
Fallopian tubes & broad ligament
Fallopian tube epithelial tumors
Serous borderline tumor
Editorial Board Member: Lucy Ma, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 21 August 2024
Last staff update: 2 January 2025
Copyright: 2024-2025, PathologyOutlines.com, Inc.
PubMed search: Serous borderline tumor


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Hamilton C, Atwi D, Hassell LA. Serous borderline tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/fallopianserousborderlinetumor.html. Accessed April 2nd, 2025.
Definition / general
- Serous borderline tumor (SBT) of the fallopian tube is a low grade, proliferative serous epithelial neoplasm that is by definition noninvasive (Pan Afr Med J 2019;32:129)
Essential features
- Serous borderline tumor arising in the fallopian tube is a rare entity with fewer than 20 cases in the literature
- Microscopically similar to SBT arising in the ovary, with numerous papillae of varying size arborizing down to smaller papillae
- Hobnailing may also be present
Terminology
- Serous borderline tumor is currently the sole recommended term for primary fallopian tumors
- Not recommended: atypical proliferative serous tumor (Am J Surg Pathol 2011;35:1605)
ICD coding
- ICD-O: 8442/1 - serous borderline tumor, NOS
- ICD-11: 2C74.Y & XH3ZK9 - other specified malignant neoplasms of fallopian tube & serous cystadenoma, borderline malignancy
Epidemiology
- Serous borderline tumor of the fallopian tube is a rare neoplasm with fewer than 20 cases reported in the literature (Arch Gynecol Obstet 2011;283:349)
- Age range is broad, from 22 to 83 years (BMC Cancer 2005;5:129)
Sites
- Fallopian tube
Pathophysiology
- Theorized to arise from papillary hyperplasia of the fallopian tube (Histopathology 2013;62:44)
- May similarly be related to BRAF V600E mutation as in serous borderline tumor of the ovary (J Natl Cancer Inst 2003;95:484)
Etiology
- Unknown
Clinical features
- Nonspecific; may be asymptomatic or may have abdominal pain (Obstet Gynecol Sci 2014;57:334)
Diagnosis
- Adnexal mass may be noted on routine gynecologic exam
- Ultrasound findings may reveal cystic mass near ovary
- On laparoscopy, dilated fallopian tube or hematosalpinx may be noted (BMC Cancer 2005;5:129)
Laboratory
- Generally, CA125 levels are normal (Pan Afr Med J 2019;32:129)
Radiology description
- Hypoechogenic cystic mass on ultrasound, sometimes with intramural papillary projections (Pan Afr Med J 2019;32:129)
Radiology images
Images hosted on other servers:

Ultrasound / CT paratubal mass
Prognostic factors
- Prognosis is excellent with surgical removal (Clin Case Rep 2023;11:e7140)
Case reports
- 25 year old woman with lower abdominal pain and abdominal mass (Obstet Gynecol Sci 2014;57:334)
- 30 year old woman with a 1 year history of pelvic pain (Clin Case Rep 2023;11:e7140)
- 61 year old woman with a left fallopian paratubal cyst (Pan Afr Med J 2019;32:129)
Treatment
- Too few cases to determine optimal treatment; however, most commonly treated through conservative surgical management via salpingectomy or salpingo-oophorectomy for fertility preservation purposes
- At times includes hysterectomy for staging (Obstet Gynecol Sci 2014;57:334)
Clinical images
Images hosted on other servers:

Right fallopian tube cyst
Gross description
- Received from surgery as cystic mass or distended fallopian tube
- Cut surface
- Multiloculated cystic mass
- Intralocular papillary projections
- Filled with serous fluid
- References: Obstet Gynecol Sci 2014;57:334, Pan Afr Med J 2019;32:129
Gross images
Images hosted on other servers:

Fallopian tube cystic mass
Frozen section description
- Gross intraoperative evaluation
- Solid areas and papillary excrescences should be evaluated histologically
- Histologic intraoperative evaluation
- Bulbous papillae branching into smaller papillae on lower power
- Hobnailing or epithelial tufting
- Comparable to serous borderline tumor of the ovary
- Reference: Gynecol Oncol 2011;123:517
Frozen section images
Contributed by Lewis A. Hassell, M.D. (source: Digital Pathology Association)

Bulbous branching papillae
Microscopic (histologic) description
- Serous borderline tumors of the fallopian tube closely resemble their ovarian counterparts
- Architecture
- Numerous papillae of variable size and width (Obstet Gynecol Sci 2014;57:334)
- These papillae occupy a variable extent of a cyst lined by pseudostratified epithelium
- Larger papillae arborize down to smaller papillae which terminate in epithelial clusters or single cells
- Hobnailing or epithelial tufting
- Cytologic features
- Ciliated cells that are cuboidal to columnar
- Up to moderate atypia: cellular enlargement, coarse chromatin, small nucleoli may be present, minimal mitotic activity
Microscopic (histologic) images
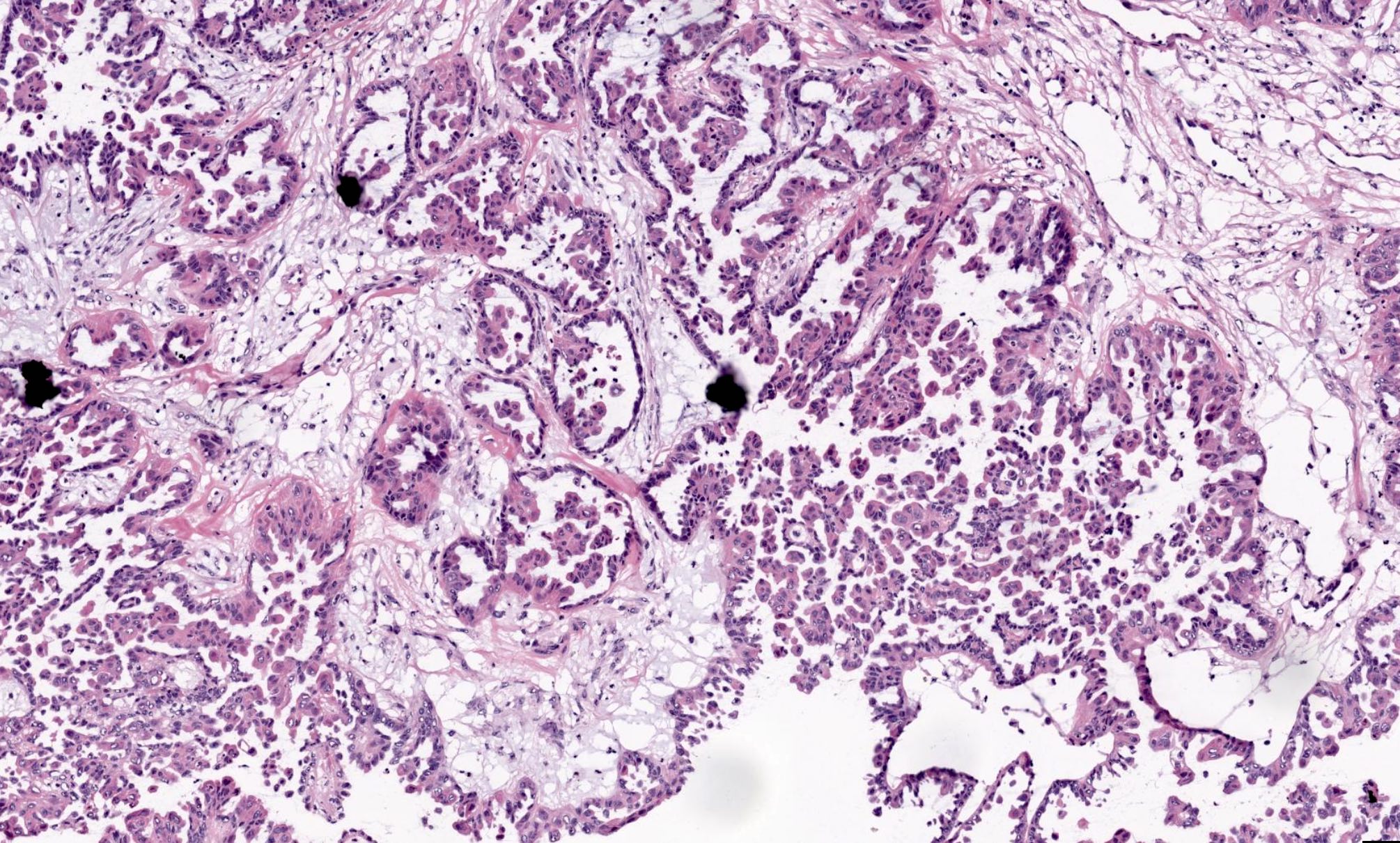
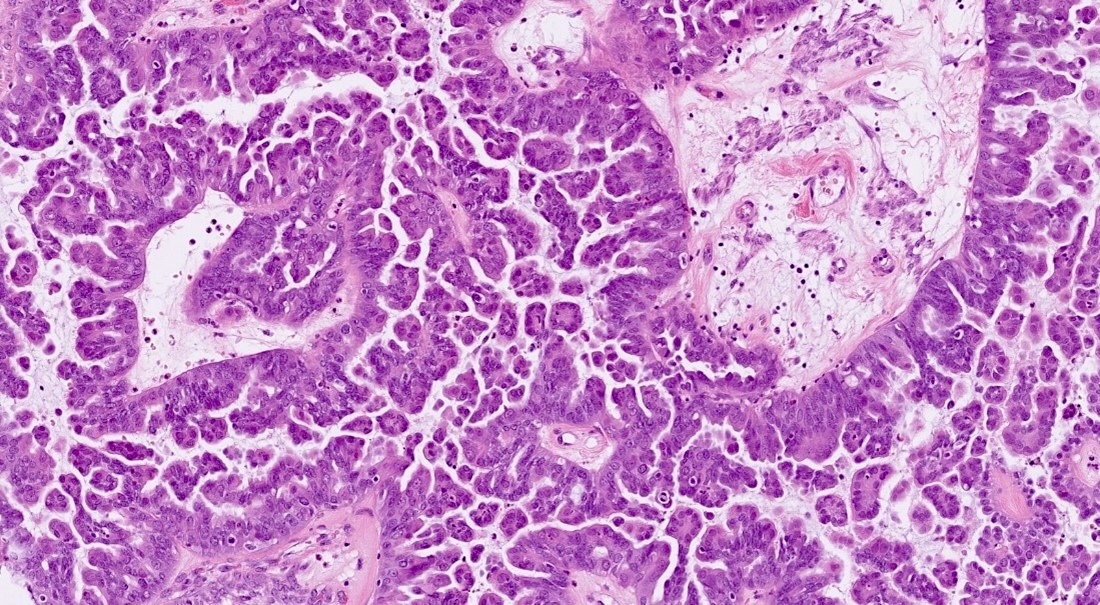
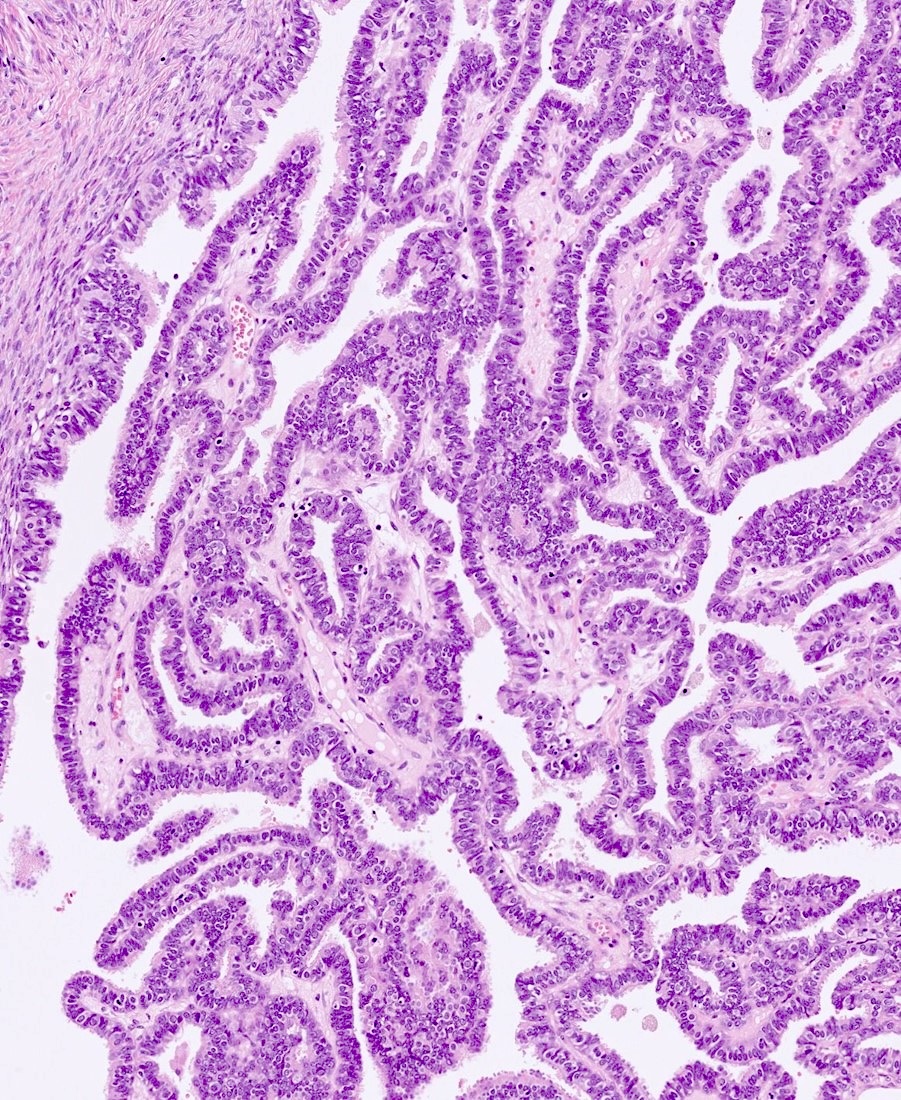
Contributed by Chad Hamilton, D.O., Lewis A. Hassell, M.D. and Anna Måsbäck, M.D., Ph.D.



Psammomatous calcifications

Arborizing papillae
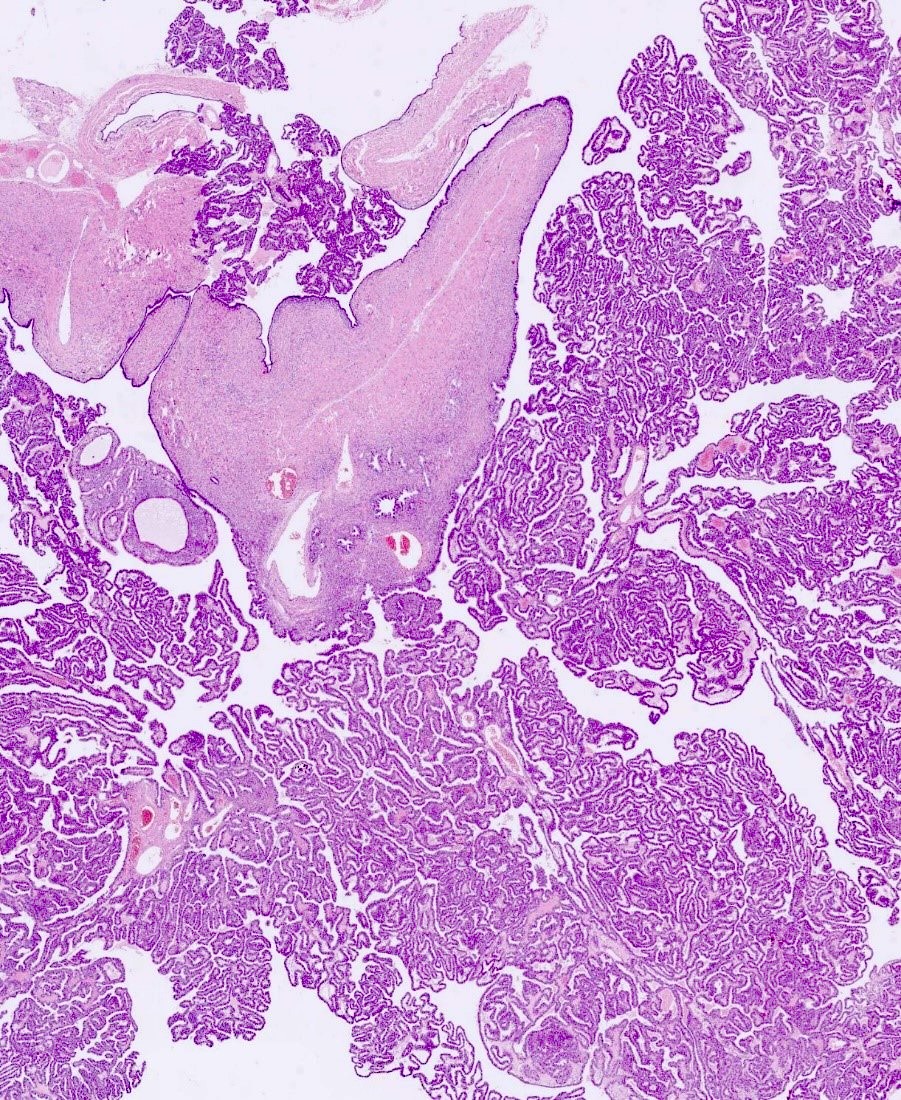
Variably sized papillae

Ciliated cells with hobnailing
Arborizing papillae
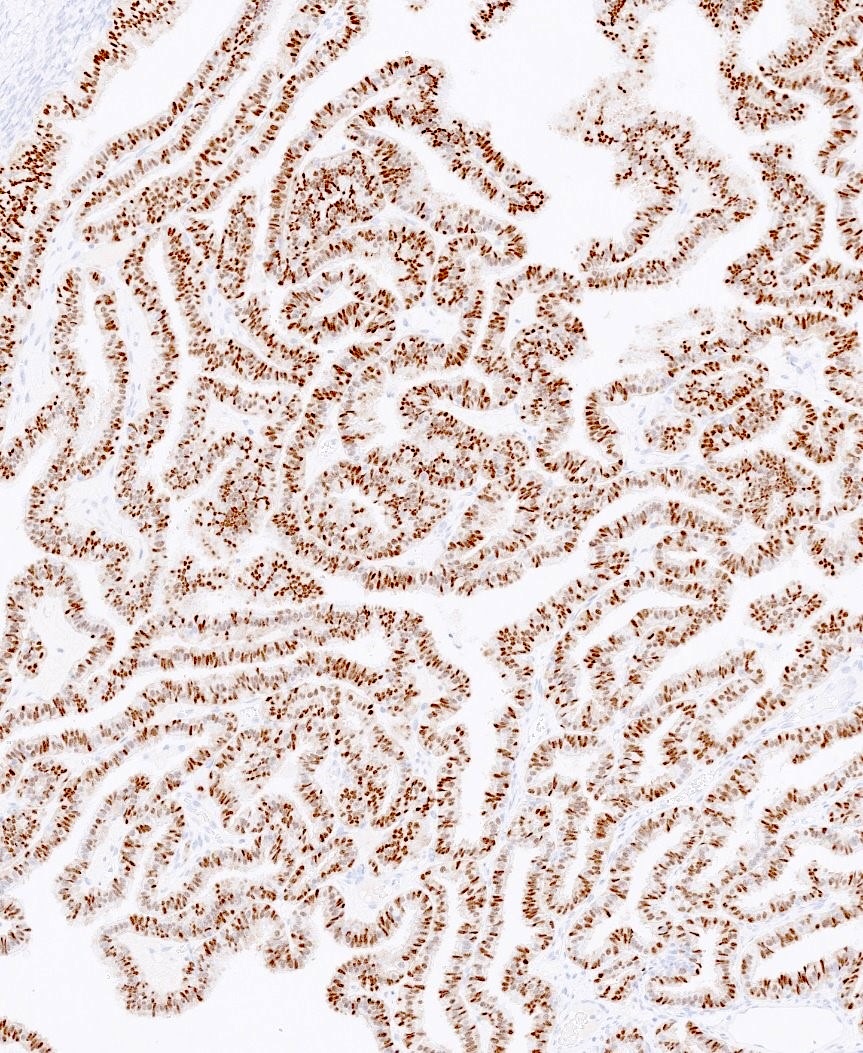
PAX8
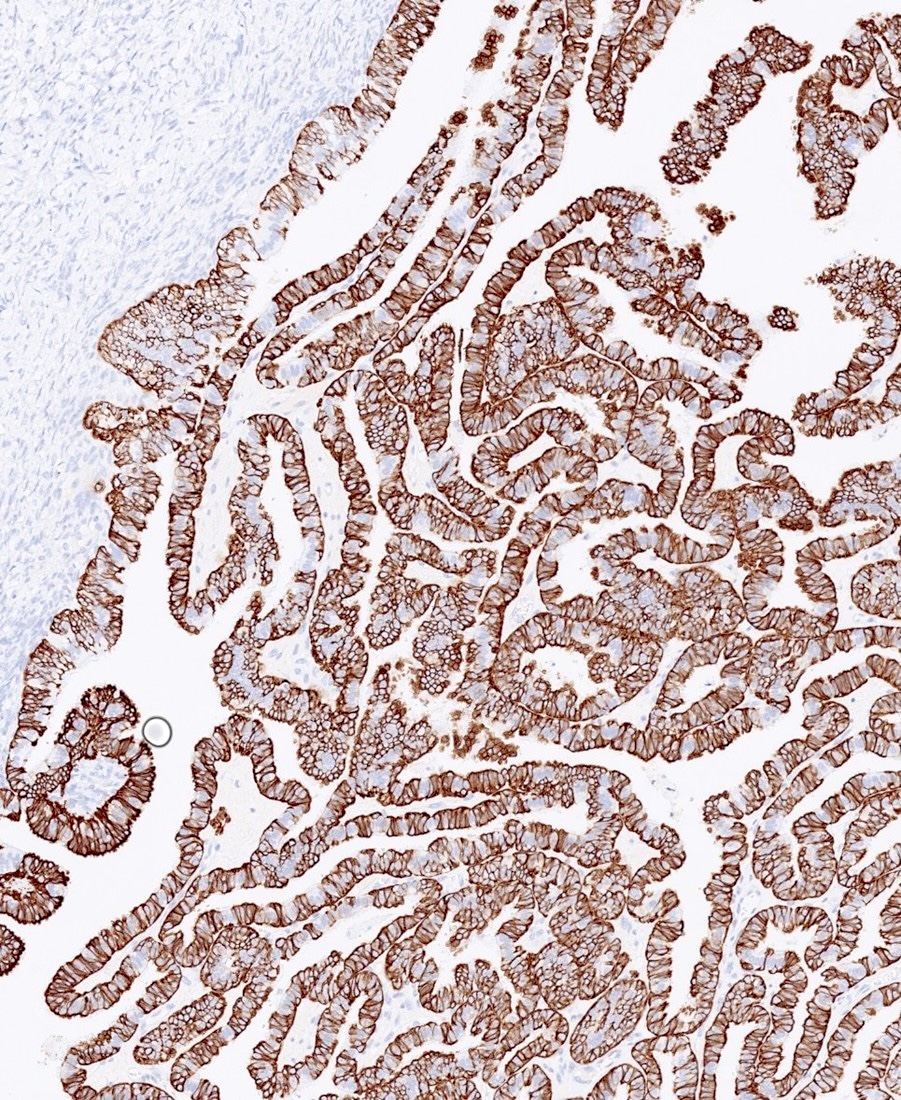
CK7
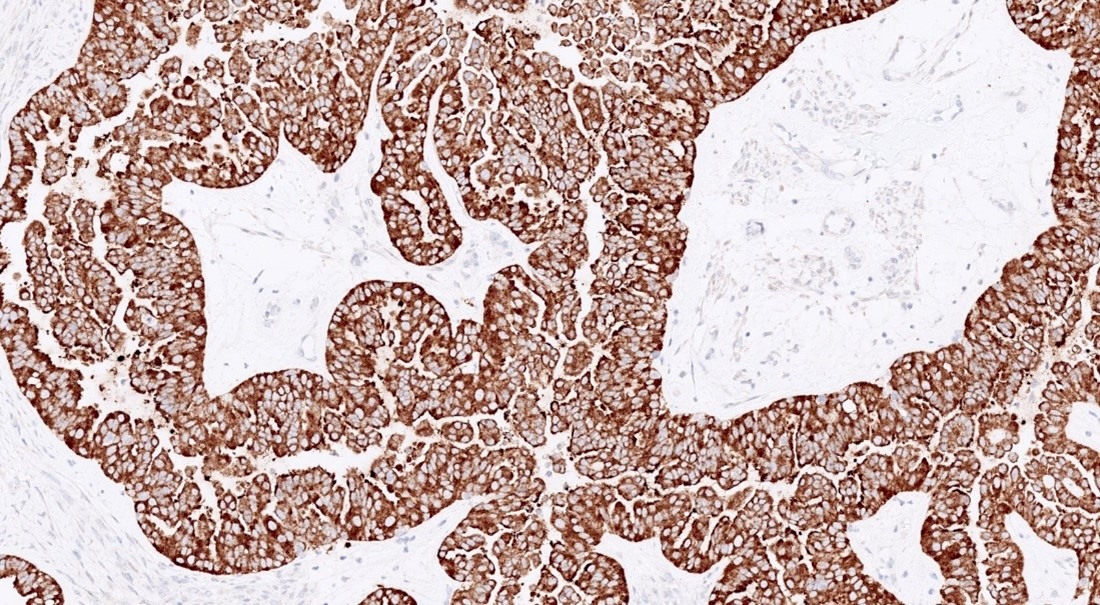
BRAF
Virtual slides
Images hosted on other servers:

SBT with micropapillary features
Sample pathology report
- Right fallopian tube and ovary, right salpingo-oophorectomy:
- Serous borderline tumor of the fallopian tube (8.5 cm) without surface involvement (see comment)
- Other organ involvement: not identified
- Comment: Immunohistochemical stains performed with adequate controls on sections of the right ovarian tumor show the tumor cells to be diffusely positive for PAX8, WT1, ER and PR, with focal / weak expression of p53 (wild type expression) and patchy positivity for p16. The combined morphologic and immunohistochemical findings support the above diagnosis.
Differential diagnosis
- Endosalpingiosis:
- Minimal architectural complexity or cytologic atypia
- Psammomatous calcifications may be present; rarely larger than a few millimeters
- Serous cystadenoma / cystadenofibroma:
- No architectural complexity (e.g., papillae, micropapillae, cribriforming or nesting)
- If there is architectural complexity but it constitutes < 10% of overall tumor then it is a serous cystadenoma / cystadenofibroma with focal epithelial proliferation
- Heterogenous population of ciliated and secretory cells but without atypia or mitoses
- Serous borderline tumor with intraepithelial / microinvasive carcinoma:
- Significant cytologic atypia and or evidence of invasion of stroma
- Usually micropapillary
- Clear cell carcinoma:
- Admixture of tubulocystic, papillary and solid architecture
- Clear cytoplasm
- High grade nuclei
- Napsin A positivity, loss of hormonal markers
Board review style question #1
The mass shown in the image above was identified in the fallopian tube of a 49 year old woman. What is the most appropriate diagnosis?
- High grade serous carcinoma
- Mesothelioma
- Paratubal cyst
- Serous borderline tumor arising from the fallopian tube
- Well differentiated endometrioid carcinoma
Board review style answer #1
D. Serous borderline tumor arising from the fallopian tube. Serous borderline tumor is far more commonly located in the ovary; however, it can also arise in the fallopian tube. Answer A is incorrect because the image does not display high grade features. Answers B, C and E are incorrect because the histology findings are more consistent with those of a serous borderline tumor.
Comment Here
Reference: Serous borderline tumor
Comment Here
Reference: Serous borderline tumor
