

Esophagus
Carcinoma
Neuroendocrine carcinoma
Author: Gillian L. Hale, M.D., M.P.H.
Editorial Board Member: David J. Escobar, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.

Last author update: 13 May 2024
Last staff update: 13 May 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Neuroendocrine carcinoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Hale G. Neuroendocrine carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/esophagusneuroendocrine.html. Accessed November 29th, 2024.
Definition / general
- Rare, high grade epithelial tumor with neuroendocrine differentiation divided into small cell or large cell types by morphology; follows an aggressive clinical course and has a poor prognosis
Essential features
- Rare malignant tumor of the esophagus with poor prognosis and frequent locoregional or distant metastasis at the time of diagnosis
- Usually involves middle or distal third of the esophagus
- Positive for either synaptophysin or chromogranin
- Divided into either small cell or large cell type by morphology, using the same criteria as for other sites in the gastrointestinal tract
- Small cell: minimal cytoplasm, nuclei with fine chromatin and nuclear molding, inconspicuous nucleoli, frequent mitoses, necrosis
- Large cell: moderately abundant cytoplasm, nuclei with clumped chromatin and prominent nucleoli, frequent mitoses, necrosis
Terminology
- Poorly differentiated endocrine carcinoma, small cell carcinoma, large cell carcinoma
ICD coding
Epidemiology
- Most esophageal neuroendocrine neoplasms are high grade tumors (Clinics (Sao Paulo) 2011;66:1671, J Oncol 2016;2016:2402417)
- Extremely rare; accounts for < 1% of all malignant neoplasms and between 0.4 - 2% of esophageal malignancies (BMC Cancer 2014;14:569, Crit Rev Oncol Hematol 2019;137:92, PLoS One 2017;12:e0173501, J Oncol 2016;2016:2402417)
- M:F = 2.5 - 3:1 (Am J Surg Pathol 2013;37:467, J Thorac Dis 2016;8:1250)
- Mean age: 60 - 70 years (Crit Rev Oncol Hematol 2019;137:92)
Sites
- Middle or lower third of the esophagus, corresponding to distribution of neuroendocrine cells (Am J Surg Pathol 2013;37:467, Int J Clin Exp Pathol 2013;6:485, J Thorac Dis 2016;8:1250, Crit Rev Oncol Hematol 2019;137:92)
Pathophysiology
- Small cell carcinoma in the esophagus was first described in 1952 (J Pathol Bacteriol 1952;64:889)
- Unknown but small studies suggest origin from totipotent progenitor cell (Hum Pathol 1984;15:460, J Thorac Cardiovasc Surg 1985;90:351)
Etiology
- Associated with high alcohol intake and smoking (Arq Gastroenterol 2017;54:4)
Clinical features
- Dysphagia (most common), weight loss, appetite loss, pain (retrosternal, epigastric, abdominal) (Int J Clin Exp Pathol 2013;6:485, Crit Rev Oncol Hematol 2019;137:92)
- Regional lymph node metastasis or widespread metastasis is common at the time of diagnosis (Am J Surg Pathol 2008;32:1404, BMC Cancer 2014;14:569)
- Metastatic sites include lungs, liver, adrenal, peritoneal, bones (Arq Gastroenterol 2017;54:4)
- Rare cases demonstrate an association with paraneoplastic neurologic syndrome (Jpn J Clin Oncol 2006;36:109)
Diagnosis
- Typically diagnosed via endoscopy with biopsy or less commonly after surgical resection (Crit Rev Oncol Hematol 2019;137:92)
Laboratory
- Testing for calcium, phosphate, alkaline phosphatase can aid in evaluating for bone metastasis
- High grade carcinomas are often nonfunctional; therefore, serum marker testing is not recommended (J Med Case Rep 2023;17:144)
Radiology description
- Imaging studies can help define the extent of esophageal involvement
- Barium esophagography can be used in the initial identification of tumors (Crit Rev Oncol Hematol 2019;137:92)
- Computed tomography (CT) imaging for defining regional or distant lymph node metastasis and systemic disease
- Whole body positron emission tomography (PET) scans to evaluate for distant metastases and monitoring response to treatment (Front Med (Lausanne) 2020;6:336, J Neuroendocrinol 2023;35:e13249)
Prognostic factors
- Neuroendocrine carcinomas (NECs) are highly aggressive with poor prognosis as in other body sites
- Patients with locoregional disease have better overall survival than those with distant metastases (Am J Surg Pathol 2008;32:1404, Dis Esophagus 2014;27:152)
- Prognosis is better in patients with mixed NEC (having both NEC and squamous cell carcinoma or adenocarcinoma) (Am J Surg Pathol 2008;32:1404)
- Median survival is 3 - 20 months (BMC Cancer 2007;7:38, Arch Pathol Lab Med 2000;124:228, Dis Esophagus 2014;27:152)
- 5 year survival is ≤ 8% (Chin Med J (Engl) 2007;120:355, Ann Surg Oncol 2013;20:4239)
Case reports
- 51 year old man with collision tumor between papillary adenocarcinoma and large cell neuroendocrine carcinoma (Arch Pathol Lab Med 2000;124:411)
- 55 year old man with large cell NEC of the esophagus (Cureus 2022;14:e28842)
- 63 year old woman with esophageal small cell carcinoma coexisting with paraneoplastic neurological syndrome (Jpn J Clin Oncol 2006;36:109)
- 66 year old man with rare collision tumor of squamous carcinoma and small cell carcinoma in esophagus with separate lymph node involvement (J Thorac Dis 2013;5:E203)
- 67 year old man found to have NEC in lower esophagus with metastasis (J Med Case Rep 2023;17:144)
- 79 year old man with dysphagia (BMJ Case Rep 2013;2013:bcr2013200468)
Treatment
- No standardized treatment
- Multimodal therapy (surgery, platinum based chemotherapy or radiation) improves survival in patients with locoregional and metastatic disease (Dis Esophagus 2014;27:152)
- Folinic acid, fluorouracil and irinotecan (FOLFIRI) can be considered for second line therapy after platinum etoposide first line chemotherapy (Lancet Oncol 2023;24:297)
Clinical images
Images hosted on other servers:

Endoscopic findings
Gross description
- Ulcerative, fungating mass with a gray-white cut surface (J Investig Med High Impact Case Rep 2020;8:2324709620918245)
Gross images
AFIP images

Bulky, ulcerated, infiltrative lesion
Images hosted on other servers:

Small cell
carcinoma (upper);
squamous cell
carcinoma (lower)
Microscopic (histologic) description
- Poorly differentiated (high grade) carcinomas
- Divided into small cell or large cell types according to WHO 2019 classification
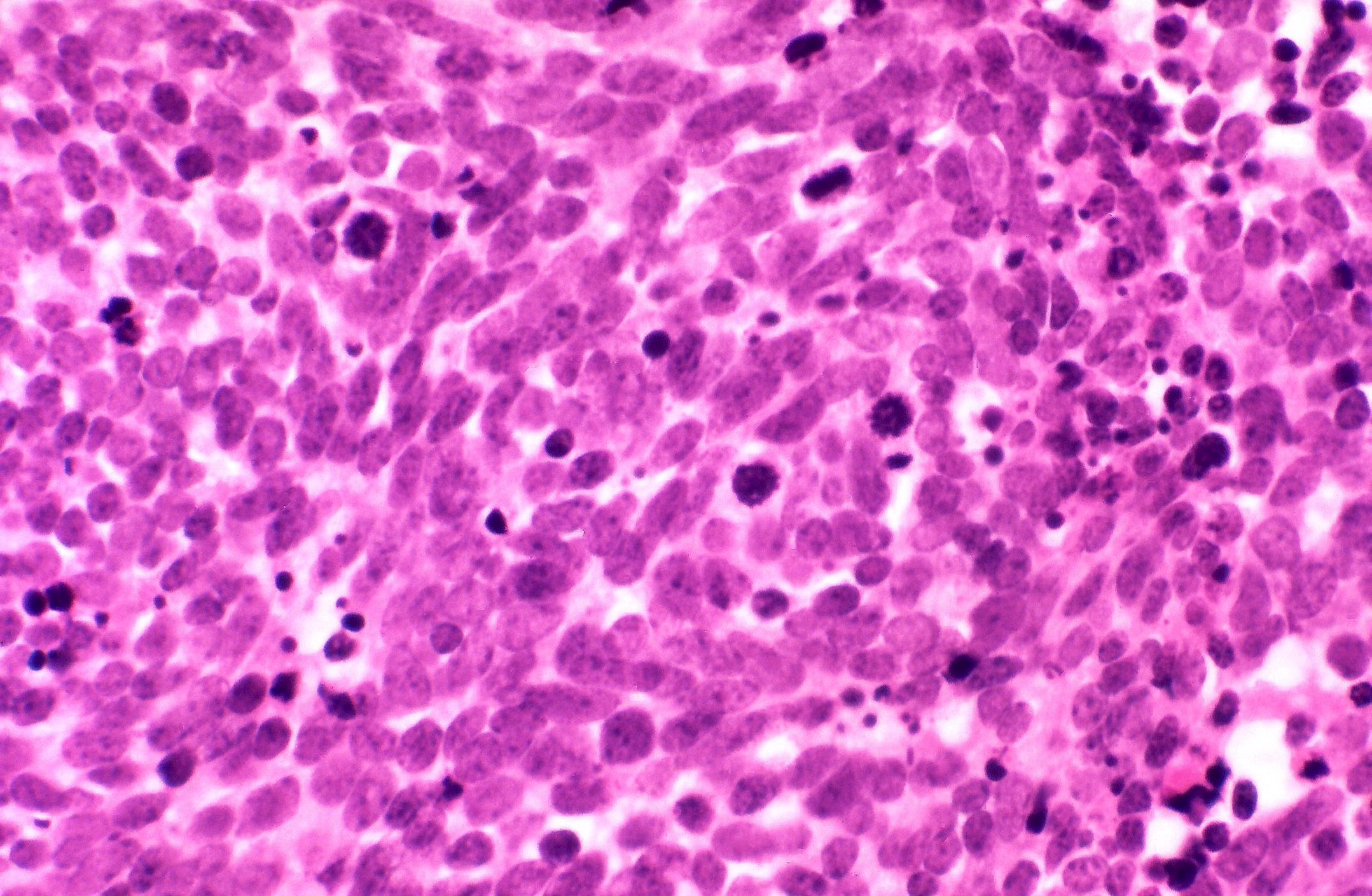
- Small cell carcinoma
- Small round to oval cells with scant cytoplasm, prominent nuclear molding, fine granular chromatin, absent or inconspicuous nucleoli
- Solid, rosette or palisading pattern of infiltration
- Brisk mitotic activity and necrosis
- Large cell carcinoma
- Medium to large tumor cells with enlarged nuclei, prominent nucleoli and moderately abundant basophilic cytoplasm
- Brisk mitotic activity and necrosis
- Small cell carcinoma
- Neuroendocrine carcinoma may have small component(s) of adenocarcinoma or squamous cell carcinoma differentiation (Arq Gastroenterol 2017;54:4)
Microscopic (histologic) images
Contributed by Gillian L. Hale, M.D., M.P.H., Mark R. Wick, M.D. and AFIP
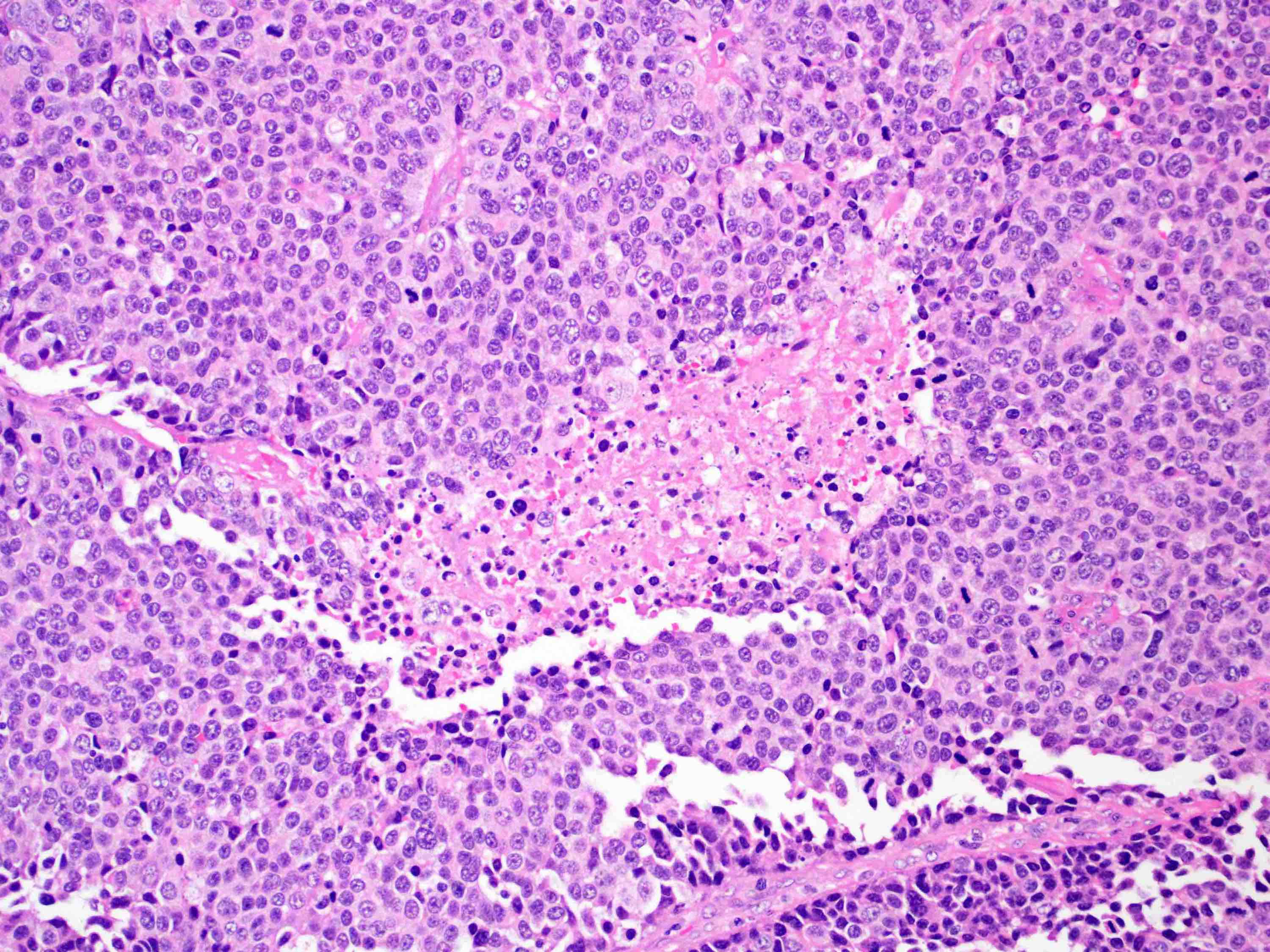
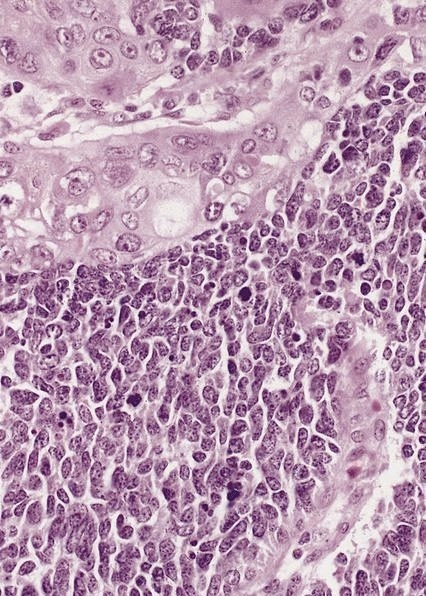
Sheets of tumor cells with central necrosis
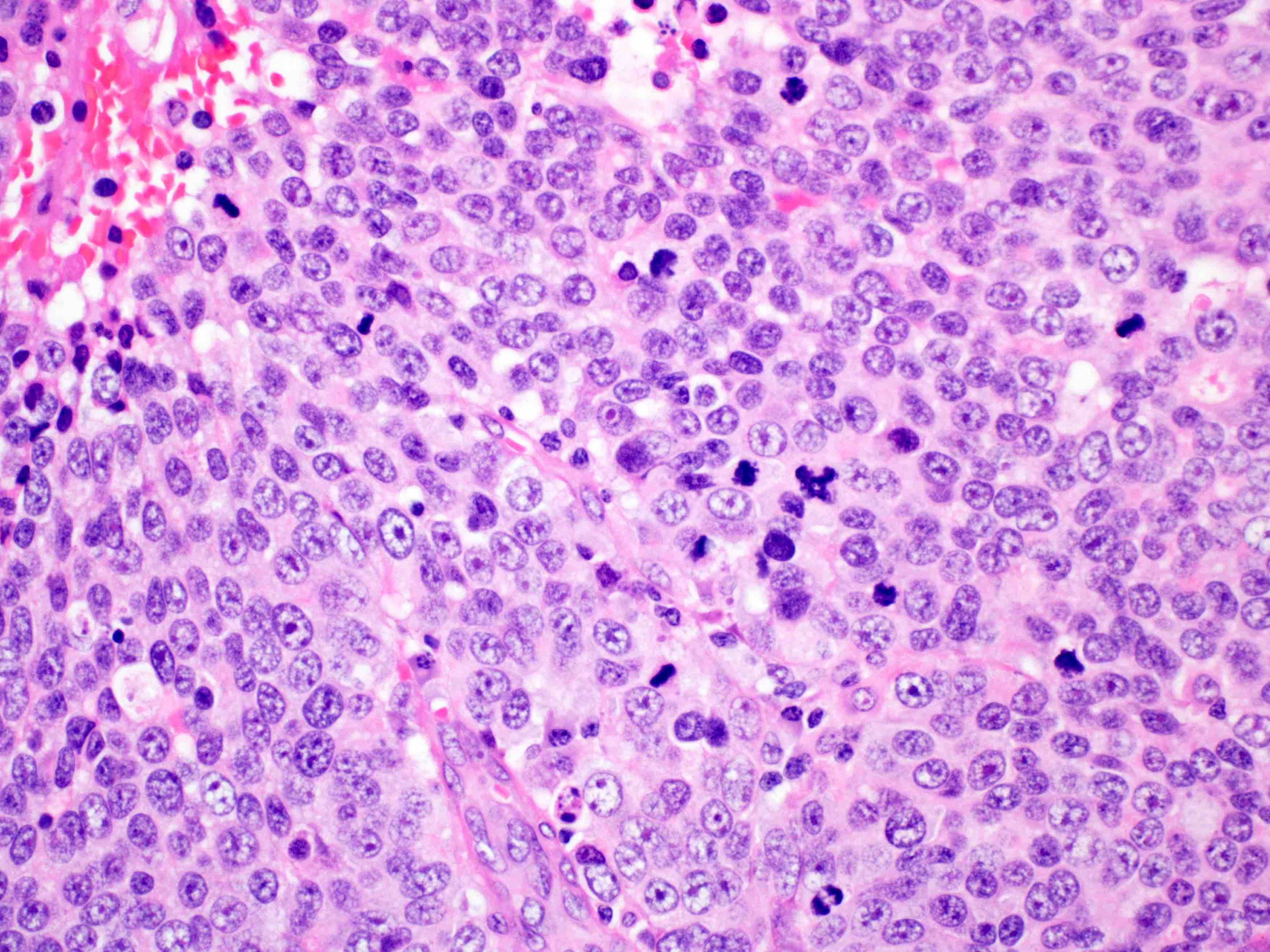
Large cells with
prominent nucleoli
and numerous
mitoses
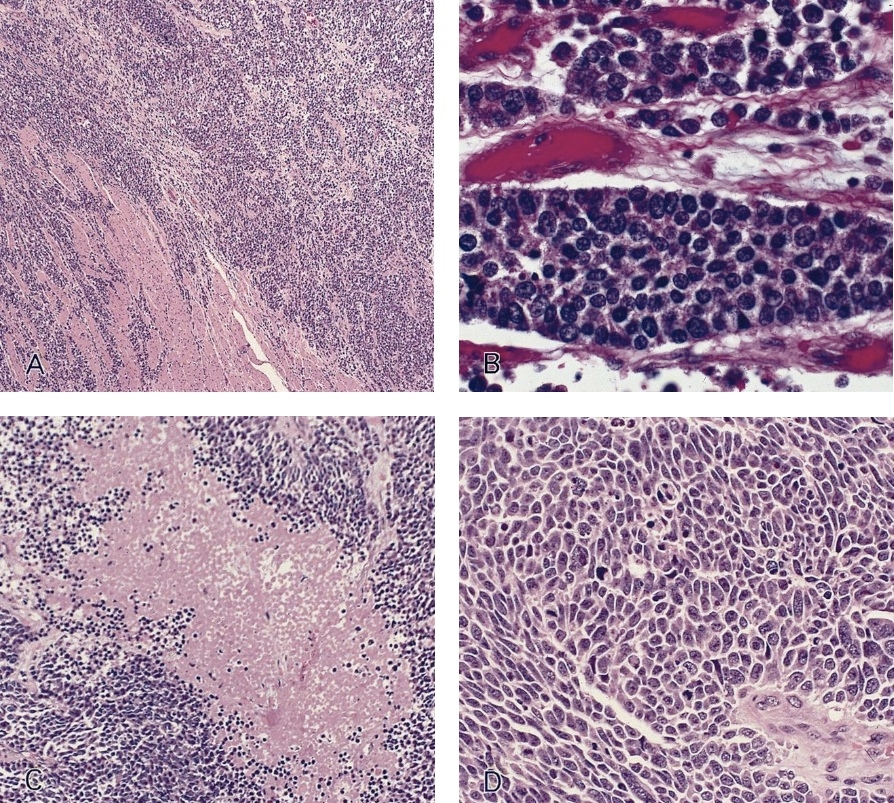

Diffusely infiltrating sheets of small cells
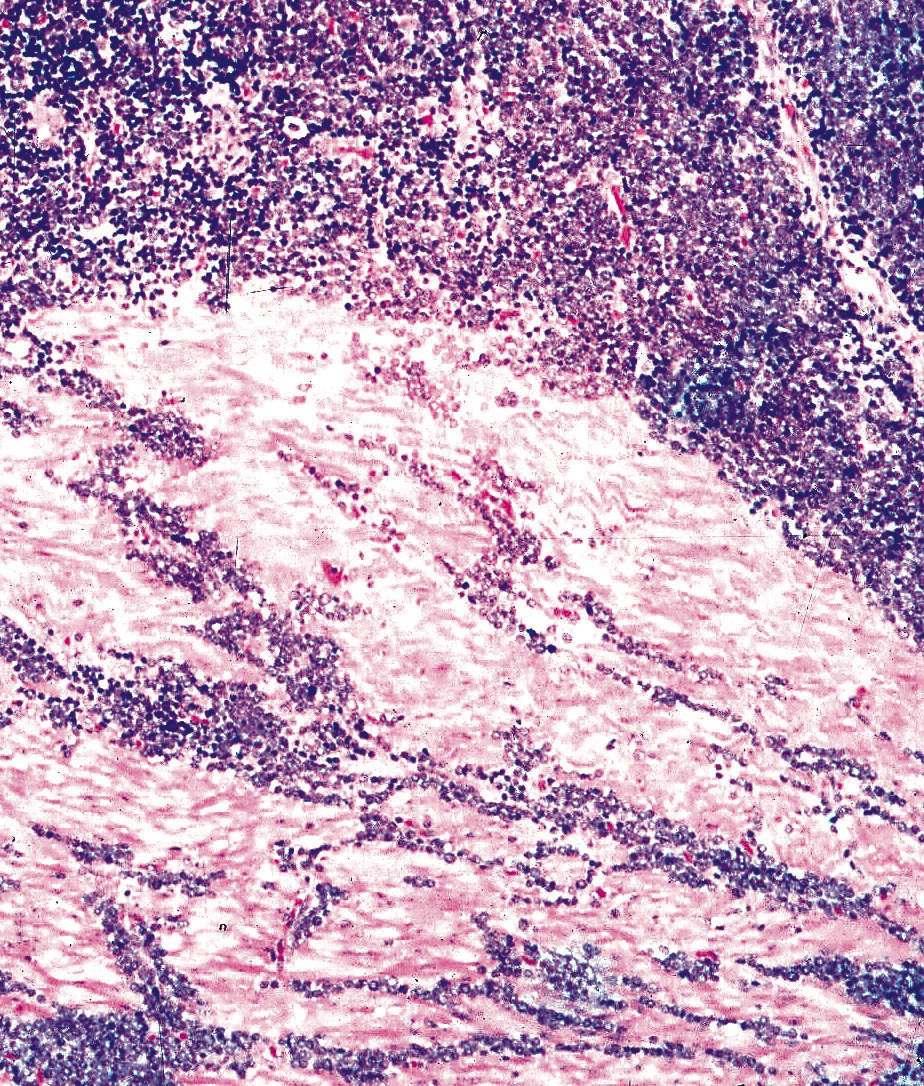
In muscularis
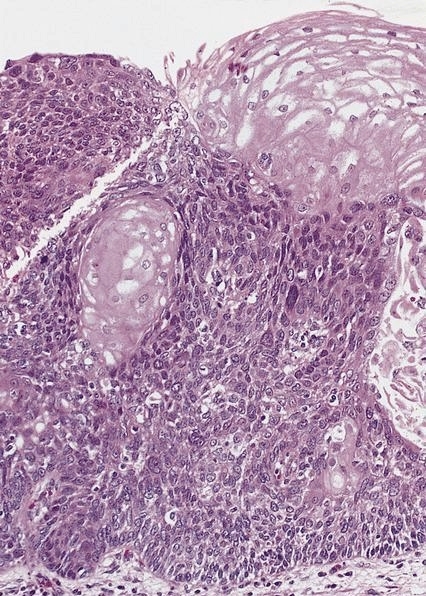
In situ component
Squamous cell differentiation
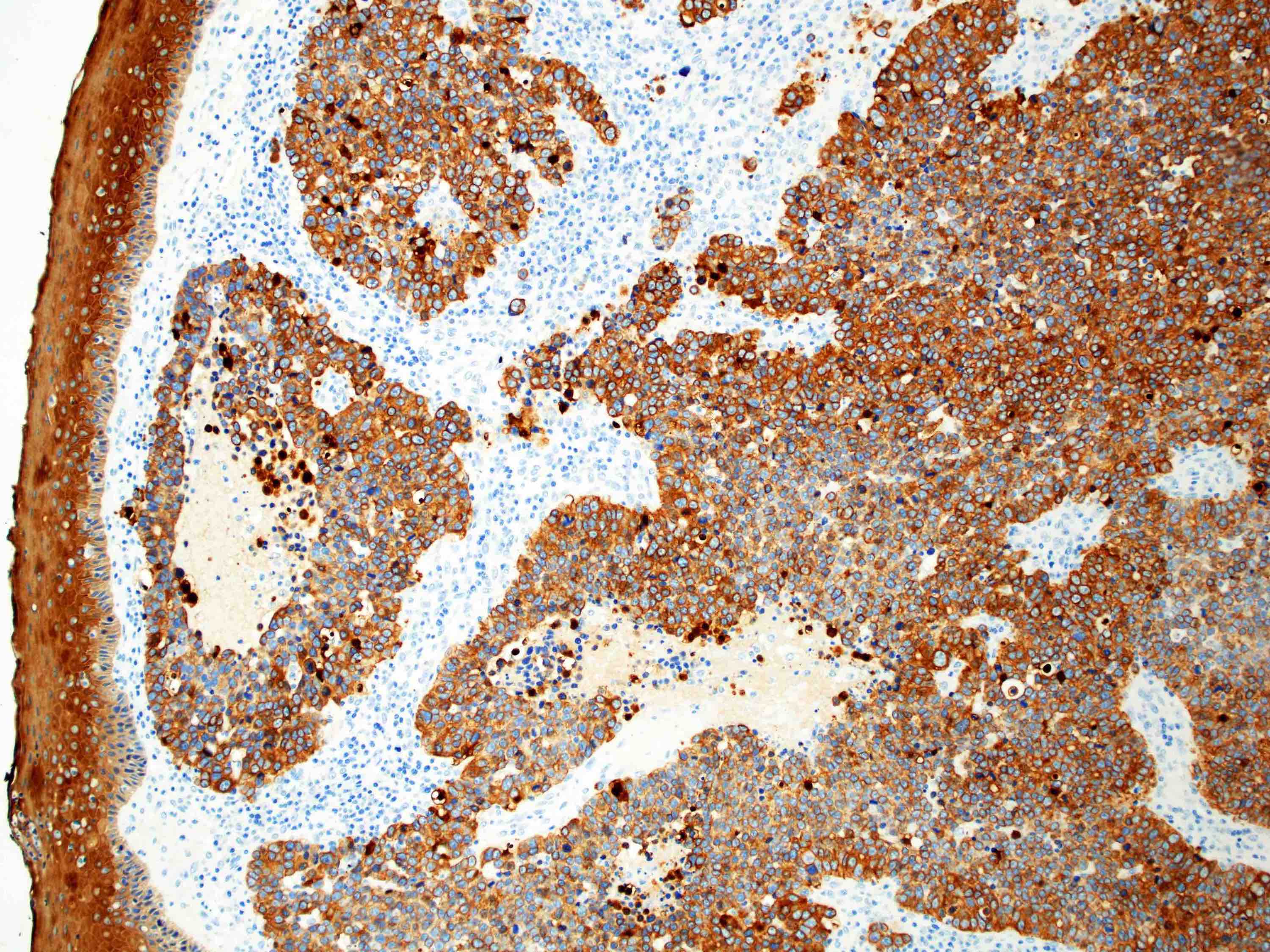
Pancytokeratin immunostain
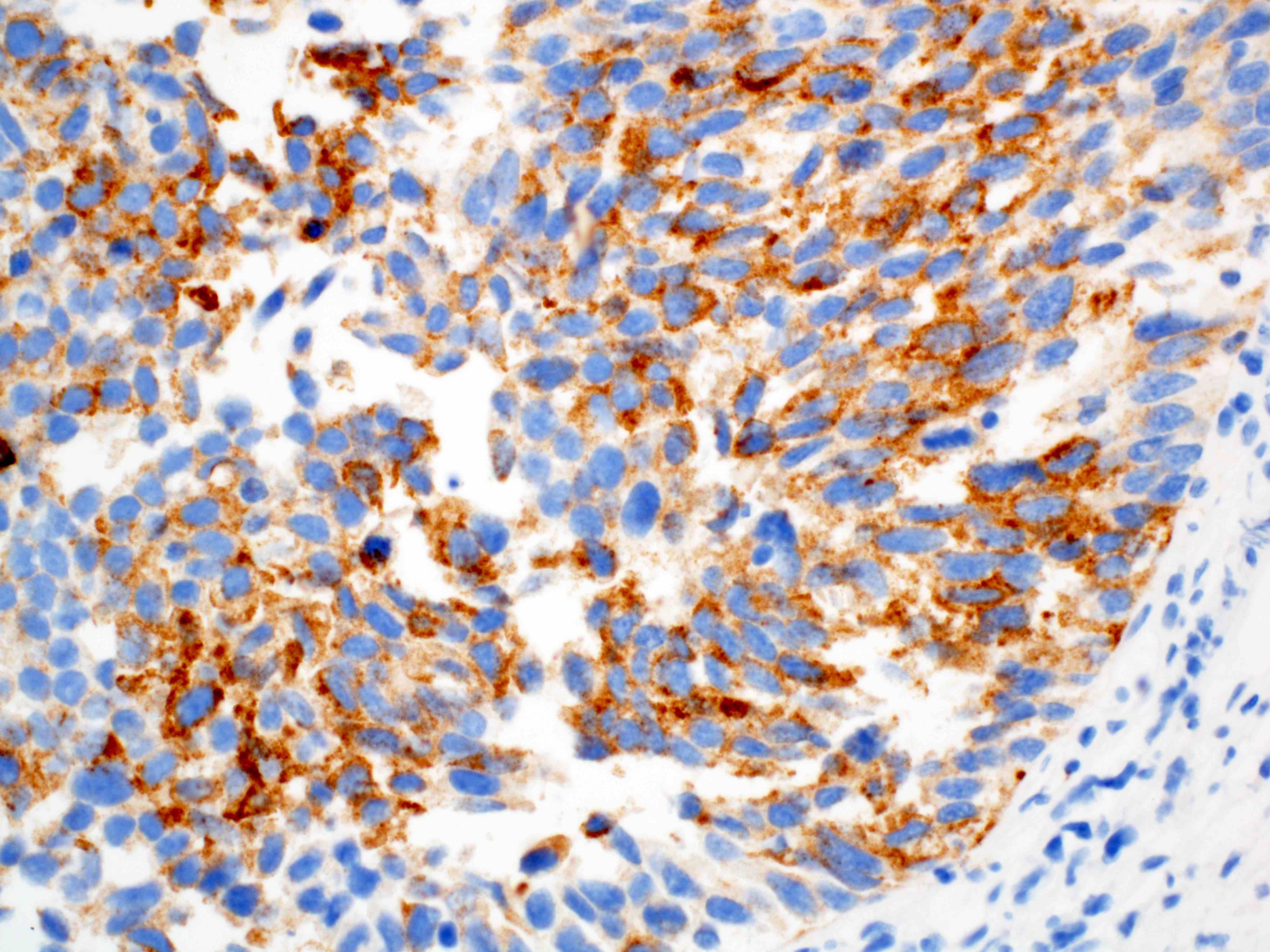
Synaptophysin immunostain
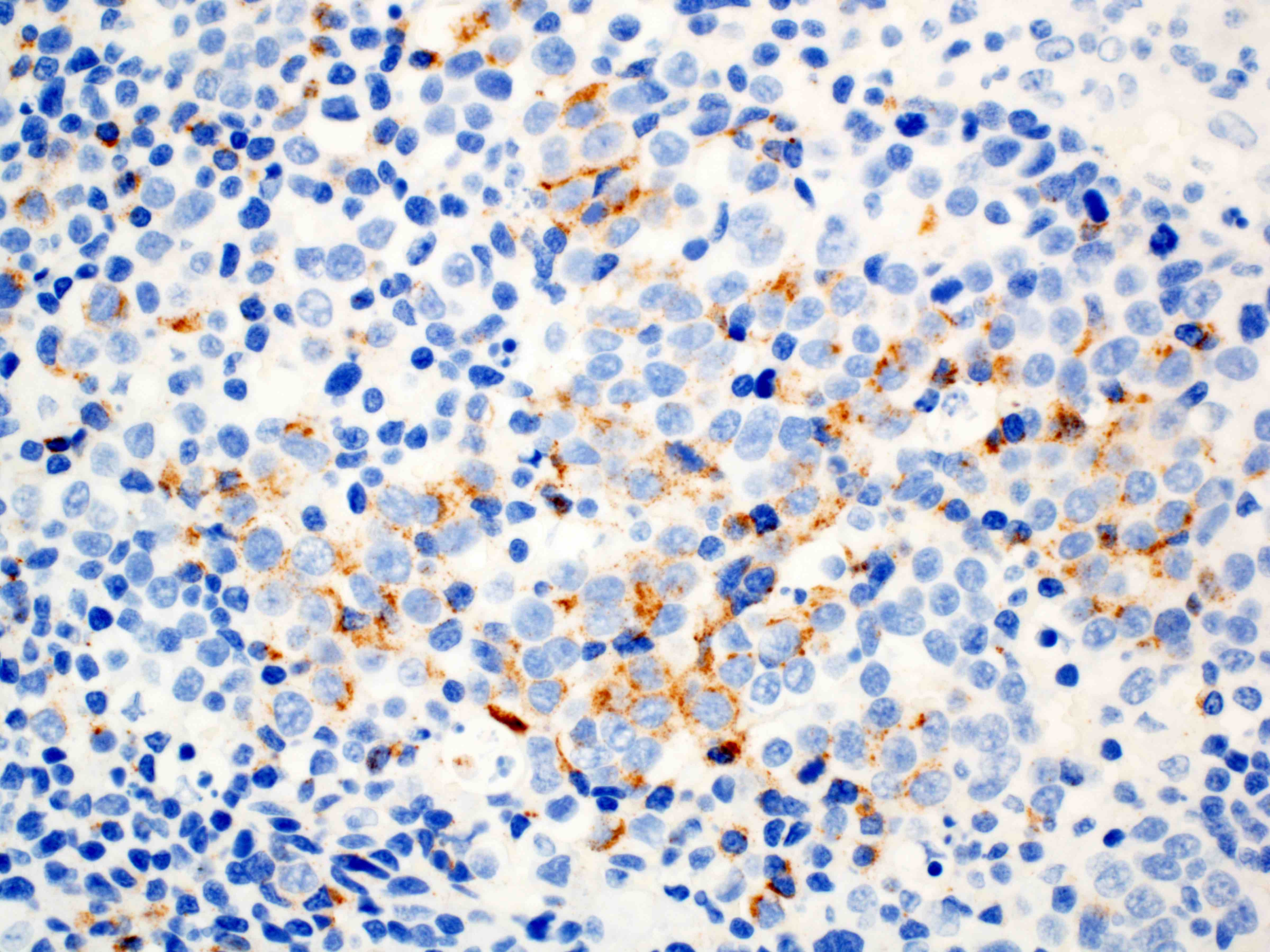
Chromogranin immunostain
Cytology description
- Small cell type: obvious pleomorphism, marked nuclear molding, hyperchromatic nuclei, inconspicuous nucleoli
- Large cell type: pleomorphic, medium to large cells, moderate cytoplasm, coarse chromatin, prominent nucleoli
- Numerous mitoses, crush artifact, necrosis
- Apoptotic figures, blue bodies
- References: Cancer 2000;90:148, Mod Pathol 1992;5:555
Cytology images
Contributed by Yale Rosen, M.D.
Small cell carcinoma
Positive stains
- Keratins (e.g., CAM 5.2, AE1 / AE3)
- Neuroendocrine markers: synaptophysin, chromogranin, CD56, INSM1
- Synaptophysin is more sensitive than chromogranin (Am J Surg Pathol 2008;32:1404)
- Proliferative index assessed by Ki67 / MIB1 immunohistochemistry is typically > 60% (Pathol Res Pract 2021;226:153614)
- TTF1 positive in 71% of esophageal neuroendocrine carcinoma (Am J Surg Pathol 2013;37:467)
- Other stains reportedly positive include p63 (55%), CD117 (86%), HER2 (16%) and p16 (84%) (Am J Surg Pathol 2013;37:467)
Negative stains
Electron microscopy description
- Neurosecretory granules
Electron microscopy images
Images hosted on other servers:

Neurosecretory granules
Molecular / cytogenetics description
- Associated with a high rate of inactivating mutations in 5 well known genes (TP53, RB1, NOTCH1, FAT1, FBXW7) and 3 genes not previously associated with esophageal carcinogenesis (PDE3A, PTPRM and CBLN2) (Cell Res 2018;28:771)
Sample pathology report
- Esophagus, mass, biopsy:
- Poorly differentiated neuroendocrine carcinoma, small cell type (see comment)
- Comment: Sections show sheets of crowded tumor cells with round to oval nuclei, inconspicuous nucleoli, prominent nuclear molding and numerous mitoses. There are broad zones of necrosis and necroinflammatory debris within the tumor. The tumor cells are highlighted by stains for pankeratin (strong, diffuse), synaptophysin (strong, diffuse) and chromogranin A (weak, patchy). Ki67 highlights a proliferative index of > 80%. The morphologic features and immunophenotype are those of a poorly differentiated neuroendocrine carcinoma, small cell type.
Differential diagnosis
- High grade carcinomas:
- Metastatic pulmonary neuroendocrine carcinoma:
- There are no reliable means of differentiating a primary esophageal neuroendocrine carcinoma from a metastatic pulmonary neuroendocrine carcinoma (Hum Pathol 2020:96:8)
- Lymphoma:
- CD45 positive
- Melanoma:
- Positive for S100, HMB45, MelanA
- Typically negative for keratin markers; rare keratin expression has been reported in dedifferentiated melanoma (Am J Dermatopathol 2019;41:502)
- Basaloid squamous cell carcinoma:
- Immunopositivity for p40 and CK5/6; however, small cell carcinoma can focally express p40 in ~34% of cases (Thorac Cancer 2019;10:1188)
- Metastatic pulmonary neuroendocrine carcinoma:
Additional references
Board review style question #1

For the lower esophageal tumor depicted in the image above, which of the following statements is true?
- Synaptophysin immunohistochemistry has greater sensitivity than chromogranin in detection
- There are established consensus guidelines on the treatment of this large cell carcinoma
- This tumor has a favorable prognosis with a median survival of 10 years
- Tumors with a concomitant adenocarcinoma or squamous cell carcinoma component have a worse prognosis
Board review style answer #1
A. Synaptophysin immunohistochemistry has greater sensitivity than chromogranin in detection. This is an esophageal small cell carcinoma, which expresses synaptophysin or chromogranin, although synaptophysin has greater sensitivity than chromogranin. Answer C is incorrect because this tumor has a poor prognosis. Answer D is incorrect because tumors with an adenocarcinoma or squamous cell carcinoma component tend to have a better prognosis than pure small cell carcinoma. Answer B is incorrect because the image depicts a small cell carcinoma (not large cell carcinoma) and there is no consensus approach to the treatment of neuroendocrine carcinomas given the rarity of the tumor and lack of randomized controlled trials; however, treatment often includes a combination of approaches including surgery, platinum based chemotherapy and radiation.
Comment Here
Reference: Neuroendocrine carcinoma
Comment Here
Reference: Neuroendocrine carcinoma

