
Kidney tumor
General
Grading
Editorial Board Members: Bonnie Choy, M.D., Debra L. Zynger, M.D.


Last author update: 27 April 2023
Last staff update: 27 April 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Nuclear grading kidney


Table of Contents
Definition / general | Essential features | WHO / ISUP 4 tier grading system | Value of grading in other RCC | Variable value of grading for RCC | Microscopic (histologic) images | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Rizkalla C, Tretiakova M. Grading. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumormalignantnucleargrading.html. Accessed March 31st, 2025.
Definition / general
- Grading of renal carcinoma is important for prognosis and is either required by reporting agencies or recommended by professional organizations such as the College of American Pathologists (CAP), International Collaboration on Cancer Reporting (ICCR), Royal College of Pathologists Australasia (RCPA), International Society of Urological Pathology (ISUP), Genitourinary Pathology Society (GUPS) and World Health Organization (WHO)
Essential features
- Important for prognosis and usually required or recommended by reporting agencies or professional organizations
- WHO / ISUP 4 tier grading system replaces Fuhrman grading system
- Based on the single high power field showing the greatest degree of pleomorphism, rather than the predominant grade
WHO / ISUP 4 tier grading system
- Replaces Fuhrman grading system (Histopathology 2016;68:475, Pathologe 2016;37:355)
- Based on the single high power field showing the greatest degree of pleomorphism, rather than the predominant grade
- Validated as a prognostic parameter for clear cell and papillary renal cell carcinoma (RCC)
- Value of grading in other RCCs is yet to be determined; in the meantime, the WHO recommends grading most RCCs for descriptive purposes and for future studies
- Grades 1 - 3: degree of nucleolar prominence (Histopathology 2019;74:4)
- Not applicable
- Example: chromophobe RCC
- Grade 1: nucleoli absent or inconspicuous and basophilic at 400x magnification
- Grade 2: nucleoli conspicuous and eosinophilic at 400x magnification, visible but not prominent at 100x magnification
- Grade 3: nucleoli conspicuous and eosinophilic at 100x magnification
- Not applicable
- Grade 4: extreme nuclear pleomorphism, anaplastic giant cells, rhabdoid morphology and sarcomatoid differentiation (Histol Histopathol 2004;19:113, Histopathology 2019;74:4)
- Other factors affecting grade:
- Modified ISUP / WHO grading system has been proposed by GU experts to incorporate microscopic tumor necrosis into grading clear cell RCC (Am J Surg Pathol 2013;37:311)
- Tumors with microscopic tumor necrosis behave as tumors with 1 grade level higher (e.g., there is no difference in cancer specific survival between patients with grade 2 with necrosis and grade 3 without necrosis)
- If the patient has undergone presurgical renal embolization, tumor necrosis cannot be assessed
- Modified ISUP / WHO grading system has been proposed by GU experts to incorporate microscopic tumor necrosis into grading clear cell RCC (Am J Surg Pathol 2013;37:311)
Comparison of historic Fuhrman grading and current WHO / ISUP grading systems for renal cell carcinoma (Am J Surg Pathol 1982;6:655)
| Grading system | |
| Grade 1
| Small, round, uniform (10 um)
| Absent / inconspicuous
| Absent / inconspicuous at 400x
| Grade 2
| Larger (15 um)
| Visible at 400x
| Eosinophilic and visible at 400x
| Grade 3
| Larger, irregular (20 um)
| Visible at 100x
| Eosinophilic and prominent at 100x
| Grade 4
| Pleomorphic, bizarre, giant
| Chromatin clumps
| Pleomorphic, giant, rhabdoid, sarcomatoid
| | |||||||||||
Value of grading in other RCC
- Chromophobe RCC (chRCC)
- Current WHO recommendation is to not grade chRCC using WHO / ISUP grading system as these tumors have innate nuclear pleomorphism, multinucleation, hyperchromasia and often lack visible nucleoli; thus, current grading does not correlate to outcomes (Virchows Arch 2020;476:409)
- Grading of chRCC is a highly controversial topic and studies are inconclusive
- A novel 3 tiered grading system discounting nuclear atypia was proposed (Am J Surg Pathol 2010;34:1233)
- Tumors with geographic nuclear crowding and anaplasia portend a higher grade
- Most recently, a 2 tiered model to predict the aggressiveness was proposed (Virchows Arch 2020;476:409)
- chRCC with necrosis or sarcomatoid differentiation of chRCC = high grade
- Although chRCC has a favorable prognosis, those that are high grade based on this definition are the ones that tend to progress (if progression were to occur)
- A novel 3 tiered grading system discounting nuclear atypia was proposed (Am J Surg Pathol 2010;34:1233)
Variable value of grading for RCC
- WHO / ISUP grading is not equally significant for all RCC subtypes; the WHO divides them into several categories based on grading value
| # | Categories | Examples |
| 1 | Validated | Clear cell RCC, papillary RCC |
| 2 | Not applicable | Chromophobe RCC, TFE3 rearranged RCC |
| 3 | Potentially useful | SDH deficient RCC, mucinous tubular and spindle cell carcinoma, ELOC mutated RCC, TFEB altered RCC, RCC (NOS), FH deficient RCC (including HLRCC RCC) |
| 4 | Inherently aggressive irrespective of grade | Collecting duct carcinoma, SMARCB1 deficient renal medullary carcinoma |
| 5 | Grading is potentially misleading | Tubulocystic carcinoma, acquired cystic disease associated RCC, eosinophilic solid and cystic RCC, eosinophilic vacuolated tumor |
| 6 | Low grade features are essential for accurate histologic classification | Papillary adenoma, multilocular cystic renal neoplasm of low malignant potential, clear cell papillary renal cell tumor |
| 7 | Neoplasms with limited data on grading or behavior | ALK rearranged RCC, other oncocytic tumors |
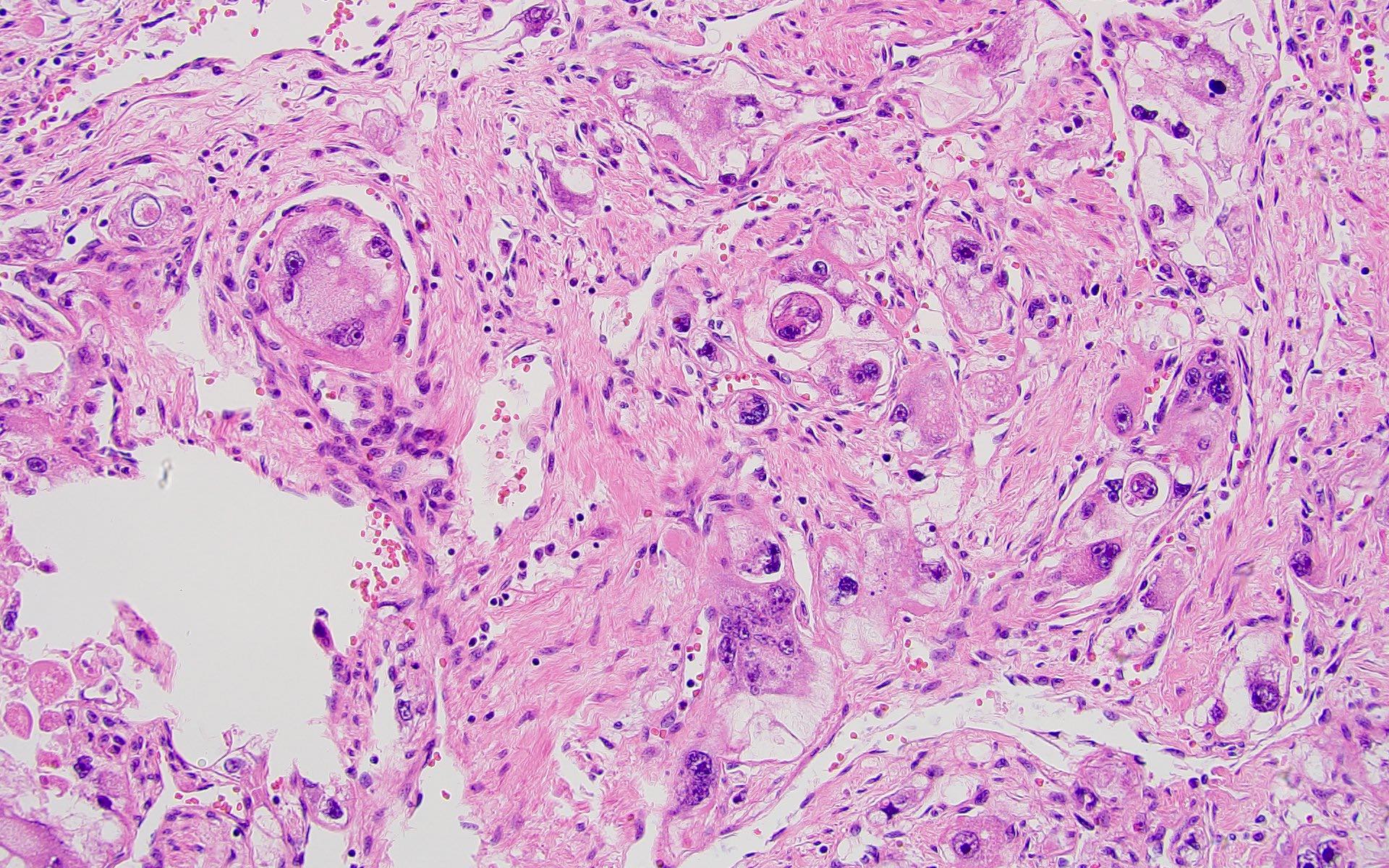
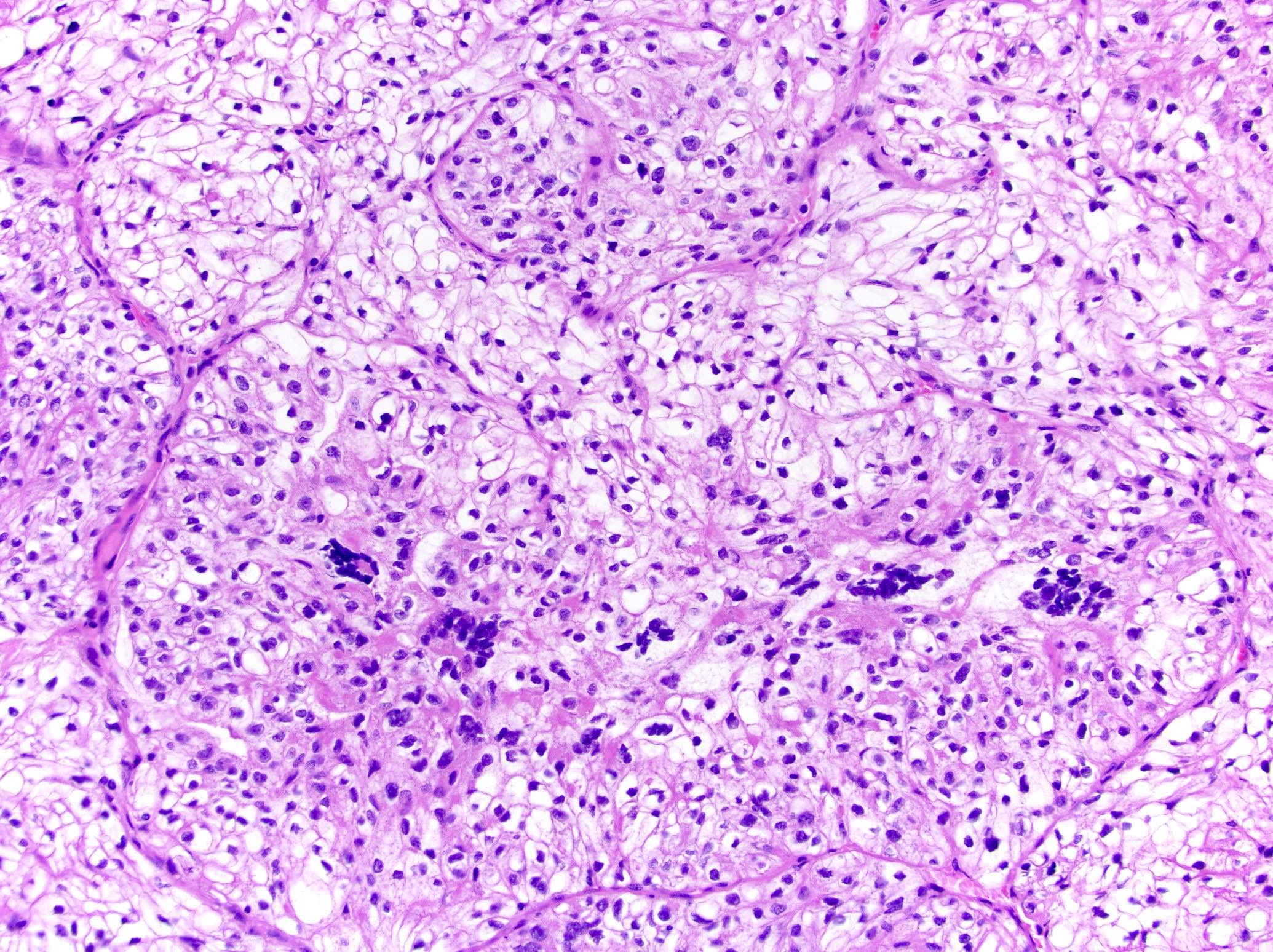
Microscopic (histologic) images
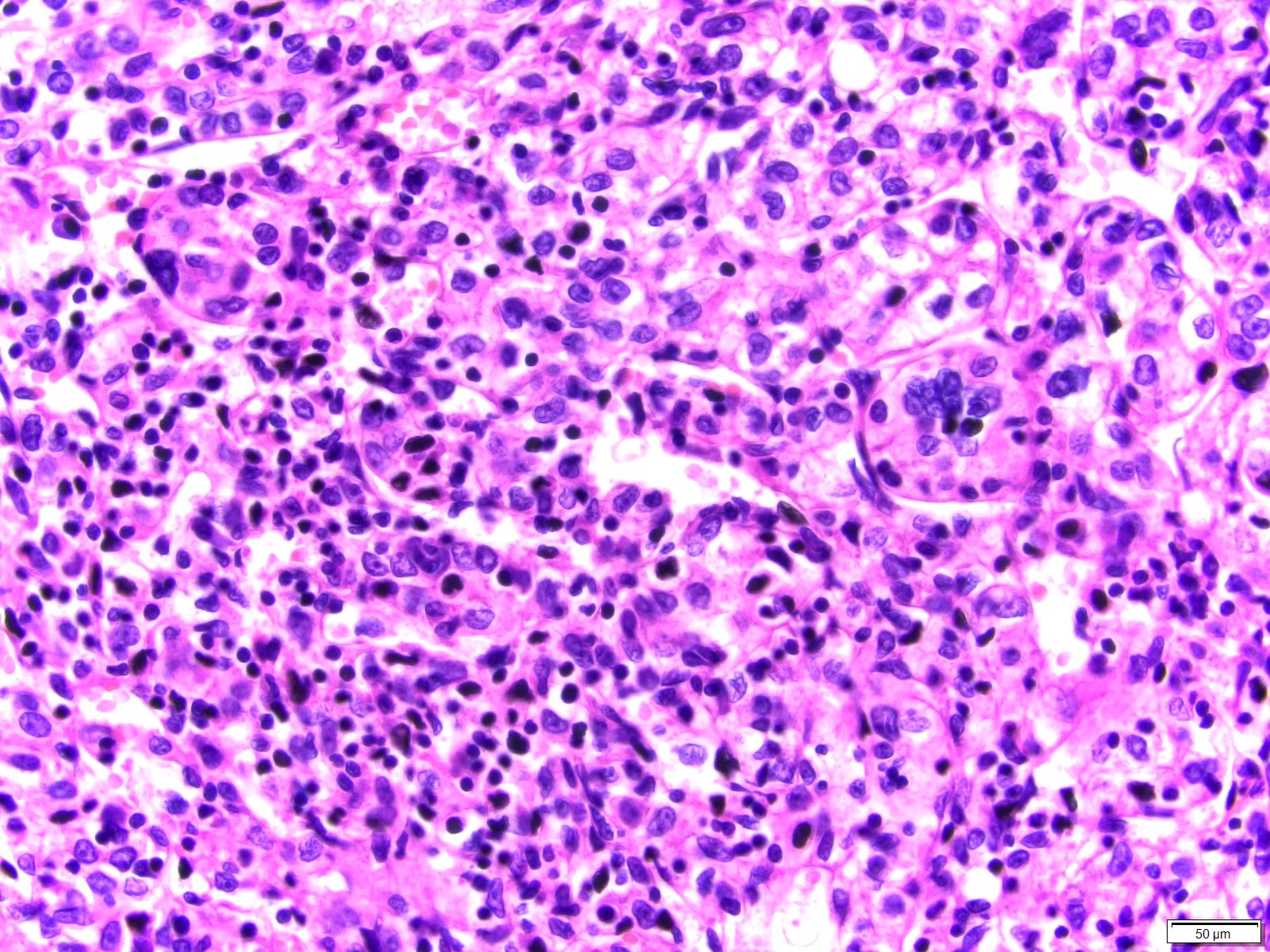
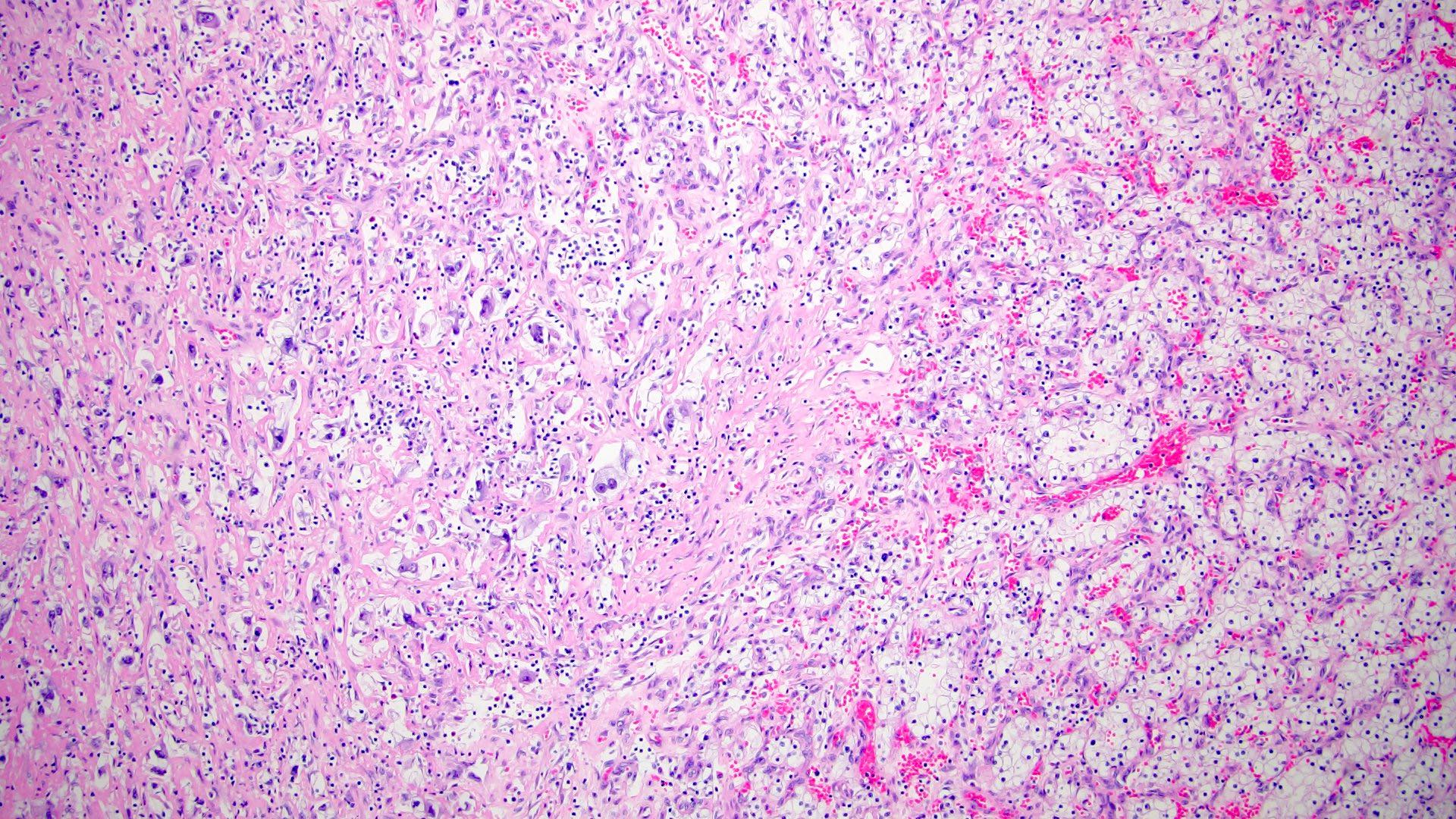
Contributed by Maria Tretiakova, M.D., Ph.D.
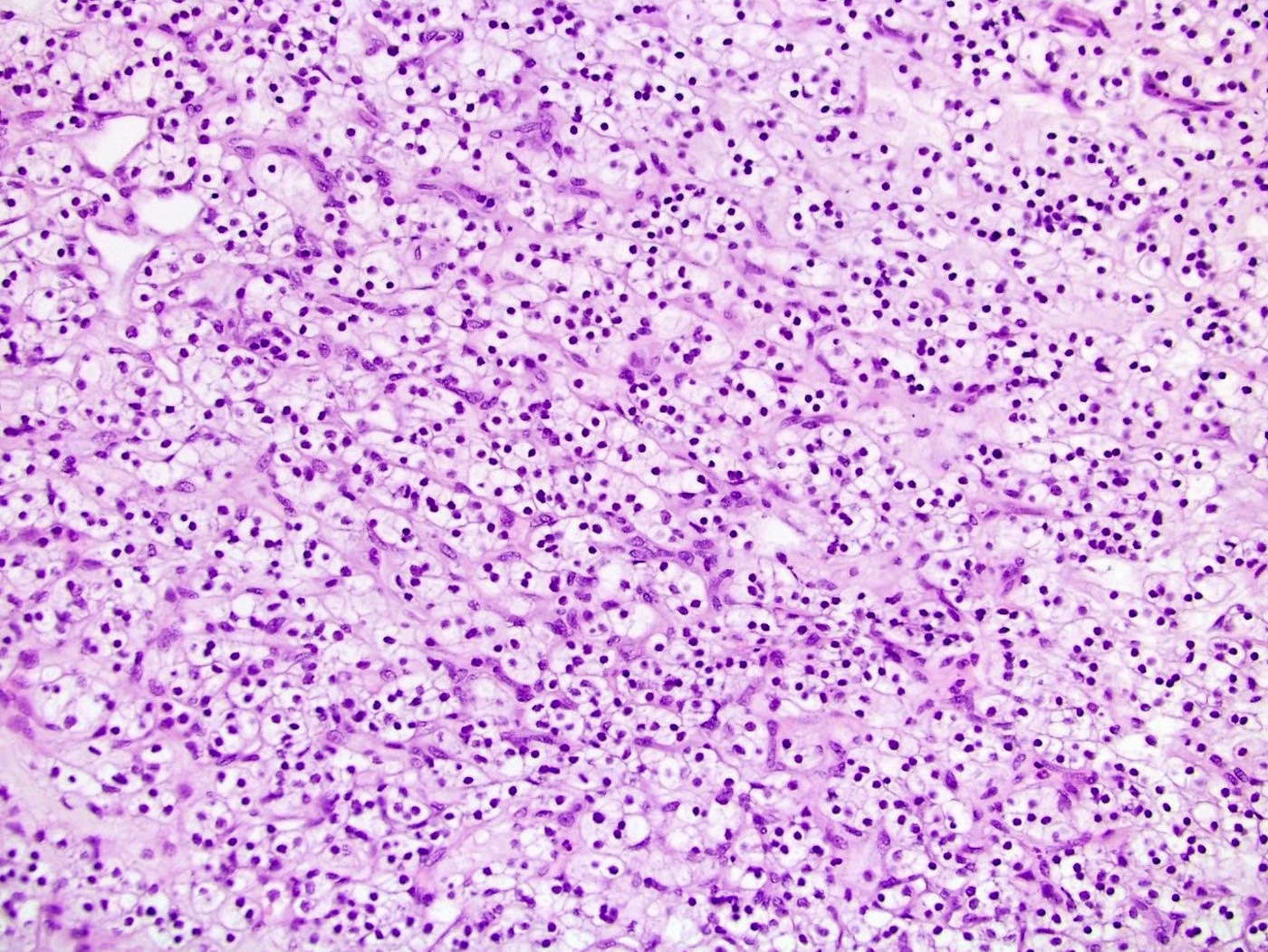
Small, dark nuclei
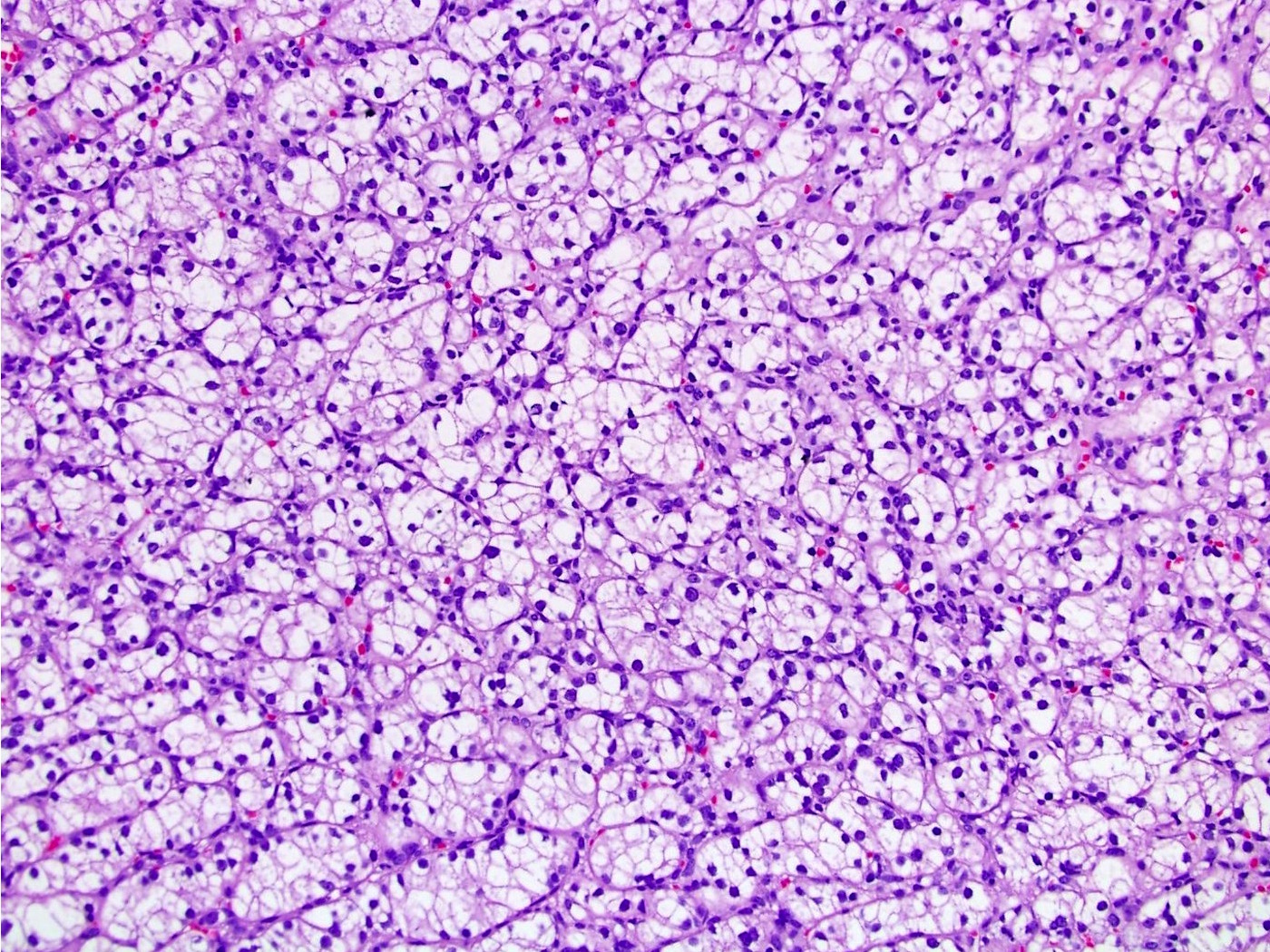
Nucleoli are barely visible
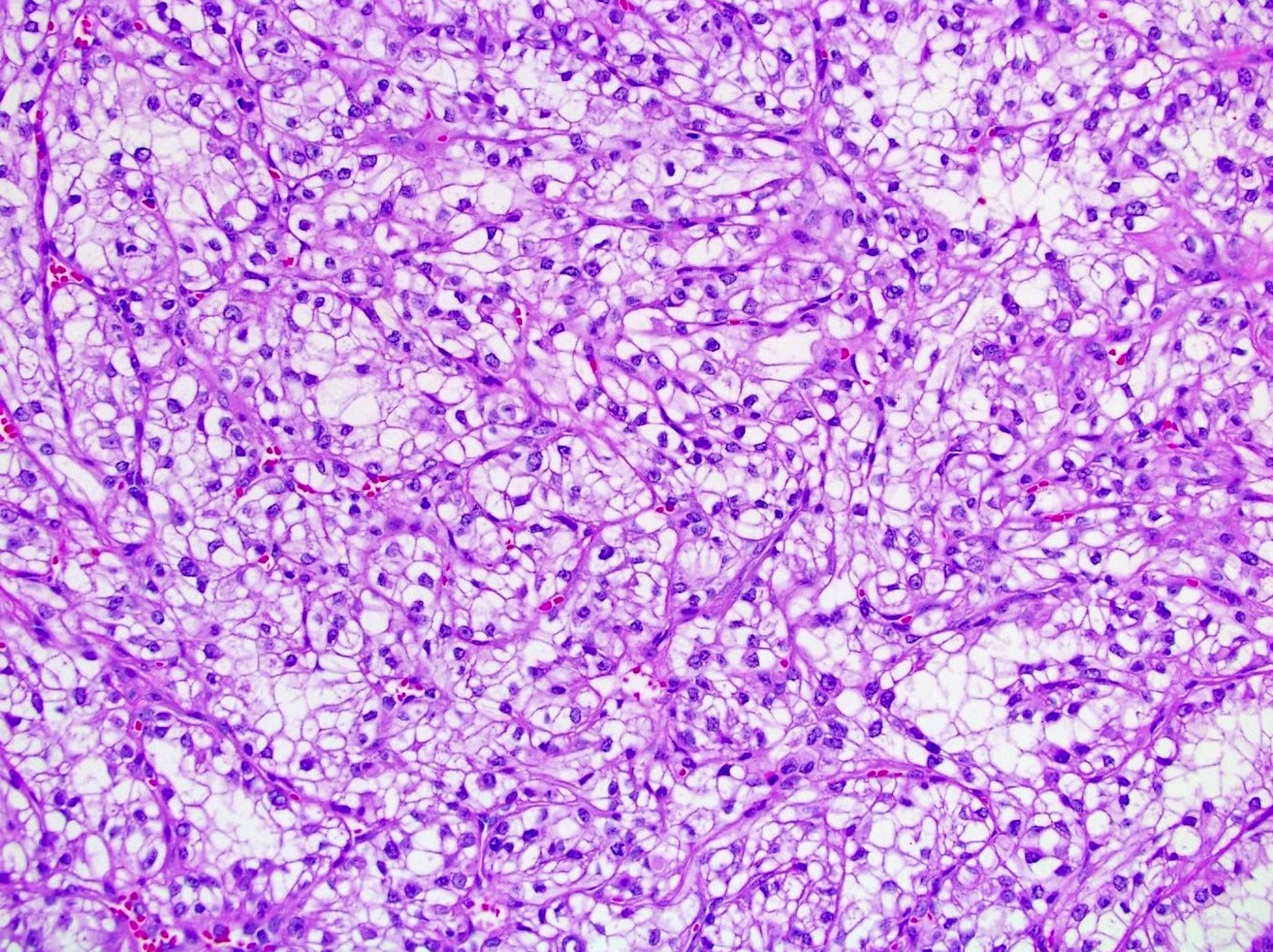
Nucleoli are easily seen
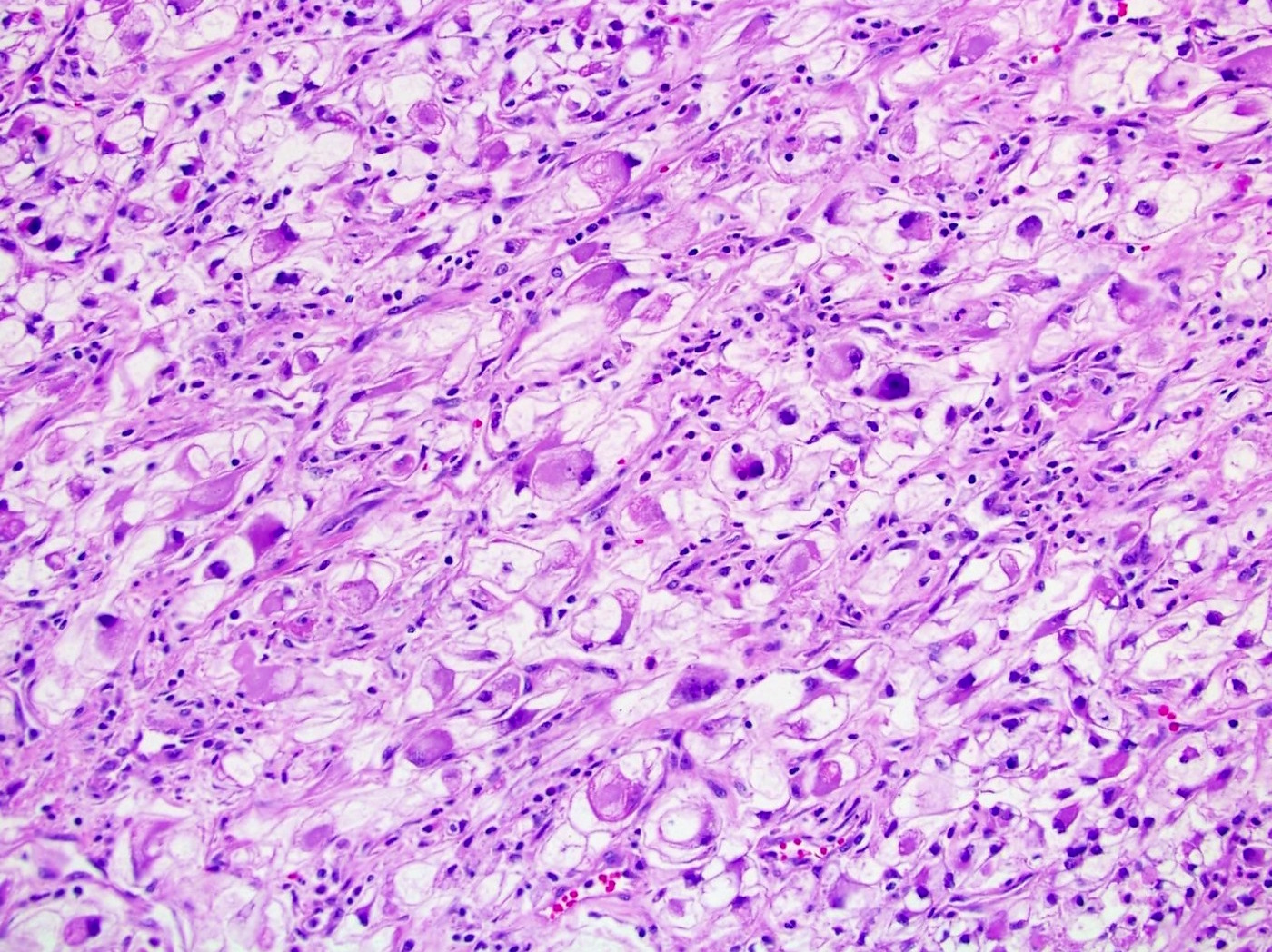
Large pleomorphic nuclei
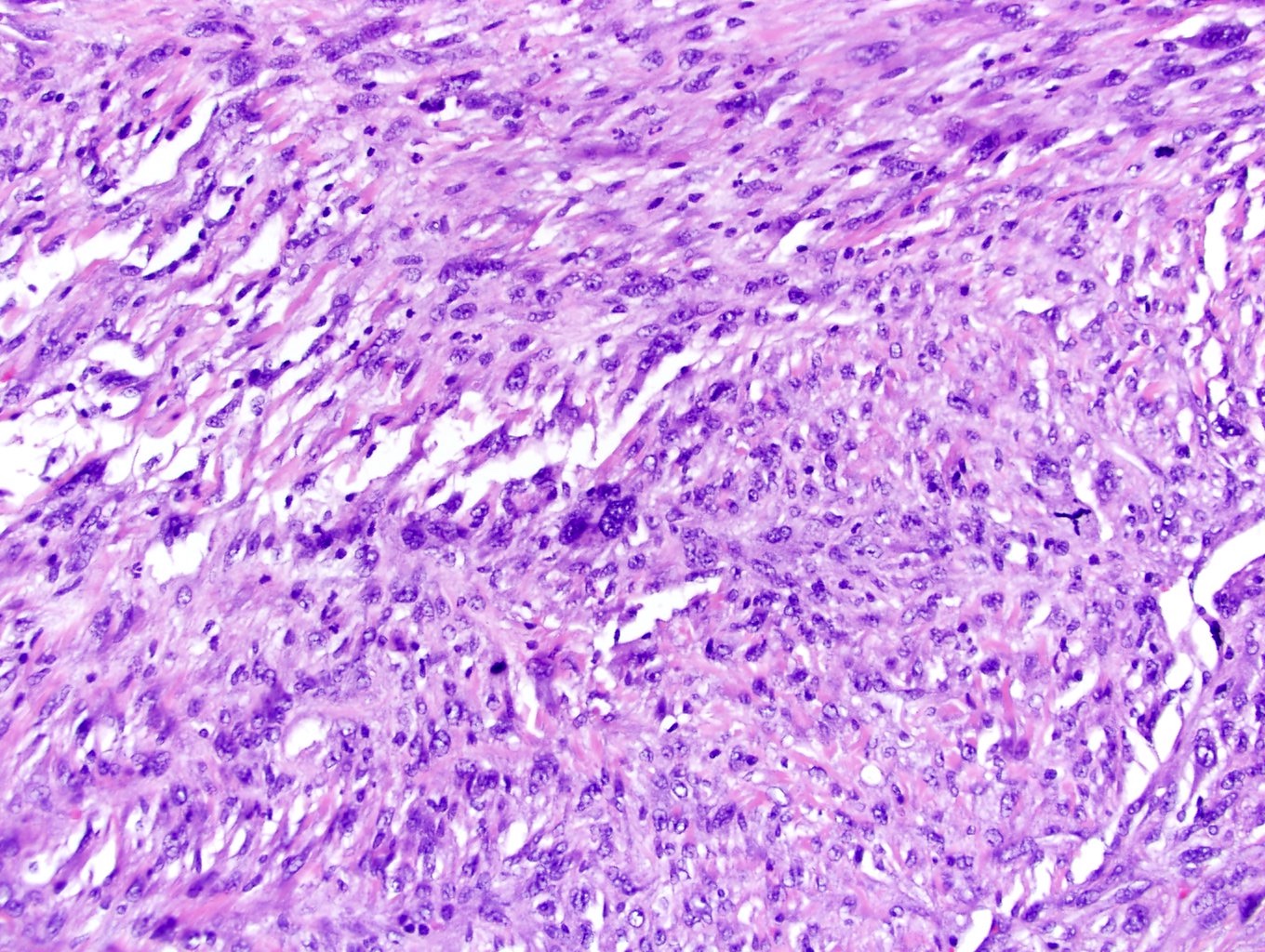
Sarcomatoid differentiation
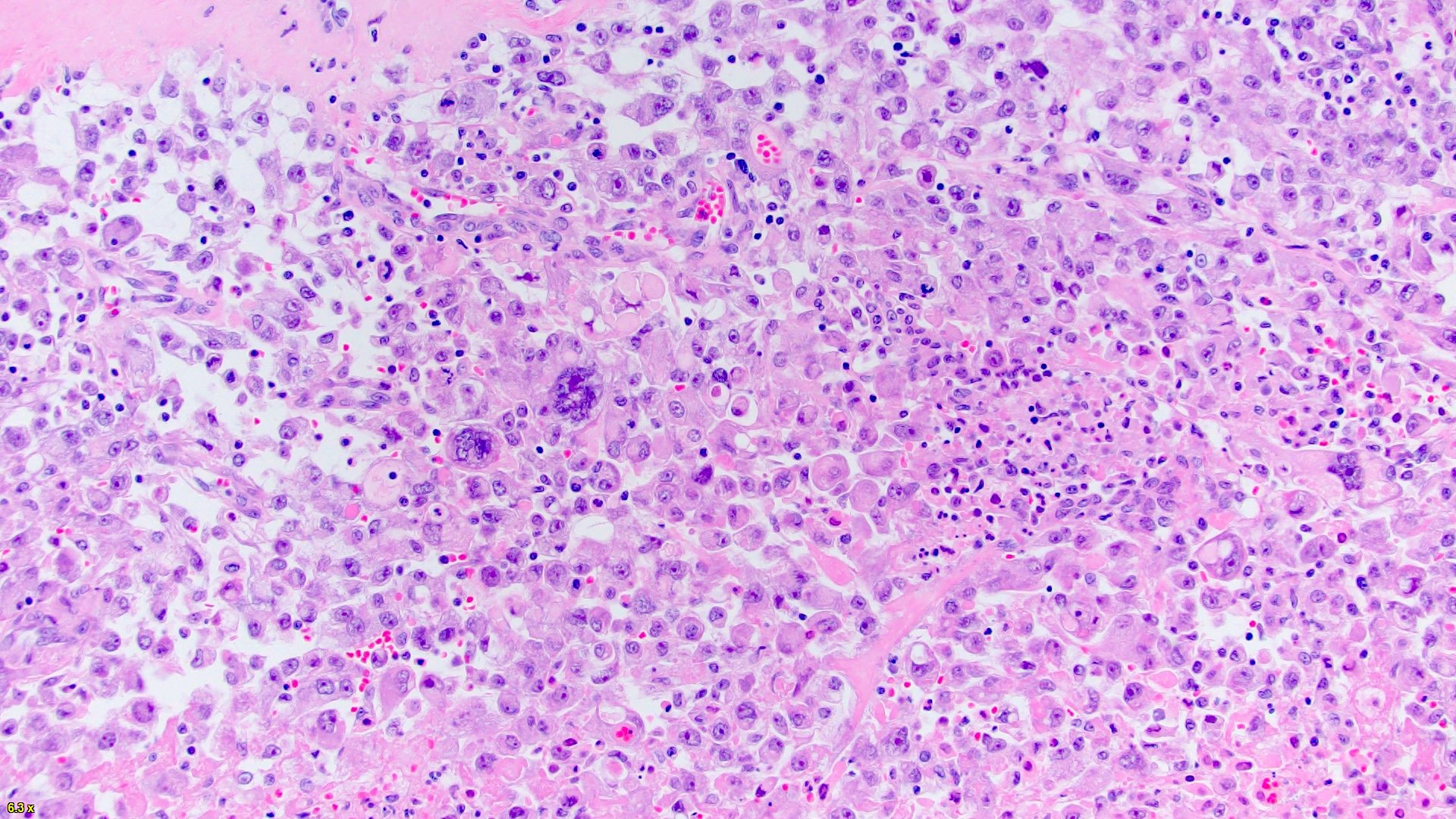
Anaplastic giant and rhabdoid cells
Anaplastic giant cells
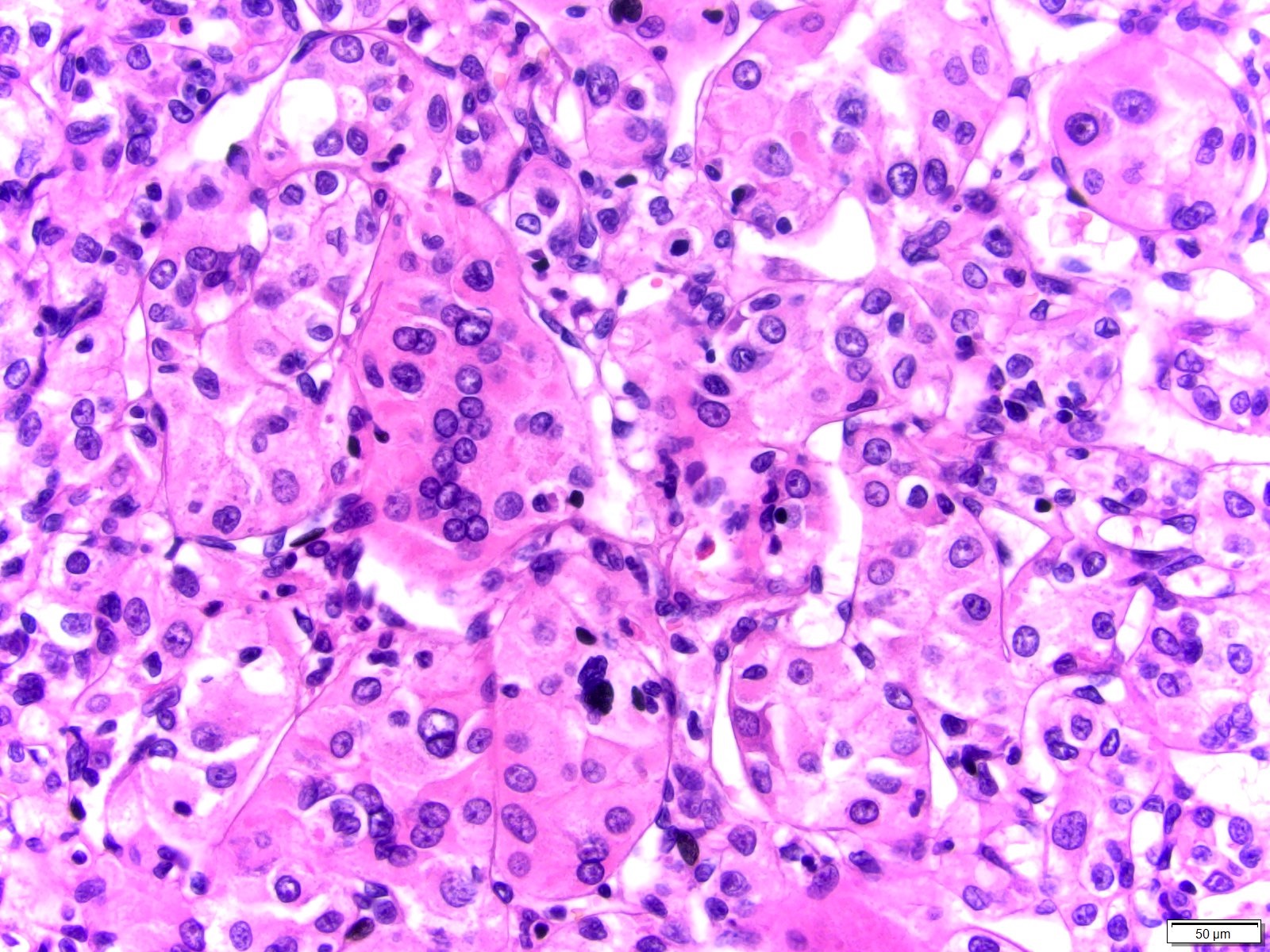
Nonanaplastic giant cells
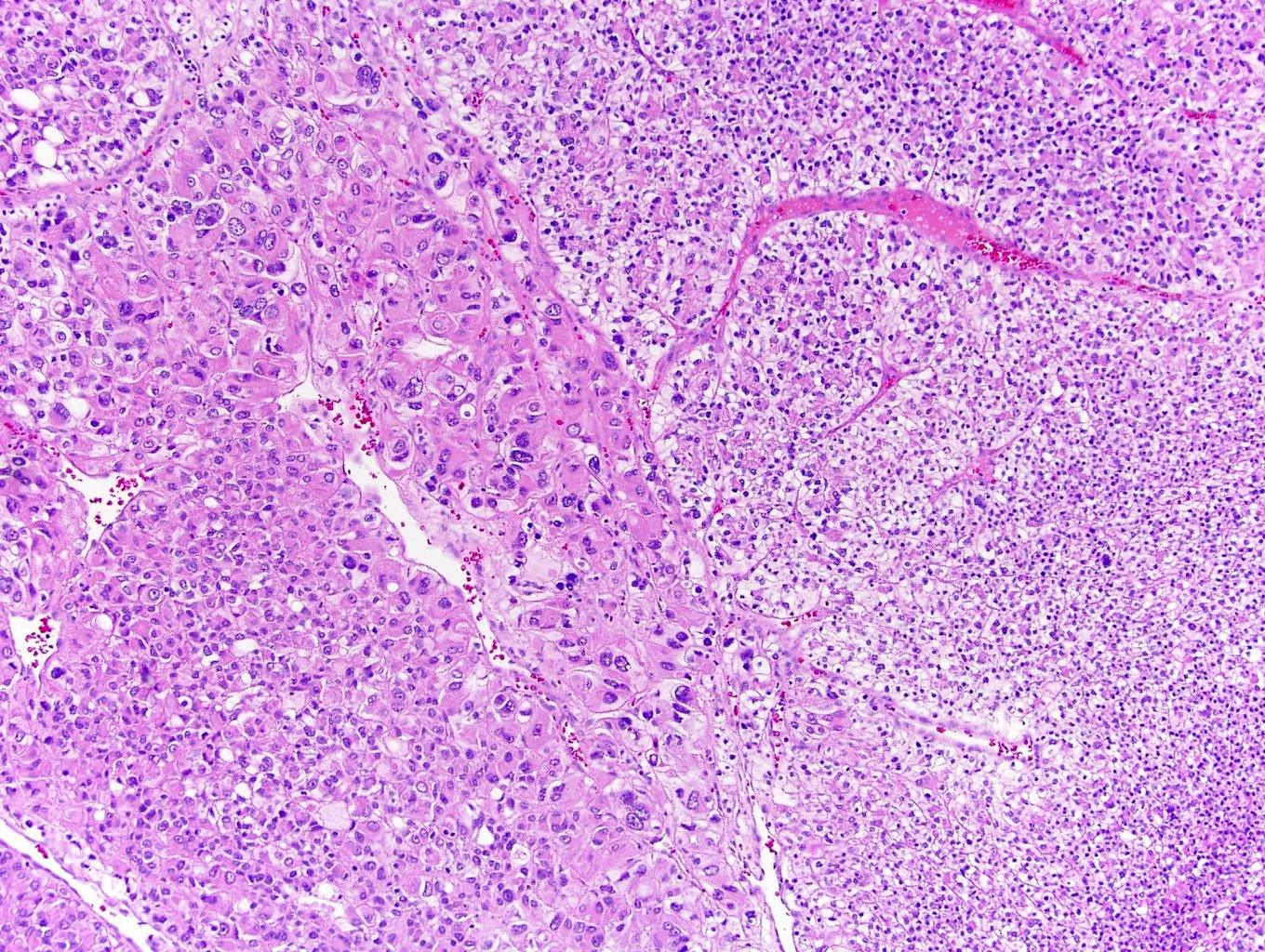
Dual low and high grade RCC
Sample pathology report
- Left kidney, radical nephrectomy:
- Clear cell renal cell carcinoma, grade 2 (see synoptic report)
Additional references
Board review style question #1
What is the grade of the renal cell carcinoma shown in the image above?
- Grade 1
- Grade 1 and 4
- Grade 3
- Grade 4
Board review style answer #1
D. Grade 4. Grading of renal cell carcinomas is based on the focus with the greatest degree of pleomorphism. Note: even if the pleomorphic component is relatively small compared to the remainder of the tumor, the highest grade overall is still used. On the right of this picture is the low grade component and on the left is the grade 4 component. To be able to decipher whether the low grade component is 1 or 2, we would need to assess the histology on 400x.
Comment Here
Reference: Kidney tumor - Grading
Comment Here
Reference: Kidney tumor - Grading
Board review style question #2
Which of the following is true regarding WHO / ISUP grading system for renal cell carcinoma?
- Grade 2: nucleoli absent or inconspicuous at 400x magnification
- Grade 2: nucleoli conspicuous at 400x magnification, visible but not prominent at 100x magnification
- Grade 3: displays sarcomatoid differentiation or rhabdoid morphology
- Grade 4: nucleoli conspicuous at 100x magnification
Board review style answer #2
B. Grade 2: nucleoli conspicuous at 400x magnification, visible but not prominent at 100x magnification. WHO / ISUP grading of renal cell carcinoma is as follows:
Comment Here
Reference: Kidney tumor - Grading
- Grade 1: nucleoli absent or inconspicuous at 400x magnification
- Grade 2: nucleoli conspicuous at 400x magnification, visible but not prominent at 100x magnification
- Grade 3: nucleoli conspicuous at 100x magnification
- Grade 4: extreme nuclear pleomorphism, anaplastic giant cells, rhabdoid morphology and sarcomatoid differentiation
Comment Here
Reference: Kidney tumor - Grading
