
Kidney nontumor / medical renal
Glomerular disease
Focal segmental glomerulosclerosis (FSGS)
FSGS-collapsing variant
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 6 November 2020
Last staff update: 12 October 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Focal segmental glomerulosclerosis collapsing variant

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Immunofluorescence description | Electron microscopy description | Electron microscopy images | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Breitbarth A, Andeen NK. FSGS-collapsing variant. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyfsgscollapsing.html. Accessed April 2nd, 2025.
Definition / general
- Morphologic variant of focal segmental glomerulosclerosis (FSGS) characterized by capillary loop collapse and prominence of overlying epithelial cells (Semin Nephrol 2003;23:209)
Essential features
- At least 1 glomerulus with capillary loop collapse and prominence of overlying podocytes or parietal epithelial cells
- Worse prognosis than other variants of focal segmental glomerulosclerosis; supersedes other variants if others present in biopsy
- May be associated with viruses, genetics, drugs, vascular injury and autoimmune diseases
Terminology
- Collapsing glomerulopathy (CG), collapsing focal segmental glomerulosclerosis (FSGS), FSGS collapsing variant
- Early descriptions as a component of HIV associated nephropathy
ICD coding
- ICD-10: N04.1
Epidemiology
- APOL1 high risk alleles common in individuals with African ancestry are associated with increased rates of kidney injury including collapsing focal segmental glomerulosclerosis (Kidney Int 2015;87:332)
Pathophysiology
- No single pathogenic trigger has been identified
Etiology
- Multiple associations described (J Am Soc Nephrol 2006;17:2854, Clin Kidney J 2017;10:443):
- Infection
- Human immunodeficiency virus (HIV)
- Parvovirus B19 (Kidney Int 2001;59:2126)
- Cytomegalovirus
- Hepatitis C
- Drugs
- Bisphosphonates (pamidronate) (J Am Soc Nephrol 2001;12:1164)
- Interferons alpha and beta (Clin J Am Soc Nephrol 2010;5:607)
- Anabolic steroids
- Heroin
- Vascular and metabolic disease (Lancet 1996;347:231)
- Thrombotic microangiopathy (Kidney Int 2016;90:1321)
- Severe diabetic nephropathy (Nephrol Dial Transplant 2014;29:392)
- Severe vascular and microvascular disease (Mod Pathol 2018 Oct 16 [Epub ahead of print])
- Genetic conditions
- APOL1 high risk alleles
- Mitochondrial abnormalities
- Autoimmune disorders
- Posttransplant, recurrent and de novo
- Donor APOL1 high risk genotypes associated with poorer allograft outcome (Kidney Int 2018 Oct 2 [Epub ahead of print])
- Infection
Clinical features
- High incidence of nephrotic syndrome
- Renal insufficiency
Diagnosis
- Renal biopsy is required for diagnosis
Laboratory
- Nephrotic range proteinuria
- Elevated serum creatinine at presentation (Am J Kidney Dis 1999;33:652)
Prognostic factors
- Worse 1 year (74%) and 3 year (33%) renal survival compared with other variants of focal segmental glomerulosclerosis (Kidney Int 2006;69:920)
- Worse prognosis if steroid unresponsive (J Am Soc Nephrol 2004;15:2169)
- Renal insufficiency at time of presentation is a poor prognostic factor (Saudi J Kidney Dis Transpl 2015;26:173)
Case reports
- 6 year old boy with hepatitis B (Indian J Nephrol 2016;26:291)
- 21 year old African American woman with sickle cell disease (J Med Case Rep 2011;5:71)
- 38 year old Chinese man with coxsackievirus infection (Exp Ther Med 2016;11:1871)
- 50 year old man with lupus and diffuse alveolar hemorrhage (Transplant Proc 2017;49:913)
- 2 patients with lambda light chain amyloidosis (Am J Kidney Dis 2018;72:612)
Treatment
- Treatment of underlying etiology, if identifiable
- In patients with HIV, highly active antiretroviral therapy (HAART) is the first line treatment and reduces rates of progression to end stage renal disease (J Am Soc Nephrol 2005;16:2412)
- In virus negative patients, steroid therapy and other immunosuppression is frequently used, although often refractory (J Am Soc Nephrol 2006;17:2854)
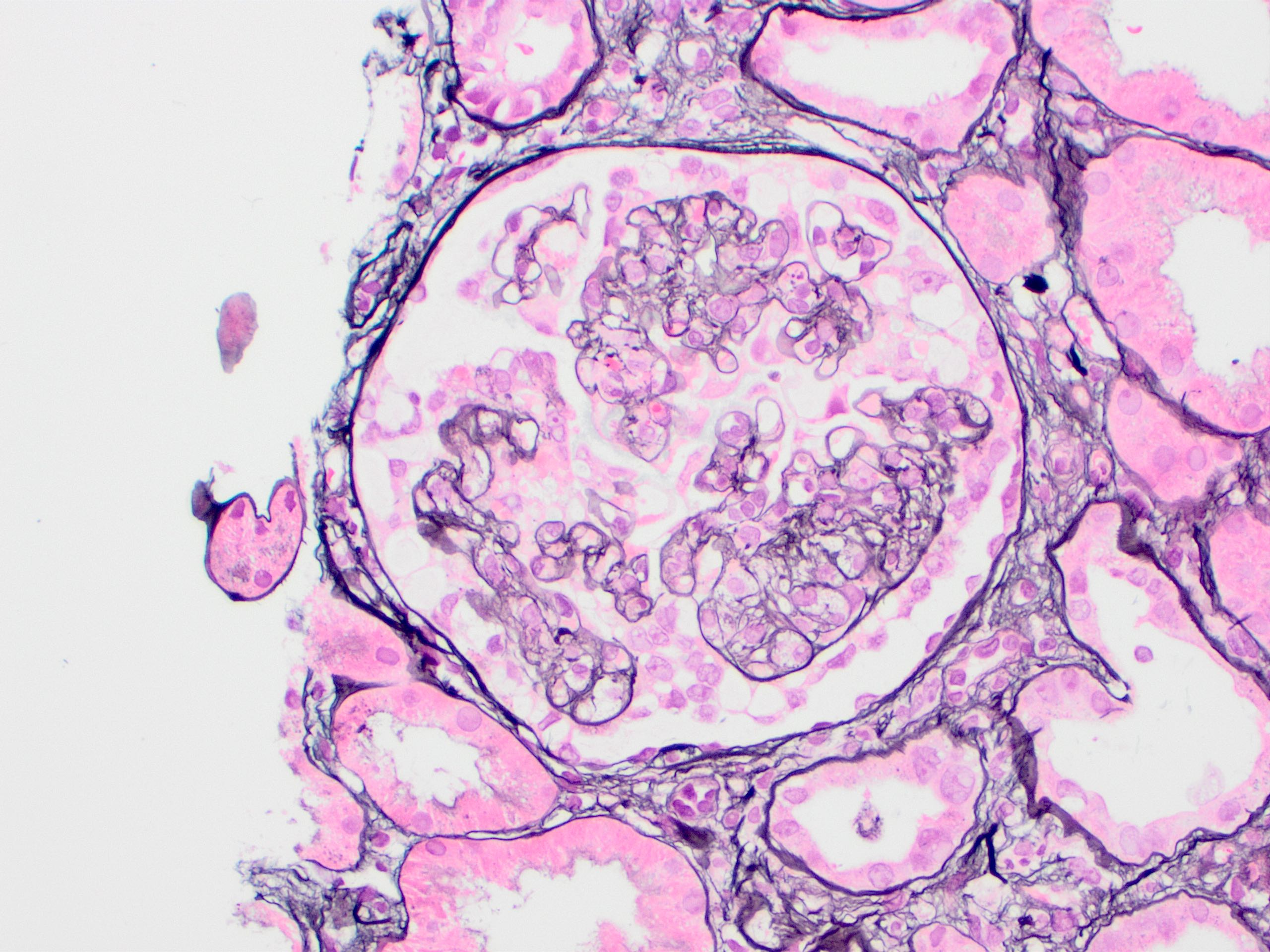
Microscopic (histologic) description
- At least 1 glomerulus with segmental collapse of the tuft, obliteration of the capillary loops and overlying podocyte or parietal cell hypertrophy or hyperplasia (Am J Kidney Dis 2004;43:368)
- May appear as pseudocrescents filling Bowman space
- Podocytes frequently form a radial corona around the glomerular tuft and have protein resorption droplets
- Lacks necrosis
- Particularly in HIV associated collapsing focal segmental glomerulosclerosis, may have significant chronic tubulointerstitial scarring and tubular microcysts
Microscopic (histologic) images
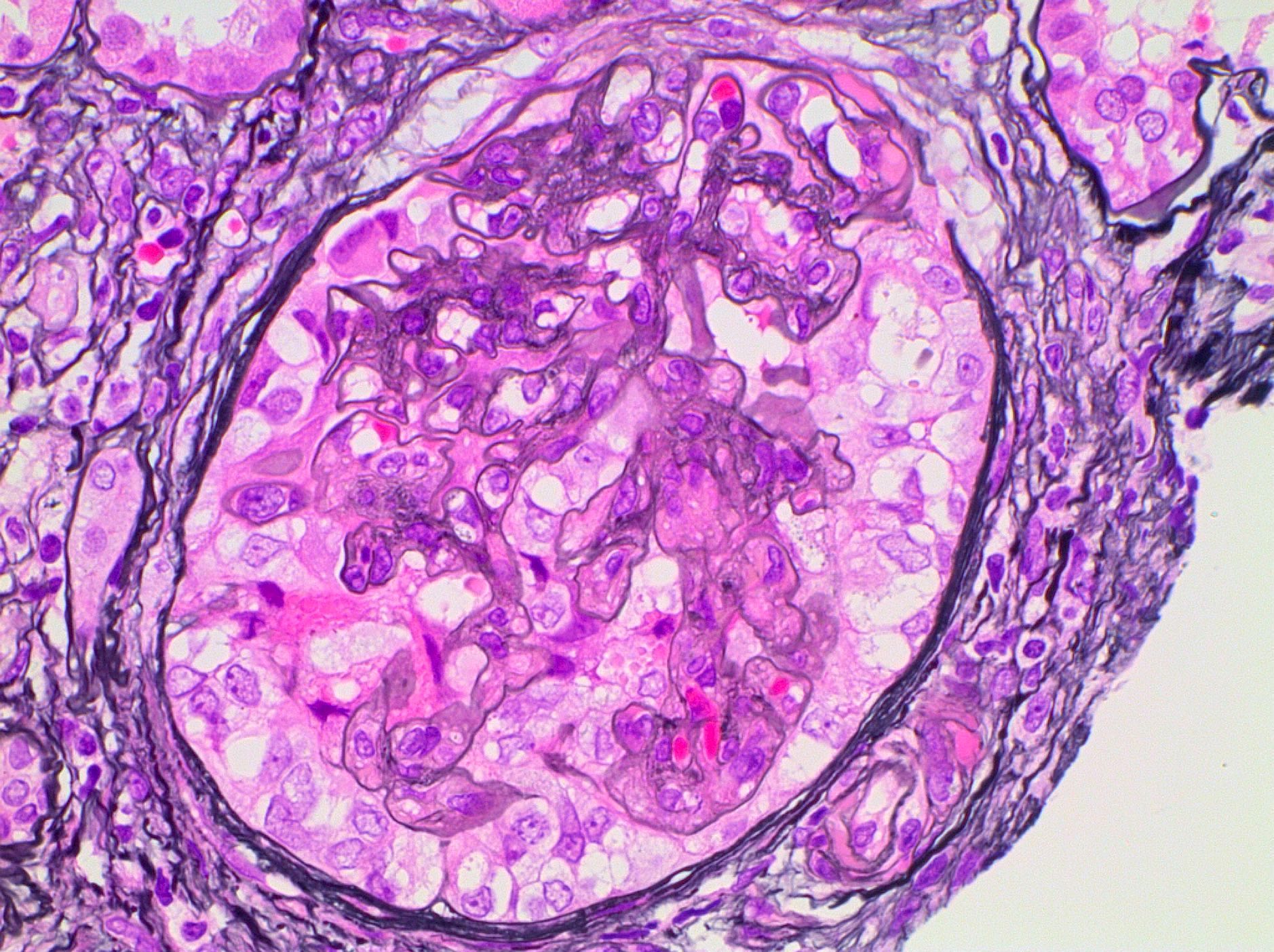
Contributed by Nicole K. Andeen, M.D.
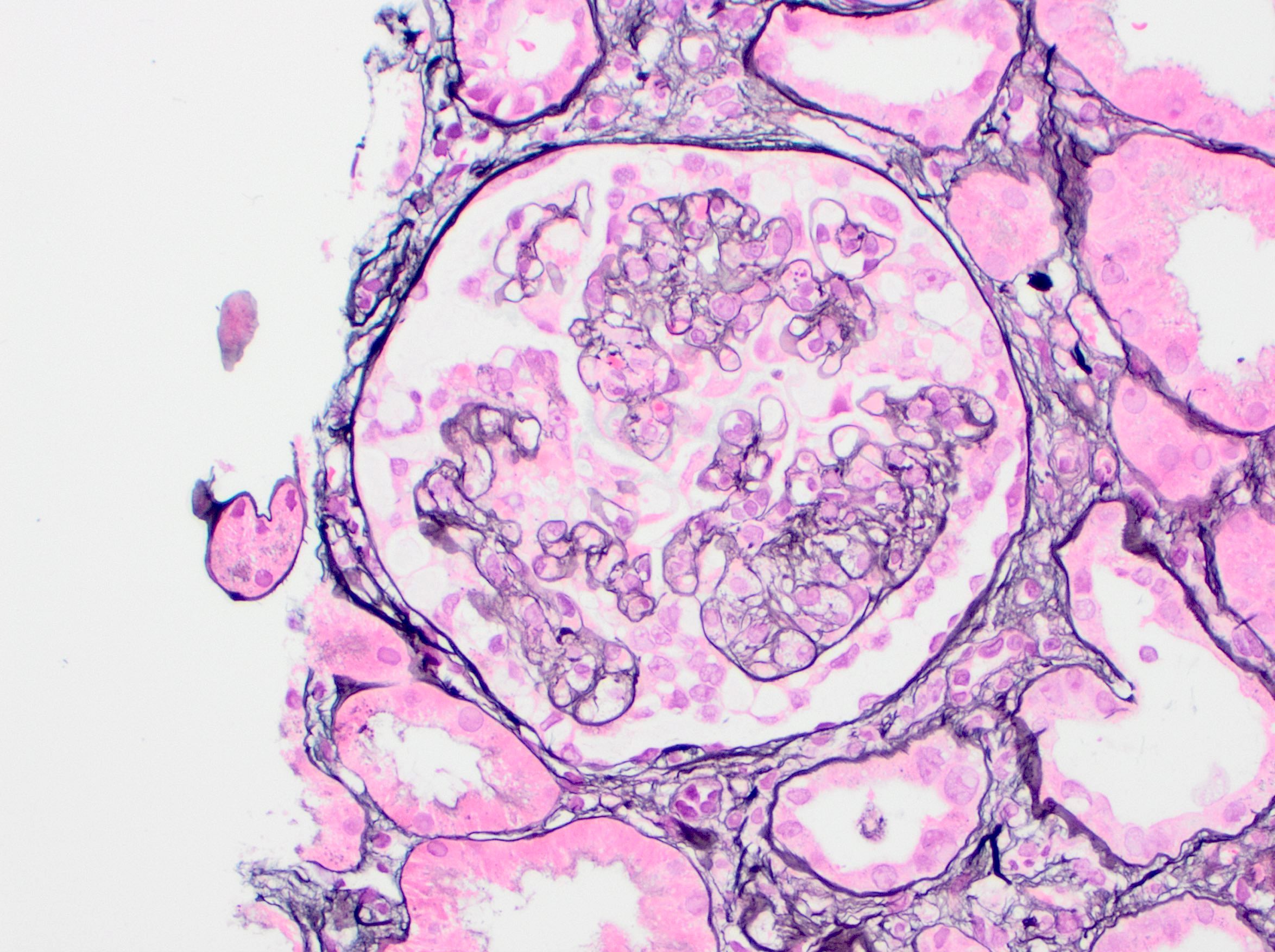
Collapse of the glomerular tuft and prominence of the overlying epithelial cells, Jones stain
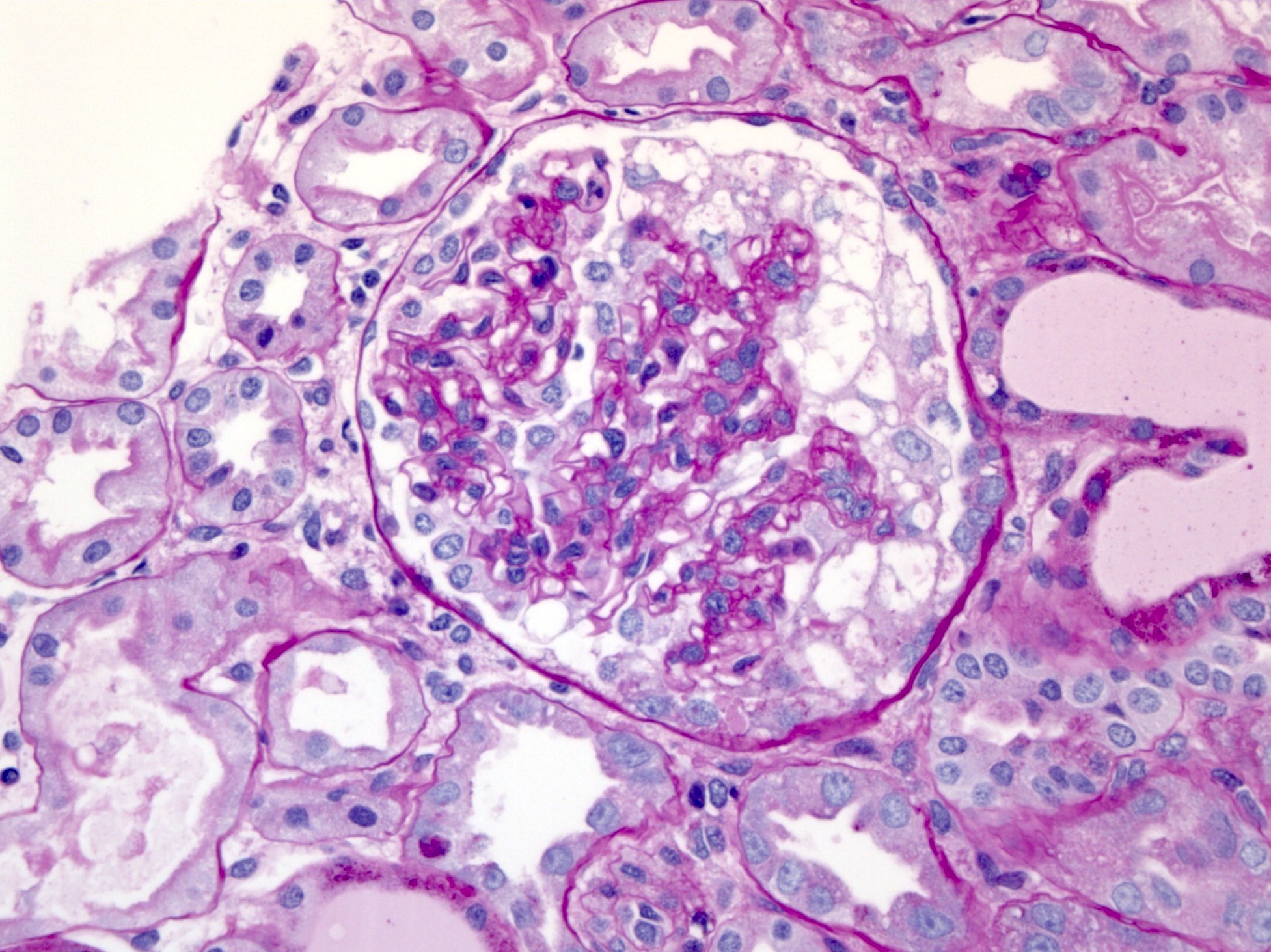
PAS
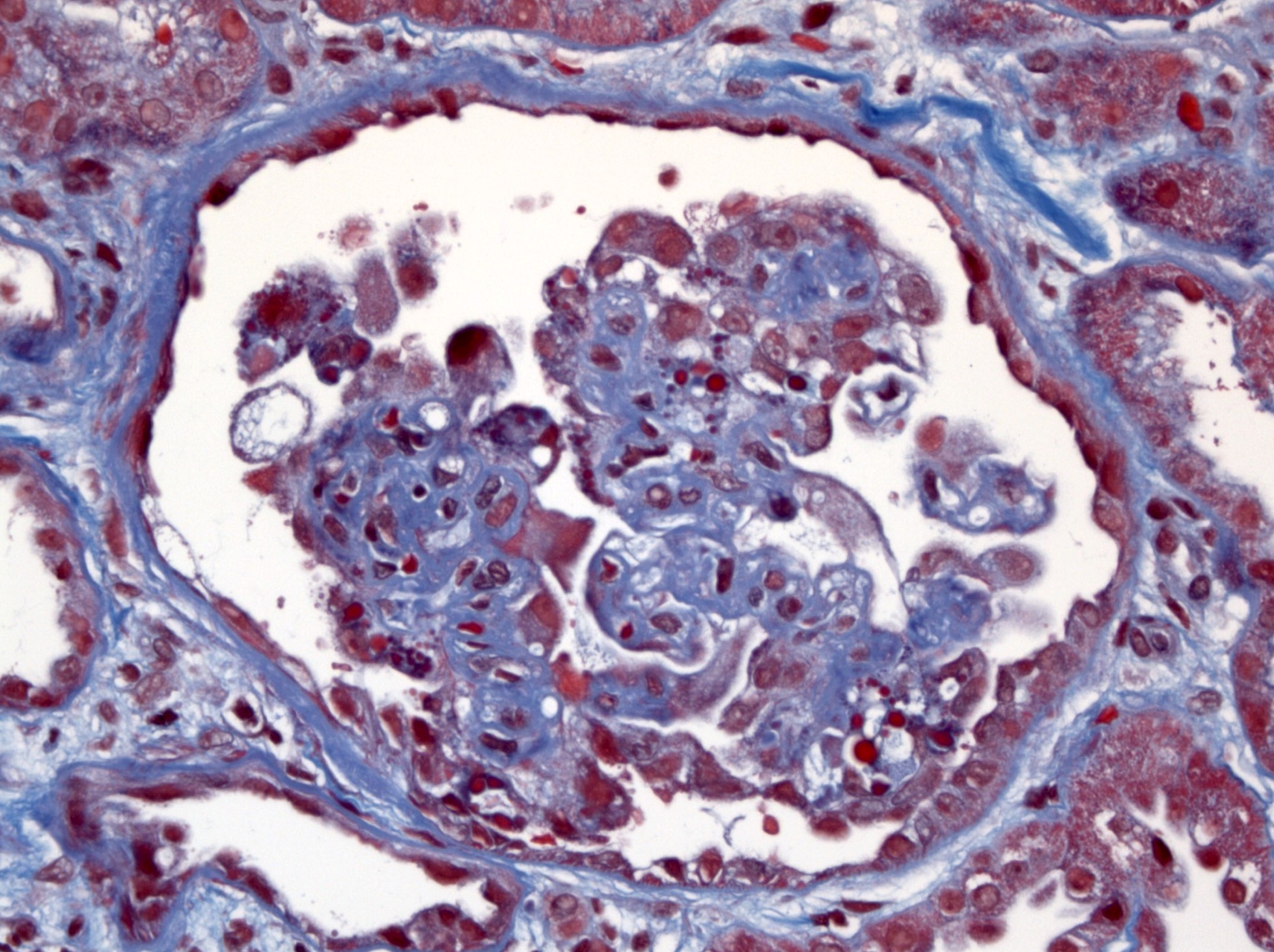
Trichrome
Images hosted on other servers:

Collapsed glomerulus

With sickle cell disease

Various images
Positive stains
- Jones methenamine silver, periodic acid Schiff (PAS): highlight glomerular architecture with basement membrane collapse
- Further stains not required and often not helpful in differential diagnosis
Negative stains
- Podocyte can have a dysregulated immunophenotype and lose expression of WT1, synaptopodin and p57 (J Am Soc Nephrol 2006;17:2854)
Immunofluorescence description
- Negative or nonspecific
- Collapsed segments with nonspecific IgM or C3 staining
- Visceral epithelial resorption droplets: IgG, IgA, light chains or albumin
- Tubular resorption droplets: IgG, IgA, light chains or albumin
Electron microscopy description
- Podocyte foot process effacement
- Endothelial tubuloreticular inclusions may be present in high interferon states, including HIV associated, lupus associated and interferon mediated collapsing glomerulopathy
Electron microscopy images
Contributed by Nicole K. Andeen, M.D.
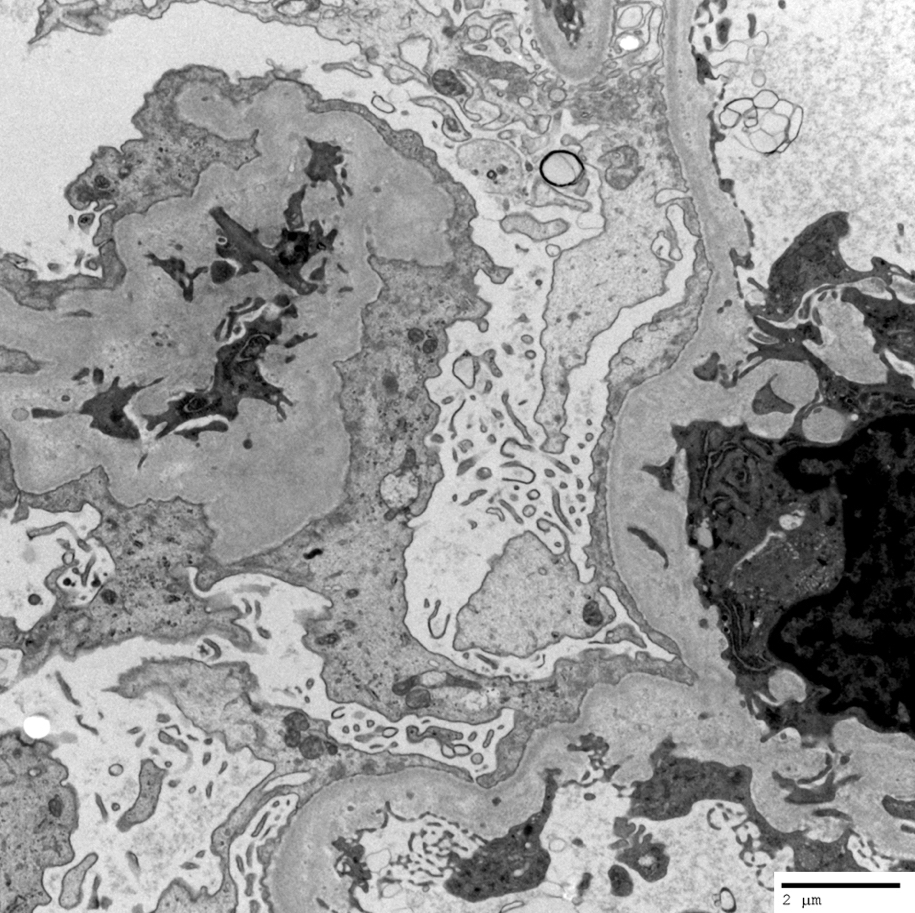
Podocyte foot process effacement
Differential diagnosis
- Focal segmental glomerulosclerosis (FSGS), cellular variant:
- Cellular variant has segmental to global endocapillary hypercellularity (occlusion of capillary loops due to influx of leukocytes, foam cells or endothelial cell swelling) and prominence of overlying epithelial cells in Bowman space
- Lacks collapse of glomerular tuft
- Crescentic glomerulonephritis:
- Segmental breaks in glomerular basement membrane and necrosis, influx of leukocytes in glomeruli and layered crescent orientation of cells in Bowman space
- May occasionally be difficult to distinguish in isolation; perform additional levels and evaluate surrounding parenchyma and clinical scenario
- Focal segmental glomerulosclerosis (FSGS), NOS:
- Lacks collapse of glomerular tuft
Board review style question #1
If present on kidney biopsy, which variant of focal segmental glomerulosclerosis (FSGS) has a significantly poorer prognosis and supersedes the presence of others (if other variants are present in the same biopsy) in the FSGS classification?
- Cellular variant
- Collapsing variant
- Hilar variant
- Tip variant
Board review style answer #1
B. Collapsing variant
Comment Here
Reference: Focal segmental glomerulosclerosis (FSGS), collapsing variant
Comment Here
Reference: Focal segmental glomerulosclerosis (FSGS), collapsing variant
Board review style question #2
A patient has a kidney biopsy for nephrotic syndrome. What does this image represent?
- Amyloidosis
- Cellular crescent
- Collapsing focal segmental glomerulosclerosis
- Minimal change disease
Board review style answer #2
C. Collapsing focal segmental glomerulosclerosis
Comment Here
Reference: Focal segmental glomerulosclerosis (FSGS), collapsing variant
Comment Here
Reference: Focal segmental glomerulosclerosis (FSGS), collapsing variant
