

Heart & vascular pathology
Benign tumors / other nonneoplastic
Cardiac myxoma
Resident / Fellow Advisory Board: David B. Chapel, M.D.


Last author update: 21 June 2023
Last staff update: 21 June 2023
Copyright: 2007-2024, PathologyOutlines.com, Inc.
PubMed Search: Cardiac myxoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Pucci A, Bartoloni G. Cardiac myxoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/hearttumormyxoma.html. Accessed December 24th, 2024.
Definition / general
- Cardiac myxoma is a rare and benign tumor, distinct from soft tissue myxoma, most often occurring as a solitary, sporadic, pedunculated mass in the left atrium; approximately 10% occur in the context of Carney syndrome
Essential features
- Most common primary tumors of the heart, usually single in sporadic forms and mainly located in the left atrium
- In rare familial forms are related to Carney complex (see below) and there may be multiple and often relapsing tumors
- May mimic malignant neoplasia because of frequent embolism, systemic or obstructive symptoms
- May cause sudden death, usually due to mitral valve obstruction
- Histologic features include polygonal (lepidic) myxoma cells, either single or forming cords, nests and perivascular cuffs, a myxoid stroma and the absence of necrosis, mitotic activity and significant cell atypia
- Excellent prognosis but treatment requires complete surgical resection to avoid / prevent relapse and embolic or systemic symptoms
Terminology
- Recommended: cardiac myxoma
- Unusual components (i.e. glands, lymphoid proliferation, thymic rests) may be noted if present
ICD coding
Epidemiology
- Although rare, they represent the most common (~50% and up to 78% in surgical series) primary tumors of the heart; their incidence ranges between 0.0017% and 0.03% in autopsy series (J Thorac Oncol 2016;11:441)
- F:M = 1.8:1
- Mean age 50 years; most patients in 30 - 60 year range
- Rarely reported in pediatric age or as a part of a genetic disease (i.e. Carney complex) in young patients without sex predilection (Eur J Endocrinol 2021;184:R99)
Sites
- Intracardiac (J Thorac Oncol 2016;11:441)
- 90% occur in atria, 75% on left side and localized to the interatrial septum, close to fossa ovalis
- 90% are solitary and pedunculated tumors
- Can be found in any other cardiac chamber (right atrium, ventricles and valves)
Pathophysiology
- Uncertain origin and histopathogenesis
- Main hypothesis suggests an origin from multipotent mesenchymal cells, the rarely reported gland component representing entrapped foregut rests (European Heart Journal 2020,41:4332, Stem Cells Int 2016,2016:2059584, Am Heart J 2000;140:134)
- Controversial role of HSV infection (Cardiovasc Pathol 2017;27:31, Am J Pathol 2003;163:2407)
- Highly vascular tumors (sometimes supplied by neovascularization from coronary artery)
- Produce growth factors, matrix metalloproteases and cytokines, including vascular endothelial growth factor (VEGF), inflammatory cytokines, interleukin 6 (Heart Vessels 2018,33:1403, Am J Pathol 2005,166:1619)
- 90% are sporadic
- 10% are familial with autosomal dominant transmission (Carney syndrome)
- Autosomal dominant disease caused by mutations in protein kinase A regulatory subunit 1 alpha (PRKAR1A)
- Characterized by multiple cardiac and extracardiac (skin) myxomas, spotty skin pigmentation, endocrine overactivity, schwannomas, epithelioid blue nevus (Circ J 2005,69:994, Nat Genet 2000,26:89, Orphanet J Rare Dis 2006;1:21, Eur J Endocrinol 2021;184:R99)
- In Carney syndrome, myxomas:
- Occur in younger patients (mean 24 years), more often in men (66%)
- Often multiple (50%)
- Greater recurrence risk (Cardiovasc Pathol 2020;49:107231)
- More frequently located in the cardiac ventricles as compared with sporadic cases (13% versus 2%)
Clinical features
- Symptoms depend on size and location
- Most common presenting symptom is systemic embolism (30 - 50% of cases), which causes syncope, dyspnea, neurologic symptoms or ischemic limb pain; rarely, complete tumor embolization occurs (J Cardiovasc Echogr 2020,30:S45, Lancet Oncol 2005,6:219, Tex Heart Inst J 2005,32:238)
- Nonspecific constitutional symptoms and signs are present in 90% of cases; fever / malaise may be associated with elevated sIL6 mediating acute phase response (Neuropathology 2021;41:49)
- Pedunculated tumors may move through atrioventricular valve at systole with a "wrecking ball" effect and cause valve obstruction, syncope and even sudden death (Cardiovasc Pathol 2020;49:107244)
- In a few cases, cardiac myxoma is asymptomatic and may be incidentally diagnosed, in vivo (usually by echocardiography) or at autopsy
Diagnosis
- Diagnosis of cardiac myxoma requires histology
- Usually done on surgically excised tumors, although endomyocardial biopsy may be performed in cases with atypical presentation (Cardiovasc Pathol 2012;21:245)
Laboratory
- Elevated erythrocyte sedimentation rate (ESR), C reactive protein, sIL6 and serum gamma globulin levels can be found but have limited specificity
Radiology description
- Echocardiography is the main tool for in vivo diagnosis of cardiac masses, including myxomas
- Shows lucencies and cystic areas due to hemorrhage (Echo Res Pract 2016;3:R65)
- Cardiac MRI provides accurate assessment of location, attachment site and functional impact of cardiac myxomas (Radiol Clin North Am 2021;59:231)
Radiology images
Contributed by Giuseppe Vergaro, M.D., Ph.D. and Vladyslav Chubuchnyi, M.D.
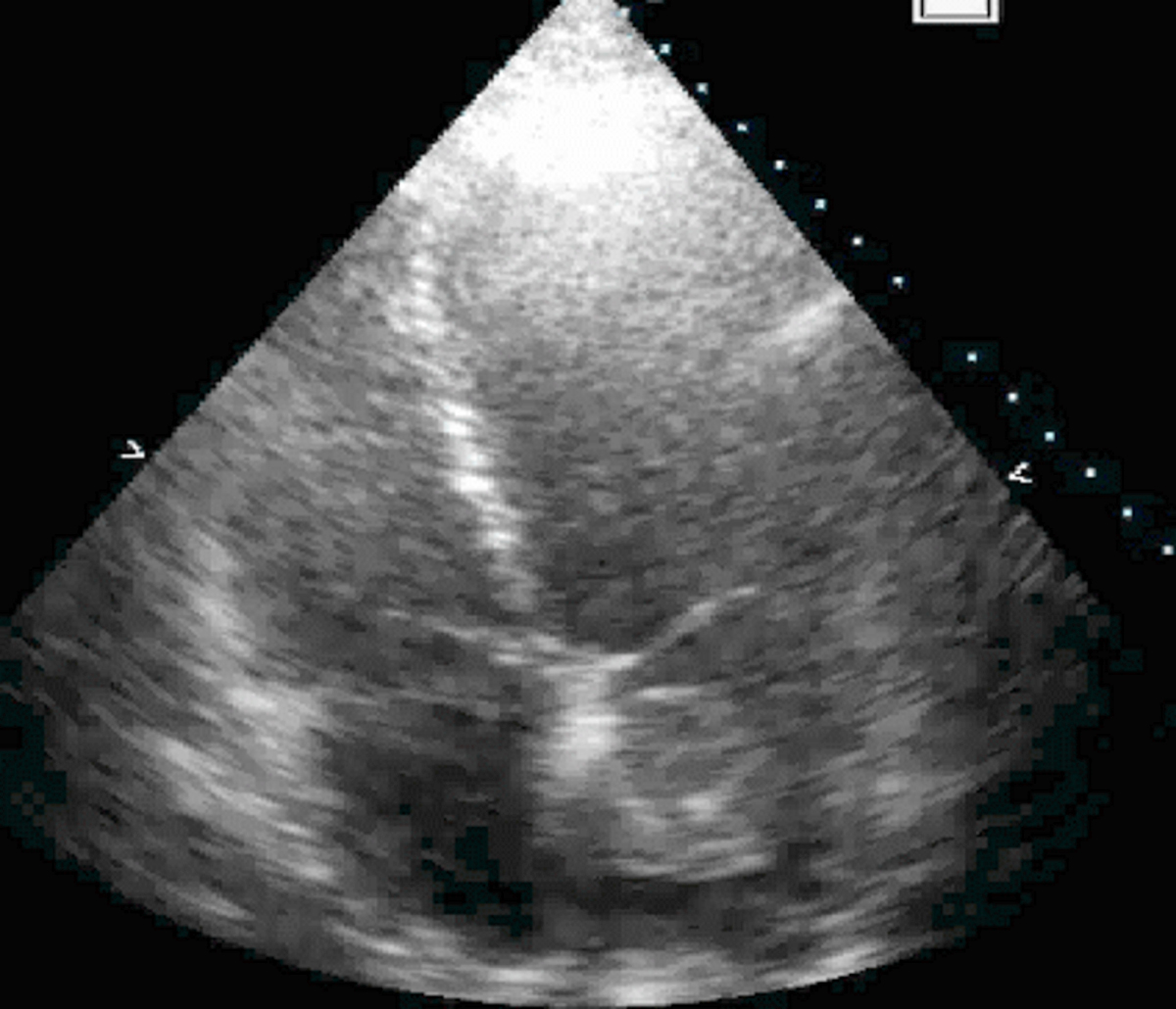
2D echocardiography

Cardiac magnetic resonance
Prognostic factors
- Typically benign tumors but possible local (after incomplete resection) or distant (due to tumor embolization) recurrence (Lancet Oncol 2005,6:219)
- If untreated, cardiac myxomas may cause systemic embolism and cerebrovascular accidents or valve obstruction and congestive heart failure
- Embolic phenomena (sometimes mimicking metastasis) might be related to overexpression of matrix metalloproteinase (MMP) (Heart Vessels 2018,33:1403, Am J Pathol 2005,166:1619)
- Greater recurrence risk in myxomas associated with Carney syndrome
- If untreated, cardiac myxomas may cause systemic embolism and cerebrovascular accidents or valve obstruction and congestive heart failure
Case reports
- 23, 55 and 57 year old men and a 45 year old woman with glandular cardiac myxoma in the left or right atrium (Virchows Arch 2003;443:618)
- 31 year old man with left atrial myxoma embolization causing ischemic stroke (Stroke 2021;52:e10)
- 43 year old man with a left ventricle myxoma and infective endocarditis (Tex Heart Inst J 2019;46:215)
- 55 year old woman with EBV positive atypical lymphoid proliferation in a left atrial myxoma (Cardiovasc Pathol 2013,22:e5)
- 69 year old man with a right atrial lithomyxoma showing extramedullary hematopoiesis (Heart 2002;88:10)
Treatment
- Radical excision; minimally invasive surgery (right lateral minithoracotomy) may be effective (Heart Lung Circ 2019;28:327)
- Rare recurrences following incomplete excision or in Carney complex (J Med Case Rep 2014,8:134)
Gross description
- Variable size, 1- 15 cm, sessile or pedunculated; 41% have surface thrombus
- Gross features: smooth, oval and lobulated or villous, friable and soft or gelatinous-like mass (J Thorac Oncol 2016;11:441)
- Rarely flat and sessile because of massive embolization
- Occasionally presents as calcified, stone-like mass (lithomyxoma) due to repeated hemorrhage
- Rarely grows on both sides of fossa ovalis
- Hemorrhagic areas are frequent, no necrosis
Gross images
Contributed by Angela Pucci, M.D., Ph.D. and Giovanni Bartoloni, M.D.
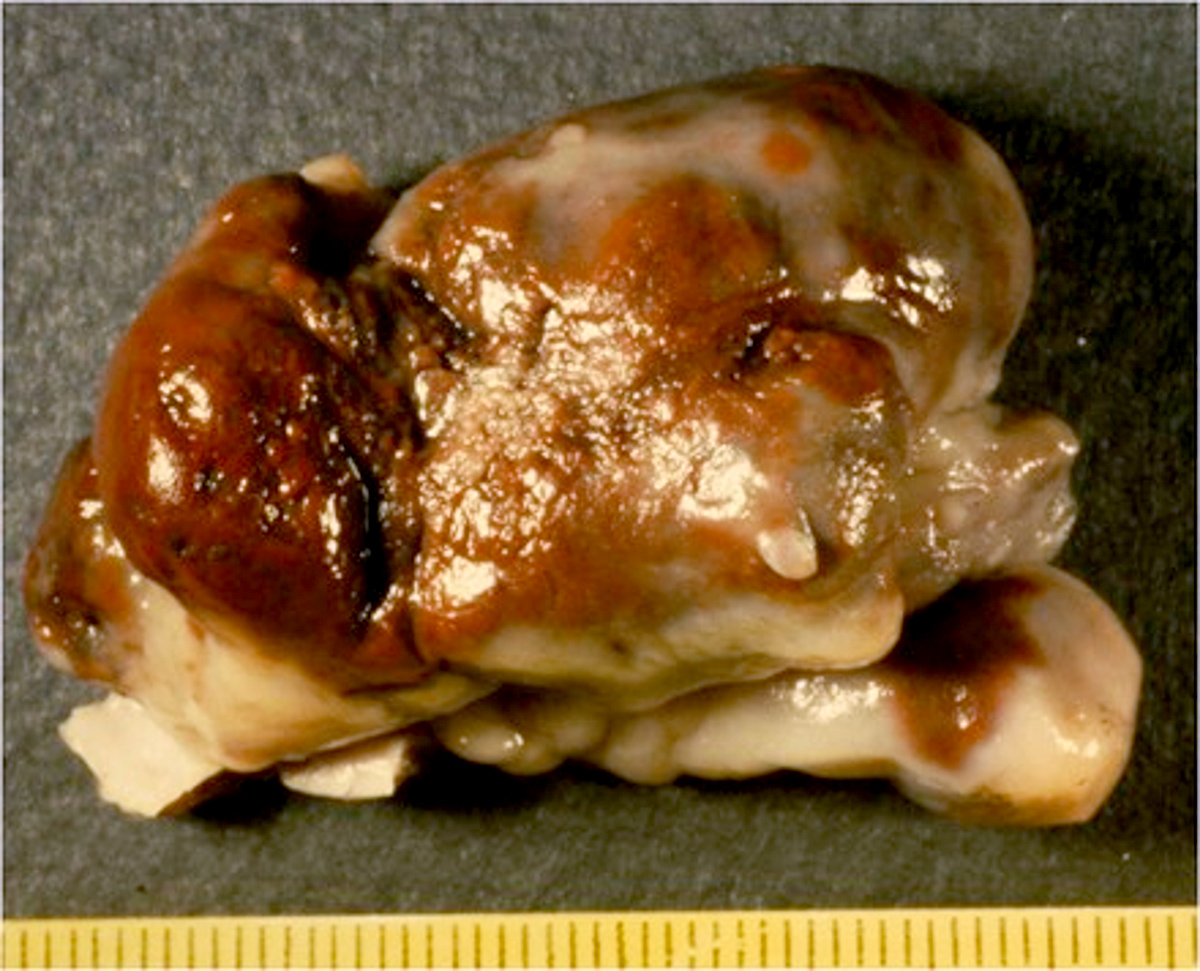
Polypoid
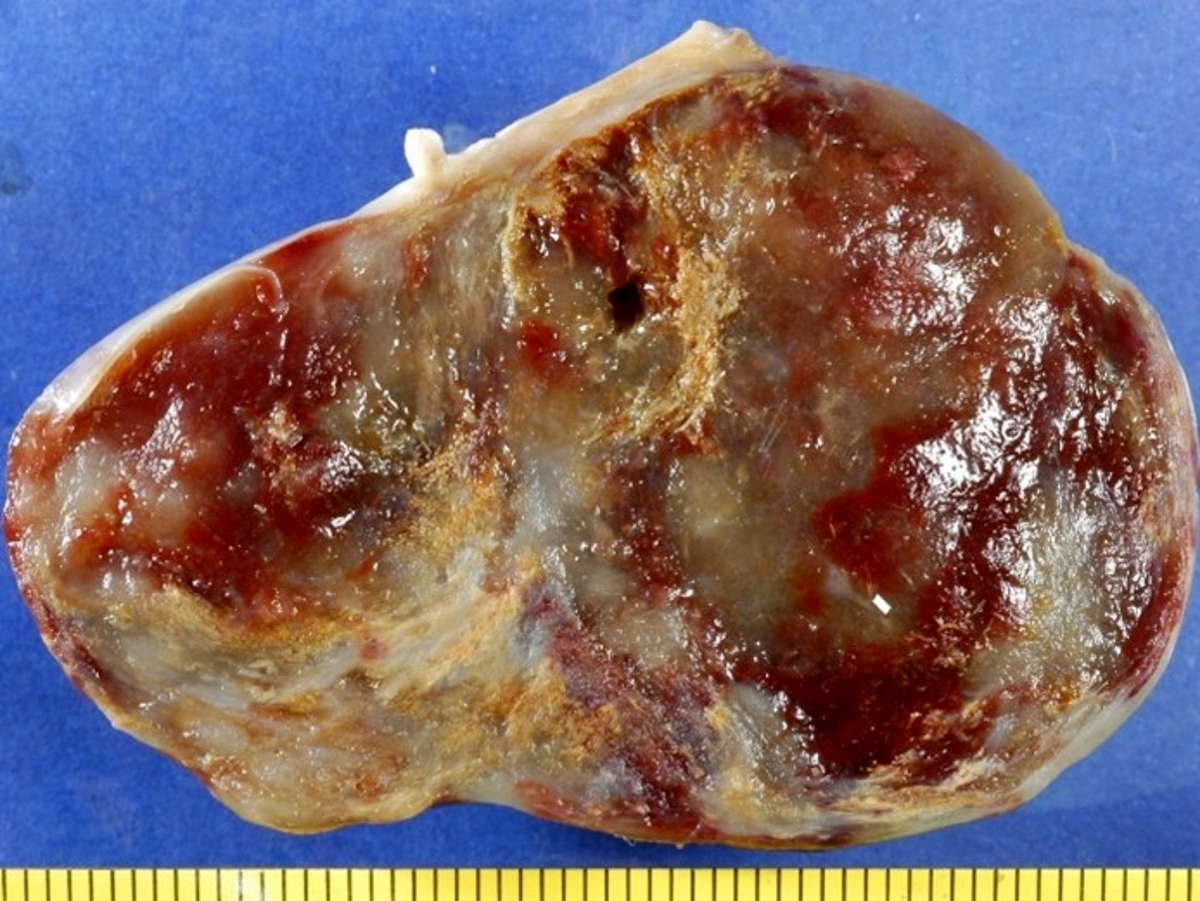
Hemorrhage
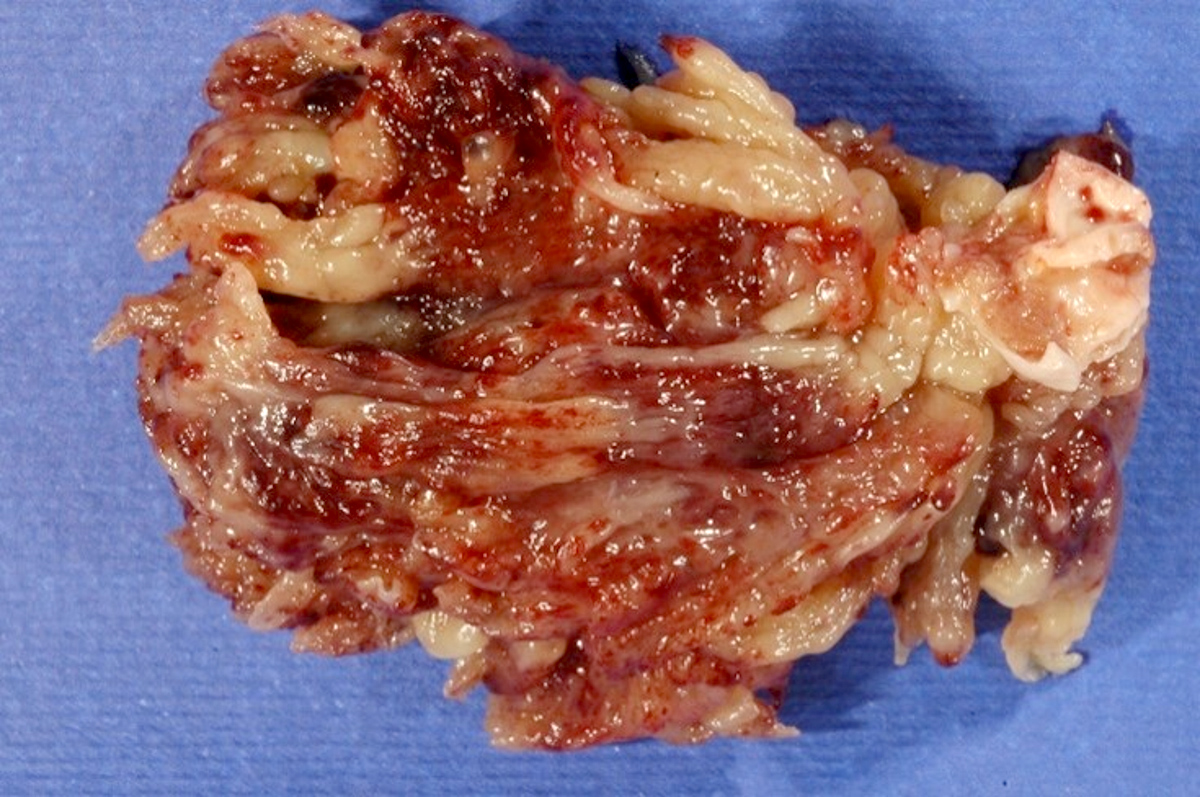
Villous morphology
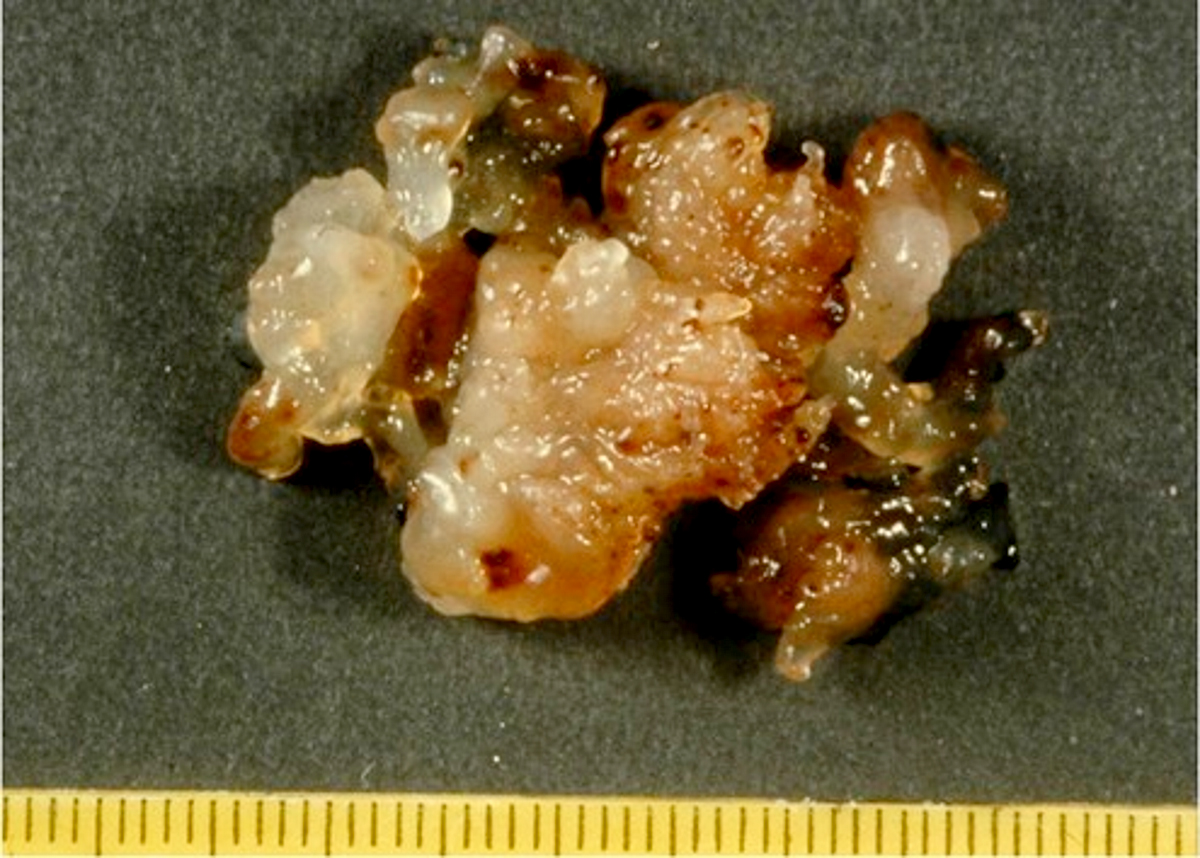
Soft and friable projections
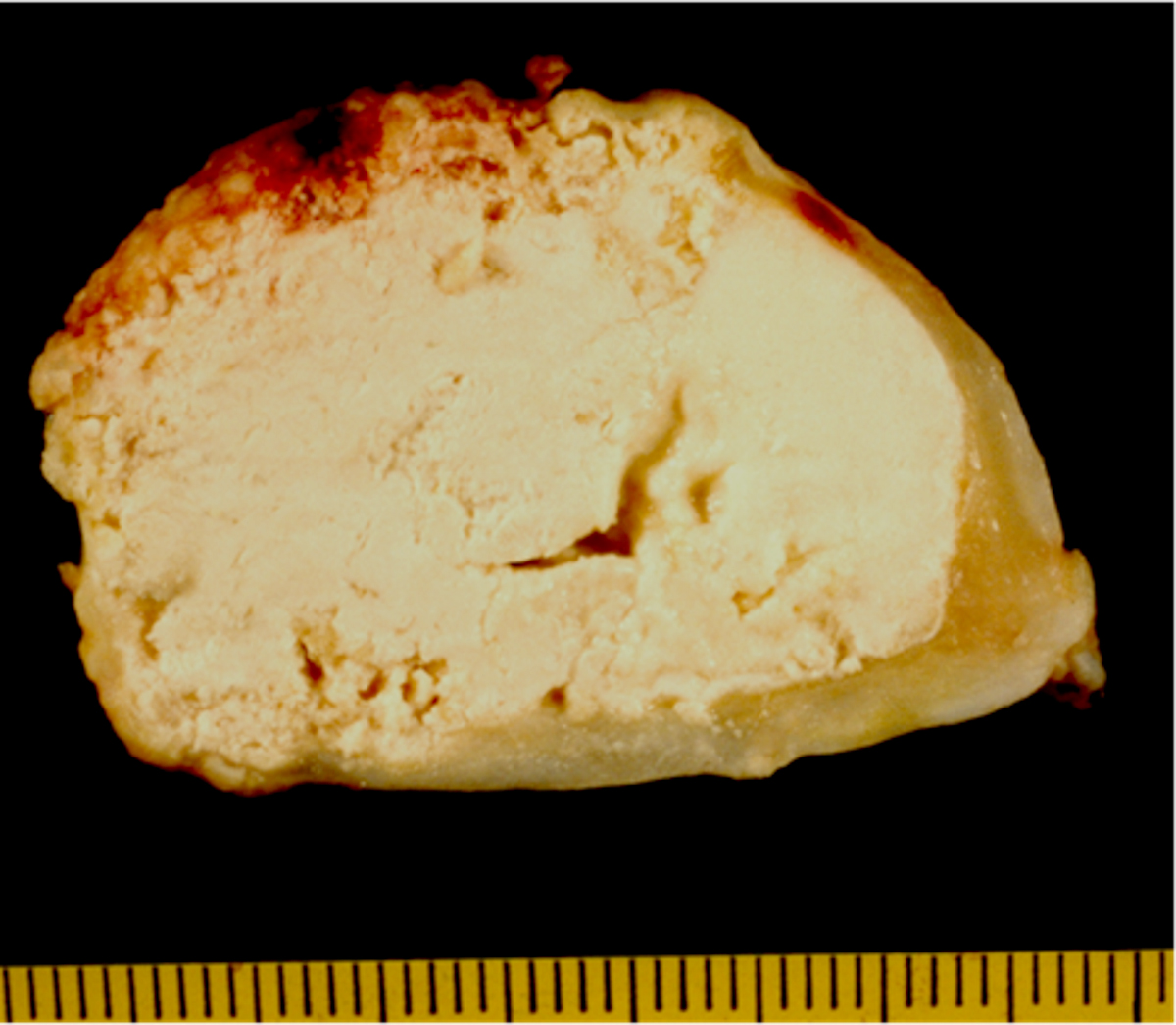
Chalky aspect
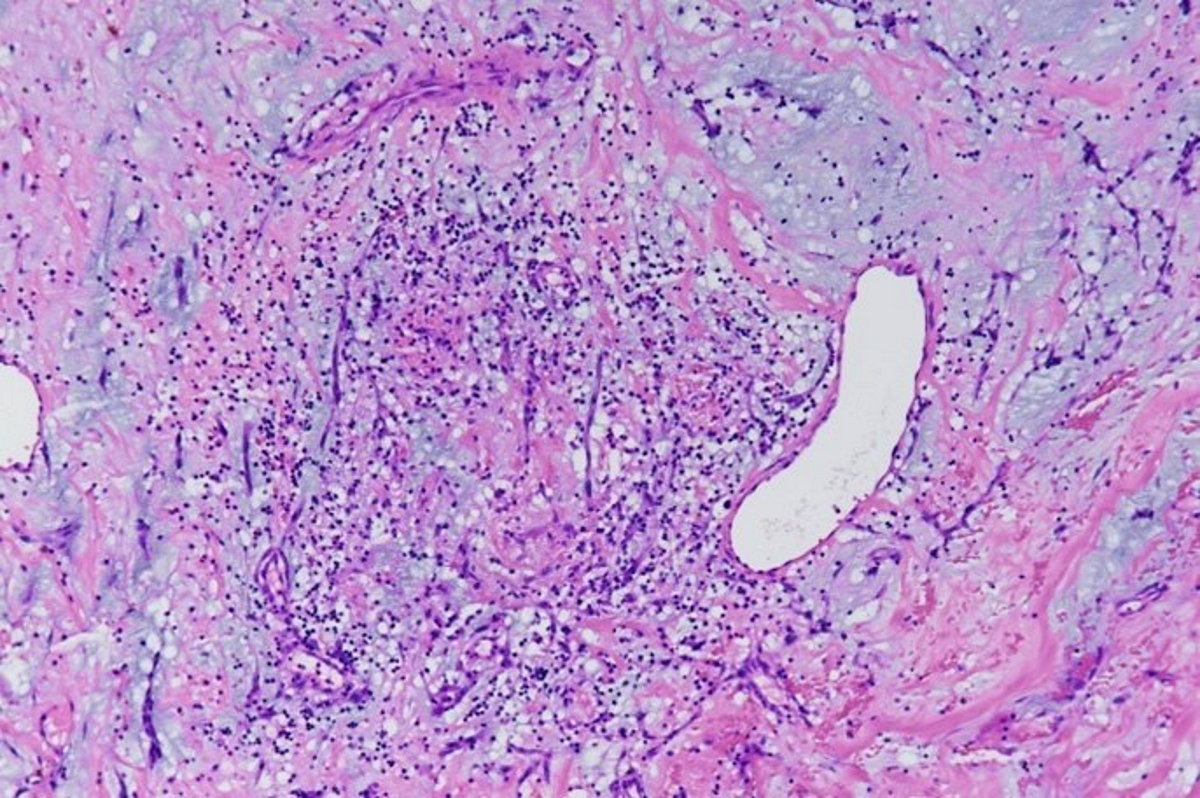
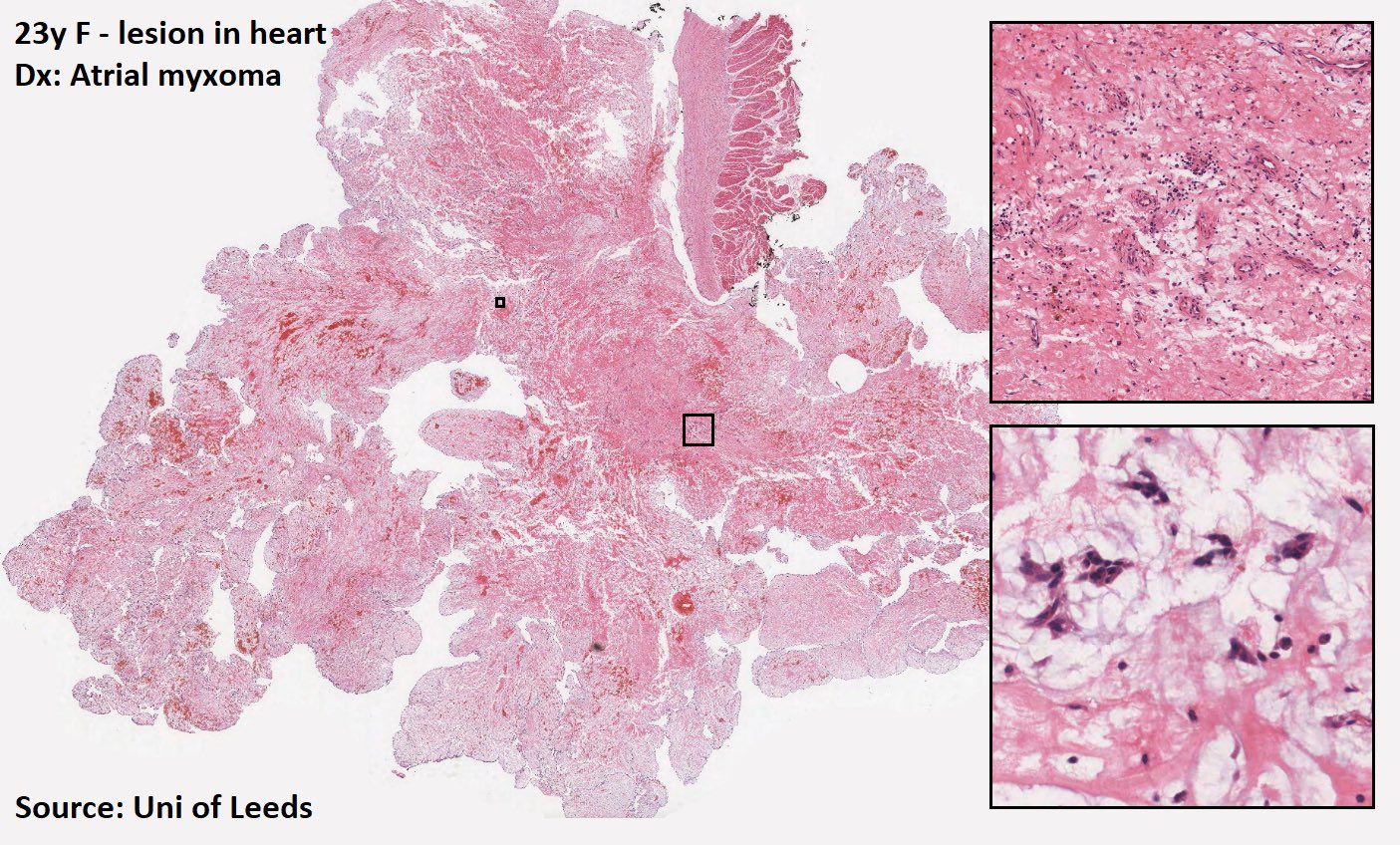
Microscopic (histologic) description
- Diagnostic criteria: neoplastic (lepidic) cells within myxoid stroma
- Complex structures resembling cords, nests or rings around blood vessels
- These structures are composed of polygonal / stellate myxoma (lepidic) cells with abundant eosinophilic cytoplasm, indistinct cell borders, oval nucleus with open chromatin and indistinct nucleolus
- Abundant mucopolysaccharide (myxoid) ground substance containing chondroitin sulfate and hyaluronic acid
- Usually present: inflammatory cells and hemorrhage with hemosiderin deposits; often smooth muscle cells within the myxoid stroma
- Neither frank mitotic activity nor necrosis in the lepidic cells of myxoma
- Variable fibrosis (41%), calcification (20%), Gandy-Gamna bodies (17%, identical to those in spleen of sickle cell anemia patients), ossification (8%), extramedullary hematopoiesis (7%, more common in children)
- Rarely, glandular structures with mucin forming glands, lymphoid proliferations mimicking lymphoma (see case report) or thymic rests or thymoma (Virchows Arch 2003;443:618, Am J Surg Pathol 2005;29:1208)
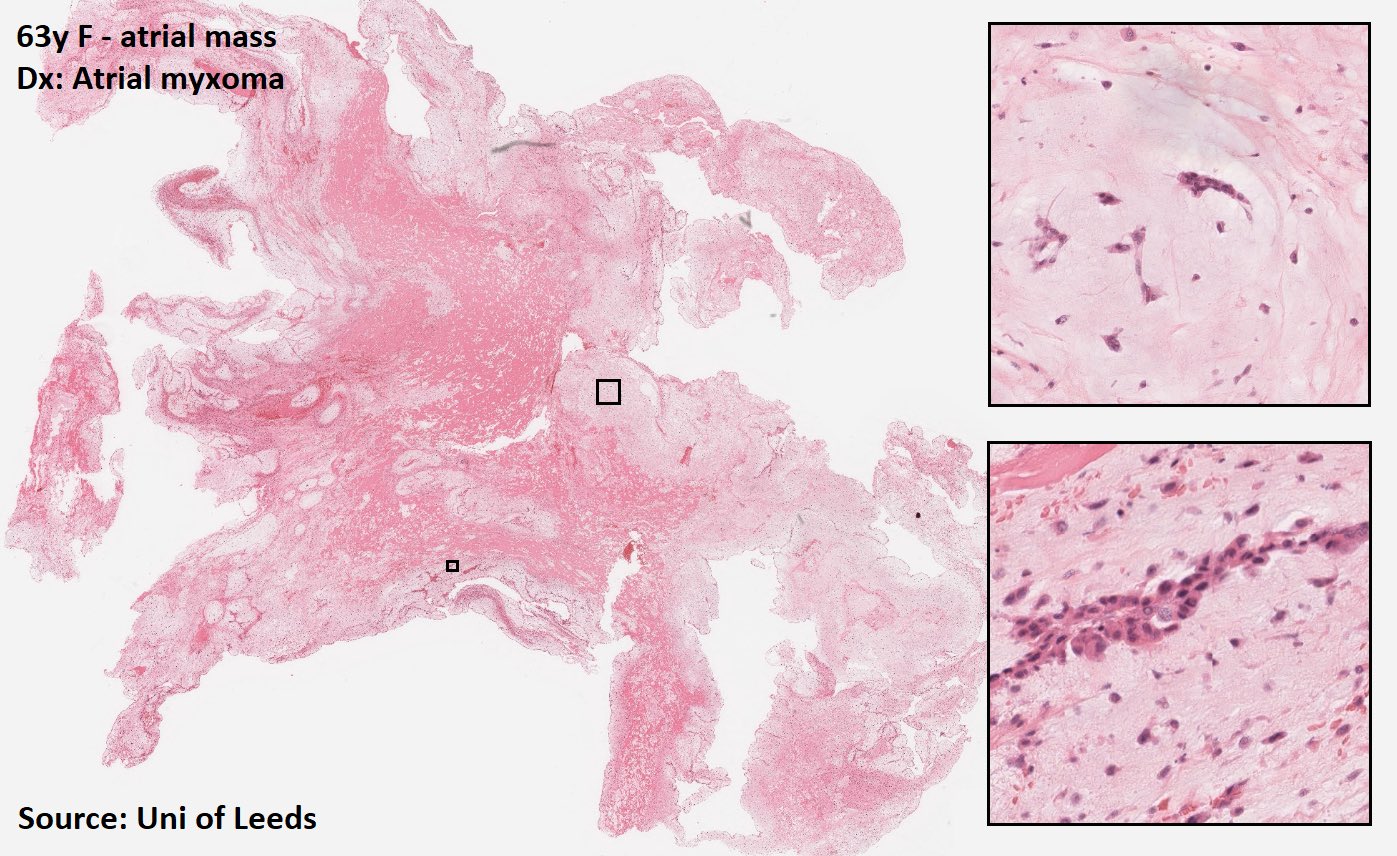
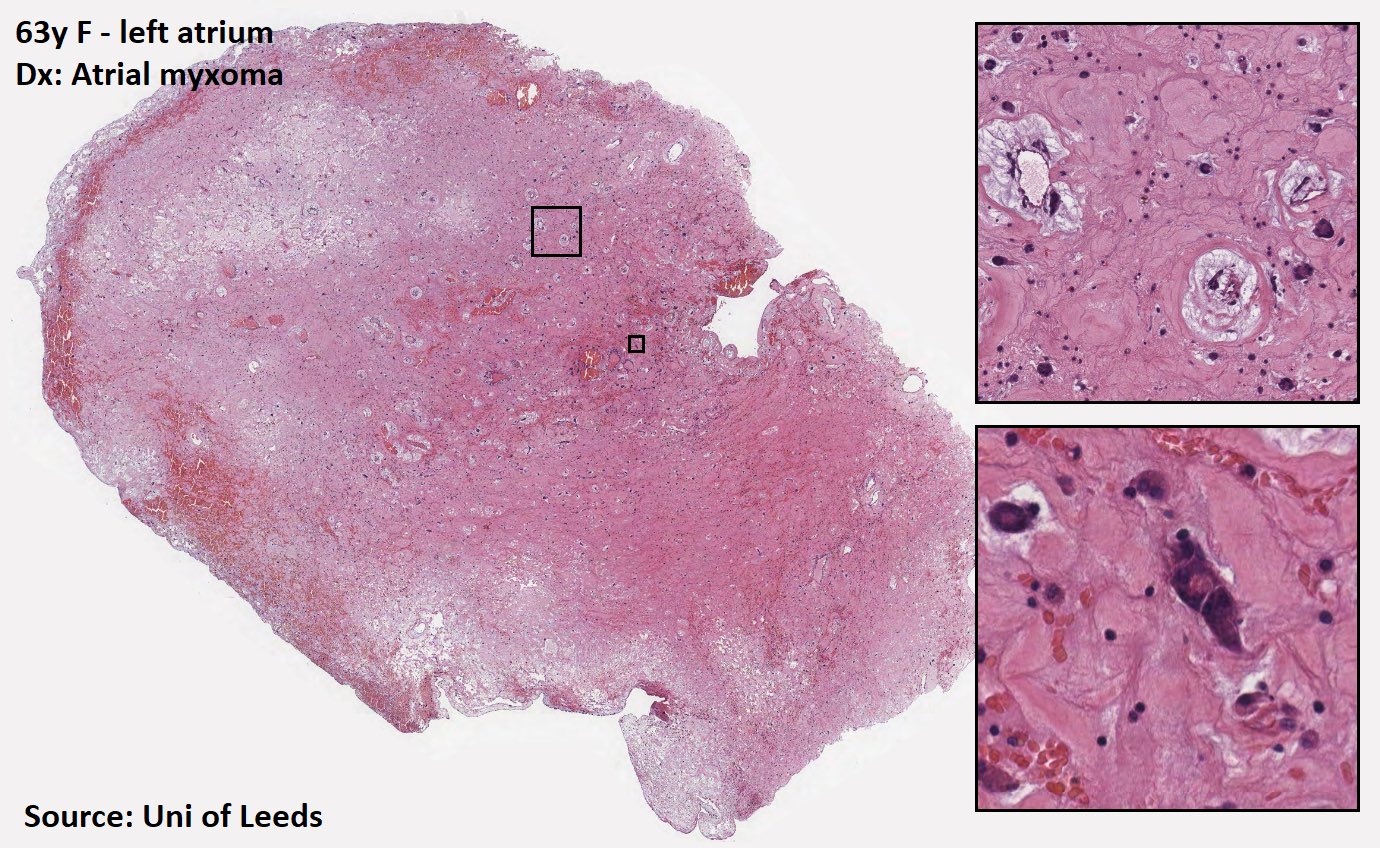
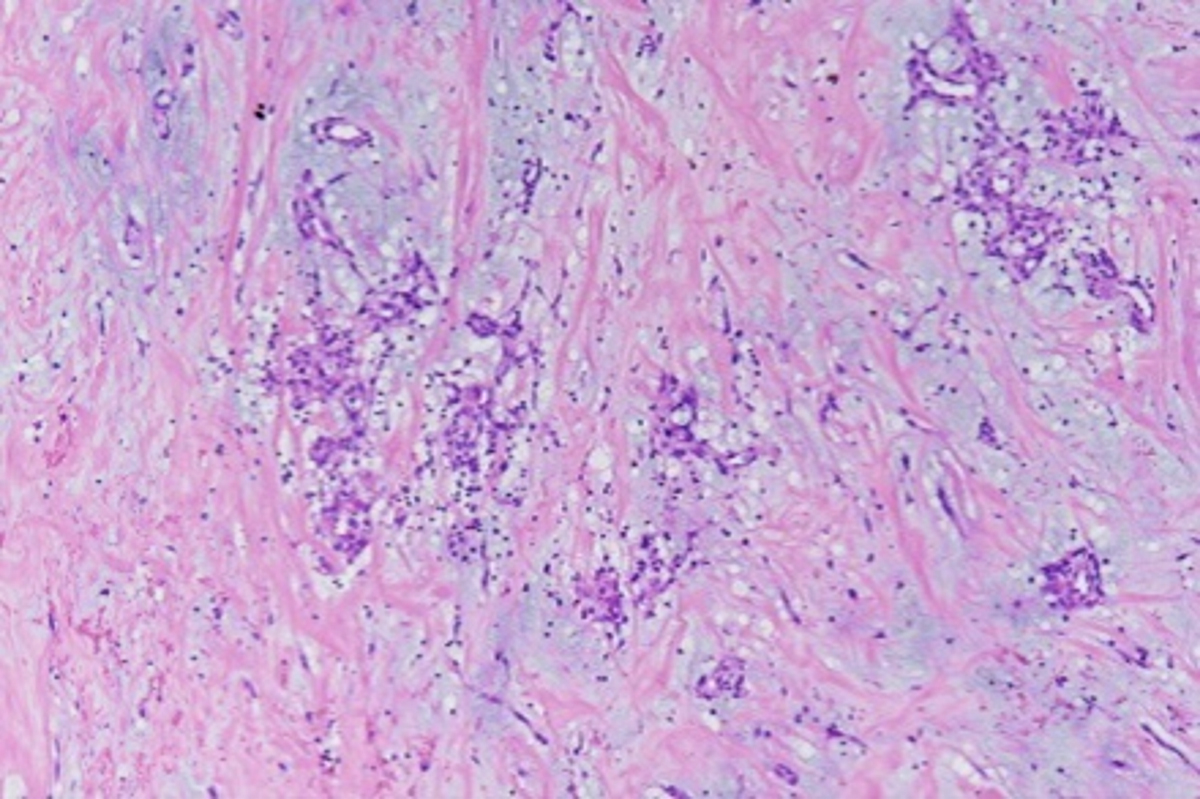
Microscopic (histologic) images
Contributed by Angela Pucci, M.D., Ph.D. and @DrTravisBrown on Twitter
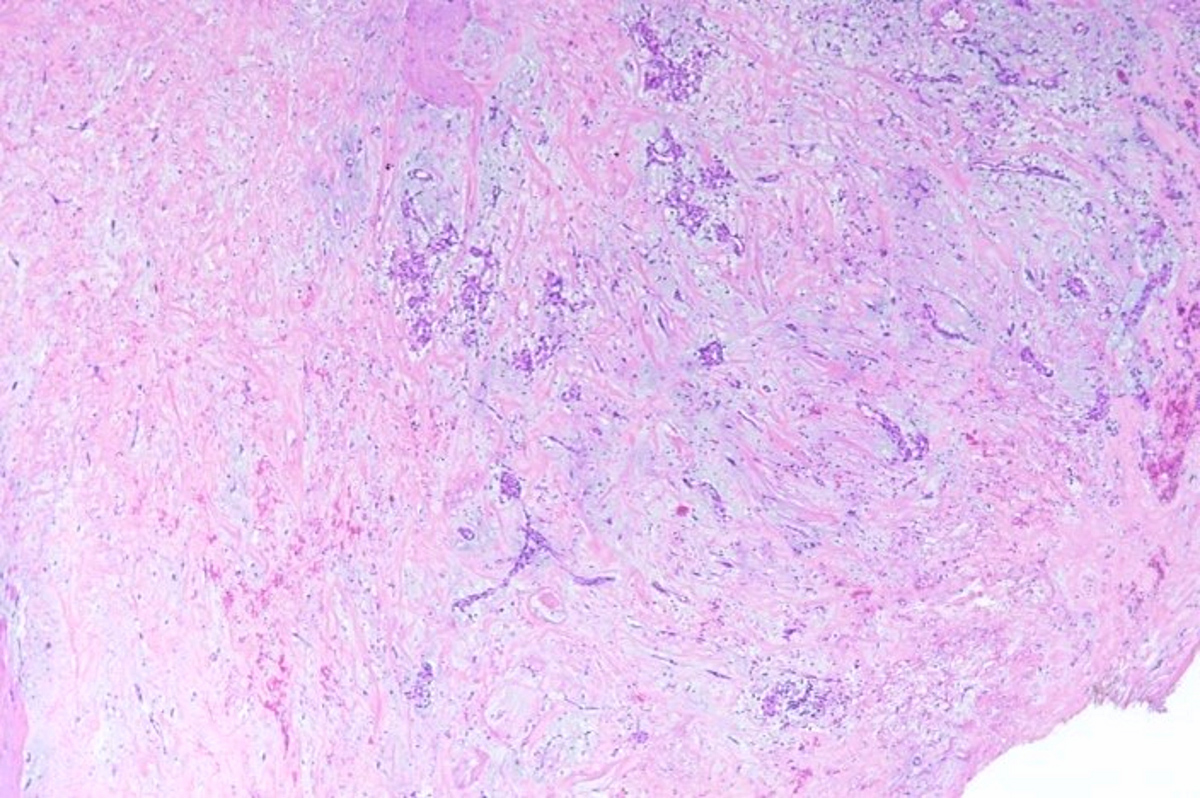
Left atrial myxoma
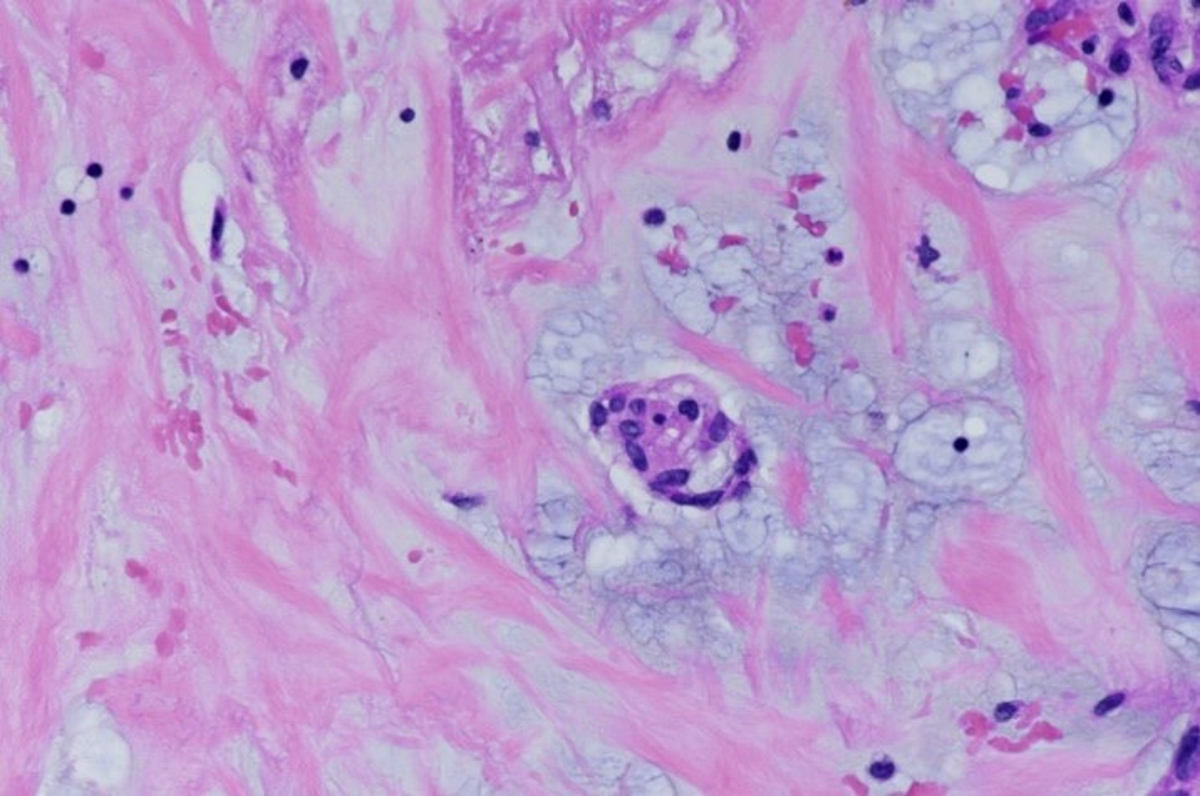
Myxoma cell nest
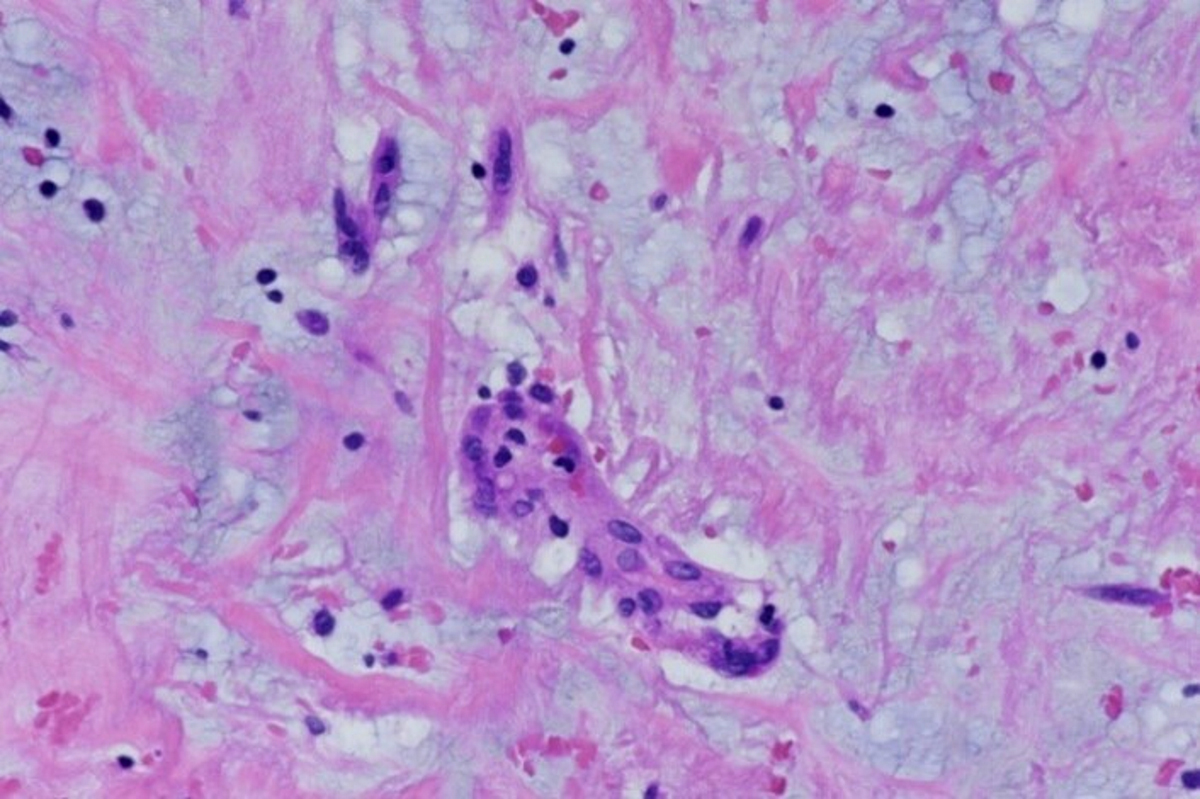
Myxoma cells in cord structure or isolated
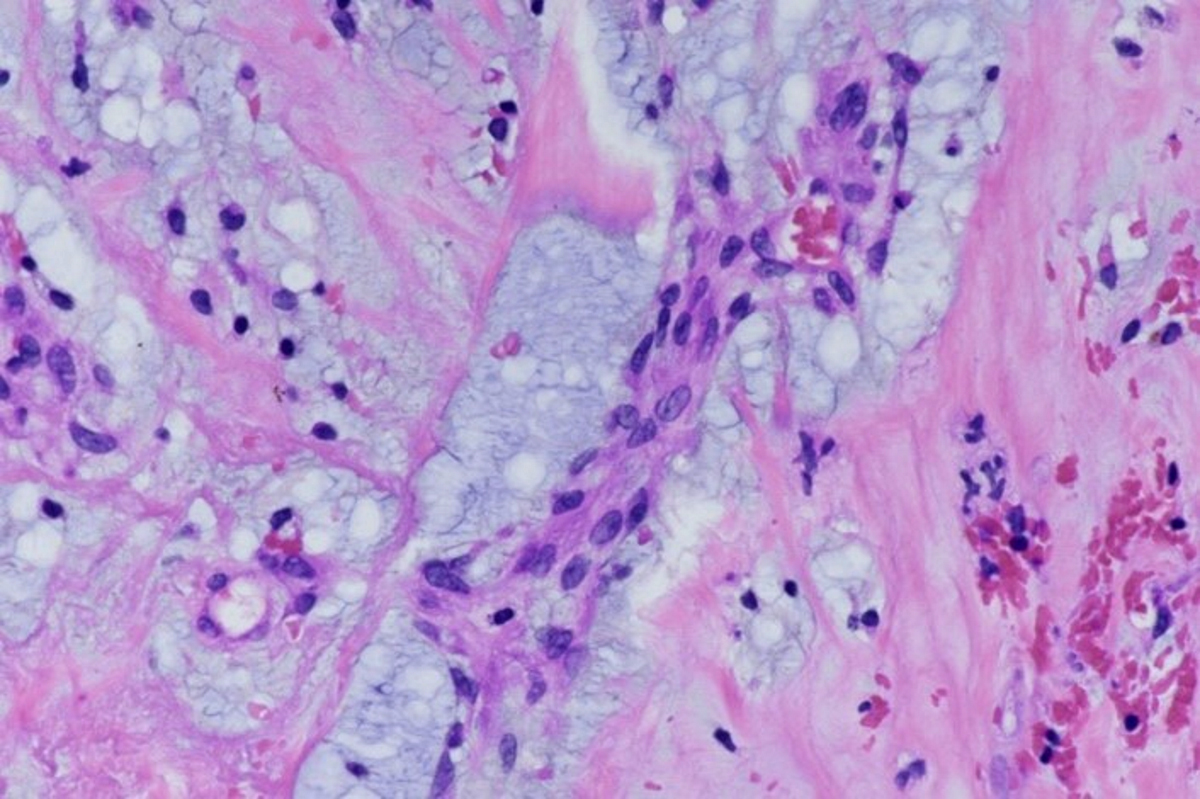
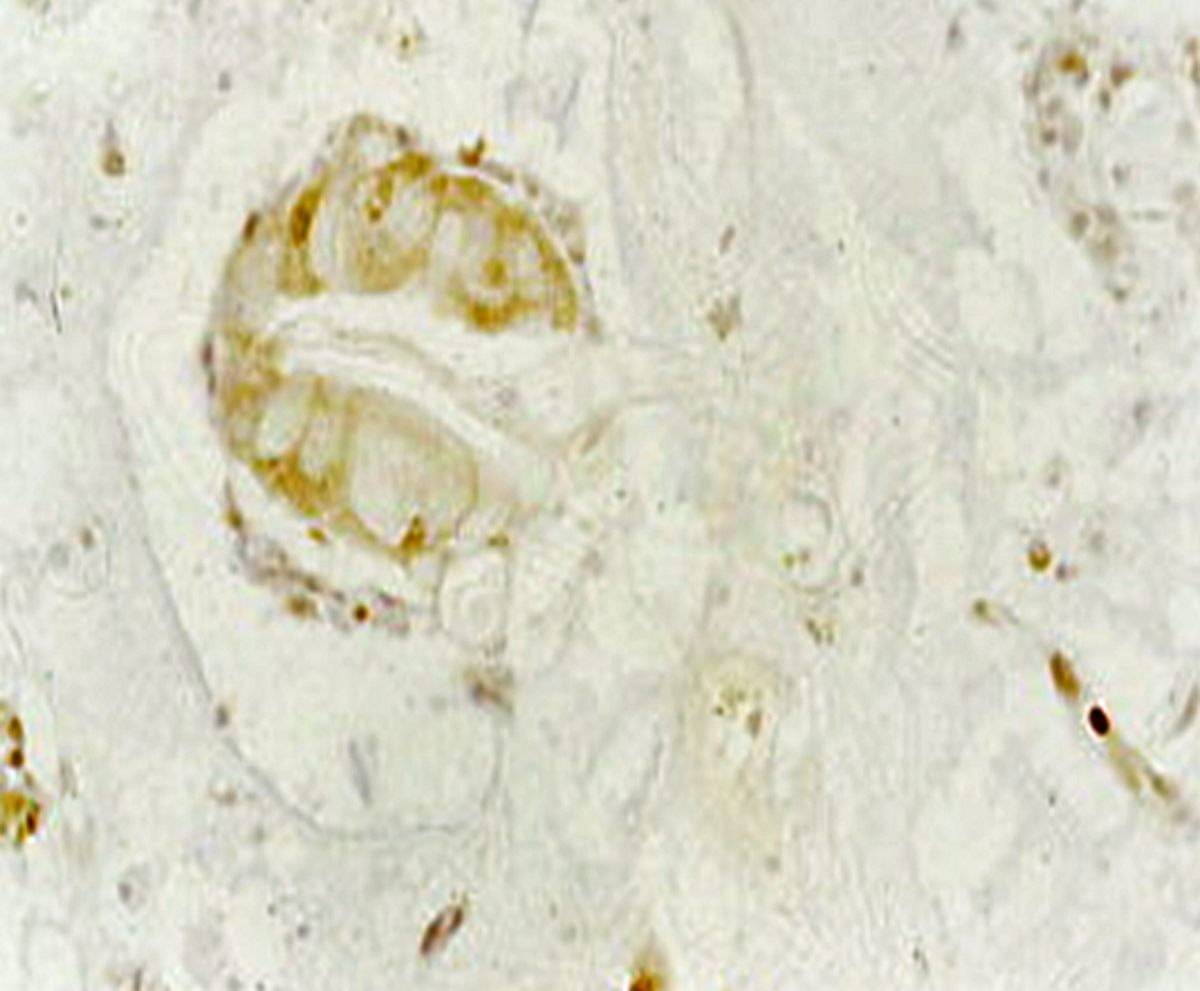
Myxoma cells around blood vessel
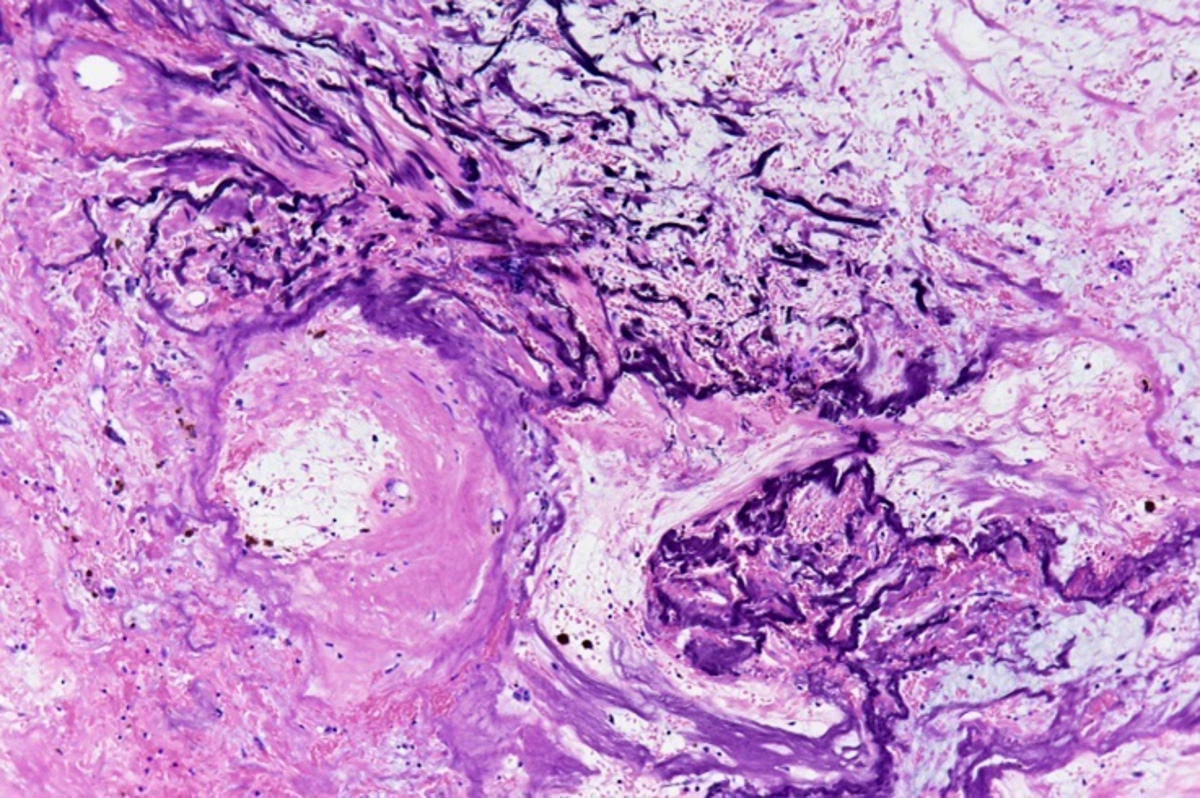
Gandy-Gamna bodies
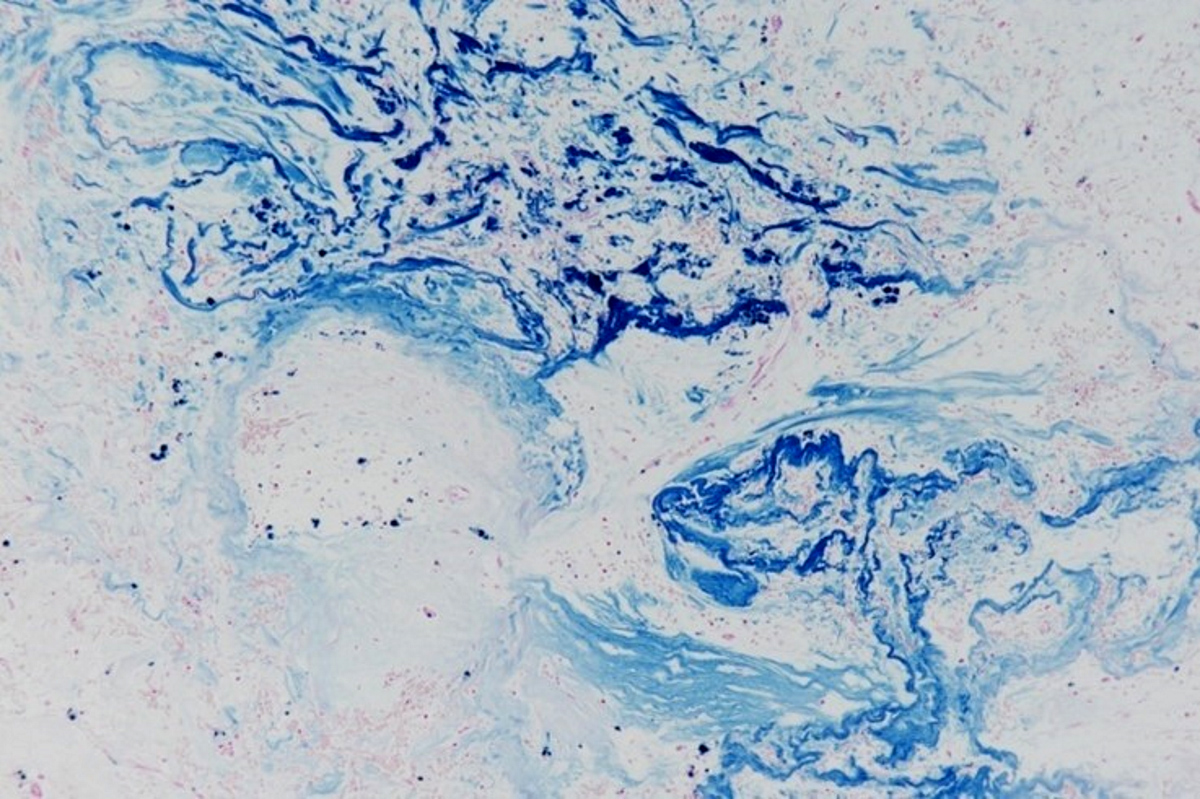
Gandy-Gamna bodies (Perls staining)
Inflammatory infiltrates
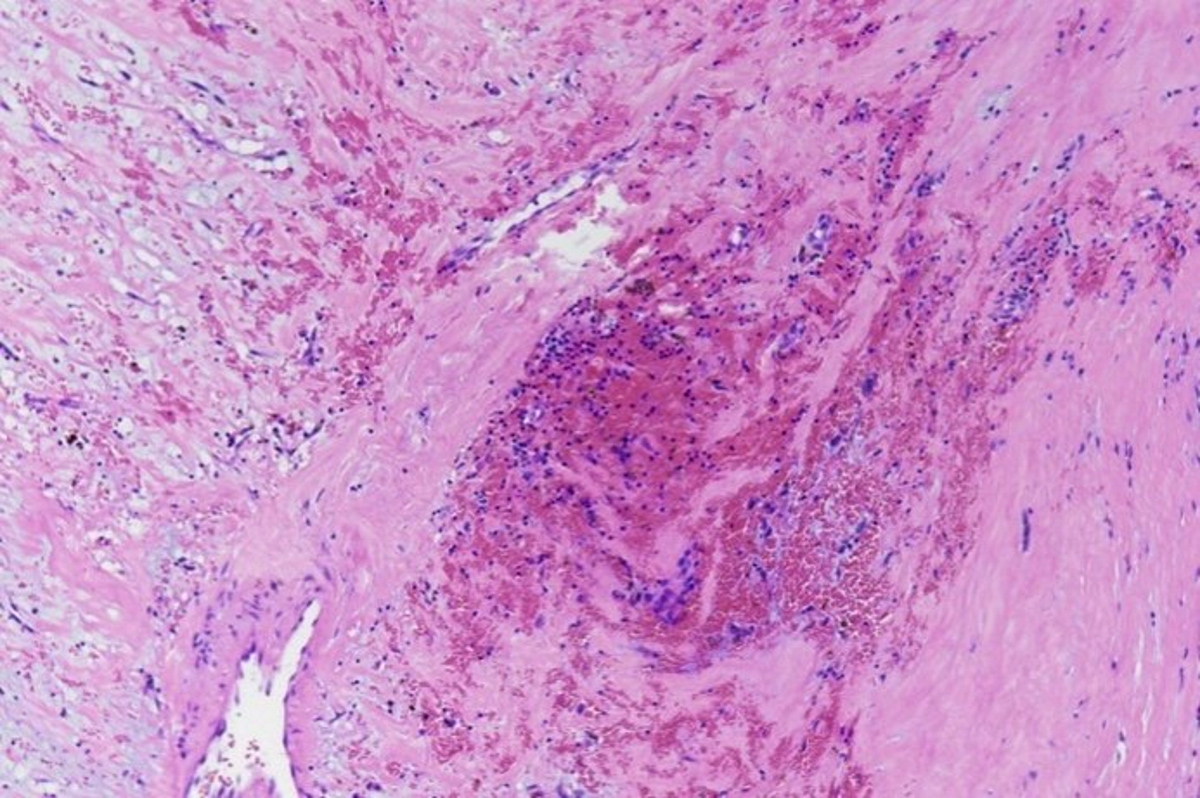
Hemorrhage
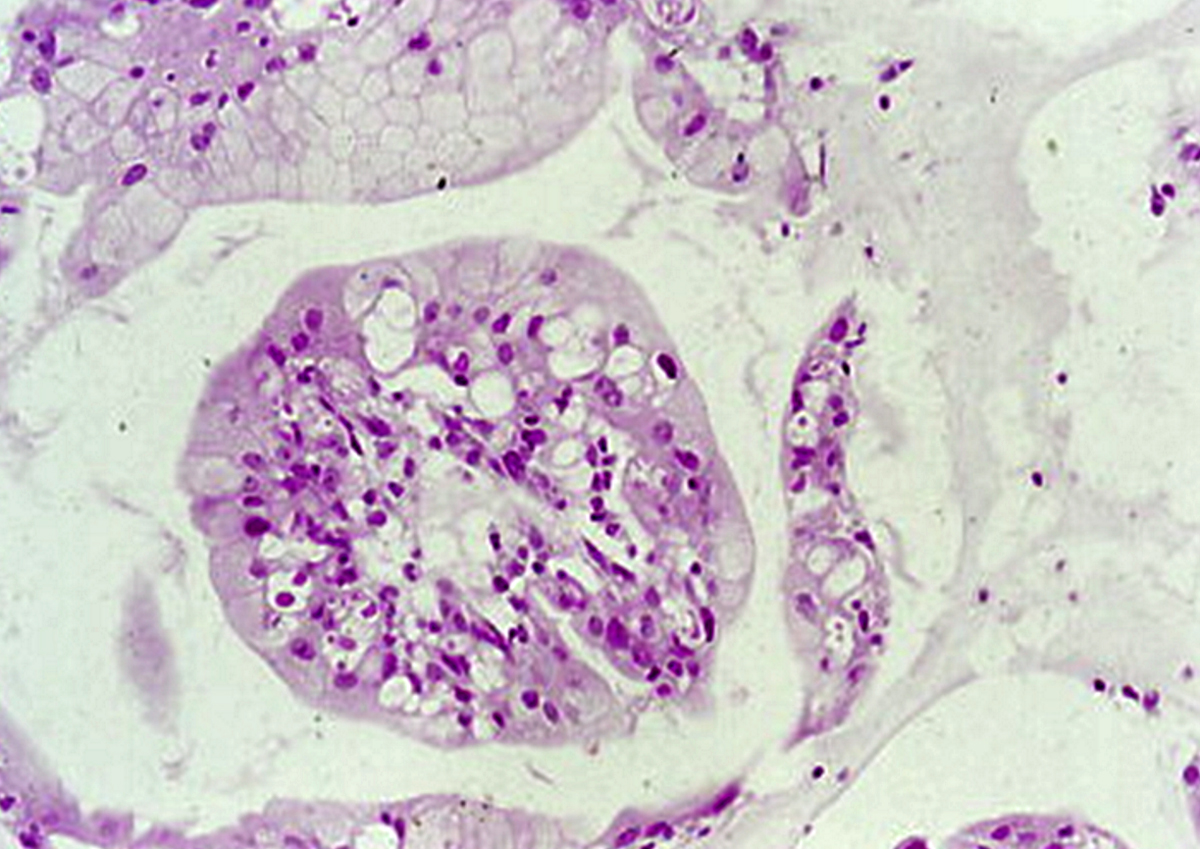
Glands in cardiac myxoma
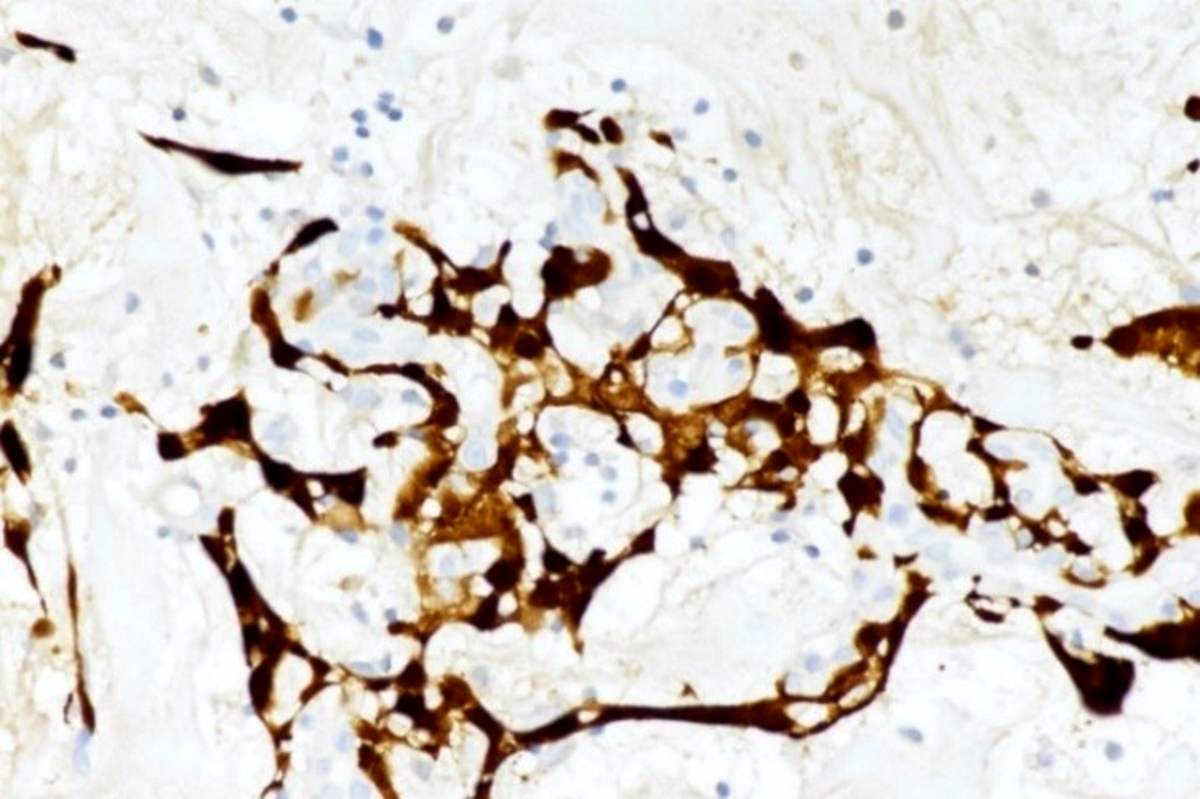
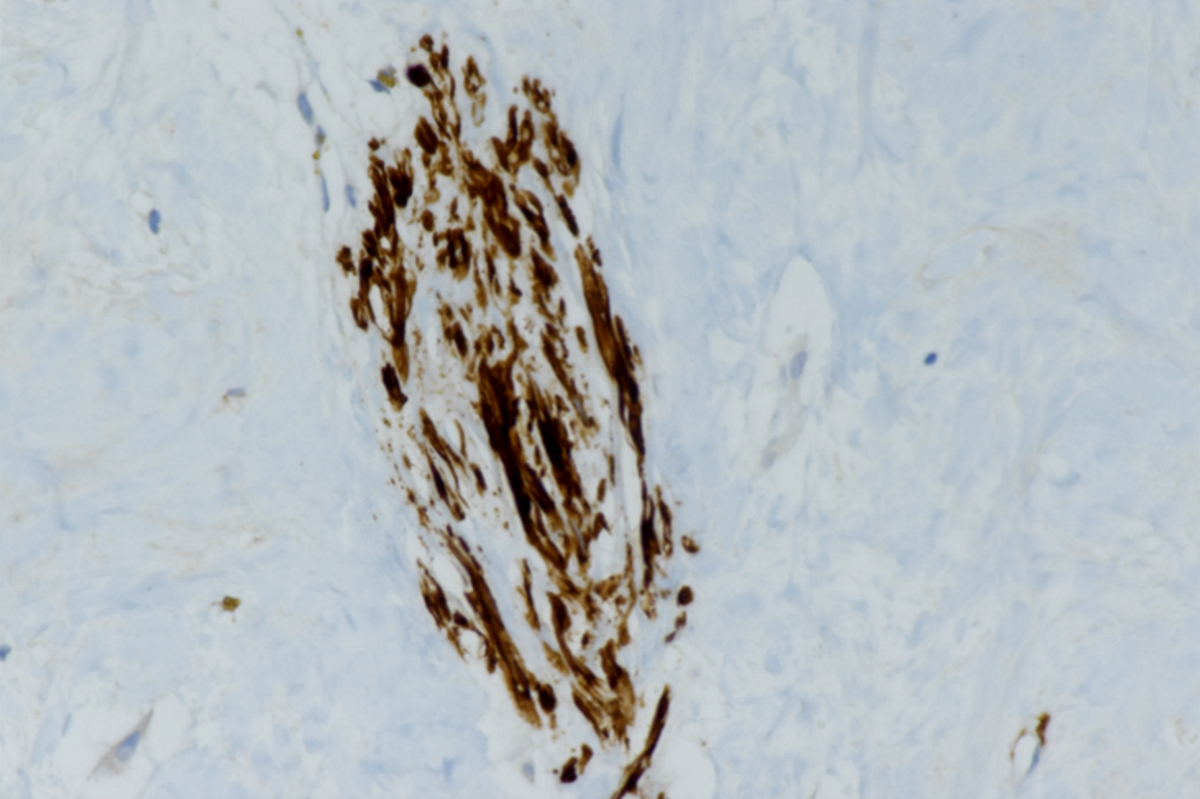
Calretinin
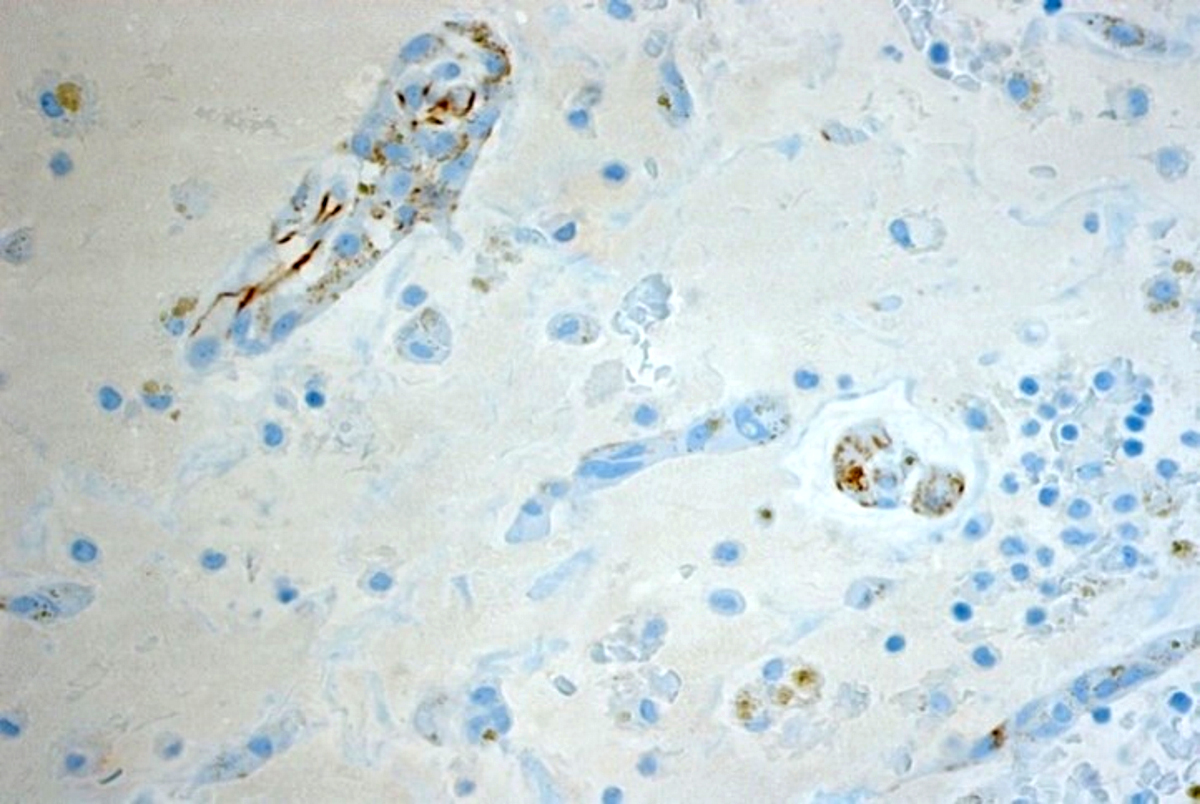
CD31+ vessels

S100 immunoreactivity
αSMA+
CK+ gland in cardiac myxoma

Cardiac myxoma
Immunofluorescence images
Contributed by Angela Pucci, M.D., Ph.D.
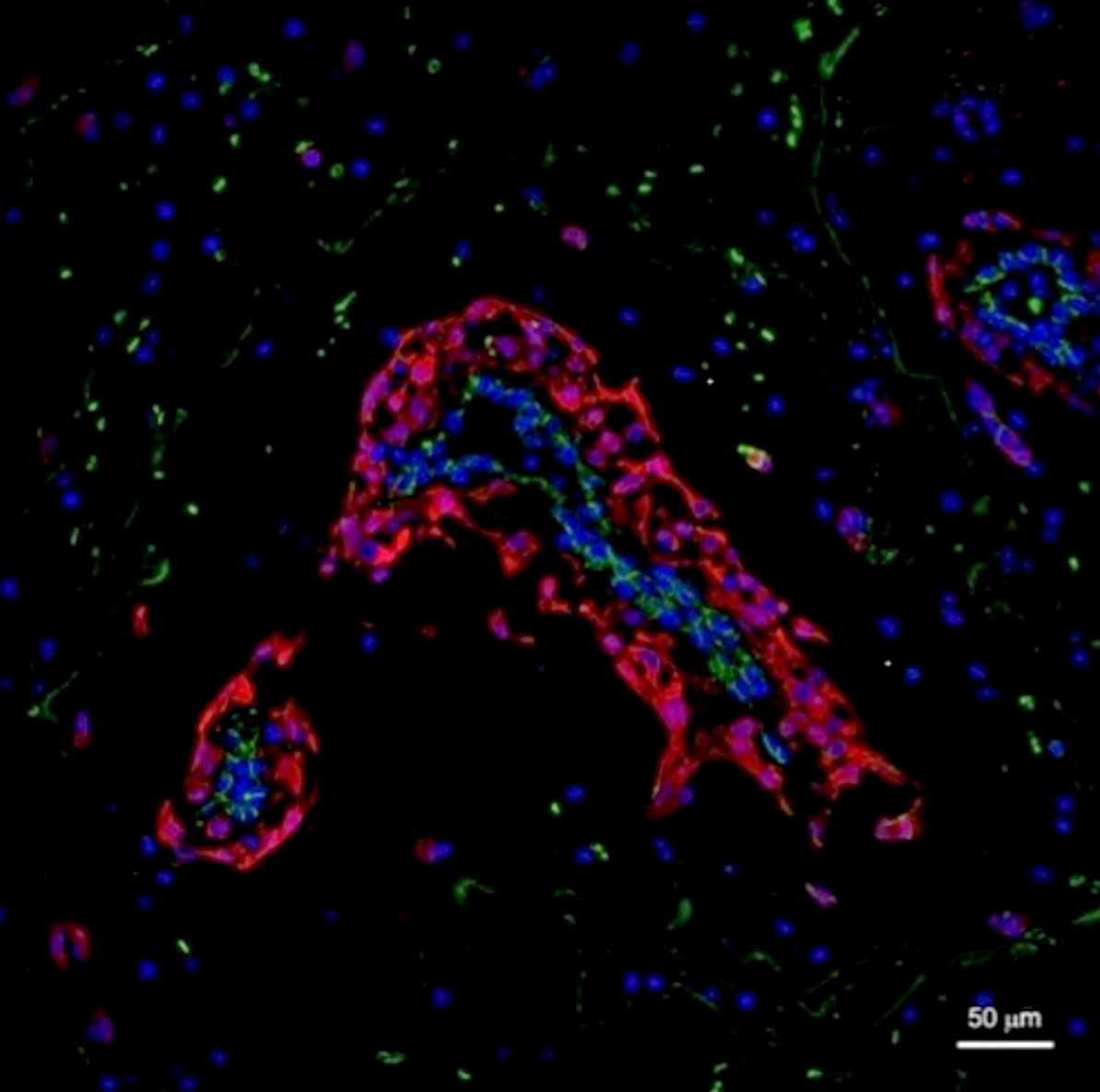
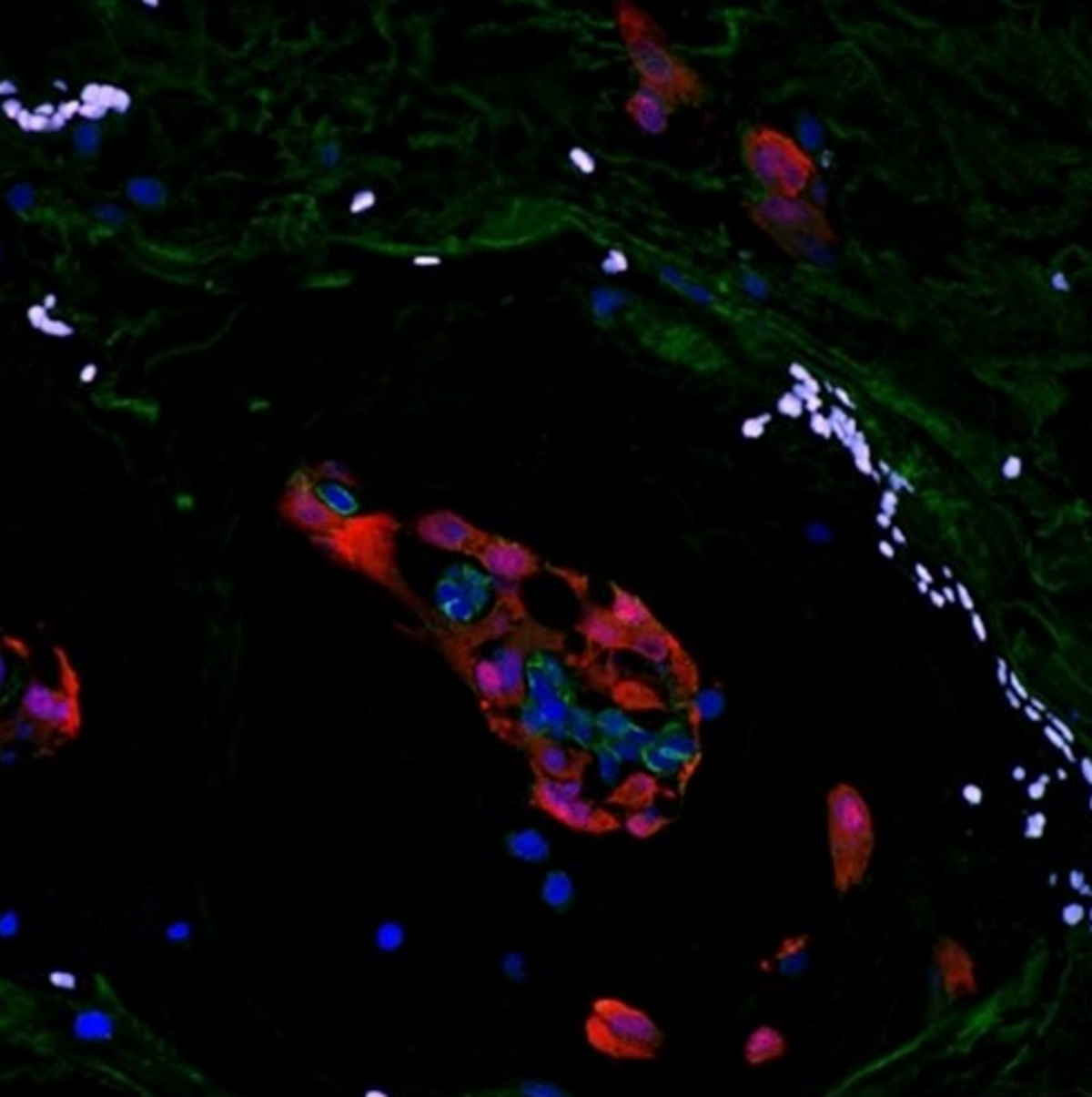
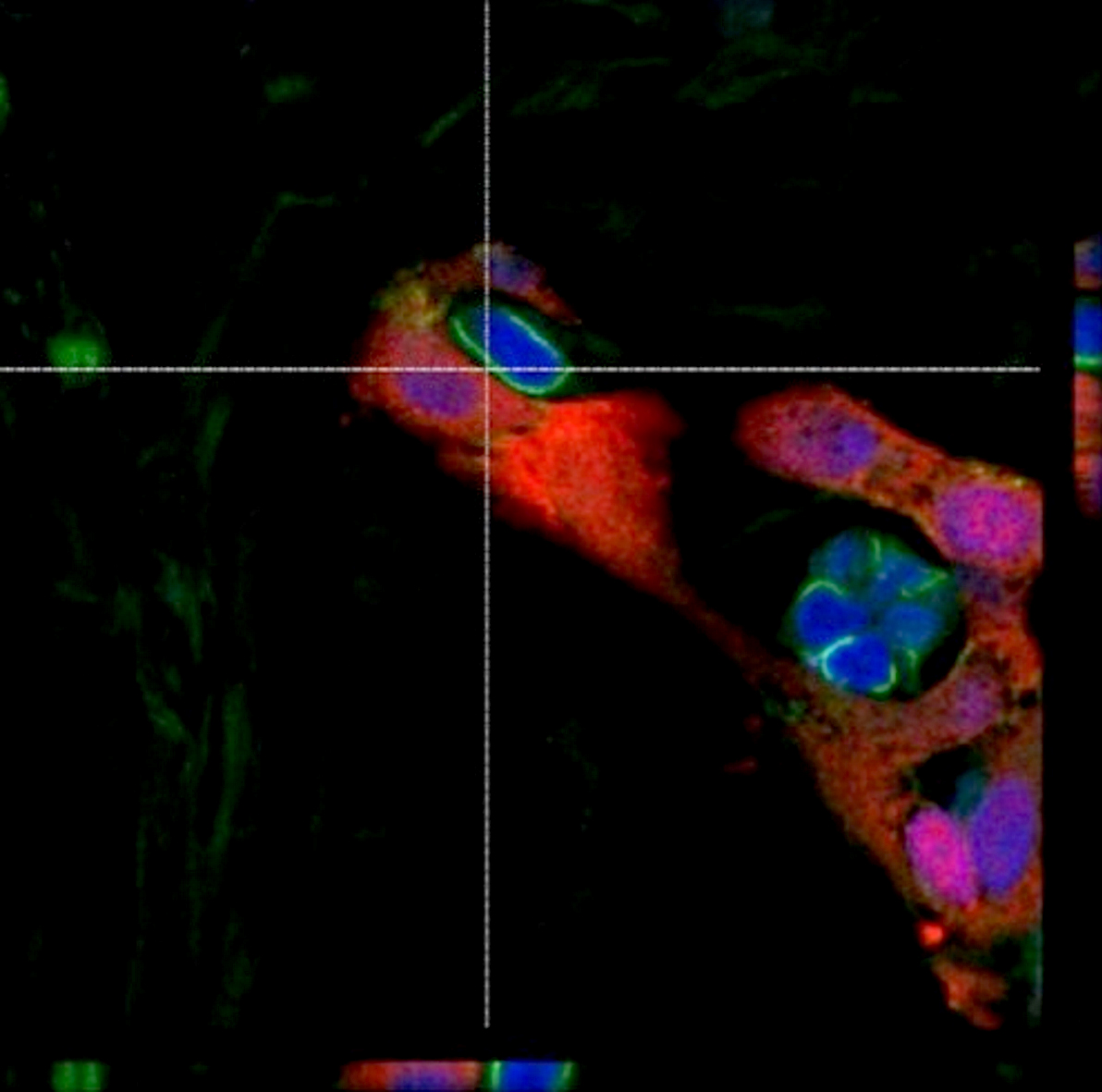
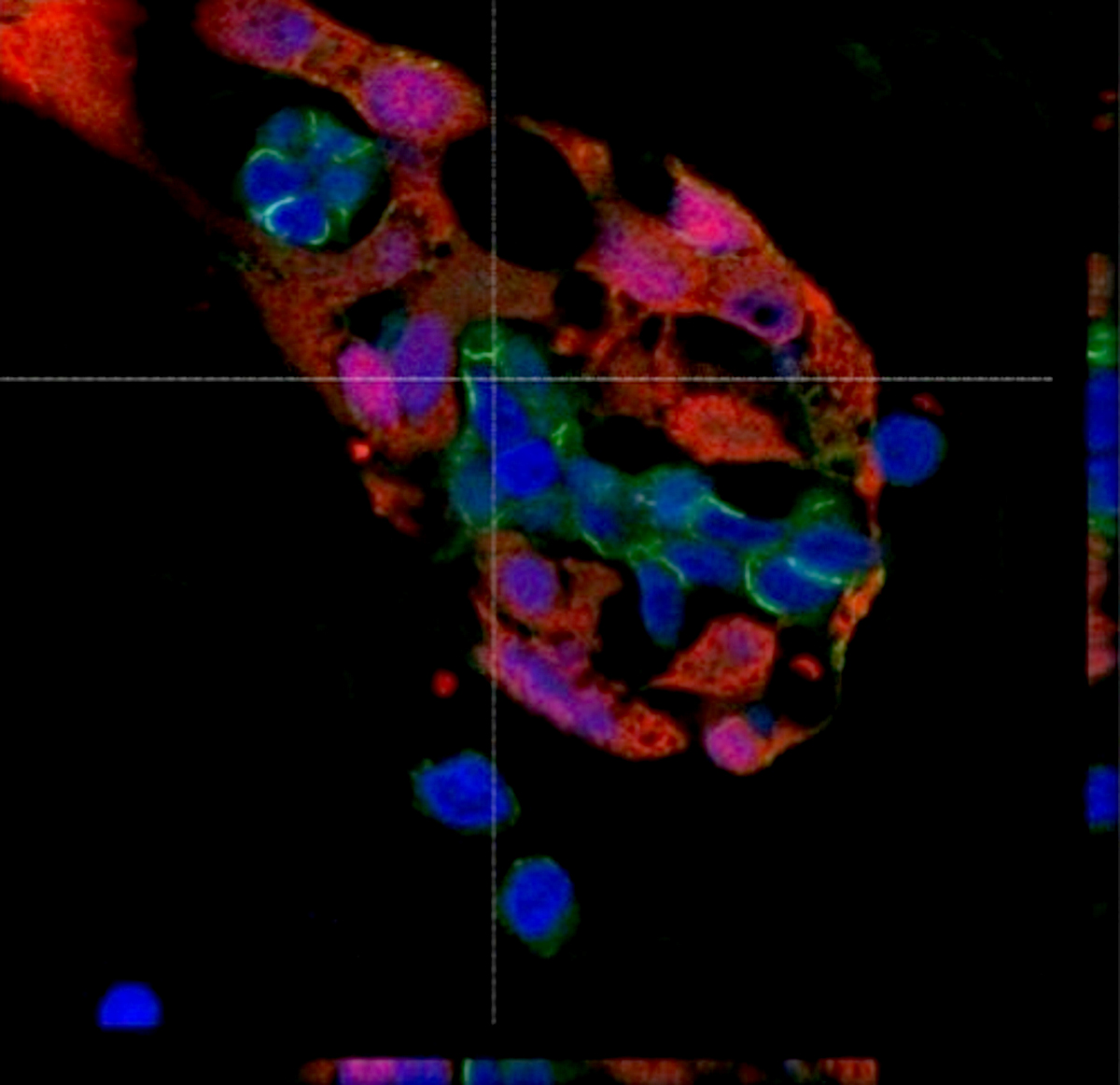
Myxoma and endothelial cells
Positive stains
- Calretinin (strong, diffuse, cytoplasmic and nuclear staining), S100, CD31 variable, CD34 variable (Heart Vessels 2018,33:1403)
- Rarely present glandular components are keratin positive (Virchows Arch 2003;443:618)
- Smooth muscle cells are alpha SMA (1A4) positive
Negative stains
- CD68 (except for associated inflammatory elements), cytokeratins (except for rare glandular elements)
Electron microscopy description
- Lepidic cells of myxoma show features of immature mesenchymal cells and are associated with endothelial and smooth muscle cells (Ultrastruct Pathol 2013;37:77)
- Lepidic cells have abundant smooth and rough endoplasmic reticulum, free ribosomes, polyribosomes, lysosomes and pinocyticvesicles, also numerous filaments and frequent iron deposits (Hum Pathol 1973;4:111)
Electron microscopy images
Contributed by Angela Pucci, M.D., Ph.D. and Giovanni Bartoloni, M.D.
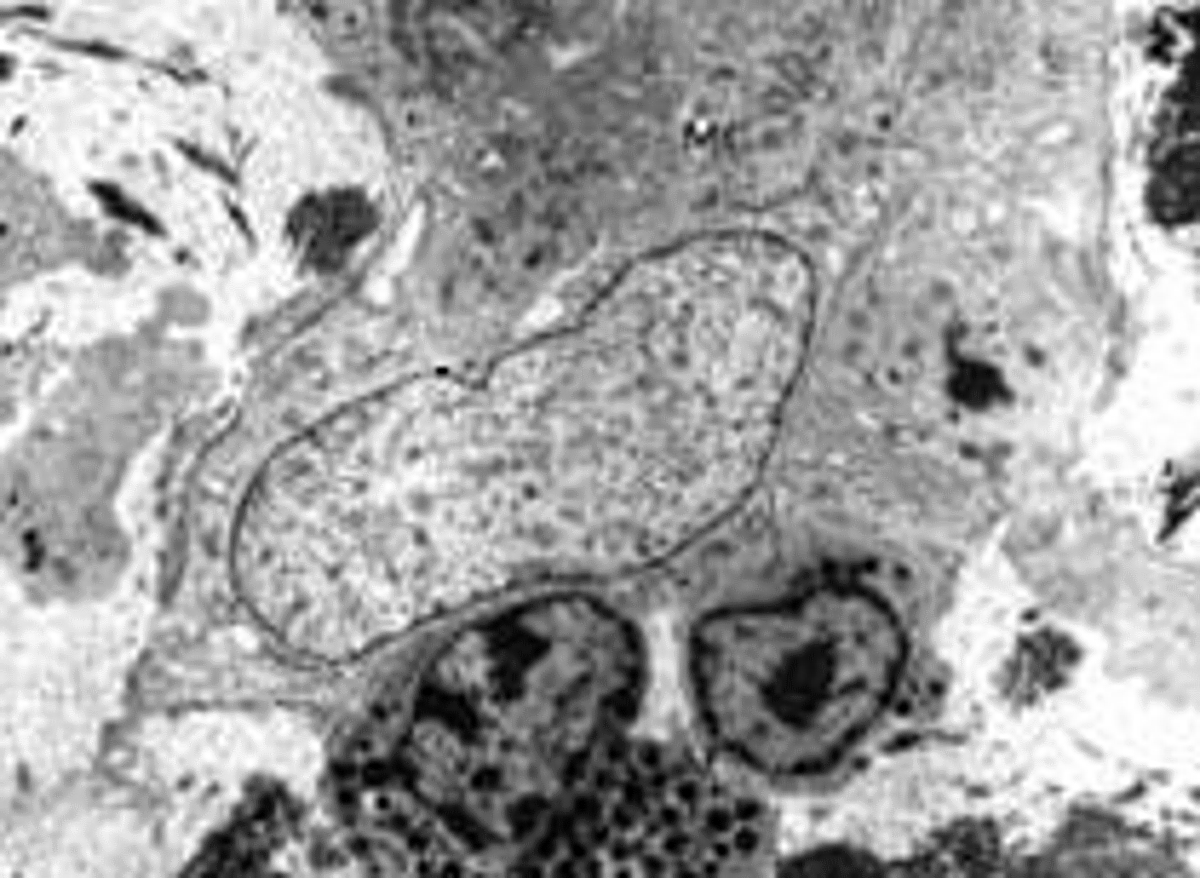
Myxoma cell
Molecular / cytogenetics description
- Expression of matrix metalloprotease (MMP) and its inhibitor (TIMP) is likely related to embolic potential (Heart Vessels 2018,33:1403, Am J Pathol 2005,166:1619)
- Carney complex is caused by heterozygous mutation of the PRKAR1A gene on chromosome 17q24, coding for the regulatory subunit type I alpha of the protein kinase A (PKA, cyclic adenosine monophosphate [cAMP] dependent protein kinase) enzyme
- PRKAR1A gene is a tumor suppressor gene
- Mutation induces haploinsufficiency, causing predisposition to tumorigenesis (OMIM: Protein Kinase, cAMP-dependent, Regulatory, Type I, Alpha; PRKAR1A [Accessed 26 April 2021])
Sample pathology report
- Left atrium, excision:
- Cardiac myxoma (see comment)
- Comment: There is a proliferation of polygonal (lepidic) cells, forming cords and nests, surrounding a central vessel or scattered within a myxoid stroma. By immunohistochemistry, the tumor cells show cytoplasmic expression of calretinin and S100, whereas they are negative for SMA, desmin and cytokeratins. Hemorrhage, calcifications and lymphoid infiltrates are abundant; glandular structures are rare. This constellation of morphological and immunohistochemical features strongly supports the diagnosis of cardiac myxoma. It may recur unless completely excised. It has embolic potential.
Differential diagnosis
- Thrombus:
- No cell nests, cords or rings
- Calretinin negative
- Metastatic carcinoma:
- Cell atypia and mitoses are present in glandular structures of metastatic adenocarcinoma
- Cardiac myxoma may have glandular structures but no mitosis or marked cell atypia is detected
- Sarcomas:
- May show prominent myxoid stroma (myxofibrosarcoma, myxoid leiomyosarcoma, myxoid liposarcoma, etc.)
- Have mitoses, cell atypia and necrosis
- Immunophenotype is usually not consistent with cardiac myxomas (J Thorac Oncol 2016;11:441)
- Papillary fibroelastoma:
- On valve cusps and is constituted by avascular papillary fronds with a fibroelastotic core and lined by endothelial cells
- Shows CD31, CD34 and factor VIII related antigen immunoreactivity
- Calretinin and S100 negative
Additional references
Board review style question #1
Regarding a cardiac myxoma, which of the following statements is true?
- Diagnostic criteria are based on the presence of myxoid stroma and lepidic cells
- Inflammatory infiltrates are uncommon
- Most patients are children
- Mostly found in the right ventricle
Board review style answer #1
A. Diagnostic criteria are based on the presence of myxoid stroma and lepidic cells
The diagnosis of cardiac myxoma, which is distinctive from soft tissue myxomas, requires the presence of the typical lepidic myxoma cells that are polygonal cells with no or mild atypia and abundant eosinophilic cytoplasm. They are arranged as single cells, nests or cordons, often around vessels, within an abundant myxoid stroma. Other findings are leukocytic infiltrates, hemorrhage, calcifications, osseous metaplasia, thymic rests or glandular structures. Most patients are between 30 and 60 years of age (mean age 50 years); cardiac myxoma can be found in younger patients and in children in rare cases, in particular in patients with Carney complex
Most cases are in the left atrium: 90% occur in atria, 75% on left side and localized to the interatrial septum and close to fossa ovalis but cardiac myxoma can be localized to any other cardiac chamber (right atrium, ventricles and valves) (J Pediatr 2013;162:964).
Comment Here
Reference: Cardiac myxoma
The diagnosis of cardiac myxoma, which is distinctive from soft tissue myxomas, requires the presence of the typical lepidic myxoma cells that are polygonal cells with no or mild atypia and abundant eosinophilic cytoplasm. They are arranged as single cells, nests or cordons, often around vessels, within an abundant myxoid stroma. Other findings are leukocytic infiltrates, hemorrhage, calcifications, osseous metaplasia, thymic rests or glandular structures. Most patients are between 30 and 60 years of age (mean age 50 years); cardiac myxoma can be found in younger patients and in children in rare cases, in particular in patients with Carney complex
Most cases are in the left atrium: 90% occur in atria, 75% on left side and localized to the interatrial septum and close to fossa ovalis but cardiac myxoma can be localized to any other cardiac chamber (right atrium, ventricles and valves) (J Pediatr 2013;162:964).
Comment Here
Reference: Cardiac myxoma
Board review style question #2
In a patient presenting with a stroke, a cardiac mass of the left atrium is shown by echocardiography. At surgery, a left atrial mass with villous projection is excised. Histology does not show necrosis or mitotic activity of the myxoid mass; calretinin is strongly expressed by the tumor cells. Which of the following is most likely the correct diagnosis?
- Cardiac myxoma
- Leiomyosarcoma
- Metastatic carcinoma
- Mesothelioma
Board review style answer #2
A. Cardiac myxoma
Cardiac myxomas are more frequently found in the left atrium and may frequently embolize, even causing stroke. Treatment requires complete surgical resection to avoid relapse and embolic or systemic symptoms. The presence of a myxoid tumor in a cardiac chamber requires histology for differential diagnosis from malignant tumors, including sarcomas, which exhibit mitotic activity, marked cell atypia, necrosis and a different immunophenotypes. Cardiac myxomas are strongly immunoreactive for calretinin and do not show significant cell atypia, necrosis or mitotic activity.
Comment Here
Reference: Cardiac myxoma
Cardiac myxomas are more frequently found in the left atrium and may frequently embolize, even causing stroke. Treatment requires complete surgical resection to avoid relapse and embolic or systemic symptoms. The presence of a myxoid tumor in a cardiac chamber requires histology for differential diagnosis from malignant tumors, including sarcomas, which exhibit mitotic activity, marked cell atypia, necrosis and a different immunophenotypes. Cardiac myxomas are strongly immunoreactive for calretinin and do not show significant cell atypia, necrosis or mitotic activity.
Comment Here
Reference: Cardiac myxoma

