

Hematology & immune disorders
Hemolytic anemia
Paroxysmal cold hemoglobinuria (PCH)
Authors: Louise Helander, M.B.B.S., Kyle Annen, D.O.
Resident / Fellow Advisory Board: Frido Bruehl, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 19 October 2023
Last staff update: 19 October 2023
Copyright: 2022-2024, PathologyOutlines.com, Inc.
PubMed Search: Paroxysmal cold hemoglobinuria

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Case reports | Treatment | Clinical images | Peripheral smear description | Sample assessment & plan | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Helander L, Annen K. Paroxysmal cold hemoglobinuria (PCH). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/hematologyPCH.html. Accessed December 21st, 2024.
Definition / general
- Acquired complement mediated intravascular hemolytic anemia due to biphasic autoantibody, usually against the P red blood cell (RBC) antigen
Essential features
- Paroxysmal cold hemoglobinuria (PCH) is an acquired complement mediated hemolytic process associated with polyclonal biphasic IgG autoantibodies against the P antigen, which bind at cold temperatures, resulting in activation of the complement cascade and intravascular hemolysis on warming to 37 °C (Hematol Oncol Clin North Am 2015;29:473)
- Most commonly seen in children < 5 years old with acute hemolysis 1 - 3 weeks after a viral or bacterial infection (Transfusion 2017;57:1332)
- Rarely seen in adults (because of the common use of antibiotics) but historically seen in association with congenital or tertiary syphilis, which causes chronic relapsing PCH (Hematol Oncol Clin North Am 2015;29:473)
- Generally transient and self limiting
Terminology
- Paroxysmal cold hemoglobinuria (PCH)
- Donath-Lansteiner hemolytic anemia
- Donath-Landsteiner test
ICD coding
Epidemiology
- Limited population data due to disease rarity
- Annual incidence estimated at 0.04 cases per 100,000 persons (Blood Adv 2023;7:2520)
- M:F ≈ 1 - 2:1 (J Clin Med 2021;10:216, Blood Adv 2023;7:2520)
- No ethnicity predilection (Lab Med 2014;45:253)
- Median age at diagnosis is 5 years old (Transfusion 2017;57:1332)
- Estimated to account for 5% in adults and associated with tertiary syphilis
- Estimated to account for up to 30% of cases of autoimmune hemolytic anemia (AIHA) in the pediatric population
Sites
- Vascular system: intravascular hemolysis (Hematol Oncol Clin North Am 2015;29:473)
- Kidneys: renal insufficiency or acute renal failure (Hematol Oncol Clin North Am 2015;29:473)
Pathophysiology
- Caused by a weak affinity biphasic autoantibody, usually IgG
- Also referred to as the Donath-Landsteiner antibody
- Reports of biphasic IgA and IgM autoantibodies (Pediatr Blood Cancer 2015;62:2044, Pediatr Int 2013;55:664)
- Autoantibodies are most commonly directed against the P red cell antigen but there have been reports of other carbohydrate antigen targets (i, I, HI, Pr) (Transfusion 2017;57:1332)
- Autoantibody most commonly forms ~1 - 3 weeks post-viral or bacterial infection (Transfusion 2017;57:1332)
- Other causes include vaccination, autoimmune disorders, hematopoietic malignancy, tertiary or congenital syphilis (historically)
- Rarely seen in adults in developed countries due to the introduction of antibiotic therapy (Hematol Oncol Clin North Am 2015;29:473)
- Mechanism of autoantibody sensitization is unknown; hypotheses include viral modification of RBC membrane, production of crossreactive antibodies or altered immune regulation (Transfusion 2017;57:1332)
- Other causes include vaccination, autoimmune disorders, hematopoietic malignancy, tertiary or congenital syphilis (historically)
- 2 phase process
- Autoantibody binds to the RBC membrane at temperatures < 37 °C
- Components of the complement cascade also bind at colder temperatures (Hematol Oncol Clin North Am 2015;29:473)
- On recirculation and rewarming to 37 °C, the autoantibody dissociates but the complement components remain bound, thus activating the terminal complement pathway with formation of the membrane attack complex on the RBC surface and resulting in intravascular RBC lysis (Hematol Oncol Clin North Am 2015;29:473)
- Free hemoglobin released during hemolytic episodes can result in acute kidney injury (Blood 2018;131:2506)
- Autoantibody binds to the RBC membrane at temperatures < 37 °C
Etiology
- More prevalent in the pediatric population
- Pediatrics: > 70% of cases post-upper respiratory tract infection (URI), viral or bacterial
- Most commonly enveloped viral infections (Transfusion 2017;57:1332)
- Also associated with gastrointestinal illness, vaccination (most common association: pneumococcal vaccination), autoimmune disorder, hematopoietic malignancy, very rarely parvovirus B19 infection (Transfusion 2017;57:1332)
- Adults: rare
- Reports of cases with non-Hodgkin lymphoma, myeloproliferative disorder and post-varicella infection (Hematol Oncol Clin North Am 2015;29:473)
- Historically, 90% of adult cases associated with tertiary syphilis, chronic relapsing form with worsening in winter (Hematol Oncol Clin North Am 2015;29:473)
- Pediatrics: > 70% of cases post-upper respiratory tract infection (URI), viral or bacterial
Clinical features
- Presentation is variable but includes some degree of intravascular hemolysis (J Clin Med 2021;10:216)
- Intravascular hemolysis at presentation can be severe, necessitating immediate intervention
- Possible symptoms include anemia, jaundice, fatigue, pallor, fever, chills, back or abdominal pain
- Most common symptom: dark urine (Blood Adv 2023;7:2520)
- Symptoms appear 1 - 3 weeks postinfection; strong relationship to viral infections in children (Transfusion 2017;57:1332)
- Symptom onset can be associated with cold exposure (e.g., outside in cold weather, air conditioning, drinking cold beverage) (J Clin Med 2021;10:216)
- Prognosis is favorable (Lab Med 2014;45:253)
- Transient, self limiting and generally does not recur
Diagnosis
- Classic presentation warrants immediate Donath-Landsteiner testing
- Hemolytic anemia in anyone under 18 years old with recent infection (viral or bacterial) (Immun Ageing 2020;17:38)
- Hemolysis may be sudden and severe
- New onset Coca-Cola colored urine reported
- Direct antiglobulin test (DAT) negative for IgG, positive for complement (most commonly)
- Hemolytic anemia in anyone under 18 years old with recent infection (viral or bacterial) (Immun Ageing 2020;17:38)
- Presence of Donath-Landsteiner antibody is pathognomonic
Laboratory
- Labs indicating hemolysis (Immun Ageing 2020;17:38)
- Increased indirect (unconjugated) bilirubin
- Low / absent haptoglobin
- Elevated lactate dehydrogenase
- Increased urinary urobilogen
- Hemosiderin in urine ~1 week after start of hemolysis
- Organ damage resulting from acute hemolysis (Hematol Oncol Clin North Am 2015;29:473)
- Relative reticulocytopenia is possible despite significant anemia; more common in children (Transfusion 2017;57:1332)
- May reflect sudden severity of hemolysis and cause depletion of reticulocytes in marrow pool
- Reticulocytes may be a target of the autoantibody
- Reticulocytopenia is not considered a poor prognostic sign in children with PCH as in adult populations with AIHA; children normally recover in 1 - 4 weeks
- May reflect sudden severity of hemolysis and cause depletion of reticulocytes in marrow pool
- Direct Coombs / DAT test is negative for IgG and positive for C3 (Clin Exp Rheumatol 2015;33:588)
- 5 - 10% of AIHA cases do not have a positive DAT (Immun Ageing 2020;17:38)
- Absence of warm autoantibodies (Transfusion 2017;57:1332)
- Positive Donath-Landsteiner test: in vitro test to measure biphasic hemolysins with anti-P specificity (Hematol Oncol Clin North Am 2015;29:473)
- Sample is required to be collected and maintained at 37 °C during transport
- Sample must be collected in tubes with no anticoagulant (red top Vacutainer)
- Can result in false negative results due to incorrect specimen handling or transient nature of the autoantibody
- Antibody titers are highest during periods of clinical hemolysis
Case reports
- 15 month old boy presented with an upper respiratory infection and sudden onset of pallor with dark urine (J Pediatr Hematol Oncol 2022;44:60)
- 23 month old girl and 4 year old girl both admitted to the hospital with acute hemolytic anemia following upper respiratory infections and otitis media in the weeks prior (Lab Med 2014;45:253)
- 4 year old boy presented with presumed viral infection and sudden onset severe hemolysis successfully treated with eculizumab therapy (Blood Adv 2019;3:3575)
- 18 year old woman in early pregnancy with acute hemolytic anemia was found to be D - L antibody positive (BMC Hematol 2015:15:3)
- 27 year old woman presented with cough and acute hemolytic anemia leading to acute kidney injury and oliguric renal failure requiring hemodialysis (Blood 2018;131:2506)
Treatment
- Supportive care: transient, self limiting disease (Transfusion 2017;57:1332)
- Warm ambient temperature
- Blood transfusions as necessary
- Hemoglobin frequently falls below 6 g/dL during active hemolysis (Blood Adv 2019;3:3575)
- P antigen negative blood is not necessary for support; only considered in refractory hemolysis despite supportive measures (Clin Exp Rheumatol 2015;33:588)
- P antigen negative RBC units are rare and difficult to find due to the high prevalence of P antigen in the population
- P antigen negative blood is not necessary for support; only considered in refractory hemolysis despite supportive measures (Clin Exp Rheumatol 2015;33:588)
- Iron, folate and B12 supplementation to support hematopoiesis if deemed necessary (Immun Ageing 2020;17:38)
- Hemoglobin frequently falls below 6 g/dL during active hemolysis (Blood Adv 2019;3:3575)
- Corticosteroid treatment is common but efficacy is unclear (J Clin Med 2021;10:216, Blood Adv 2023;7:2520)
- Chronic, refractory or recurrent cases: corticosteroids, intravenous immunoglobulin, rituximab and eculizumab have all been used with limited efficacy (Indian J Pathol Microbiol 2021;64:613)
- Plasmapheresis can help clear antibody in severe hemolytic or refractory cases (Clin Exp Rheumatol 2015;33:588)
- Treat the underlying condition: syphilis related PCH resolves with curative antibiotic therapy for syphilis (Hematol Oncol Clin North Am 2015;29:473)
Clinical images
Contributed by Samantha Mack, M.D.

Donath-Landsteiner
assay interpretation
worksheet
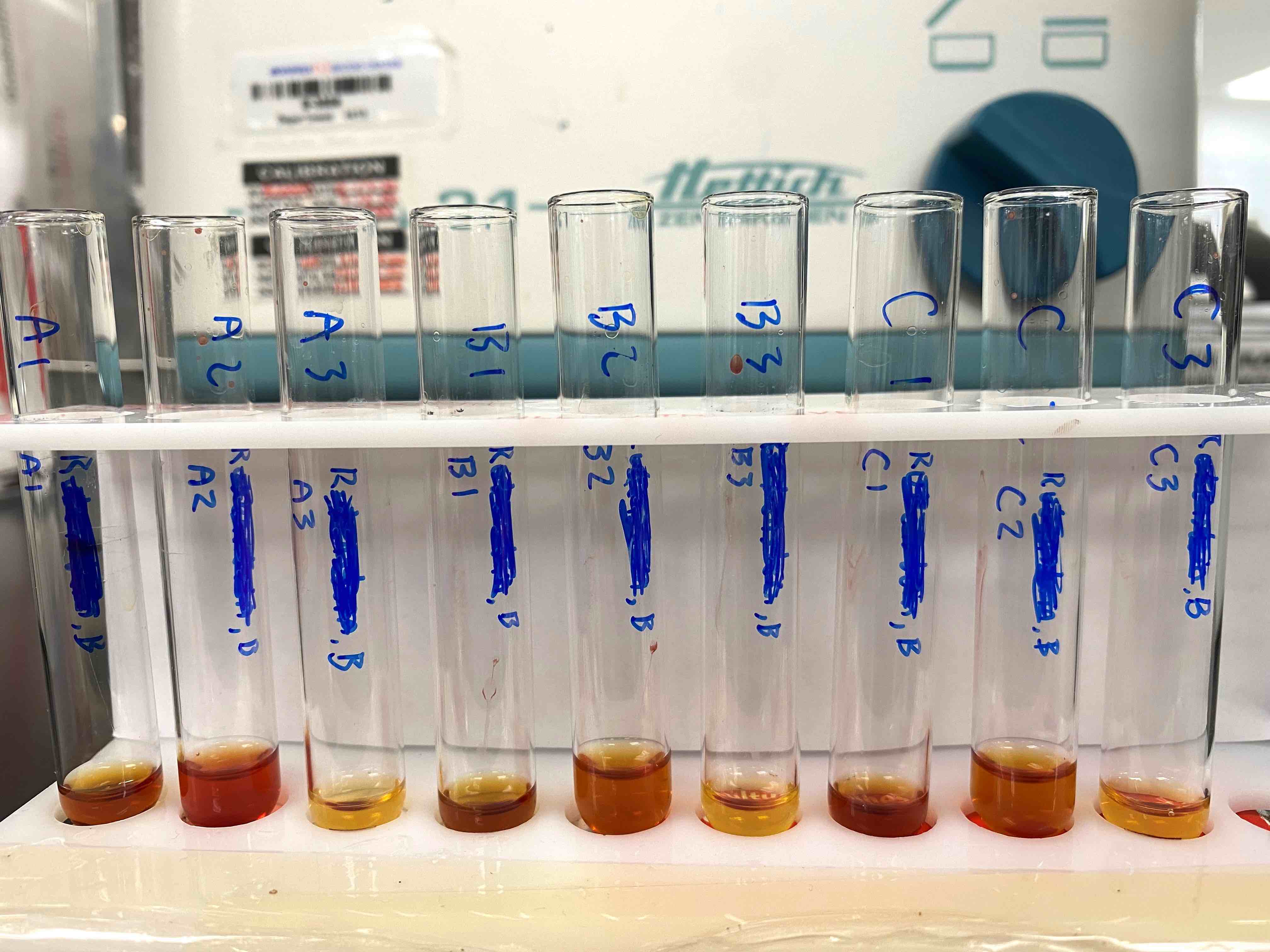
Donath-Landsteiner tube assay example
Peripheral smear description
- Peripheral smear may show (Transfusion 2017;57:1332)
- Evidence of hemolysis: spherocytosis (50% of cases), autoagglutination / rouleaux formation (17 - 25% of cases)
- Bone marrow compensation: polychromasia (if reticulocytosis present)
- Neutrophil erythrophagocytosis and neutrophil rossettes, while rare, are strongly associated with PCH (Hematol Oncol Clin North Am 2015;29:473, Blood 2020;135:393)
Sample assessment & plan
- Assessment: Johnny is a 5 year old boy who presented with 1 week of symptoms consistent with an upper respiratory infection (cough, fever, congestion), anemia and new onset hemoglobinuria. Send out testing identified the presence of a biphasic antibody (Donath-Landsteiner antibody).
- Plan: The patient presentation and laboratory workup are consistent with a diagnosis of paroxysmal cold hemoglobinuria.
- Transfuse pRBCs as clinically indicated. A blood warmer is recommended.
- Recommend patient avoid cold climates while antibody is present.
- No special transfusion requirements or precautions.
Differential diagnosis
- Autoimmune hemolytic anemia (AIHA) (Immun Ageing 2020;17:38):
- Mixed autoimmune hemolytic anemia (J Clin Med 2021;10:216):
- Cold agglutinin syndrome (CAS) (Immun Ageing 2020;17:38):
- Presents similarly to PCH with intravascular hemolysis precipitated by recent infection (Mycoplasma pneumoniae or Epstein-Barr virus most frequently)
- DAT positive for C3 but high titer IgM autoantibody with anti-Ia specificity
- Cold agglutinin titer positive
- Symptoms of both intravascular and extravascular hemolysis
Additional references
Board review style question #1
Which of the following is considered the definitive test for diagnosis of paroxysmal cold hemoglobinuria (PCH)?
- Bone marrow biopsy
- Coombs test
- Donath-Landsteiner test
- Flow cytometry
Board review style answer #1
C. Donath-Landsteiner test. The Donath-Landsteiner test, an in vitro test to measure biphasic hemolysins with anti-P specificity, is positive in cases of PCH. Answer A is incorrect because bone marrow biopsy could range from normal to evidence of bone marrow compensation (e.g., erythroid hyperplasia) due to hemolysis in a patient with PCH. Erythroid hyperplasia is a nonspecific sign that can be seen in many disease states where hemolysis or anemia are present. Answer B is incorrect because the direct antiglobulin (Coombs) test is a nonspecific test. Both positive and negative results can be seen in a wide variety of disease states and it does not definitively define PCH. Answer D is incorrect because unlike paroxysmal nocturnal hemoglobinuria, there are no specific flow cytometry markers associated with PCH.
Comment Here
Reference: Paroxysmal cold hemoglobinuria (PCH)
Comment Here
Reference: Paroxysmal cold hemoglobinuria (PCH)
Board review style question #2
Which red cell antigen is the biphasic Donath-Landsteiner autoantibody usually reactive against?
- A antigen
- I antigen
- O antigen
- P antigen
Board review style answer #2
D. P antigen. The P antigen is a part of the globoside blood group system. It is a receptor for parvovirus B19 and some forms of E. coli. Antibodies to the P antigen have a known association with paroxysmal cold hemoglobinuria (PCH). Answers A and C are incorrect because blood group antigens A and O (the absence of blood group antigens A and B) have no known association with PCH. Answer B is incorrect because I antigens occur at the branching points of type II oligosaccharide chains. Decreased I antigen expression is associated with some leukemias. There is no known association with PCH.
Comment Here
Reference: Paroxysmal cold hemoglobinuria (PCH)
Comment Here
Reference: Paroxysmal cold hemoglobinuria (PCH)

