
Kidney tumor
Non-renal cell tumors
Leiomyoma
Authors: Alcino Pires Gama, M.D., Bonnie Choy, M.D.
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.

Last author update: 12 July 2022
Last staff update: 12 July 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Kidney leiomyoma


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gama AP, Choy B. Leiomyoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorleiomyoma.html. Accessed April 2nd, 2025.
Definition / general
- Rare benign mesenchymal tumor of the kidney arising from smooth muscle fibers of the renal capsule, renal pelvis or vascular smooth muscle of renal vessels
Essential features
- Benign smooth muscle tumor with female predominance
- Arises from smooth muscle fibers of the renal capsule, renal pelvis or vascular smooth muscle of renal vessels
- Bland spindle cells in intersecting fascicles with eosinophilic cytoplasm
- Positive for smooth muscle markers, ER and PR and negative for melanocytic markers, cathepsin K, cytokeratins, CD117, S100 and CD34
ICD coding
Epidemiology
- 0.5% in surgically resected renal tumors (Am J Surg Pathol 2016;40:1557)
- 4 - 5.5% in autopsy studies (J Urol 1971;106:503)
- Higher prevalence in middle aged women (Am J Surg Pathol 2016;40:1557)
Sites
- Kidney: renal cortex or renal capsule, less commonly in muscularis propria of the renal pelvis and smooth muscle of cortical vessels
- Seen equally in the left and right kidney
- More frequently reported in the lower pole of the kidney (Urol Case Rep 2017;13:3)
Pathophysiology
- Arises from smooth muscle fibers of the renal capsule, renal pelvis or vascular smooth muscle of renal vessels (J Urol 1990;143:994)
Etiology
- Unknown
Clinical features
- Most are asymptomatic and found incidentally
- Larger tumors may present as a palpable mass or with flank pain or hematuria, especially if located on the renal pelvis (Pathology 2006;38:454)
Diagnosis
- Histologic examination of tissue
- Imaging modalities are not conclusive
Radiology description
- Ultrasound: most are hypoechoic, some with mixed echogenicity (Radiat Med 1993;11:81)
- CT: well circumscribed margins, minimal parenchymal distortion, no evidence of extrarenal invasion (Urol Int 1992;48:219, J Urol 1987;138:853, J Urol 1990;143:994)
- Angiography: hypovascularity or slight vascularity, absence of features indicative of malignancy (e.g., vessel encasement, renal vein invasion, arteriovenous shunting) (Radiat Med 1993;11:81)
Radiology images
Images hosted on other servers:


Ultrasound and CT

CT

CT

CT
Prognostic factors
- Benign
- Excellent prognosis
Case reports
- 20 year old woman presenting with large symptomatic renal leiomyoma (Radiol Case Rep 2020;15:515)
- 39 year old man presenting with right flank mass (Urol Case Rep 2017;13:3)
- 79 year old woman with small subcortical renal leiomyoma (Urol Case Rep 2021;39:101792)
Treatment
- Surveillance or surgical resection depending on the tumor size, location and symptoms
Gross description
- Solid, well circumscribed, tan to white with whorled and bulging cut surface
- Focal cystic degeneration, hemorrhage or irregular calcifications may be present
- Often solitary but occasionally multiple (Scand J Urol Nephrol 1999;33:138)
- Most are small but the largest reported tumor measured 57.5 cm (Br J Surg 1956;43:497)
Gross images
Images hosted on other servers:

Solid, tan-white mass

Whorled, bulging cut surface
Microscopic (histologic) description
- Arranged in intersecting fascicles
- Spindle cells with blunt ended, cigar shaped nuclei and eosinophilic cytoplasm
- Minimal to no nuclear pleomorphism / atypia
- Low mitotic activity
- No necrosis
- Reference: Am J Surg Pathol 2016;40:1557
Microscopic (histologic) images
Contributed by Alcino Pires Gama, M.D. and Bonnie Choy, M.D.
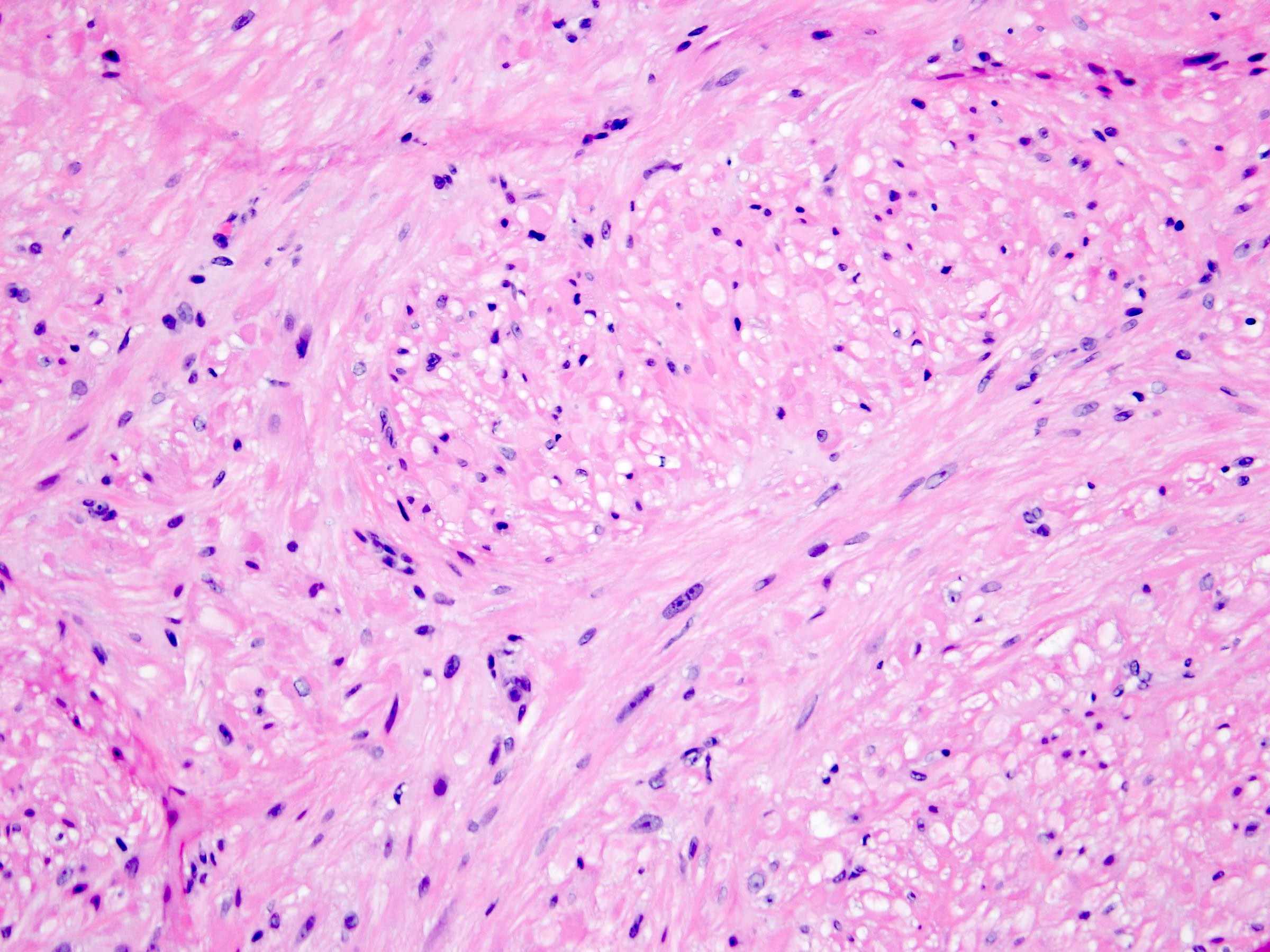
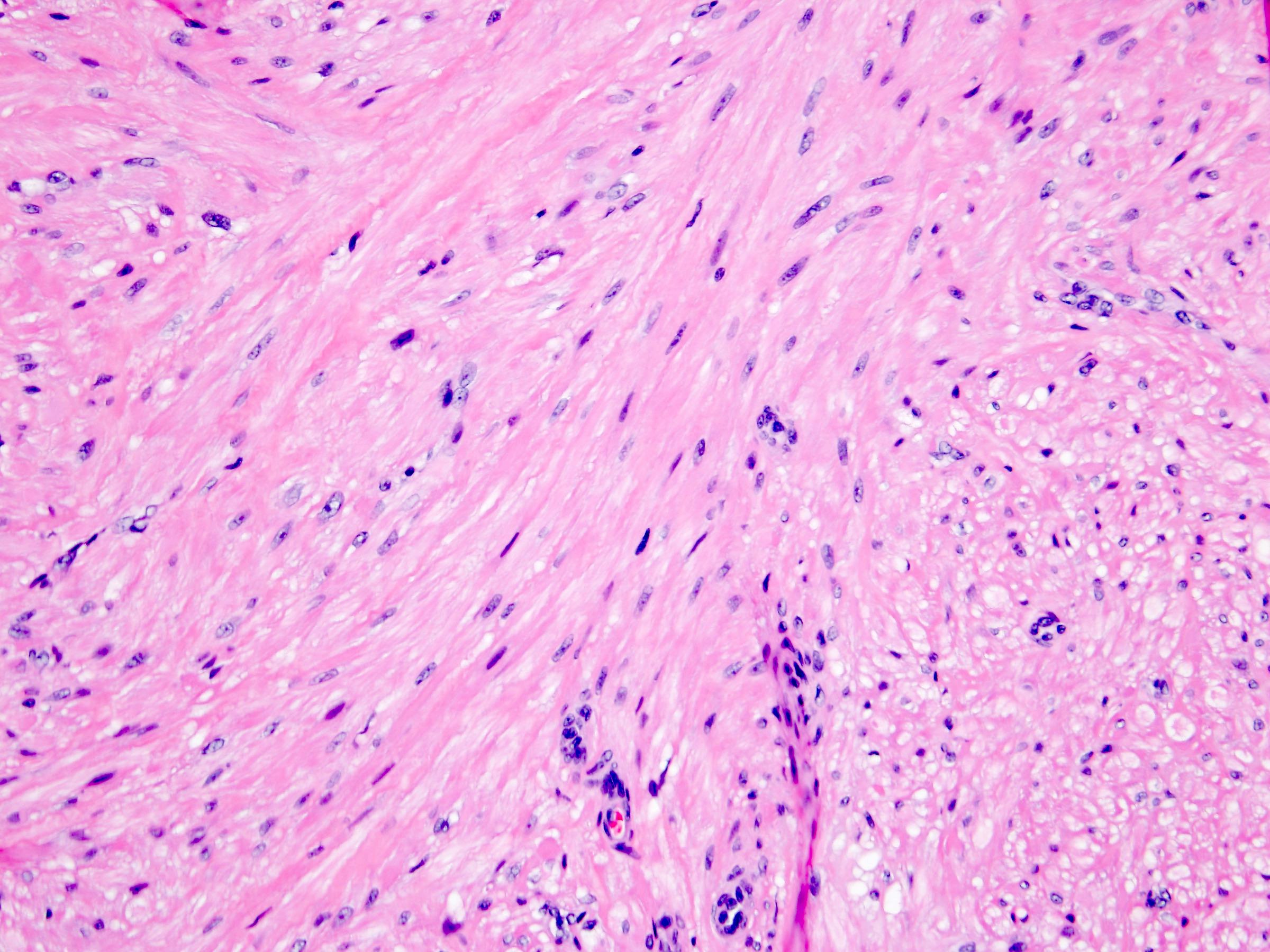
Intersecting fascicles
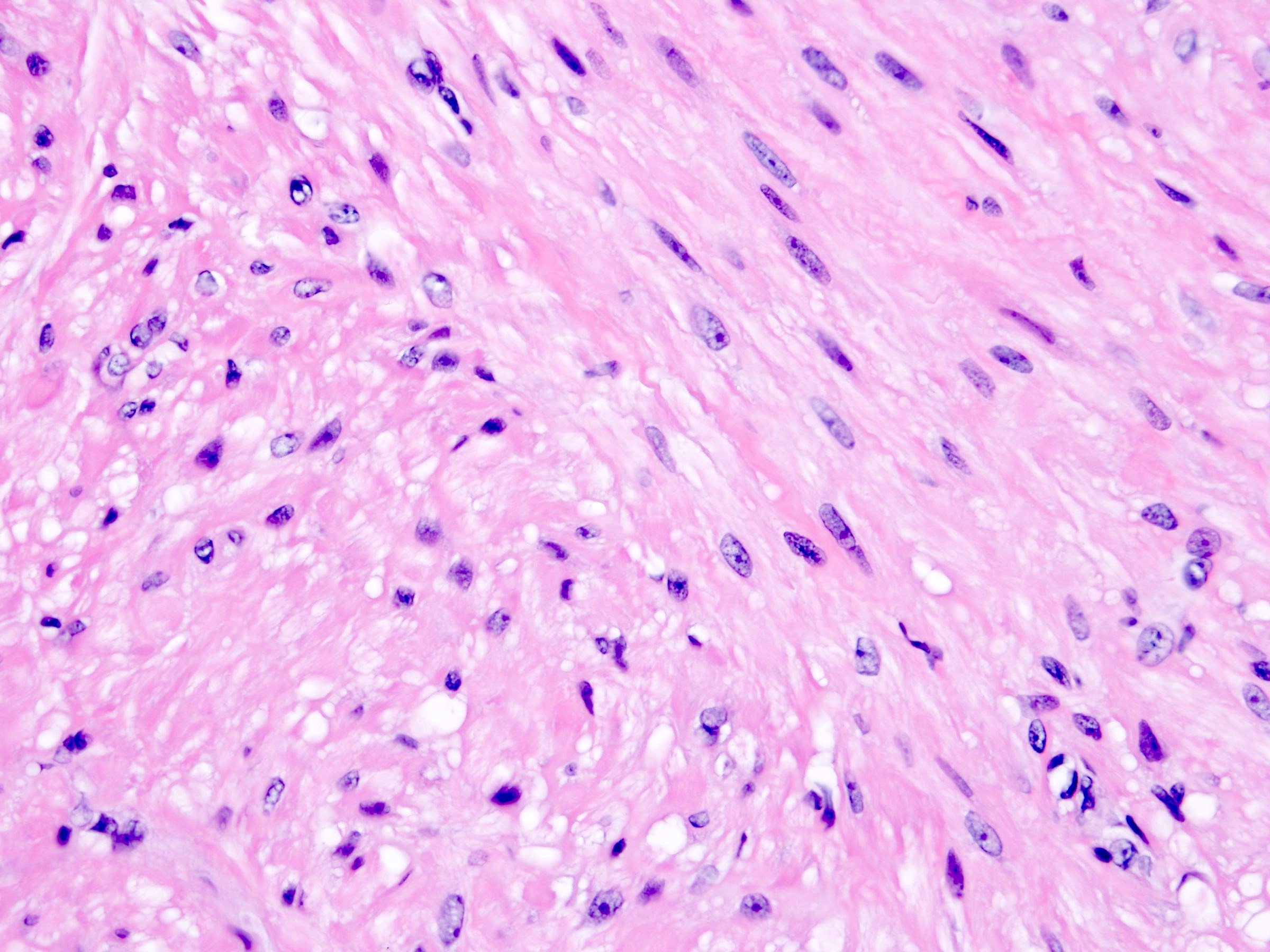
Bland spindle cells
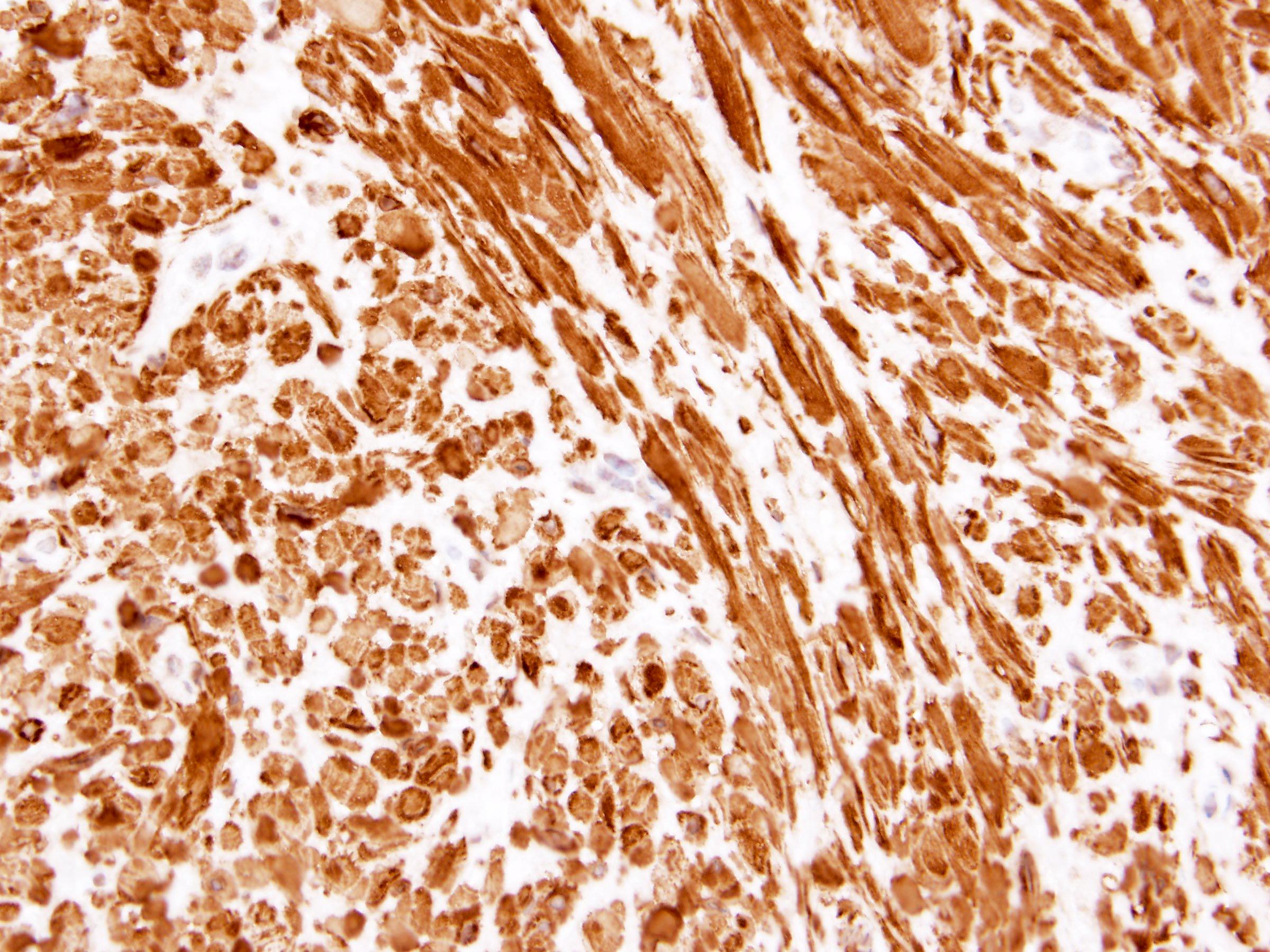
h-caldesmon
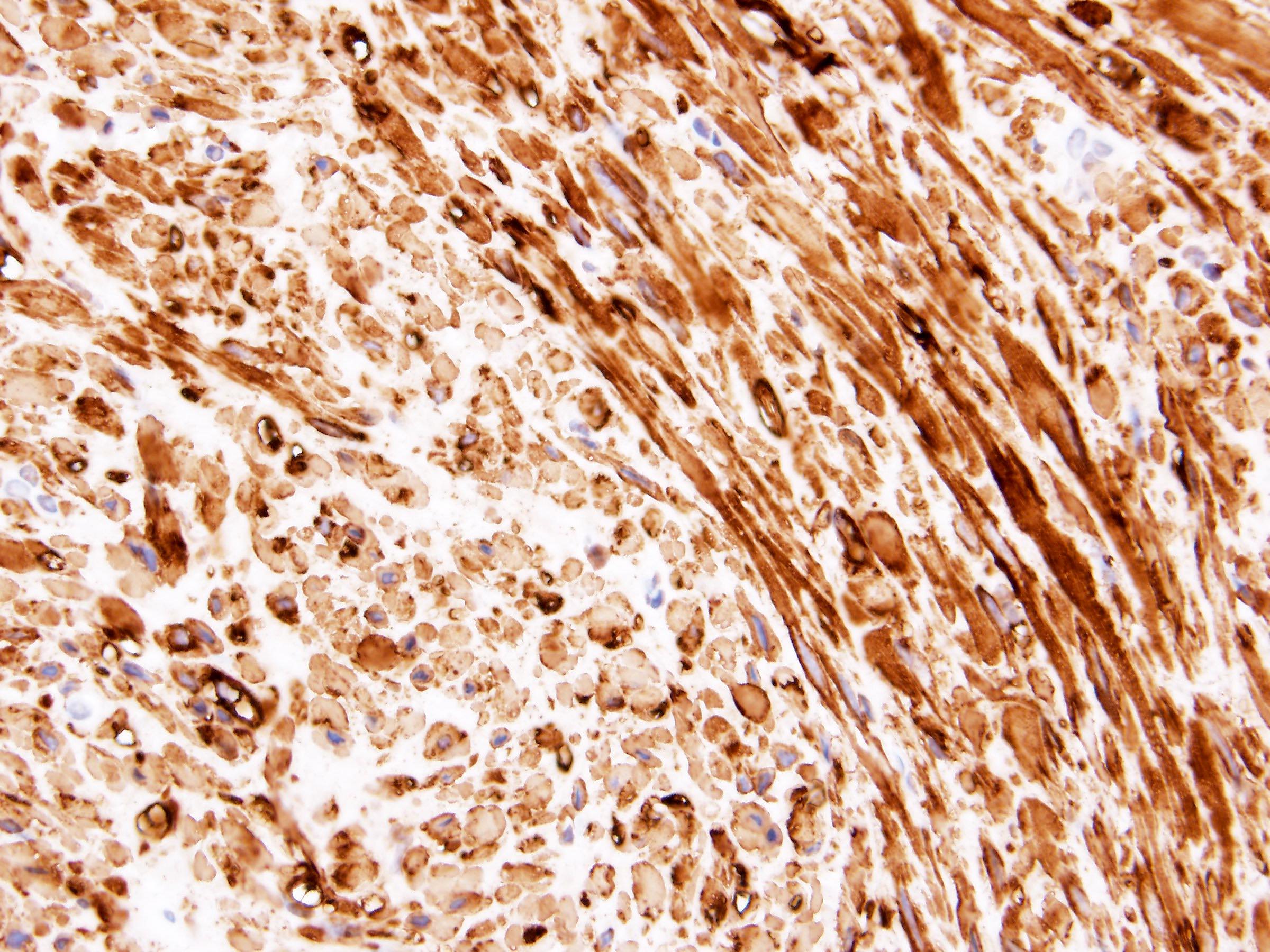
SMA
Positive stains
- Smooth muscle markers: SMA, desmin, h-caldesmon, calponin (Am J Surg Pathol 2016;40:1557)
- ER (87%) and PR (87%) (Am J Surg Pathol 2015;39:349, Am J Surg Pathol 2016;40:1557)
- WT1 (73%) (Am J Surg Pathol 2016;40:1557)
Negative stains
- Cytokeratins (Am J Surg Pathol 2016;40:1557)
- RCC, PAX8, PAX2 (Urol Case Rep 2017;13:3)
- Myogenin, MyoD1 (Am J Surg Pathol 2016;40:1557, Urol Case Rep 2017;13:3)
- CD117 (Am J Surg Pathol 2016;40:1557, Urol Case Rep 2017;13:3)
- S100 (Urol Case Rep 2017;13:3, J Int Med Res 2021;49:3000605211032802, Korean J Urol Oncol 2011;9:130)
- CD34 (Urol Case Rep 2017;13:3, Korean J Urol Oncol 2011;9:130)
- BCL2 (Urol Case Rep 2017;13:3)
- HMB45, although positivity in renal capsular leiomyomas has been reported (Am J Surg Pathol 2015;39:349, Mod Pathol 1996;9:664)
- Cathepsin K (Am J Surg Pathol 2015;39:349)
- Ki67 proliferation rate: low (Am J Surg Pathol 2016;40:1557)
Molecular / cytogenetics description
- Breakpoints in the q13-15 region of chromosome 12 (Pediatr Pathol 1993;13:435)
- Single study showed combined losses of chromosomes 4, 6, 12 and 14 (Histol Histopathol 2007;22:883)
Sample pathology report
- Right kidney, mass, partial nephrectomy:
- Renal leiomyoma, measuring 1.5 cm in greatest dimension (see comment)
- Surgical margins, negative for tumor
- Comment: The sections show a well circumscribed tumor composed of bland spindle cells in intersecting fascicles. Immunohistochemistry was performed to show positivity for SMA, desmin, h-caldesmon, ER and PR. Cytokeratin AE1 / AE3, PAX8, S100, CD117 and CD34 are negative. The overall findings support the above diagnosis of a renal leiomyoma.
Differential diagnosis
- Angiomyolipoma:
- Smooth muscle component with mature adipose tissue and thick walled vessels but could be difficult to distinguish from fat poor (leiomyomatous) variant
- Melanocytic markers (MelanA, HMB45) and cathepsin K positive
- Both smooth muscle markers (SMA) positive
- Leiomyosarcoma:
- Spindle cells with moderate to severe nuclear pleomorphism
- Tumor necrosis and high mitotic activity (with atypical mitoses)
- Infiltrative border
- Sarcomatoid renal cell carcinoma:
- Atypical spindle and giant cells with marked nuclear pleomorphism
- Atypical mitotic figures
- PAX8, cytokeratin positive
- Renomedullary interstitial cell tumor:
- Small, well circumscribed nodules in the renal medulla
- Spindle to stellate cells in basophilic stroma
- Entrapped tubules at the periphery
- Desmin negative
- Mixed epithelial and stromal tumor (MEST):
- Schwannoma:
- Solitary fibrous tumor:
- Synovial sarcoma:
- Monophasic subtype: monotonous spindle cell proliferation with staghorn vessels
- Mast cells commonly seen
- TLE1 positive; desmin, h-caldesmon negative
- Inflammatory myofibroblastic tumor:
- Myofibroblastic proliferation: spindle cells admixed with inflammatory cells, including lymphocytes, plasma cells and eosinophils
- ALK1 (60%) positive
- Gastrointestinal stromal tumor:
Board review style question #1
A 26 year old woman presents with back pain. CT scan located a 2.8 cm, well circumscribed, subcapsular mass in the right kidney. She underwent partial nephrectomy. Grossly, the mass was tan-white with a whorled and bulging cut surface. Microscopically, it consisted of a low grade, monotonous, spindle cell proliferation with blunt ended, cigar shaped nuclei and eosinophilic cytoplasm. No coagulative necrosis, abnormal vessels or fatty infiltration were noted. What is the most likely diagnosis?
- Angiomyolipoma
- Leiomyoma
- Leiomyosarcoma
- Sarcomatoid renal cell carcinoma
Board review style answer #1
B. Leiomyoma. Renal leiomyomas are benign tumors that arise from smooth muscle fibers of the renal capsule, renal pelvis or vascular smooth muscle of renal vessels. It is characterized by a monotonous, spindle cell proliferation with blunt ended, cigar shaped nuclei and eosinophilic cytoplasm. The low grade features are distinct from its malignant counterpart (leiomyosarcoma), as well as sarcomatoid renal cell carcinoma. The lack of mature adipose tissue and thick walled vessels makes angiomyolipoma less likely.
Comment Here
Reference: Leiomyoma
Comment Here
Reference: Leiomyoma
Board review style question #2
A 45 year old woman with a 2.2 cm mass in the right renal pelvis and ipsilateral hydronephrosis, underwent a radical nephrectomy. On H&E, the tumor was composed of bland spindle cells with cigar shaped nuclei. No coagulative necrosis or abnormal vessels were noted. Which of the following immunostaining profiles supports the diagnosis of leiomyoma?
- HMB45+, MelanA+, cathepsin K+, desmin+, caldesmon+
- PAX8+, CK7-, CD117+, CAIX-, vimentin-, AMACR-
- PAX8+, cytokeratins+, vimentin+, CD10+, CK7-, CAIX+ (box-like pattern), S100-
- SMA+, desmin+, ER+, PAX8-, CD34-, cathepsin K-
Board review style answer #2
D. SMA+, desmin+, ER+, PAX8-, CD34-, cathepsin K-. Renal leiomyomas are positive for smooth muscle markers (SMA, desmin, h-caldesmon, calponin), ER and PR. They are negative for cytokeratins, PAX8, CD117, CD34, melanocytic markers and cathepsin K.
Comment Here
Reference: Leiomyoma
Comment Here
Reference: Leiomyoma
