

Kidney nontumor / medical renal
Renal allograft
Acute / chronic active T cell mediated rejection
Author: Arzu Sağlam, M.D.
Editorial Board Member: Nicole K. Andeen, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 11 January 2021
Last staff update: 15 February 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Kidney (acute OR chronic) cellular rejection[TI]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Banff scoring of histological lesions | Microscopic (histologic) images | Immunofluorescence description | Special stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Sağlam A. Acute / chronic active T cell mediated rejection. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyacutechroniccellularrejection.html. Accessed December 2nd, 2024.
Definition / general
- Alloimmune reaction to major histocompatibility complex (MHC) and non-MHC donor alloantigens resulting in damage to the kidney allograft
- Mediated by T cells and hence referred to as T cell mediated rejection (TCMR) in the Banff 2019 classification (Am J Transplant 2020;20:2318)
- 2 major subcategories:
- Acute T cell mediated rejection: characterized by an acute immunologic reaction
- Chronic active T cell mediated rejection: chronic renal injury due to persistent / recurrent TCMR
Essential features
- Tubulitis and active interstitial inflammation
- Coded by the i and t Banff scores (see Banff grading below)
- Intimal arteritis or vasculitis may also be present (can sometimes be the sole component)
- This lesion can be caused by T cell mediated rejection (TCMR), active antibody mediated rejection or both
Terminology
- Acute T cell mediated rejection: also referred to as acute cellular rejection, acute interstitial rejection, acute tubulointerstitial rejection
- Chronic active T cell mediated rejection: also referred to as chronic cellular rejection
ICD coding
- ICD-10: T86.11 - kidney transplant rejection
Epidemiology
- With currently used combination therapies, 1 year acute rejection rates have decreased to 10 - 15%
Sites
- Renal disease
Pathophysiology
- T cells are sensitized and react against donor antigens expressed on antigen presenting cells and donor cells; delayed type hypersensitivity is also involved (Clin Biochem 2016;49:320, Nephron 2016;132:227)
- Macrophages and granulocytes are frequently recruited and also mediate tissue injury
- Tissue injury is manifested predominantly as tubular epithelial injury (tubulitis) and endothelial cell injury (intimal arteritis)
Etiology
- Due to transplantation of foreign donor kidney allograft into recipient
Clinical features
- Acute T cell mediated rejection (TCMR):
- Usually seen during the first month after transplantation or later as immune suppression decreases due to noncompliance, adjustment of medication by physicians (as complications present), gastrointestinal diseases, metabolic diseases, etc.
- Presents with acute renal failure or oliguria; may also be asymptomatic (diagnosed on protocol biopsies)
- Chronic active TCMR: chronic renal failure with or without proteinuria; may also be asymptomatic (diagnosed on protocol biopsies)
Diagnosis
- Established via indication or protocol biopsies
Diagnostic criteria and Banff classification / grading (modified from the Banff 2019 revision, Am J Transplant 2020;20:2318):
- Suspicious / borderline for acute T cell mediated rejection (TCMR):
- Tubulitis (t1, t2, t3) with interstitial inflammation comprising 10 - 25% of the nonscarred cortex (i1)
- Interstitial inflammation comprising > 25% of the nonscarred cortex (i2 or i3) with mild tubulitis (t1, pertaining to 1 - 4 inflammatory cells per tubular cross section)
- No arteritis
- Acute TCMR:
- Grade IA: interstitial inflammation involving > 25% of nonscarred cortex (i2 or i3) with moderate tubulitis (t2) of at least one tubule, excluding atrophic tubules
- Grade IB: interstitial inflammation involving > 25% of nonscarred cortex (i2 or i3) with severe tubulitis (t3) of at least one tubule, excluding atrophic tubules
- Grade IIA: mild to moderate intimal arteritis (v1) with or without interstitial inflammation or tubulitis
- Grade IIB: severe intimal arteritis (v2) with or without interstitial inflammation or tubulitis
- Grade III: transmural arteritis or arterial fibrinoid necrosis of medial smooth muscle with accompanying mononuclear cell intimal arteritis (v3) with or without interstitial inflammation or tubulitis
- Chronic active TCMR:
- Grade IA: interstitial inflammation involving > 25% of the total cortex (ti2 or ti3) and > 25% of the scarred cortex (i-IFTA2 or i-IFTA3) with moderate tubulitis (t2 or t-IFTA2) of at least one tubule, excluding severely atrophic tubules; other known causes of i-IFTA should be ruled out
- Grade IB: interstitial inflammation involving > 25% of the total cortex (ti2 or ti3) and > 25% of the scarred cortex (i-IFTA2 or i-IFTA3) with severe tubulitis (t3 or t-IFTA3) of at least one tubule, excluding severely atrophic tubules; other known causes of i-IFTA should be ruled out
- Grade II: chronic allograft arteriopathy
- Prior to Banff classification, cooperative clinical trials in transplantation (CCTT) criteria set the threshold for acute TCMR as active interstitial inflammation in ≥ 5% of cortex and at least 3 tubules with tubulitis in 10 consecutive high power fields from the most severely affected areas (J Am Soc Nephrol 1997;8:1930)
Laboratory
- Acute T cell mediated rejection (TCMR): acute increase in serum creatinine levels
- Chronic active TCMR: chronic increase in serum creatinine levels, proteinuria may develop eventually
Radiology description
- Contrast enhanced ultrasound has been shown to be of diagnostic value in identifying cases of vascular rejection (Clin Hemorheol Microcirc 2018;69:77)
- New technologies for identification of acute rejection are at the experimental stage (Am J Nucl Med Mol Imaging 2019;9:110)
- Imaging seems to rely on analysis of changes in blood flow, which decreases with acute rejection induced inflammation and detection of recruitment of activated leucocytes with 18F-fluoro-deoxy-glucose positron emission tomography (Clin Kidney J 2017;10:97)
Prognostic factors
- Vascular rejection is associated with a poor long term outcome and is generally resistant to antirejection therapy (Kidney Int 2002;61:1516)
- Eosinophils and plasma cells within the inflammatory infiltrate is associated with poor long term outcome and resistance to antirejection therapy
Case reports
- 24 year old woman with severe interstitial lymphoplasmacytic infiltrate (Exp Clin Transplant 2020;18:106)
- 39 year old man with refractory CD20+ cellular rejection (Exp Clin Transplant 2019;17:823)
- 56 year old man with refractory cellular rejection treated with photopheresis (Nefrologia 2016;36:327)
Treatment
- Pulse steroid therapy for grade I acute T cell mediated rejection (TCMR) (Talanta 2014;130:542)
- Anti-T cell agents for grade II acute TCMR
- Grade III acute TCMR is resistant to therapy
- Newer immunosuppresive agents with more potent activity are emerging (Expert Opin Emerg Drugs 2017;22:123)
Gross description
- Acute T cell mediated rejection (TCMR): kidney is swollen, cortex is pale and shiny; hemorrhage and necrosis may be present in severe cases with vascular involvement
- Chronic active TCMR: kidney may be shrunken with surface depressions due to scarring of the underlying parenchyma; corticomedullary junction is blurred
Gross images
Contributed by Arzu Sağlam, M.D.

Chronic active TCMR, allograft nephrectomy
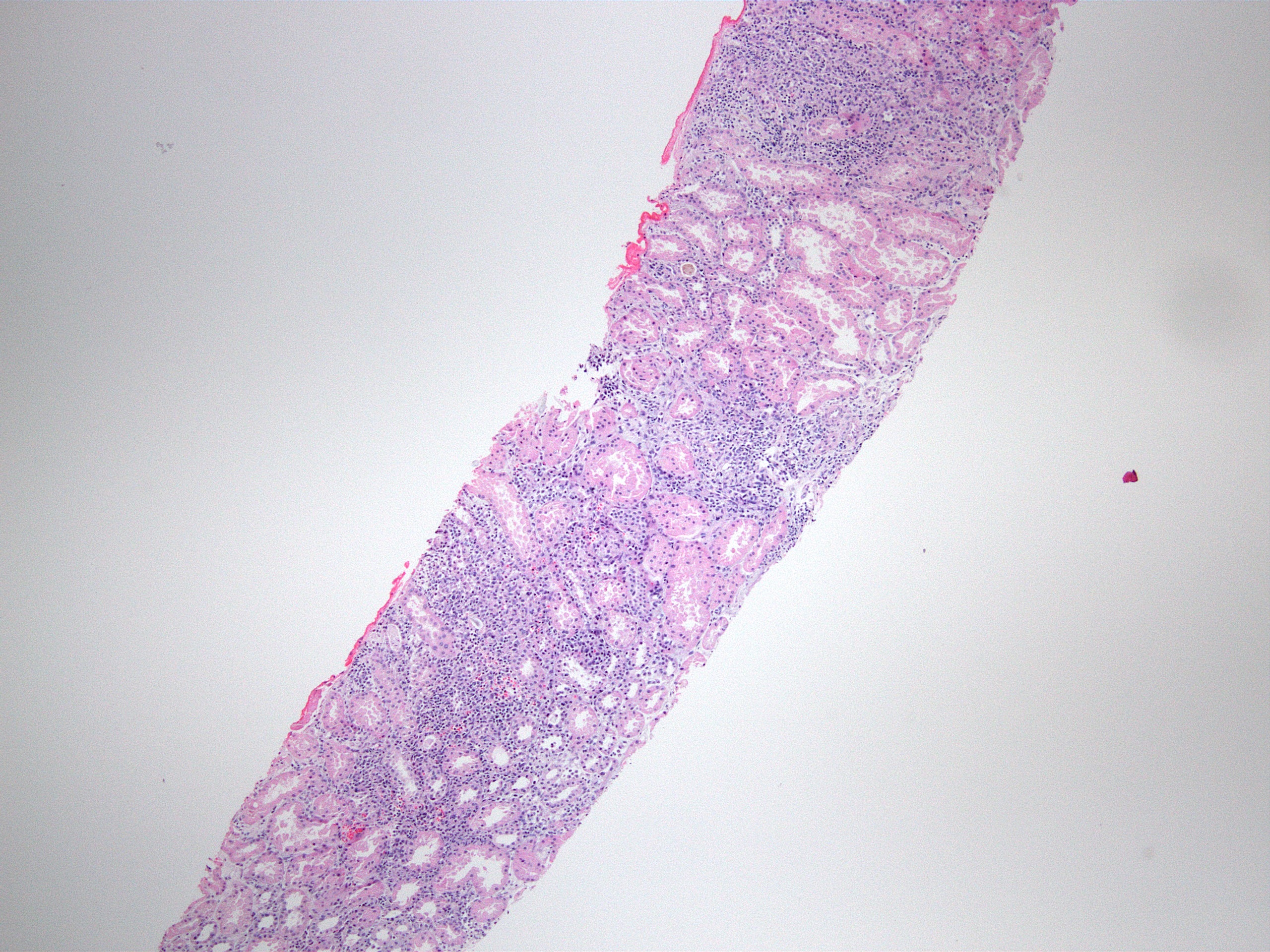
Microscopic (histologic) description
- Acute T cell mediated rejection (TCMR):
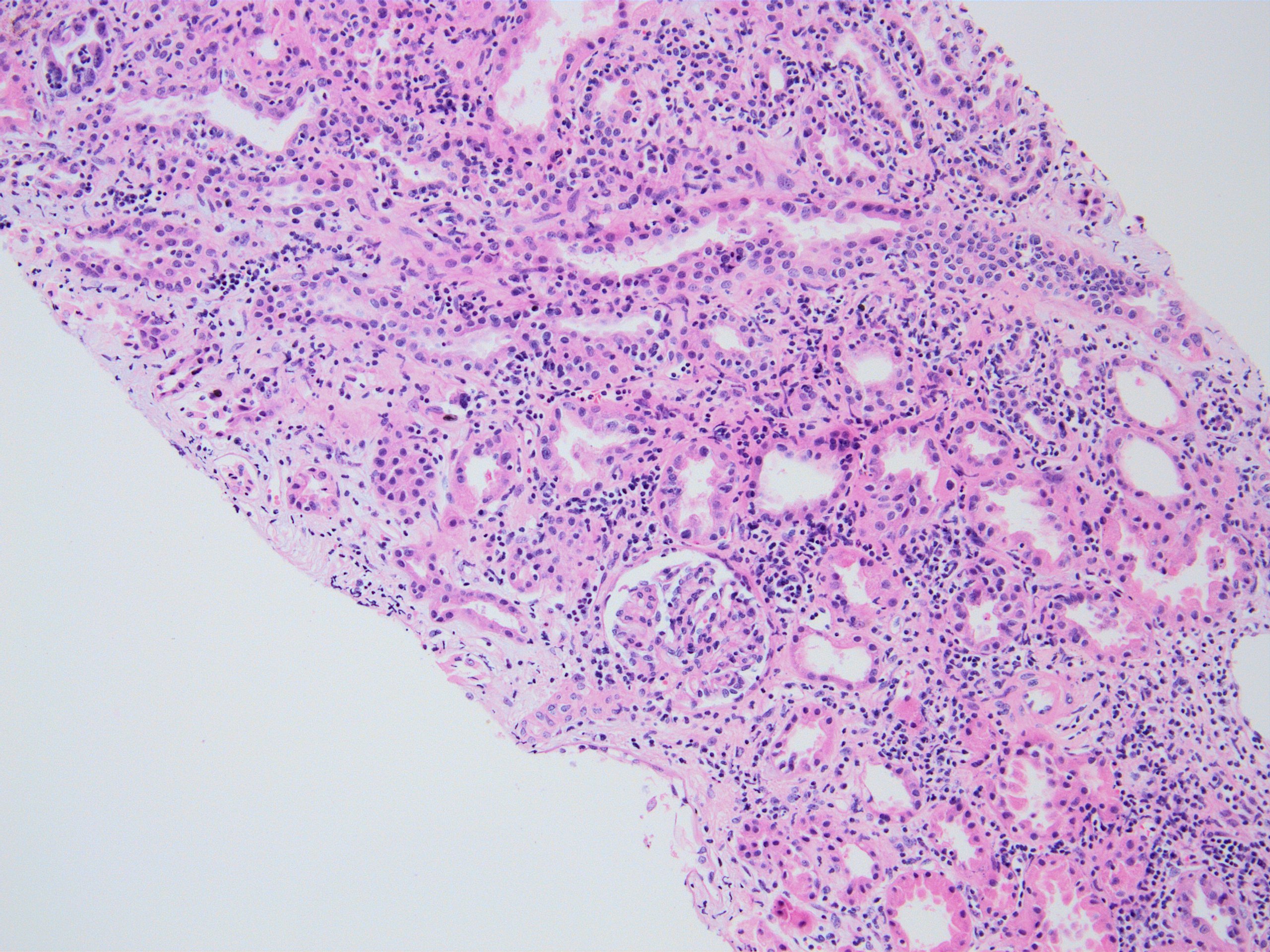
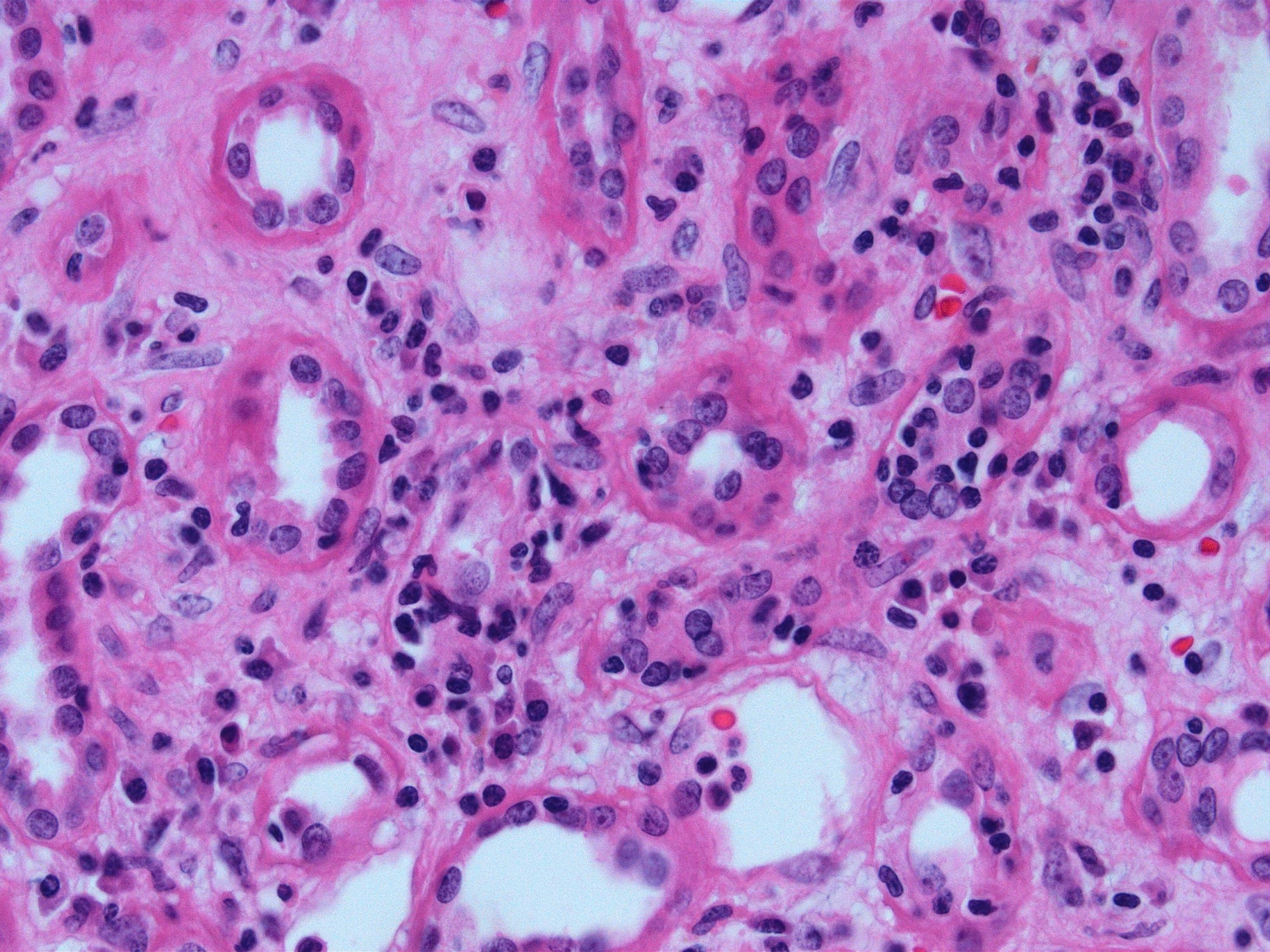
- Interstitial edema and inflammatory infiltrate involving at least 25% of the nonscarred cortex; graded according to severity (i score ≥ 2)
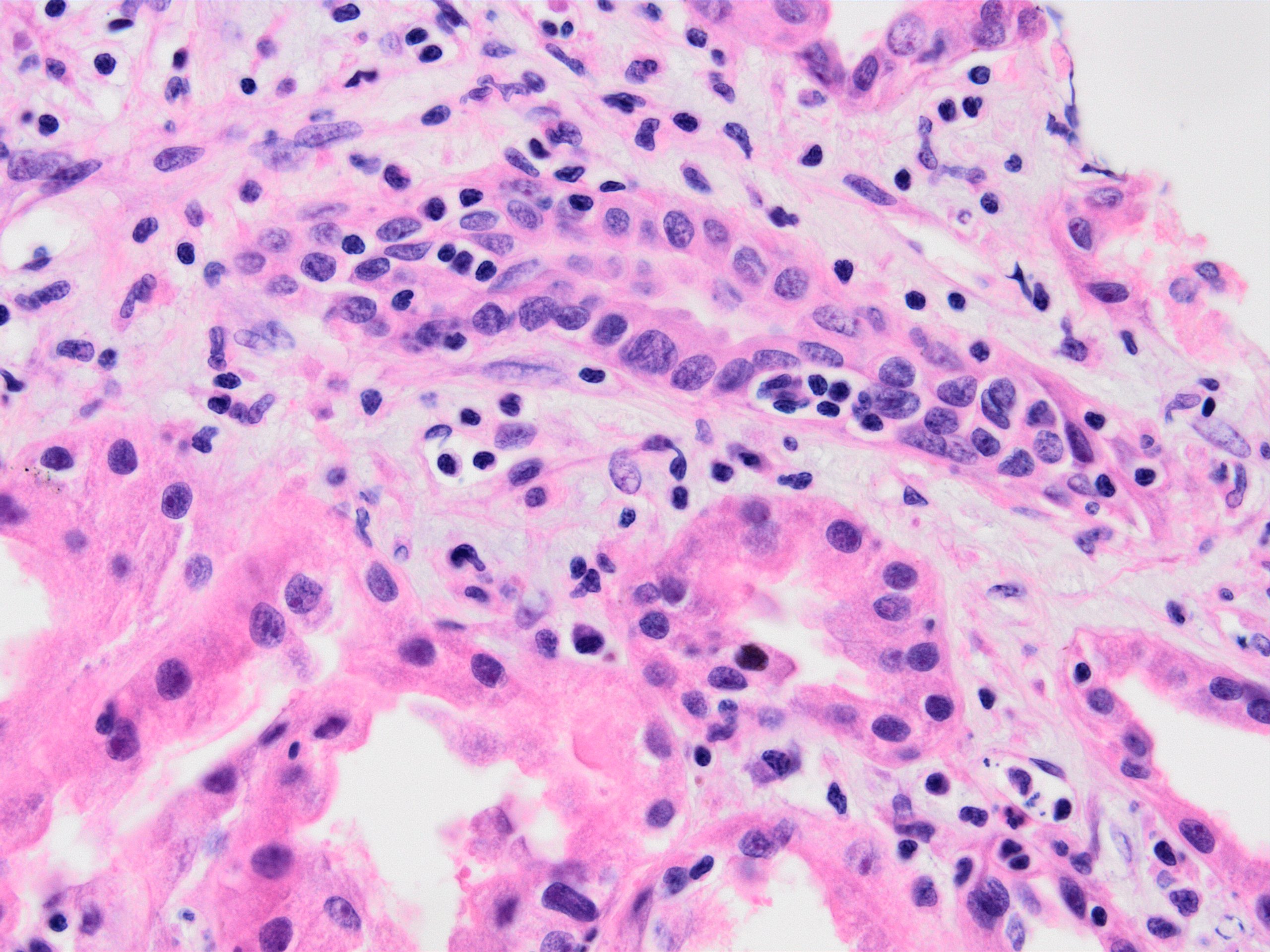
- Presence of tubulitis: inflammatory cells within and among tubular epithelial cells within the confines of the basement membrane; is graded according to severity (t score ≥ 2)
- Lesser degrees of inflammation (10 - 25% of the nonscarred cortex - i1) or inflammation involving ≥ 25% of the nonscarred cortex (i score ≥ 2) but accompanied by only mild tubulitis (t1 - up to 4 inflammatory cells / tubular cross section) is considered suspicious / borderline for acute TCMR
- Some studies suggest a lower threshold for diagnosis of rejection (t1i1) (Transplantation 2018;102:2120)
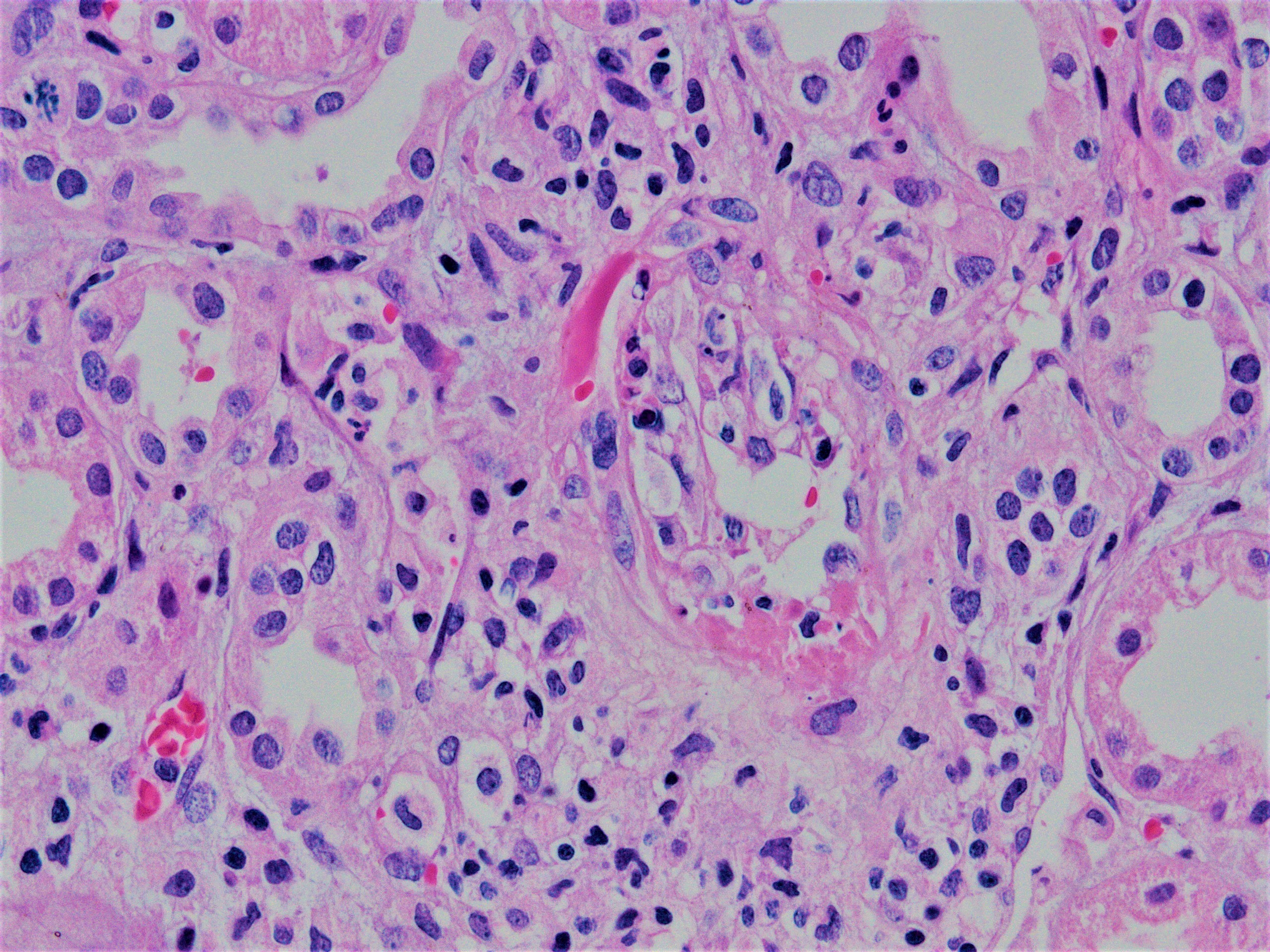
- Inflammatory population is mainly mononuclear - T cells and macrophages, CD4+ T cells dominate
- Eosinophils and plasma cells may also be present, especially in severe cases and more commonly if acute TCMR develops late (after the first year of transplantation)
- Glomeruli usually spared; however, in cases with accompanying vascular involvement, endothelial swelling and mesangiolysis may be present - acute allograft glomerulopathy
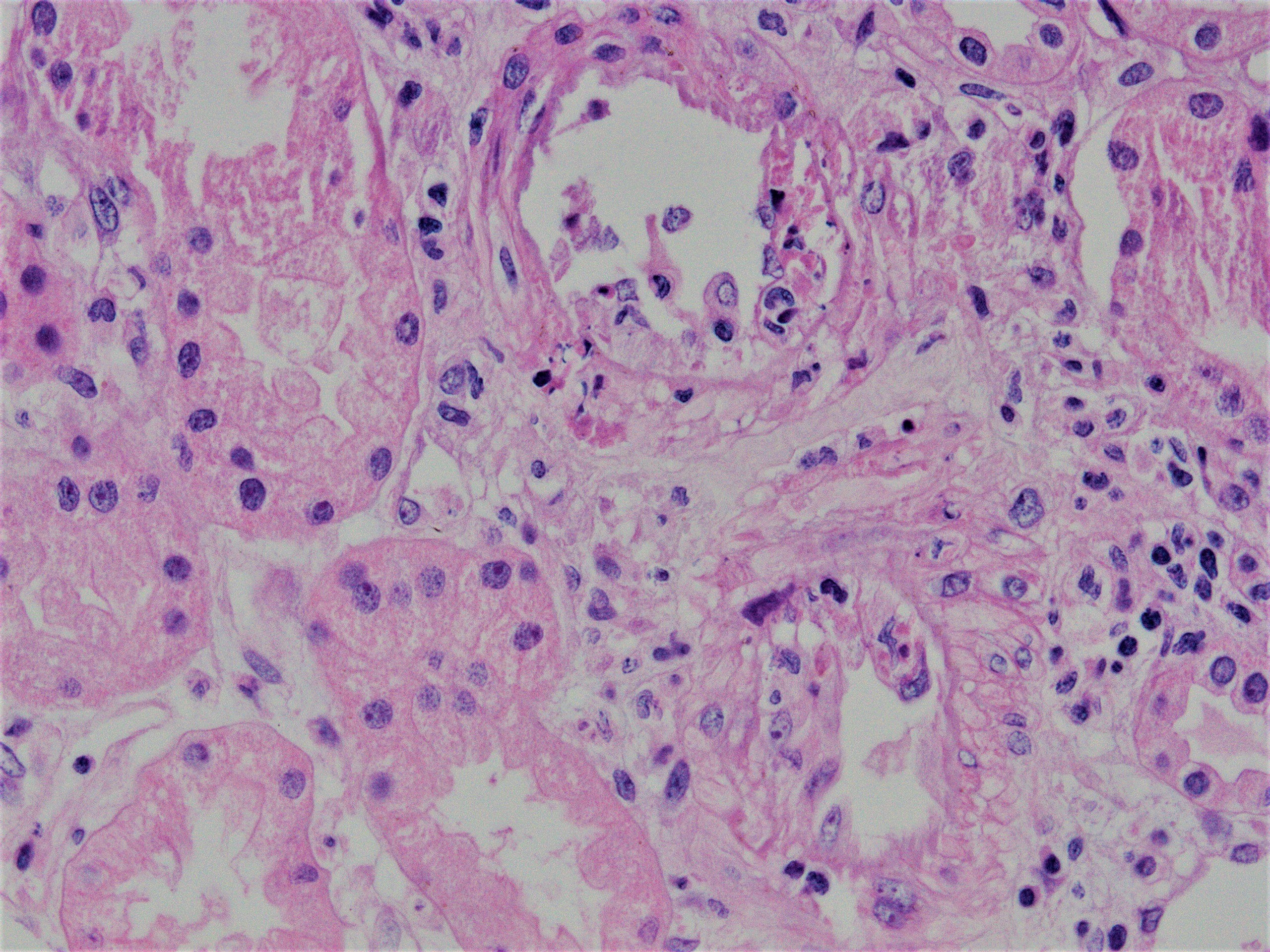
- Vascular involvement (type II and III): inflammation of the arterial or arteriolar wall, intimal infiltration (intimal arteritis, endarteritis, endothelialitis) or transmural infiltration by lymphocytes and macrophages, with or without accompanying fibrinoid necrosis; note that these vascular lesions can also be a part of active antibody mediated (humoral) rejection and are not a defining feature (unlike tubulitis)
- Chronic active TCMR:
- Areas of tubular atrophy and interstitial fibrosis with mononuclear inflammatory infiltrate and tubulitis; this morphology is referred to as i-IFTA (inflammation in areas of interstitial fibrosis / tubular atrophy) and t-IFTA (tubulitis in areas of interstitial fibrosis / tubular atrophy) (Am J Transplant 2018;18:364, Am J Transplant 2018;18:377)
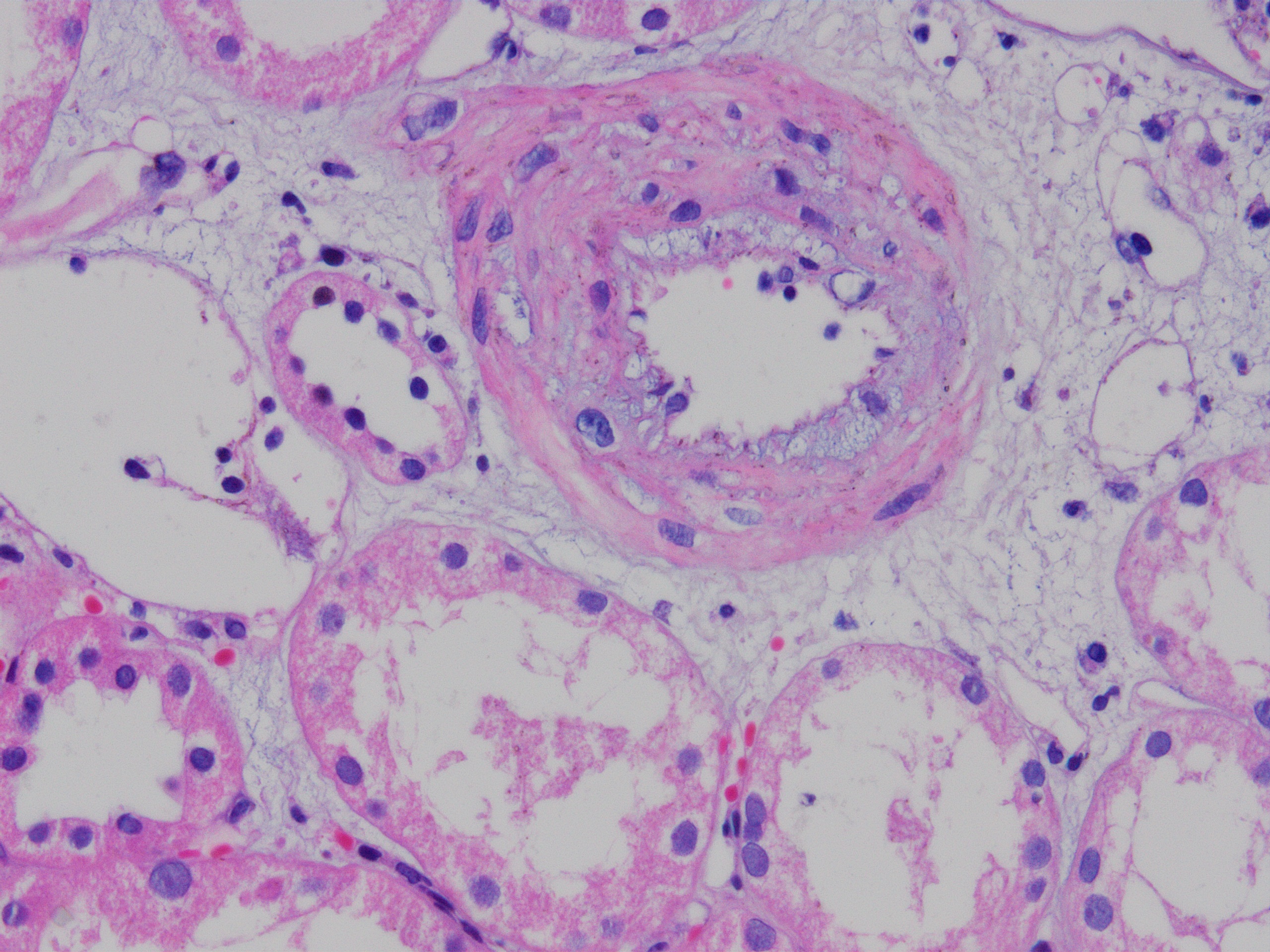
- Transplant arteriopathy: intimal fibrosis together with mononuclear cells and foam cells in the intima
- Glomeruli may show focal segmental and global sclerosis
- Other causes of i-IFTA (such as BK virus nephropathy, chronic pyelonephritis, antibody mediated rejection, recurrent glomerulonephritis) should be ruled out because i-IFTA is a nonspecific lesion
- References: Transplantation 2018;102:1795, Nephrology (Carlton) 2018;23 Suppl 2:45
Banff scoring of histological lesions
- Banff i interstitial inflammation scoring (Am J Transplant 2008;8:753, Zhou: Silva's Diagnostic Renal Pathology, 2nd Edition, 2017):
- i0: < 10% of nonfibrotic cortex
- i1: 10 - 25% of nonfibrotic cortex
- i2: 26 - 50% of nonfibrotic cortex
- i3: > 50% of nonfibrotic cortex
- Banff t tubulitis scoring:
- t0: no mononuclear cells in tubules
- t1: 1 - 4 cells / tubular cross section
- t2: 5 - 10 cells / tubular cross section
- t3: > 10 cells / tubular cross section
- v - vascular inflammation: the most severely affected artery dictates the score
- v0: no arteritis
- v1: intimal arteritis with < 25% luminal area lost (minimum = 1 cell, 1 artery)
- v2: intimal arteritis with ≥ 25% of luminal area lost in 1+ arteries
- v3: transmural arteritis or fibrinoid necrosis (medial smooth muscle necrosis) with lymphocyte infiltrate in vessels
- cv - transplant arteriopathy: arterial fibrointimal thickening; percentage of narrowing of lumen of most severely affected artery
- cv0: none
- cv1: ≤ 25% of the luminal area
- cv2: 26 - 50% of the luminal area
- cv3: > 50% of the luminal area
- i-IFTA and t-IFTA scored similarly to “i” and “t”, only in areas of interstitial fibrosis / tubular atrophy
- Reference: Transplantation 2018;102:1795
Images hosted on other servers:

Banff lesion scores
Microscopic (histologic) images
Contributed by Arzu Sağlam, M.D.

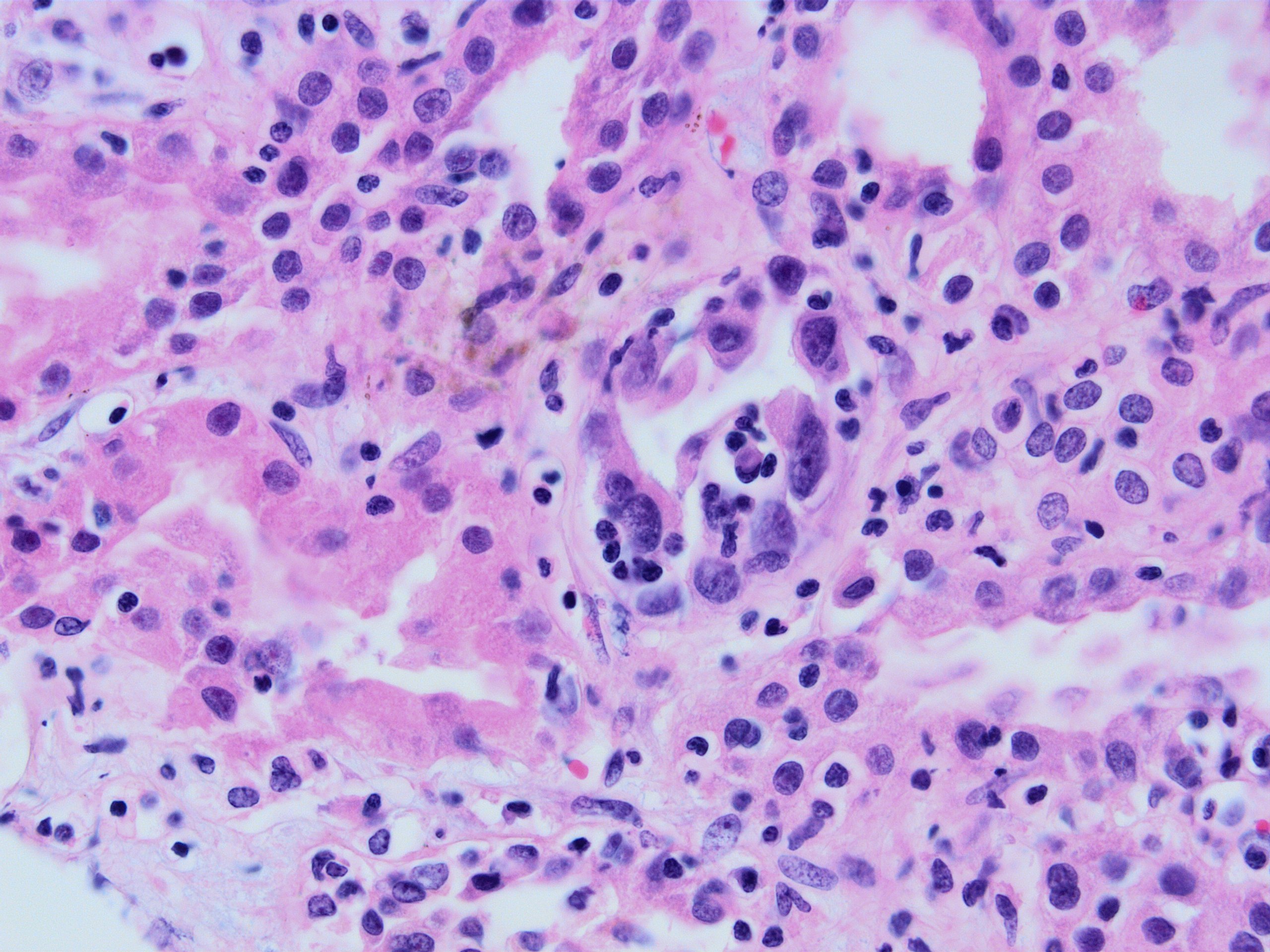
Interstitial inflammation
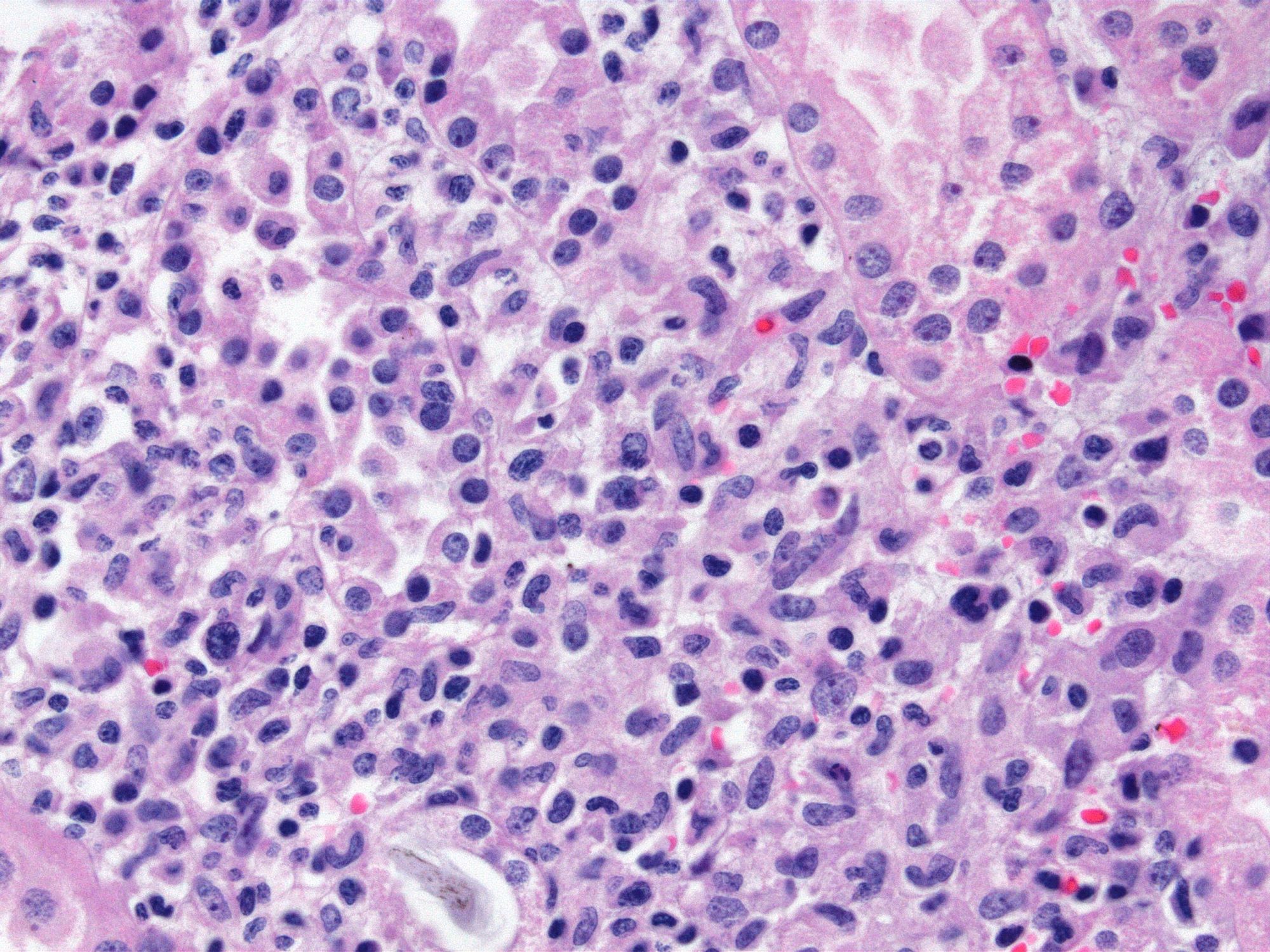
Interstitial inflammation - macrophage predominant
Tubulitis
Severe tubulitis
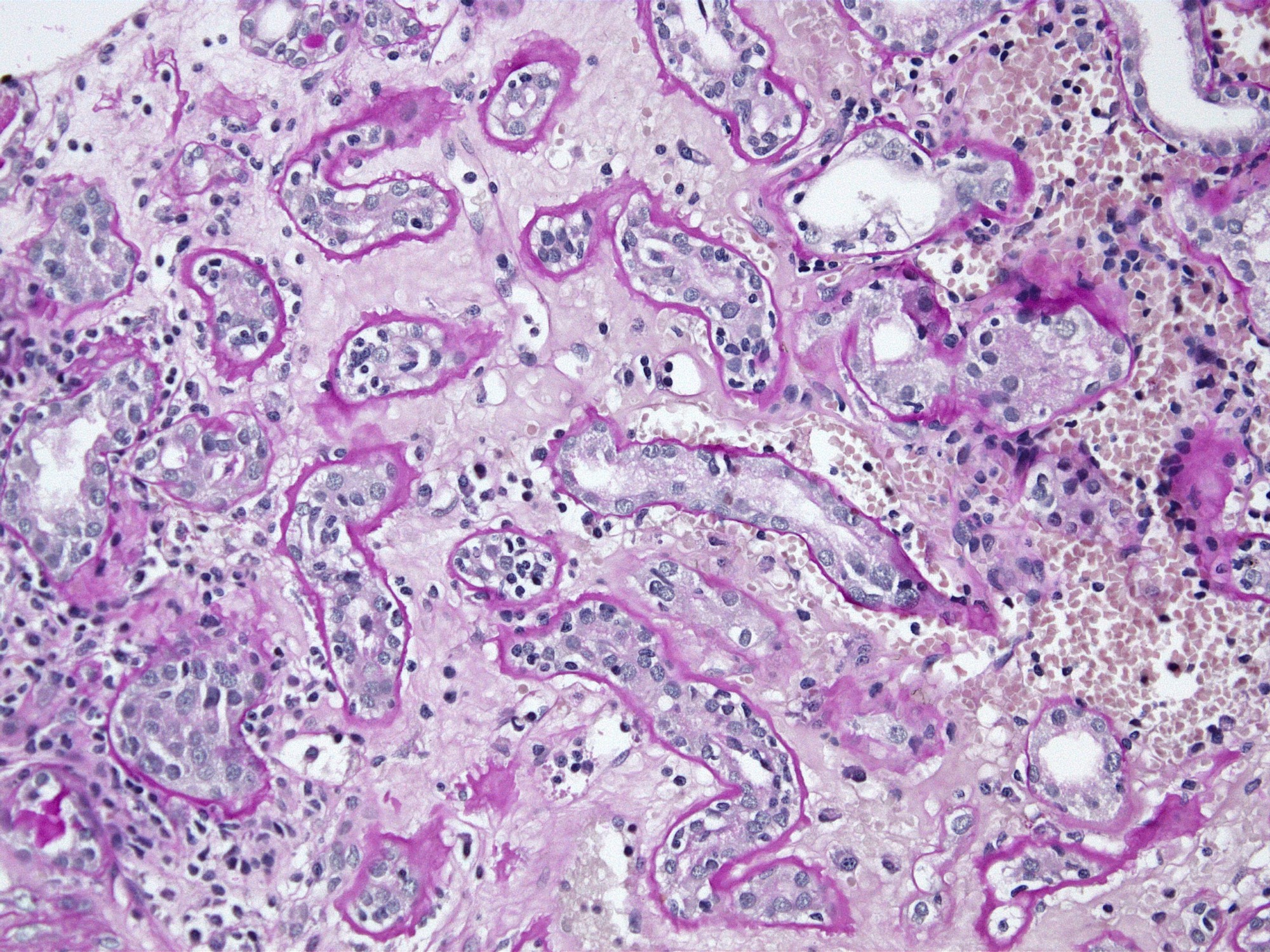
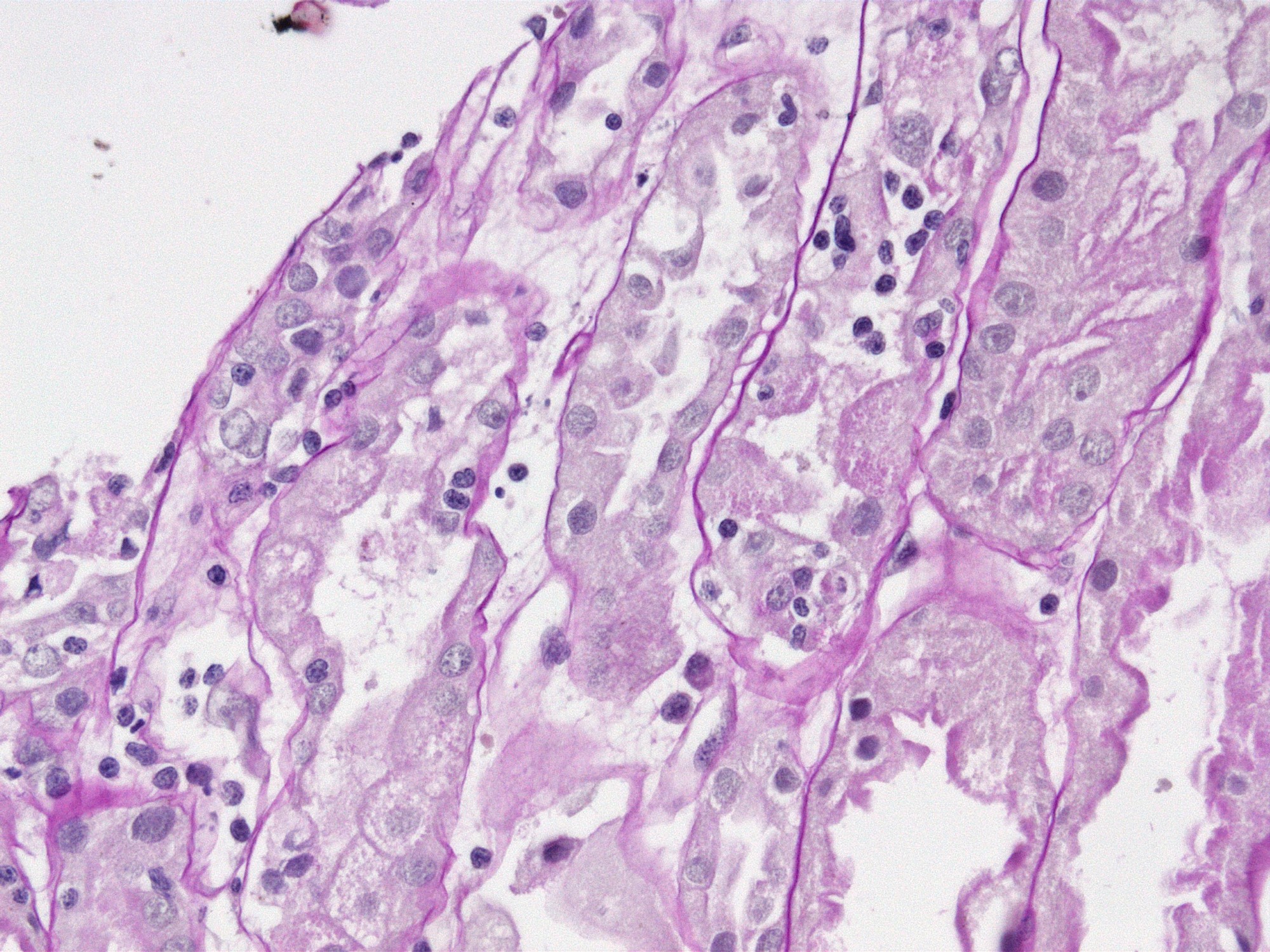
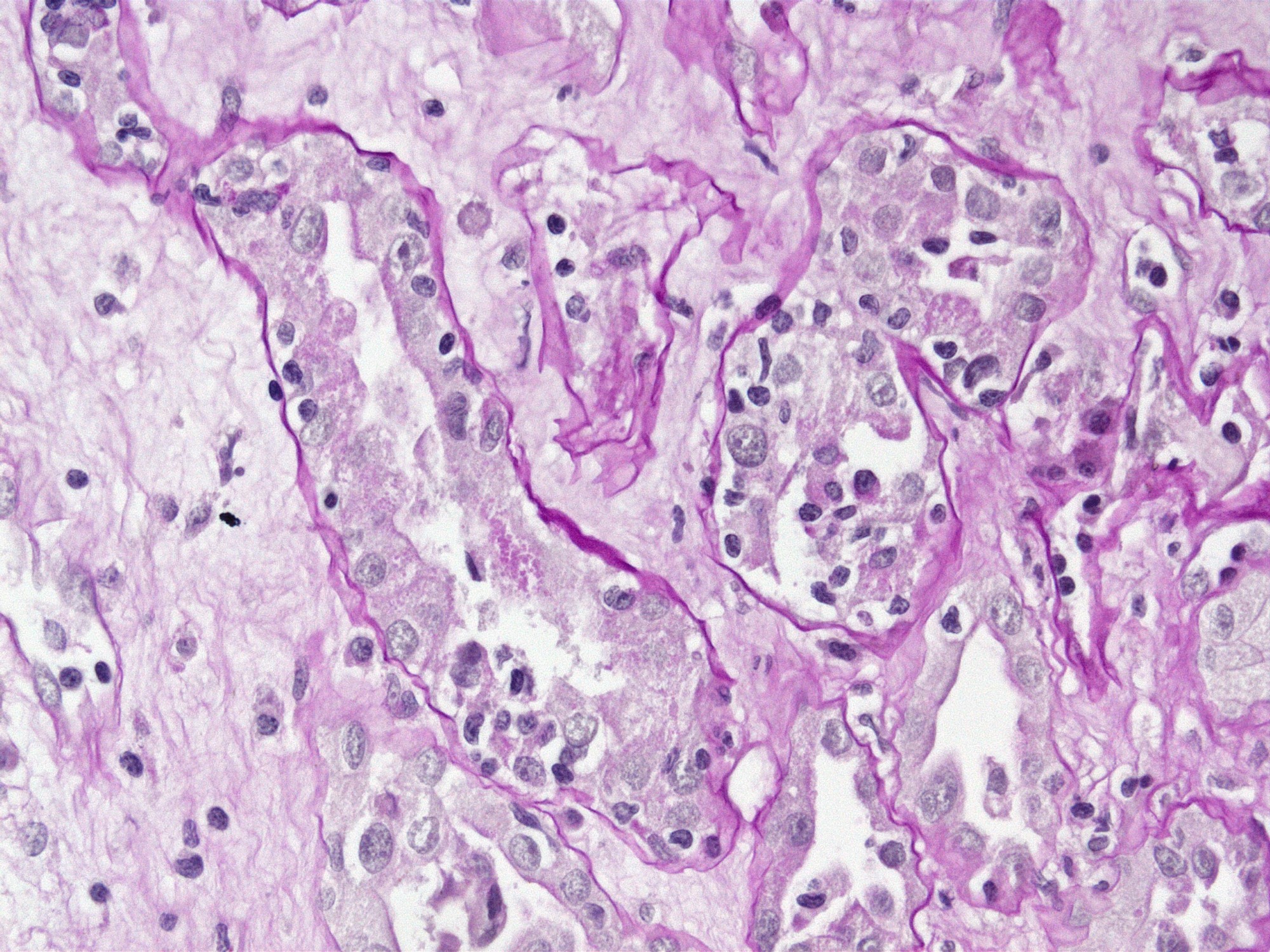
Tubulitis, PAS stain
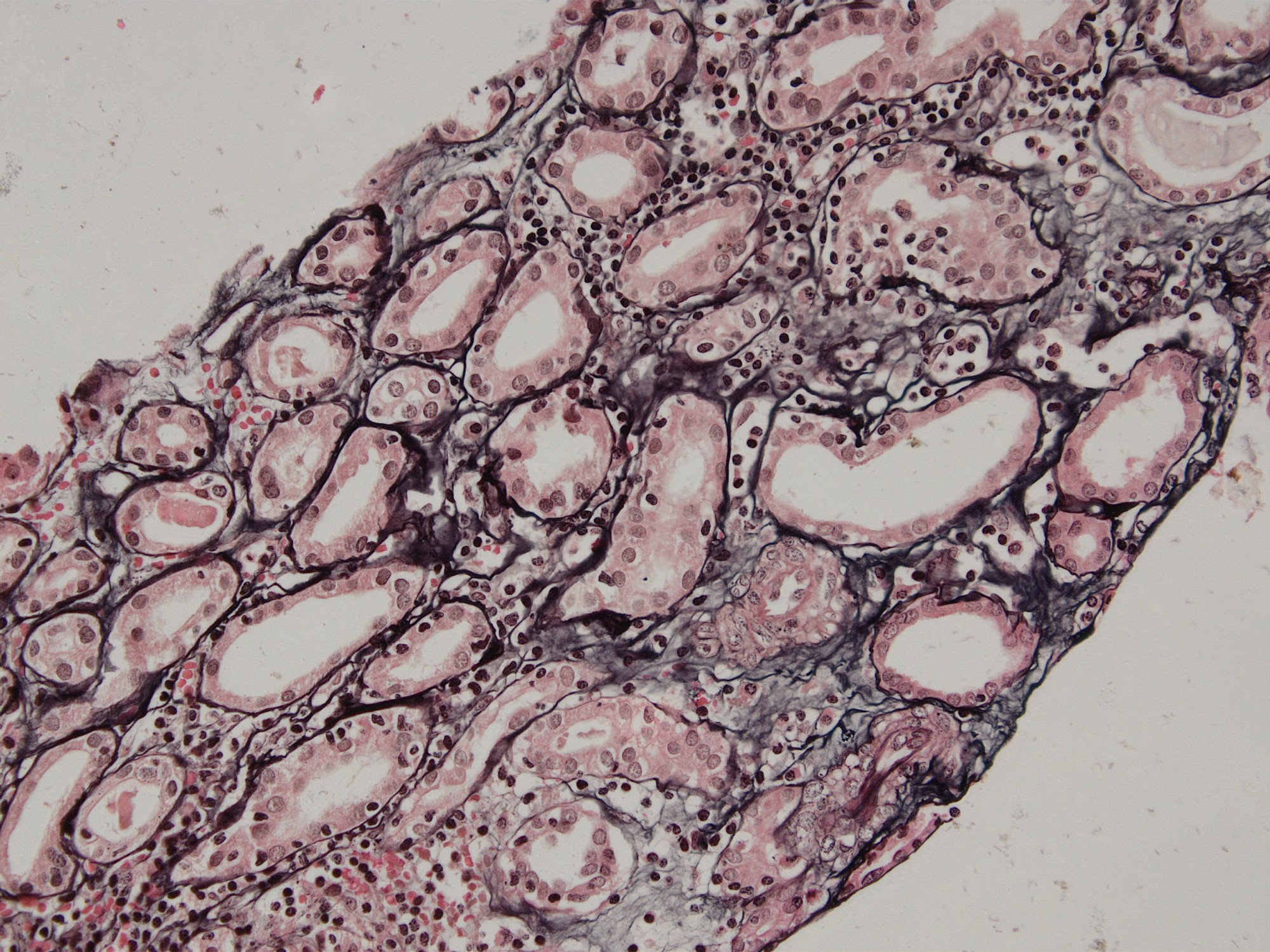
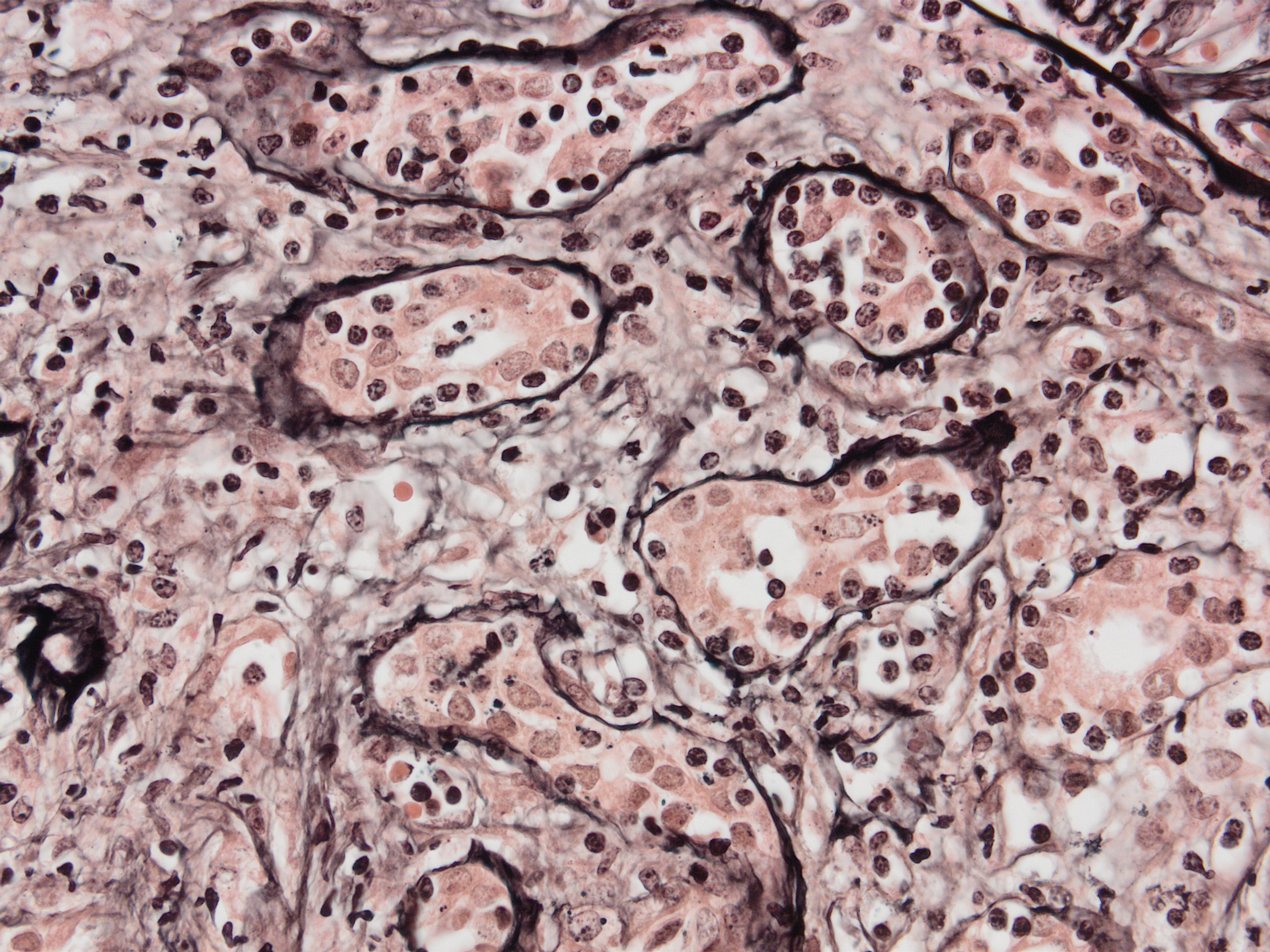
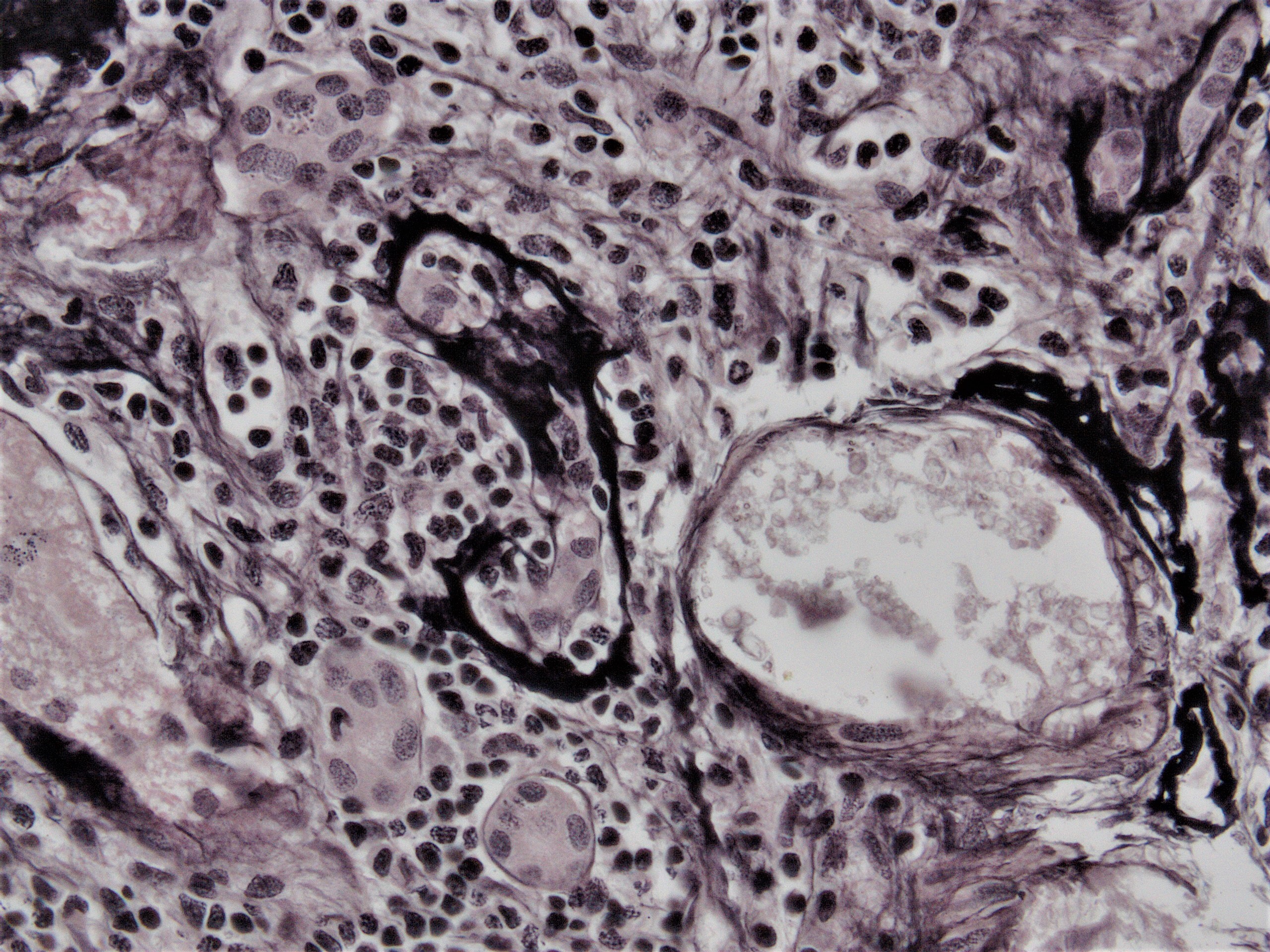
Tubulitis, JMS stain
Intimal edema and lymphocyte margination
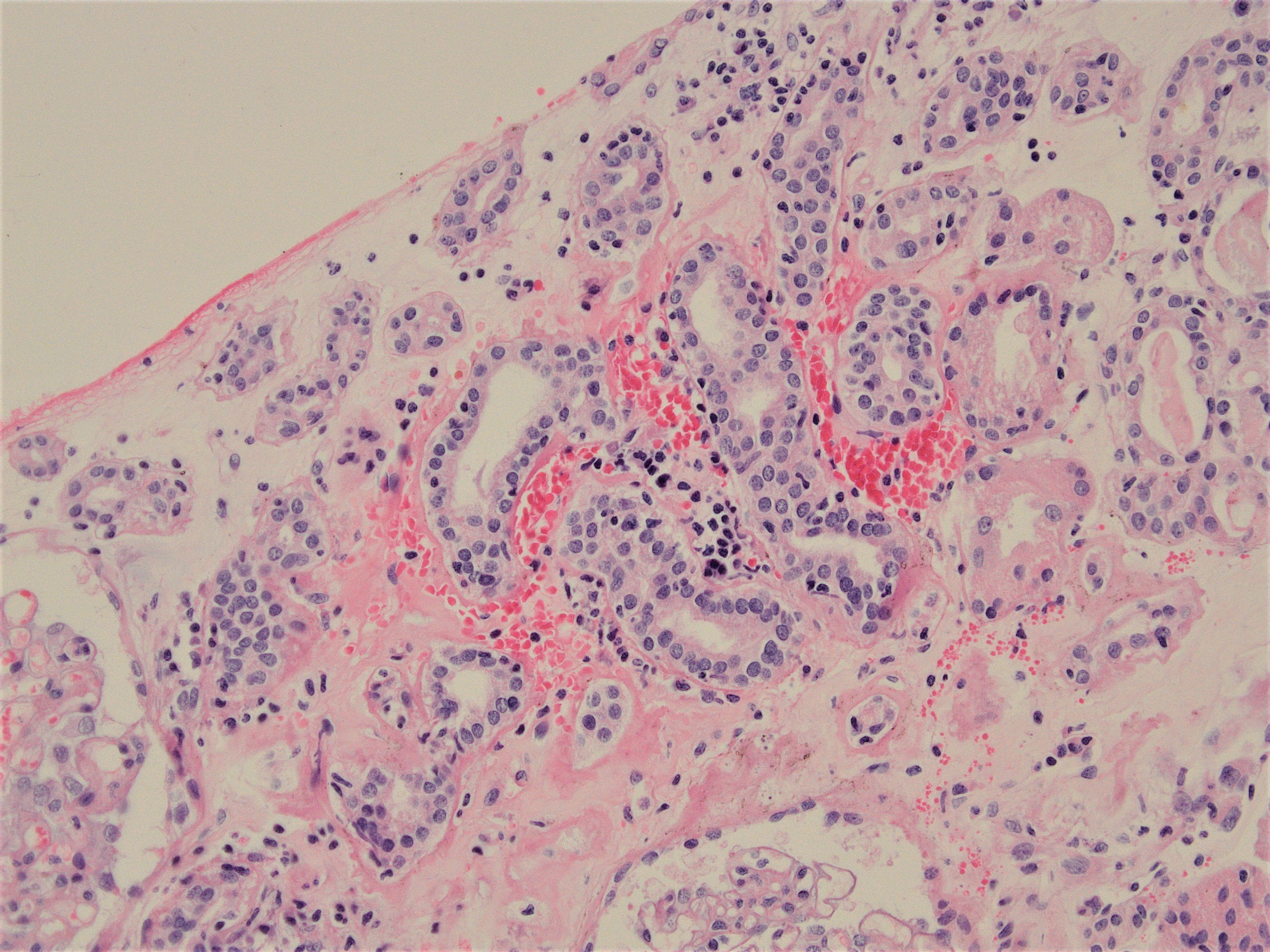
Interstitial hemorrhage
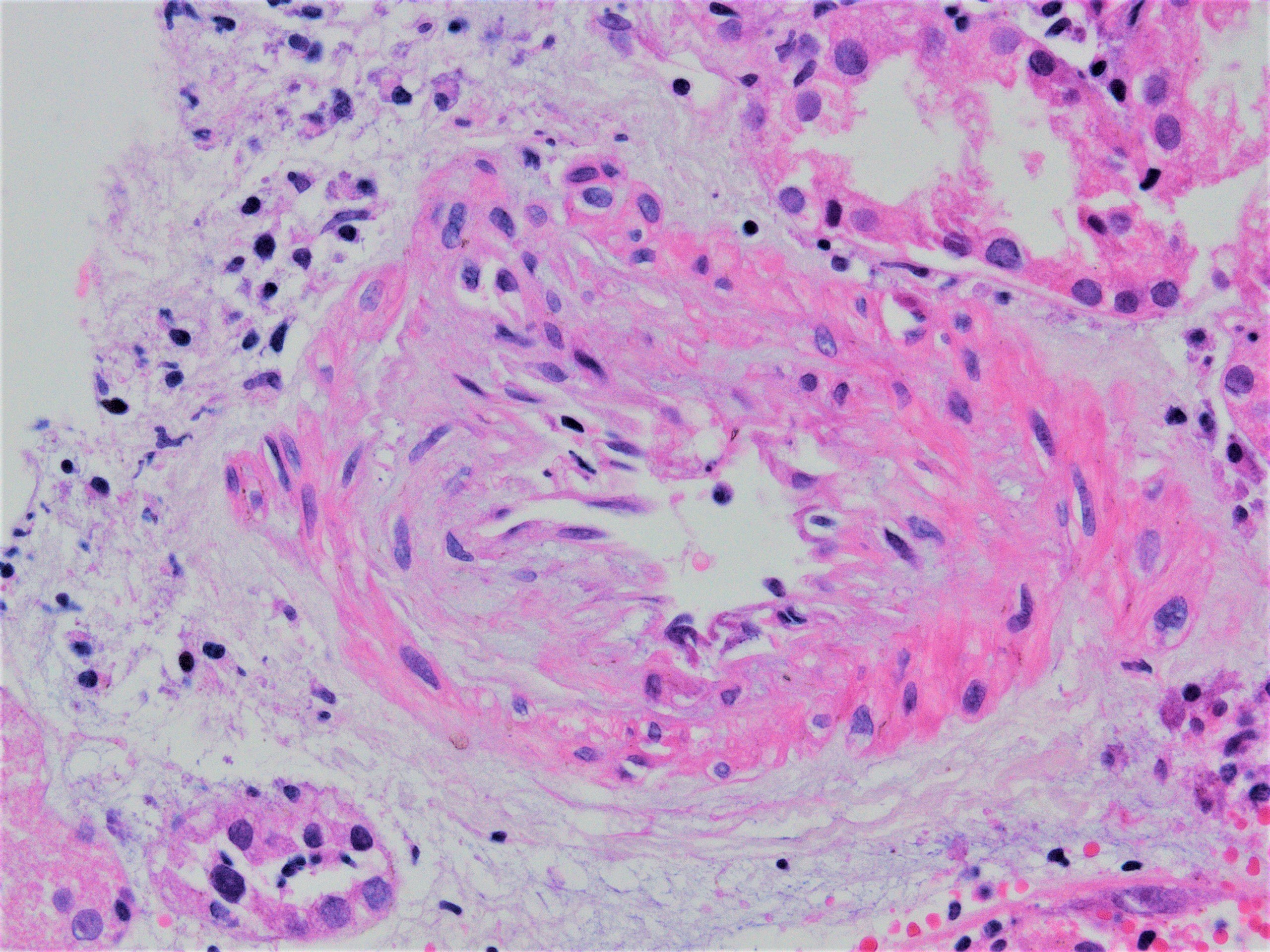
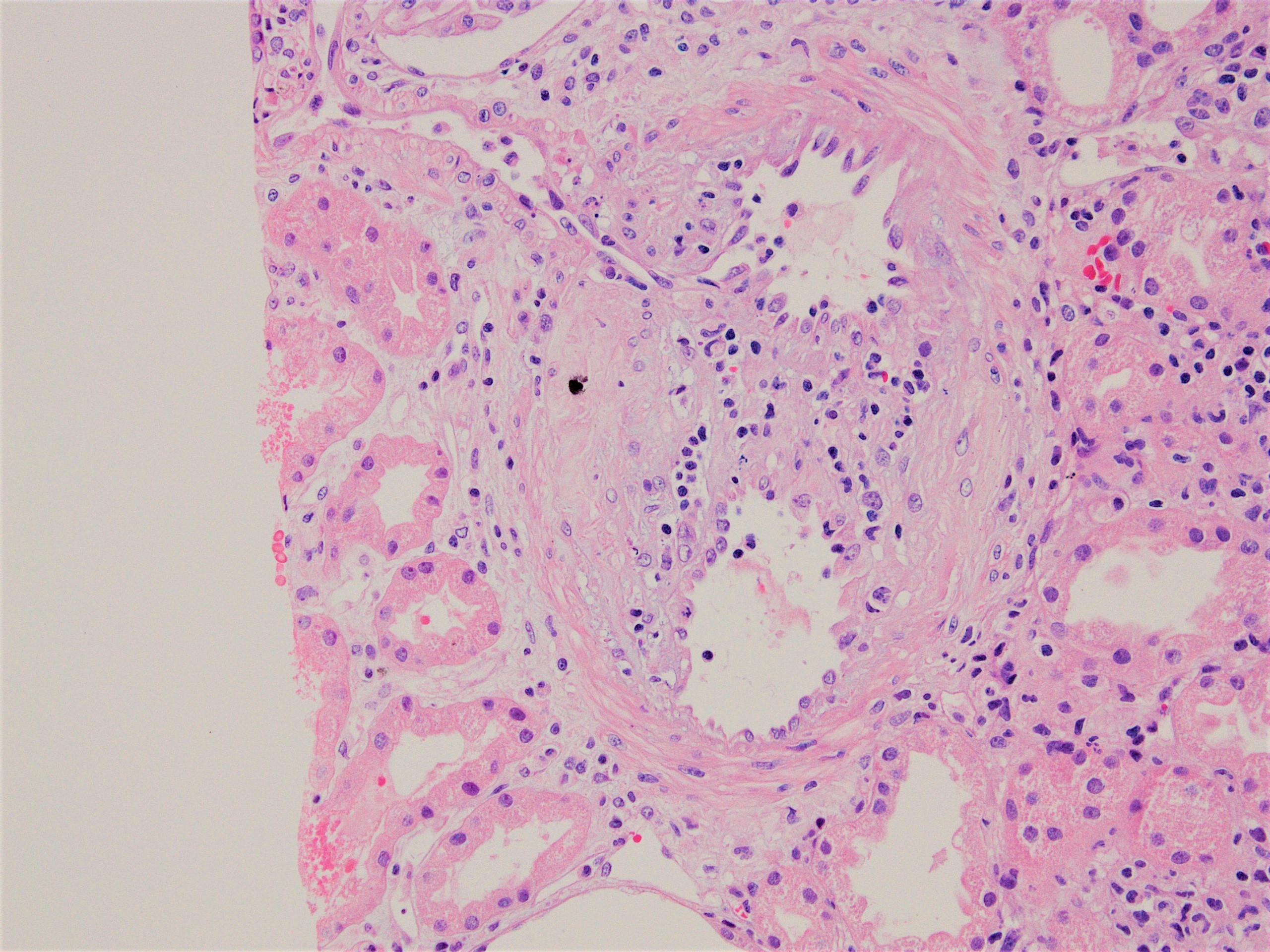
Intimal arteritis

Intimal arteritis, JMS stain
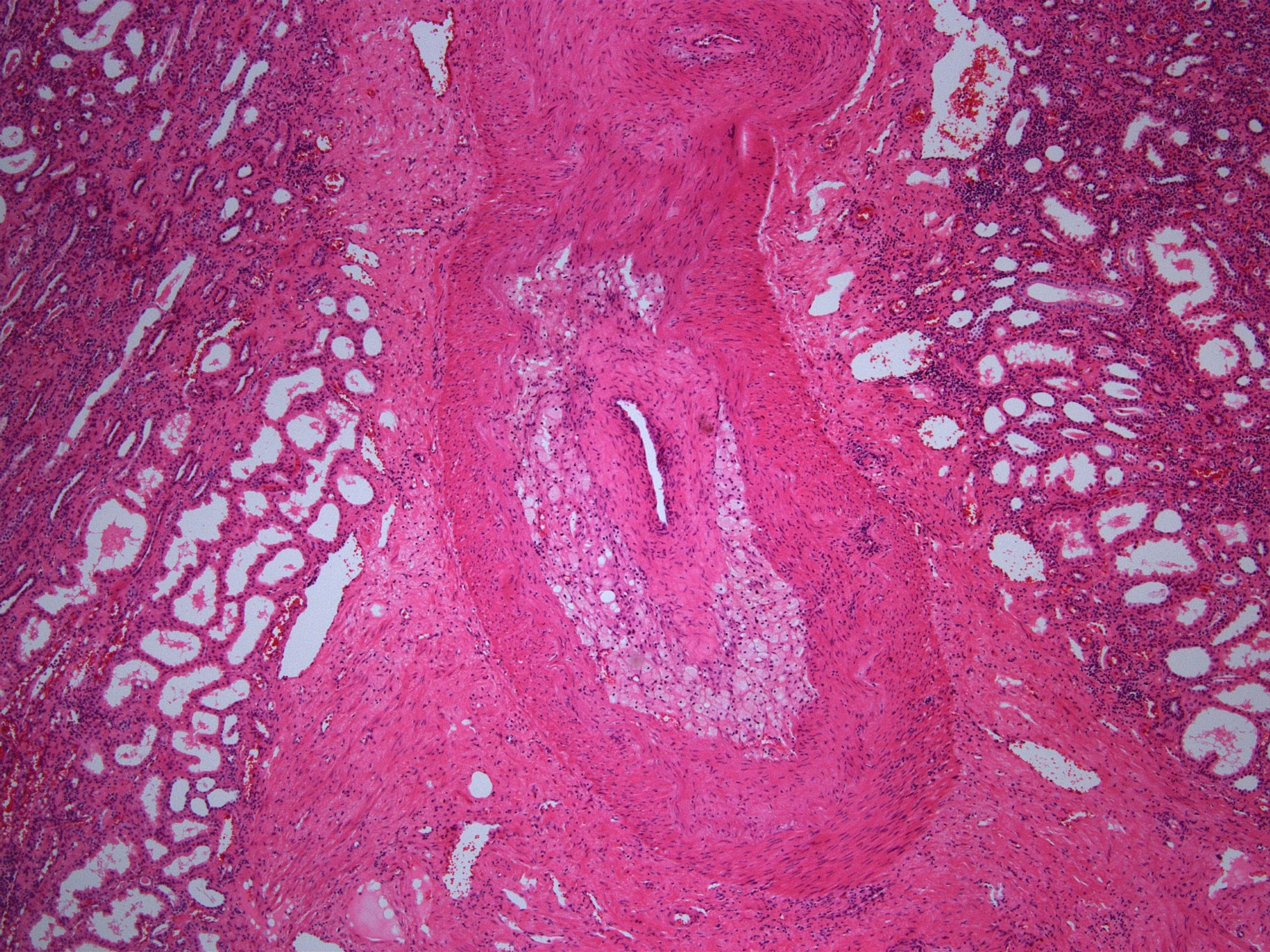
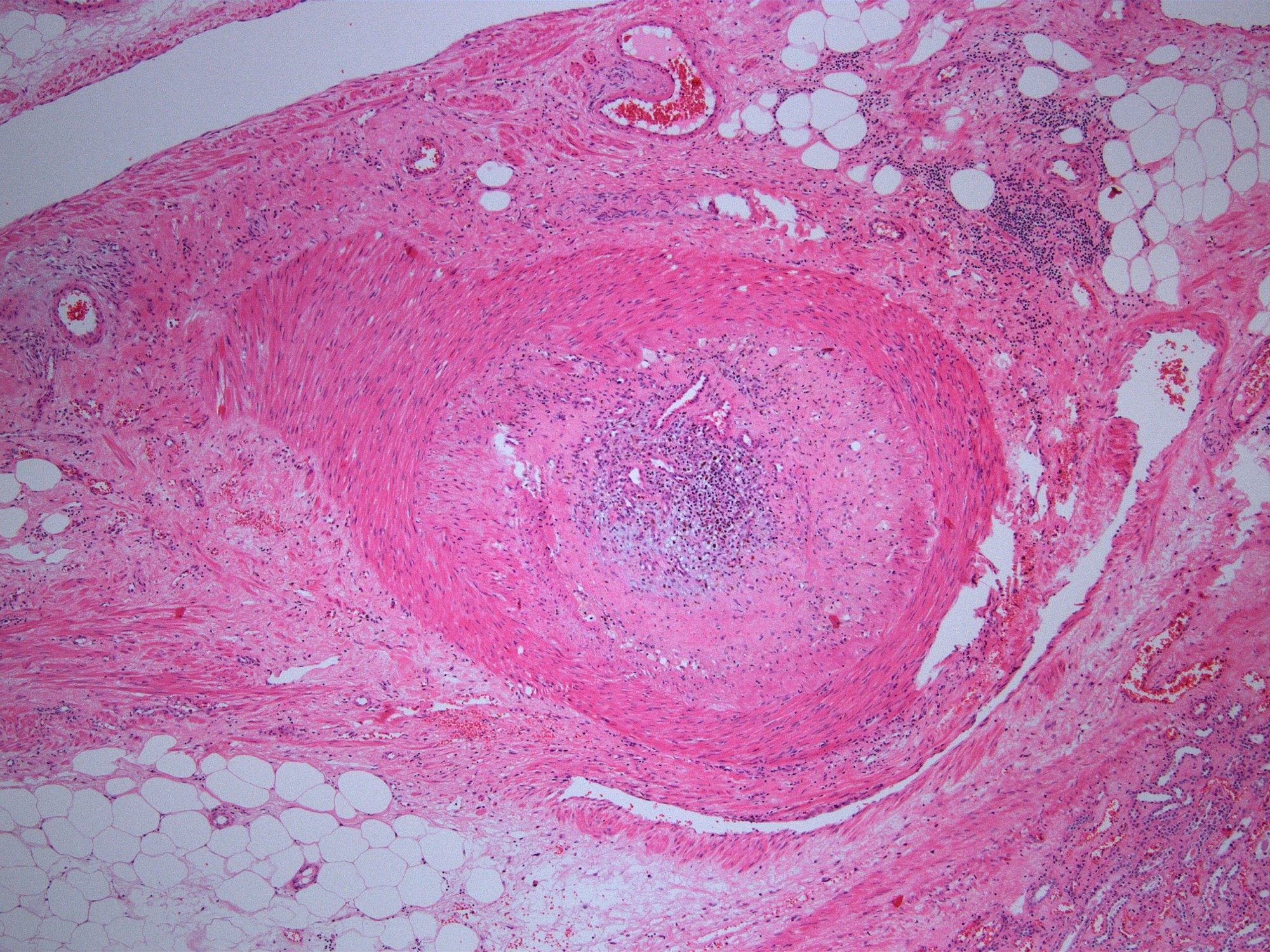
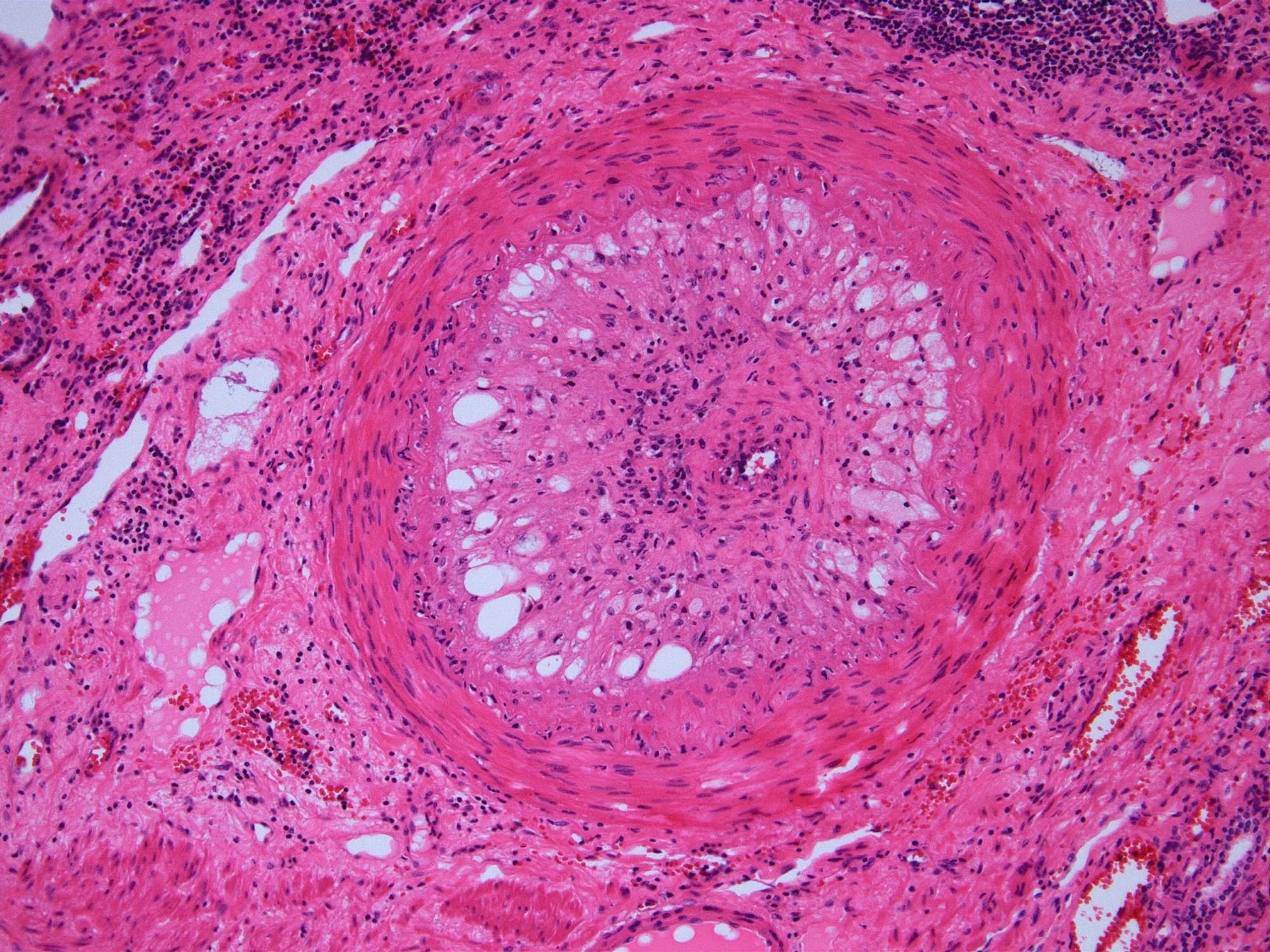
Transmural arteritis
Transmural arteritis and fibrinoid necrosis
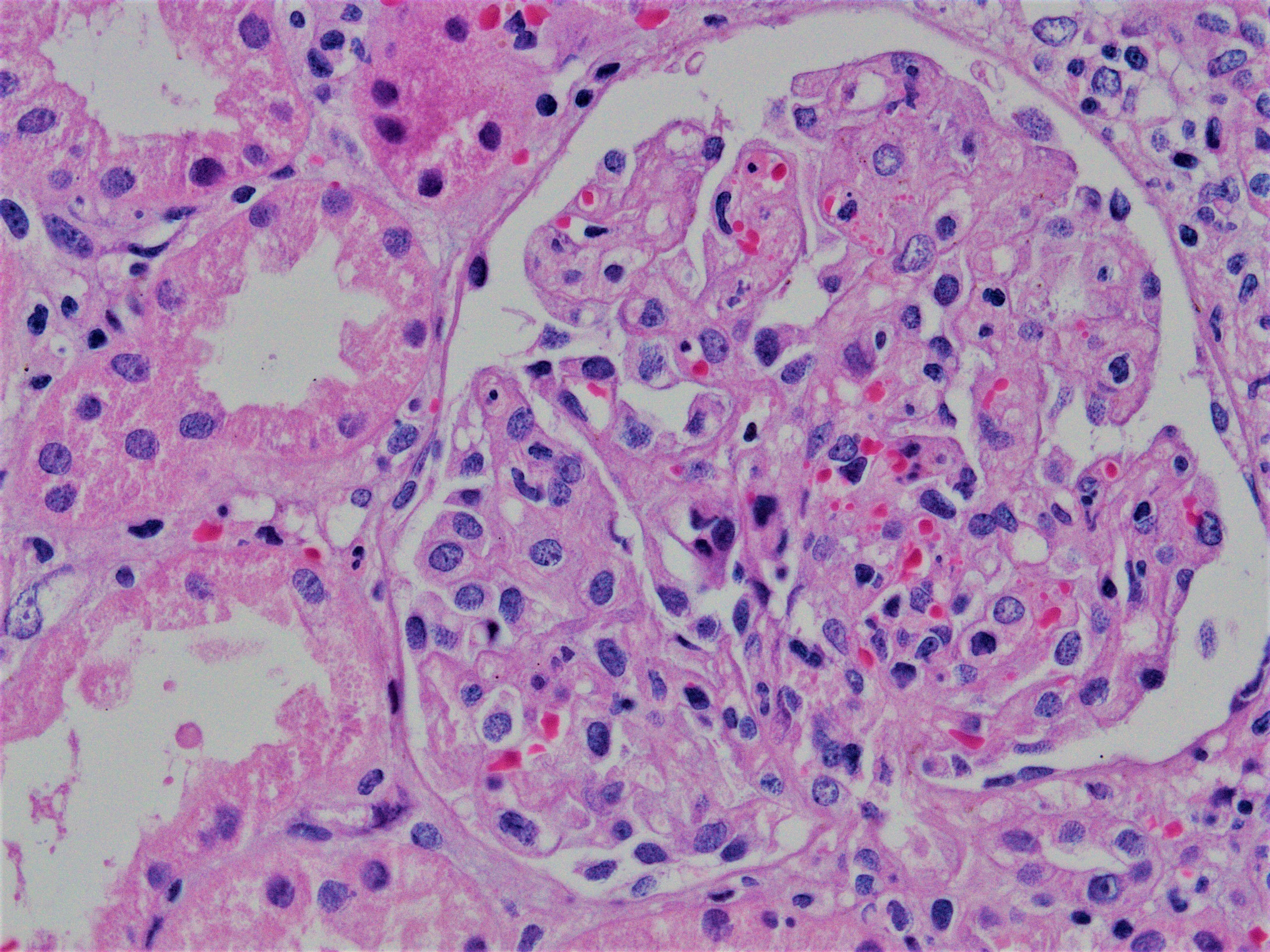
Acute allograft glomerulopathy
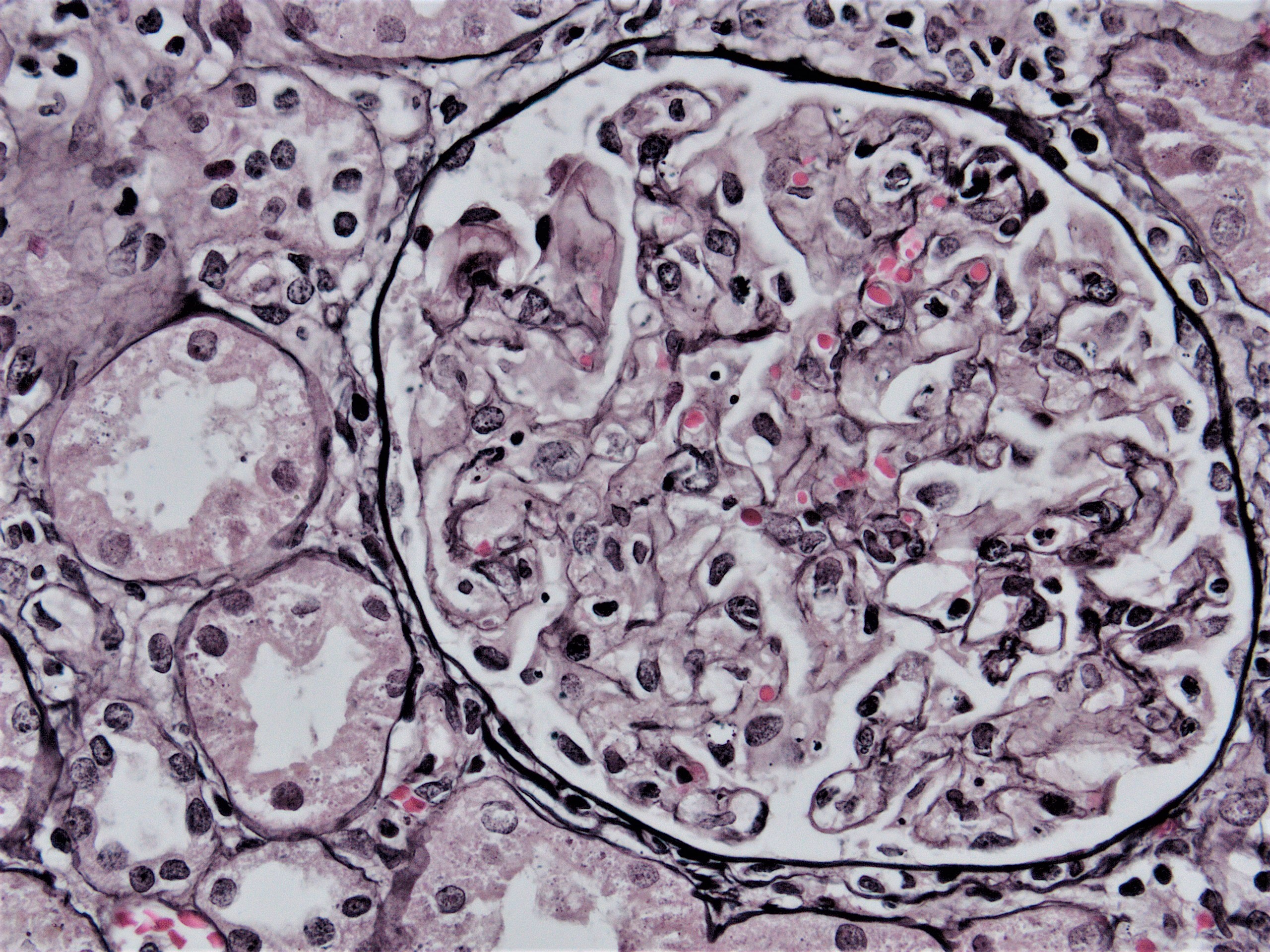
Acute allograft glomerulopathy JMS stain
Severe acute allograft glomerulopathy

i-IFTA
Tubulitis of atrophic tubuli
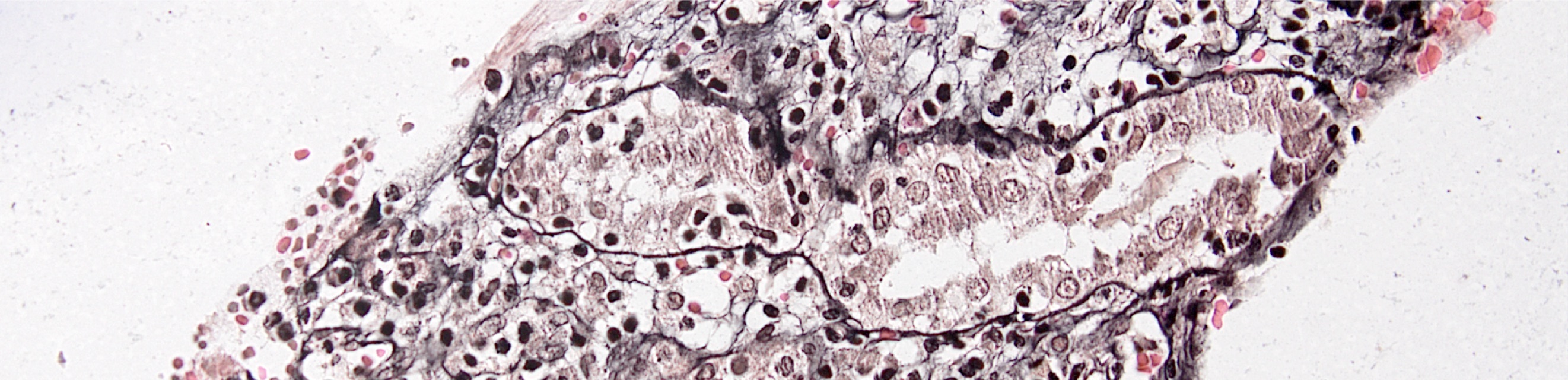
Tubulitis of atrophic tubuli, JMS stain

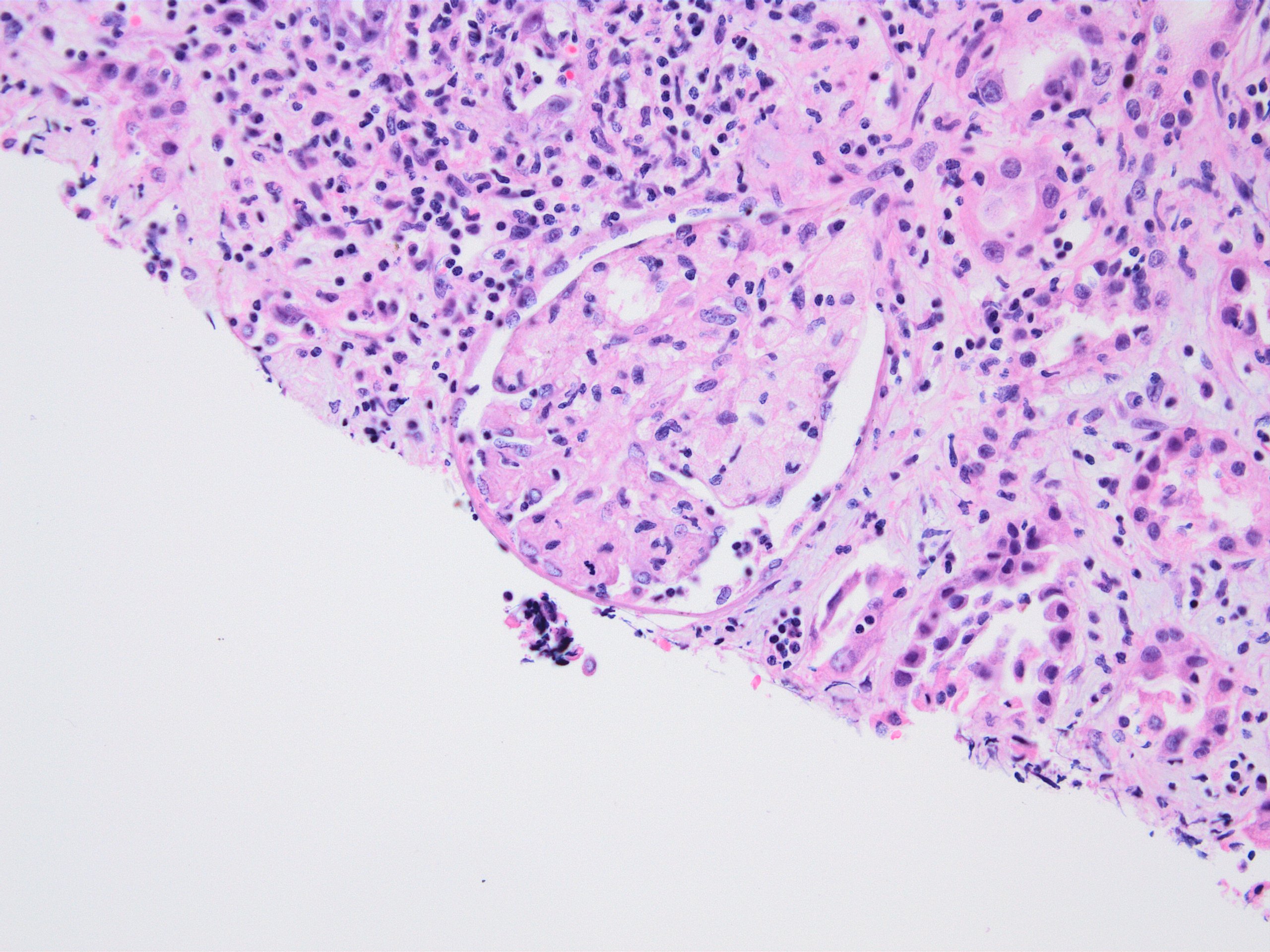
Preserved renal parenchyma
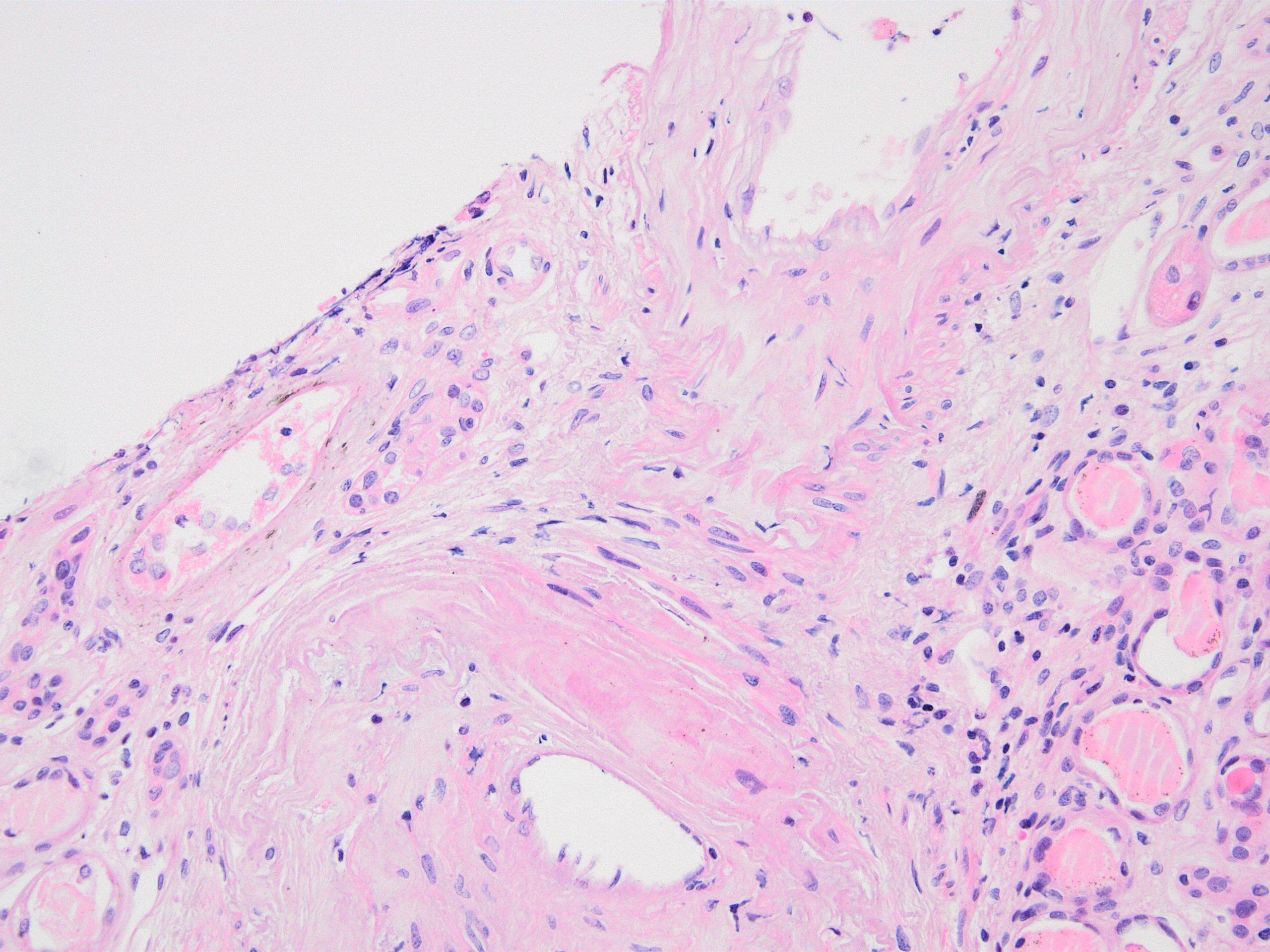
Transplant arteriopathy
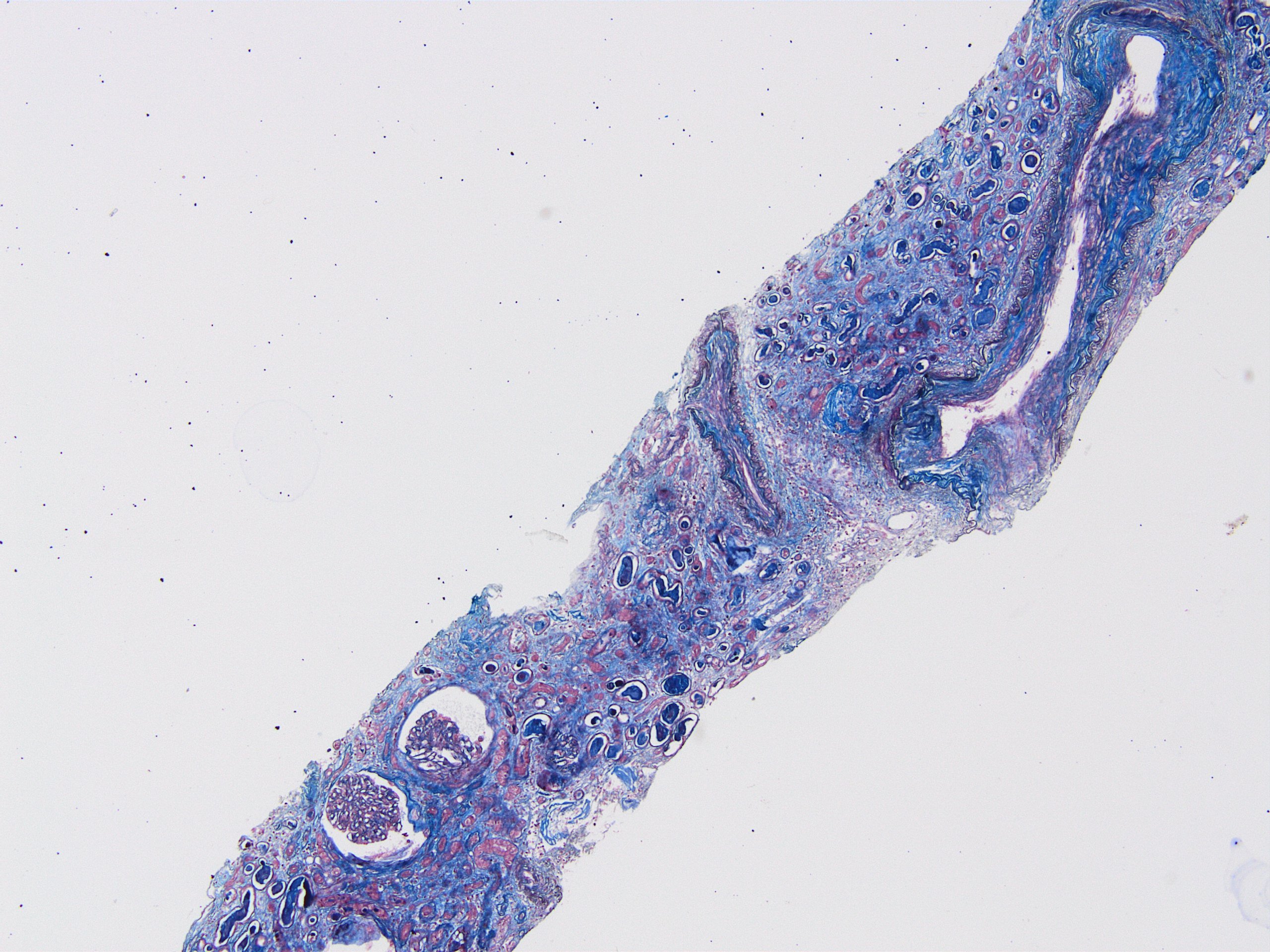
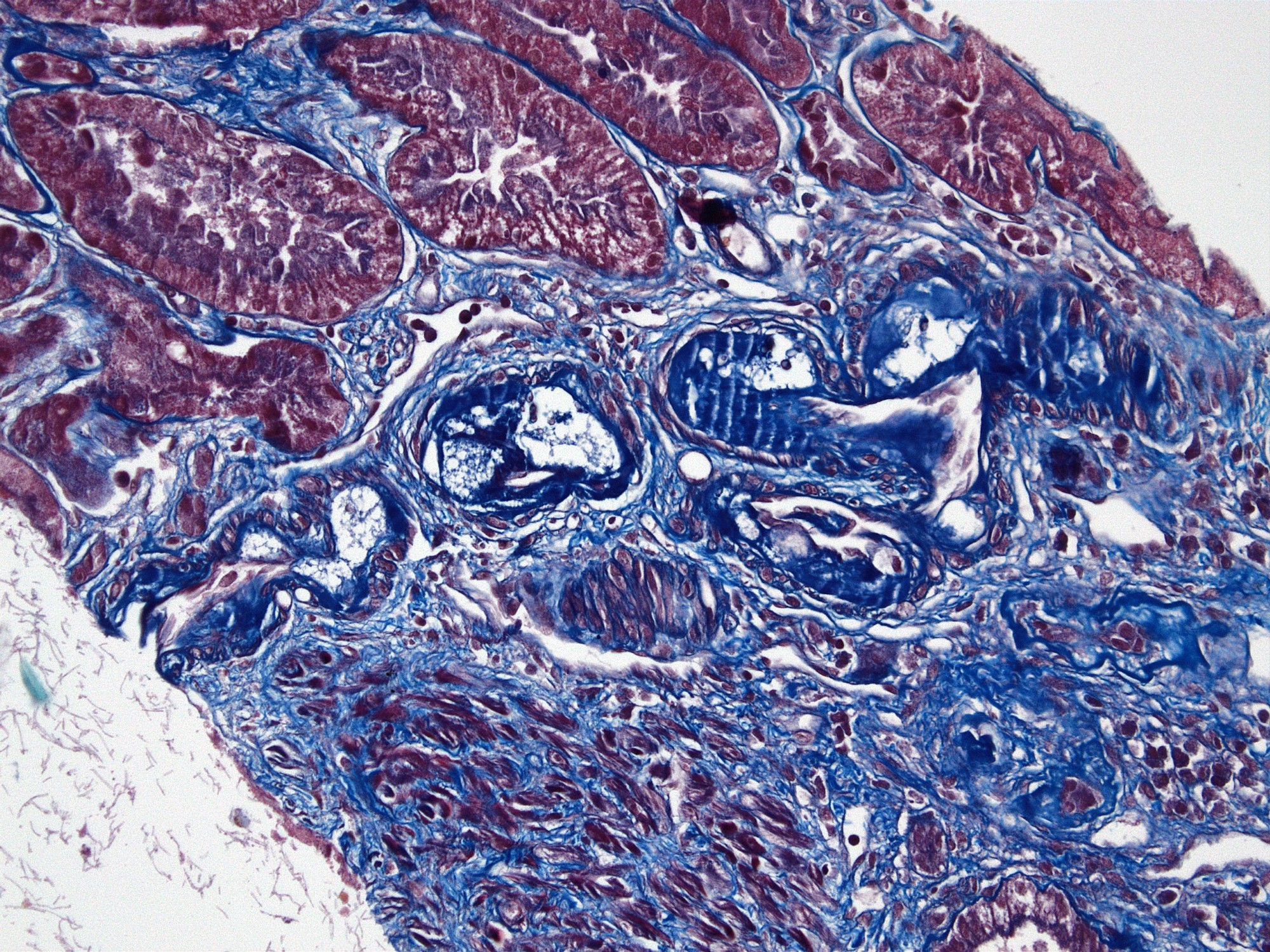
Transplant arteriopathy and IFTA, MTC stain
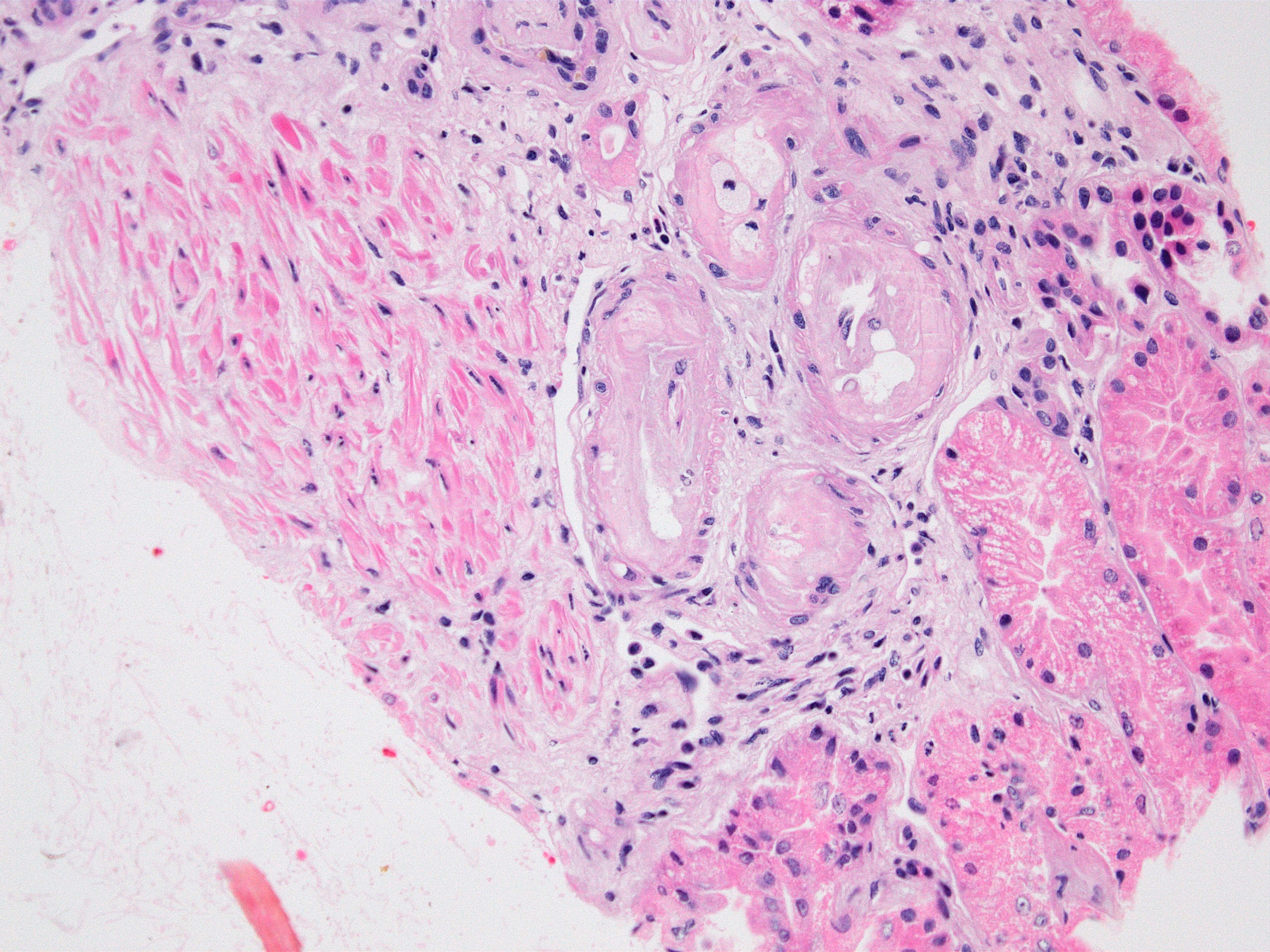
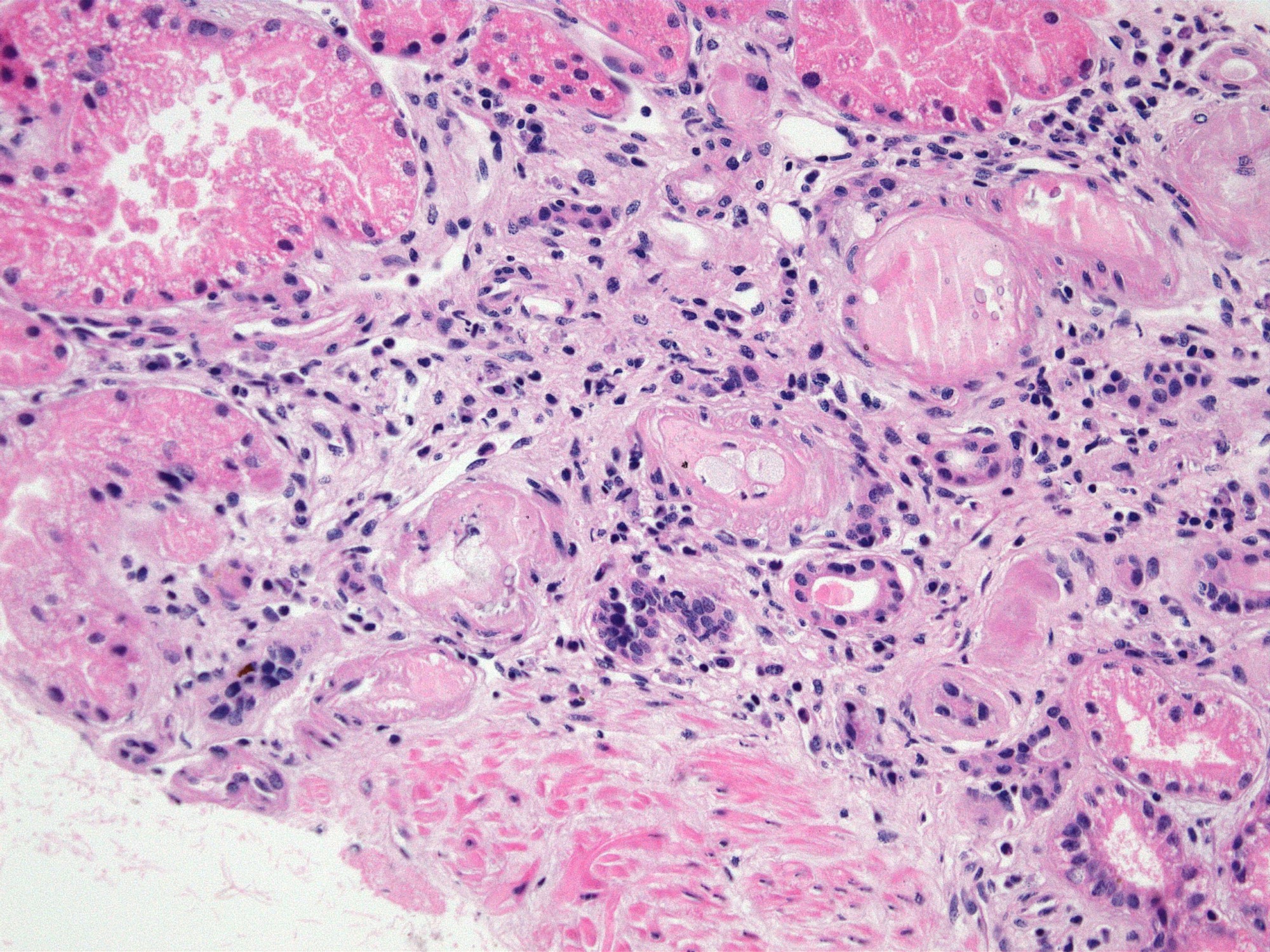
Intimal foam cells in small artery
Intimal foam cells and fibrosis in small artery, MTC
Immunofluorescence description
- No immunoglobulin or only nonspecific scarce staining
- C3 may be present along tubular basement membranes, interstitium and vessel walls
- C4d negative if not accompanied by concurrent antibody mediated rejection
Special stains
- PAS, Jones methenamine silver and periodic acid silver methenamine stains are very useful for identifying tubulitis by highlighting the basement membrane and stromal epithelial interface
- Silver and trichrome stains are useful for identifying fibrinoid necrosis
- SV40 and C4d immunohistochemistry negative
Molecular / cytogenetics description
- Genome wide expression studies in kidney transplants have identified certain sets of genes / transcripts, which correlate with T cell mediated rejection (TCMR) (BMC Nephrol 2015;16:132)
- Top molecules involved with T cell effector mechanisms: granzyme, perforin
- Top molecules involved with γ interferon effects: CXCL9, CXCL10, CXCL11
- Top molecules involved with effector / inflammatory cell recruitment: CCL5, PSMB9
- Molecular phenotype for TCMR, however, is not present amongst the criteria for TCMR in the most recent Banff classification
- A 770 gene panel encompassing genes involved in rejection, tolerance, viral infections, innate and adaptive immune responses, the Banff Human Organ Transplant Panel (B-HOT), has been made commercially available and is going to be used on the NanoString platform for research purposes (Am J Transplant 2020;20:2305)
- A simplified molecular panel will hopefully be standardized and integrated into the Banff classification criteria in the near future
Sample pathology report
- Kidney, allograft biopsy
- Microscopic description: Serial sectioning shows 37 glomeruli, 6 of which are globally sclerotic. Glomeruli appear close to normal by light microscopy. Endocapillary or extracapillary proliferation, necrosis, intracapillary inflammatory cells (g0), intracapillary thrombi or double contouring of the capillary walls are absent (cg0). İnterstitium shows multifocal edema and inflammatory infiltrate comprising 26 - 50% of the nonscarred cortical parenchyma (i2). The infiltrate is composed predominantly of mononuclear cells. Tubulitis can easily be identified, ranging from mild to severe (t3). Patchy narrow foci of IFTA can be identified, comprising about 15% of the cortical parenchyma (i-IFTA1, ci1, ct1). No significant peritubullary capillaritis is seen (ptc0). Immunohistochemical staining for C4d and SV40 is negative. Arteries display mild intimal fibrosis, arterioli show multifocal mild to moderate hyalinosis (ah2). Intimal arteritis not identified (v0).
- Immunofluorescence microscopy: 3 glomeruli observed
- Anti IgG Ab: no deposits
- Anti IgA Ab: no deposits
- Anti IgM Ab: no glomerular deposits, blush segmental reactivity on walls of arterioli
- Anti C3 Ab: no glomerular deposits, blush segmental reactivity on walls of arterioli
- Anti c1q Ab: no deposits
- Anti kappa Ab: no glomerular deposits, 2+ staining of tubular casts
- Anti lambda Ab: no glomerular deposits, 2+ staining of tubular casts
- Diagnosis: Acute T cell mediated rejection, Banff classification grade IB. Patchy interstitial fibrosis and tubular atrophy (Banff grade 1). Arterial intimal fibrosis (mild), arteriolar hyalinosis (ah2).
- Comment: Biopsy findings are consistent with mild acute T cell mediated rejection, findings suggestive of chronic damage are minimal. Vascular sclerosis is most probably donor related.
Differential diagnosis
- Acute T cell mediated rejection (TCMR):
- Acute allergic / drug induced tubulointerstitial nephritis:
- Tubulitis may be less prominent, eosinophils may be more prominent but differentiation from acute TCMR is not possible on morphologic grounds
- Active antibody mediated rejection (active ABMR):
- Inflammatory infiltrate mostly confined to lumen of peritubular capillaries, signs of microvascular endothelial cell injury (peritubular capillaritis, glomerulitis, thrombotic microangiopathy) and peritubular C4d positivity (immunofluorescence or immunohistochemistry) are present; active AMR frequently accompanies acute TCMR
- Acute pyelonephritis:
- Usually patchy inflammatory infiltrate with predominance of polymorphonuclear leucocytes, neutrophilic tubulitis and neutrophil casts within tubular lumen
- Polyomavirus infection:
- Usually patchy inflammatory infiltrate, viral cytopathic changes in tubular epithelial cells and positive polyomavirus immunostain (should be performed on every allograft renal biopsy specimen)
- Posttransplant lymphoproliferative disease (PTLD):
- Is mainly of differential diagnostic concern in cases of PTLD where inflammatory infiltrate is polymorphic; however, the presence of transformed atypical large B lymphocytes within the infiltrate is a clue to diagnosis; stains to detect EBV will help in the differential
- Acute allergic / drug induced tubulointerstitial nephritis:
- Chronic active TCMR:
- All entities that can cause chronic renal damage (chronic active antibody mediated rejection, diabetes, hypertension, medications - such as seen with chronic calcineurin inhibitor toxicity, recurrent glomerulonephritis, recurrent pyelonephritis, etc.)
- Differentiation on morphological grounds is very difficult, if not impossible
- Identification of transplant arteriopathy suggests rejection; however, this lesion is usually not represented in small needle biopsies and is a feature of chronic rejection in general (both chronic active TCMR and chronic active AMR)
Additional references
Board review style question #1
Which of the following regarding arteritis lesions in allograft transplant biopsies is correct?
- Are always characterized by fibrinoid necrosis
- Are associated with a good prognosis
- Are only associated with chronic rejection
- Can be seen in both T cell mediated and antibody mediated rejections
- Indicate mild rejection
Board review style answer #1
D. Can be seen in both T cell mediated and antibody mediated rejections
Comment Here
Reference: Acute / chronic cellular rejection
Comment Here
Reference: Acute / chronic cellular rejection
Board review style question #2
A 32 year old renal transplant patient wished to become pregnant. Her medication was adjusted accordingly. Within 2 months, her creatinine levels increased from 0.67 to 4.28 mg/dl. The biopsy sample displayed the finding shown above. What is the most probable diagnosis?
- Acute pyelonephritis
- Acute T cell mediated rejection
- Chronic active antibody mediated rejection
- Chronic active T cell mediated rejection
- Posttransplant lymphoproliferative disorder
Board review style answer #2

