
Esophagus
Other nonneoplastic
Esophagitis dissecans superficialis / sloughing esophagitis
Authors: Divya Salibindla, M.D., Divya Sharma, M.D.
Editorial Board Member: Claudio Luchini, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 7 May 2024
Last staff update: 7 May 2024
Copyright: 2017-2025, PathologyOutlines.com, Inc.
PubMed search: Esophagitis dissecans superficialis / sloughing esophagitis


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Salibindla D, Sharma D. Esophagitis dissecans superficialis / sloughing esophagitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/esophaguseds.html. Accessed March 28th, 2025.
Definition / general
- Benign clinical condition characterized by sloughing of the esophageal mucosa with unclear pathogenesis
Essential features
- Rare condition diagnosed incidentally on endoscopy
- Strips of vertically sloughed mucosal fragments evident on endoscopy
- Histologically, characterized by intraepithelial splitting, prominent parakeratosis, intraepithelial cystic degeneration and basal cell hyperplasia
- 2 tone esophagus
- Resolves spontaneously without complications
Terminology
- Sloughing esophagitis; this entity was first reported by B. Rosenberg in 1892 (Abdom Radiol (NY) 2021;46:5050, Centrolblf allg Path u path Anat 1892;3:753)
ICD coding
- ICD-10: K20.9 - esophagitis, unspecified
Epidemiology
- Usually occurs in older age group (Int J Biomed Sci 2014;10:282)
Sites
- Mid or distal part of esophagus
- However, it can affect the entire length of the esophagus
Pathophysiology
- Unknown
- Can result from ischemia or a direct insult to the esophageal mucosa caused by chemical, thermal, physical or immunological mechanisms (Gastroenterology Res 2016;9:108)
Etiology
- Mostly idiopathic
- Consumption of hot beverages and exposure to chemical irritants
- Malignancy
- Esophageal trauma
- Use of medications such as bisphosphonates, nonsteroidal anti-inflammatory drugs, psychoactive medications (e.g., SSRIs or SNRIs), methotrexate and potassium chloride
- Presence of celiac disease, collagen disorders and autoimmune bullous dermatoses (Cureus 2023;15:e43549)
- Can occur following immune checkpoint inhibitor therapy (Curr Probl Cancer Case Rep 2021;3:100044)
- Gastrointestinal side effects of COVID-19 or potentially aspirin consumption (Middle East J Dig Dis 2022;14:346)
Clinical features
- Usually diagnosed incidentally on endoscopy
- Few patients can present with dysphagia, heartburn, odynophagia, regurgitation, dyspepsia, upper gastrointestinal bleeding, anemia and weight loss
- In some extreme cases, patients can vomit mucosal casts (Am J Gastroenterol 1998;93:655)
- Associated with different autoimmune conditions such as celiac disease, lupus, pemphigus vulgaris, bullous pemphigoid and Stevens-Johnson syndrome (Am J Surg Pathol 2009;33:1789)
Diagnosis
- Upper gastrointestinal endoscopy (i.e., esophagogastroduodenoscopy [EGD]), which shows the characteristic appearance of sloughed mucosal fragments, along with a biopsy to confirm the diagnosis and rule out other possible conditions
- Meeting 3 of the following endoscopic criteria is consistent with esophagitis dissecans superficialis (EDS) (Ulster Med J 2020;89:39)
- Strip(s) of sloughed esophageal mucosa > 2 cm in length
- Normal underlying esophageal mucosa
- Lack of ulcerations or friability of immediately adjacent esophageal mucosa
Radiology description
- Sloughed out mucosal strips highlighted by barium can be seen on the barium esophagram in few cases (Abdom Radiol (NY) 2021;46:5050)
Prognostic factors
- Favorable prognosis as it commonly resolves spontaneously without complications (Curr Probl Cancer Case Rep 2021;3:100044)
Case reports
- 20 year old man with pemphigus vulgaris presented with acute onset of dysphagia, odynophagia and hemoptysis (Cutis 1999;63:157)
- 50 year old man with a medical history of human immunodeficiency virus (HIV) was hospitalized due to a 3 week course of oropharyngeal dysphagia (Case Rep Infect Dis 2019;2019:4616937)
- 65 year old woman presented with nausea, vomiting, odynophagia and throat pain after ingesting a colored hair dye (Clin Pract 2021;11:185)
- 71 year old man with dysphagia and odynophagia (J Investig Med High Impact Case Rep 2019;7:2324709619892726)
- 81 year old woman with unintentional weight loss of 8 pounds (Cureus 2023;15:e44372)
Treatment
- No standard treatment is available as the condition is self limiting
- Treatment is often decided based on the severity of symptoms
- Proton pump inhibitors are commonly used, although their primary outcome seems to involve minimizing additional injuries, rather than addressing the root cause (Ann N Y Acad Sci 2016;1380:178)
- Patients with resistance to proton pump inhibitors may undergo treatment involving a trial dose of steroids (J Investig Med High Impact Case Rep 2019;7:2324709619892726)
Clinical images
Contributed by Divya Sharma, M.D.

Tissue paper esophagus
Images hosted on other servers:

Vertical white sloughing mucosal strips

Sloughing of large
esophageal mucosa
fragments

Endoscopy showing EDS

Vertical fissures in
distal esophagus with
sloughing of mucosa
Microscopic (histologic) description
- Characterized by intraepithelial splitting, which results in detached fragments of superficial epithelium
- Prominent parakeratosis is the most common histological finding
- Variably sized cysts and bullae (termed intraepithelial cystic degeneration by Hart et al.) (Dig Dis Sci 2015;60:2049)
- Dual tone appearance of esophageal epithelium
- Overlying superficial layer of necrotic, deeply eosinophilic squamous cells
- Deep layer of viable epithelium without degeneration or inflammation
- Basal cell hyperplasia
- Detached fragments may show an association with fungal or bacterial colonies, typically characterized by minimal or focal acute inflammatory responses
Microscopic (histologic) images
Contributed by Divya Sharma, M.D. and @Rasamh86 on Twitter
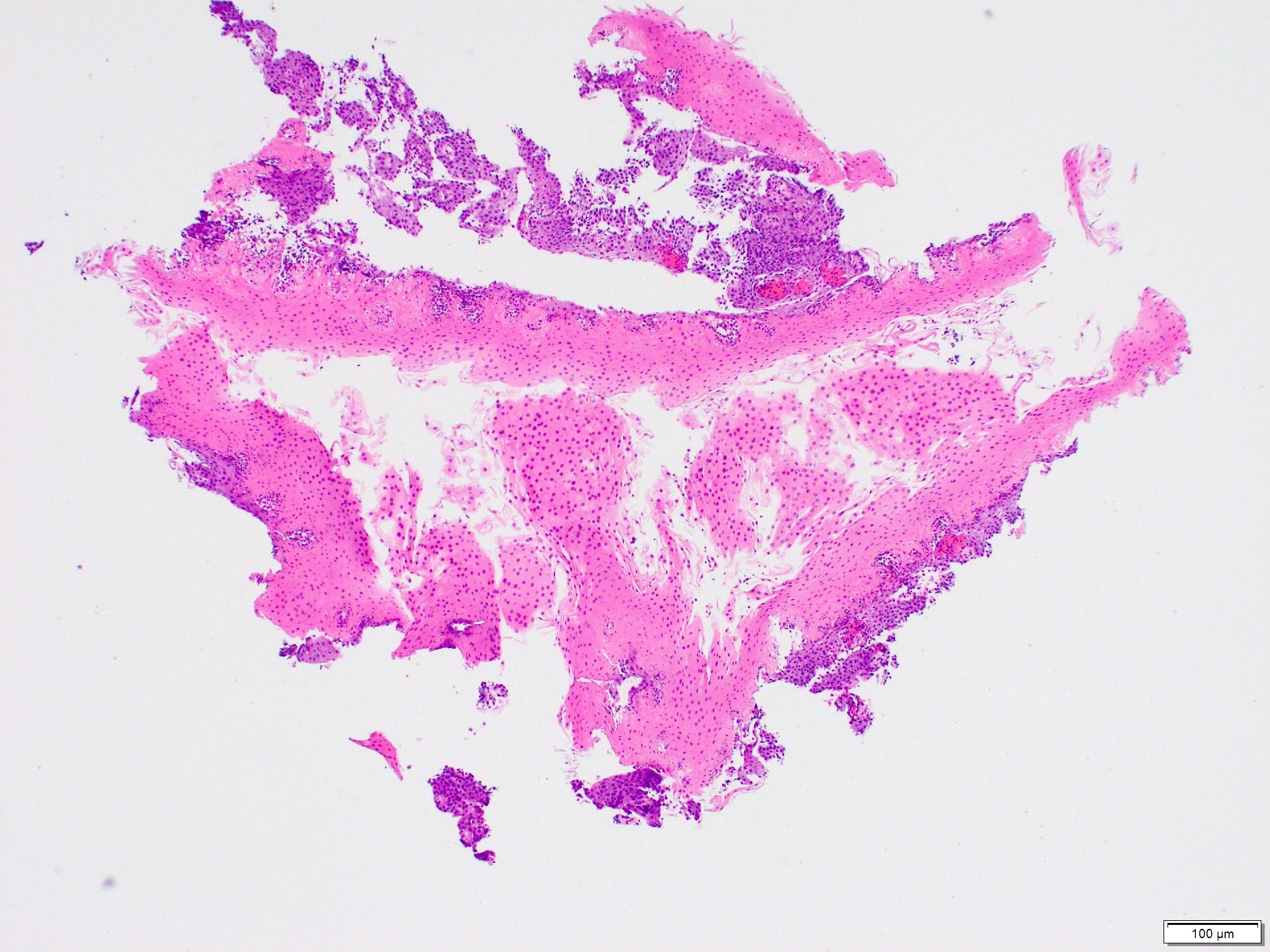
2 tone esophagus
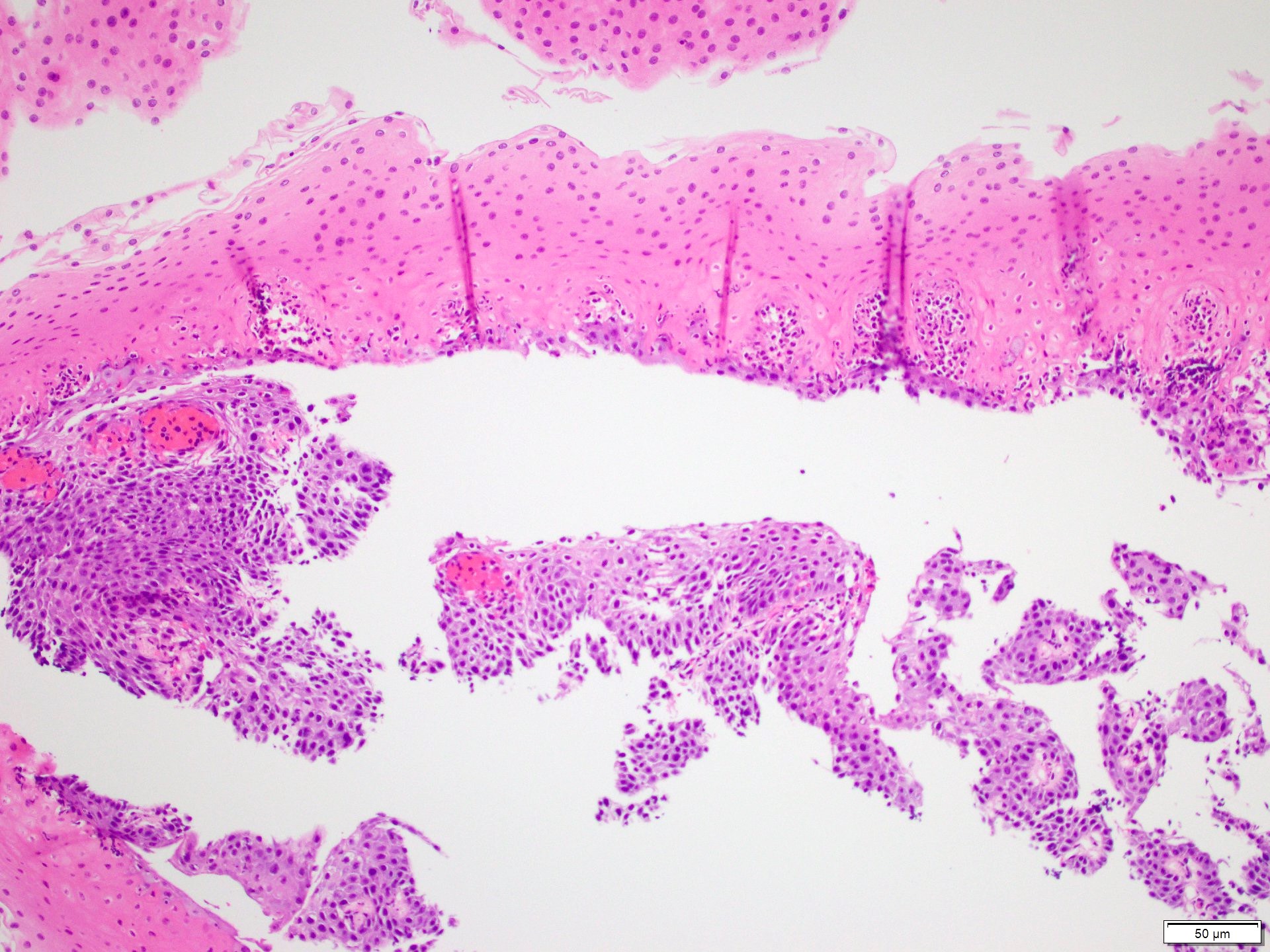
Prominent parakeratosis
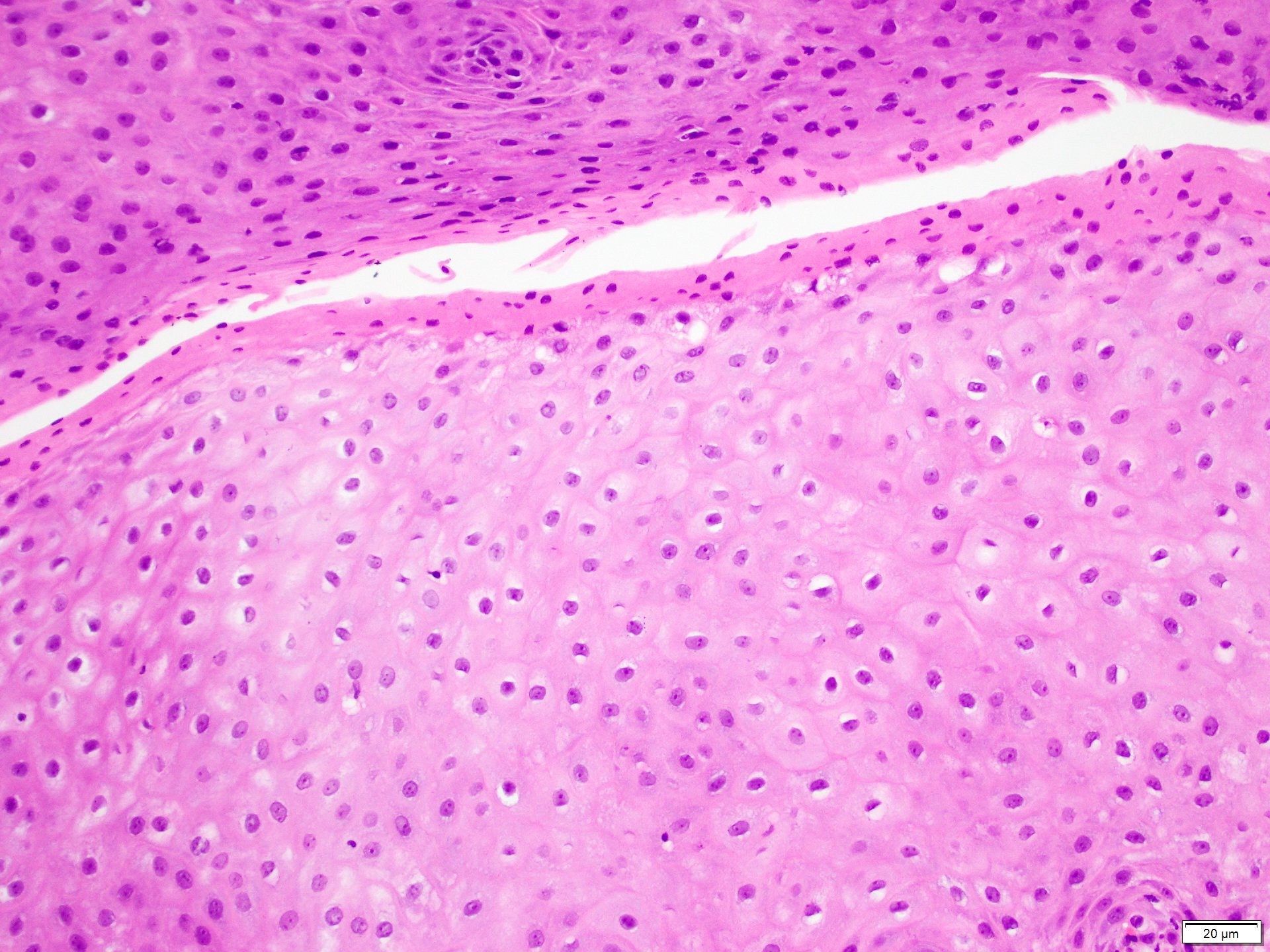
Intraepithelial splitting
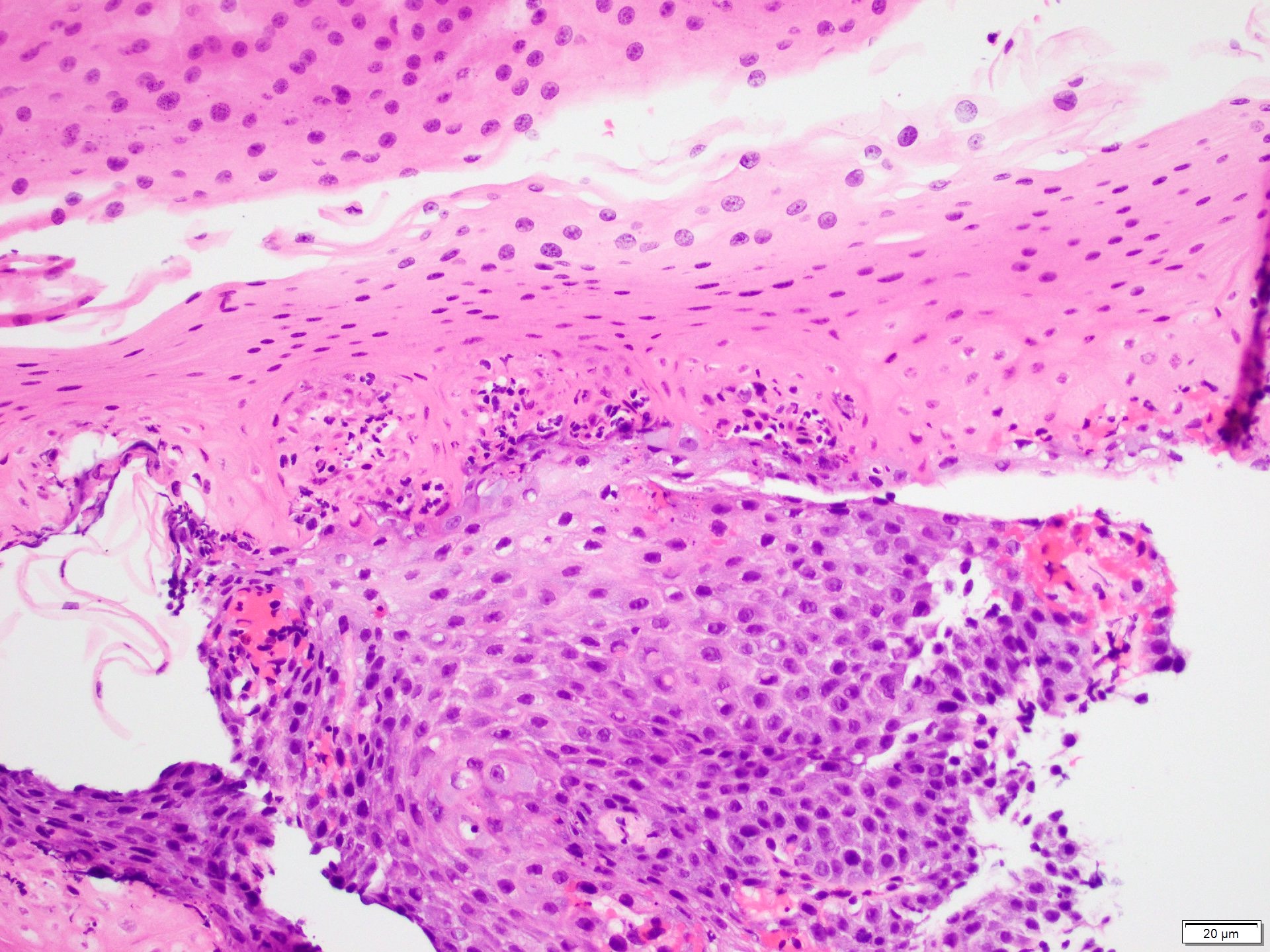
Dense parakeratosis

Intraepithelial cystic degeneration
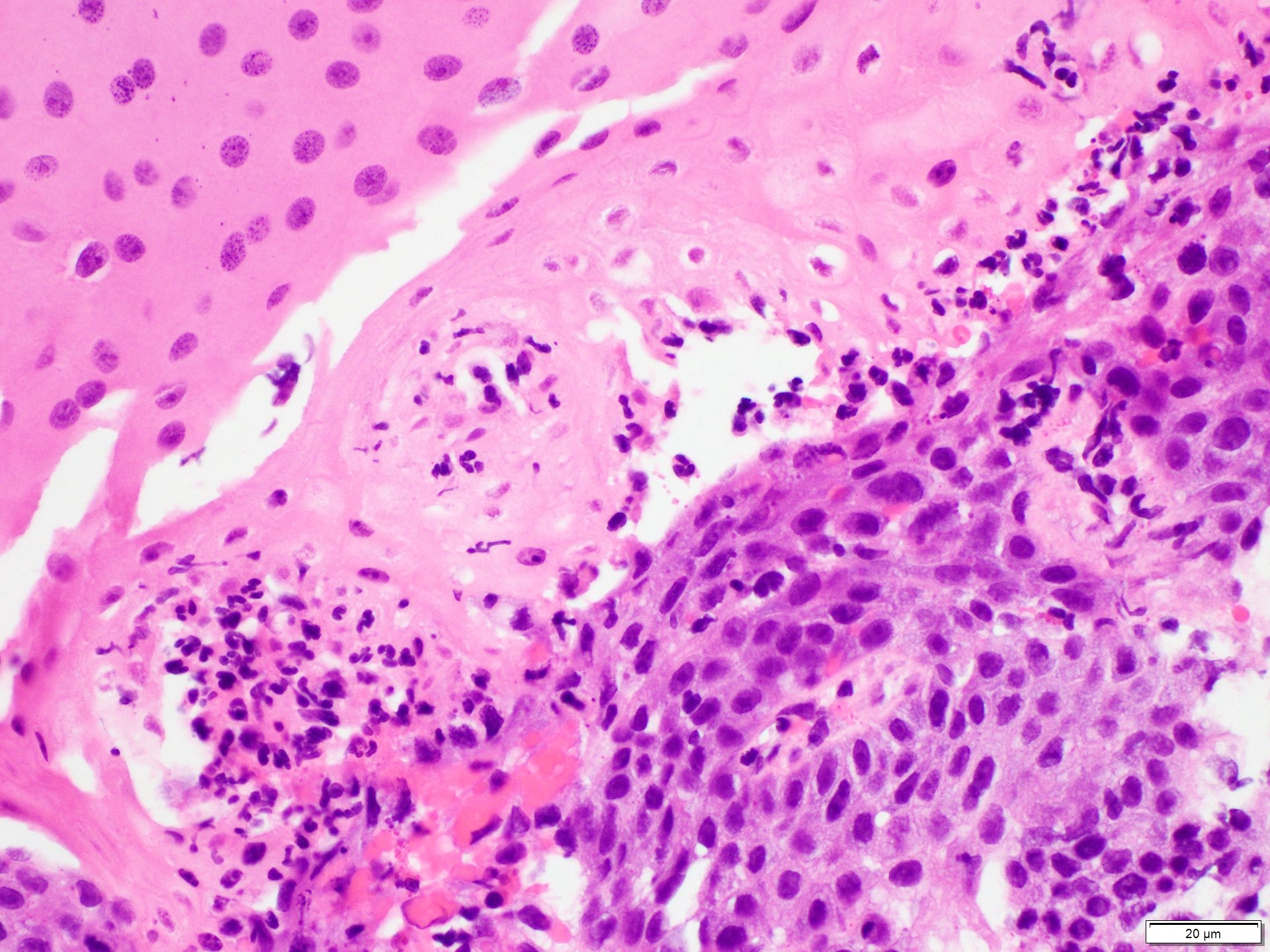
Inflammatory infiltrate

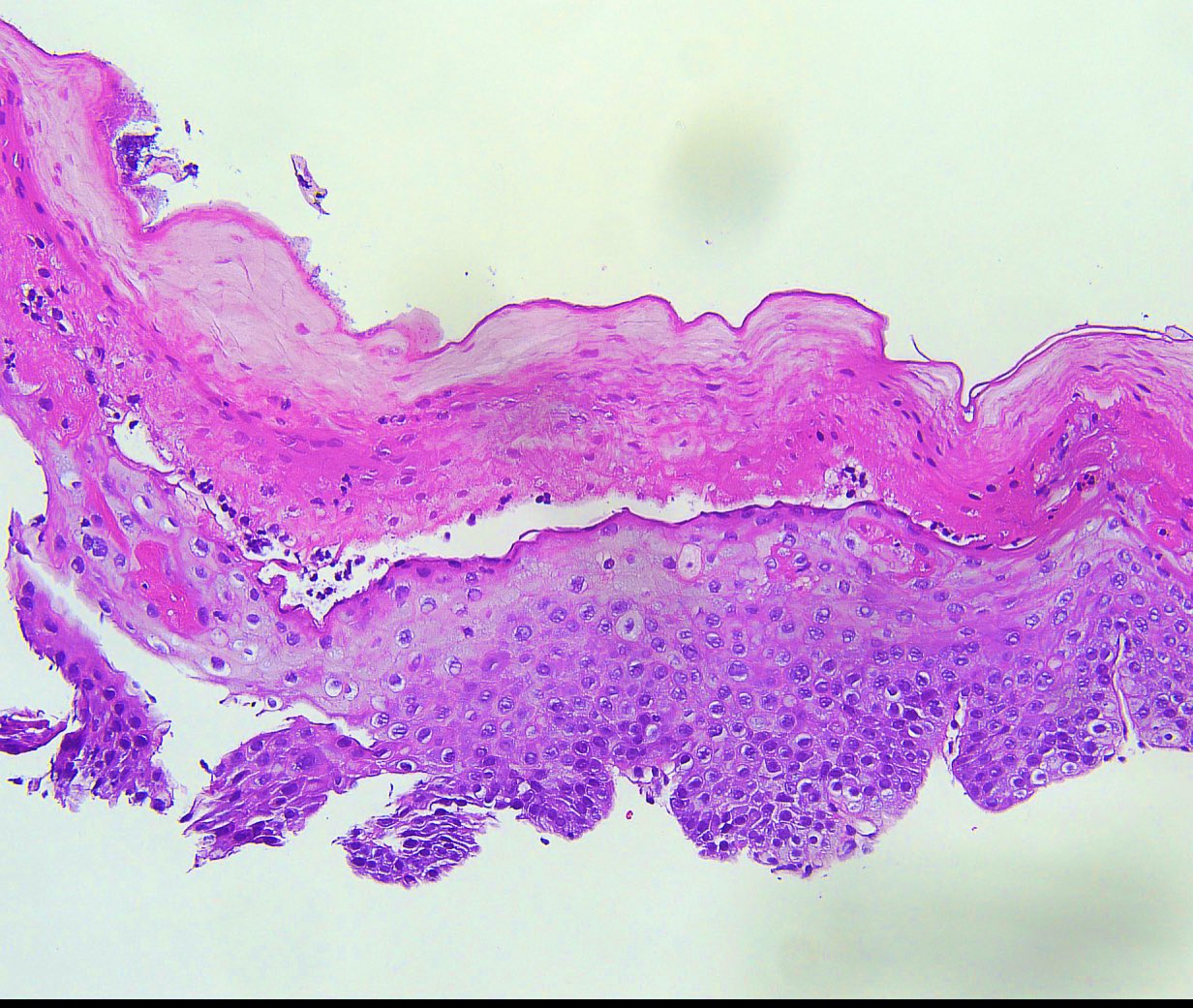
Esophagitis dissecans superficialis
Negative stains
- Grocott methenamine silver (GMS) and Alcian - PAS to rule out Candida
Videos
Sloughing esophagitis
Sample pathology report
- Esophagus, biopsy:
- Morphologic features concerning for esophagitis dissecans superficialis / sloughing esophagitis (see comment)
- Negative for intramucosal eosinophilia, dysplasia or malignancy
- Comment: The etiology is usually unknown but condition has been associated with some medications, bullous dermatoses, motility disorders, physical / thermal injury and autoimmune diseases.
Differential diagnosis
- Candida esophagitis:
- Similar appearance of white plaques on endoscopy
- Erosive esophagitis pattern of injury with acute inflammation, intraepithelial neutrophilic abscesses and epithelial edema most prominent in the superficial epithelial layers on microscopy
- Basal zone hyperplasia, parakeratosis and hyperkeratosis are frequently associated
- Yeast forms and pseudohyphae can be identified on GMS stain
- Epidermoid metaplasia:
- Well demarcated white plaque in the mid to distal esophagus
- Esophageal squamous epithelium with a prominent granular layer and orthokeratosis / hyperorthokeratosis
- Abrupt transition from the adjacent normal squamous epithelium
- Lacks superficial necrosis, epithelial detachment
- Bullous dermatoses involving esophagus (pemphigoid, pemphigus, Stevens-Johnson syndrome):
- Characterized by immune mediated split at different anatomic levels within the basement membrane zone with inflammatory infiltrates
- Complement and Ig deposits can be identified on immunofluorescence using fresh / frozen tissues
- Iatrogenic trauma (endoscopy or specimen handling during biopsy):
- This can result in artifactual intraepithelial splitting
Additional references
Board review style question #1
Which histologic feature is commonly seen in esophagitis dissecans superficialis (EDS)?
- Dual tone appearance of esophagus
- More than 20 eosinophils per high powered field
- Prominent granular layer with orthokeratosis
- Psuedohyphae and yeast forms
Board review style answer #1
A. Dual tone appearance of esophagus is a common histological finding for EDS. Answer D is incorrect because fungal elements (pseudohyphae and yeast forms) are seen in esophageal candidiasis. Answer B is incorrect because increased eosinophils are usually seen with eosinophilic esophagitis. Answer C is incorrect because a prominent granular layer with orthokeratosis is seen in epidermoid metaplasia.
Comment Here
Reference: Esophagitis dissecans superficialis / sloughing esophagitis
Comment Here
Reference: Esophagitis dissecans superficialis / sloughing esophagitis
Board review style question #2
The image above is from an esophageal biopsy in a 46 year old man with dysphagia. Endoscopy of the esophagus shows strips of sloughed esophageal mucosa. Which of the following would be a possible etiology for these endoscopic findings?
- Allergic contact dermatitis
- Chemical exposure
- Immunosuppression
- Use of proton pump inhibitors
Board review style answer #2
B. Chemical exposure can be a causative factor for esophagitis dissecans superficialis (EDS). Answer C is incorrect because immunosuppression can predispose an individual to esophageal candidiasis. Answer A is incorrect because allergic dermatitis can be associated with eosinophilic esophagitis. Answer D is incorrect because proton pump inhibitors are commonly used in the treatment of EDS and do not contribute to causing EDS.
Comment Here
Reference: Esophagitis dissecans superficialis / sloughing esophagitis
Comment Here
Reference: Esophagitis dissecans superficialis / sloughing esophagitis
