

Colon
Carcinoma
Serrated adenocarcinoma (SAC)
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 21 January 2022
Last staff update: 21 January 2022
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Serrated adenocarcinoma[TIAB]


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Hernandez Gonzalo D, Feely M. Serrated adenocarcinoma (SAC). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumorserratedadeno.html. Accessed January 18th, 2025.
Definition / general
- Morphologic variant first recognized in the fourth edition of WHO; accounts for approximately 9.1% of all colorectal carcinomas (Hum Pathol 2010;41:1359)
Essential features
- Likely arises from malignant transformation of some sessile serrated polyps and traditional serrated adenomas (Mod Pathol 2019;32:1390)
- Can be diagnosed on histologic grounds alone without having to resort to recognition of residual serrated lesion
- Considered an end point carcinoma of the so called serrated pathway that can be reliably identified by morphologic features
- Most carcinomas arising from serrated precursors do not represent serrated adenocarcinomas (Mod Pathol 2019;32:1390)
ICD coding
- ICD-O: 8213/3 - serrated adenocarcinoma
Epidemiology
- M = F (Hum Pathol 2010;41:1359)
Sites
- More often proximal colon than conventional carcinoma, only in men (this association is not observed in women) (Hum Pathol 2010;41:1359)
Clinical features
- More frequently with lymph node metastases (51.8%) than conventional carcinomas (39.9%) (Hum Pathol 2010;41:1359)
- Node positive serrated adenocarcinomas have worse survival than node positive conventional carcinomas; left sided ones have the worst prognosis (Hum Pathol 2010;41:1359)
- Synchronous carcinomas are more often found in serrated adenocarcinoma than in conventional carcinoma (12.9% versus 3%) (Hum Pathol 2010;41:1359)
- Frequently encountered in more advanced stages than conventional carcinomas
- Less favorable 5 year survival than conventional carcinoma (especially left sided) (Hum Pathol 2010;41:1359)
Diagnosis
- Generally discovered on colonoscopy and confirmed on biopsy
Prognostic factors
- GNAS mutant serrated adenocarcinoma appears to be related to a poor prognosis and advanced stage (Histopathology 2017;70:1079)
Case reports
- 48 year old man with rectal tumor and perianal disease (Histopathology 2002;41:177)
- 70 year old woman with 6 carcinomas underwent right hemicolectomy (J Pathol 2000;190:444)
Treatment
- Surgical excision, with adjuvant chemotherapy for advanced / metastatic cases
- No treatment related differences between serrated adenocarcinoma and conventional carcinoma
- Treatment based on whether they are microsatellite stable or microsatellite instable (PD1 inhibitors but not 5FU are potential therapies if instable) and BRAF / KRAS / NRAS status (EGFR inhibitors not an option if any are mutated)
Clinical images
Contributed by David Hernandez Gonzalo, M.D. and Michael Feely, D.O.
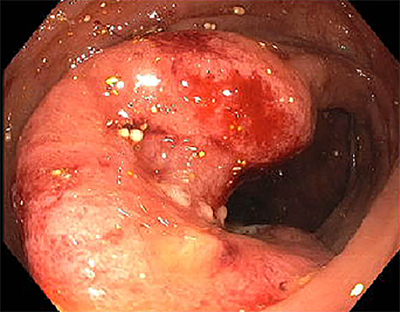
Colonoscopy
Microscopic (histologic) description
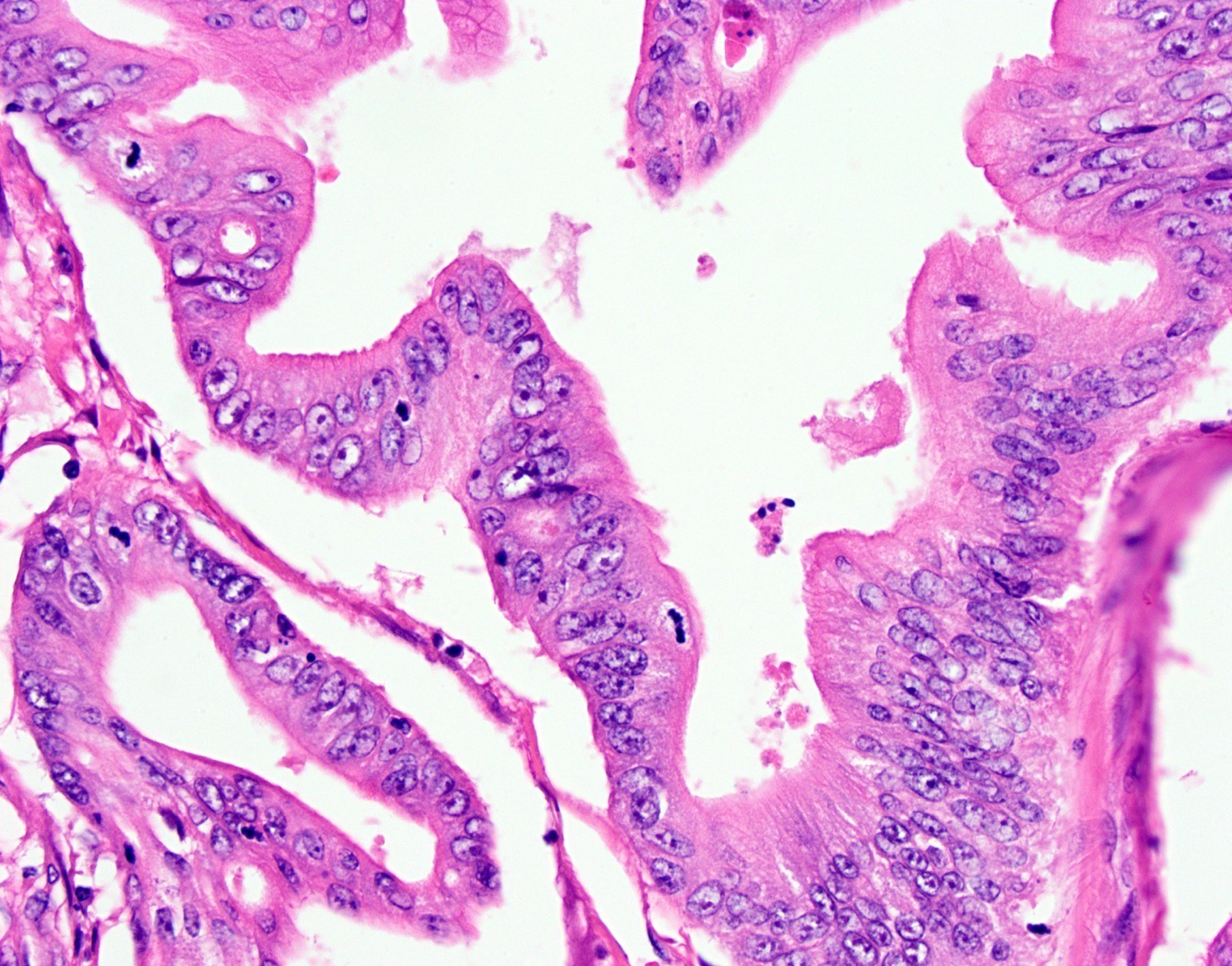
- Sawtoothed epithelial serrations
- Abundant clear or eosinophilic cytoplasm
- Vesicular nuclei with chromatin condensation at the nuclear envelope
- Absence of necrosis or < 10% of the total surface area
- Mucin production (cell balls and papillary rods in mucinous areas of tumor)
- A serrated polyp with or without dysplasia can sometimes be seen around its edges (Histopathology 2007;50:131)
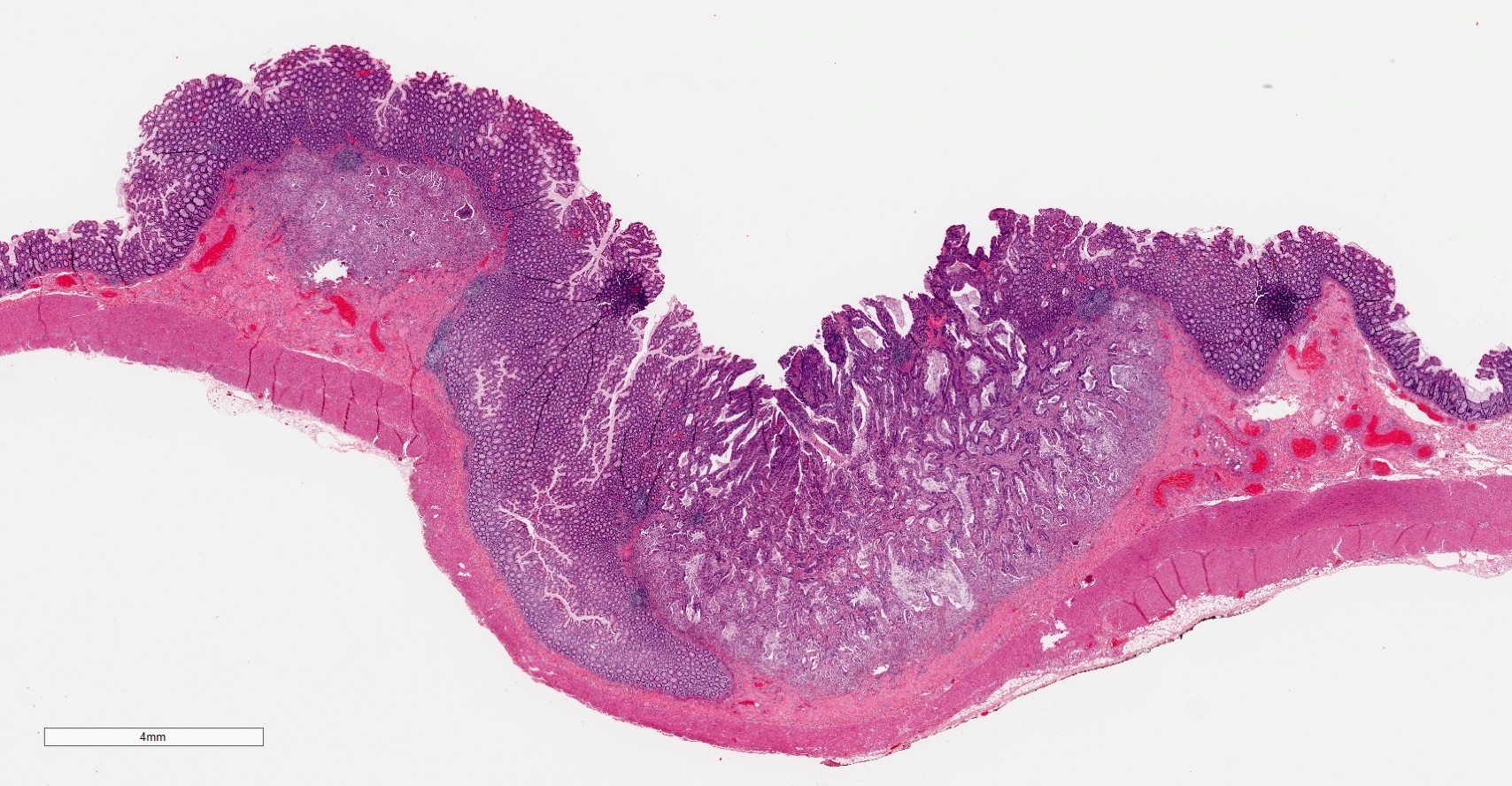
Microscopic (histologic) images
Contributed by David Hernandez Gonzalo, M.D. and Michael Feely, D.O.
Precursor lesions

Adjacent epithelium

Tumor and depth
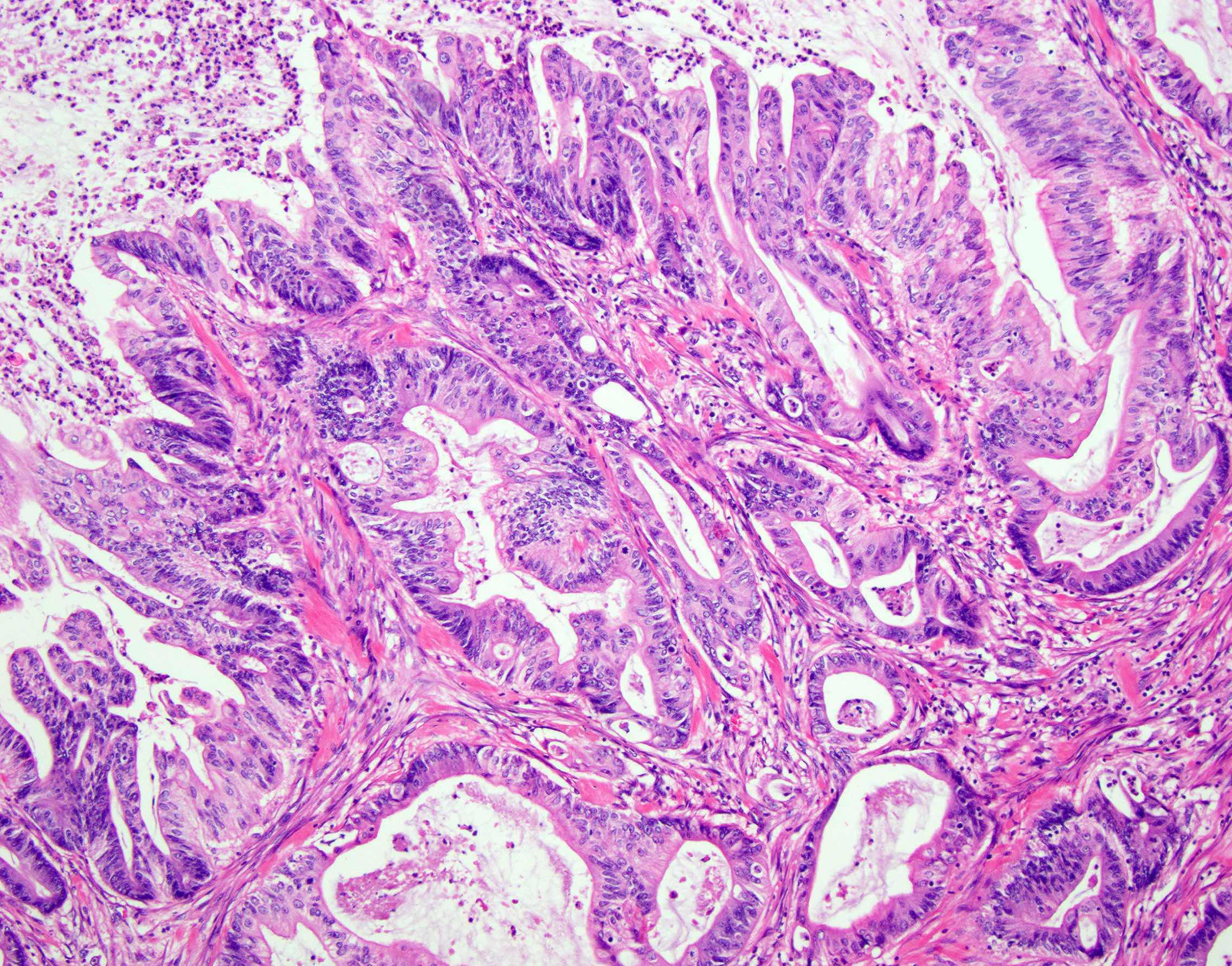
Architectural changes
Cytologic changes
Positive stains
- Not used in routine practice but reported to be valuable:
- Annexin A10 (sensitivity 42% and specificity 98%) (Virchows Arch 2015;466:5)
- Fascin 1: associated with tumor cell invasion (Int J Cancer 2013;132:297)
- Hippocalcin (antiapoptotic gene) (Int J Cancer 2013;132:297)
Molecular / cytogenetics description
- KRAS mutations (45%)
- BRAF mutations (33%)
- Microsatellite instable - high (18.9%)
- Microsatellite stable or microsatellite instable - low (81.1%) (Histopathology 2011;58:679)
Sample pathology report
- Colon, transverse, resection:
- Invasive serrated adenocarcinoma (see synoptic report)
- 54 lymph nodes, negative for carcinoma (0/54)
Differential diagnosis
- Conventional colorectal adenocarcinoma:
- Classic intestinal type cytology, cribriform architecture, dirty necrosis
- Mucinous (colloid) adenocarcinoma:
- More than half of tumor consists of extracellular mucin
- Mucin not typically diffuse in serrated adenocarcinoma
- No epithelial serrations in mucinous adenocarcinomas
Board review style question #1

Which of the following is true about this variant of colorectal adenocarcinoma?
- Diagnosis requires the presence of a serrated polyp adjacent to the serrated adenocarcinoma
- Extensive necrosis is usually present
- Most carcinomas arising from serrated precursors have this morphology
- This variant accounts for approximately 9.1% of all colorectal carcinomas
Board review style answer #1
D. Serrated adenocarcinoma accounts for approximately 9.1% of all colorectal carcinomas. A precursor serrated lesion is not always identified (A). There is no or little necrosis (< 10%) in serrated adenocarcinoma (B). Most carcinomas arising from serrated polyps have a microsatellite instable - high histology (such as medullary, mucinous, signet ring cells, lack of dirty necrosis, tumor infiltrating lymphocytes) (C).
Comment Here
Reference: Serrated adenocarcinoma
Comment Here
Reference: Serrated adenocarcinoma
Board review style question #2
Which of the following is true regarding the molecular aspect of serrated adenocarcinoma?
- Chemotherapy regimens are currently different for serrated adenocarcinoma compared to conventional adenocarcinoma
- GNAS mutant serrated adenocarcinoma has a better prognosis
- KRAS or BRAF mutations are present in over 75% of cases
- Most serrated adenocarcinomas are microsatellite instable - high
Board review style answer #2
C. Mutually exclusive mutations in KRAS or BRAF are present in over 75% of cases. There are no treatment related differences between serrated adenocarcinoma and conventional carcinoma (A). GNAS mutant serrated adenocarcinoma appears to be related to a poor prognosis and advanced stage (B). Microsatellite instability - high is only seen in 18.9% of serrated adenocarcinoma cases (D). Remember, in general, a serrated pathway can lead to microsatellite instable - high, microsatellite instable - low or microsatellite stable cancer.
Comment Here
Reference: Serrated adenocarcinoma
Comment Here
Reference: Serrated adenocarcinoma

