
Cytopathology
Cerebrospinal fluid
Overview


Copyright: 2023-2025, PathologyOutlines.com, Inc.
PubMed Search: Cerebrospinal fluid cytopathology
Cerebrospinal fluid
Overview
Authors: Thomas J. Laux, D.O., Maria Luisa C. Policarpio-Nicolas, M.D., Maria Cecilia D. Reyes, M.D.
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Chunyu Cai, M.D., Ph.D.
Last author update: 4 March 2025
Last staff update: 4 March 2025
Copyright: 2023-2025, PathologyOutlines.com, Inc.
PubMed Search: Cerebrospinal fluid cytopathology

Table of Contents
Definition / general | Essential features | CPT coding | Sites | Laboratory | Radiology description | Radiology images | Case reports | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Laux TJ, Policarpio-Nicolas MLC, Reyes MCD. Overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cytopathologycerebrospinalfluid.html. Accessed April 1st, 2025.
Definition / general
- Cerebrospinal fluid (CSF) cytology is the examination of CSF and its cells to assess for pathology
- Purpose of CSF cytology is to identify primary central nervous system (CNS) malignancies, to stage hematologic neoplasms, to exclude metastatic tumors and to evaluate for CNS infections
Essential features
- Normal CSF in adults contains < 5 cells/mm3 (5,000 cells/mL)
- Newborns will have more cells
- Can be reported as negative, atypical, suspicious for malignancy or positive for malignancy
- > 90% are negative for malignancy
- Approximate overall sensitivity of 60% and specificity of 97 - 98%
CPT coding
Sites
- Lumbar puncture (LP), typically L3 - L4 or L4 - L5 (Ulster Med J 2014;83:93)
- Shunt fluid (CSF drawn from cerebral shunt device) (Neurol India 2021;69:S471)
- Directly aspirated from a lateral ventricle through an Ommaya reservoir (an implanted subcutaneous silicone pouch) in patients undergoing chemotherapy (StatPearls: Ommaya Reservoir [Accessed 3 January 2025])
- Rarely, it may be taken from the cisterna magna at the base of the brain (StatPearls: Mega Cisterna Magna [Accessed 3 January 2025])
Laboratory
- At least 1 cc should be collected but as much as 10 cc can be collected and 3 cc is optimum (Handb Clin Neurol 2017;145:563)
- 3 - 4 tubes of CSF are usually drawn for laboratory studies, with tube number 3 typically used for cytology (McPherson: Henry's Clinical Diagnosis and Management by Laboratory Methods, 24th Edition, 2021)
- Should be collected fresh and processed within 48 hours
- Cytospin and thin layer preparations are done
- Ancillary testing (Am Fam Physician 2021;103:422, Am Fam Physician 2003;68:1103, JAMA 2006;296:2012)
- Gram stain and culture
- Cell count: white blood cell (WBC), red blood cell (RBC) and total
- Protein
- Glucose
- Electrolytes
- pH
- pO2 and pCO2
- Angiotensin converting enzyme
- Oligoclonal bands
- Tumor markers
- Flow cytometry
- Immunohistochemistry
- Molecular / polymerase chain reaction (PCR)
Radiology description
- Mollaret meningitis: imaging is limited and nonspecific, similar to other causes of viral meningitis (e.g., herpes simplex type 2) (Radiopaedia: Viral Meningitis [Accessed 3 January 2025])
- Computed tomography (CT): not directly visible
- Magnetic resonance imaging (MRI) (fluid attenuated inversion recovery [FLAIR]): leptomeningeal enhancement with high signal in the sulcal CSF
- Pyogenic meningitis (Radiopaedia: Pyogenic Meningitis [Accessed 3 January 2025])
- CT: sulcal effacement and slight hyperattenuation on unenhanced CT, false positives common
- MRI: increased FLAIR signal relative to normal cortex (nonspecific)
- Postcontrast MRI: thin and linear leptomeningeal enhancement (~50% of patients)
- Primary brain lesions
- Glioblastoma (Radiopaedia: Glioblastoma, IDH Wildtype [Accessed 3 January 2025])
- CT: thick enhancing margins, iso to hyperattenuating with irregular hypodense center representing necrosis
- MRI: iso to hypointense mass in white matter with central heterogeneous signal representing necrosis or hemorrhage
- Medulloblastoma (Radiopaedia: Medulloblastoma [Accessed 3 January 2025])
- Localized to the cerebellum (94%) and protrudes into the fourth ventricle
- CT: hyperdense mass arising from the vermis, effacing the fourth ventricle / basal cisterns, causing an obstructive hydrocephalus
- MRI: hypointense to gray matter on T1; heterogeneous and iso to hyperintense on T2
- Glioblastoma (Radiopaedia: Glioblastoma, IDH Wildtype [Accessed 3 January 2025])
- Brain metastasis (Radiopaedia: Brain Metastases [Accessed 3 January 2025])
- Localization: cerebral hemisphere (80%), cerebellum (15%) and basal ganglia (3%)
- Features
- Hemorrhage: melanoma, renal cell carcinoma, choriocarcinoma, thyroid cancer, lung and breast cancer
- Vasogenic edema
- CT
- Precontrast: isodense, hypodense or hyperdense compared to normal brain parenchyma
- Contrast: variable enhancement that is intense, punctate, nodular or ring enhancing
- MRI
- T1: iso to hypointense
- T2 / FLAIR: hyperintense
- Diffusion weighted imaging (DWI) / apparent diffusion coefficient (ADC): edema appears dark and out of proportion with tumor size
- Metastatic melanoma
- MRI (Radiopaedia: Metastatic Melanoma [Accessed 24 February 2025])
- Frequently involving the cortex
- Less frequently involves the gray-white matter junction, the dura and the leptomeninges
- Hyperintense T1 and reduced T2 signal
- Gd: peripheral rim enhancement with a heterogeneous pattern of enhancement
- MRI (Radiopaedia: Metastatic Melanoma [Accessed 24 February 2025])
- Primary diffuse large B cell lymphoma (DLBCL) of the CNS
- Noncontrast CT (AJNR Am J Neuroradiol 2023;44:358)
- Single to multiple, solid and homogenous hyperattenuating supratentorial lesion(s) that range from well defined expansive to ill defined infiltrative patterns with associated leptomeningeal or subependymal extension and crosses the corpus callosum
- Typical perivascular histologic pattern correlates with a perivascular enhancement on imaging
- Noncontrast CT (AJNR Am J Neuroradiol 2023;44:358)
- Secondary CNS lymphoma
- Leptomeninges
- MRI with contrast
- Leptomeningeal, subependymal, dural or cranial nerve enhancement
- Superficial cerebral lesion
- Communicating hydrocephalus
- MRI with contrast
- Parenchymal metastasis (AJNR Am J Neuroradiol 2011;32:984, AJNR Am J Neuroradiol 2023;44:358)
- Single to multiple enhancing lesions with a periventricular or superficial location may be accompanied by leptomeningeal metastases
- Difficult to distinguish from primary CNS lymphoma
- Leptomeninges
Radiology images
Images hosted on other servers:

Mollaret meningitis: axial and coronal normal findings
Case reports
- Mollaret meningitis
- 9 year old girl with 3 day history of fever, headache and vomiting (Neurol India 2020;68:1229)
- 50 year old woman with headache, fever, neck stiffness, nausea and vomiting (Neurol India 2020;68:1229)
- 83 year old man with an isolated episode of aseptic meningitis 3 years prior, presented with a 2 day history of fever, generalized weakness and worsening essential tremor of the right hand (Cureus 2021;13:e15264)
- Diffuse leptomeningeal glioneuronal tumor
- 19 year old man with a 6 month history of severe headaches and bilateral papilledema (Cytojournal 2005;2:16)
- 19 year old man presented with a 10 day history of worsening morning headaches, nausea and vomiting (Cytopathology 2022;33:738)
- Intracranial embryonal carcinoma
- 19 year old man with drowsiness and a right temporal headache (Int J Clin Exp Pathol 2020;13:1216)
- Pediatric ependymoma
- 19 month old girl presented unresponsive and intubated (Acta Biomed 2021;92:e2021107)
- Encephalomyelitis
- 4 year old boy with slurring of speech, difficulty in swallowing and fever for 2 days (TJ Family Med Prim Care 2014;3:443)
- Primary central nervous system lymphoma
- 54 year old woman with a 3 month history of numbness and weakness in the right leg (BMC Neurol 2019;19:90)
- Metastasis
- 72 year old man presented with multiple intraventricular lesions, an anterior mediastinal mass and a rectal mass (J Biomed Res 2019;34:318)
Cytology description
- Normal elements
- Benign elements in CSF
- Common
- Lymphocytes: small number of mature lymphocytes
- Monocytes: moderate cytoplasm and folded bean shaped nuclei
- Rare encounters
- Choroid plexus / ependymal cells
- Round to oval nucleus and moderate amount of cytoplasm
- Isolated in small clusters
- Brain fragments
- Fibrillary texture with glial cells, neurons and capillaries
- Seen in samples directly from ventricles
- Germinal matrix (GM) (Diagn Cytopathol 2021;49:449)
- Immature, blast‐like cells in clusters with cytoplasmic projections, round to oval nucleus, delicate chromatin and scant basophilic cytoplasm
- Mimicker of lymphoblasts, medulloblastoma, ependymoma, neuroblastoma and metastatic tumors
- Metabolically active and dependent on vascular supply
- Choroid plexus / ependymal cells
- Common
- Abnormal inflammatory cells
- Neutrophils
- May be seen in peripheral blood contamination, bacterial meningitis, viral meningitis, cytomegalovirus (CMV) radiculopathy, Toxoplasma meningoencephalitis and intravenous immunoglobulin (IVIG) treatment
- Macrophages
- Can be seen in multiple sclerosis, subarachnoid hemorrhage, meningitis, cerebral infarct and posttreatment
- Eosinophils
- Can be seen with parasites, shunts, medications, malignancies, Coccidioides immitis, Rocky Mountain spotted fever
- Plasma cells
- May be associated with multiple sclerosis, tuberculosis, Lyme disease, syphilis, cysticercosis and viral meningitis
- Abnormal plasma cells can be seen in infectious, autoimmune neurologic disorders (INDs), meningeal and cerebral involvement by hematologic disorders
- Neutrophils
- Contaminants
- Peripheral blood from a traumatic tap
- Best detected on air dried preparations (alcohol will lyse the RBCs)
- Chondrocytes and bone marrow
- Lumbar puncture needle inserted to far anterior
- Chondrocytes: pyknotic nucleus surrounded by purple mucopolysaccharide matrix
- Bone marrow: erythroid and myeloid elements are present when a vertebral body is hit by the needle
- Peripheral blood from a traumatic tap
- References: Biomedicines 2023;11:1461, Curr Issues Mol Biol 2022;44:3666, Neuro Oncol 2024;26:1781, Cells 2023;12:754, Front Neurol 2023;14:1076310
- Benign elements in CSF
Cytology images
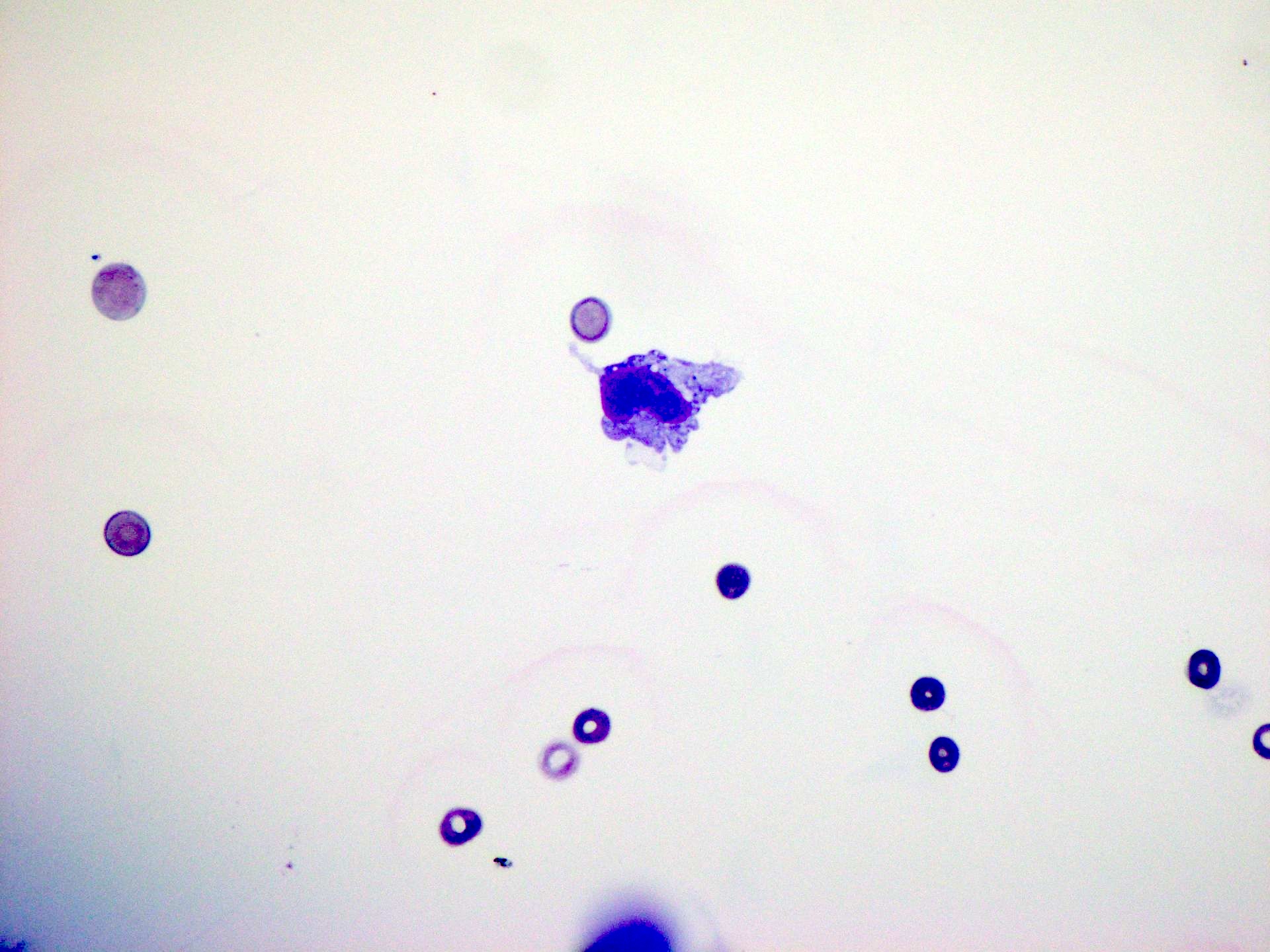
Contributed by Maria Cecilia D. Reyes, M.D. and Maria Luisa C. Policarpio-Nicolas, M.D.
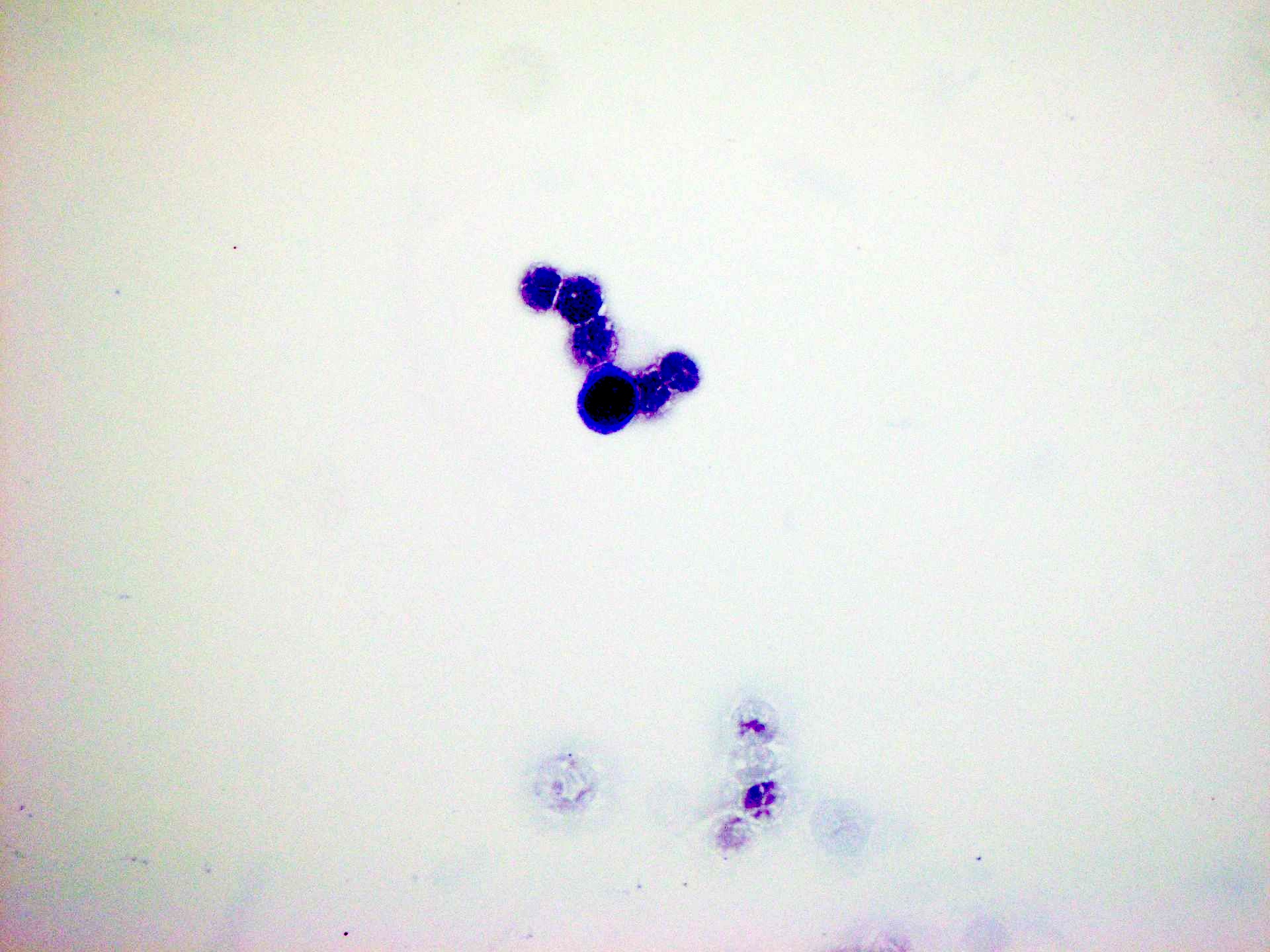
Lymphocyte
Monocyte
Plasma cell
Plasmablast
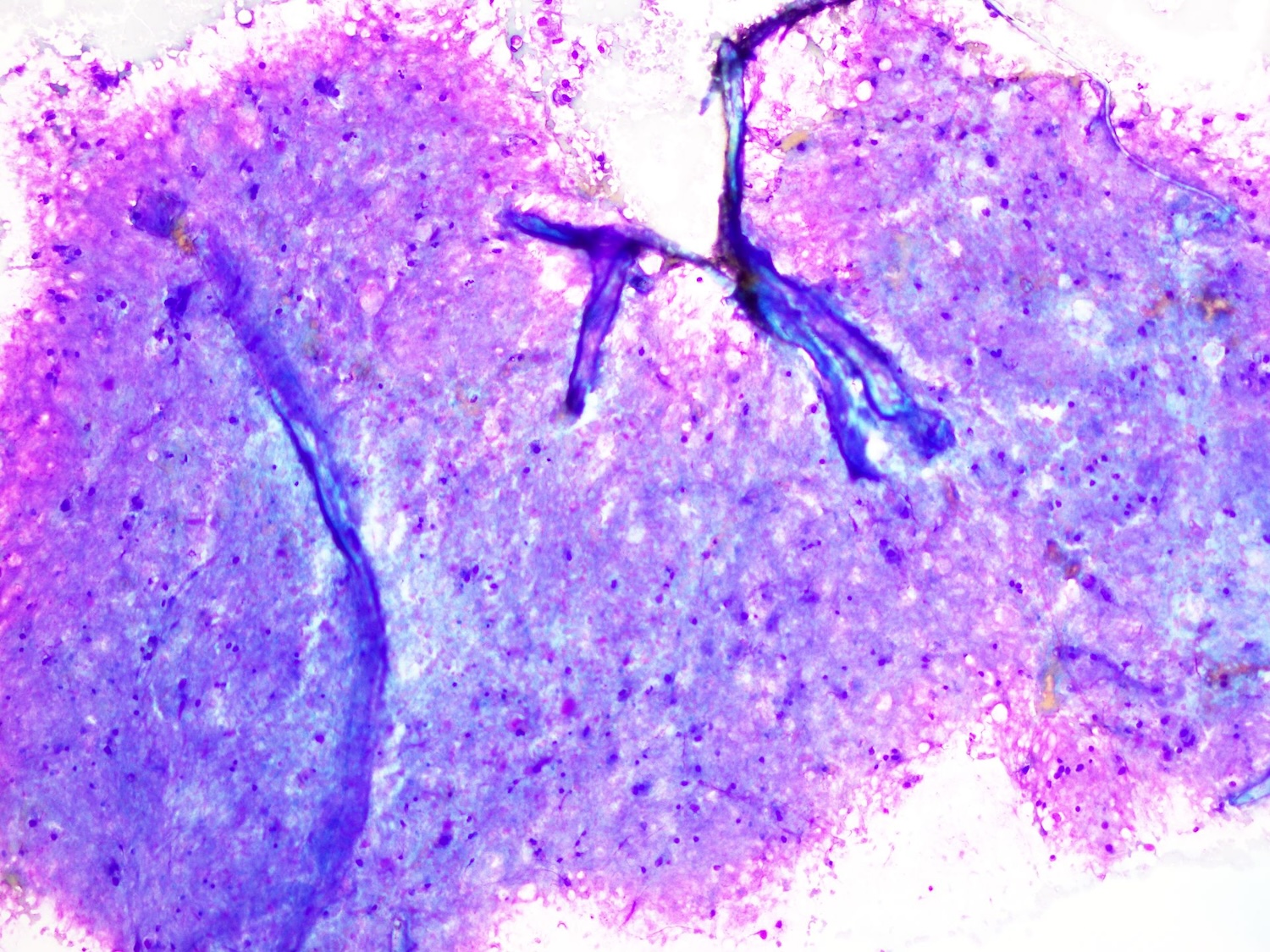
Brain tissue seen in CSF
Ependymal cell
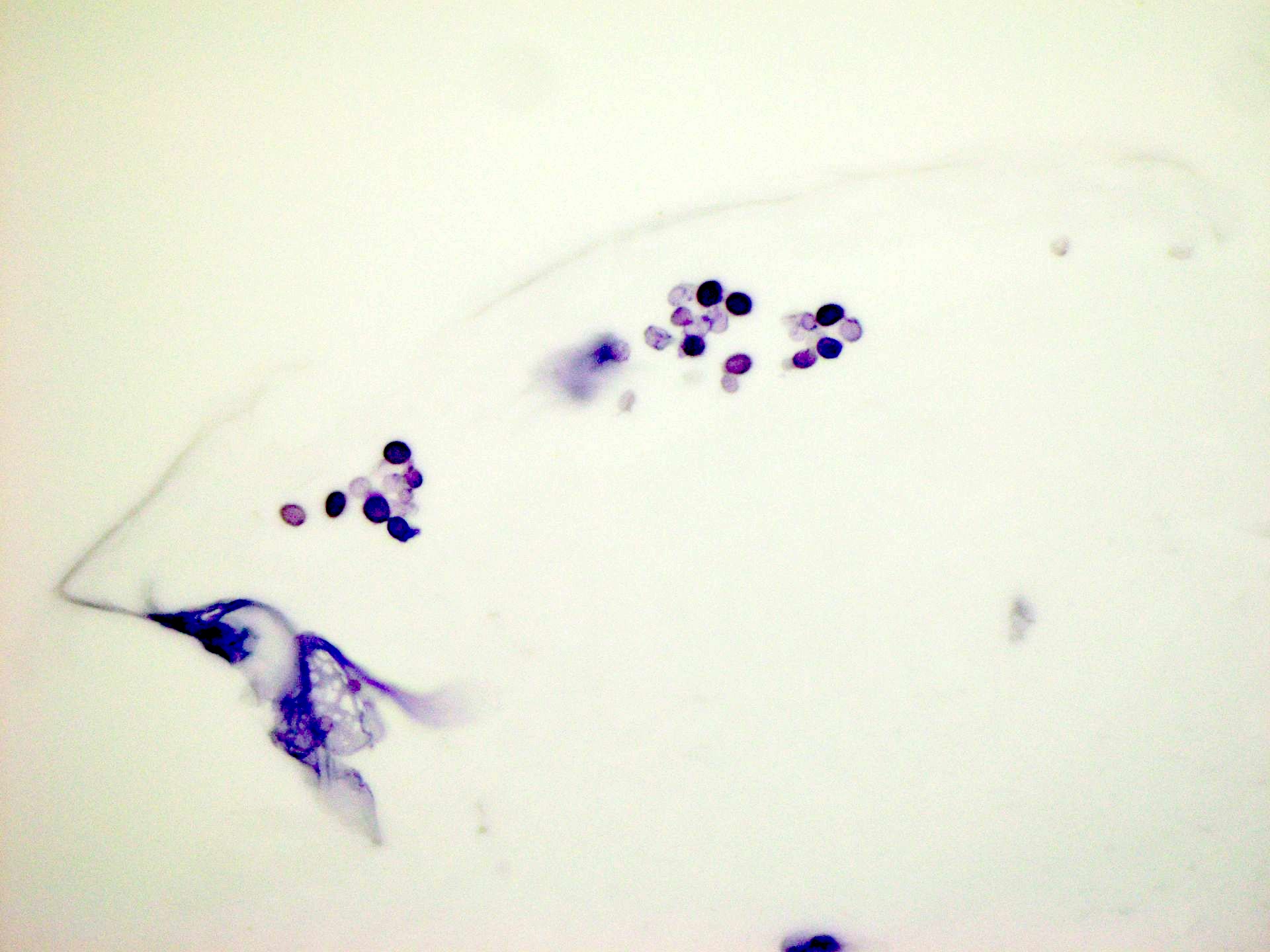
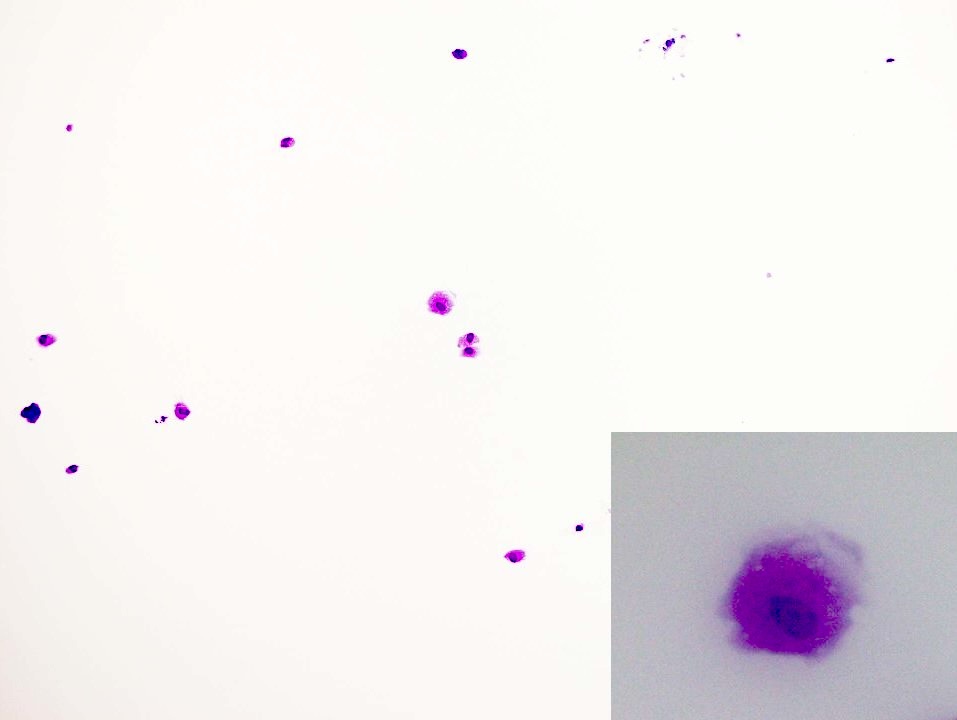
Cryptococcus in CSF
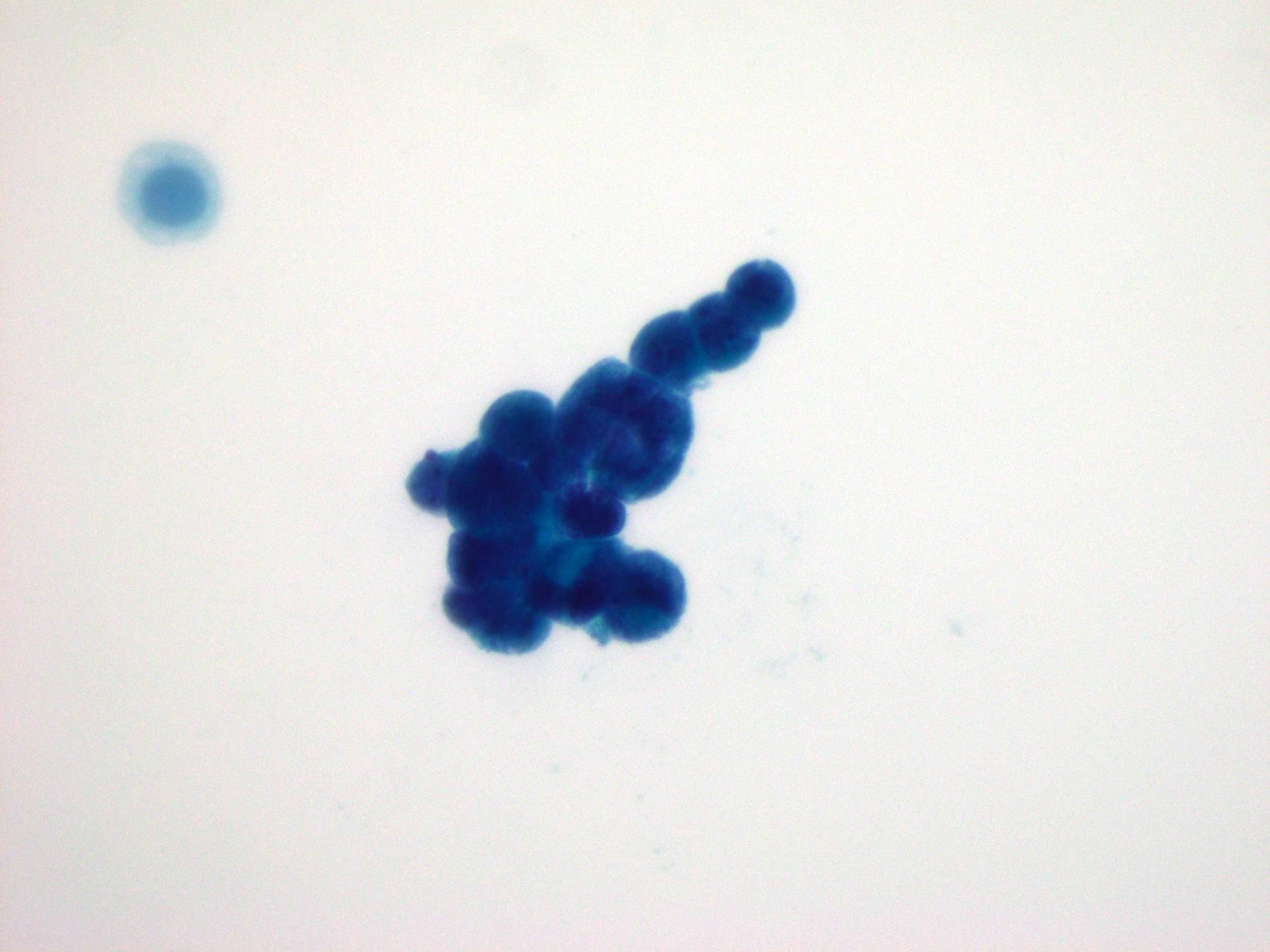
Glioblastoma in CSF
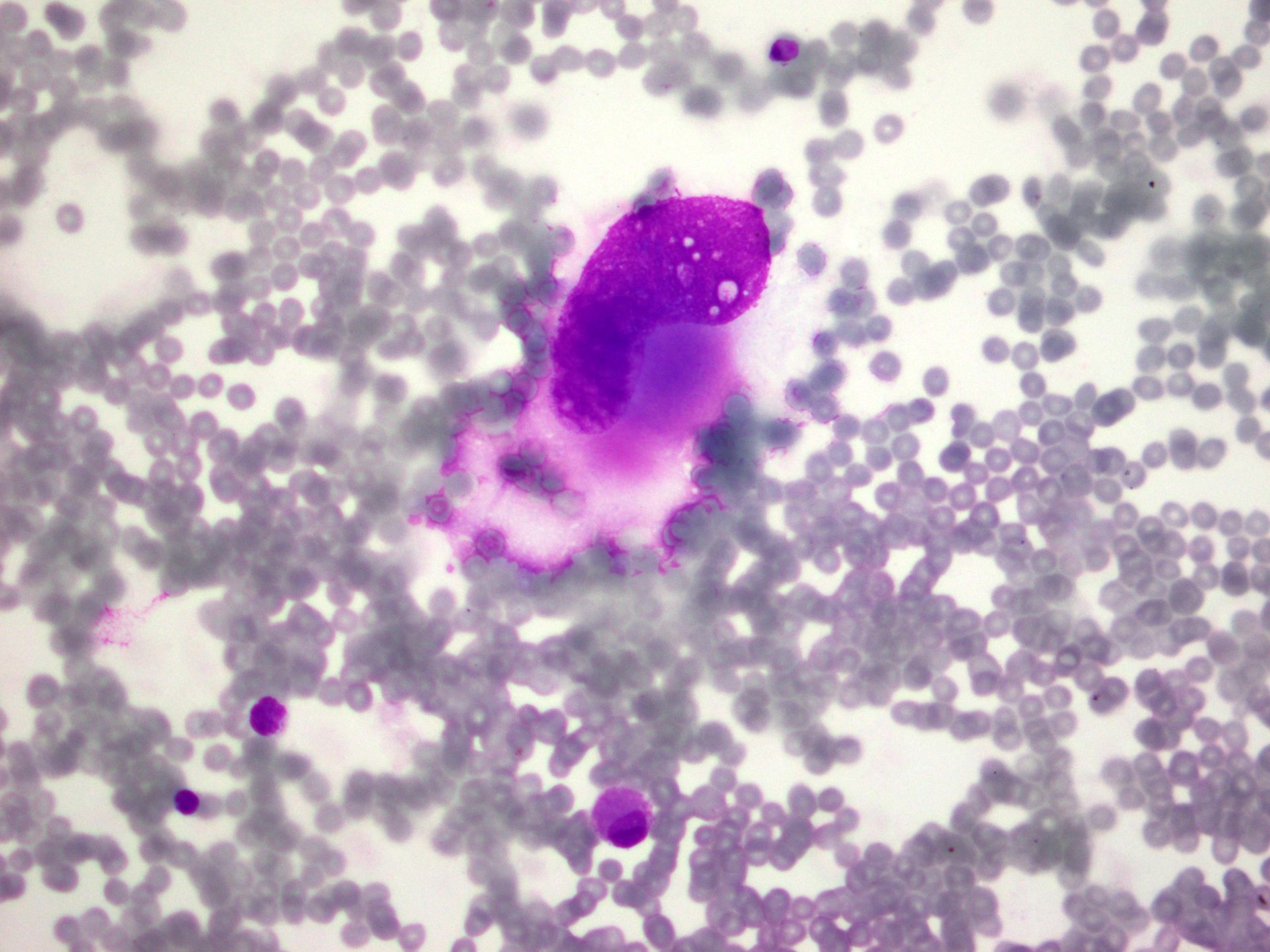
Metastatic breast adenocarcinoma
Images hosted on other servers:

Monocytoid cells with irregular nucleus
Sample pathology report
- Cerebrospinal fluid, lumbar puncture:
- Negative for malignancy (see comment)
- Comment: A paucicellular sample of lymphocytes and monocytes.
- Cerebrospinal fluid, lumbar puncture:
- Positive for malignancy (see comment)
- Comment: Blasts are present.
- Cerebrospinal fluid, lumbar puncture:
- Positive for malignancy, metastatic adenocarcinoma (see comment)
- Comment: Linear rows and isolated single large cells with scant cytoplasm, round nucleus and prominent nucleolus are present.
Differential diagnosis
- Nonneoplastic
- Traumatic tap (BMJ 2015;350:h568, Cal J Emerg Med 2007;8:3):
- No xanthochromia
- Red blood cell count < 2,000 x 106/L
- Acute bacterial meningitis:
- Numerous neutrophils with or without bacteria
- Aseptic meningitis:
- Increase in lymphocyte and monocyte numbers
- Atypical lymphocytes
- Cryptococcal meningitis:
- Round yeast forms with asymmetric, narrow based budding
- Mucopolysaccharide capsule (Papanicolaou stain)
- Refractile (air trapping)
- Toxoplasma meningoencephalitis:
- Neutrophils and mononuclear cells
- Tachyzoites
- Cysticercosis:
- Eosinophils and mononuclear cells
- Traumatic tap (BMJ 2015;350:h568, Cal J Emerg Med 2007;8:3):
- Neoplastic
- Hematologic neoplasms
- Acute lymphoblastic leukemia:
- L1: small blasts with scant basophilic cytoplasm, fine chromatin and round nucleus
- L2: larger blasts with abundant cytoplasm, irregular nucleus, fine chromatin and prominent nucleolus
- L3: blasts with dark blue cytoplasm, cytoplasmic vacuolates, coarse chromatin and multiple nucleoli
- Acute myeloid leukemia:
- Fine chromatin and prominent nucleolus
- Round or irregular nucleus
- Azurophilic granules
- Mature granulocytes
- Malignant lymphoma:
- Singly dispersed cells that are larger than lymphocytes and have irregular nuclear contours, abnormal chromatin and prominent nucleolus
- Meningeal and cerebral involvement in multiple myeloma patients:
- Singly dispersed cells with high N:C ratio, prominent nucleoli and central to eccentrically located nuclei
- Acute lymphoblastic leukemia:
- Primary tumors of the central nervous system
- Medulloblastoma:
- Small to medium sized cells with scant cytoplasm, hyperchromatic nucleus, molding and variably prominent nucleolus
- Astrocytomas and glioblastomas:
- Small anaplastic cells with hyperchromatic nuclei or large pleomorphic cells
- Oligodendroglioma:
- Distinct cell borders, clear cytoplasm, uniform round nucleus, fine chromatin and prominent nucleolus
- Ependymoma:
- Cuboidal or columnar with eccentric round or oval bland nucleus
- Atypical teratoid / rhabdoid tumor:
- Rhabdoid medium to large cells with homogeneous cytoplasm, round eccentric nucleus and prominent nucleolus
- Choroid plexus tumors
- Choroid plexus papilloma:
- Large clusters, with cuboidal cells and round nuclei
- Choroid plexus carcinoma:
- Clusters or single cells, pleomorphic nuclei and prominent nucleoli
- Can be mistaken for adenocarcinoma
- Choroid plexus papilloma:
- Pineal tumors:
- Indistinguishable from medulloblastoma
- Germ cell tumors:
- Single cells with moderate cytoplasm, large round nucleus and prominent nucleolus
- Medulloblastoma:
- Metastatic tumors
- Metastatic lung adenocarcinoma:
- Clusters or isolated large cells with abundant cytoplasm and eccentric nucleus
- Metastatic small cell carcinoma:
- Clustered or isolated cells with scant cytoplasm, nuclear molding and karyorrhexis
- Metastatic ductal breast carcinoma:
- Small groups, isolated cells, linear rows or rings
- Large cells with scant cytoplasm, round nucleus and prominent nucleolus
- Metastatic lobular breast carcinoma:
- Isolated small to medium sized cells with signet ring shapes
- Metastatic melanoma:
- Large cells with macronucleolus with or without melanin
- Melanophages
- Metastatic lung adenocarcinoma:
- Hematologic neoplasms
Additional references
Board review style question #1
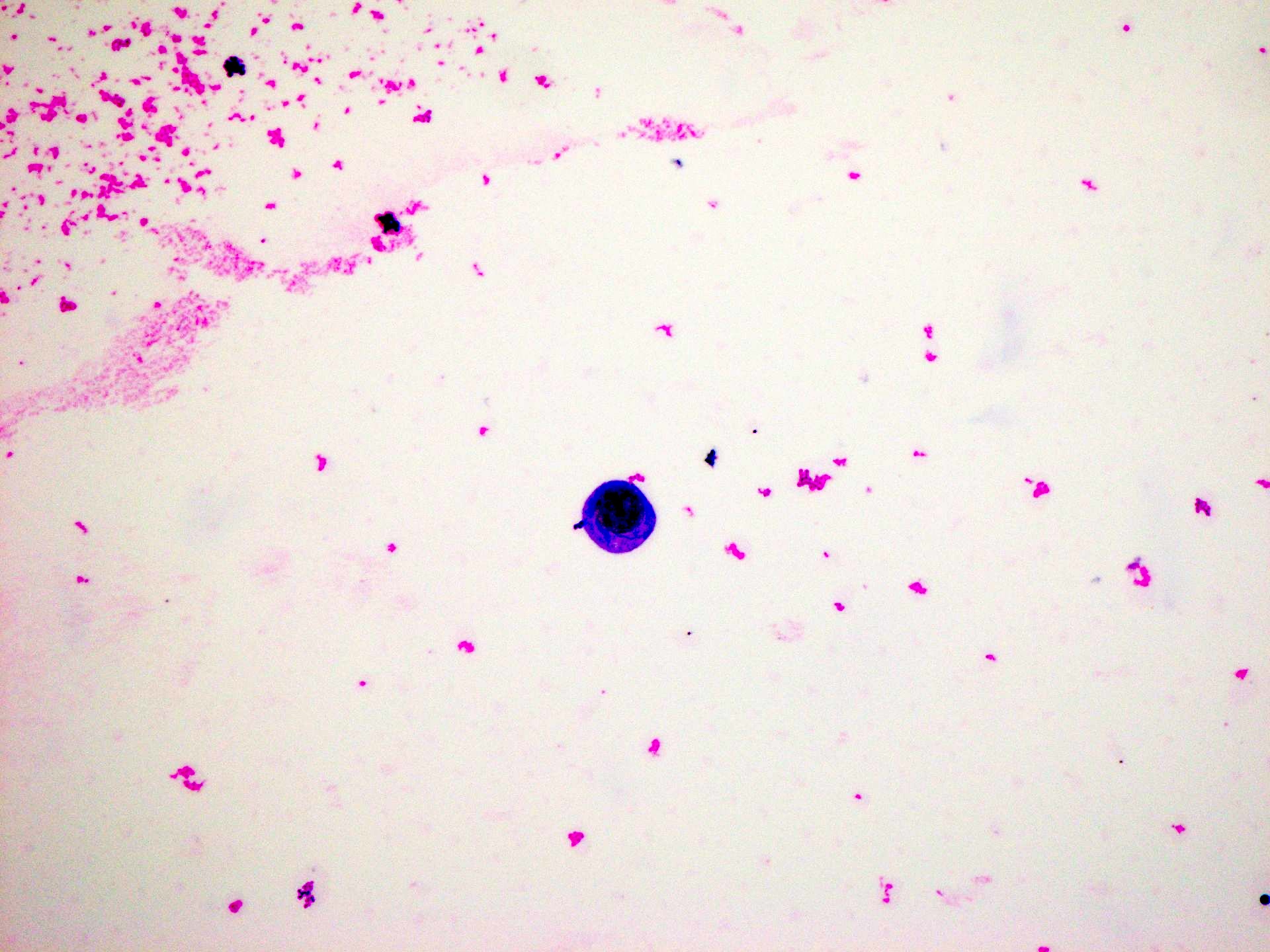
A human immunodeficiency virus (HIV) positive 35 year old man from New Mexico presented with headache, fever and confusion. A lumbar puncture was performed and cerebrospinal fluid (CSF) was submitted for cytological examination. On microscopic evaluation, the findings shown above were noted and described as round refractile organisms surrounded by a clear halo. What is the most likely diagnosis?
- Aspergillus fumigatus
- Candida albicans
- Coccidioides immitis
- Cryptococcus neoformans
- Histoplasma capsulatum
Board review style answer #1
D. Cryptococcus neoformans is a yeast that can cause meningoencephalitis, especially in immunocompromised patients. On CSF cytology, round refractile yeast forms with narrow based budding and mucopolysaccharide capsules are present. It is classically identified using an India ink preparation, which demonstrates the encapsulated yeast cells with a characteristic clear halo representing the polysaccharide capsule. Answer B is incorrect because Candida albicans has pseudohyphae and lacks the characteristic capsule. Answer E is incorrect because Histoplasma capsulatum is usually seen as small intracellular yeast forms in macrophages without a capsule. Answer C is incorrect because Coccidioides immitis appears as large spherules containing endospores. Answer A is incorrect because Aspergillus fumigatus will have septate hyphae with acute angle branching.
Comment Here
Reference: Cerebrospinal fluid overview
Comment Here
Reference: Cerebrospinal fluid overview
Board review style question #2
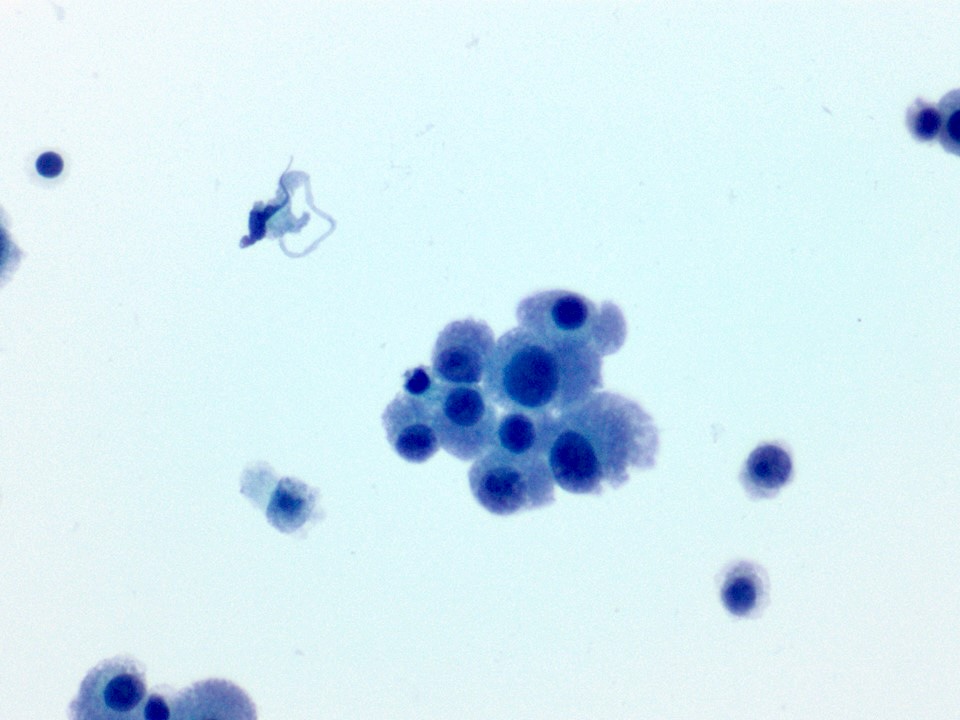
A cytological preparation is performed on a lumbar puncture cerebral spinal fluid specimen and reveals the image shown above. What is the most likely diagnosis?
- Astrocytoma
- Bacterial meningitis
- Cryptococcal meningitis
- Metastatic breast adenocarcinoma
- Mollaret meningitis
Board review style answer #2
D. Metastatic breast adenocarcinoma shows linear rows of cells with scant cytoplasm. Answer E is incorrect because it is classically associated with the monocytoid Mollaret cells with a stamped out nucleus. Answer C is incorrect because cryptococcal organisms are round refractile yeast forms with asymmetric, narrow based budding. Answer B is incorrect because bacterial meningitis is typically associated with numerous neutrophils and the bacteria may or may not be visualized or phagocytized. Answer A is incorrect because astrocytoma is associated with small anaplastic cells with hyperchromatic nuclei or large pleomorphic cells.
Comment Here
Reference: Cerebrospinal fluid overview
Comment Here
Reference: Cerebrospinal fluid overview
