

Esophagus
Carcinoma
Undifferentiated carcinoma
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 27 April 2021
Last staff update: 21 May 2021
Copyright: 2021, PathologyOutlines.com, Inc.
PubMed Search: Esophagus - Undifferentiated carcinoma [TIAB]

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Kendziora R, Graham RP. Undifferentiated carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/esophagusundiffcarcinoma.html. Accessed December 26th, 2024.
Definition / general
- Rare and aggressive esophageal carcinoma
- Histologically characterized by sheets of cells with high grade features, frequent rhabdoid appearance and monotony
Essential features
- Neoplastic cells appear high grade with frequent rhabdoid appearance
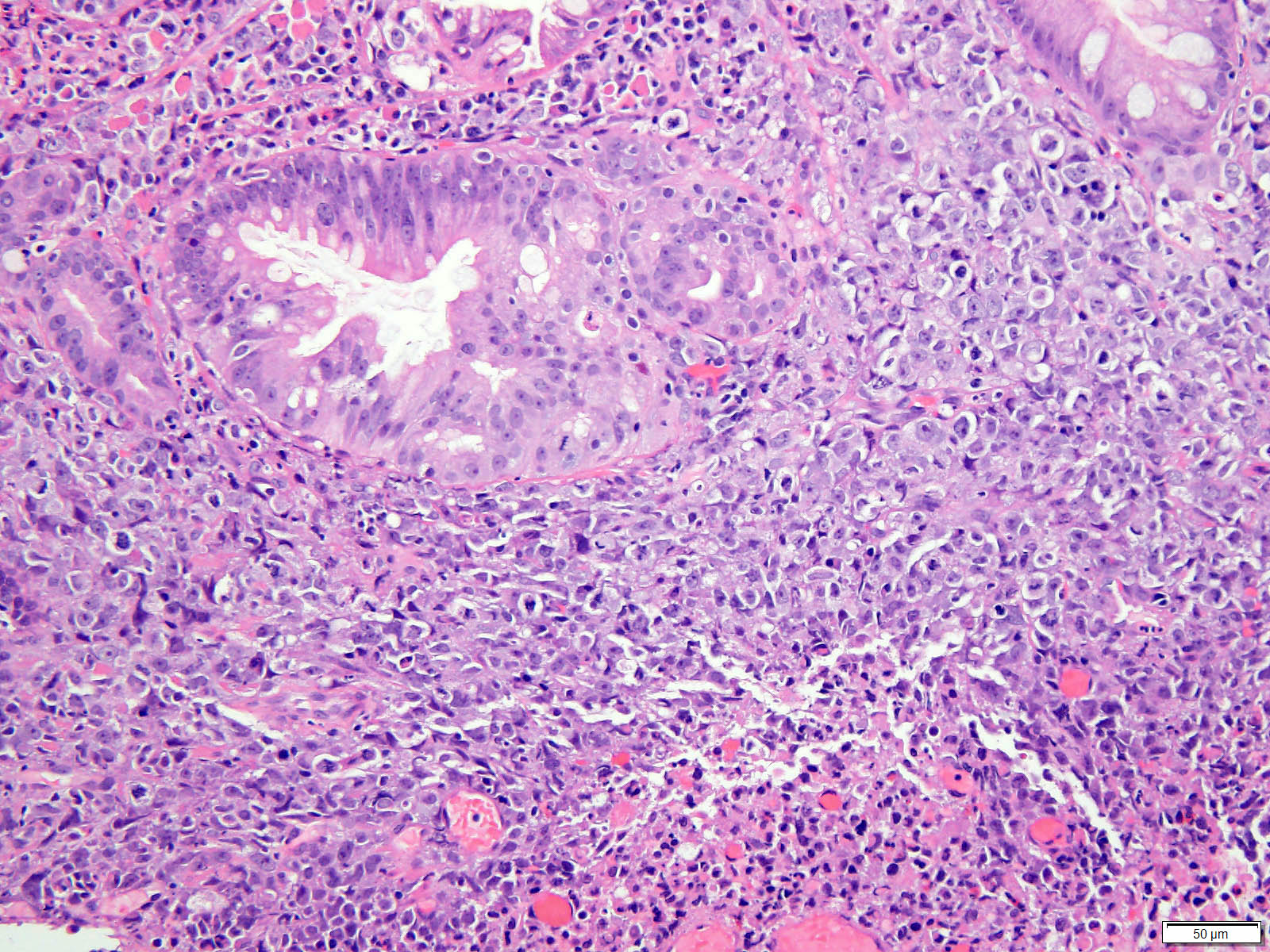
- Background Barrett esophagus with or without dysplasia may be identified
- May have limited or absent expression of pancytokeratins
- Characterized by frequent loss of SMARCA4 or SMARCA2
- Dismal prognosis with frequent recurrence or metastasis
ICD coding
Epidemiology
- M > F
- Median age in seventh decade
- Likely related to Barrett esophagus associated adenocarcinomas
- Very rare: as low as 0.15% of esophageal carcinomas (Dis Esophagus 2009;22:1)
Sites
- Distal esophagus
- Gastroesophageal junction
Pathophysiology
- Likely dedifferentiation / high grade progression of adenocarcinoma
- Subset of cases has associated Barrett esophagus and Barrett associated dysplasia
- Mutant p53 pattern by immunohistochemistry
- Frequent loss of SMARCA4 or SMARCA2 by immunohistochemistry
Etiology
- Same as Barrett esophagus associated adenocarcinoma
Clinical features
- Presentation similar to other esophageal cancers
- Progressive dysphagia
- Symptoms of gastroesophageal reflux disease
- Unexplained weight loss (Hum Pathol 2015;46:366)
- Typically locally advanced at diagnosis
Diagnosis
- Seen as exophytic mass on esophagogastroduodenoscopy
- Confirmed by histology and immunohistochemistry
Prognostic factors
- Poor prognosis overall: currently 20% 1 year survival rate
- As many as 67% will have local recurrence or metastasis (Hum Pathol 2015;46:366)
Case reports
- 67 year old man with ulcerative mass of gastroesophageal junction (Surg Case Rep 2019;5:8)
- 71 year old woman with mass of middle esophagus (Int J Clin Exp Pathol 2020;13:1902)
- 79 year old man with EBV infection (Int J Clin Exp Med 2013;6:219)
Treatment
- Neoadjuvant chemotherapy followed by esophagogastrectomy
- Palliative care
Gross description
- Exophytic mass
- Raised edges
- Central ulceration
- Pushing border
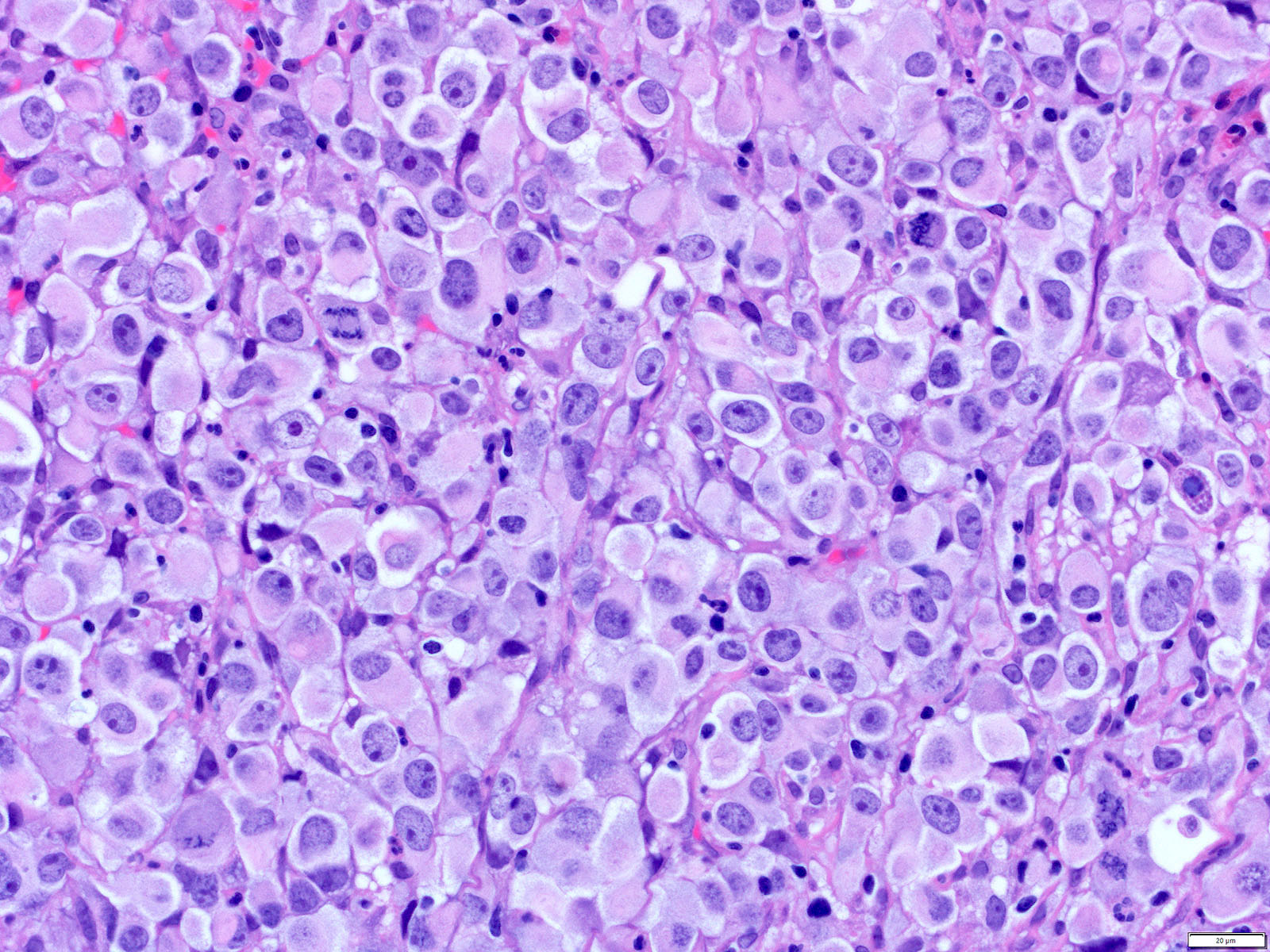
Microscopic (histologic) description
- Nests and sheets of cells
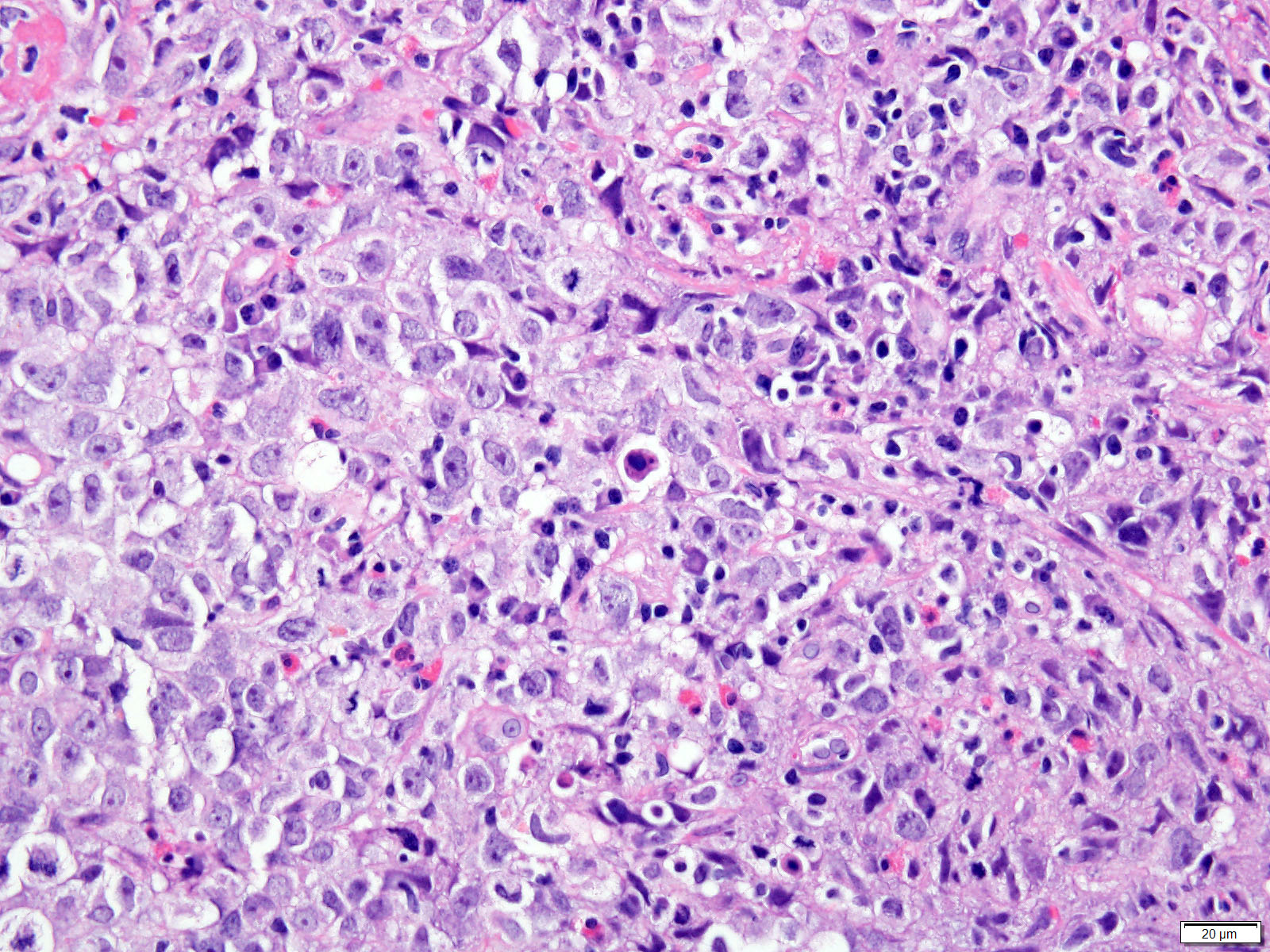
- Cytology is high grade with large nuclei and high nucleus to cytoplasm ratio
- Can have rhabdoid features
- Sheets of necrosis
- Lymphoepithelioma-like carcinoma a distinct subtype
- Sheets of epithelioid cells surrounded by dense lymphoplasmacytic inflammatory infiltrate
- Absence of identifiable signs of differentiation (adenocarcinoma, squamous cell carcinoma, neuroendocrine carcinoma)
Microscopic (histologic) images
Contributed by Rondell P. Graham, M.B.B.S.
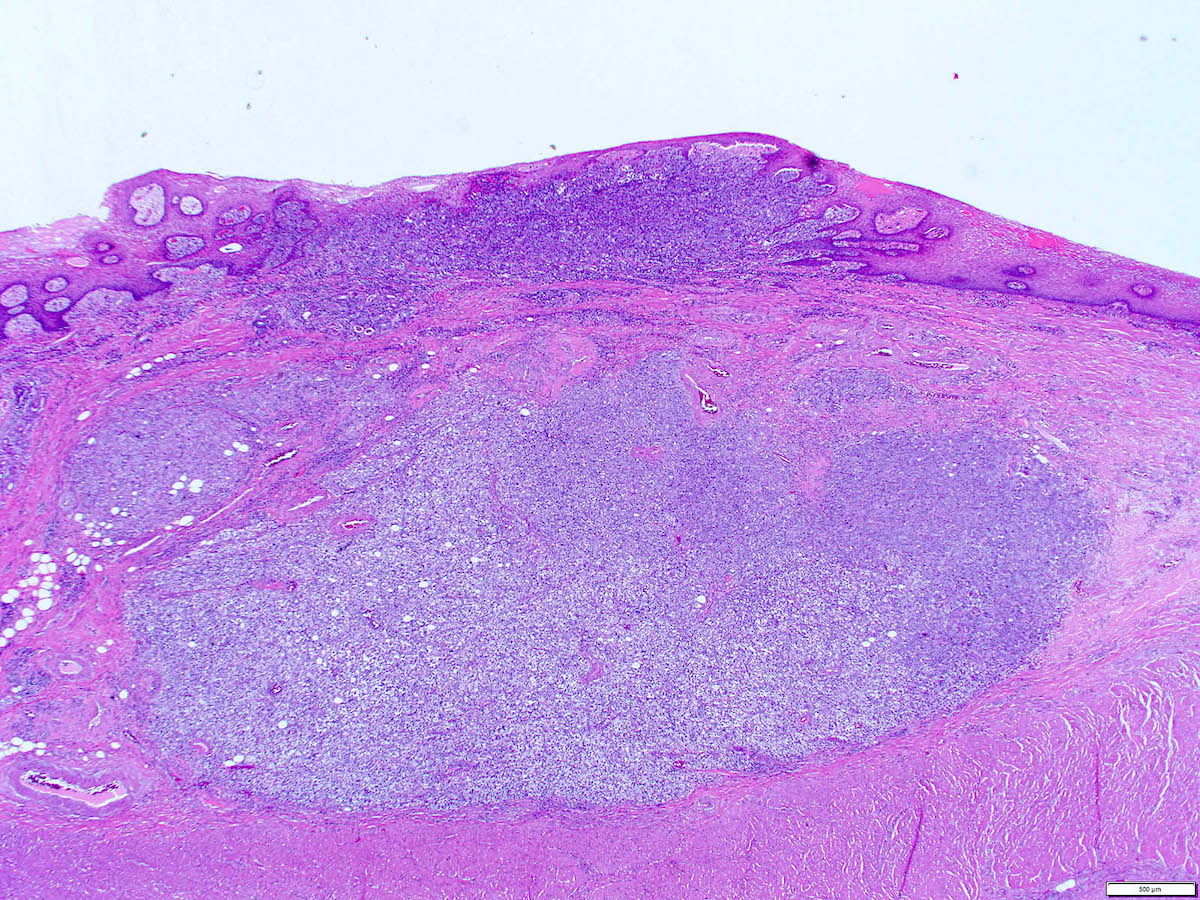
Sheets of cells
Low grade to high grade carcinoma
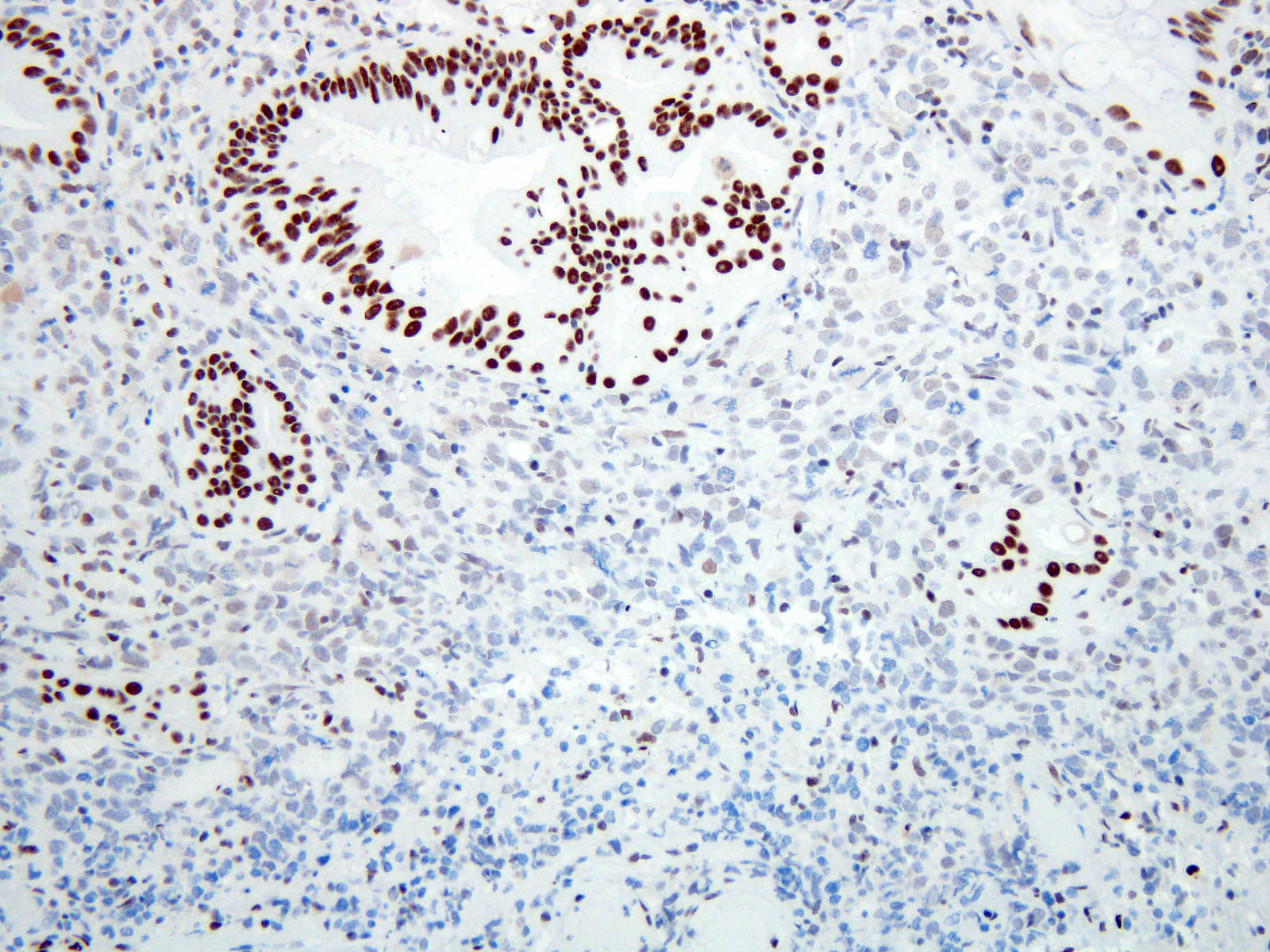
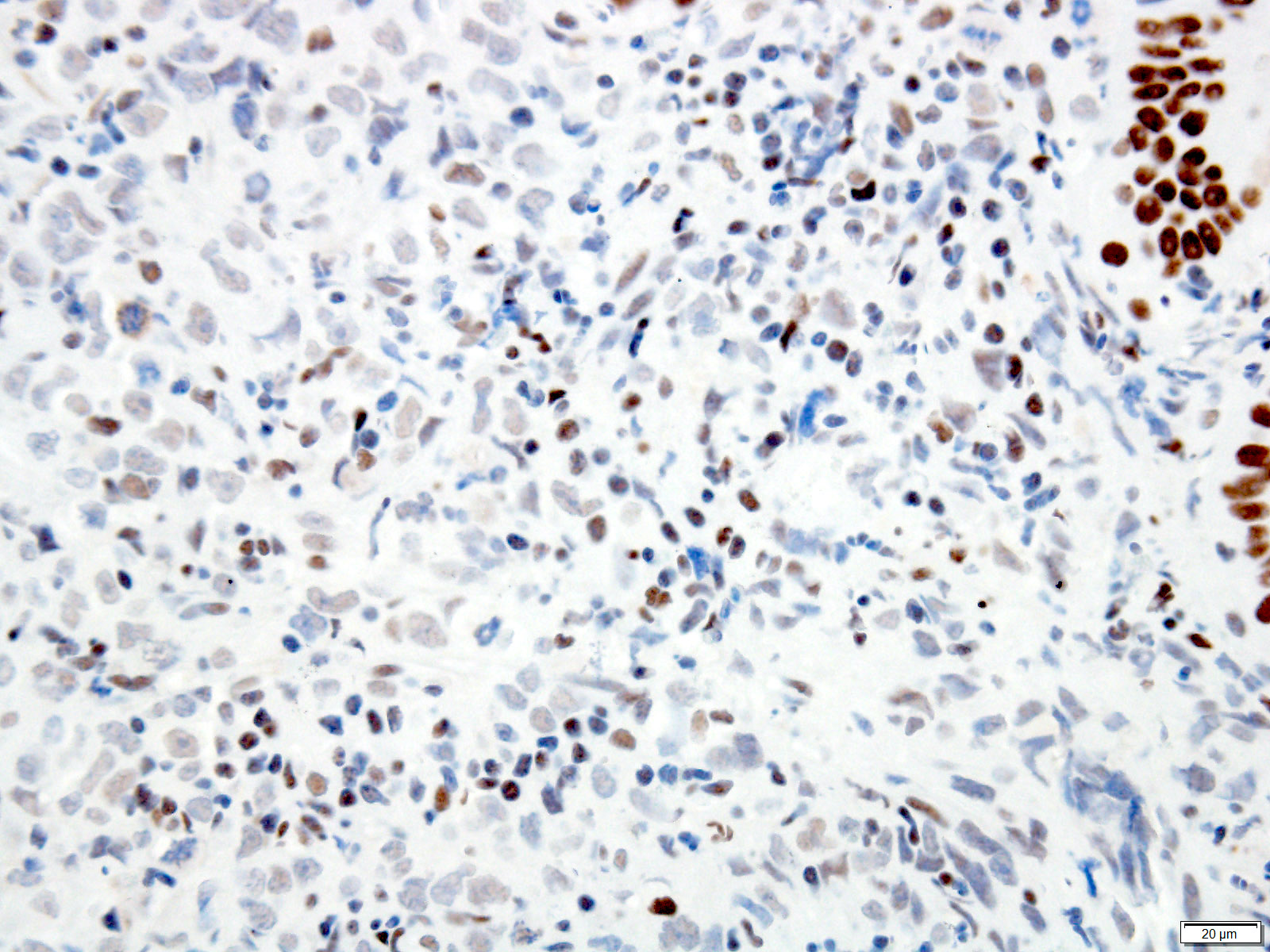
Loss of SMARCA4 (BRG1)
Positive stains
- Pancytokeratin: variable expression, ranging from diffuse to patchy or negative (Hum Pathol 2015;46:366, Am J Surg Pathol 2021;45:414)
- p53 can display mutant pattern of expression (either diffusely strong positive or total loss) (Am J Surg Pathol 2021;45:414)
- EBV positivity can be seen in lymphoepithelioma-like variant
Negative stains
- SMARCA4 (BRG1), SMARCA2 (BRM) or SMARCB1 (INI1) aberrant loss (Dis Esophagus 2009;22:1, Am J Surg Pathol 2021;45:414)
Sample pathology report
- Esophagus, biopsy:
- Undifferentiated carcinoma (see comment)
- Comment: SMARCA4 loss is seen by immunohistochemistry.
Differential diagnosis
- Poorly differentiated neuroendocrine carcinoma:
- Potentially also with nested / sheet-like architecture but would express synaptophysin and chromogranin
- Poorly differentiated squamous cell carcinoma:
- Stains for squamous markers (e.g. p40)
- More consistent pattern of cytokeratin positivity
- Malignant melanoma:
- Can also show nested architecture but would express melanocytic markers such as MelanA
- Hematolymphoid malignancy:
- Also would be negative for pancytokeratin but would express hematolymphoid markers (e.g. CD34 / LCA)
Additional references
Board review style question #1
A patient undergoes esophagogastrectomy for a tumor of the distal esophagus. A representative hematoxylin and eosin photomicrograph of the lesion is shown. The tumor lacks any immunohistochemical signs of differentiation, including negativity for pancytokeratin, MelanA, synaptophysin, chromogranin and CD34. An esophageal carcinoma of this subtype is characterized by what immunophenotype?
- Keratin 7 expression
- Wild type p53
- Loss of SMARCA4 or SMARCA2
- Expression of Rb
Board review style answer #1
C. Loss of SMARCA4 or SMARCA2. This is an undifferentiated carcinoma of the esophagus.
Comment Here
Reference: Undifferentiated carcinoma
Comment Here
Reference: Undifferentiated carcinoma

