

Heart & vascular pathology
Systemic conditions
Sarcoidosis
Editorial Board Members: Jefree J. Schulte, M.D., David B. Chapel, M.D.


Last author update: 8 December 2022
Last staff update: 20 July 2023
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Cardiac sarcoidosis

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Charles MGK, Glass C. Sarcoidosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/heartsarcoidosis.html. Accessed December 27th, 2024.
Definition / general
- Cardiac sarcoidosis is a type of infiltrative cardiomyopathy and a potential cause of heart failure
Essential features
- Nonnecrotizing granulomata are classic
- Presents with symptoms of cardiac dysfunction (arrhythmias, conduction disturbances)
- Often clinically silent and subsequently diagnosed on explant hearts or autopsy
Epidemiology
- Occurs in approximately 5% of patients with systemic or pulmonary manifestations of sarcoidosis (Clin Chest Med 2015;36:657)
- U.S. autopsy studies revealed cardiac manifestations in 20 - 29% of patients with systemic sarcoidosis
- Average age at presentation: 50 years old (Circulation 2015;131:624)
Sites
- Myocardium is most frequently involved
- Involvement of pericardium and endocardium usually results from extension of myocardial disease (Semin Respir Crit Care Med 2014;35:372)
Pathophysiology
- Not fully understood; some consider as spectrum of autoimmune etiology
- Nonnecrotizing granulomata are classic
- Often presents initially with local inflammation, which then progresses to fibrotic scarring; however, disease progression is highly variable (Intern Med 2014;53:1595)
Etiology
- Not fully known; however, mycobacteria, propionibacteria, Borellia, Rickettsia and herpes have been suggested as possible antigens leading to granuloma formation (Postgrad Med J 2014;90:582, Dis Mon 2009;55:649)
Clinical features
- Atrioventricular (AV) block
- Supraventricular and ventricular arrythmias
- Heart failure
- Sudden cardiac death
- Hypercalcemia
- Acute coronary syndrome, rarely (Clin Cardiol 2009;32:E68)
Diagnosis
- Electrocardiogram (ECG): PR lengthening, T wave abnormalities, Q waves
- Echocardiograms: decreased left ventricular ejection fraction, ventricular aneurysm, regional wall motion abnormality, basal septal thinning (Heart Rhythm 2014;11:1305)
- Cardiac imaging (see Radiology description)
Laboratory
- Elevated erythrocyte sedimentation rate
- Increased levels of angiotensin converting enzyme (Indian Pacing Electrophysiol J 2020;20:184)
- Hypercalcemia
- Increased levels of IL12, IL10, IL6 and interferon gamma (Front Immunol 2020;11:1443)
Radiology description
- Cardiovascular magnetic resonance imaging (CMR): multifocal areas of late gadolinium enhancement (LGE), midmyocardial and subepicardial LGE, extension of LGE from the left ventricle to the right ventricle (JACC Cardiovasc Imaging 2013;6:501, Curr Opin Pulm Med 2009;15:507)
- Fluorodeoxyglucose (FDG) PET may reveal FDG uptake, which is a nonspecific finding that indicates inflammation
Radiology images
Images hosted on other servers:

Late gadolinium enhancement (LGE)
Prognostic factors
- Prognosis is poor if complicated by heart failure
- In the U.S., 13 - 25% of deaths from sarcoidosis have been attributed to cardiac sarcoidosis (Sarcoidosis Vasc Diffuse Lung Dis 2002;19:220)
- 5 year estimate of event free survival is 70 - 80% (J Am Heart Assoc 2021;10:e019415)
- Patients with right ventricular involvement have a worse prognosis
Case reports
- 40 year old woman with dyspnea on exertion in the setting of heart failure (Cureus 2021;13:e18685)
- 49 year old woman with dyspnea and negative CMR (HeartRhythm Case Rep 2021;7:139)
- 54 year old man with fatigue and ventricular tachycardia on ECG (CASE (Phila) 2021;5:213)
- 56 year old woman with exertional chest pressure and dyspnea initially diagnosed as giant cell myocarditis (Eur Heart J Case Rep 2021;5:ytab042)
- 58 year old man currently being treated with ixekizumab for psoriasis presents with acute onset heart failure (CJC Open 2020;3:118)
Treatment
- Management largely involves treatment of underlying cardiac dysfunction and prevention of cardiovascular disease
- Patients may be candidates for cardiac transplant, pacemaker or implantable cardioverter defibrillator
- Heart failure medications and antiarrhythmics are often indicated
- Patients with evidence of current myocardial inflammation and cardiac dysfunction may be eligible for immunosuppressive medications (Chest 2012;141:154)
- Corticosteroids are the mainstay of treatment
- Methotrexate has also been suggested (J Am Heart Assoc 2019;8:e010952)
Gross description
- Diffuse myocardial infiltrates with irregular borders, which can vary from yellow to white / gray (Arch Pathol Lab Med 2010;134:1039)
- There may be ventricular dilation and aneurysms present (Virchows Arch 2011;458:671)
- If present, fibrosis may be focal or diffuse and is usually most prominent in the basal septum and left ventricular free wall
- Pericardial thickening
Gross images
Images hosted on other servers:

Myocardial infiltrates
Microscopic (histologic) description
- Nonnecrotizing granulomas and multinucleated giant cells in transmural or focal distribution (Clin Cardiol 2018;41:1386)
- Giant cell inclusions may be present
- Schaumann bodies: oval, concentrically laminated intracytoplasmic inclusions
- Asteroid bodies: stellate shaped with cytoplasmic clearing
- Giant cell inclusions may be present
- Transmural or focal interstitial fibrosis (Arch Pathol Lab Med 2010;134:1039)
- Small coronary arteries may be involved
Microscopic (histologic) images
Contributed by Carolyn Glass, M.D., Ph.D.
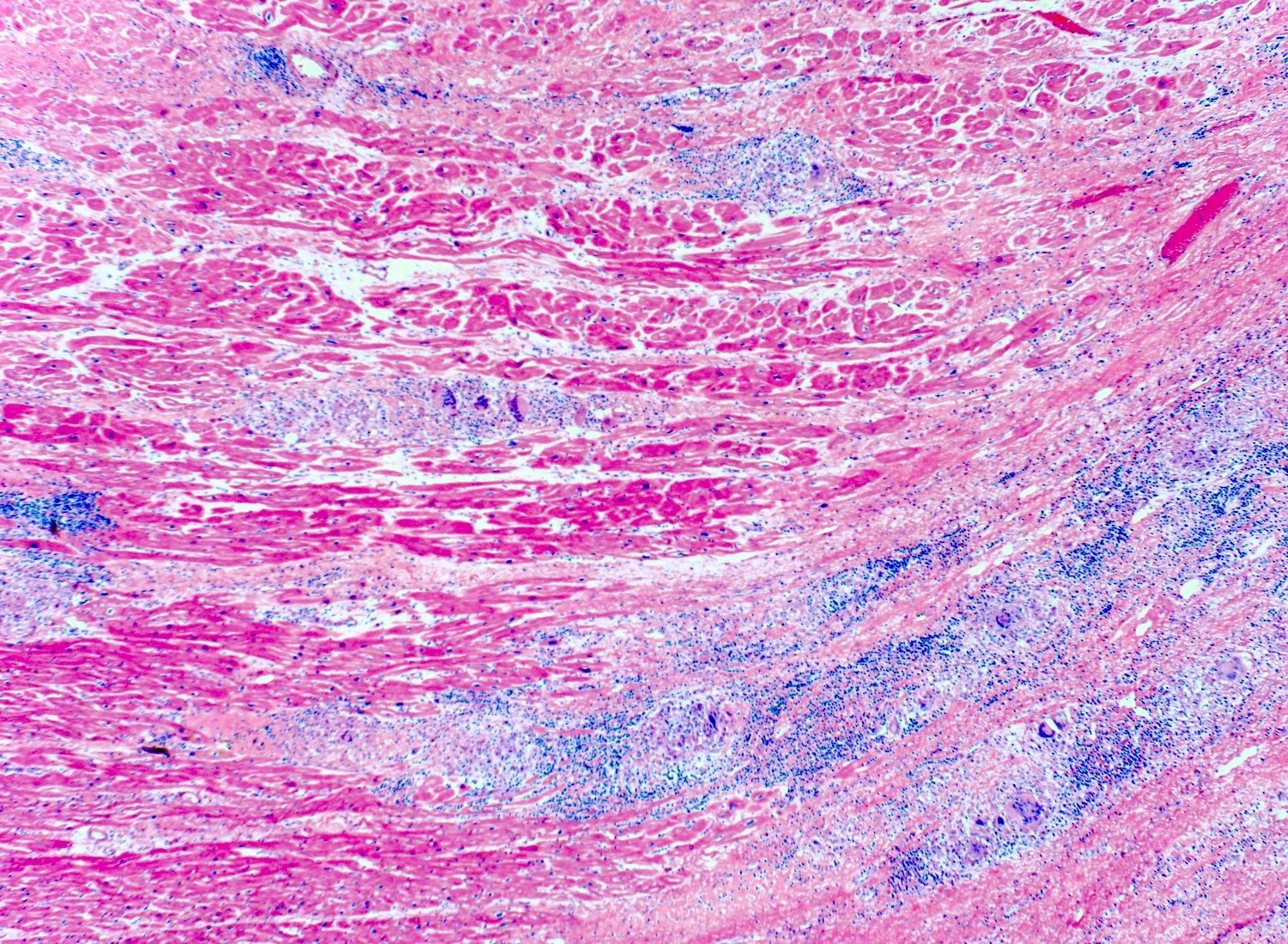

Cardiac biopsy
Sample pathology report
- Heart, left ventricle, endomyocardial biopsy:
- Cardiac sarcoidosis (see comment)
- Comment: Biopsy contains several well formed granulomas with multinucleated giant cells containing intracytoplasmic inclusions. Moderate fibrosis is present. Microscopic appearance consistent with clinical diagnosis of cardiac sarcoidosis.
Differential diagnosis
- Foreign body granulomas:
- Granulomas are not well formed
- Polarized light reveals foreign material
- Giant cell myocarditis:
- Not associated with systemic disease
- Granulomas are not well formed
- Eosinophils
- Fibrosis not seen acutely
- Fungal / mycobacterial infections:
- Lyme carditis:
- Transmural lymphocytic inflammation
- No granulomas
- Other symptoms of systemic lyme disease present
Board review style question #1
A 40 year old woman presented with dyspnea on exertion and several pulmonary nodules seen on a prior abdominal CT scan. Additional CT scan of the chest showed cardiomegaly and subsequent endomyocardial biopsy revealed the histology seen above. What is the diagnosis?
- Amyloidosis
- Giant cell myocarditis
- Hemochromatosis
- Sarcoidosis
Board review style answer #1
D. Sarcoidosis. This patient has nonnecrotizing granulomas on cardiac biopsy. In the setting of pulmonary nodules on prior imaging, this most likely represents sarcoidosis with cardiac involvement. Her shortness of breath may represent development of heart failure.
Comment Here
Reference: Sarcoidosis
Comment Here
Reference: Sarcoidosis
Board review style question #2
A 28 year old woman with no significant medical history presents with dizziness. On further questioning, the patient describes a sensation of blacking out. Electrocardiogram (ECG) is performed and reveals sinus rhythm with PR prolongation. Chest Xray reveals bilateral lung opacities. What is the diagnosis?
- Coronary artery disease
- Hyperthyroidism
- Sarcoidosis
- Viral myocarditis
Board review style answer #2
C. Sarcoidosis. This patient likely has presyncope due to conduction abnormalities, as evidenced by atrioventricular (AV) block on ECG. In the setting of lung opacities on chest Xray and with no other explanation for AV block in this young patient who is otherwise healthy, this is most likely due to sarcoidosis with cardiac involvement.
Comment Here
Reference: Sarcoidosis
Comment Here
Reference: Sarcoidosis

