
Colon
Mesenchymal tumors
Gastrointestinal stromal tumor
Author: Raul S. Gonzalez, M.D.

Last author update: 24 February 2021
Last staff update: 12 June 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Gastrointestinal stromal tumor
See Also: Appendix, Esophagus, Small bowel, Soft tissue, Soft tissue-staging, Stomach


Table of Contents
Definition / general | Essential features | Terminology | Sites | Clinical features | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gonzalez RS. Gastrointestinal stromal tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumorgist.html. Accessed March 31st, 2025.
Definition / general
- Tumors that differentiate along lines of interstitial cells of Cajal, the gut's pacemaker cells (Mod Pathol 2003;16:366)
Essential features
- Mesenchymal spindle cell neoplasm caused by KIT or PDFRGA mutations
- Risk stratification is based on location, size and mitotic rate
- Very rare in colon; rectal GISTs account for roughly 5% of all GISTs
Terminology
- Leiomyoblastoma and gastrintestinal autonomic nerve tumor (GANT) are old terms no longer used
Sites
- 5% or fewer of GISTs occur in the colorectum (usually the rectum) (Arch Pathol Lab Med 2006;130:1466)
Clinical features
- Median age 67 years (Am J Surg Pathol 2000;24:1339)
- The majority of lesions are aggressive and lead to patient death
- Asymptomatic microscopic "seedling" GISTs are quite rare (Am J Surg Pathol 2008;32:867)
Prognostic factors
- Risk of disease progression for rectal GISTs depends on tumor size and mitotic rate (Semin Diagn Pathol 2006;23:70)
- If mitotic rate is < 5 per 5 square mm, risk of progression is 0% (< 2 cm), 8.5% (> 2 to < 5 cm) or 57% (> 10 cm) (insufficient data for > 5 to < 10 cm)
- If mitotic rate is > 5 per 5 square mm, risk of progression is 54% (< 2 cm), 52% (> 2 to < 5 cm) or 71% (> 10 cm) (insufficient data for > 5 to < 10 cm)
- There is insufficient data for progression estimation in colonic GISTs
Case reports
- Man in mid 40s with GIST of the transverse colon
- 65 year old man with prostatic stromal sarcoma and rectal GIST (Urology 2006;68:672.e11)
- 71 year old man with a large rectal adenoma and interstitial cell of Cajal hyperplasia (Case #428)
Treatment
- Tyrosine kinase inhibitors, including imatinib mesylate (first line) and sunitinib malate
Gross description
- Often large, bulky, intramural masses
- Fish flesh or tannish brown parenchyma with hemorrhage, necrosis and cystic softening
Microscopic (histologic) description
- Mesenchymal tumor usually centered in the muscularis propria
- Spindle cell GISTs: intersecting fascicles of plump spindled cells with eosinophilic cytoplasm within variably hyalinized or edematous stroma
- Epithelioid GISTs: rounded epithelioid cells with pseudo compartmental organization
- Skeinoid fibers (extracellular collagen globules) may be seen
- Muscle infiltration is common but not predictive of behavior
- Rarely has osteoclast-like giant cells (Arch Pathol Lab Med 2004;128:440)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
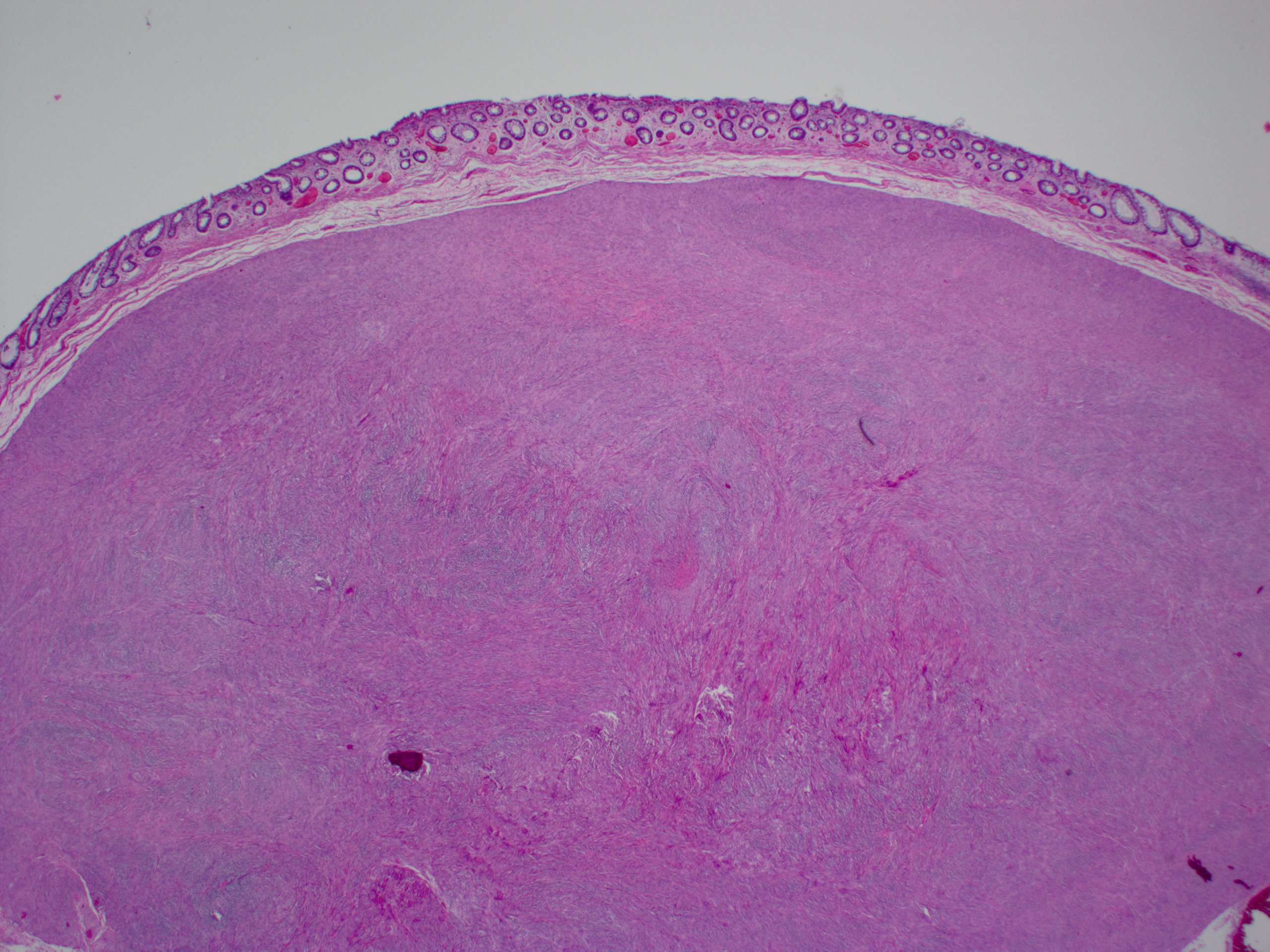
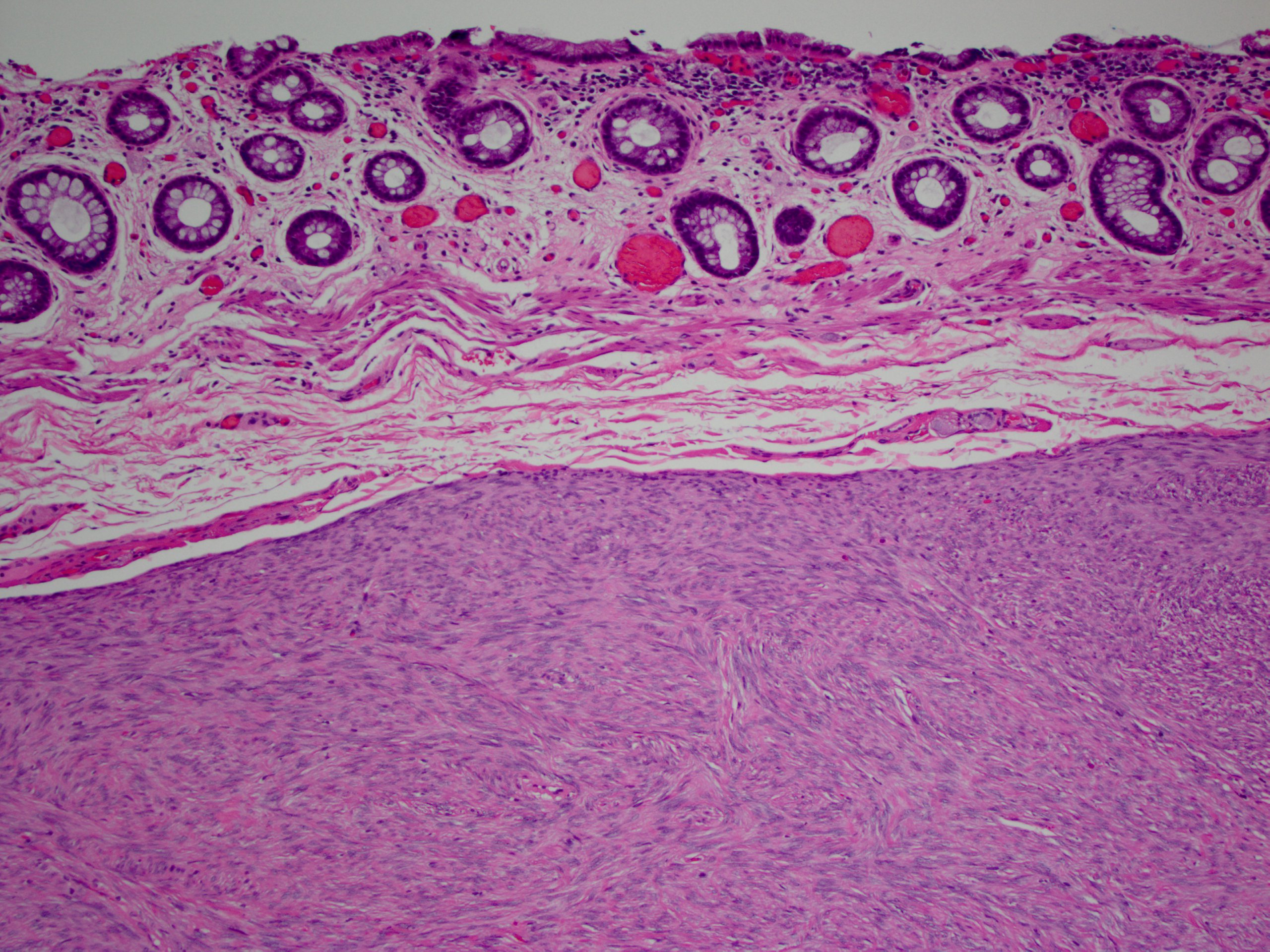
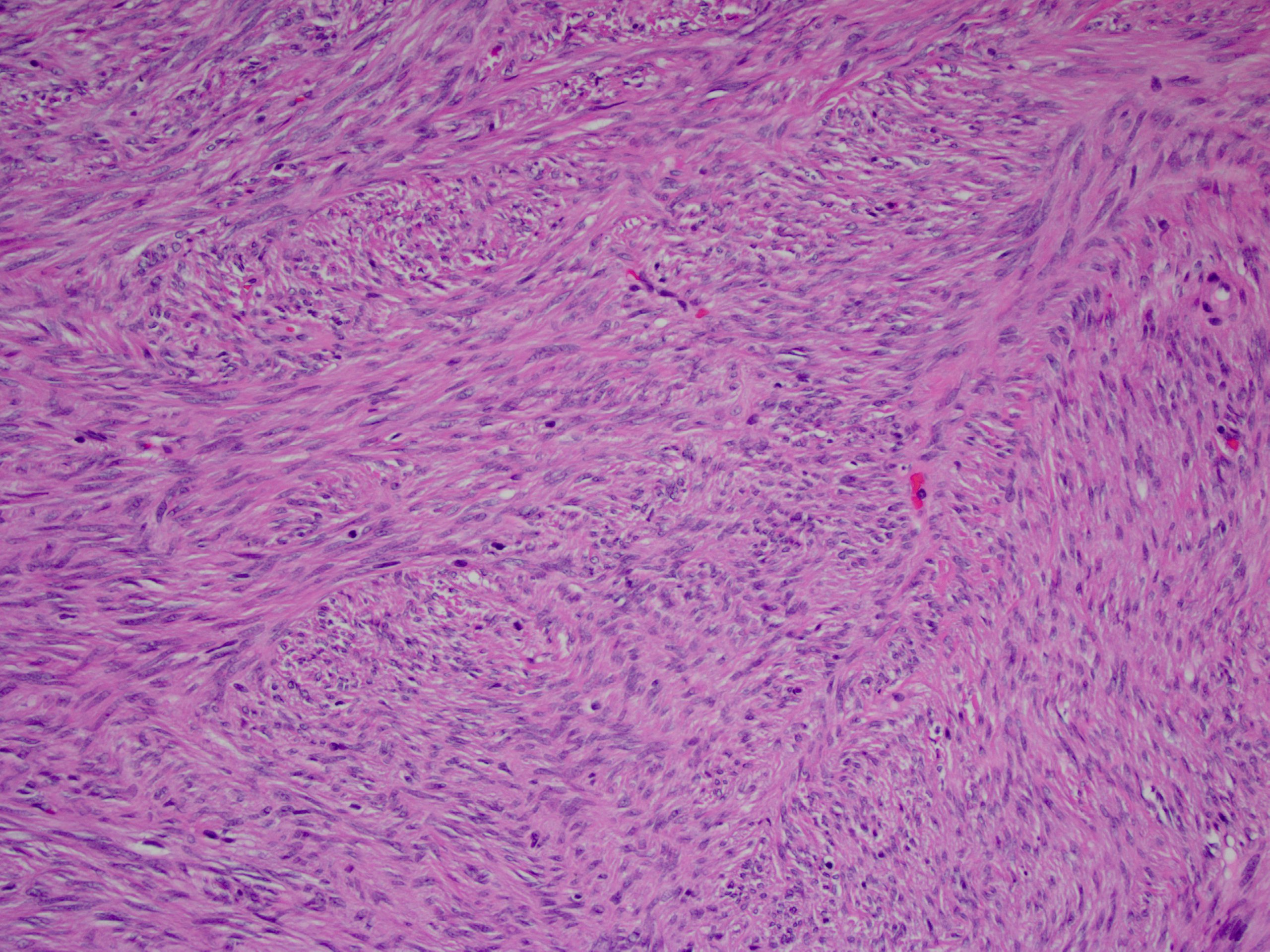
Rectal GIST
Images hosted on other servers:

Epithelioid cells and osteoclast-like giant cells

Spindled cells

KIT+

CD34+

PDGFRA+
Positive stains
- DOG1 (ANO1), CD117, protein kinase C-theta, CD34 (Am J Surg Pathol 2009;33:1401)
- Alpha smooth muscle actin (30% - 40%), S100 (rare)
- Variable keratin (rare, weak)
Negative stains
Electron microscopy description
- Processes or cell bodies with intermediate filaments showing solitary focal densities
- Attachment plaques with incomplete lamina, rare myofilaments and smooth endoplasmic reticulum (Ultrastruct Pathol 2002;26:269)
Molecular / cytogenetics description
- 80% have mutations in KIT, which encodes CD117; exons affected include 11, 9, 13 and 17 (Nat Rev Cancer 2011;11:865)
- 10% have mutations in PDGFRA; exons affected include 18, 14 and 12; these GISTs are often gastric and epithelioid
- Both mutations have been identified in small incidental GISTs, affirming their importance
- Up to 10% have neither mutation and are associated with syndromes such as neurofibromatosis type 1 and Carney's triad
Sample pathology report
- Ascending colon, resection:
- Gastrointestinal stromal tumor (4.3 cm) (see synoptic report and comment)
- Comment: The tumor is positive for KIT and DOG1 by immunohistochemistry. The mitotic rate is 2 per 5 square mm. Risk stratification for colonic GISTs has not been established but the risk in this case is likely relatively low (an analogous rectal GIST would have a risk of progression of 8.5%).
Differential diagnosis
- Fibromatosis:
- Long, sweeping fascicles and dilated, thin walled blood vessels; nuclear positivity for beta catenin; may be positive for CD117 (Am J Surg Pathol 2000;24:947)
- Inflammatory fibroid polyp:
- Inflammatory myofibroblastic tumor:
- Leiomyoma:
- Bland and brightly eosinophilic; positive for actin and desmin; negative for CD117 (Int J Colorectal Dis 2006;21:84)
- Leiomyosarcoma:
- Marked atypia and necrosis; positive for smooth muscle actin or desmin; negative for CD117; no KIT mutations
Board review style question #1
What is the most common site for gastrointestinal stromal tumors in the large intestine?
- Appendix
- Cecum
- Rectum
- Transverse colon
Board review style answer #1
Board review style question #2
What 2 factors are used to estimate risk of progression in gastrointestinal stromal tumors?
- Ki67 index and necrosis
- Ki67 index and size
- Mitotic rate and necrosis
- Mitotic rate and size
Board review style answer #2
