

Kidney tumor
Renal cell carcinoma - molecularly defined
FH deficient
Last author update: 1 May 2016
Last staff update: 15 November 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: HLRCC renal cancer



Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Prognostic factors | Case reports | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Differential diagnosis | Additional referencesCite this page: Andeen NK, Tretiakova M. FH deficient. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorHLRCC.html. Accessed December 3rd, 2024.
Definition / general
- Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome associated renal cancer may be papillary, solid and infiltrative
- It has characteristic inclusion-like nucleoli with perinucleolar clearing
- Due to germline fumarate hydratase (FH) mutations
- Other common clinical manifestation is nonrenal leiomyomatosis
Essential features
- Oncogenesis driven by metabolic derangements due to defective fumarate hydratase enzyme
- High grade, papillary, solid or infiltrative with prominent CMV inclusion-like nucleoli with perinucleolar clearing (may be only focal)
- Immunohistochemically shows overexpression of modified cysteine (2SC) and loss of fumarate hydratase
- May be confirmed by germline fumarate hydratase mutation
Terminology
- HLRCC syndrome has germline mutations of fumarate hydratase gene, conferring an increased risk of uterine and cutaneous leiomyomata as well as renal cancer
- The associated renal cell carcinoma is termed HLRCC associated renal cancer
- Also called FH deficient
Epidemiology
- Rare
- HLRCC syndrome has been reported in more than 300 families worldwide (GeneReviews 2006;2015:NBK1252)
Sites
- Kidney
- Leiomyomas in uterus and skin in HLRCC syndrome
Pathophysiology
- Mutations in the Fumarate Hydratase (FH) gene lead to a defective FH enzyme in the citric acid cycle, causing metabolic derangement, "pseudohypoxic" upregulation of hypoxia inducible factor 1 alpha (HIF1a) and nonenzymatic modification of cysteine residues in multiple proteins (succination), altering their function and ultimately driving oncogenesis (Am J Surg Pathol 2014;38:567, Oncogene 2014;33:2547)
Diagrams / tables
Images hosted on other servers:

Proposed
mechanisms of
tumorigenesis
in HLRCC
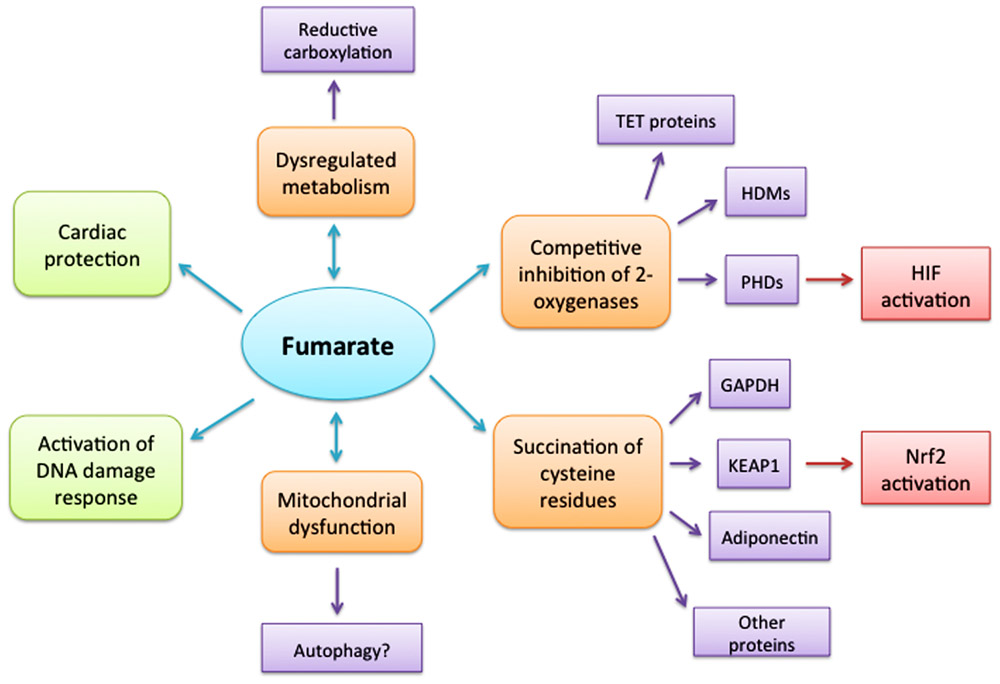
Consequences
of elevated
cellular
fumarate

TCA cycle enzyme
Clinical features
- HLRCC associated renal cancer occurs in 1/3 with HLRCC germline mutation
- Mean age of presentation with renal cancer: 36 years (Am J Surg Pathol 2014;38:627)
- Leiomyomas of skin and uterus are the most common features (seen in 85%), usually develop in the 3rd decade
- Uterine leiomyomas are often numerous and large, 50% of women have hysterectomy before age 30 (18 - 52 years)
Diagnosis
- Description of clinical and genetic diagnostic criteria for HLRCC syndrome (GeneReviews 2006;NBK1252:)
Prognostic factors
- HLRCC has a poor prognosis, with early and widespread metastases, even with small tumors
Case reports
- Decreased fumarate hydratase activity and identification of FH mutation in circulating lymphocytes in 2 young patients with fibroids (J Obstet Gynaecol Res 2013;39:410)
- Development of cutaneous leiomyomas and diagnosis of HLRCC syndrome in pregnancy (J Cutan Med Surg 2016;20:334)
- 59 year old woman with widespread metastases (Am J Surg Pathol 2014;38:567)
- 64 year old man and his 39 year old son without cutaneous leiomyomata (BMC Res Notes 2014;7:203)
Gross description
- Solitary, unilateral
- Solid or cystic, 2.5 - 12 cm
Microscopic (histologic) description
- High grade with various patterns: papillary, tubular, solid, cribriform, cystic, collecting duct carcinoma-like, sarcomatoid (Am J Surg Pathol 2014;38:627)
- Prominent eosinophilic CMV-like nucleoli with perinucleolar halo (may be only focal)
- May have hyalinized and edematous fibrovascular cores with micropapillary fronds but no foamy histiocytes (Am J Surg Pathol 2014;38:627)
Microscopic (histologic) images
Contributed by Debra Zynger, M.D., Nicole K. Andeen, M.D. and Maria Tretiakova, M.D., Ph.D.

FH deficient RCC

FH
CAIX

PAX8
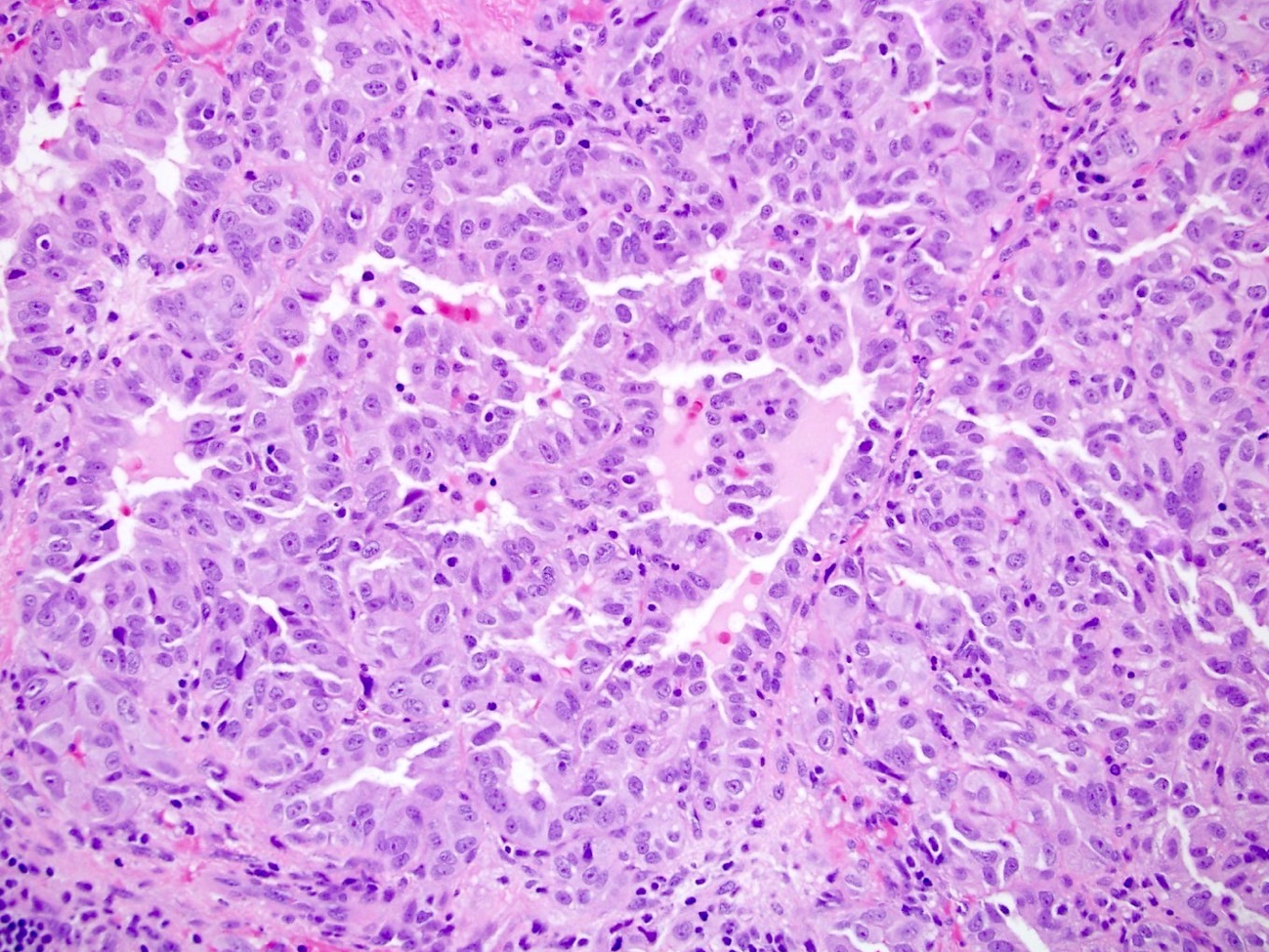
HLRCC with
tubulopapillary
growth and
eosinophilic cells

HLRCC with pale
eosinophilic cytoplasm
and inclusion-like
nucleoli

Uterine leiomyoma
from a patient
with HLRCC, with
multinucleation
Images hosted on other servers:




Findings in patient with HLRCC and RCC


HLRCC renal tumors

Clear cell RCC

Uterine leiomyomas in HLRCC

2SC IHC shows
diffuse and strong
reactivity in HLRCC
renal cancer

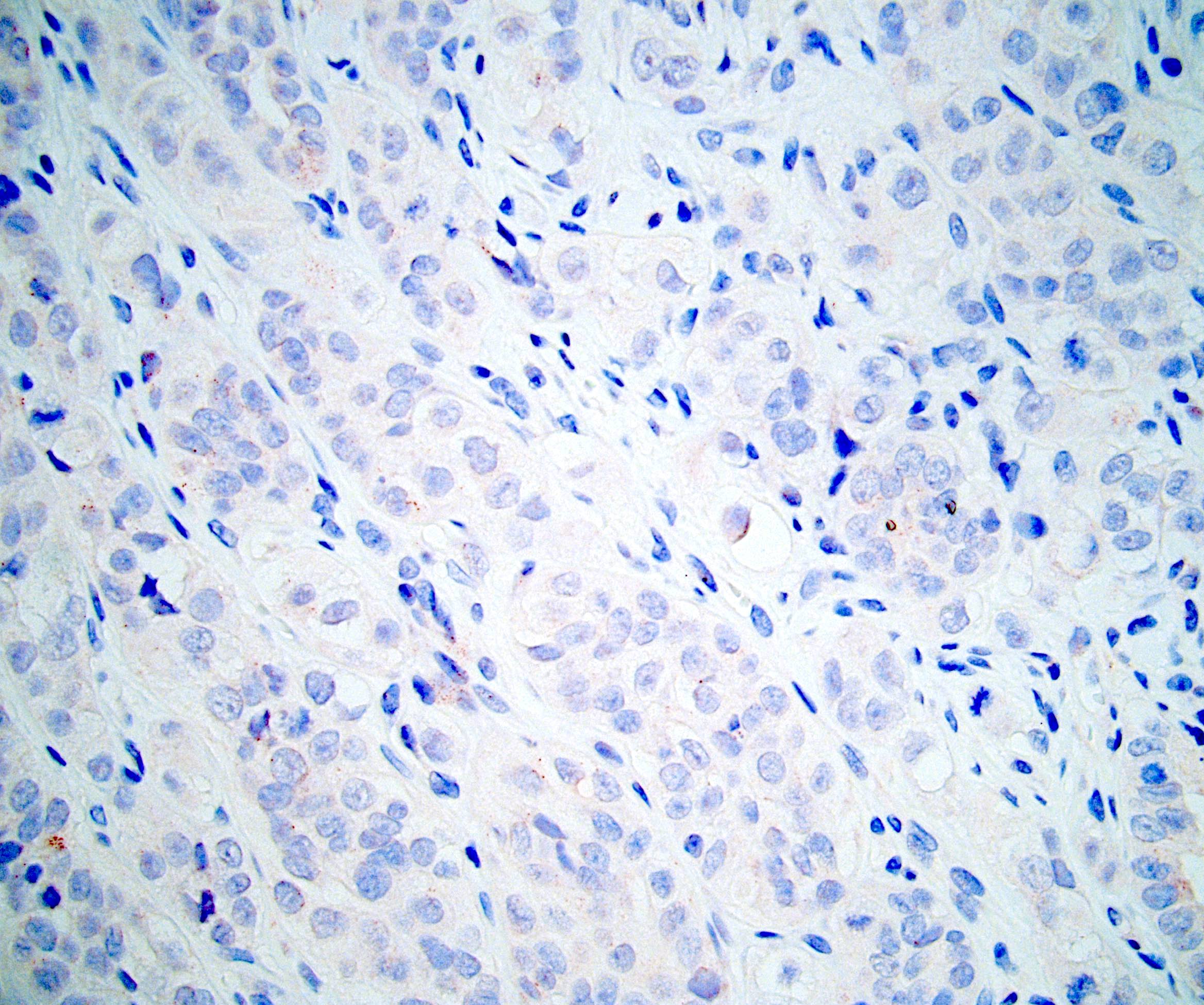
2SC IHC shows
cytoplasmic staining
pattern in a few
unclassified RCC
Positive stains
- PAX8, vimentin, GLUT1, p53, S100A1, SDHB, INI1 (Am J Surg Pathol 2018;42:279, Histopathology 2018;72:588)
- 2-succino-cysteine / 2SC overexpression (nuclear and cytoplasmic staining), which is more sensitive and specific for FH gene mutation than loss of FH by IHC (Am J Surg Pathol 2016;40:982, Am J Surg Pathol 2015;39:1529)
Negative stains
Molecular / cytogenetics description
- Fumarate Hydratase (FH) gene is located on 1q42-43, and consists of 10 exons
- Autosomal dominant inheritance
- In HLRCC, oxidative phosphorylation is impaired, and cells undergo a metabolic shift to aerobic glycolysis (Clin Cancer Res 2013;19:3345)
- Without fumarate hydratase activity, fumarate increases and acts as an oncometabolite
- Fumarate impairs the function of hypoxia inducible factor prolyl hydroxylase, resulting in increased levels of HIF1alpha (WHO 2016)
Differential diagnosis
- Overall, careful examination for characteristic nucleolar features, cytoplasmic and nuclear reactivity for S (2 succino) cysteine (2SC) and loss of fumarate hydratase expression appear to be most useful in the differential diagnosis
- Papillary type 2 RCC: unlike HLRCC, often expresses AMACR, may express CK7 (20%)
- 22% show cytoplasmic reactivity for 2SC, but nuclear staining is less likely to be diffuse compared with HLRCC (Am J Surg Pathol 2014;38:627)
- FH deficient RCC
- Remarkably similar to HLRCC clinically
- Morphologically and immunophenotypically similar, but harbor somatic and not germline mutations (Am J Surg Pathol 2016;40:865)
- Clear cell RCC: has membranous CAIX staining and no 2SC reactivity, unlike HLRCC
- Collecting duct carcinoma: CD10 and 2SC negative
- Microphthalmia transcription factor (MiT) family translocation associated RCC: TFE3 positive, 2SC negative
- Unclassified RCC: 2SC negative (Am J Surg Pathol 2014;38:627)
Additional references

