
Ear
Middle ear and inner ear tumors - benign / nonneoplastic
Cholesteatoma
Author: Kelly Magliocca, D.D.S., M.P.H.
Editorial Board Members: Ruta Gupta, M.D., Molly Housley Smith, D.M.D.

Last author update: 18 January 2023
Last staff update: 17 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Cholesteatoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Classification | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Magliocca K. Cholesteatoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/earcholesteatoma.html. Accessed April 2nd, 2025.
Definition / general
- Cholesteatoma is a benign, nonneoplastic destructive lesion in the middle ear or mastoid, most commonly unilateral
- Accumulation of keratinizing stratified squamous epithelium and keratinous debris, with stromal fibrosis and associated inflammatory reaction, leads to destruction of adjacent structures (e.g., bone) including components of ossicular chain, eventually producing clinical symptoms
Essential features
- Located in middle ear or mastoid, may involve medial external canal
- Cystic strips of nonneoplastic, nondysplastic keratinizing squamous epithelium, with a prominent granular layer, keratin debris and background stromal inflammation
- History of chronic otitis media is present in most
- 2 general forms: congenital and acquired; acquired cholesteatoma is more common than congenital cholesteatoma
- Clinical findings include expansile pearly cyst within the middle ear or mastoid cavity
- Pathophysiology is likely multifactorial and remains controversial
- Treatment is surgical but may recur locally
- Untreated cholesteatoma progresses, can become infected and can lead to conductive hearing loss and serious intracranial complications
Terminology
- Cholesteatoma (chole = cholesterol, steat = fat, oma = benign tumor) is a misnomer, as the lesion is nonneoplastic and diagnostic microscopic features do not include cholesterol or fat
- Less frequently used terms for middle ear cholesteatoma: epidermal cyst, epidermoid cysts or epidermal inclusion cyst
- Also known as keratoma, although this term can be confused with keratosis obturans, which is an external auditory canal lesion and is not typically osteolytic
- Middle ear atelectasis and retraction pockets are not considered cholesteatomas as long as they do not retain keratin debris (Otol Neurotol 2019;40:63)
ICD coding
- ICD-10: H60.41 - cholesteatoma of right external ear
Epidemiology
- Annual incidence ranges between 3 - 14 per 100,000 children and 9.2 - 13 per 100,000 adults, with slight male predilection (M:F = 1.4:1) (Acta Otolaryngol 1999;119:568, Eur Arch Otorhinolaryngol 2004;261:6)
- Incidence and detection of congenital cholesteatoma is on the rise, possibly due to technological advances (Eur Ann Otorhinolaryngol Head Neck Dis 2010;127:143)
- Due to treatment advances in otic pathology, acquired cholesteatoma is decreasing due to adequate treatment of otitis media (Eur Ann Otorhinolaryngol Head Neck Dis 2010;127:143)
- Conditions involving cleft palate or ear anomalies show increased tendency for cholesteatoma formation (Auris Nasus Larynx 2014;41:101, Int J Pediatr Otorhinolaryngol 2013;77:1403)
- Association with allergic rhinitis (Laryngoscope 2018;128:547)
Sites
- Usually the middle ear is affected with potential destruction of surrounding structures, including bone, ossicular chain, erosion into external ear, inner ear and cranial cavity
- Congenital cholesteatoma tends to arise in the superior anterior middle ear, possibly in area of tensor tympani (Eur Arch Otorhinolaryngol 2020;277:987, Head Neck Pathol 2022;16:224)
- Acquired cholesteatoma tends to arise in the superior posterior middle ear, posterior epitympanic (pars flaccida) or posterior mesotympanic (posterior superior quadrant of the pars tensa) (Braz J Otorhinolaryngol 2017;83:126)
- External ear cholesteatoma has been rarely reported and remains controversial and difficult to distinguish from keratosis obturans (J Am Acad Dermatol 2011;65:e88, Otol Neurotol 2013;34:91, Otolaryngol Head Neck Surg 2015;152:326)
Pathophysiology
- Pathophysiology of congenital and acquired cholesteatoma remains controversial
- Congenital:
- Epidermoid formation suggested as etiology; pathophysiology of cholesteatoma formation is unknown (Head Neck Pathol 2018;12:419, Pediatr Ann 2016;45:e167)
- Tensor tympani tendon suggested as etiology; pathophysiology of cholesteatoma formation is unknown (Head Neck Pathol 2022;16:224)
- Acquired (Otolaryngol Clin North Am 2006;39:1143, J Laryngol Otol 2007;121:1013, Otolaryngol Head Neck Surg 2009;140:884, J Laryngol Otol 1989;103:149, Laryngoscope 2015;125:234):
- Mechanism by which the epithelium enters the middle ear is probably via a combination of 1 or more of the proposed mechanisms below:
- Retraction theory: retraction pockets of pars flaccida (or pars tensa or both) is caused by negative pressure of the middle ear leading to cholesteatoma; during these processes, an inclusion of keratinized squamous epithelium may occur, leading in a few cases to cholesteatoma formation
- Migration theory: migration of squamous epithelium from the external surface of tympanic membrane or external canal, through a traumatic or iatrogenic defect
- Squamous metaplasia: still others believe cholesteatoma is due to middle ear metaplasia, essentially due to chronic irritation
- Basal cell hyperplasia (papillary ingrowth) theory: formation of keratin filled microcysts in the basal layer of the epithelium
- Mechanism by which the epithelium enters the middle ear is probably via a combination of 1 or more of the proposed mechanisms below:
Etiology
- Congenital cholesteatoma:
- Persistent epidermoids (Head Neck Pathol 2018;12:419, Pediatr Ann 2016;45:e167):
- Most commonly accepted etiology is an embryologic defect known as persistent epidermoids (squamous epithelium present in the fetus in middle ear mucosa adjacent to the tympanic membrane), that fail to resorb
- These structures are found on the lateral anterior superior surface of the middle ear in the temporal bones after 15 week gestation and typically disappear during the first postpartum year
- If epidermoid formations fail to resorb, they presumably continue to grow and develop into congenital cholesteatomas
- Tensor tympani tendon (Head Neck Pathol 2022;16:224):
- Histologic examination confirmed the connection between the cholesteatomatous sac and tensor tympani tendon; one group correlated imaging, intraoperative findings and histology, proposing that the tensor tympani tendon could be the primary site from which congenital cholesteatoma originates
- Persistent epidermoids (Head Neck Pathol 2018;12:419, Pediatr Ann 2016;45:e167):
- Acquired cholesteatoma can be due to recurrent otitis media, traumatic or iatrogenic tympanic membrane perforation
Diagrams / tables
Images hosted on other servers:

Acquired cholesteatoma
Clinical features
- Congenital cholesteatomas:
- Clinical appearance: white or yellow mass, may have foul odor
- Most commonly unilateral
- Age: infancy and early childhood
- Gender predilection: none
- Most common location: anterior superior quadrant of the middle ear
- Status of tympanic membrane: intact
- Otorrhea: absent
- History of otologic surgery: none
- History of otitis media: possible
- Symptoms: many asymptomatic; may vary depending on extent of disease
- Conductive hearing loss: possible
- Acquired cholesteatomas:
- Clinical appearance: white or yellow mass, may have foul odor
- Most commonly unilateral, bilateral in ~15 - 17% (Braz J Otorhinolaryngol 2017;83:126)
- Age: any, most commonly adults
- Gender predilection: slight male
- Most common location: posterior superior
- Status of tympanic membrane: intact or disrupted
- Otorrhea: present or absent
- History of otologic surgery: yes
- History of otitis media: yes, prevalence of cholesteatoma in patients with chronic otitis media 20 - 25%
- Symptoms: otalgia, conductive hearing loss, vertigo, tinnitus; may vary depending on disease extent
Classification
- Cholesteatoma is separated into 2 types: congenital and acquired
- Acquired cholesteatoma comprises the majority of cases (95 - 98%)
- One additional type, unclassifiable cholesteatoma, has been suggested, although it remains controversial
- Congenital cholesteatoma:
- Rare, 2 - 5% of cholesteatoma cases
- Presumed to be present at birth and diagnosed in childhood
- Etiology and pathophysiology debated
- Most commonly used criteria for distinction from acquired (Levenson's criteria) (Otolaryngol Clin North Am 1989;22:941):
- White mass in middle ear cavity, medial to an intact tympanic membrane
- Normal pars flaccida and pars tensa of the tympanic membrane
- No past history of otorrhea and perforations
- No prior otologic surgery
- Past history of otitis media should not be an exclusion criterion
- Acquired cholesteatoma:
- Primary acquired (PAC): usually arises in the setting of retraction of the tympanic membrane (TM), as a result of otitis media or chronic eustachian tube dysfunction; negative middle ear pressure due to eustachian tube dysfunction, poor pneumatization of the mastoid, inflammation or TM atrophy leads to TM retraction
- Arises as a diverticulum from the pars flaccida > pars tensa
- Invagination is the most accepted theory of PAC
- Progressive retraction forms a pocket resulting in disrupted normal epithelial migration and drainage of keratin debris
- As this process progresses, a cholesteatoma forms
- Secondary acquired (SA): occurs in the setting of TM perforation, with subsequent epithelial migration
- TM perforation is associated with inflammation and eustachian tube dysfunction
- Results in proliferation of keratinizing epithelium
- External canal cholesteatoma (ECC):
- ECC as a third type of acquired cholesteatoma remains controversial
- Generally occurs in older aged individuals
- Present with otorrhea and unilateral chronic pain
- Does not produce a conductive hearing loss
- Probably arises as result of a minor trauma in external ear canal, inducing an osseous defect secondary to periostitis and osteonecrosis
- Surrounding squamous epithelium will then invaginate and proliferate within the affected bone and squamous keratinized material will accumulate in the external ear canal
- Tympanic membrane generally intact
- Primary acquired (PAC): usually arises in the setting of retraction of the tympanic membrane (TM), as a result of otitis media or chronic eustachian tube dysfunction; negative middle ear pressure due to eustachian tube dysfunction, poor pneumatization of the mastoid, inflammation or TM atrophy leads to TM retraction
- Unclassified cholesteatoma:
- Cholesteatoma whose origin cannot be accurately determined; difficult to establish confidently whether the cholesteatoma is congenital or acquired
- Distinction supported by The European Academy of Otology and Neurotology and Japan Otological Society (EAONO / JOS)
Diagnosis
- Clinical symptoms (see Clinical features)
- Detailed otoscopic examination findings: most commonly pearly white masses (intact) or white-yellow debris in the middle ear
- Clinical findings during operative exploration
- Imaging measures, such as high resolution computed tomography (HRCT) and in some cases, non echo planar diffusion weighted magnetic resonance imaging (MRI)
- Pure tone and speech audiogram essential
- Histopathology additionally supports the diagnosis
Radiology description
- Radiology essential to identify landmarks and the extent of disease in the preoperative and follow up setting
- CT and MRI are complementary studies for cholesteatoma
- High resolution CT highlights abnormalities of the thin and complex bony structures, provides precise localization of the opacity and assessment of postsurgical or congenital additional temporal bone anomalies
- Sharply demarcated, nonenhancing mass in Prussak space, with retraction of the tympanic membrane and erosion of the ossicles is common
- Likelihood of cholesteatoma increases when the soft tissue opacity is nondependent
- Blunting or erosion of the scutum is a common finding (bony prominence in the lateral portion of the middle ear and superior portion of the external auditory canal)
- CT has high sensitivity but low specificity for cholesteatoma and is not capable of differentiating between granulation, fibrous tissue, fluid and cholesteatoma (Pol J Radiol 2022;87:e51)
- MRI displays spatial relationships and has the ability to differentiate soft tissues and fluid in the middle ear and mastoid; specifically, non echo planar based, diffusion weighted MRI has been shown to have a high reliability in detecting cholesteatoma, particularly recurrence (Pol J Radiol 2022;87:e51)
Radiology images
Contributed by Ashley Aiken, M.D.
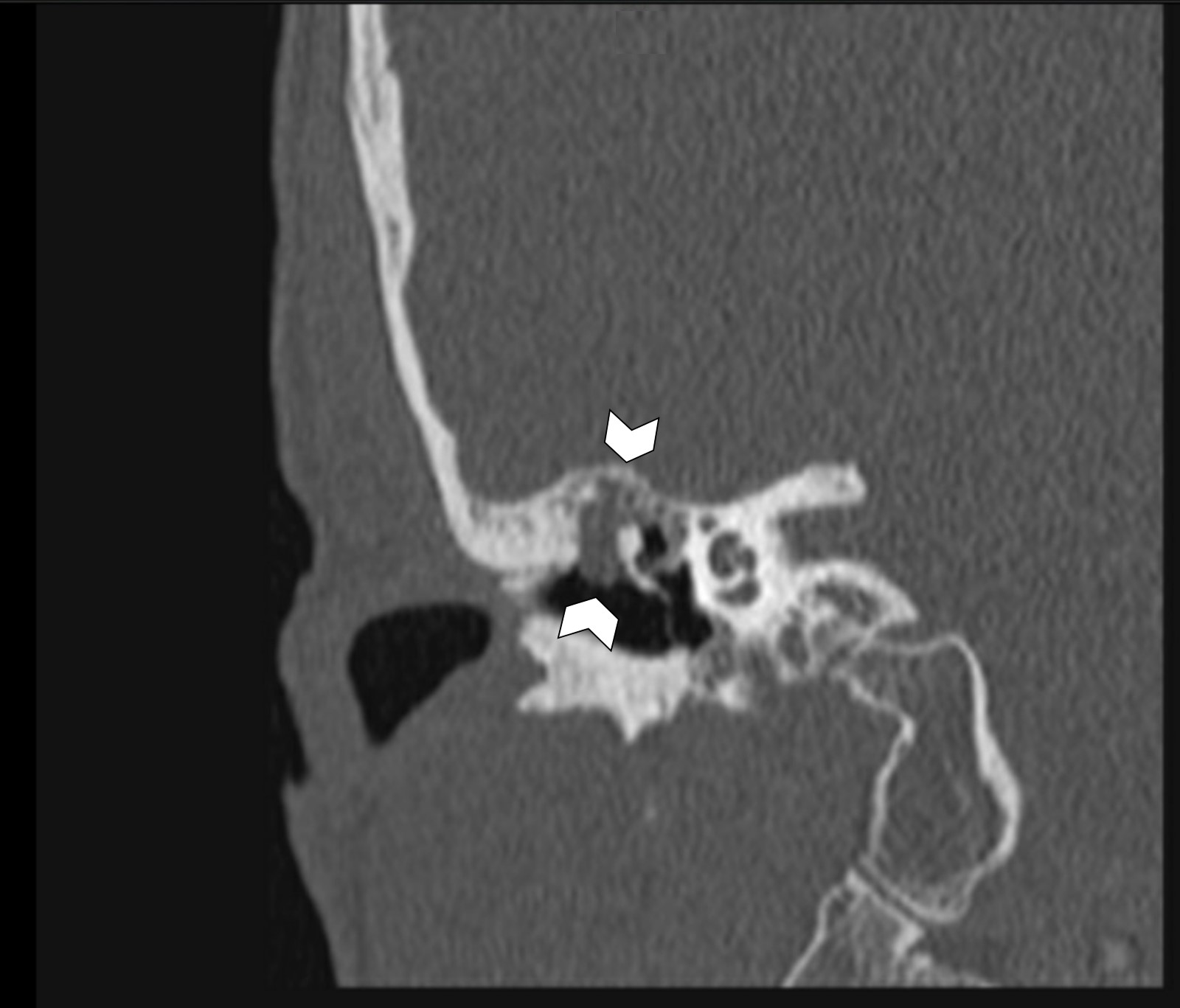
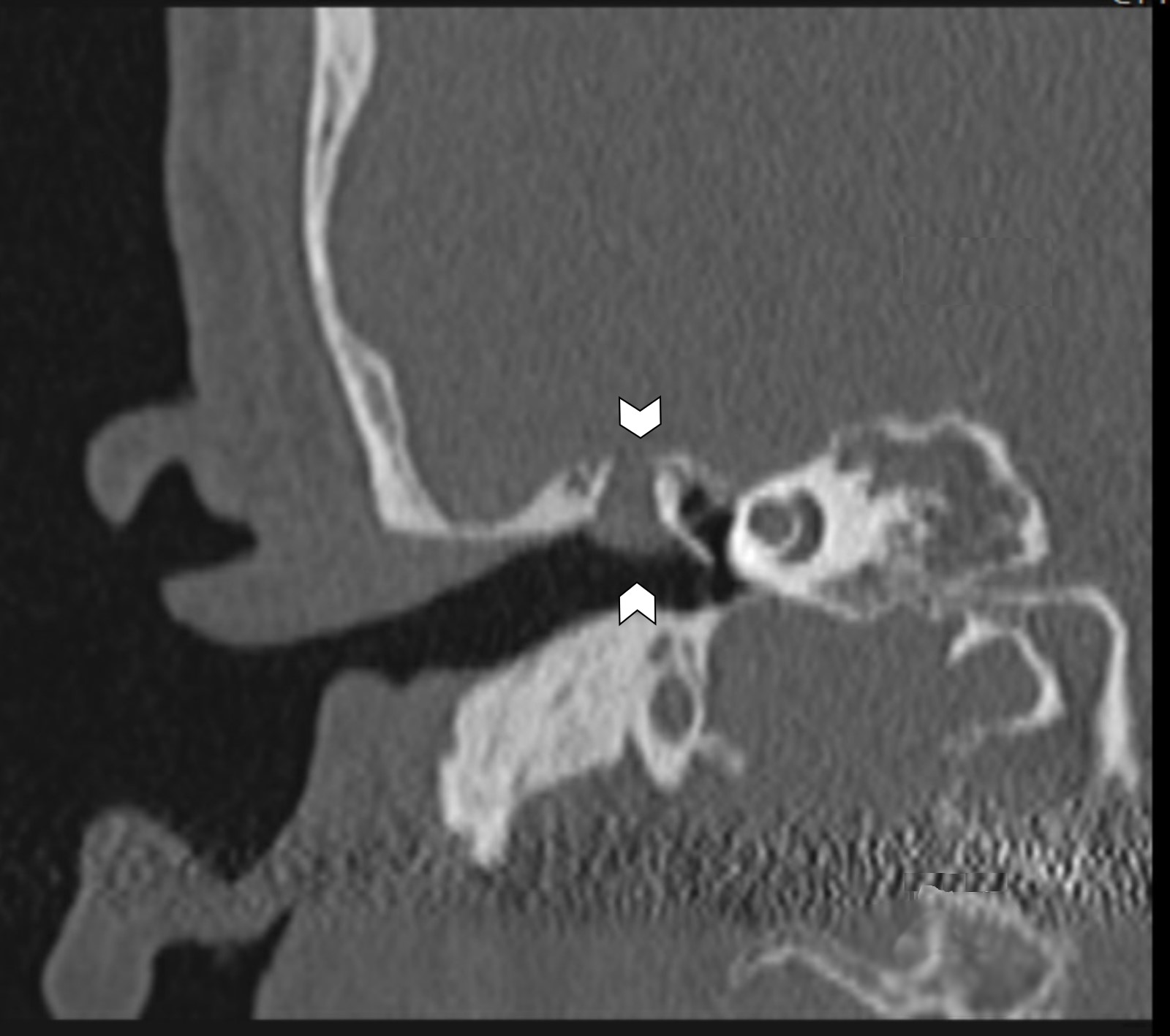
CT, coronal
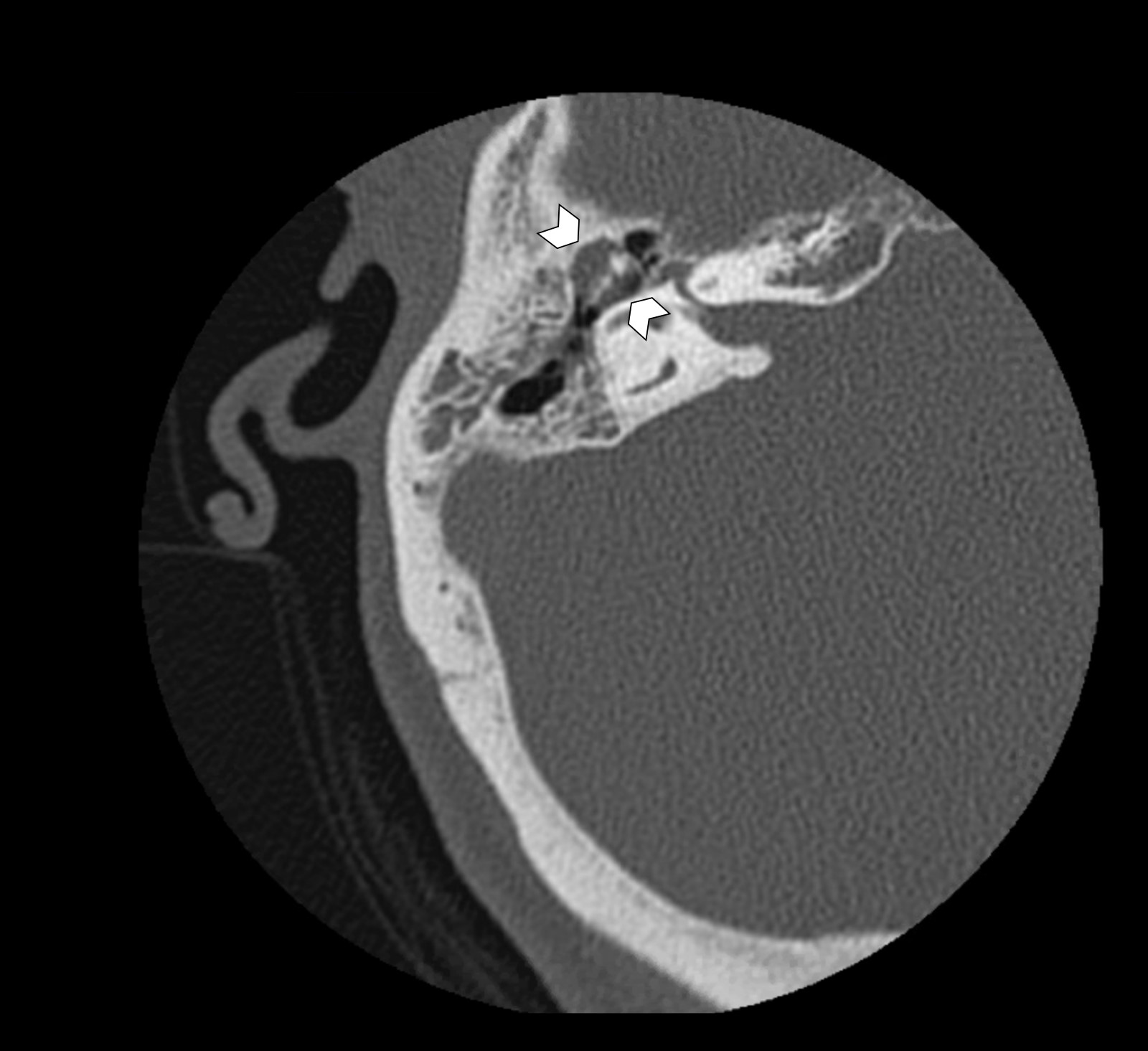
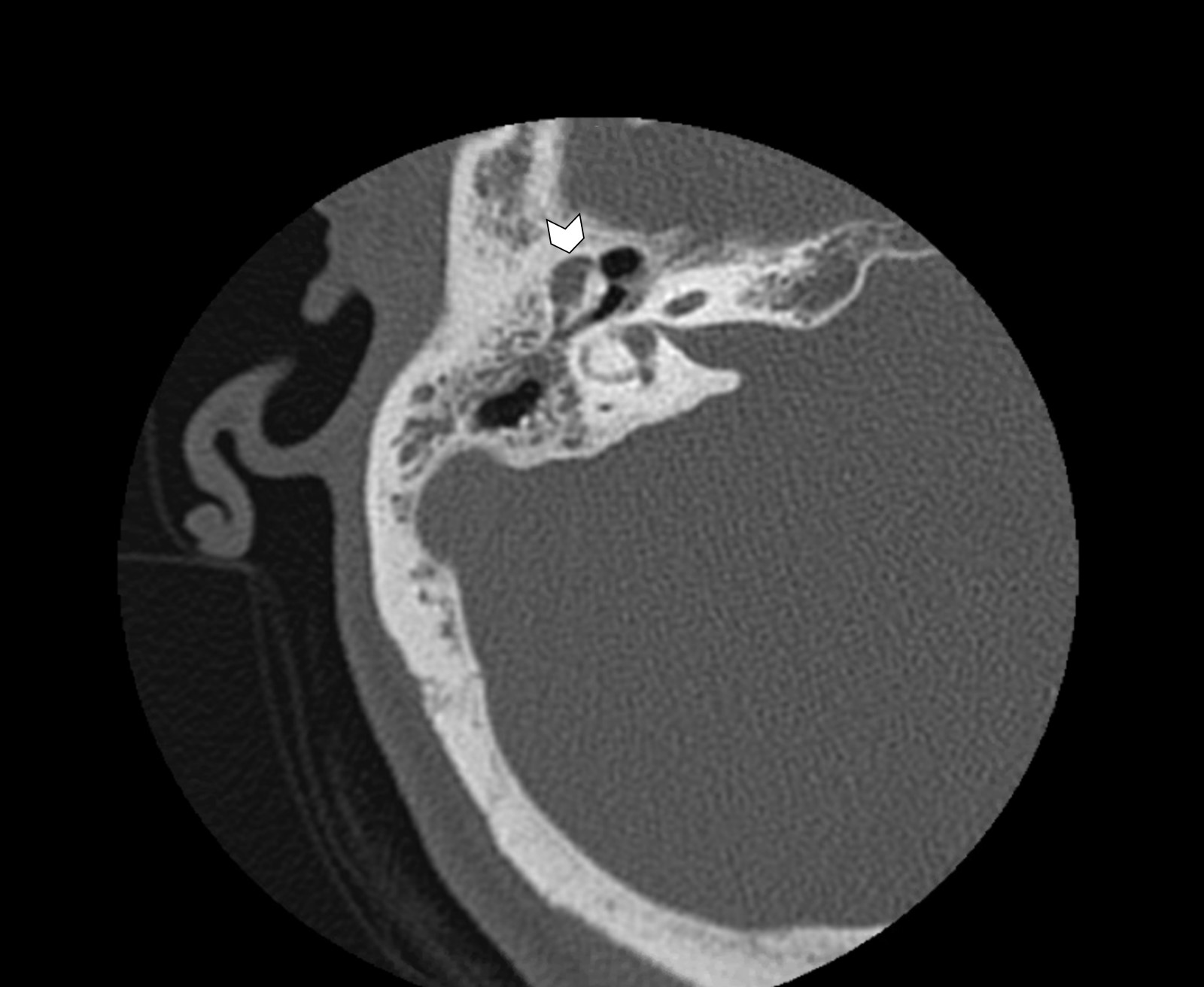
CT, axial
Prognostic factors
- Hearing loss and tinnitus are the most reported postoperative complaints
- Prognosis and potential for complications influenced by elements such as (Eur Arch Otorhinolaryngol 2022 Apr 10 [Epub ahead of print]):
- Ossicular chain status
- Ossicular chain reconstruction
- Extension of cholesteatoma
- Labyrinthine fistula (abnormal communication between the inner ear and the middle / mastoid cavity) (Front Neurol 2022;13:804915)
- Infection or abscess
- Cranial nerve dysfunction:
- Facial paralysis (Acta Otolaryngol 2022;142:30)
- Loss of taste (Otol Neurotol 2022;43:e582)
- Residual disease: cholesteatoma extension to the sinus tympani or widespread in the mastoid, as well as absence of the stapes superstructure, were predictive of residual disease (Braz J Otorhinolaryngol 2020;86:201, Otol Neurotol 2022;43:472)
- Recurrence (Int Arch Otorhinolaryngol 2020;24:e18, J Laryngol Otol 2022;136:119):
- 15 - 20% in adults
- 35 - 40% in children
- Young age and low tegmen is associated with increased risk
- Discharging ear in preoperative state
- Marked ossicular chain erosion or destruction
- Polypoid mucosal disease or extensive disease and mastoid involvement
- Chronic otorrhoea and reperforation are most common signs of late recurrences
- Squamous cell carcinoma, arising in association with cholesteatoma, remains a controversial topic and would be regarded as exceptionally rare (J Neurol Surg Rep 2022;83:e13)
Case reports
- 23 year old man with a parotid gland cholesteatoma (SAGE Open Med Case Rep 2017;5:2050313X17749083)
- 25 year old woman with progressive hearing loss and blocked sensation in left ear for 1.5 months and past history of myringoplasty (Iran J Otorhinolaryngol 2019;31:311)
- 45 year old woman with 8 months of left ear pain and swelling (J Clin Diagn Res 2017;11:ED08)
- 56 year old man with cholesteatoma originating in the sella turcica (Medicine (Baltimore) 2016;95:e2938)
- 67 year old man with temporomandibular joint symptoms as first manifestation of external auditory canal cholesteatoma (Ann Med Surg (Lond) 2022;74:103287)
- 82 year old diabetic woman with sphenoid sinus cholesteatoma (Clin Med Insights Case Rep 2019;12:1179547619835182)
Treatment
- Treatment of cholesteatoma is surgical
- Surgical objectives: total removal of disease and optimal hearing restoration
- Complete removal is essential to minimize risk of residual pathology and prevent recurrent disease (Otol Neurotol 2019;40:63)
Clinical images
Contributed by Esther Vivas, M.D.
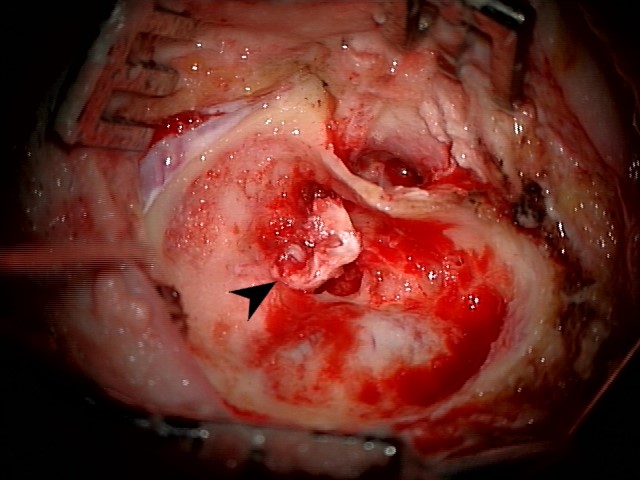
Mastoid cholesteatoma, right ear
Images hosted on other servers:

Bilateral congenital cholesteatoma

Congenital cholesteatoma

Acquired cholesteatoma
Gross description
- Cholesteatoma rarely intact after surgical removal
- Surgical specimens usually consist of multiple, irregular, gray-white to yellow fragments
- Innumerable minute, detached white flakes (keratin debris) within specimen container
- Possible minute bone fragments
- All tissue should be submitted for histologic examination to definitively confirm the diagnosis
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.

Fragments of hemorrhagic soft tissue
Frozen section description
- Abundant detached anucleate keratin, keratinizing stratified squamous epithelium and inflamed fibrous connective tissue stroma components appear similar to that identified in routine processing
Frozen section images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
Keratin, benign stratified squamous epithelium
Keratin debris
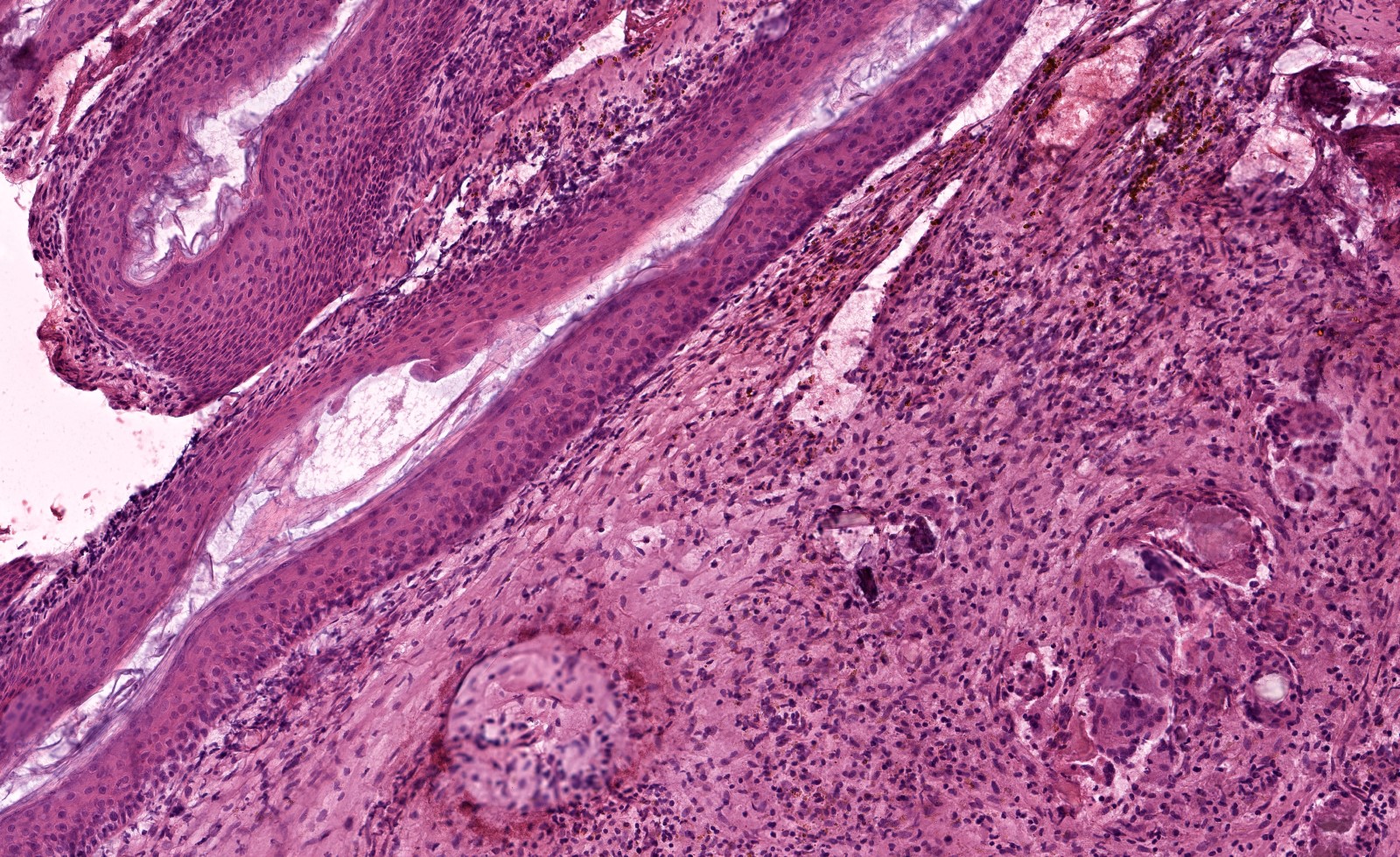
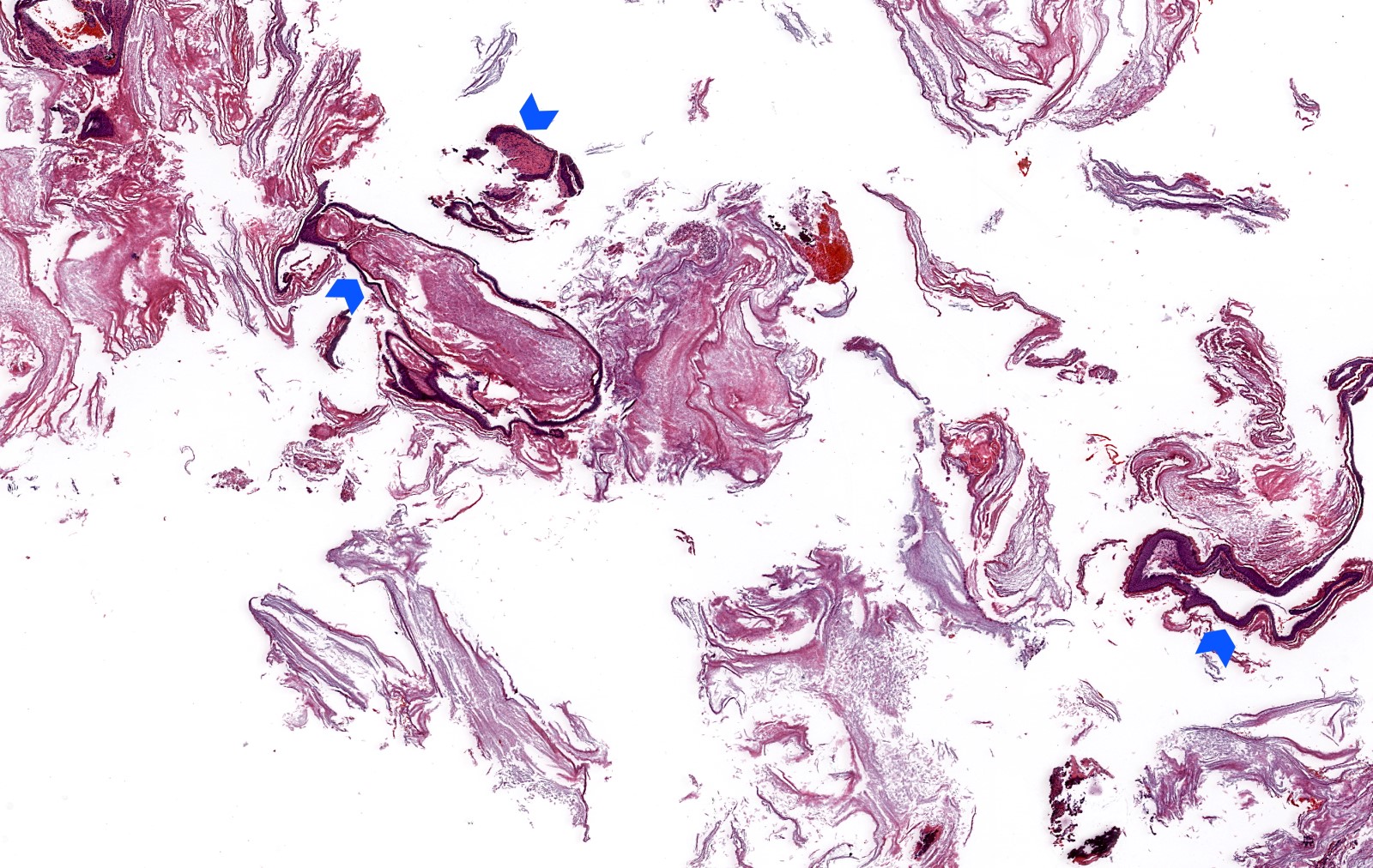
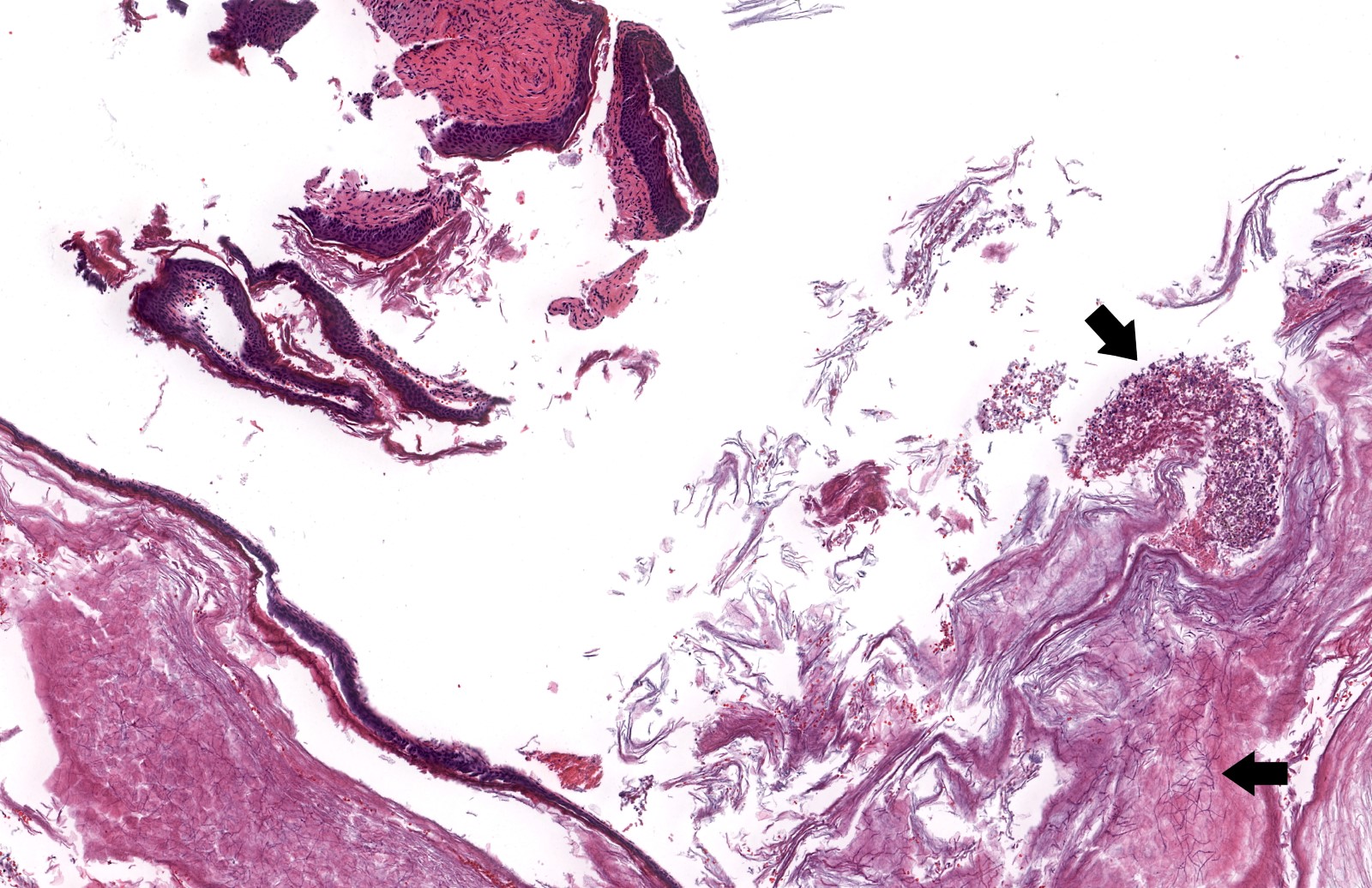
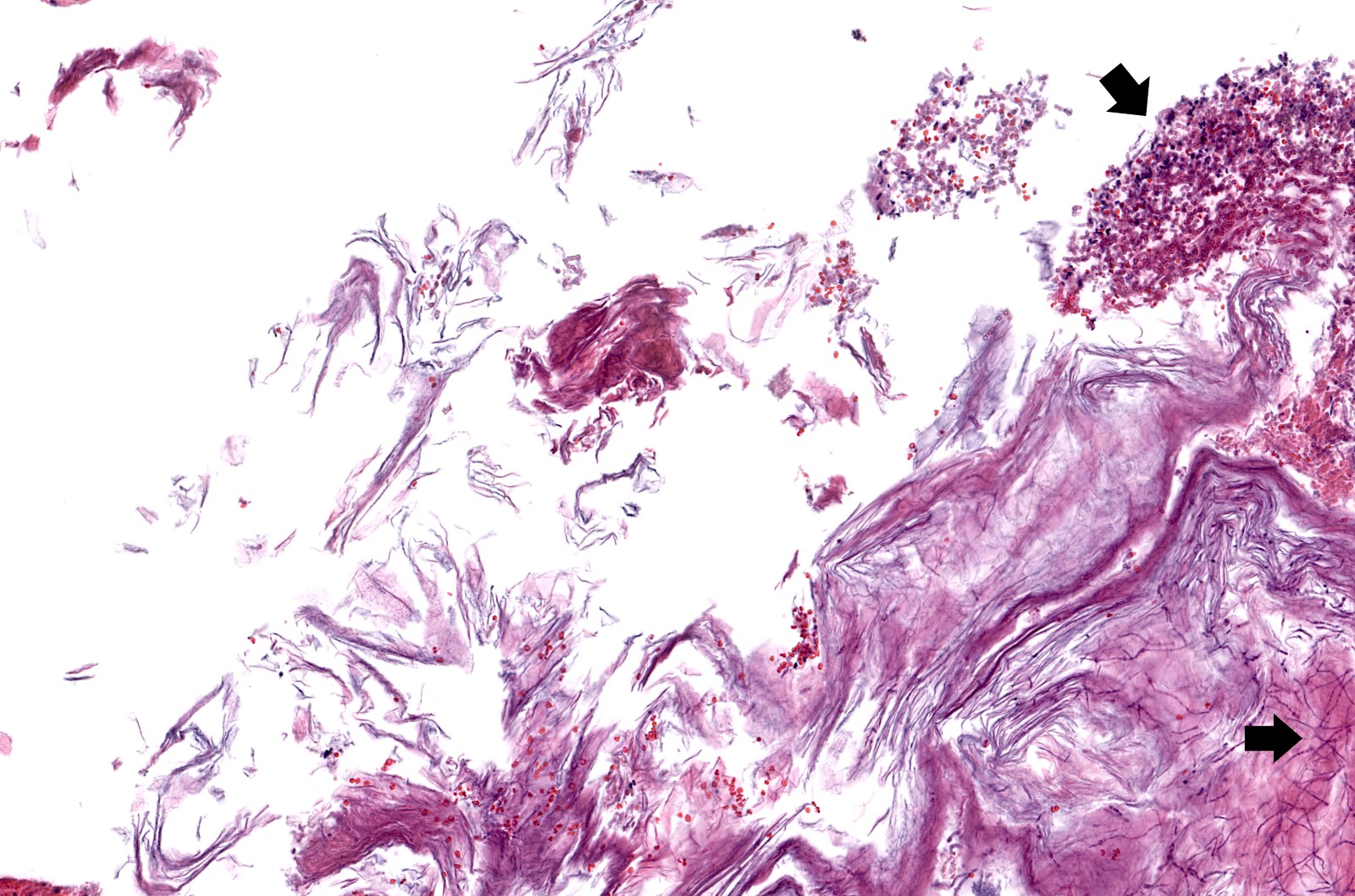
Microscopic (histologic) description
- Normal histology of the middle ear epithelium includes cuboidal or columnar glandular epithelium
- If the specimen unequivocally originates from the middle ear, then any squamous epithelium is abnormal
- Diagnosis rests on the presence of 3 key components:
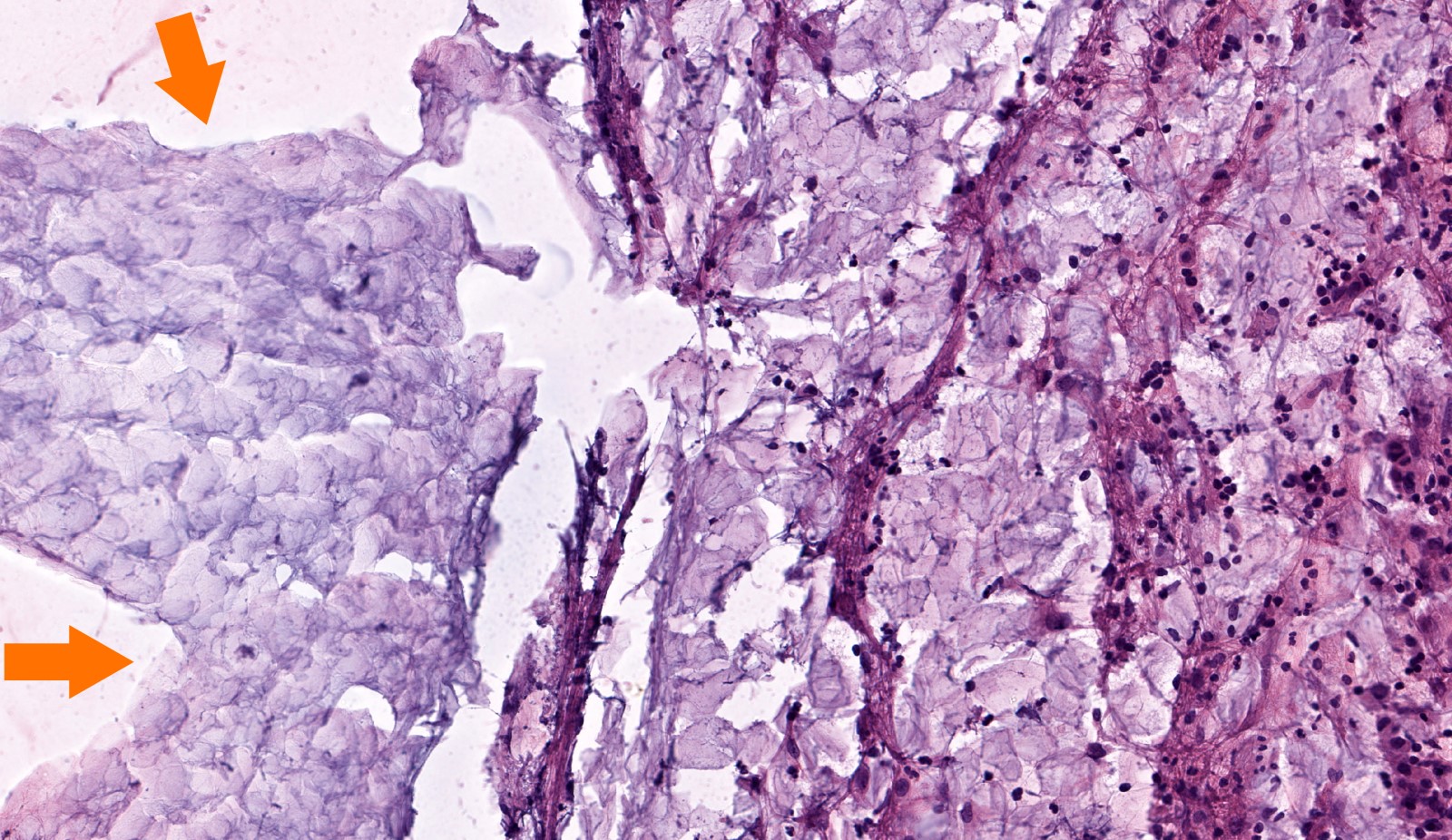
- Keratinous material (anucleate keratin squamous)
- Clinically, commonly referred to as cyst content
- Abundant detached anucleate keratin, can be laminated or disorganized aggregates
- May show bacteria or fungal overgrowth
- Note: the presence of keratin debris alone is not diagnostic of a cholesteatoma and should be interpreted with caution
- Keratinizing stratified squamous epithelium
- Also known as matrix (clinically synonymous term)
- Prominent granular layer and absent rete pegs
- Cellular maturation and lack of any significant atypia
- Inflamed fibrous connective tissue stroma
- Also known as perimatrix (clinically synonymous term)
- May be middle ear mucosa included
- Infiltrate is usually comprised of lymphocytes, plasma cells, histiocytes and mast cells
- Foreign body type giant cells to keratin debris common
- Cholesterol clefts may be seen
- Keratinous material (anucleate keratin squamous)
- Incidental findings possible:
- Cholesterol granuloma, otic polyp, tympanosclerosis, acquired encephalocele and paraganglioma
- Reference: Head Neck Pathol 2018;12:419
Microscopic (histologic) images
Contributed by Kelly Magliocca D.D.S., M.P.H.
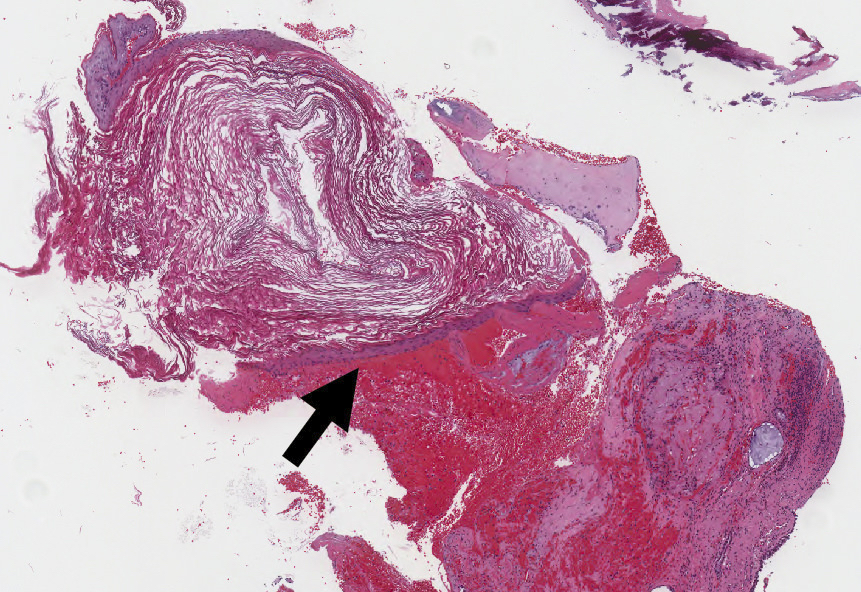
Cholesteatoma epithelium and keratin
Fungal forms within keratin debris
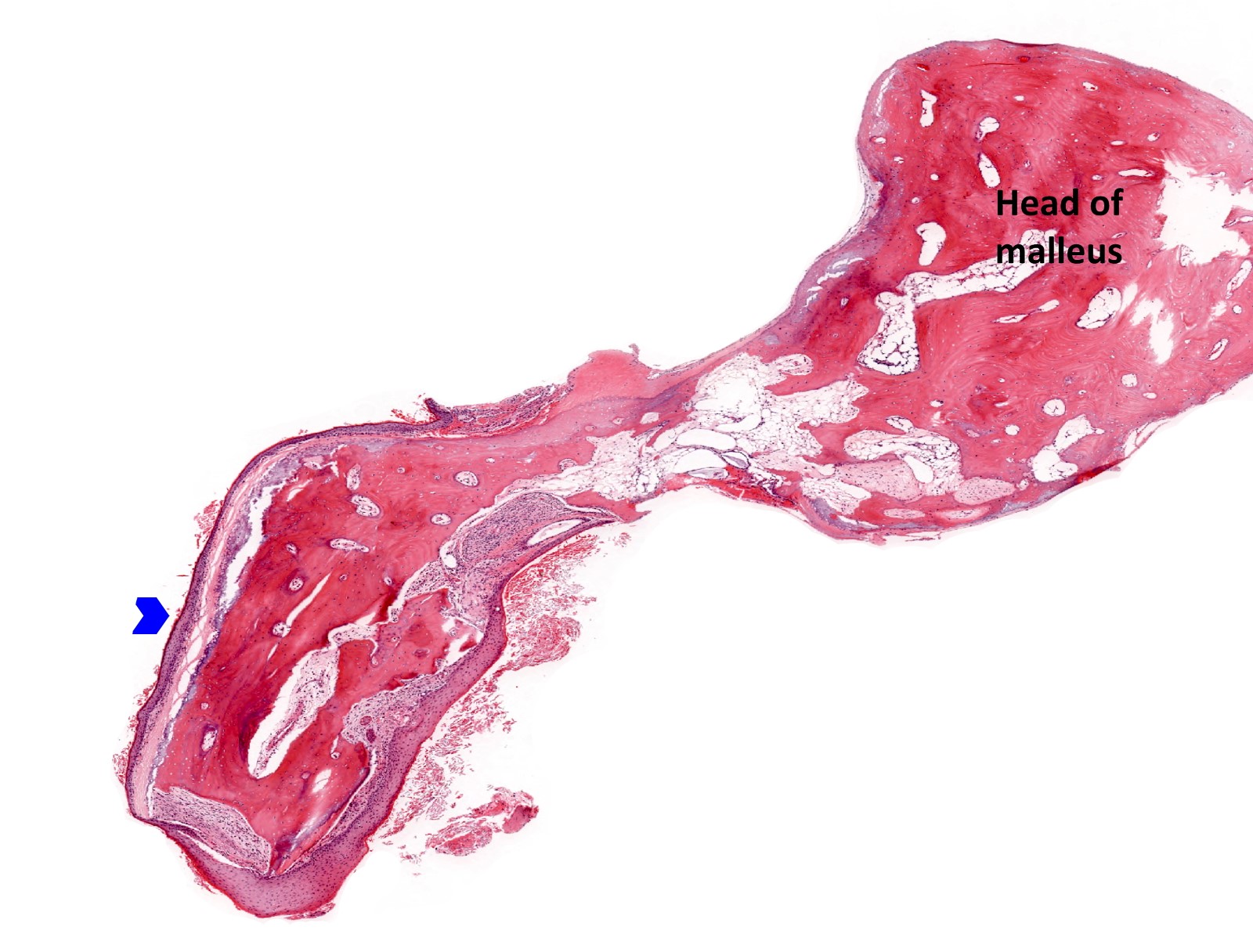
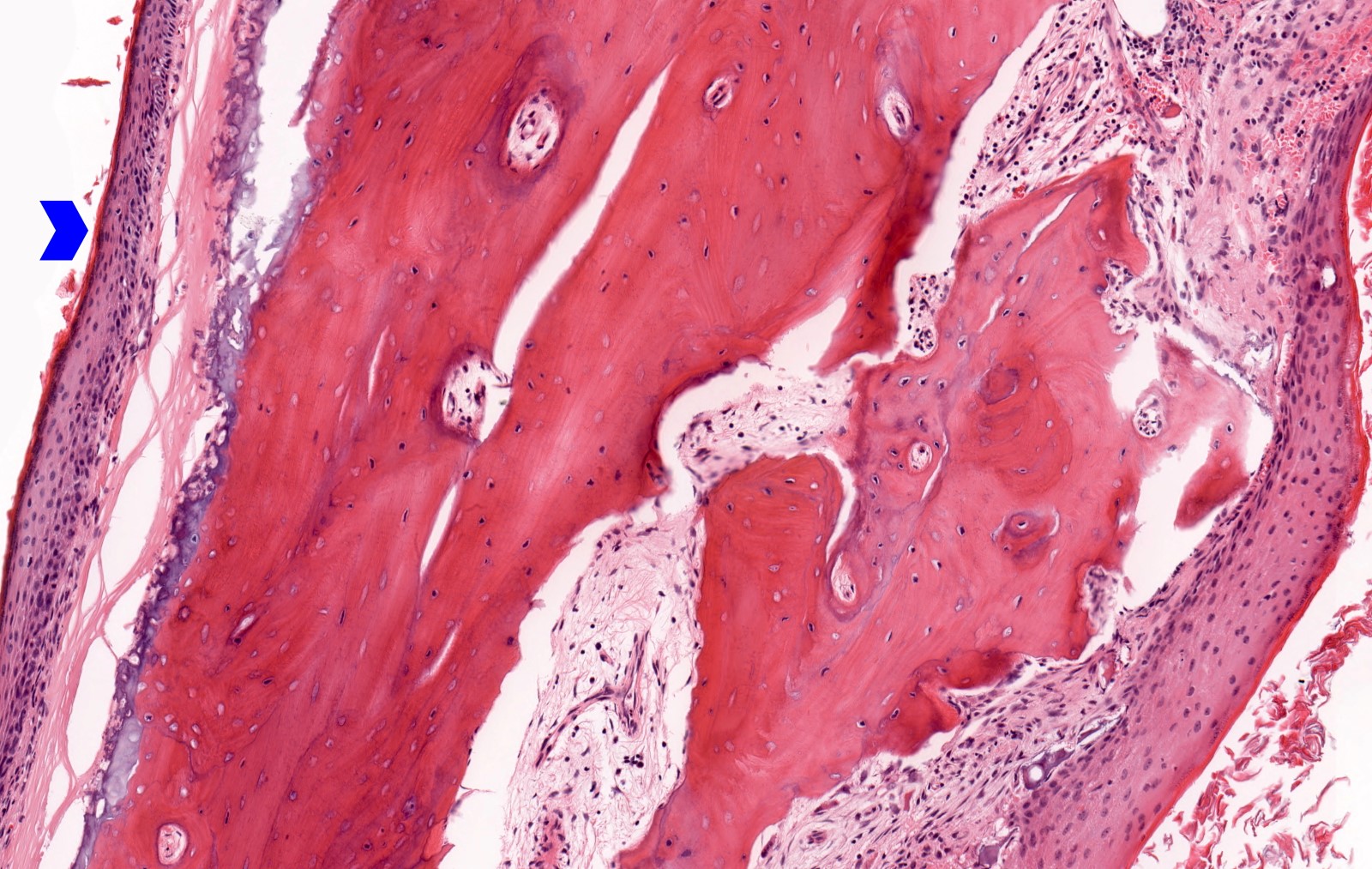
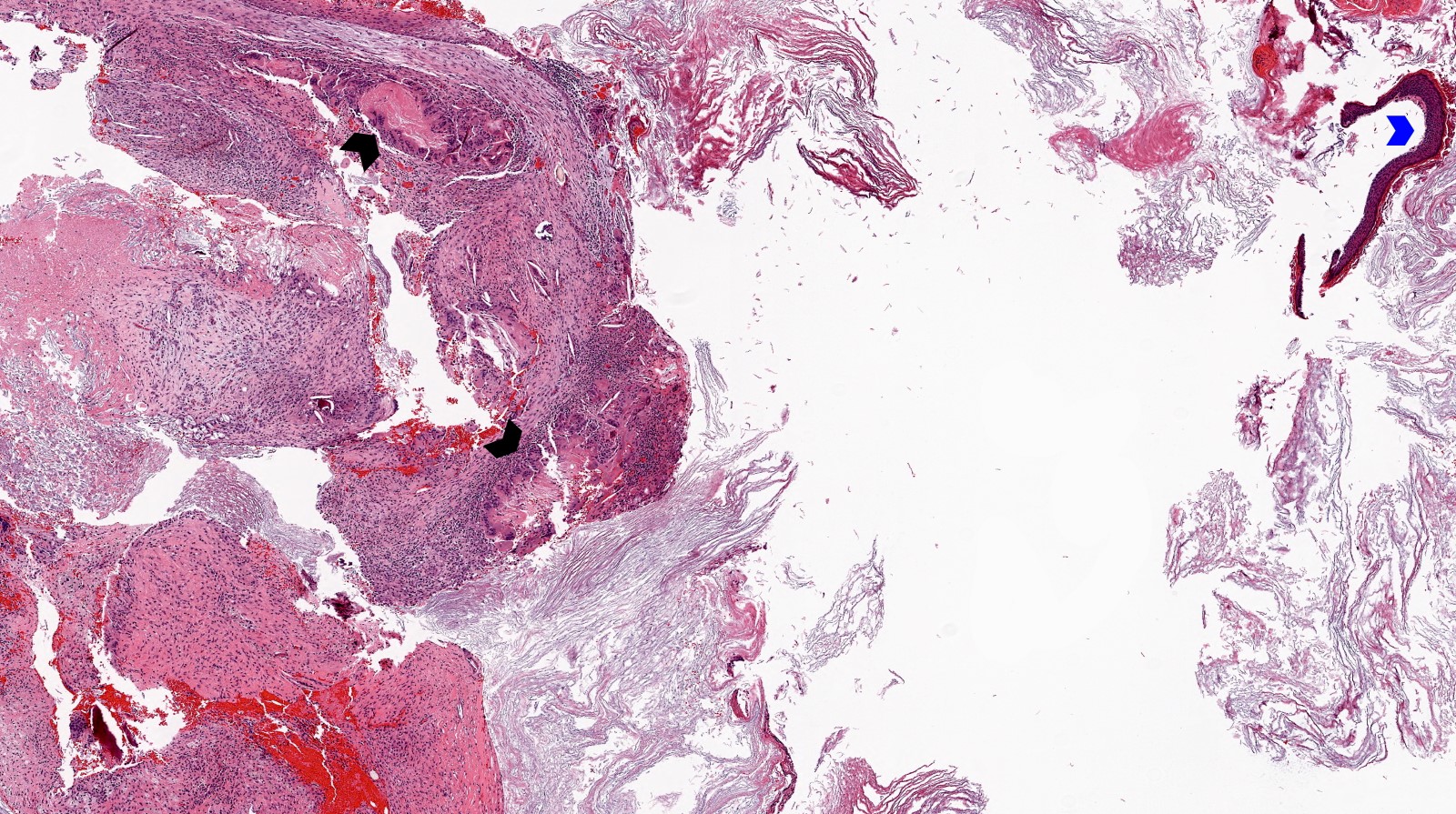
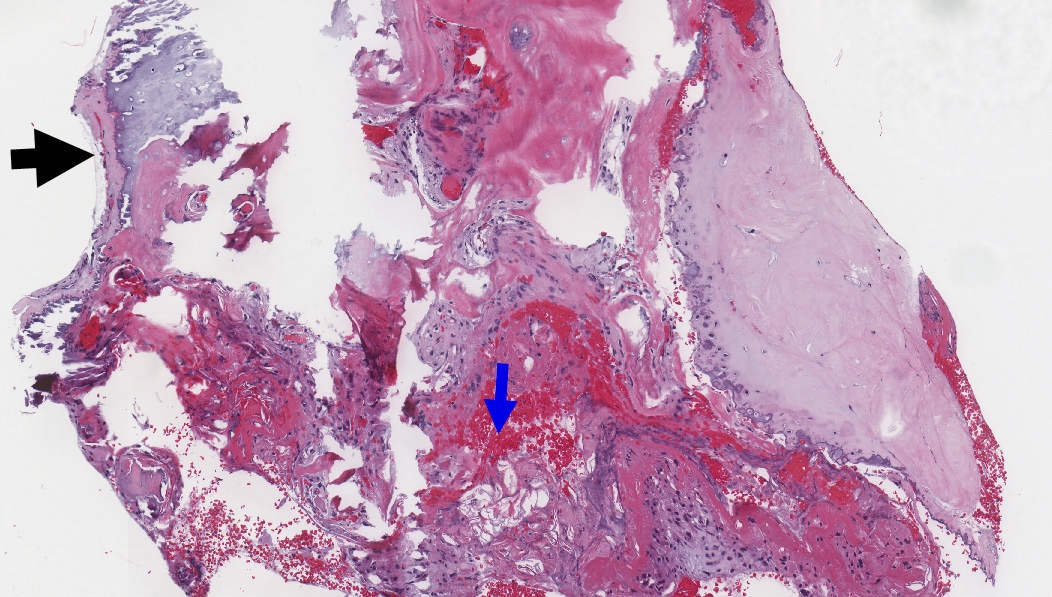
Cholesteatoma eroding malleus
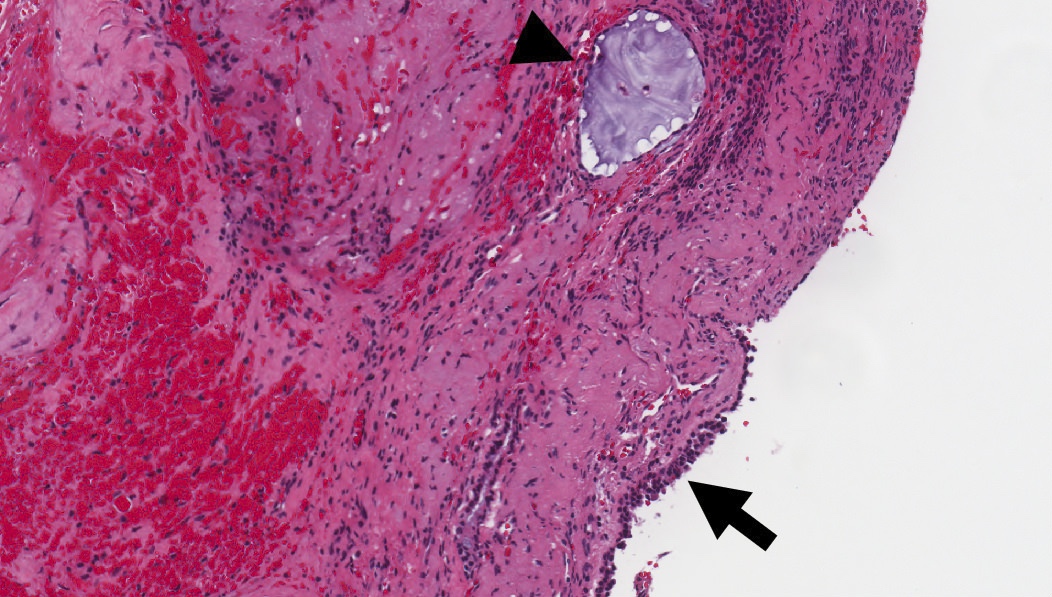
Cholesteatoma and middle ear mucosa
Cholesteatoma, inflamed
Cholesteatoma epithelium and keratin
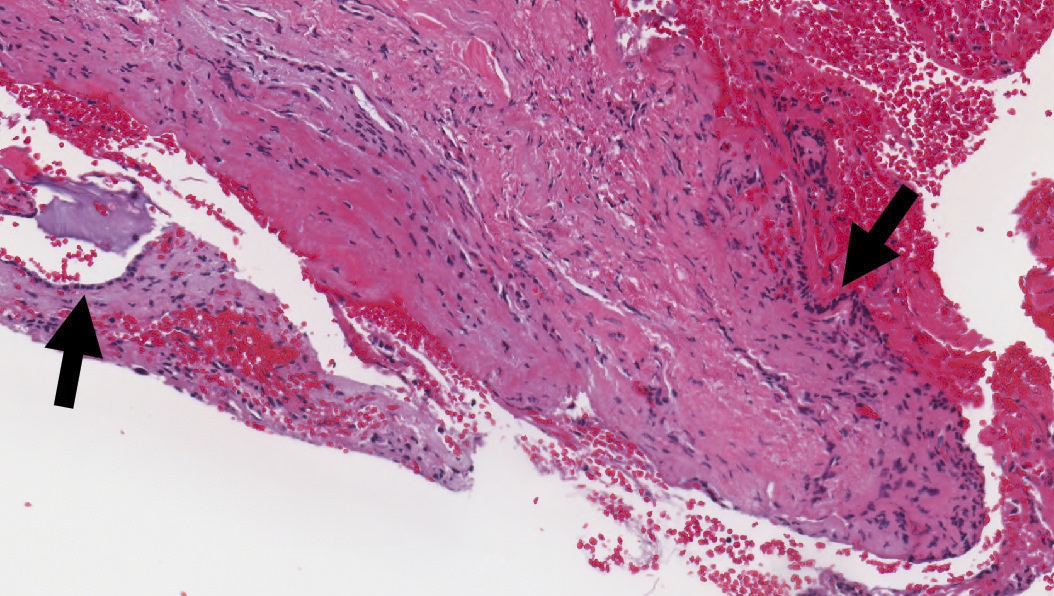
Inflamed middle ear mucosa
Residual fibrous tissue and underlying cartilage
Middle ear mucosa with hyperplasia
Cuboidal middle ear epithelium
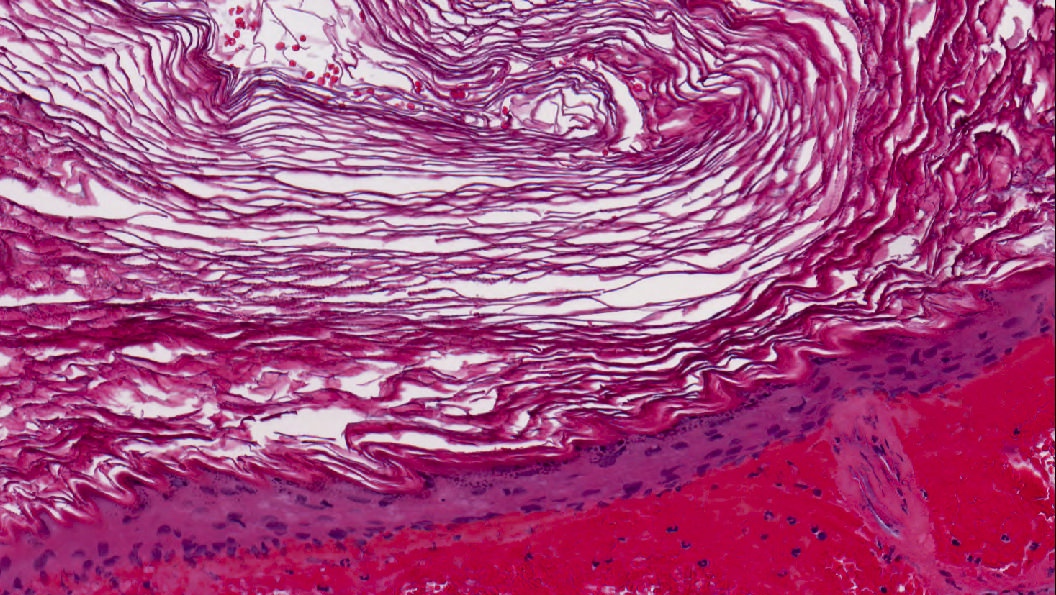
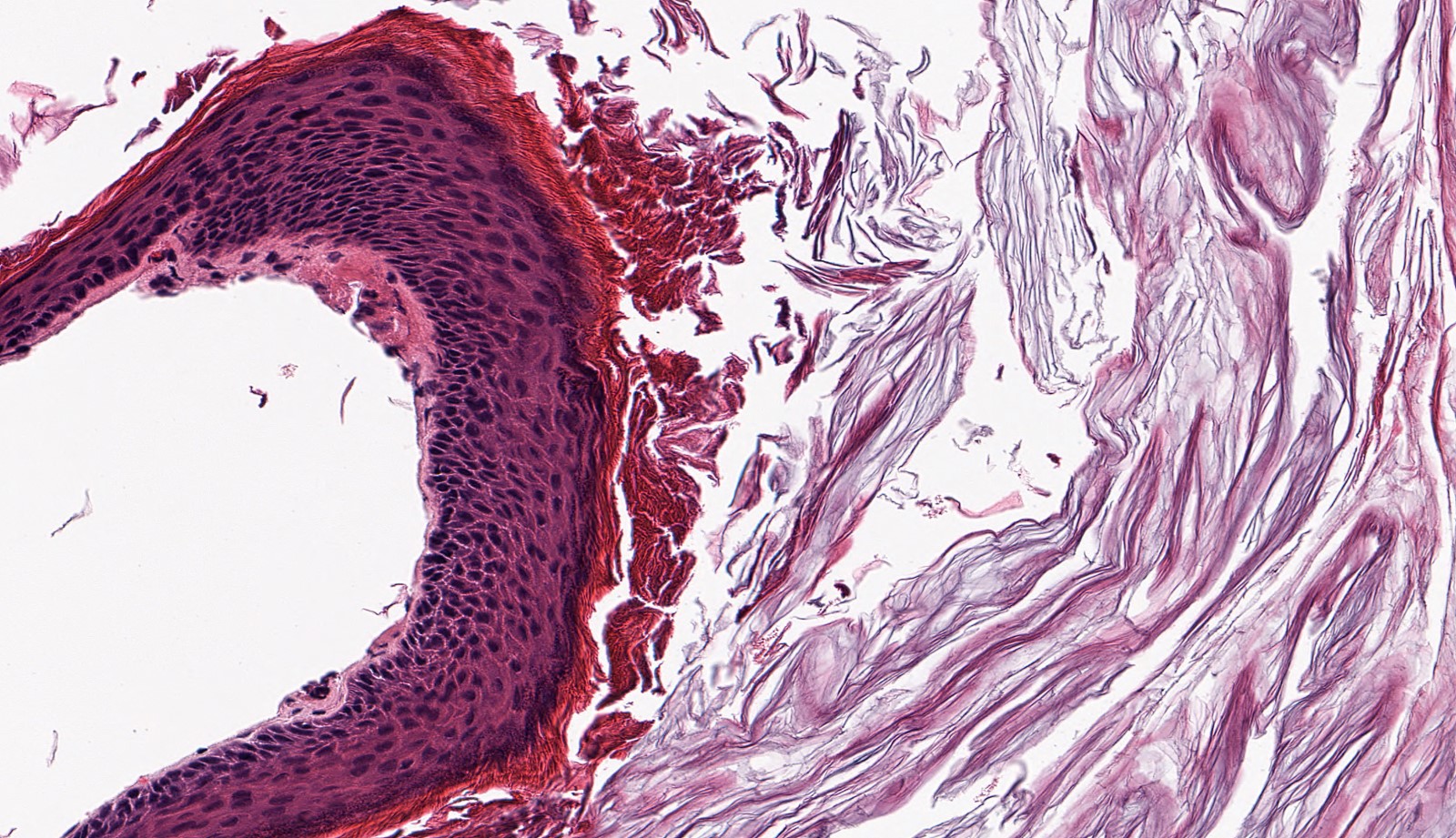
Keratinizing stratified squamous epithelium

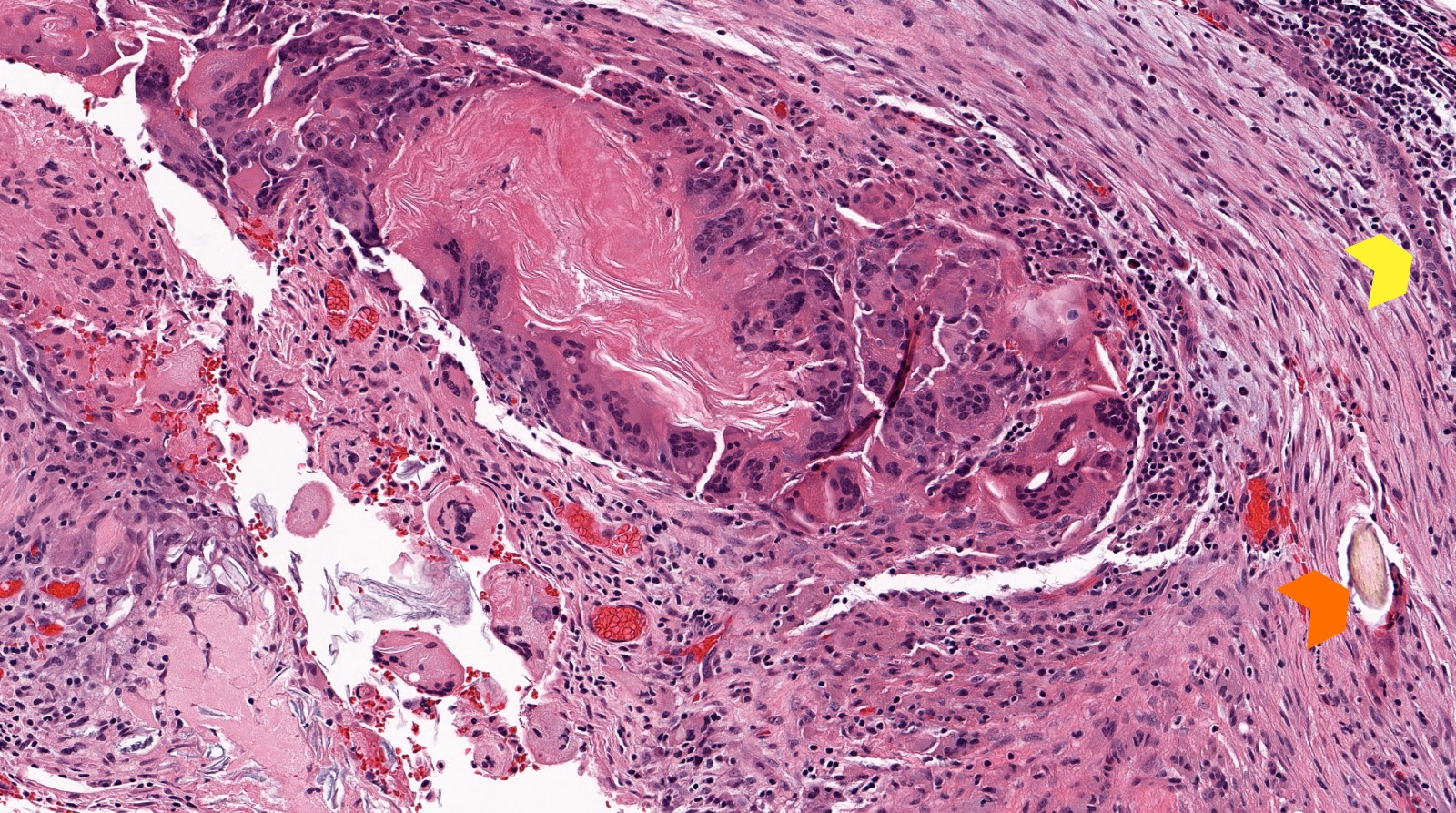
Keratin granuloma within ossicular tissue
Positive stains
- No specific immunohistochemistry required for cholesteatoma
- Squamous epithelium expected to be immunoreactive for cytokeratins, p63 and p40
- GMS fungal stain may highlight yeasts and fungal elements in keratinous debris
- References: J Assoc Res Otolaryngol 2018;19:223, Front Microbiol 2021;12:761111
Videos
Primary and secondary acquired cholesteatoma
Sample pathology report
- Left middle ear and mastoid contents:
- Cholesteatoma
- Middle ear mucosa with acute and chronic inflammation
Differential diagnosis
- Cholesterol granuloma:
- Elongated clefts (spaces) in tissue remaining after cholesterol crystals are dissolved in processing
- Clefts are associated with an adjacent or surrounding foreign body type giant cell reaction
- Rich granulation type inflammatory infiltrate, including hemosiderin laden macrophages
- Otic (aural) polyp:
- Polypoid chronic inflammation and granulation tissue only
- Lacking keratinizing squamous epithelial proliferation
- Lacking anucleate squames
- Chronic otitis media:
- Lacks the proliferative squamous epithelium or the anucleate squames
- Keratosis obturans:
- Accumulation of keratin debris within the medial aspect of the external auditory canal
- May show bony erosion
- More commonly bilateral
- Tympanic membrane intact
- Microscopically some cases may be identical to cholesteatoma, though if middle ear is preserved, no middle ear mucosa will be seen microscopically
- Squamous cell carcinoma:
- Lack of epithelial cell maturation or polarity, atypical mitosis, pleomorphism, dyskeratosis or individual cell keratinization
Additional references
Board review style question #1
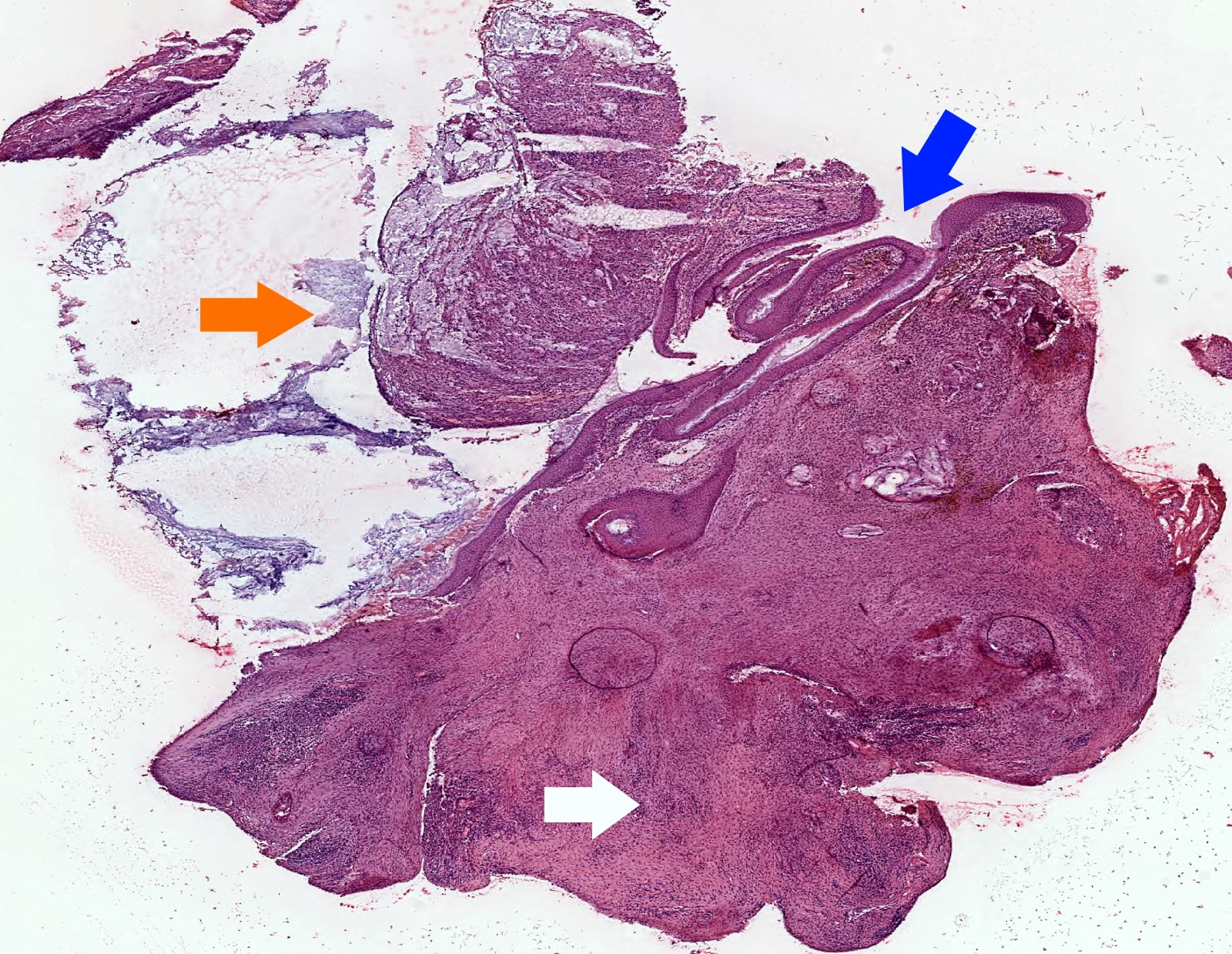
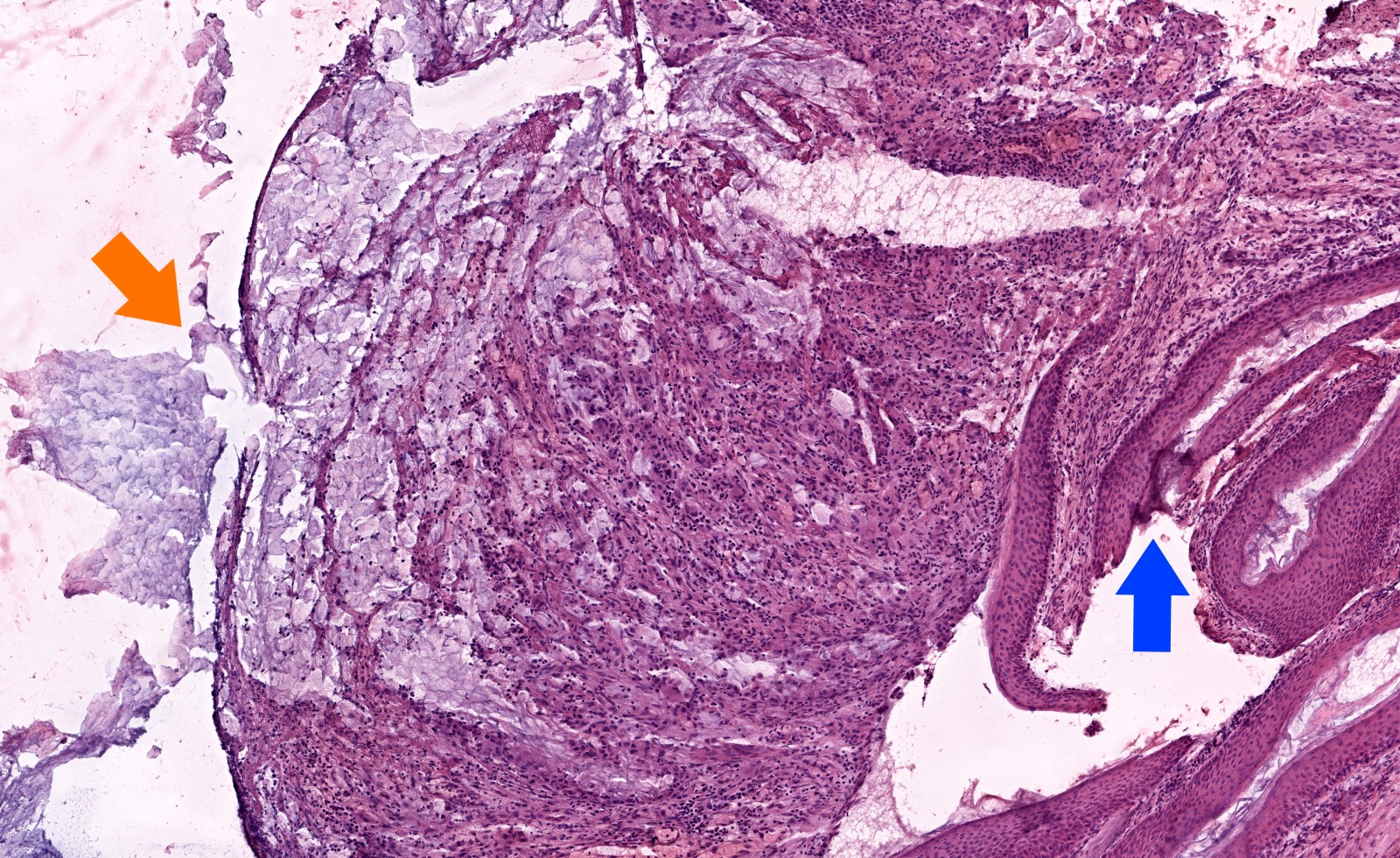
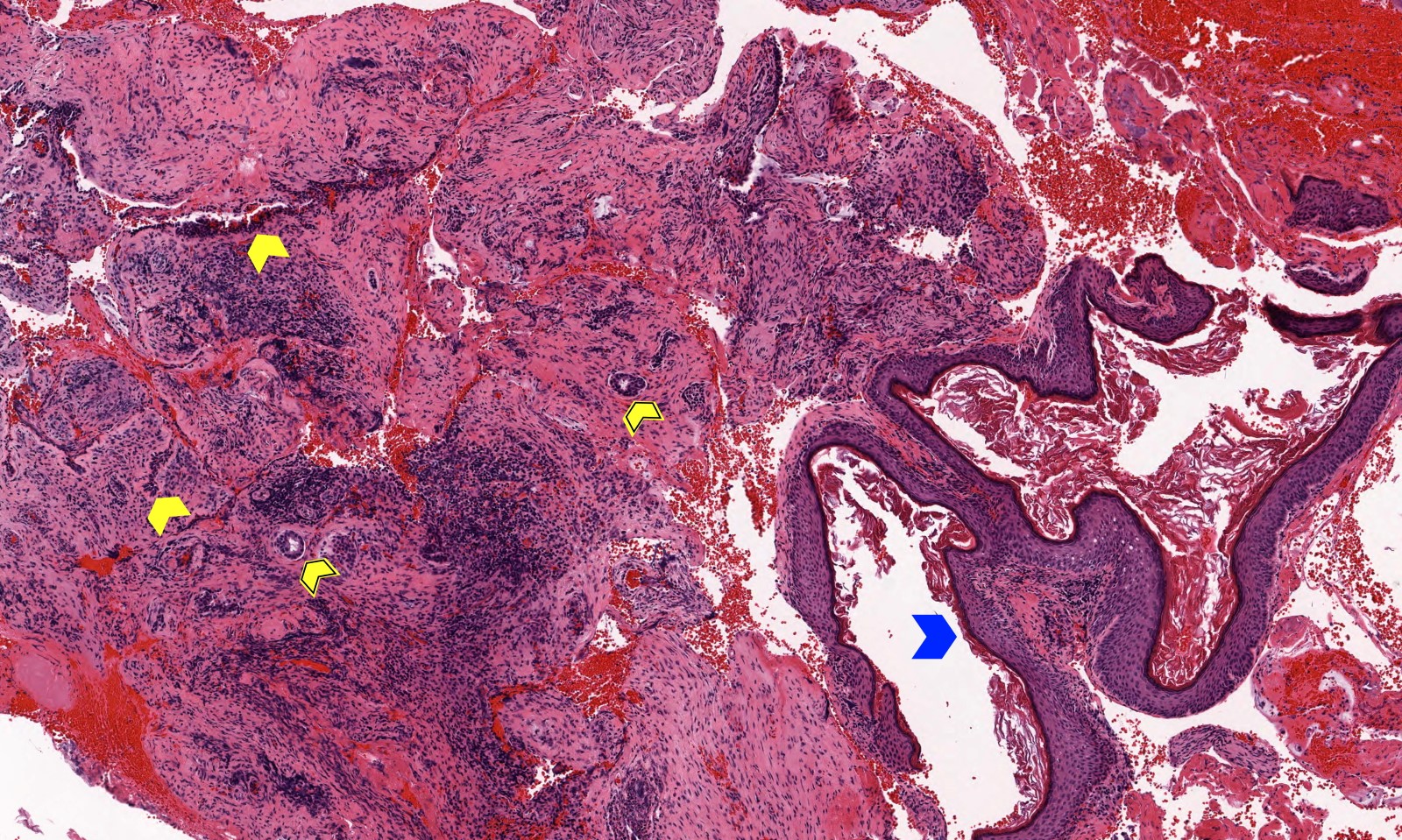
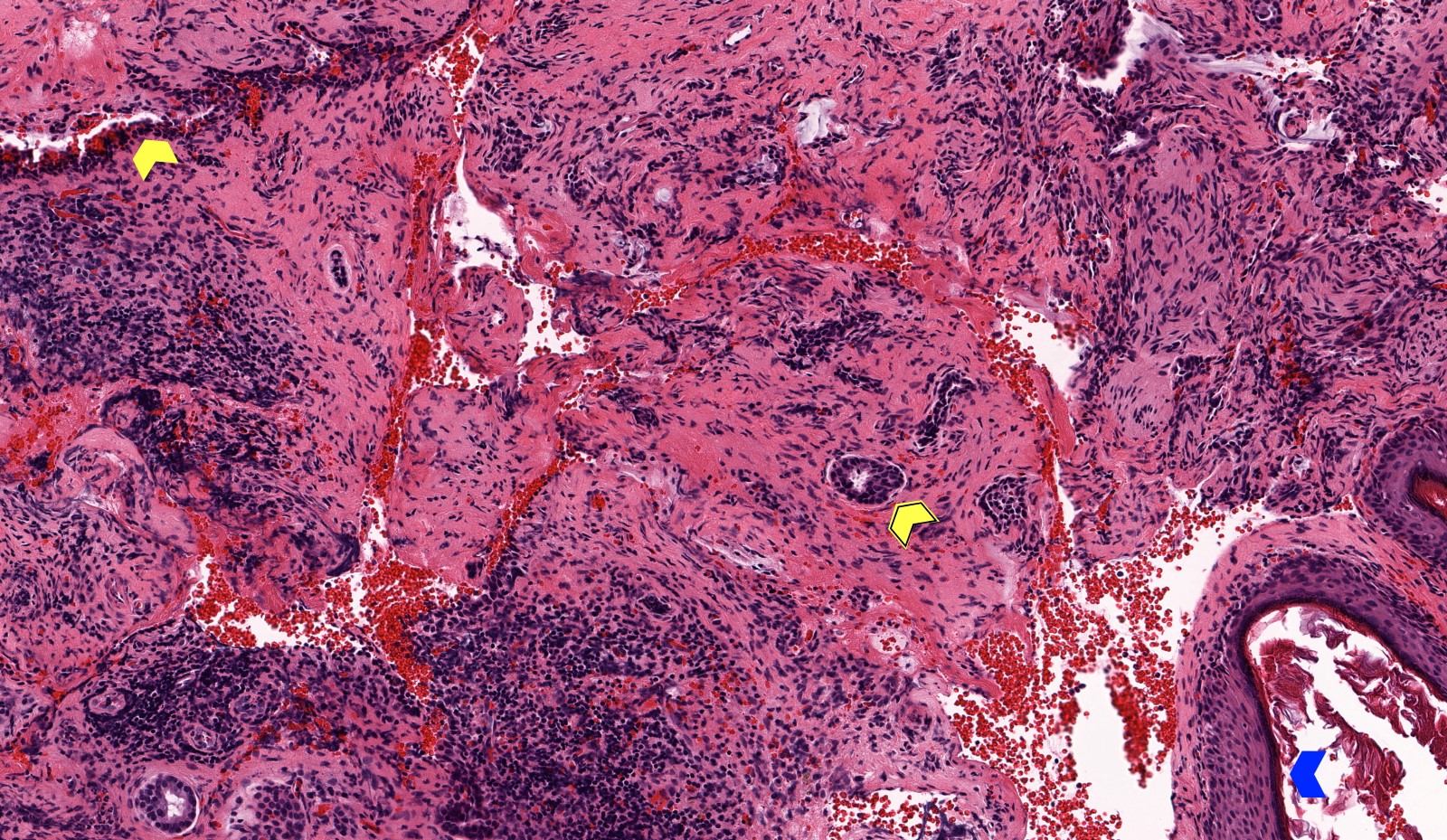
The keratinizing squamous epithelium (blue arrow in image shown above) of cholesteatoma is also known as
- Cholesterol clefts
- Cystic contents
- Matrix
- Perimatrix
Board review style answer #1
C. Matrix. Matrix, perimatrix and cystic contents are terms that are more commonly used clinically and refer to the keratinizing squamous epithelium, connective tissue wall and keratin debris, respectively.
Comment Here
Reference: Cholesteatoma
Comment Here
Reference: Cholesteatoma
Board review style question #2
How does congenital cholesteatoma typically present?
- White-yellow mass in anterior superior quadrant of the middle ear, disrupted tympanic membrane, slowly progressive sensorineural hearing loss
- White-yellow mass in anterior superior quadrant of the middle ear, intact tympanic membrane, slowly progressive conductive hearing loss
- White-yellow mass in posterior superior retraction pocket, disrupted tympanic membrane, slowly progressive sensorineural hearing loss
- White-yellow mass in posterior superior retraction pocket, intact tympanic membrane, slowly progressive conductive hearing loss
Board review style answer #2
B. White-yellow mass in anterior superior quadrant of the middle ear, intact tympanic membrane, slowly progressive conductive hearing loss. Congenital cholesteatoma usually arises in the middle ear, most commonly in the absence of otorrhea, related to an intact tympanic membrane. Most patients are asymptomatic, although this, in addition to other symptoms, depends on the extent of disease. Over time, patients will develop conductive hearing loss related to cholesteatoma formation.
Comment Here
Reference: Cholesteatoma
Comment Here
Reference: Cholesteatoma
