin production
Spindle cell
- Spindle cells with overt features of malignancy such as pleomorphism, high mitotic rate, atypical mitoses
- May contain a conventional SCC component or intraepithelial dysplasia
- Heterologous differentiation may be present
- WHO diagnostic criteria
- Essential: a mucosa based carcinoma with a malignant spindle cell component
- Desirable
- Polypoid tumor
- Intraepithelial dysplasia
- Invasive conventional SCC
- Immunoreactivity for cytokeratin or p63 / p40 (in selected cases)
Lymphoepithelial
- Syncytial growth with a prominent lymphoplasmacytic infiltrate: may obscure tumor cells
- Solid or nested growth pattern
- Tumor cells usually have prominent nucleoli and a high mitotic rate
- Conventional SCC component may be present
- WHO diagnostic criteria
- Essential
- Tumor with syncytial growth
- Inflammatory infiltrate
- Vesicular chromatin
- Prominent nucleoli
- Desirable
- Positivity for pankeratin and squamous markers (e.g., p40, CK5/6)
- Exclusion of direct extension or metastasis
- Essential
Microscopic (histologic) images
Contributed by Jamie Brown, M.D. and Ruta Gupta, M.D.
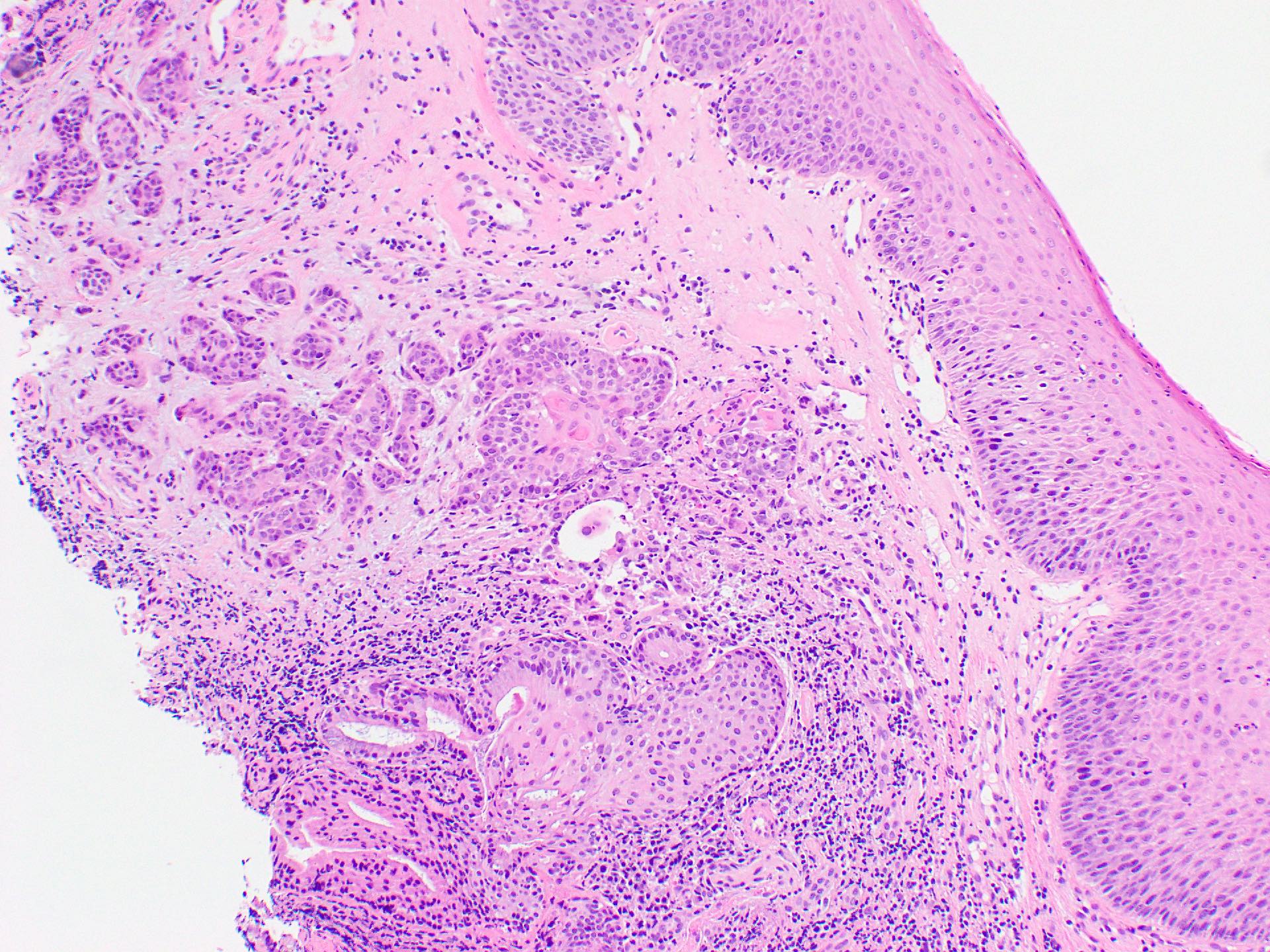
Conventional laryngeal SCC
Verrucous SCC
Spindle cell SCC
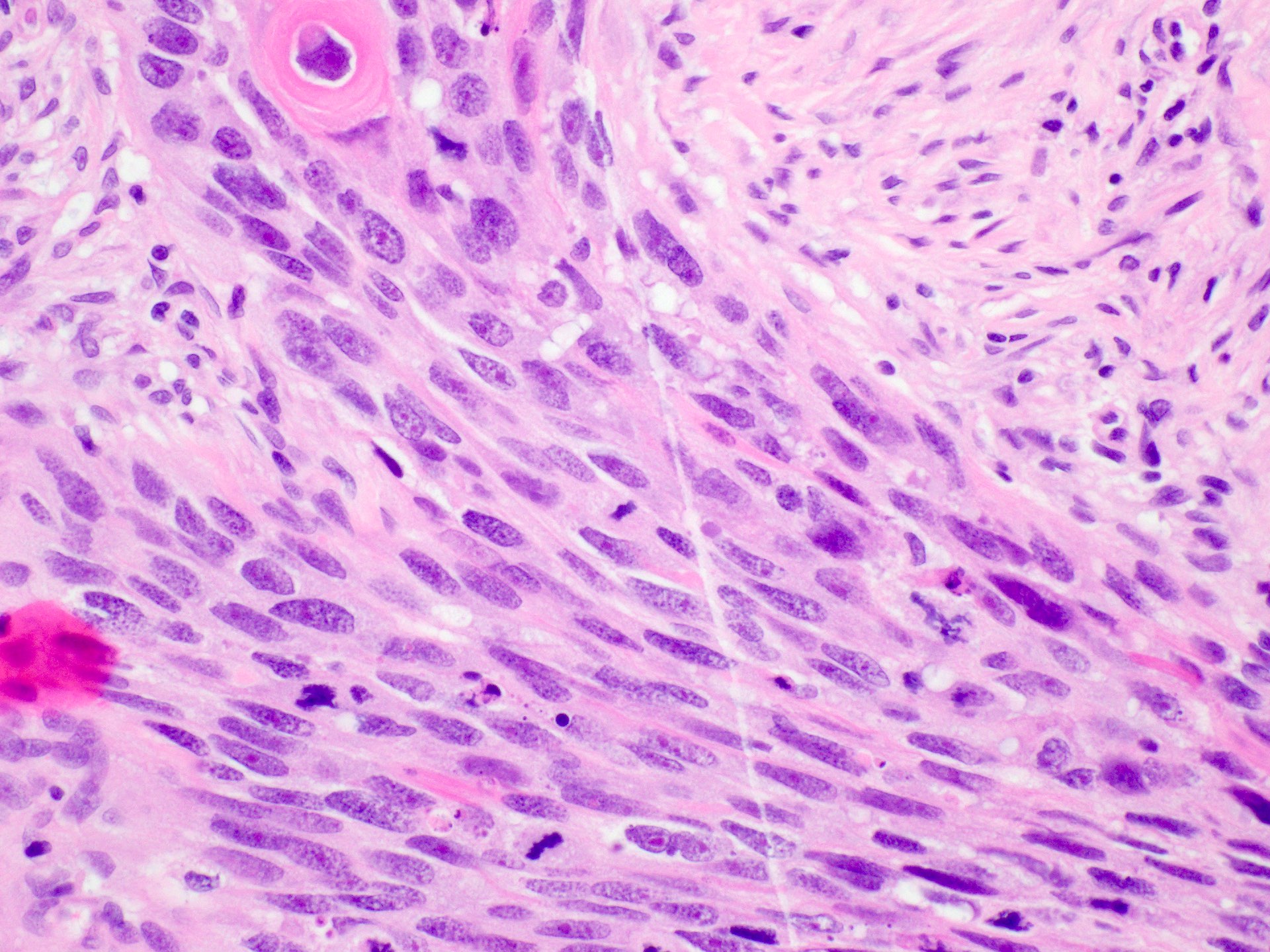
Spindle cell SCC
Drop invasion
Positive stains
- Cytokeratin
- p63 / p40
- Adenocarcinoma component of adenosquamous carcinoma is usually CK7 and CEA positive
- Majority (59%) of basaloid SCC: SOX10 (Head Neck Pathol 2019;13:543)
- p16 overexpression should not be interpreted as HPV infection (Br J Cancer 2015;112:1098)
Negative stains
- Synaptophysin, chromogranin, INSM1, SMA, S100, MelanA, HMB45, muscle specific actin and GFAP, CD45 (LCA), CD20, TTF1, napsin A
- Spindle cell SCC may be SMA (47%) and desmin (28%) positive (Virchows Arch 2021;479:729)
Sample pathology report
- Larynx, laryngectomy:
- Moderately differentiated invasive squamous cell carcinoma of the glottis, 22 mm, margins clear by at least 5 mm
- No lymphovascular or perineural invasion
- 0/7 lymph nodes involved (see synoptic report)
Differential diagnosis
Well to moderately differentiated conventional SCC
Poorly differentiated conventional SCC
Papillary
Verrucous SCC
Basaloid SCC
Adenosquamous
Spindle SCC
Lymphoepithelial carcinoma
- Pseudoepitheliomatous hyperplasia:
- Overlying necrotizing sialometaplasia, granular cell tumor or infection
- Generally seen in the setting of inflammation; granulomas or giant cells may be present
- Identification of underlying causes
- Verrucous SCC:
- Broad tongues of invasion below the adjacent normal epithelium
- Prominent keratinization
- Lacks significant atypia
- Papillary SCC:
- Exophytic growth of papillary fronds with fibrovascular cores
Poorly differentiated conventional SCC
- Malignant melanoma:
- Lymphomas, particularly diffuse large B cell lymphoma:
- CD45 positive
- Cytokeratin and p40 / p63 negative
- Neuroendocrine neoplasms:
- Chromogranin, synaptophysin and INSM1 positive
- p40 / p63 negative
Papillary
- Verrucous SCC:
- Lacks significant cytological atypia and prominent keratinization
- Laryngeal papilloma:
- Lacks cytological atypia; lack of stromal infiltration (not required for papillary SCC diagnosis)
Verrucous SCC
- Verrucous hyperplasia:
- Histologically identical but lacks invasion
- Well differentiated conventional SCC:
- Irregular, infiltrative growth and more cytological atypia
Basaloid SCC
- Adenoid cystic carcinoma:
- No significant pleomorphism, no mitotic activity and no squamous differentiation
- Small cell carcinoma:
- Positive neuroendocrine markers
Adenosquamous
- Conventional SCC or basaloid SCC with entrapped nonneoplastic glands
- Lobular architecture and bland morphology of entrapped of glands
- Mucoepidermoid carcinoma (MEC):
- Lack of in situ component
- Lacks true squamous differentiation (instead has intermediate cells)
- Lacks MAML2 translocation (FISH)
Spindle SCC
- Stromal reaction in conventional SCC, especially following radiotherapy:
- Other sarcomas (e.g., chondrosarcoma):
- Lack of cytokeratin / p40 / p63 expression
- Lack of in situ or conventional component
- Inflammatory myofibroblastic tumor:
Lymphoepithelial carcinoma
- Large cell lymphomas (e.g., diffuse large B cell lymphoma):
- Lack of cytokeratin reactivity
- Positive for lymphoid markers (e.g., CD45)
- Metastatic / locally advanced nasopharyngeal carcinoma:
- Clinical correlation
- EBV positive
Additional references
Board review style question #1
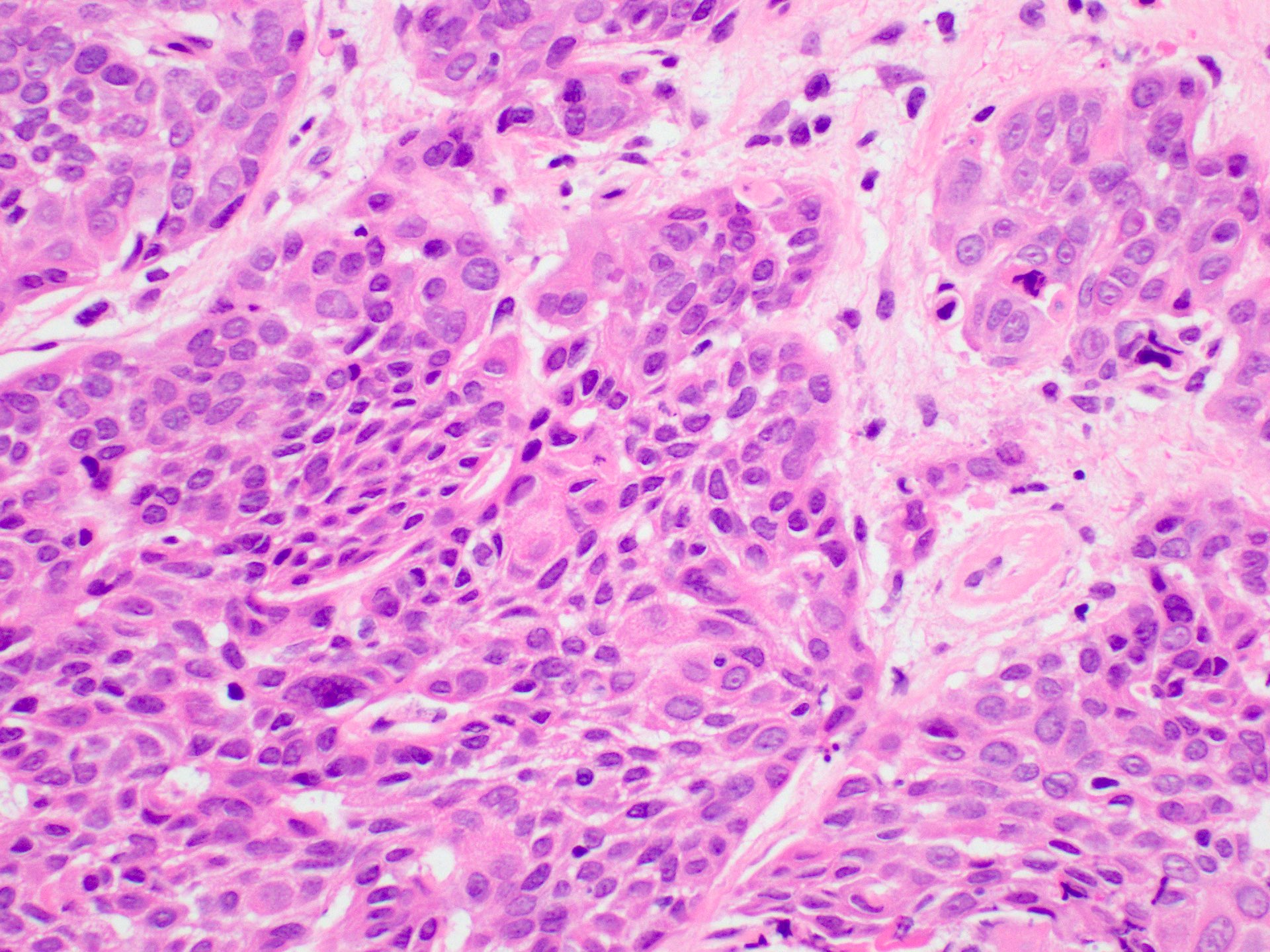
The image above shows an invasive lesion present on the larynx of a 52 year old man. Which of the following is true?
- The patient is likely to be a past or current smoker
- The patient is likely to have a family history of laryngeal cancer
- The patient is likely to have had a high risk HPV infection in the past
- The patient is likely to have had an EBV infection in the past
- The patient is likely to have poorly controlled diabetes
Board review style answer #1
A. The patient is likely to be a past or current smoker. Laryngeal squamous cell carcinoma (SCC) is strongly associated with smoking. Answer C is incorrect because unlike mucosal SCC at other head and neck sites, laryngeal SCC is not generally associated with HPV infection. Answer D is incorrect because laryngeal SCC is not associated with EBV infection. Answer E is incorrect because laryngeal SCC is not associated with diabetes. Answer B is incorrect because most laryngeal SCC cases are sporadic.
Comment Here
Reference: Squamous cell carcinoma of larynx
Comment Here
Reference: Squamous cell carcinoma of larynx
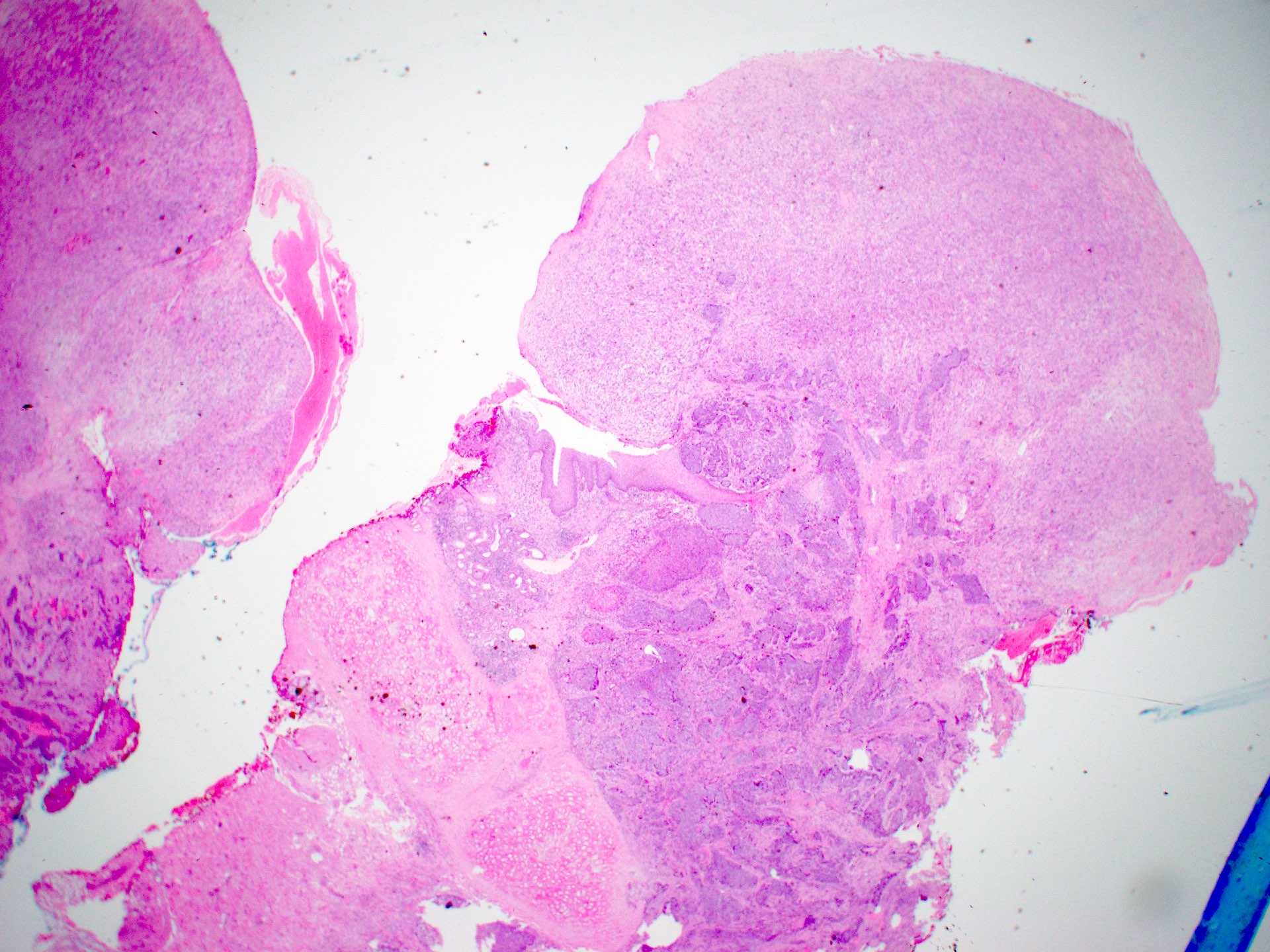
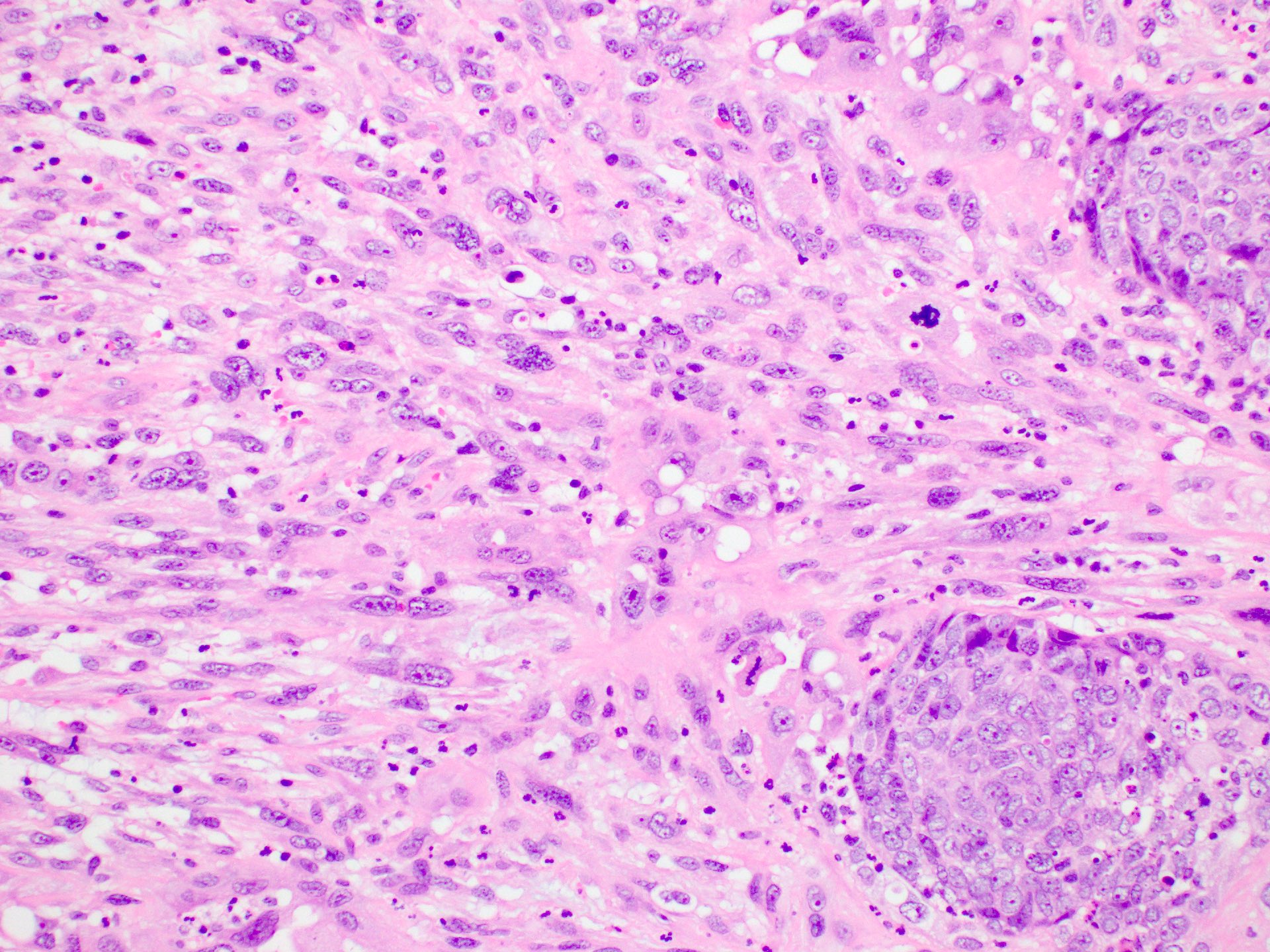
Board review style question #2
The image above shows an incisional biopsy of a suspicious lesion from a false vocal cord in a 62 year old man. The lesion is centered in the glottis and extends superiorly. Which of the following is true about regional node involvement in this case?
- Can be excluded due to the glottic location of the tumor
- Less likely as the micrograph shows HPV associated SCC
- Less likely due to the involvement of supraglottic structures
- More likely due to the involvement of supraglottic structures
- Unlikely as the micrograph shows the verrucous subtype
Board review style answer #2
D. More likely due to the involvement of supraglottic structures. The micrograph shows conventional invasive squamous cell carcinoma. We are told that the lesion is centered on the glottis, which has a poor lymphatic supply. Supraglottic structures, such as the false vocal cords, have better lymphatic supply and their involvement increases the risk of regional node involvement. Answer B is incorrect because HPV status has not been shown to affect the risk of regional node involvement in laryngeal squamous cell carcinoma. Answer C is incorrect because supraglottic structures have a better lymphatic supply than the glottis (on which the tumor is centered) and therefore increase the risk of regional node involvement. Answer E is incorrect because the micrograph shows conventional SCC with irregular infiltrative nests as opposed to the broad invasive front of verrucous SCC. Answer A is incorrect because regional lymph node involvement cannot be excluded on the basis of an incisional biopsy, regardless of the location.
Comment Here
Reference: Squamous cell carcinoma of larynx
Comment Here
Reference: Squamous cell carcinoma of larynx
