

Kidney tumor
Renal cell carcinoma - rare
Rhabdoid
Last author update: 1 April 2015
Last staff update: 15 November 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Renal cell carcinoma [title] rhabdoid



Table of Contents
Definition / general | Terminology | Epidemiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains (rhabdoid component) | Negative stains (rhabdoid component) | Molecular / cytogenetics description | Differential diagnosisCite this page: Andeen NK. Rhabdoid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumormalignantclearcellrhabdoid.html. Accessed December 26th, 2024.
Definition / general
- An adult renal cell carcinoma (RCC), usually clear cell type, with a population of neoplastic cells (5% - 90%) which morphologically resemble rhabdomyoblasts but do not have true muscle differentiation by ultrastructure or immunohistochemistry
- Independent poor prognostic indicator (Am J Surg Pathol 2014;38:1260)
Terminology
- Rhabdoid morphology is classically defined as "sheets and clusters of variably cohesive, large epithelioid cells with vesicular nuclei, prominent nucleoli and large paranuclear intracytoplasmic inclusions" (Am J Surg Pathol 2000;24:1329)
- Rhabdoid tumor of the kidney is a distinct mesenchymal neoplasm in children (see separate topic) but not in adults
Epidemiology
- Incidence is 4% - 7% of RCCs, most frequently clear cell RCC type but also other subtypes (Am J Surg Pathol 2000;24:1329)
- Mean age 53 - 62 years; M:F = 2:1 (Am J Surg Pathol 2013;37:1490)
Etiology
- Likely represents morphologic and genetic clonal evolution of neoplastic epithelial cells (Hum Pathol 2015;46:9)
Clinical features
- Kidney mass; rarely hematuria or flank pain
- Aggressive behavior with metastases in up to 70% of cases (Am J Surg Pathol 2013;37:1490); often into regional lymph nodes or lung (J Urol 2011;186:675)
- Rhabdoid phenotype in maintained in 65% of metastases; RCC should be strongly considered in evaluating an unknown primary with rhabdoid differentiation (Am J Surg Pathol 2014;38:1260)
- Median survival 8 to 31 months (Am J Surg Pathol 2013;37:1490)
Diagnosis
- International Society of Urologic Pathologists (ISUP) Consensus recommends:
- Report as underlying histologic subtype (i.e. clear cell RCC) with rhabdoid differentiation
- No need to specify % of rhabdoid area; and
- Tumors are ISUP grade 4 (Am J Surg Pathol 2013;37:1490)
Prognostic factors
- RCC with rhabdoid differentiation has increased risk of death (hazard ratio 5.25) when compared with RCC without rhabdoid differentiation, independent of nonrhabdoid component grade, tumor stage and presence of necrosis (Am J Surg Pathol 2014;38:1260)
- Usually high stage and high grade nuclei (Fuhrman 3 or 4) in nonrhabdoid component and aggressive behavior similar to sarcomatoid carcinoma (Arch Pathol Lab Med 2007;131:102)
Case reports
- 53 year old man with extensive peritoneal carcinomatosis secondary to renal cell carcinoma with sarcomatoid and rhabdoid differentiation (BMJ Case Rep 2013 Apr 22;2013)
- 56 year old man with acquired cystic disease associated renal cell carcinoma with sarcomatoid change and rhabdoid features (Ann Diagn Pathol 2011;15:462)
- 84 year old woman with malignant mixed epithelial and stromal tumor of the kidney with rhabdoid features (Hum Pathol 2007;38:1432)
Treatment
- Resection
- Targeted therapy (tyrosine kinase inhibitors, VEGF inhibitors, mTOR inhibitors), cytokine therapy
Gross description
- Rhabdoid component is white, firm, homogeneous
Gross images
Images hosted on other servers:
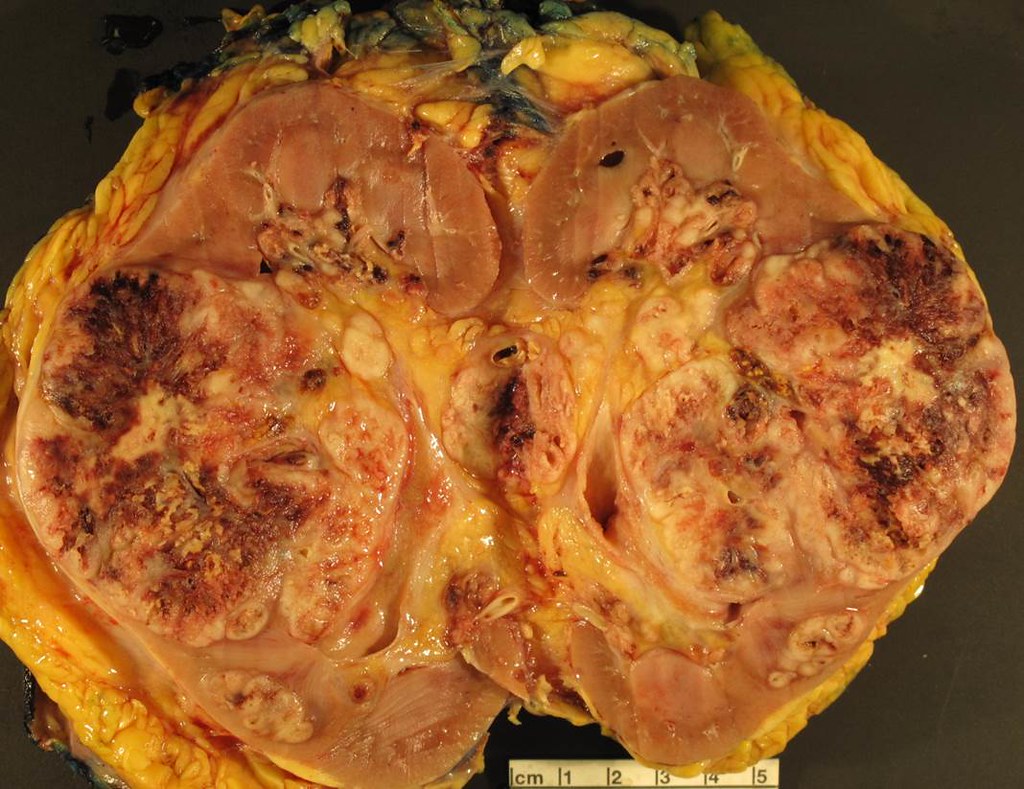
Rhabdoid component is solid, white
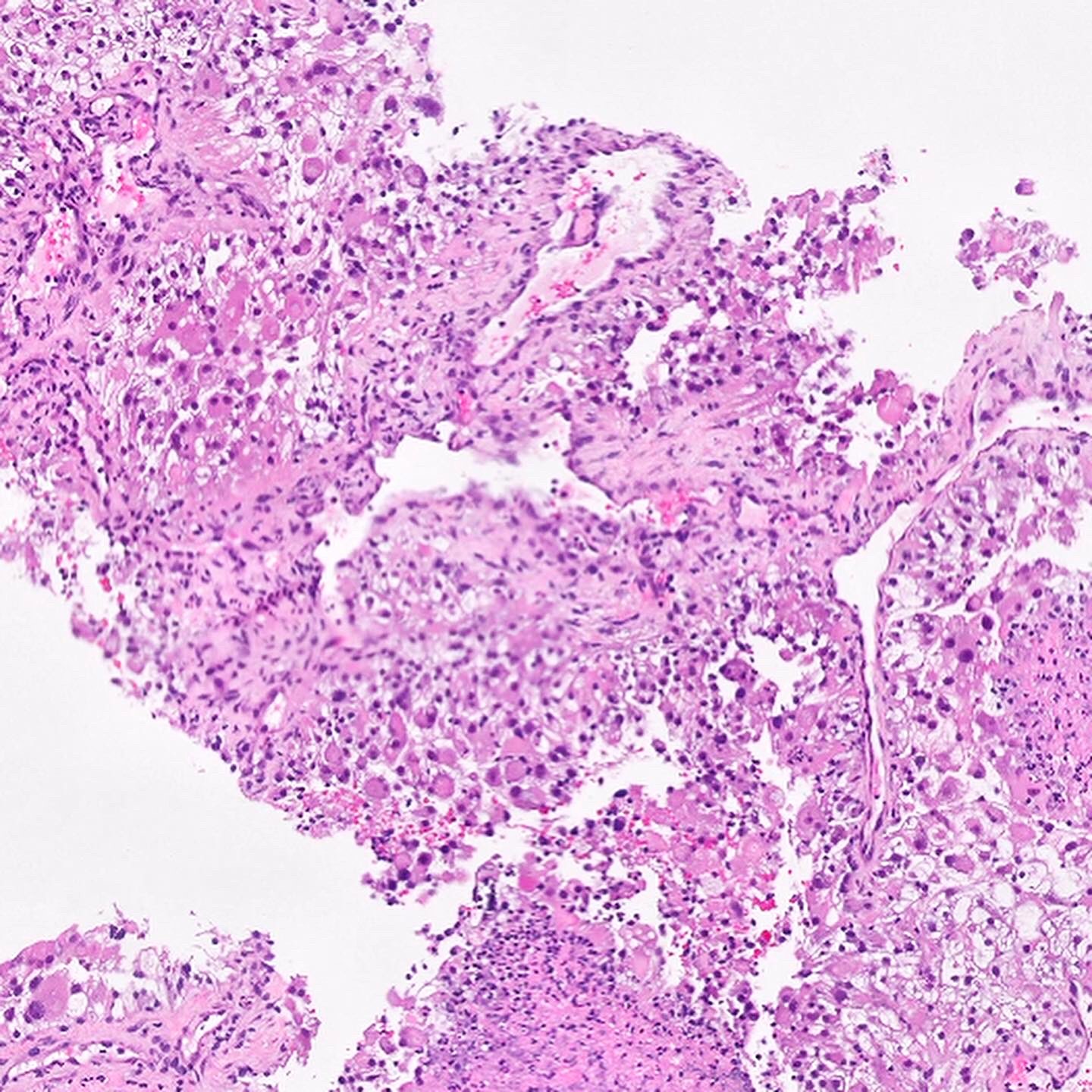
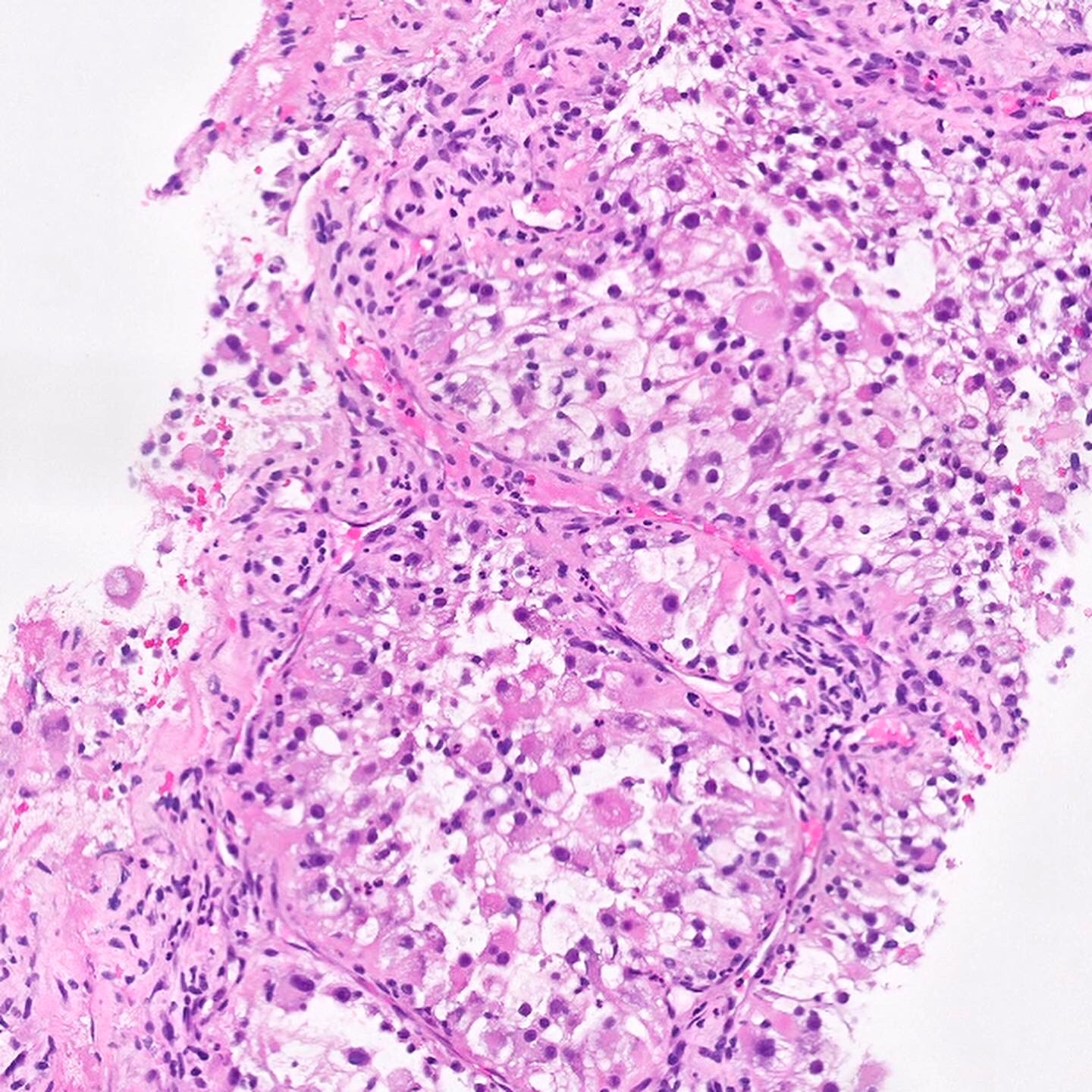
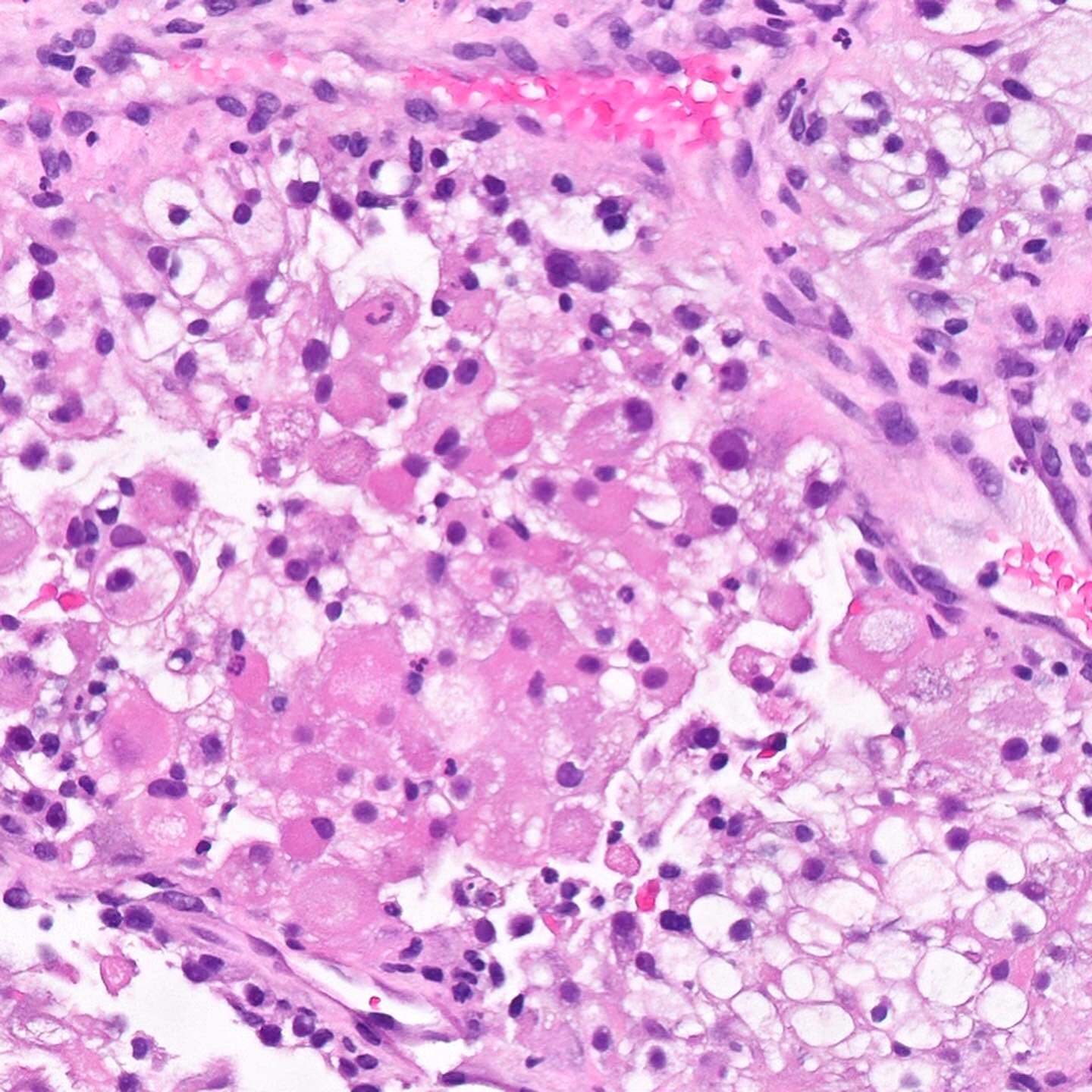
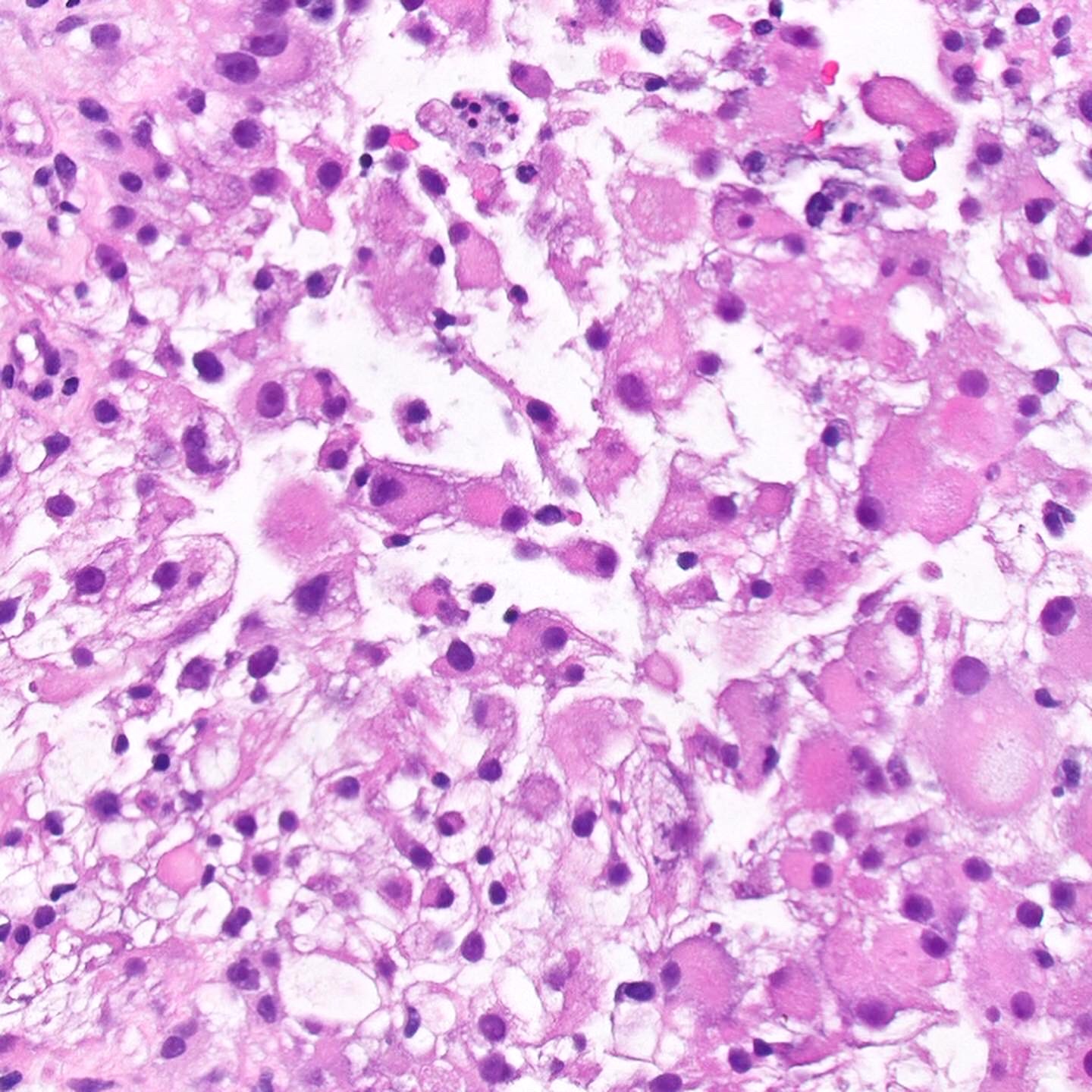
Microscopic (histologic) description
- Solid clusters and sheets of variably cohesive large epithelioid cells with central eosinophilic intracytoplasmic inclusions
- Large, eccentric and irregular nuclei and prominent nucleoli
- Tumor necrosis common and sometimes extensive
- Transition areas between RCC and rhabdoid morphology
Microscopic (histologic) images
Contributed by Nicole K. Andeen, M.D.
Discohesive rhabdoid cells with eccentrically placed nuclei, prominent nucleoli and densely eosinophilic cytoplasm
Abrupt transition between conventional clear cell carcinoma and rhabdoid morphology
Rhabdoid cells express CAIX, similar to coexistent conventional clear cell component
Contributed by @SueEPig on Twitter
Adult renal cell carcinoma - rhabdoid variant
Positive stains (rhabdoid component)
- Majority of cases positive for vimentin, EMA, pan CK, p53, CAIX, PAX2, PAX8, CD10, NSE, PAS (Am J Surg Pathol 2000;24:1329, Ann Diagn Pathol 2015;19:57)
- Retained INI1 expression, except in cases with renal medullary carcinoma (Am J Surg Pathol 2013;37:1490, Mod Pathol 2008;21:647)
- Immunophenotype is similar to nonrhabdoid component
Negative stains (rhabdoid component)
Molecular / cytogenetics description
- Mutations in tumor suppressor genes BAP1 or PBRM1 located on chromosome 3p (Nat Genet 2012;44:751)
- Loss of 11p specific to rhabdoid differentiation in one study (n = 20; 11p loss seen in 29% of rhabdoid areas but not in clear cell areas)
- Rhabdoid cells share many chromosomal aberrations with coexisting clear cell RCCs but have greater number of copy variations (Hum Pathol 2015;46:9)
Differential diagnosis
- Eosinophilic change in usual RCC: no resemblance to rhabdomyoblasts
- Renal rhabdoid tumors: pediatric patients, loss of INI1 gene / protein
- Rhabdomyosarcoma: skeletal muscle differentiation and lack of usual RCC

