
Ear
External ear tumors - malignant
Squamous cell carcinoma of the external auditory canal
Author: Nat Pernick, M.D.

Last author update: 1 October 2013
Last staff update: 12 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma external auditory canal

Table of Contents
Definition / general | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Differential diagnosis | Additional referencesCite this page: Pernick N. Squamous cell carcinoma of the external auditory canal. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/earsccexternal.html. Accessed April 2nd, 2025.
Definition / general
- 15% of primary cutaneous carcinomas of external ear and auditory canal
- Usually age 60+ years
- Poor prognostic factors: > 2 cm, depth > 4 mm, poorly differentiated tumors, perineural invasion, development within a scar, previously treated squamous cell carcinoma at the site, immunosuppression, location within inner portion of canal with deep involvement of temporal bone
- Tumor spread: tumors of helix spread along helix, to antihelix, to posterior surface of ear; tumors of antihelix spread concentrically; tumors of posterior surface spread to helix; tumors of canal tend to invade bone, may destroy tympanic membrane and penetrate middle ear
- Adenoid squamous carcinoma:
- Unusual variant
- Also called pseudoglandular or acantholytic
- Often face and scalp in sun exposed areas, particularly periauricular area
- Due to a desmosomal defect that causes lack of cell adhesion (acantholysis)
Case reports
- 65 year old woman with pigmented squamous cell carcinoma with dendritic melanocyte colonization in the external auditory canal (Pathol Int 1999;49:909)
- 69 year old man with bilateral squamous cell carcinoma of the external auditory canals (Laryngoscope 2002;112:1003)
- 72 year old man with bilateral auditory canal squamous cell carcinoma (HNO 2006;54:41)
- 89 year old man with angiolymphoid hyperplasia with eosinophilia associated to a squamous cell carcinoma of the ear (Dermatol Surg 2004;30:1367)
- Squamous cell carcinoma in situ of external auditory canal (J Laryngol Otol 2006;120:684)
Treatment
- Complete excision (mastoidectomy or temporal bone resection for canal tumors), possibly radiation therapy
- Tumors of external ear have low recurrence rate (Dermatol Surg 2005;31:1423)
- Canal tumors often recur (19%) or metastasize (11%); death may occur due to intracranial extension
Gross description
- Polypoid, firm / rubbery nodules, frequent ulceration
Microscopic (histologic) description
- Well differentiated:
- Most common, composed of infiltrating nests of cells with keratin pearls or individual cell keratinization and intercellular bridges
- Variable nuclear atypia
- Frequent mitotic activity with atypical forms; invasion may be superficial with irregular budding of basal epithelium or irregular tongues of tumor projecting downward
- Moderated differentiated:
- Scattered individually keratinized cells; no keratin pearls
- Poorly differentiated:
- No obvious keratinization but squamous epithelial dysplasia, pavement-like cellular pattern, foci with intercellular bridges
- Spindle cell variant:
- Infiltrating tumor with interlacing bundles or fascicular growth
- Spindled and epithelioid cells with amphophilic or eosinophilic cytoplasm, pleomorphic and hyperchromatic nuclei, increased N/C ratios, frequent mitotic activity with atypical forms
- Often surface ulceration, surface epithelial dysplasia and differentiated squamous cell carcinoma
- May produce chondroid or osteoid matrix
- Adenoid squamous carcinoma:
- Pseudoglandular appearance due to tumor cell acantholysis in center of tumor nests
- Usually dysplastic surface epithelium
Microscopic (histologic) images
Contributed by Semir Vranic, M.D., Ph.D.
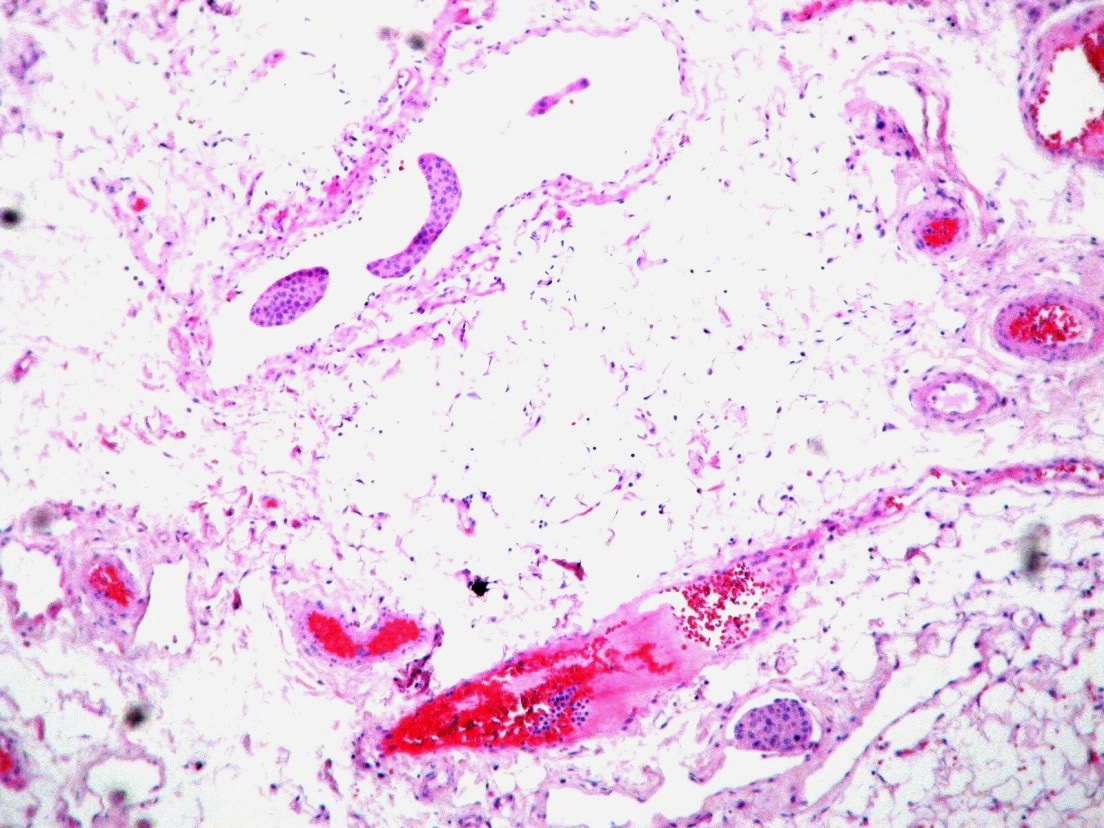
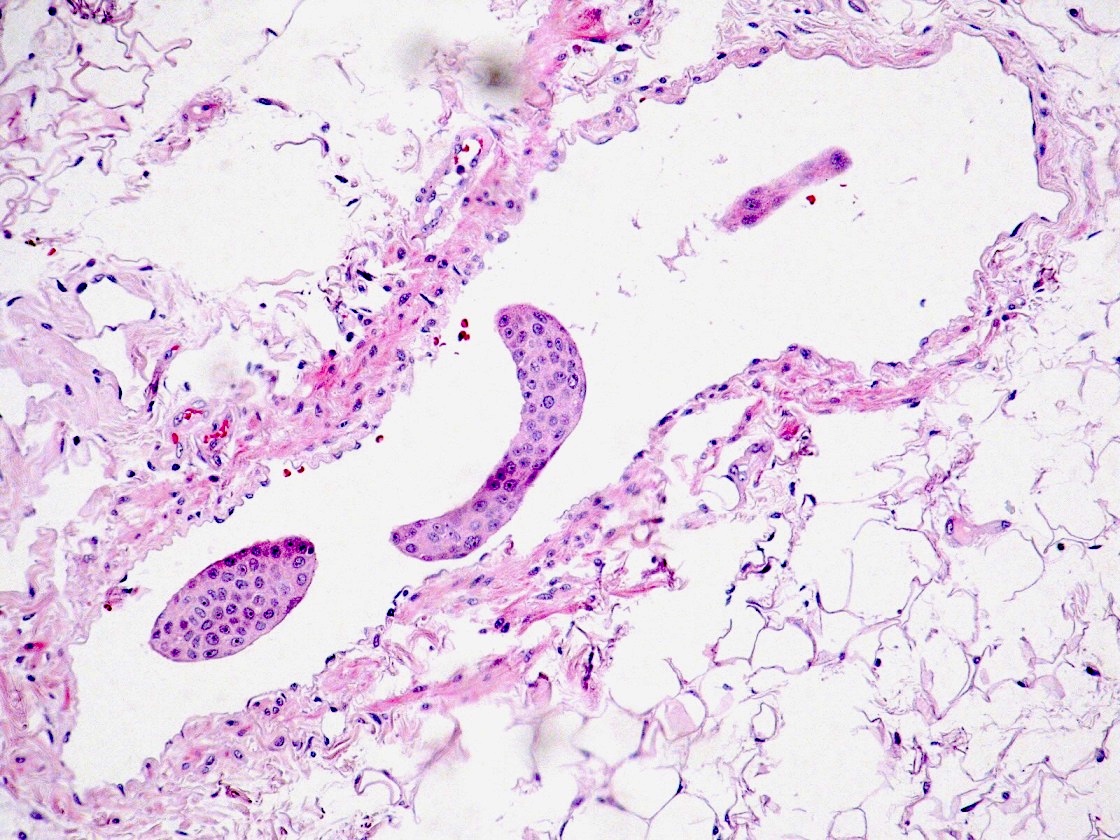
Angiolymphatic invasion
Negative stains
- Adenoid squamous carcinoma: mucin
Differential diagnosis
- Irritated seborrheic keratosis
- Malignant fibrous histiocytoma
- Melanoma
- Pseudoepitheliomatous hyperplasia (Laryngoscope 1998;108:620)
- Adenocarcinoma
- Adenosquamous carcinoma
- Vascular tumors
Additional references
