
Skin nonmelanocytic tumor
Cysts
Epidermoid / epidermal inclusion cyst
Authors: Martina Blazevic, B.S., Bethany R. Rohr, M.D.
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 19 November 2024
Last staff update: 13 January 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Epidermal (epidermoid) cyst

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Blazevic M, Rohr BR. Epidermoid / epidermal inclusion cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocytickeratinouscystepidermal.html. Accessed April 1st, 2025.
Definition / general
- Epidermoid cysts arise as well demarcated dermal papules or nodules, often skin colored to yellow in appearance with a central punctum; they occur most commonly on the face and upper trunk
- Derived from the follicular infundibulum and result in a cystic cavity lined by a stratified squamous epithelium with lamellated keratin flakes in the cyst lumen
Essential features
- Benign lesion
- Cystic cavity is lined by stratified squamous epithelium with a granular layer
- Cyst lumen is filled with lamellated keratin flakes, which grossly appear as a malodorous, cheesy material
- Surgical excision is curative
Terminology
- Epidermoid cyst, epidermal inclusion cyst, epidermal cyst, infundibular cyst, sebaceous cyst (not recommended), keratin cyst
ICD coding
Epidemiology
- Most common cutaneous cyst (Int J Dermatol 2020;59:457)
- M:F = 2:1 (StatPearls: Epidermoid Cyst [Accessed 24 September 2024])
- Adults 20 - 40 years old predominantly affected (StatPearls: Epidermoid Cyst [Accessed 24 September 2024])
Sites
- More commonly face, neck, scalp, trunk, genitalia (Baykal: Clinical Atlas of Skin Tumors, 2014, Actas Urol Esp 2010;34:274, Int Urogynecol J 2022;33:2589)
- Less commonly oral cavity, spine, intrapancreatic accessory spleen (J Nippon Med Sch 2018;85:343, World Neurosurg 2020;139:39, World J Surg Oncol 2016;14:98)
- May occur on buttocks, palms and plantar surface if due to trauma (J Hand Surg Eur Vol 2009;34:792)
- Possibly affects any body part
Pathophysiology
- Occurs spontaneously or from injury induced implantation of epithelium (Eur J Radiol Open 2019;6:291)
- Results from occluded pilosebaceous units at the follicular orifice by bacteria and keratin
- Surface epidermal cells proliferate within the dermis
- Keratin and cell debris accumulate within the cyst sac, leading to cystic dilation
- Typically asymptomatic unless cyst ruptures
- Rarely, squamous cell carcinoma and basal cell carcinoma may arise from the cyst wall (Am J Dermatopathol 1999;21:174)
Etiology
- Sporadic lesions
- Familial inheritance possible in Gardner syndrome (familial adenomatous polyposis) and Gorlin syndrome (StatPearls: Gardner Syndrome [Accessed 25 September 2024], Turk Arch Pediatr 2024;59:170)
- Often found in Favre-Racochot disease, a sporadic disease caused by solar elastotic changes (Int J Dermatol 2004;43:167)
- Medications such as BRAF inhibitors, imiquimod and cyclosporine may increase the risk of developing epidermal cysts (Curr Derm Rep 2013;2:84, Cutis 1992;50:36, Ann Dermatol 2011;23:S182)
Diagrams / tables
Images hosted on other servers:

Resection of epidermoid cyst

Age distribution

Site distribution
Clinical features
- Presents as a well demarcated, dome shaped papule or nodule
- Central punctum is commonly found on the surface (Eur J Radiol Open 2019;6:291)
- Varies in size from a few millimeters to centimeters
- Usually freely mobile unless ruptured, in which case a foreign body giant cell reaction may cause adherence to surrounding connective tissue (J Am Podiatr Med Assoc 1998;88:410)
- Yellow to erythematous in color if inflamed (Eur J Radiol Open 2019;6:291)
- Inflamed cysts may become swollen and tender to palpation or external manipulation (Eur J Radiol Open 2019;6:291)
- White to yellow, foul smelling, cheesy, keratin material may be expressed from the punctum (Eur J Radiol Open 2019;6:291)
- Secondary bacterial infection is possible
Diagnosis
- Clinical diagnosis is most common
- Histopathologic examination in clinically unclear cases
- Laboratory and radiologic examinations are unnecessary
- Reference: StatPearls: Epidermal Inclusion Cyst [Accessed 4 October 2024]
Laboratory
- No specific laboratory findings
Radiology description
- Ultrasound
- Intact epidermoid cysts appear as round or oval anechoic or hypoechoic structures with well defined borders (J Ultrasound Med 2023;42:521)
- Punctum appears as an anechoic tract connecting the cyst to the epidermis (J Ultrasound Med 2023;42:521)
- MRI
- On T1 weighted images, epidermoid cysts display a hypointense signal (Eur J Radiol Open 2019;6:291)
- On T2 weighted images, epidermoid cysts display an intermediate to high intensity signal (Eur J Radiol Open 2019;6:291)
Radiology images
Images hosted on other servers:

Hypoechoic lesion with connecting punctum

MRI
Prognostic factors
- Epidermoid cysts are benign
- May remain small, decrease in size or increase in size
- May rupture and become inflamed or secondarily infected
- Recurrence rates are low following adequate excision
- Reference: StatPearls: Epidermal Inclusion Cyst [Accessed 4 October 2024]
Case reports
- 4 year old girl with pararectal epidermoid cyst following incision and drainage of a right gluteal abscess (Cureus 2024;16:e60989)
- 24 year old man with a penile epidermoid cyst mimicking an ectopic testis mass (Urol Case Rep 2021;40:101962)
- 25 year old man with a sublingual epidermoid cyst (Indian J Otolaryngol Head Neck Surg 2023;75:1137)
- 41 year old woman with squamous cell carcinoma arising from epidermoid cyst of the breast (J Korean Soc Radiol 2023;84:776)
- 64 year old man with intrarenal epidermoid cyst mimicking renal cell carcinoma (Clin Case Rep 2024;12:e9086)
- 68 year old man with epidermoid cyst in the left lobe of the thyroid (Ann Med Surg (Lond) 2024;86:2214)
Treatment
- No treatment required
- Surgical excision of the cyst wall is curative
Clinical images
Images hosted on other servers:

Epidermoid cyst with central punctum

Inflamed epidermoid cyst
Gross description
- Unilocular pearly cyst wall containing white to yellow, malodorous, cheesy material
Gross images
Contributed by the University of Colorado Department of Pathology

Disrupted cyst wall and adjacent soft tissue
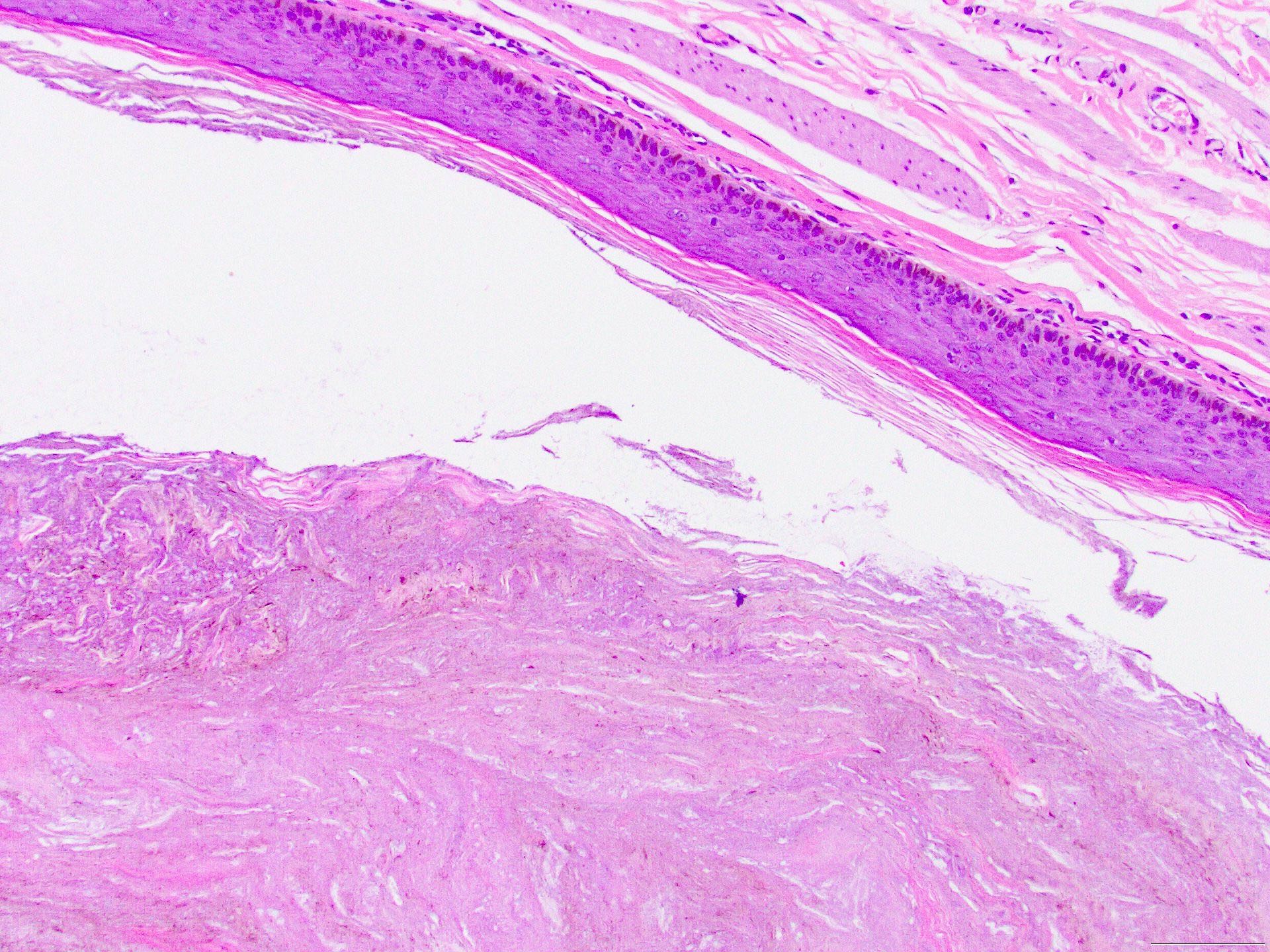
Microscopic (histologic) description
- Stratified squamous epithelium lines the cyst (StatPearls: Epidermoid Cyst [Accessed 24 September 2024])
- Cyst epithelium lacks rete ridges
- Cyst wall contains granular layer filled with keratohyalin granules
- Cyst wall does not contain eccrine glands, sebaceous glands or hair follicles
- Lacks atypia
- Laminated keratin is located within the cyst (StatPearls: Epidermoid Cyst [Accessed 24 September 2024])
- May see connection to the overlying epidermis
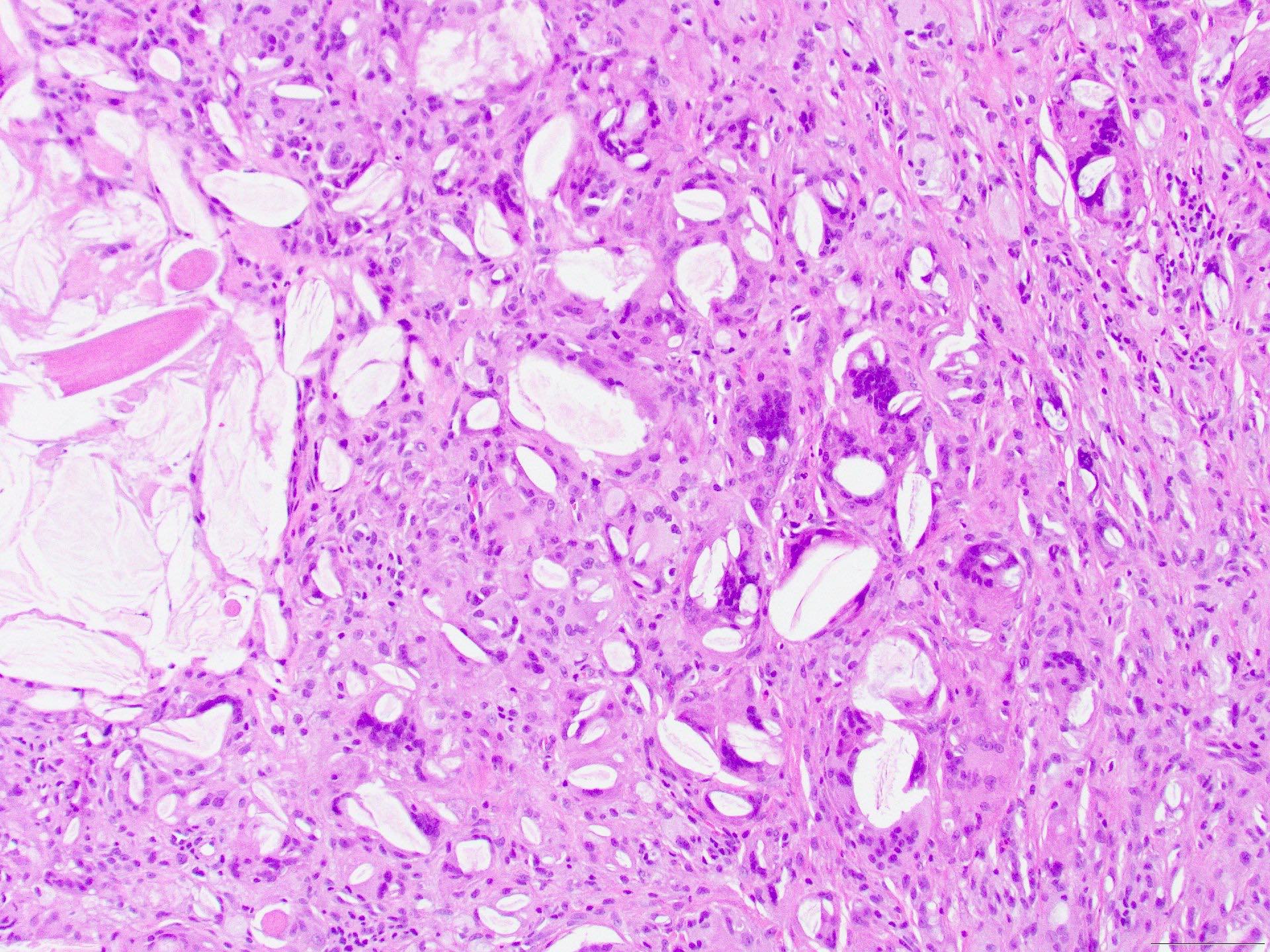
- When ruptured
- Fragments or absences of epithelial lining
- Neutrophilic and histiocytic infiltrate with cyst contents when acute
- Multinucleated giant cells may contain fragments of keratin
- Variants of epidermoid cysts include verrucous cysts, proliferating epidermoid cysts, epidermoid cysts with pilomatrical differentiation and hair matrix cysts (Eur J Dermatol 1998;8:186, J Am Acad Dermatol 1983;8:639, J Cutan Pathol 1995;22:394)
- May be found as a component of hybrid follicular cysts (Am J Dermatopathol 1991;13:228)
Microscopic (histologic) images
Contributed by Bethany R. Rohr, M.D.
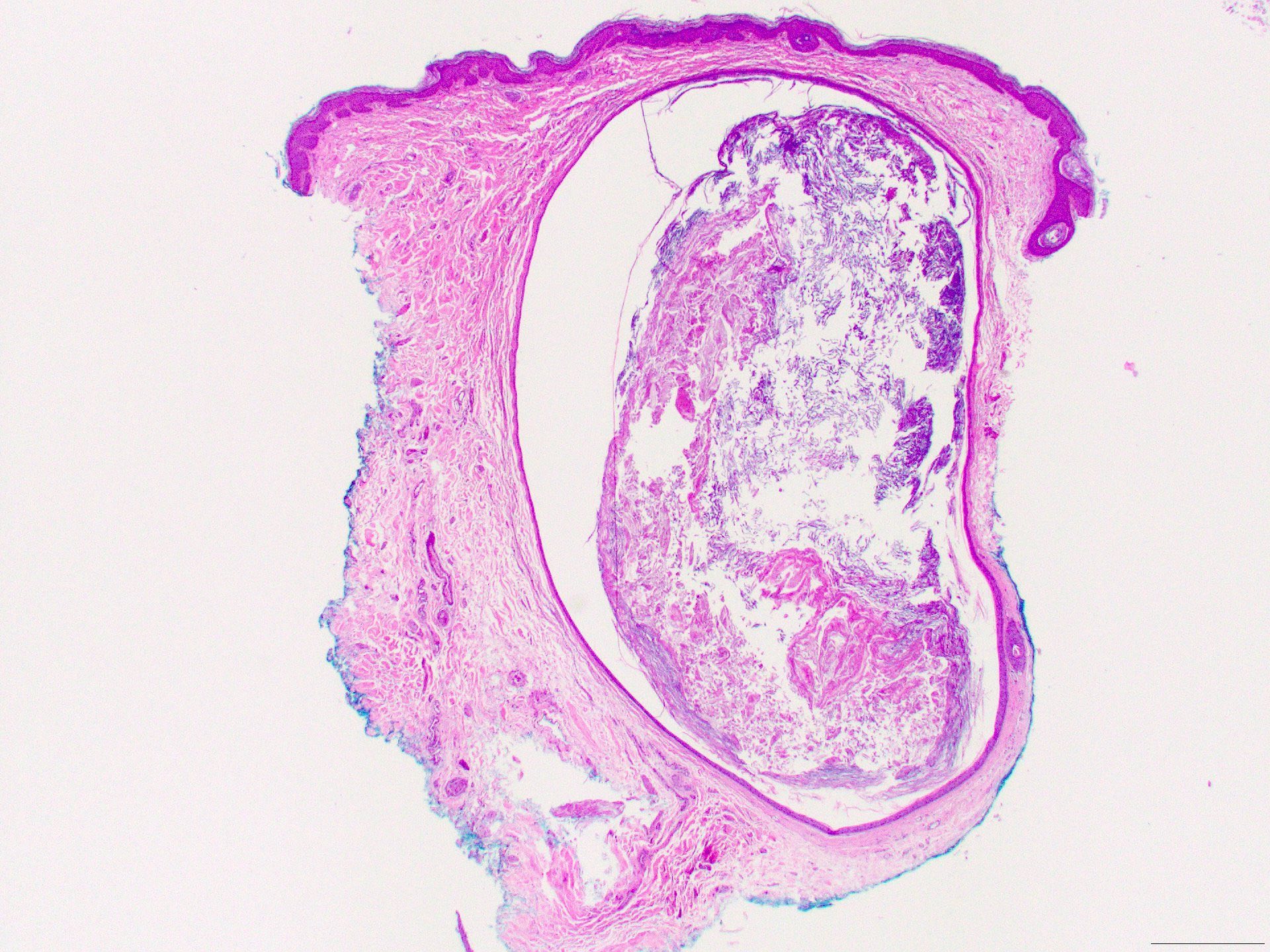
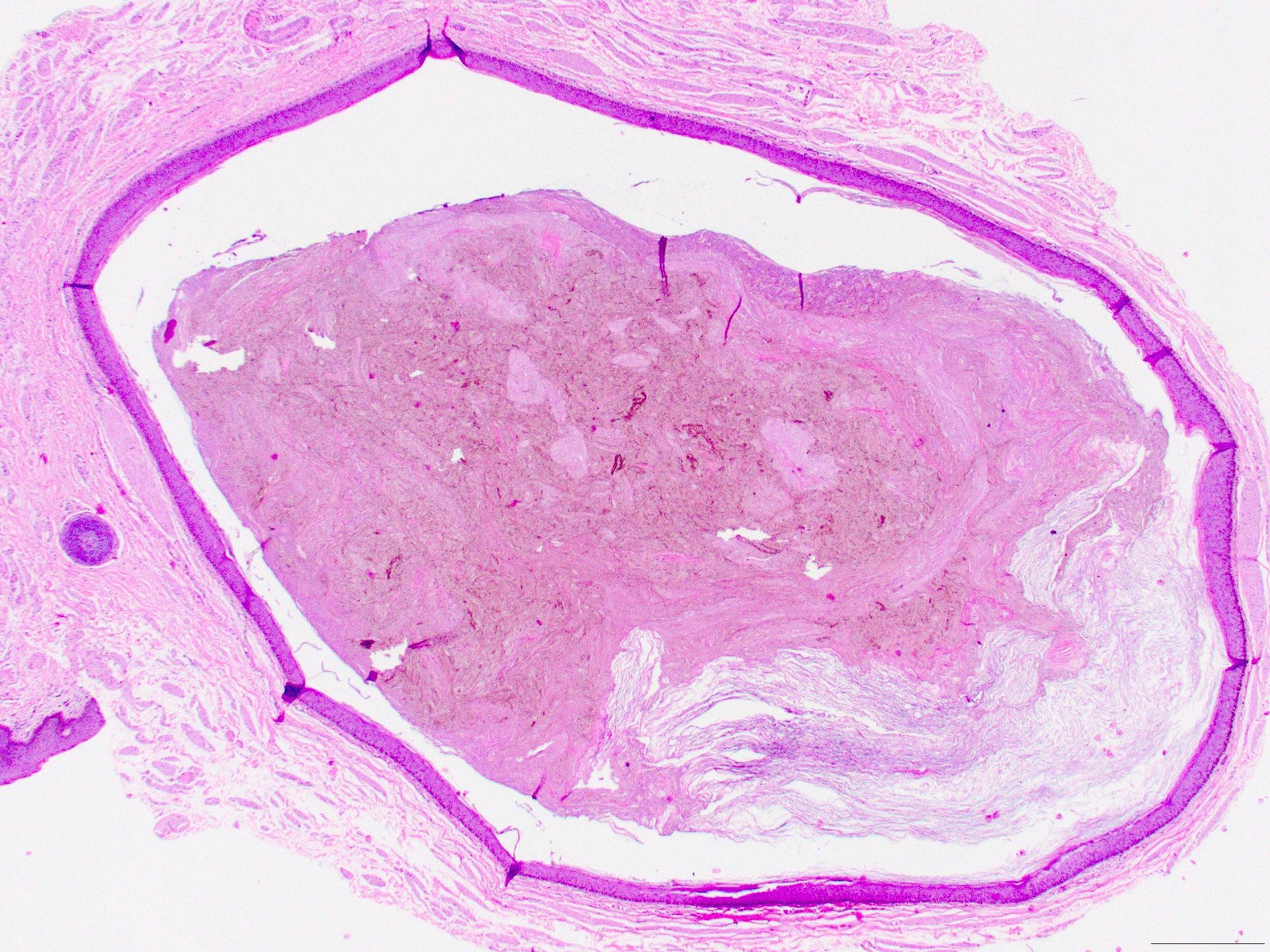
Well circumscribed dermal cyst
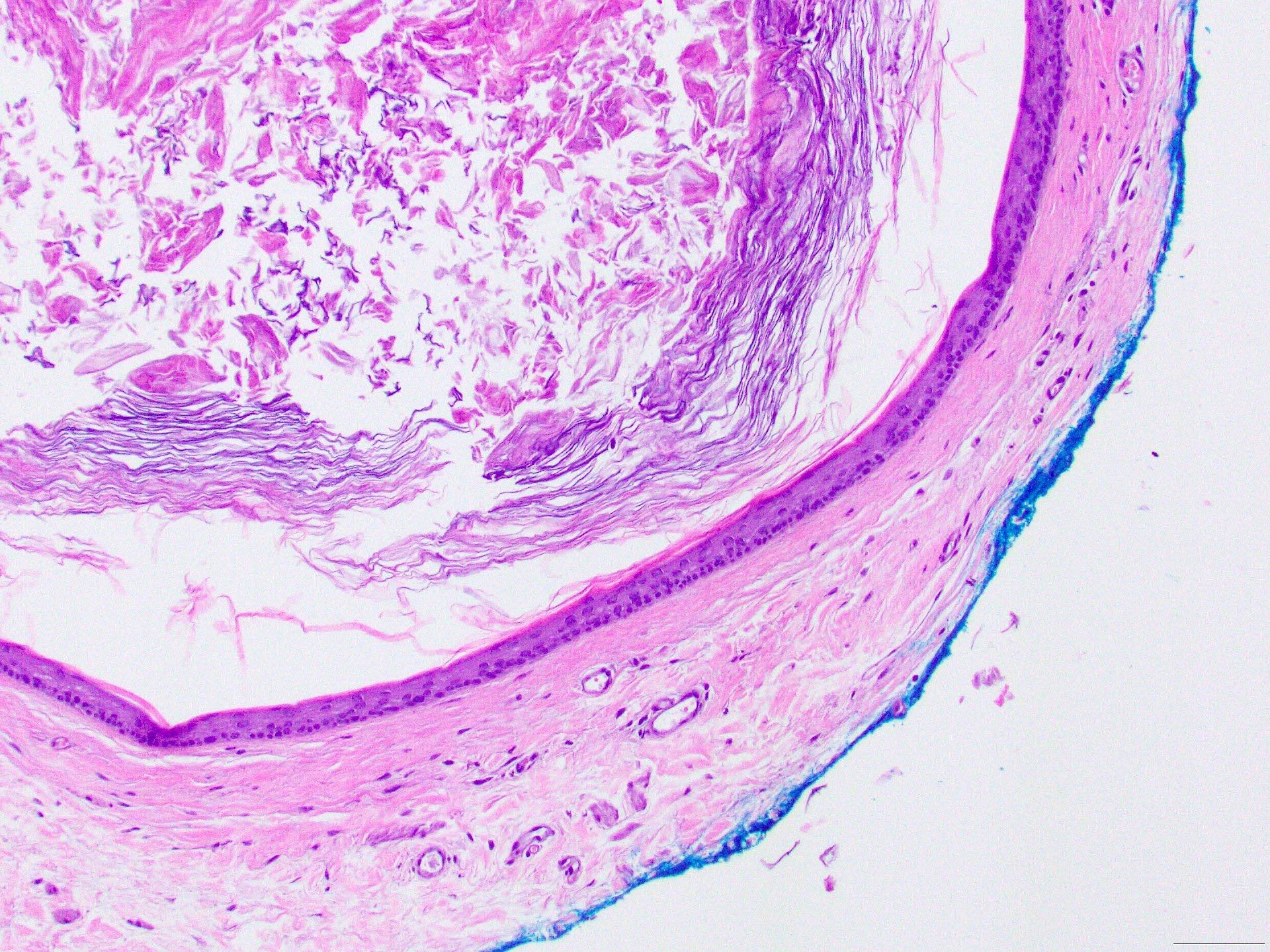
Stratified squamous epithelial cyst lining
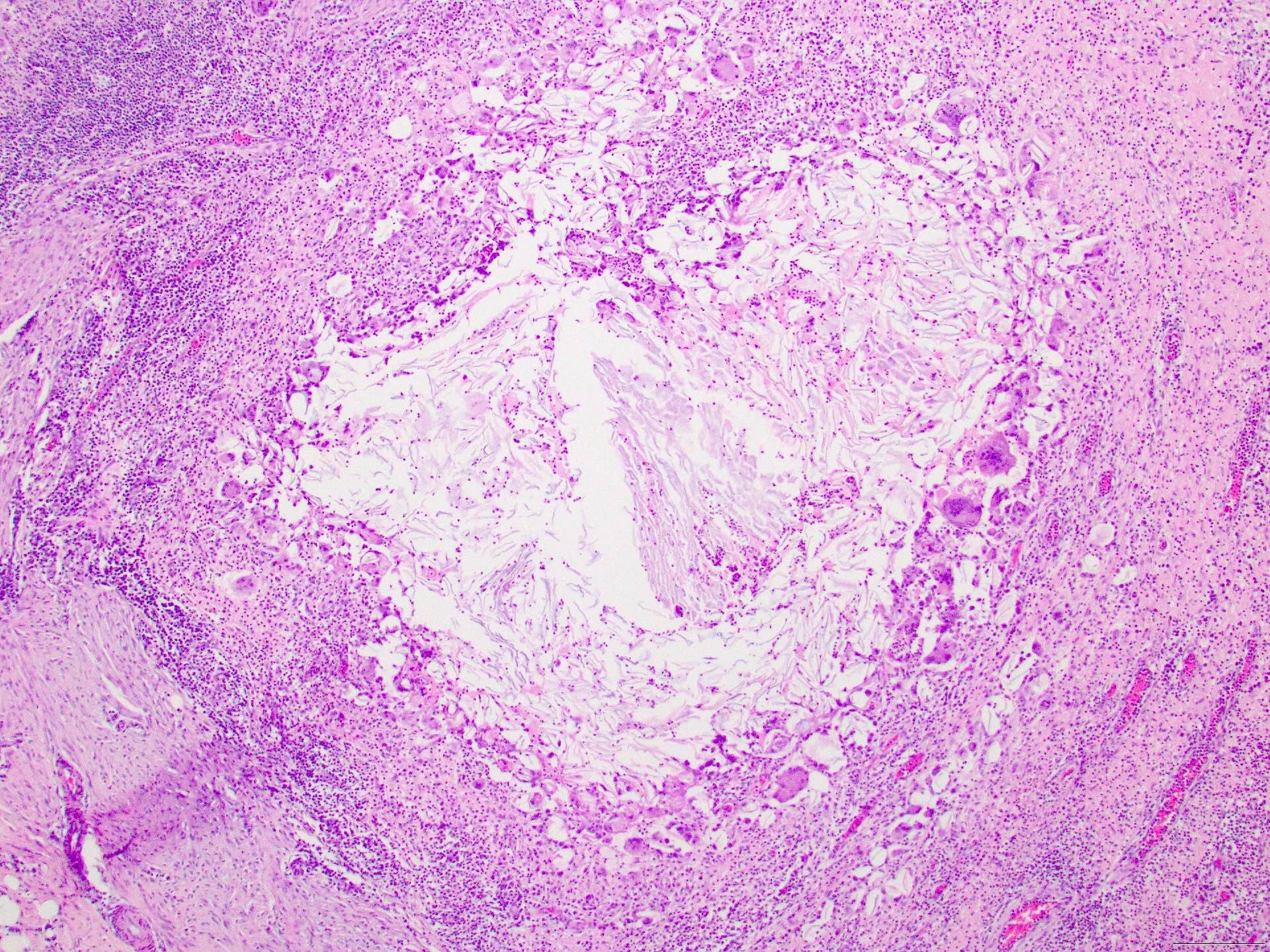
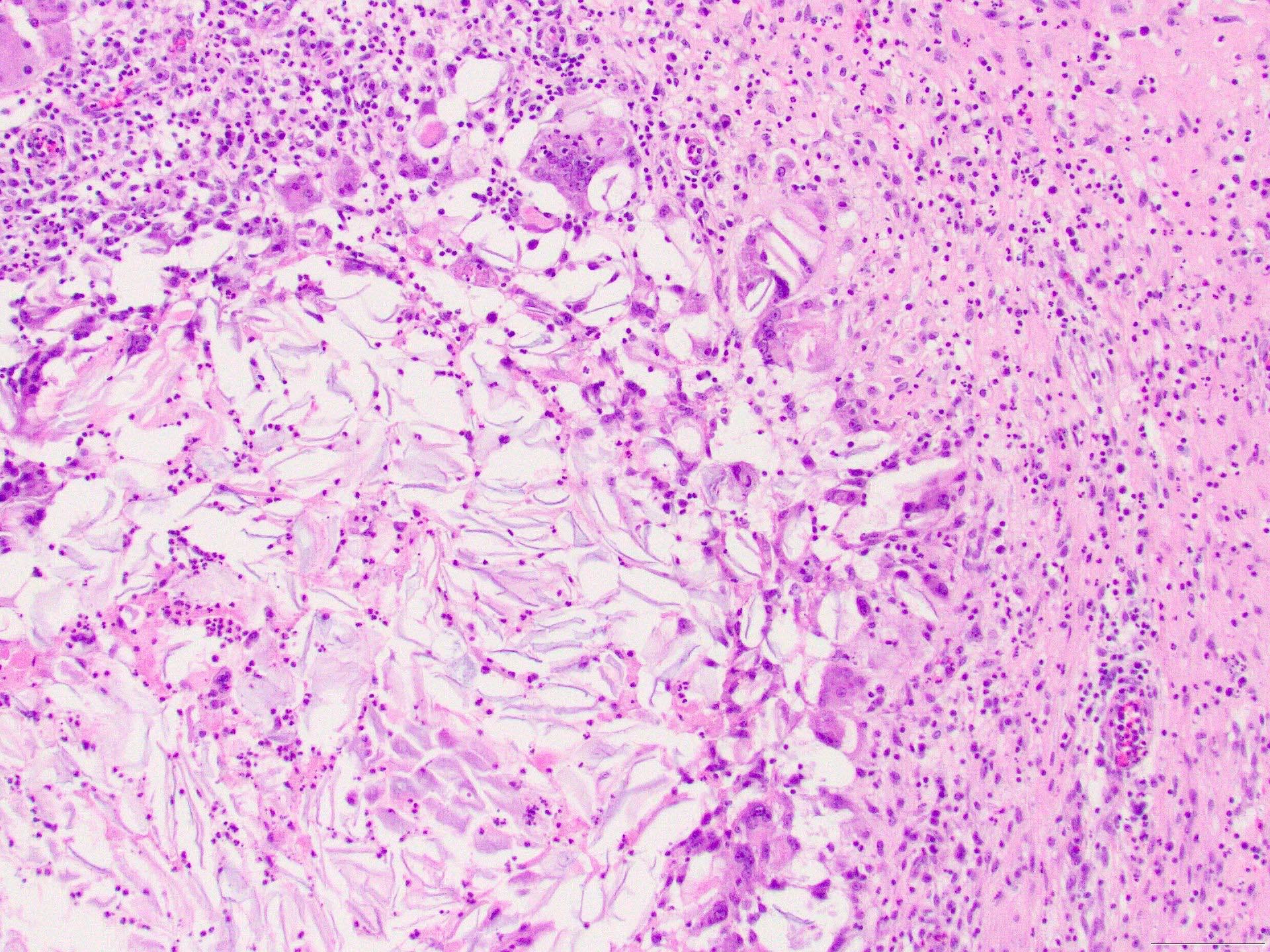
Ruptured cyst
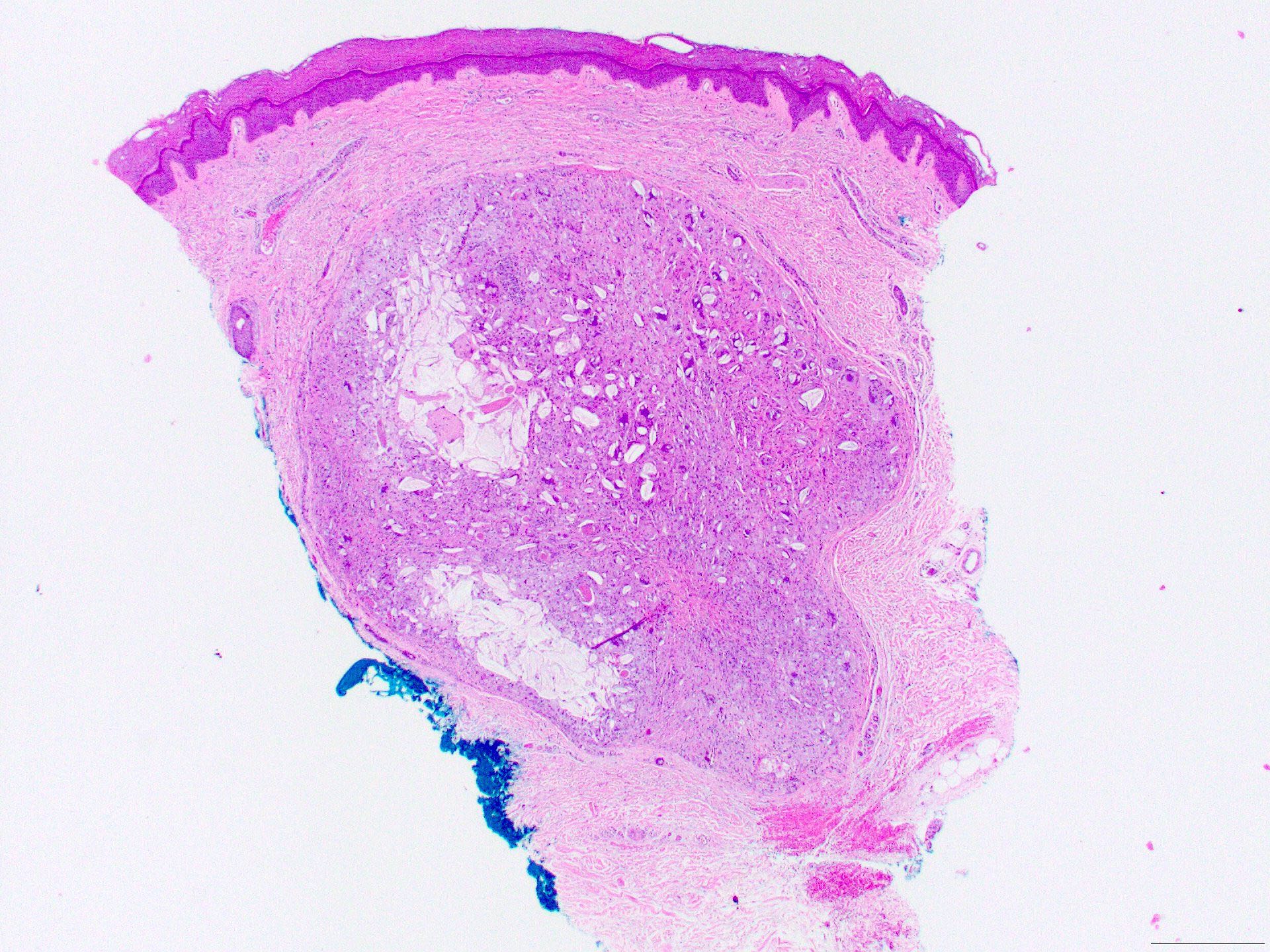
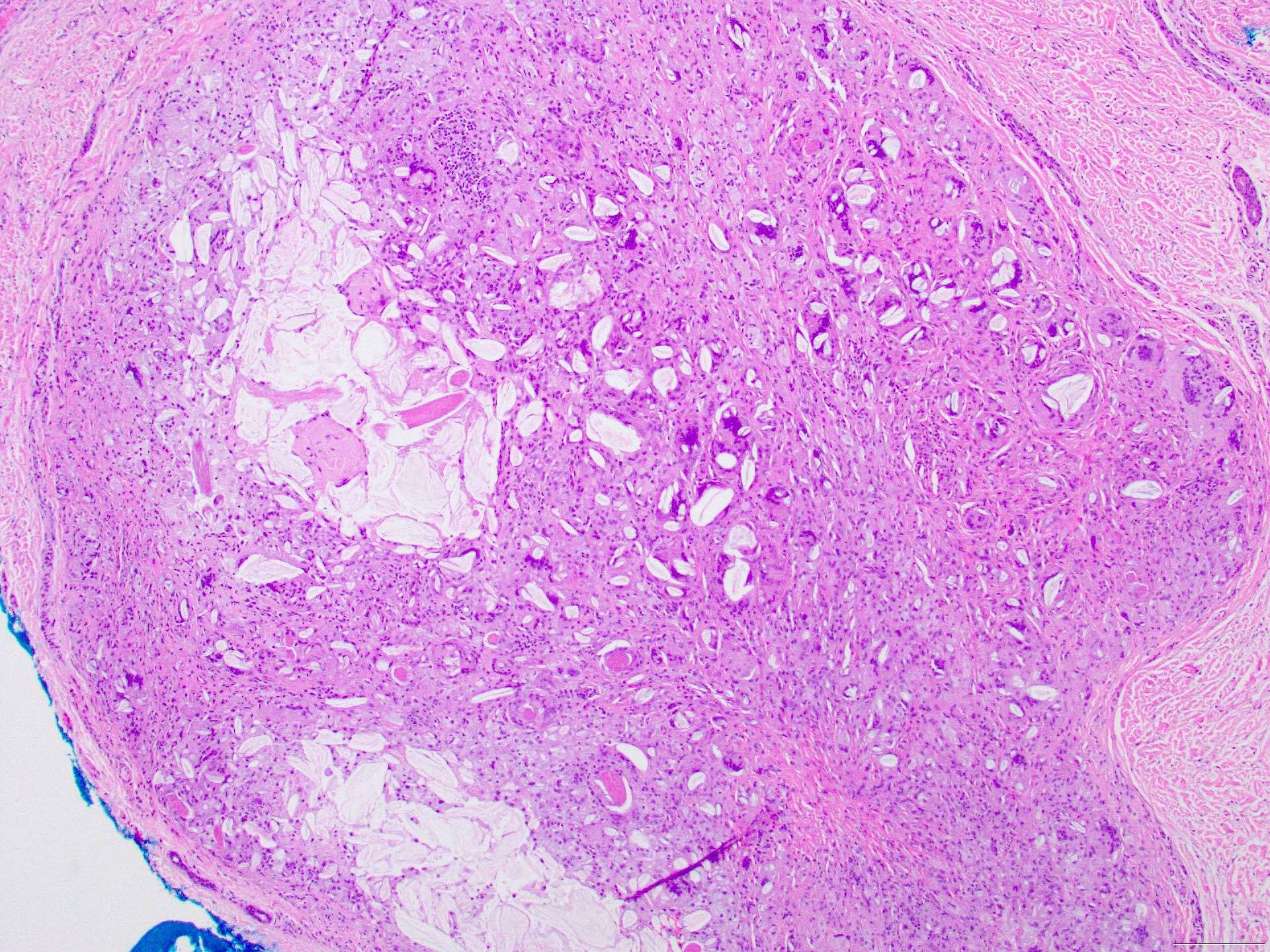
Ruptured epidermoid cyst
Pigmented epidermoid cyst
Positive stains
- Not needed for diagnosis
- Keratin markers will be positive
Negative stains
- Not needed for diagnosis
Videos
Ruptured epidermoid cyst pathology
Sample pathology report
- Skin, back, excision:
- Benign epidermoid cyst (see comment)
- Comment: Microscopic exam reveals a dermal cyst lined by stratified squamous epithelium. Lamellated keratinous material is present in the cyst lumen.
Differential diagnosis
- Trichilemmal (pilar) cyst:
- Firm subcutaneous nodule without a central punctum
- More likely to present on the scalp
- Surrounded by a thick capsule
- Vellus hair cyst:
- Most likely to present on the central chest
- Small, dome shaped papules
- May be dimpled or umbilicated
- Cyst wall contains vellus follicular components
- Histopathology reveals stratified squamous epithelium with a retained granular layer similar to epidermoid cyst; however, the cystic space contains a variable number of vellus hair shafts
- Cutaneous ciliated cyst:
- More likely to present on the lower limb of women
- Presents as a subcutaneous nodule without a central pore
- Histopathology shows a dermally based cyst lined by ciliated simple cuboidal or columnar epithelium
- Cyst lumen filled with debris and secretions
- Pilomatricoma:
- More commonly occurs in pediatric patients
- Derived from hair matrix cells
- Often angulated in shape (tent sign) clinically
- Calcification is often present within the lesion making it hard and bony to palpation
- Eosinophilic cellular outlines of squamous cells (ghost cells) and basophilic matrical cells on histology
- Epidermal cyst with pilomatrical differentiation (hybrid cyst):
- Demonstrates epidermal and trichilemmal cyst features
- Characteristic in Gardner syndrome (familial adenomatous polyposis syndrome)
- Dermoid cyst:
- Stratified squamous cyst epithelial lining with various adnexal structures within the cyst wall
- Eosinophilic cuticle lines the cyst
- Arises on fusion lines from sites of embryonic closure
- Pilonidal cyst / sinus:
- Pseudocyst
- Typically affects the base of the spine or the intergluteal cleft
- Demonstrates dense inflammation of the dermis often with erosion and ulceration of the overlying epidermis
- Contains broken free hair shafts
- Steatocystoma:
- Soft, semitranslucent papulonodules
- Contains an oily, yellow liquid with or without vellus hairs
- Thin walled squamous lining with compressed sebaceous gland within the cyst wall
- Eosinophilic cuticle lines the cyst
- Odontogenic keratocyst:
- Intraosseous lesion
- Contains keratin debris within cyst lumen like epidermoid cysts
- Layered appearance on histology with fibrous tissue on outer layer and stratified squamous epithelium with parakeratosis (Am J Cancer Res 2022;12:3479)
- Lipoma (clinical differential diagnosis):
- Smooth, rubbery, mobile tumor
- Composed of mature adipose tissue with a thin fibrous capsule
Additional references
Board review style question #1
A 50 year old man presents with a 6 mm subcutaneous nodule. Punch excision is shown. What is the most likely diagnosis?
- Dermoid cyst
- Epidermoid cyst
- Lipoma
- Steatocystoma
- Trichilemmal (pilar) cyst
Board review style answer #1
B. Epidermoid cyst. Epidermoid cysts characteristically demonstrate a stratified squamous epithelium with retention of the granular layer. The lining is devoid of eccrine glands, sebaceous glands or hair follicles as shown in the image. Answer A is incorrect because in dermoid cysts, both adnexal and often mesodermal components would be expected on histology including sebaceous glands, hair follicles and shafts in the cyst wall. Answer C is incorrect because lipomas would demonstrate mature adipocytes contained within a thin fibrous tissue. Answer D is incorrect because steatocystomas show a thin walled squamous lining with compressed sebaceous glands within the cell wall. Answer E is incorrect because on histopathology, pilar cysts lack a granular layer and contain dense lamellated keratin unlike the flaky appearance of keratin in epidermoid cysts. Trichilemmal (pilar) cyst walls also lack a granular layer, unlike epidermoid cysts.
Comment Here
Reference: Epidermal (epidermoid) cyst
Comment Here
Reference: Epidermal (epidermoid) cyst
Board review style question #2
Which of the following components is most likely to be found on histopathology of an epidermoid cyst?
- Abrupt keratinization with absence of a granular layer
- Compressed sebaceous glands within the cyst wall
- Dermal structure lined by ciliated simple cuboidal epithelium
- Squamous cells with an eosinophilic cellular outline (shadow cells)
- Stratified squamous epithelium with a retained granular layer
Board review style answer #2
E. Stratified squamous epithelium with a retained granular layer. Epidermoid cysts are characteristically defined on histology by the retained granular layer filled with keratohyalin granules in the cyst wall. Answer A is incorrect because abrupt keratinization with absence of a granular layer is characteristic of trichilemmal (pilar) cysts. Answer B is incorrect because steatocystomas contain compressed sebaceous glands within the cyst wall. Epidermoid cysts do not contain sebaceous glands, reinforcing the preference for discontinuing the use of the term sebaceous cyst. Answer C is incorrect because ciliated cuboidal epithelium found in a dermal structure is the description of a cutaneous ciliated cyst. Answer D is incorrect because squamous cells with an eosinophilic cellular outline are a description of the shadow or ghost cells found in pilomatricoma. Occasionally, foci of pilomatrical differentiation may be seen in epidermoid cysts and may represent a cutaneous marker for Gardner syndrome.
Comment Here
Reference: Epidermal (epidermoid) cyst
Comment Here
Reference: Epidermal (epidermoid) cyst
