



Fallopian tubes & broad ligament
Broad ligament miscellaneous tumors
STK11 adnexal tumor
Editorial Board Member: David B. Chapel, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 10 June 2024
Last staff update: 10 June 2024
Copyright: 2023-2024, PathologyOutlines.com, Inc.
PubMed search: STK11 adnexal tumor


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Elgenaid SN, Hassell LA. STK11 adnexal tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/fallopianSTK11adnexaltumor.html. Accessed July 15th, 2024.
Definition / general
- Aggressive tumor that arises in paratubal / paraovarian soft tissues, has variable morphology and immunohistochemistry and harbors pathognomonic alterations in STK11
Essential features
- Associated with Peutz-Jeghers syndrome in ~50% of cases
- STK11 alterations
- Adnexal or paratubal mass
ICD coding
- ICD-10: C57.4 - malignant neoplasm of uterine adnexa, unspecified
Epidemiology
- Age: wide range from middle age to elderly (mean: 40 years old) (Am J Surg Pathol 2021;45:1061)
- Rare pediatric case (16 years old) has been reported (Pediatr Dev Pathol 2023;26:486)
Sites
- Paratubal (most common)
- Fallopian tubes
- Ovaries
- Uterine serosa
- Less commonly, the abdomen and pelvis
- Reference: Am J Surg Pathol 2021;45:1061
Pathophysiology
- Associated with Peutz-Jeghers syndrome in ~50% of cases
- Can be sporadic
- Histogenesis of this tumor (Wolffian versus sex cord stromal versus epithelial or mesothelial origins) remains uncertain (Am J Surg Pathol 2021;45:1061)
- Reference: Pediatr Dev Pathol 2023;26:486
Clinical features
- Abdominal / pelvic pain or mass
- Abdominal distension
- Urinary tract symptoms
- Abnormal uterine bleeding
- Can be incidental finding
- Metastatic tumor at presentation (50%)
- Reference: Am J Surg Pathol 2021;45:1061
Diagnosis
- Pelvic ultrasound or magnetic resonance imaging (MRI) and histopathologic diagnosis
Prognostic factors
- Recurrences at 3 - 79 months (mean: 29) after initial diagnosis, most commonly in the omentum, abdominal wall, peritoneum and pelvis
- Metastasis: most commonly to omentum and uterine serosa; less commonly to bladder peritoneum, anterior abdominal wall, small bowel, liver, paraaortic lymph node and pouch of Douglas
- Reference: Am J Surg Pathol 2021;45:1061
Case reports
- 16 year old girl with large, bilateral, solid and cystic adnexal masses (Pediatr Dev Pathol 2023;26:486)
- 29 year old woman peritubal neoplastic lesion with STK11 mutation and response to mTOR inhibitor (Gynecol Oncol Rep 2021;37:100838)
- 22 cases of paratubal adnexal tumors that harbored STK11 alterations (Am J Surg Pathol 2021;45:1061)
Treatment
- Surgery with or without chemotherapy or radiation (Gynecol Oncol Rep 2021;37:100838)
Clinical images
Images hosted on other servers:

Laparoscopic findings
Gross description
- Adnexal mass that ranges from 4.5 to 25.5 cm in size (mean: 12.4 cm)
- Solid, cystic or both
- Variable in color (tan, white, gray, yellow, pink)
- Hemorrhage and necrosis are often present
- Reference: Am J Surg Pathol 2021;45:1061
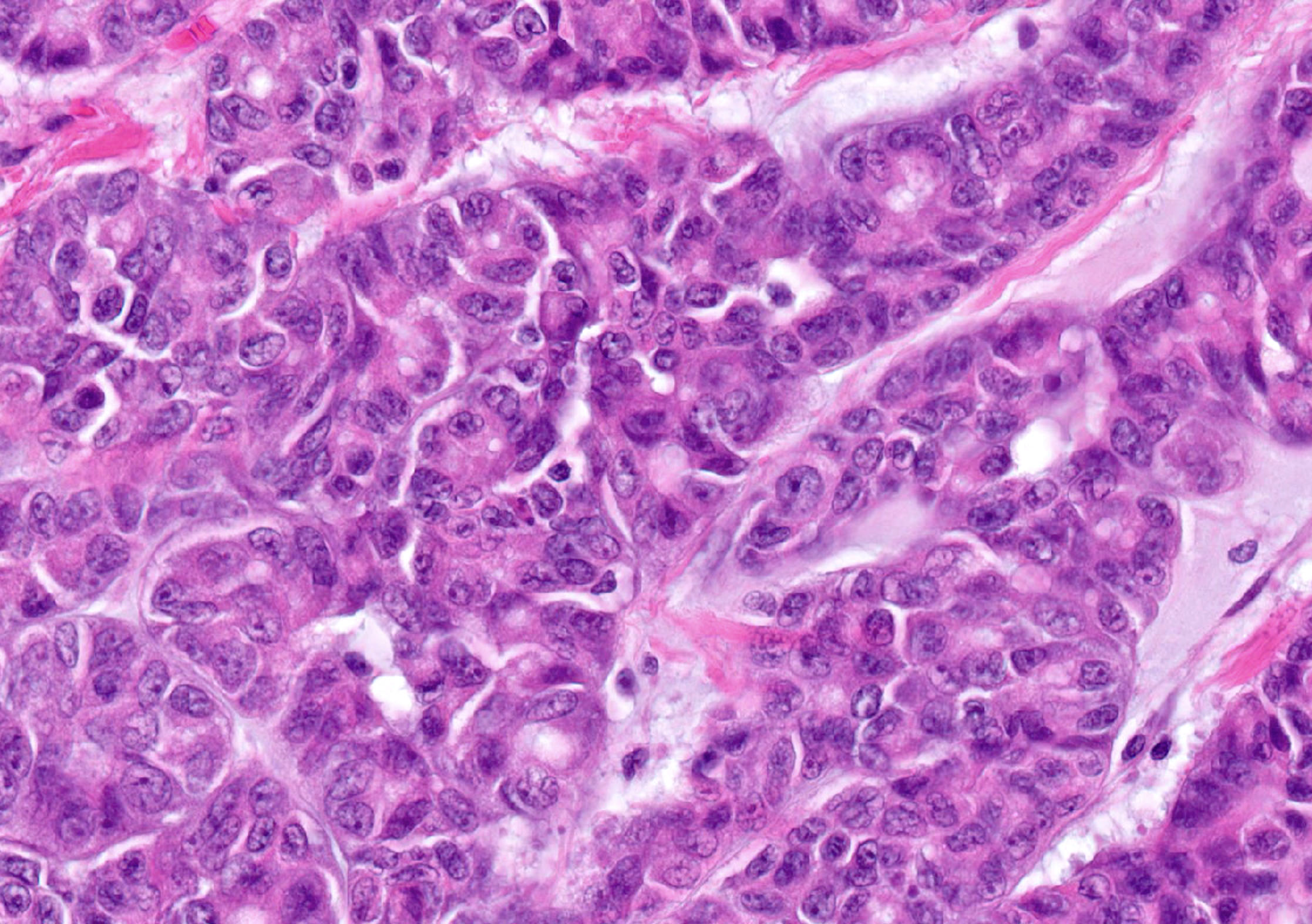
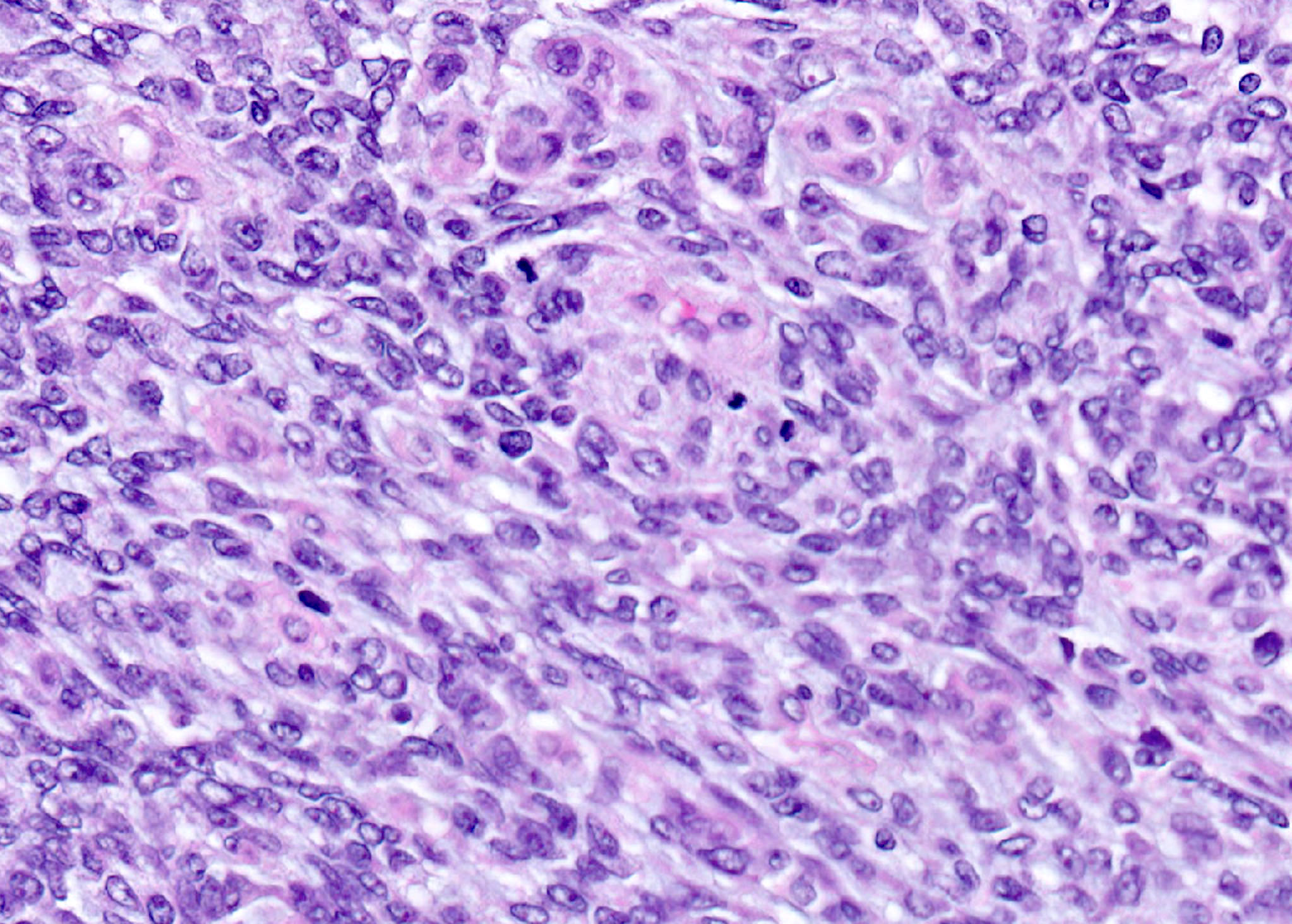
Microscopic (histologic) description
- Mixed architectural patterns are characteristically present within a single tumor and may be key to recognition
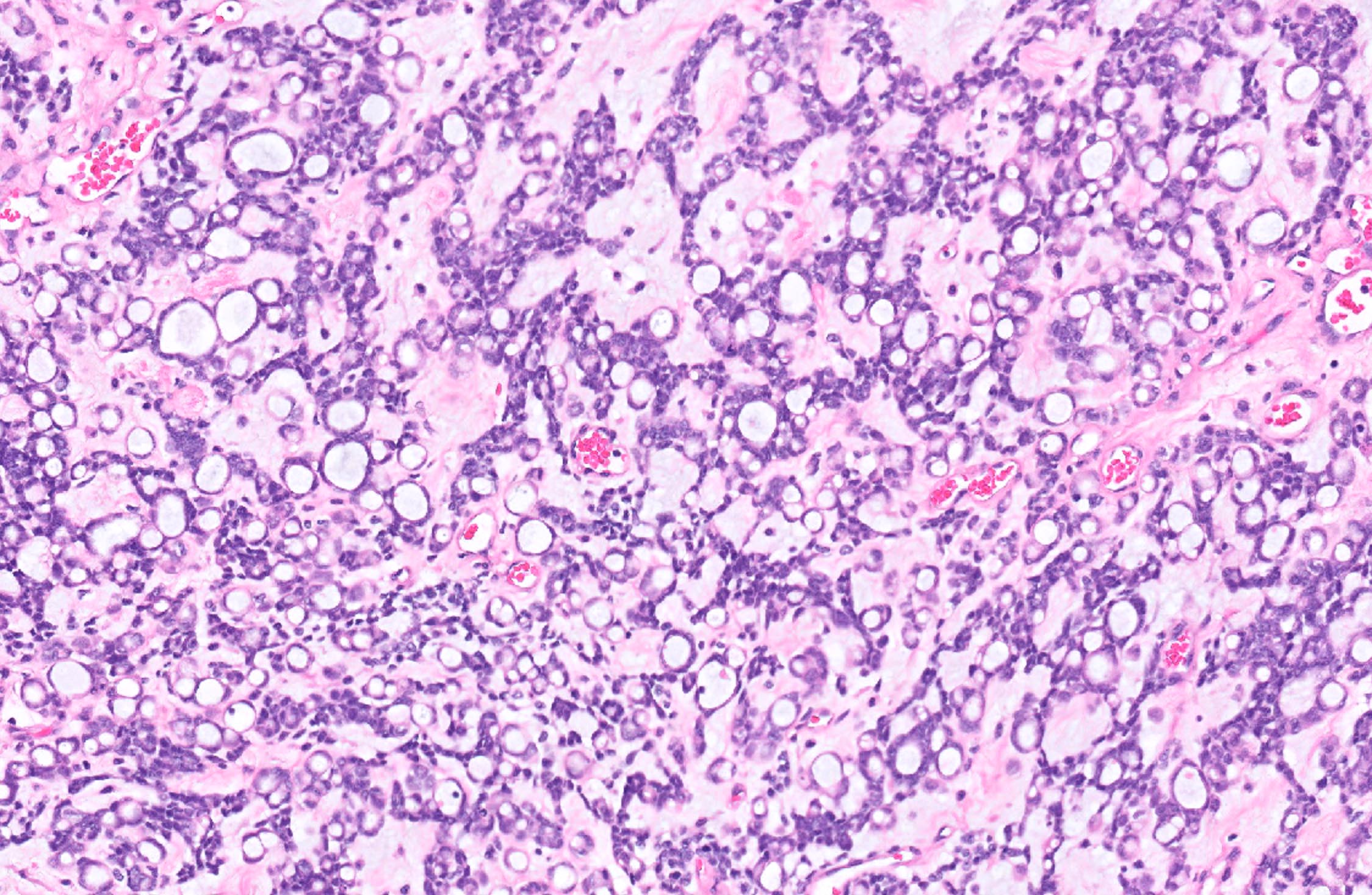
- Architecture
- Interanastomosing cords and trabeculae that can form tubular, cystic, cribriform or microacinar architecture
- Solid growth, large nests, broad columns or nodules of varying sizes
- Whorling tumor cells with vaguely glomeruloid appearance
- Focal macrofollicular pattern, pseudofollicular, papillary or pseudopapillary growth
- Villoglandular configuration
- Focally dilated glands or salivary gland type
- Basophilic secretions
- Stroma
- Prominent myxoid stroma (Am J Surg Pathol 2021;45:1061)
- Other ranges from scant to abundant and is either edematous, loosely collagenous or rarely hyalinized
- Cell morphology
- Mostly, columnar to cuboidal cells but a spindled morphology can be seen
- Nuclei are round to ovoid with irregular, often angulated contours and vesicular chromatin
- Prominent nucleoli and inconspicuous nuclear grooves
- Cytoplasm can be eosinophilic, finely vacuolated or clear
- Rarely, squamoid or signet ring-like appearance
- No overt pleomorphism
- Other
- Mitoses range from 2 to 20 (mean: 10) per 10 high power fields
- Incidental findings: sex cord tumor with annular tubules
- References: Pediatr Dev Pathol 2023;26:486, Am J Surg Pathol 2021;45:1061
Microscopic (histologic) images
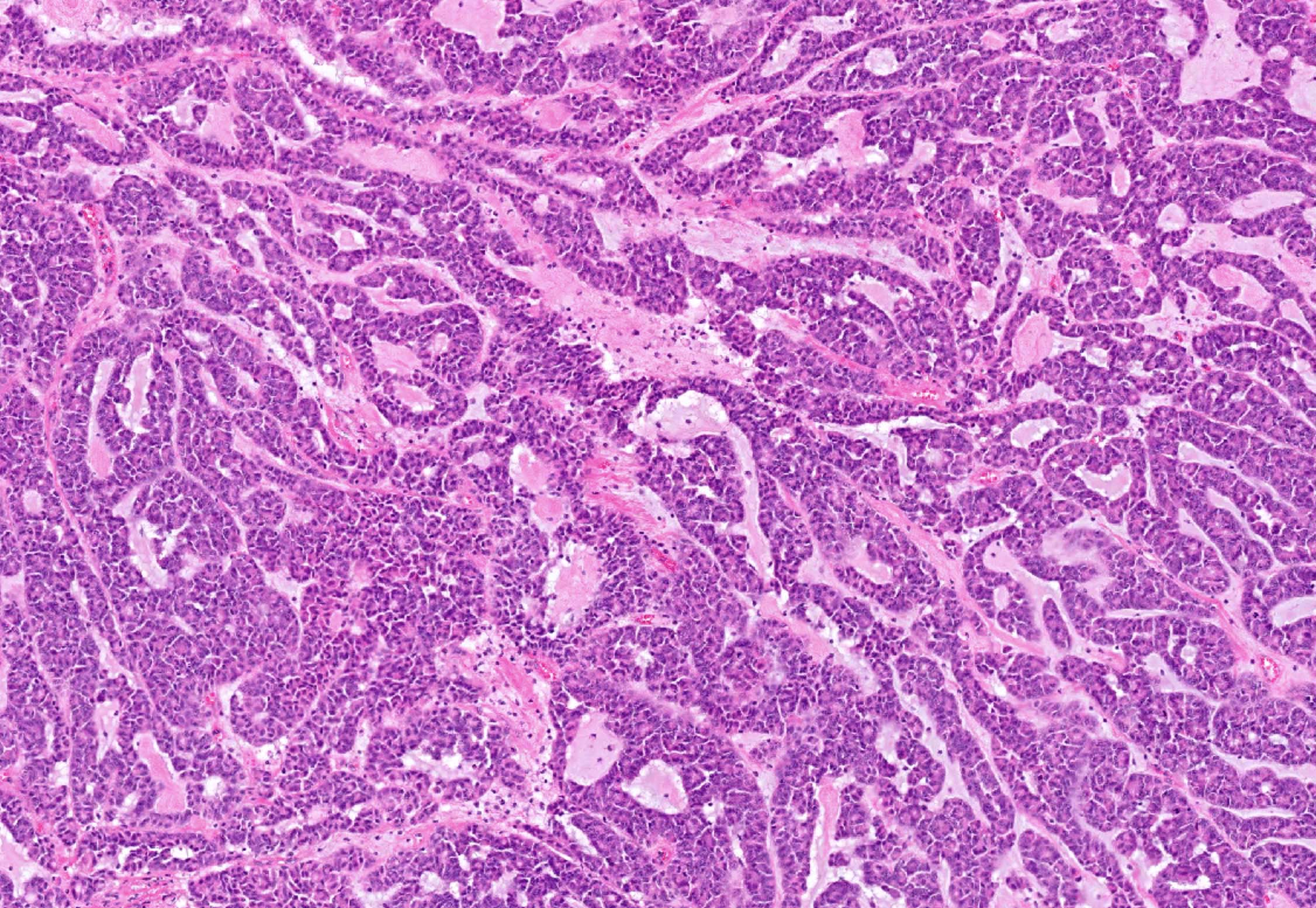
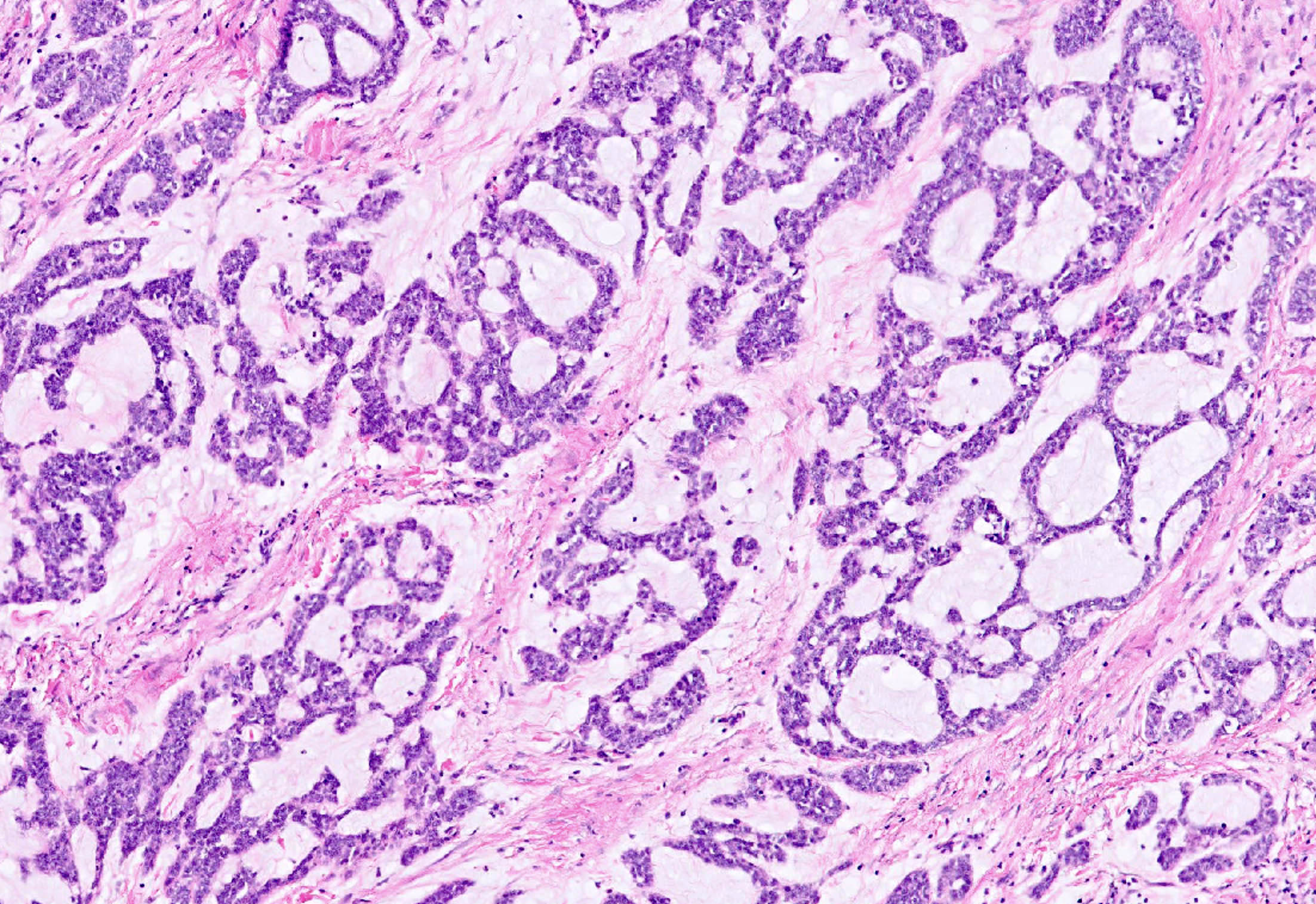
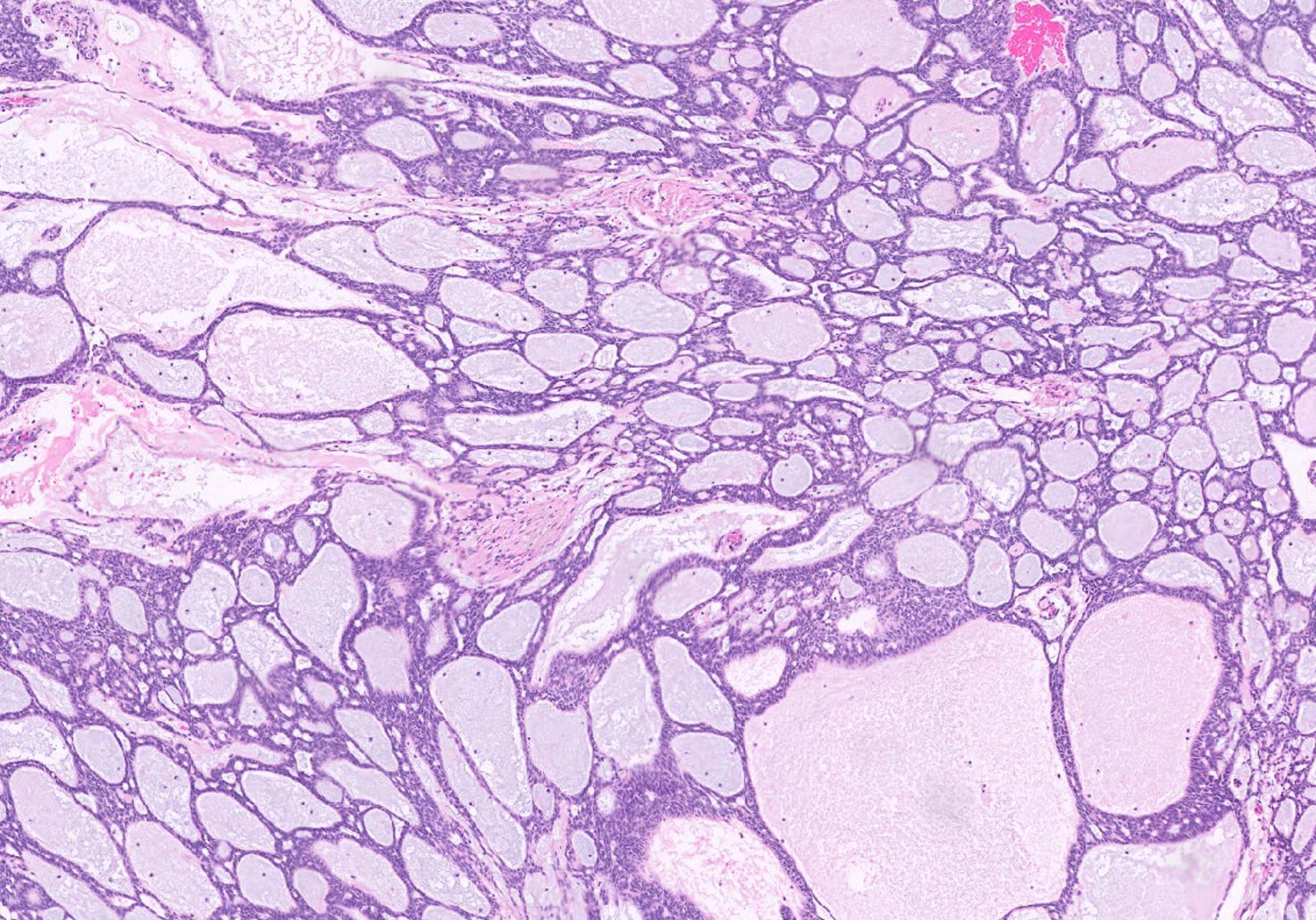
Contributed by Jennifer A. Bennett, M.D.
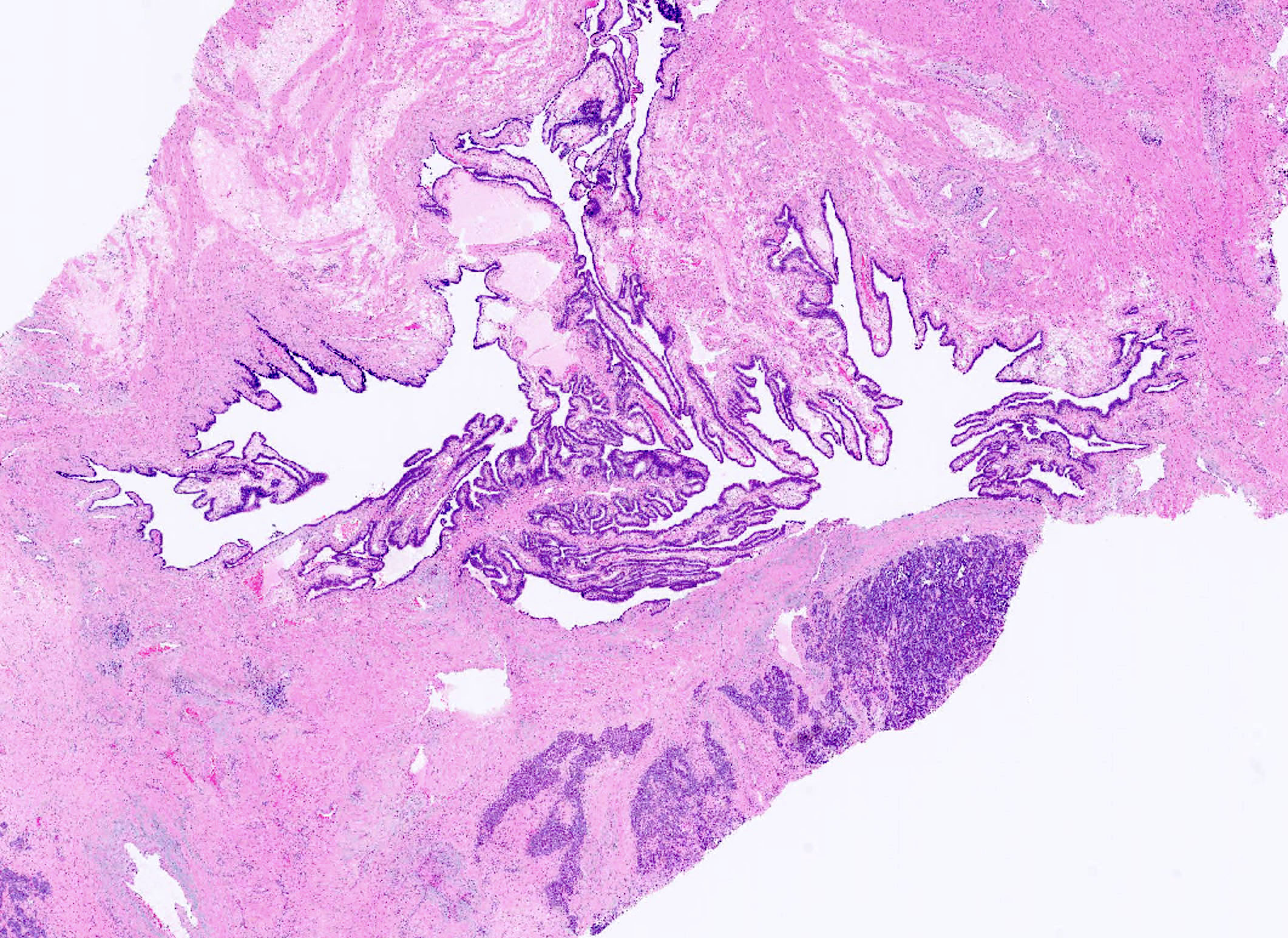
Paratubal location
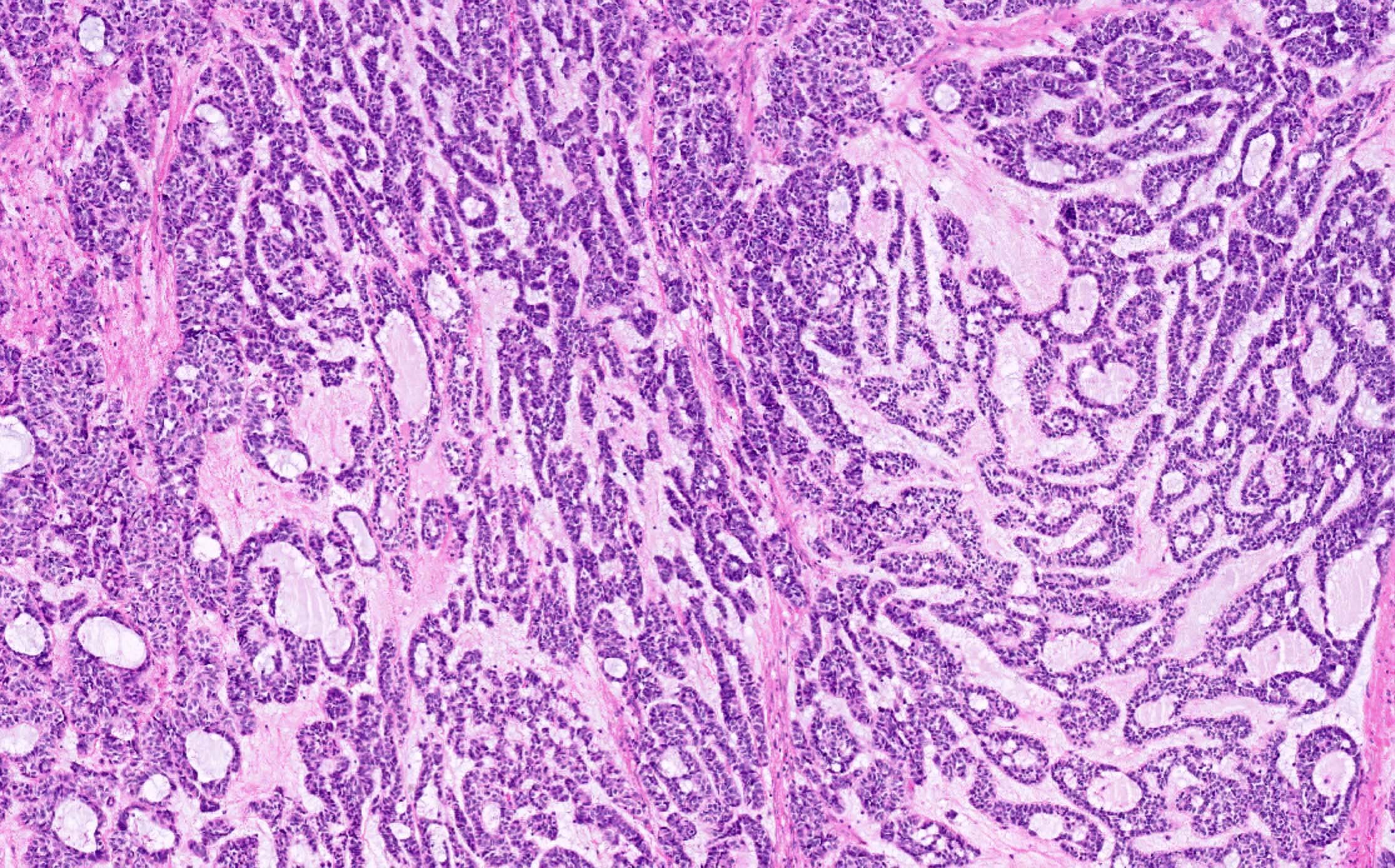
Cord and trabeculae architecture
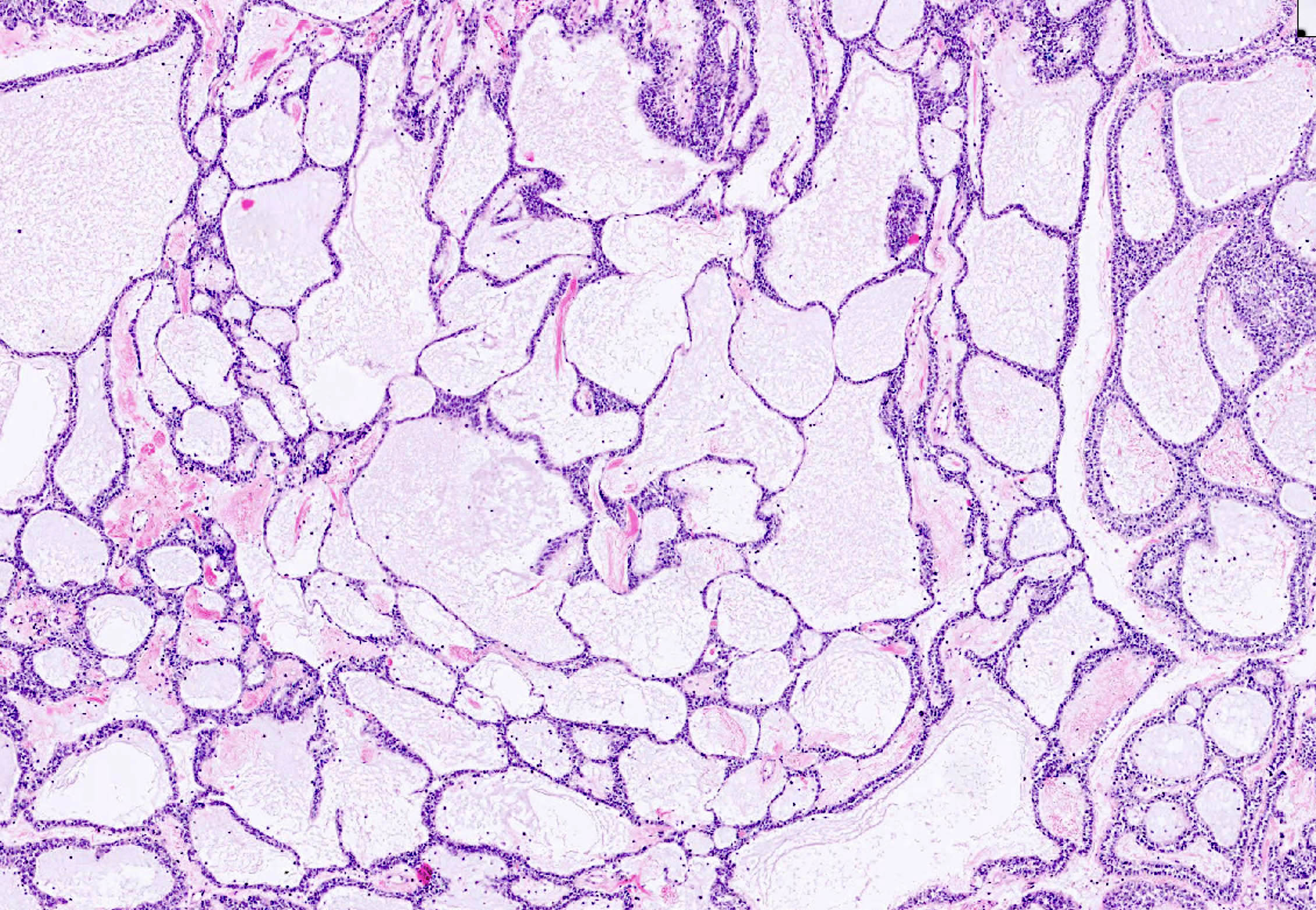
Cystic architecture
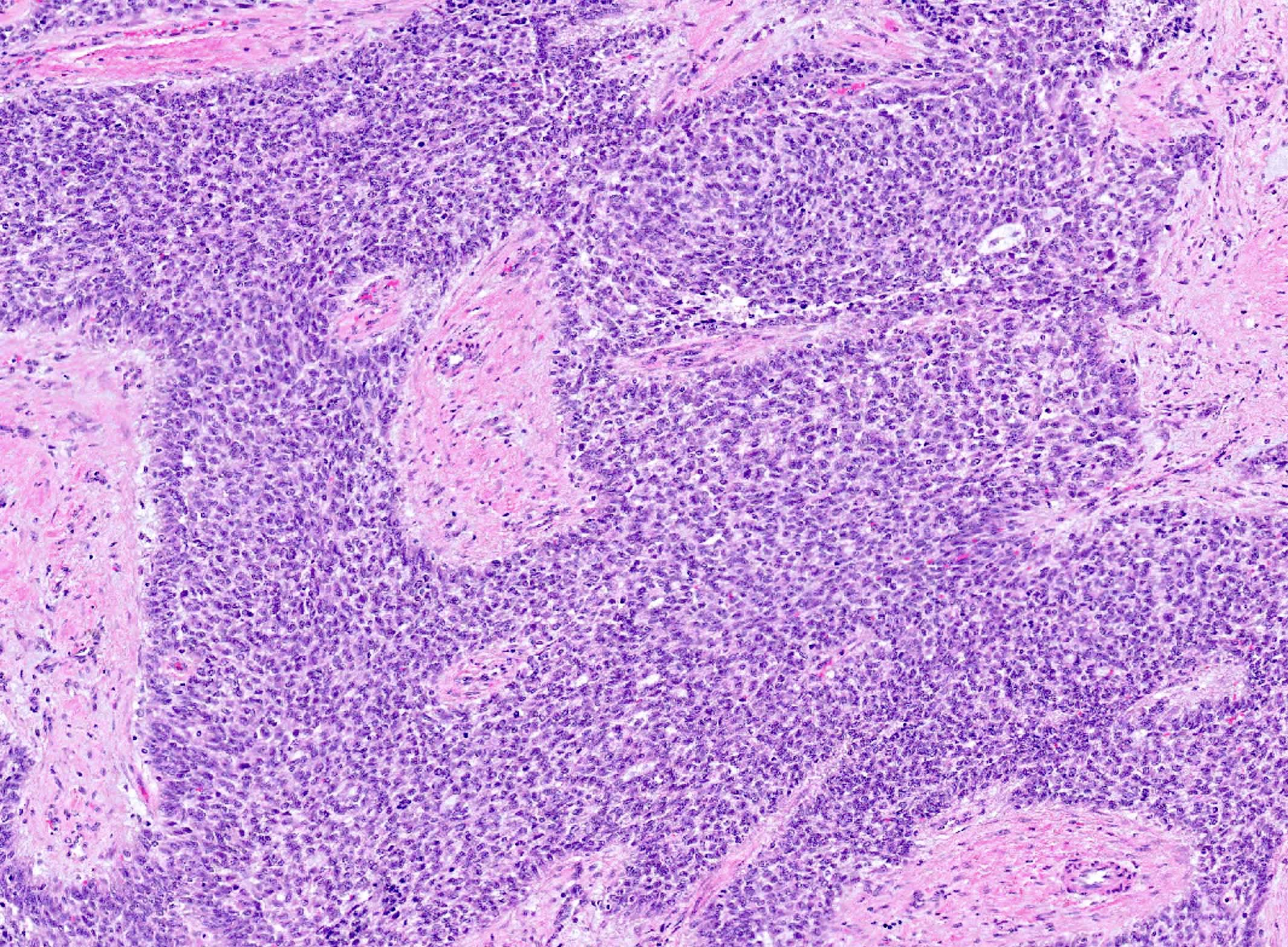
Broad columns
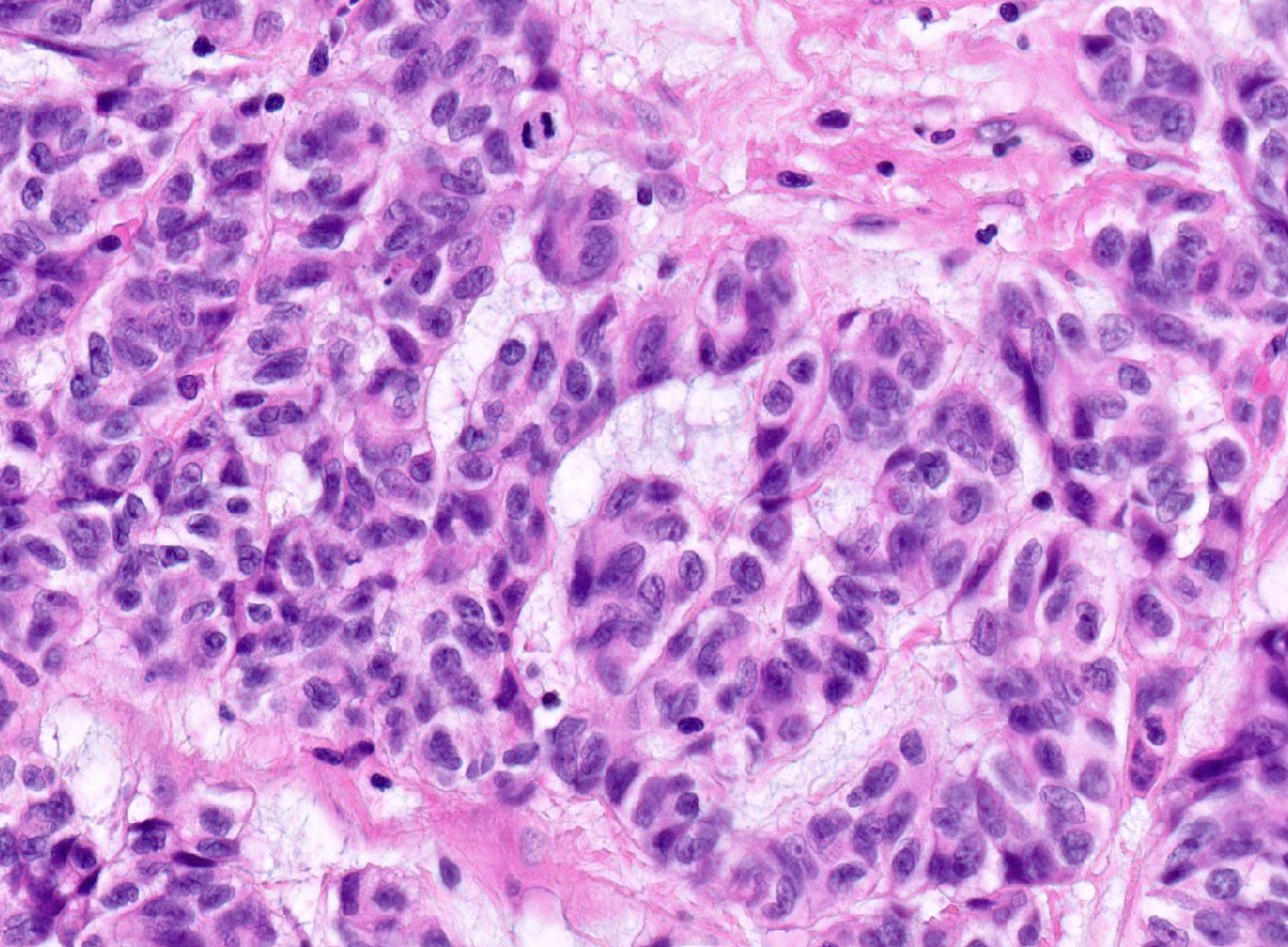
Nuclear features
Mitosis
Signet ring-like cells
Virtual slides
Images hosted on other servers:


STK11 adnexal tumor
Positive stains
- Strong CAM5.2 (94%), strong AE1 / AE3 (93%) and focal CK7 (60%)
- Inhibin (90%), calretinin (100%), WT1 (100%)
- AR (93%), ER (80%), PR (76%)
- Variable D2-40 (75%)
- Focal CD10 (81%)
- Reference: Pediatr Dev Pathol 2023;26:486, Am J Surg Pathol 2021;45:1061
Negative stains
- Claudin4
- FOXL2
- TTF1
- Focal SF1 (30% positive) (Am J Surg Pathol 2021;45:1061)
- Focal PAX8 (25% positive) (Am J Surg Pathol 2021;45:1061)
- Weak focal GATA3 (5% positive)
- Weak to moderate EMA staining (Am J Surg Pathol 2021;45:1061)
- Rare p63 (< 1% positive)
- Reference: Pediatr Dev Pathol 2023;26:486
Molecular / cytogenetics description
- STK11 alterations
- Pathogenic mutations, most commonly loss of heterozygosity (LOH)
- Deletions
- Variants of uncertain significance also reported
- References: Am J Surg Pathol 2021;45:1061, Jpn J Cancer Res 1999;90:629
Videos
Pathology of fallopian tube
Sample pathology report
- Uterus, bilateral fallopian tubes and ovaries; total hysterectomy with bilateral salpingo-oophorectomy:
- Right paratubal soft tissue: STK11 adnexal tumor, 15 cm (see note and synoptic summary)
- Fallopian tubes: unremarkable, fimbriated
- Ovaries: unremarkable
- Endometrium: proliferative
- Myometrium: adenomyosis
- Uterine serosa and cervix: unremarkable
- Note: The clinical history of Peutz-Jeghers syndrome is noted. STK11 adnexal tumor is a recently described neoplasm that is often associated with Peutz-Jeghers syndrome.
Differential diagnosis
- Female adnexal tumor of probable Wolffian origin (FATWO):
- Sex cord stromal tumors:
- Endometrioid carcinoma:
- Mesothelioma:
- Diffuse or plaque-like growth
- Rarely, the pleura may harbor STK11 mutations but in association with other alterations (BAP1 mutations or CDKN2A / CDKN2B deletions)
- Loss of BAP1
- Mesonephric adenocarcinoma and mesonephric-like carcinoma:
- Tubular pattern with back to back round tubules with or without eosinophilic secretions
- Uniform nuclei with mild to (at most) moderate cytologic atypia and variable mitotic activity
- AR and inhibin positive in ~33% of cases
- GATA3 and TTF1 positive
- ER / PR, WT1 negative and PAX8 positive
- Positive EMA, claudin4
- KRAS, NRAS mutations
- ARID1A, ARID1B or SMARCA4 mutations in ~60% of cases
- Rarely, metastatic adenoid cystic carcinoma:
- Dual population of cells (epithelial / ductal and myoepithelial)
Additional references
Board review style question #1
A 45 year old woman presents with a 10 cm adnexal mass demonstrating the pattern of cystic spaces surrounded by cuboidal epithelium shown above. The tumor shows the following immunophenotype: ER / PR positive, CK7 positive, PAX8 positive, GATA3 negative, inhibin positive, TTF1 negative, FOXL2 negative, p53 wild type. Which of the following is the best diagnosis for this tumor?
- Female adnexal tumor of probable Wolffian origin (FATWO)
- High grade serous carcinoma
- Mesonephric adenocarcinoma
- STK11 adnexal neoplasm
- Sex cord stromal tumor, NOS
Board review style answer #1
D. STK11 adnexal neoplasm. The immunophenotype and microscopic appearance are characteristic of STK11 adnexal tumor. Answer A is incorrect because FATWO is typically negative for hormonal markers. Answer B is incorrect because high grade serous carcinoma tumors uniformly harbor TP53 mutations, reflected in abnormal p53 staining patterns. Answer C is incorrect because mesonephric adenocarcinoma tumors are typically TTF1 and GATA3 positive. Answer E is incorrect because sex cord stromal tumors, while manifesting positive stromal markers like inhibin, are also FOXL2 positive.
Comment Here
Reference: STK11 adnexal tumor
Comment Here
Reference: STK11 adnexal tumor
Board review style question #2
A patient with Peutz-Jeghers syndrome may manifest which of the following components?
- Cutaneous dermatofibromas with hyperpigmentation
- Desmoid type fibromatoses
- Juvenile polyps of the intestinal tract
- Sertoli-Leydig tumors of the ovary or testis
- STK11 adnexal tumors
Board review style answer #2
E. STK11 adnexal tumors. Peutz-Jeghers syndrome is associated with STK11 in 50% of cases. Answer C is incorrect because Peutz-Jeghers syndrome is associated with distinctive hamartomatous polyps not of the juvenile type. Answer D is incorrect because Sertoli-Leydig tumors are associated with DICER1 syndrome. Answer A is incorrect because the pigmented lesions of Peutz-Jeghers syndrome are lentiginous hyperpigmentation only. Answer B is incorrect because desmoid fibromas are characteristic of familial adenomatous polyposis or Gardner syndrome.
Comment Here
Reference: STK11 adnexal tumor
Comment Here
Reference: STK11 adnexal tumor
