
Colon
Other nonneoplastic
Sclerosing mesenteritis
Author: Raul S. Gonzalez, M.D.

Last author update: 17 February 2021
Last staff update: 10 May 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed search: sclerosing mesenteritis colon


Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Etiology | Clinical features | Radiology description | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Gonzalez RS. Sclerosing mesenteritis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colonsclerosingmes.html. Accessed March 31st, 2025.
Definition / general
- Uncommon nonneoplastic condition that causes thickening and shortening of colonic mesentery (JBR-BTR 2011;94:241)
Essential features
- Benign fibrotic / inflammatory condition involving the mesentery
- Some cases are IgG4 related
Terminology
- Older terms include idiopathic retractile mesenteritis, mesenteric panniculitis and mesentery lipodystrophy (Am J Surg Pathol 1997;21:392)
Epidemiology
- Common in rural areas of Peru, otherwise fairly uncommon (Rev Gastroenterol Peru 1998;18:114)
- Possibly underdiagnosed in life, as indicated by 1 autopsy series (Schweiz Med Wochenschr 1985;115:1218)
Sites
- Affects the mesentery; small bowel mesentery is involved more often than colonic
Etiology
- Usually idiopathic but some cases likely a form of IgG4 sclerosing disease (J Clin Pathol 2008;61:1093)
Clinical features
- Usually men with median age of 65 years; most common symptom is abdominal pain; can lead to patient death (Clin Gastroenterol Hepatol 2007;5:589)
Radiology description
- Mesentery can show fat attenuation or a fibrofatty mass
Case reports
- 40 year old man with large mesenteric mass (Arch Pathol Lab Med 2001;125:443)
- 46 year old woman with rectosigmoid disease (Surg Today 1996;26:435)
Treatment
- Various medications (including corticosteroids) and surgery, depending on clinical severity (Int Arch Med 2011;4:17)
Clinical images
Images hosted on other servers:

Thick mesentery with yellow nodules
Gross description
- Markedly thickened and rubbery mesentery causing bowel twisting
Microscopic (histologic) description
- Fibrosis with dense collagen, fat necrosis, chronic inflammation (especially around vessels) and variable focal calcification
- Minimal atypia, no or few mitoses
- IgG4 related cases lack fat necrosis and show obliterative phlebitis and increased inflammation
Microscopic (histologic) images
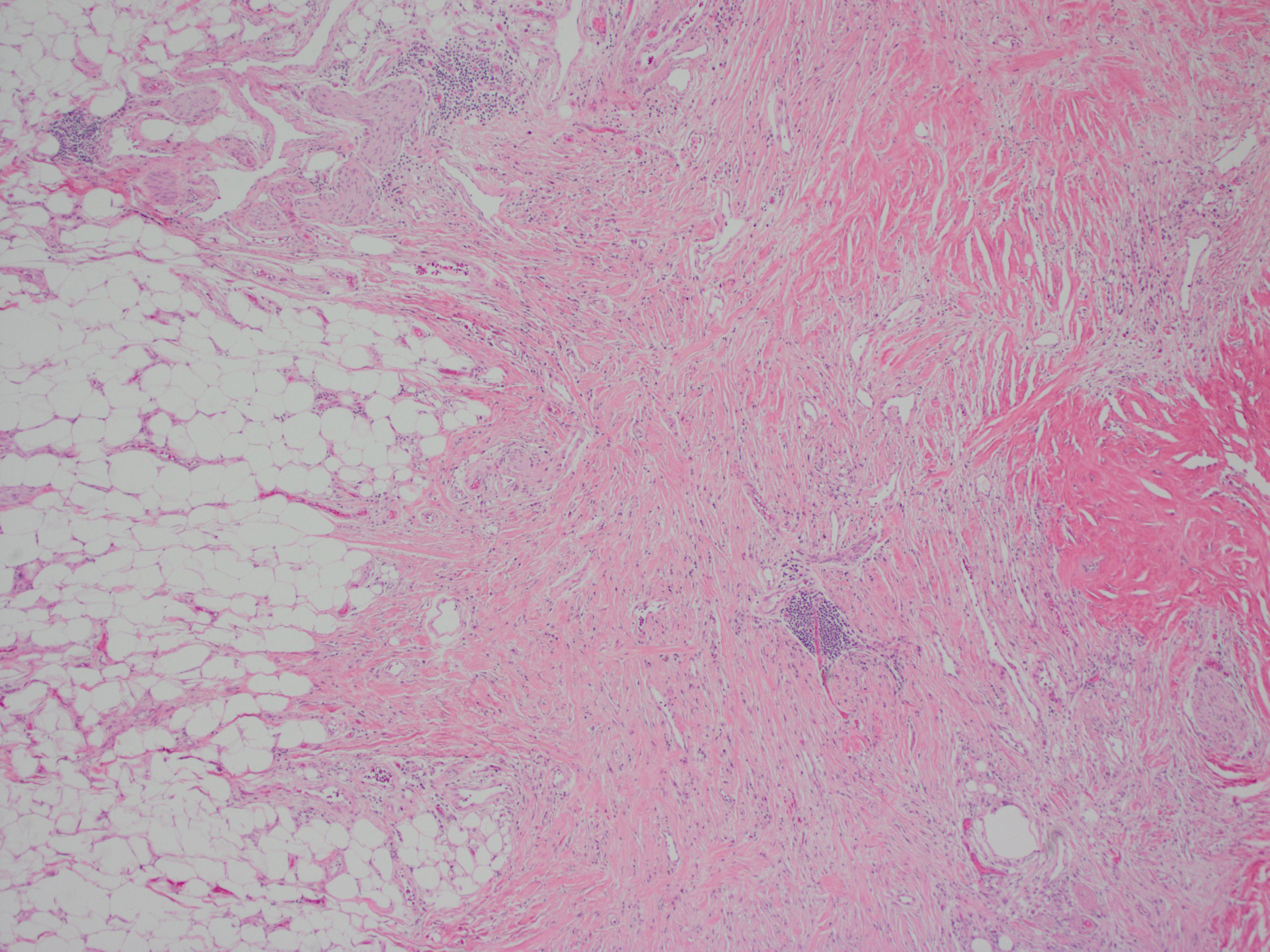
Contributed by Raul S. Gonzalez, M.D.
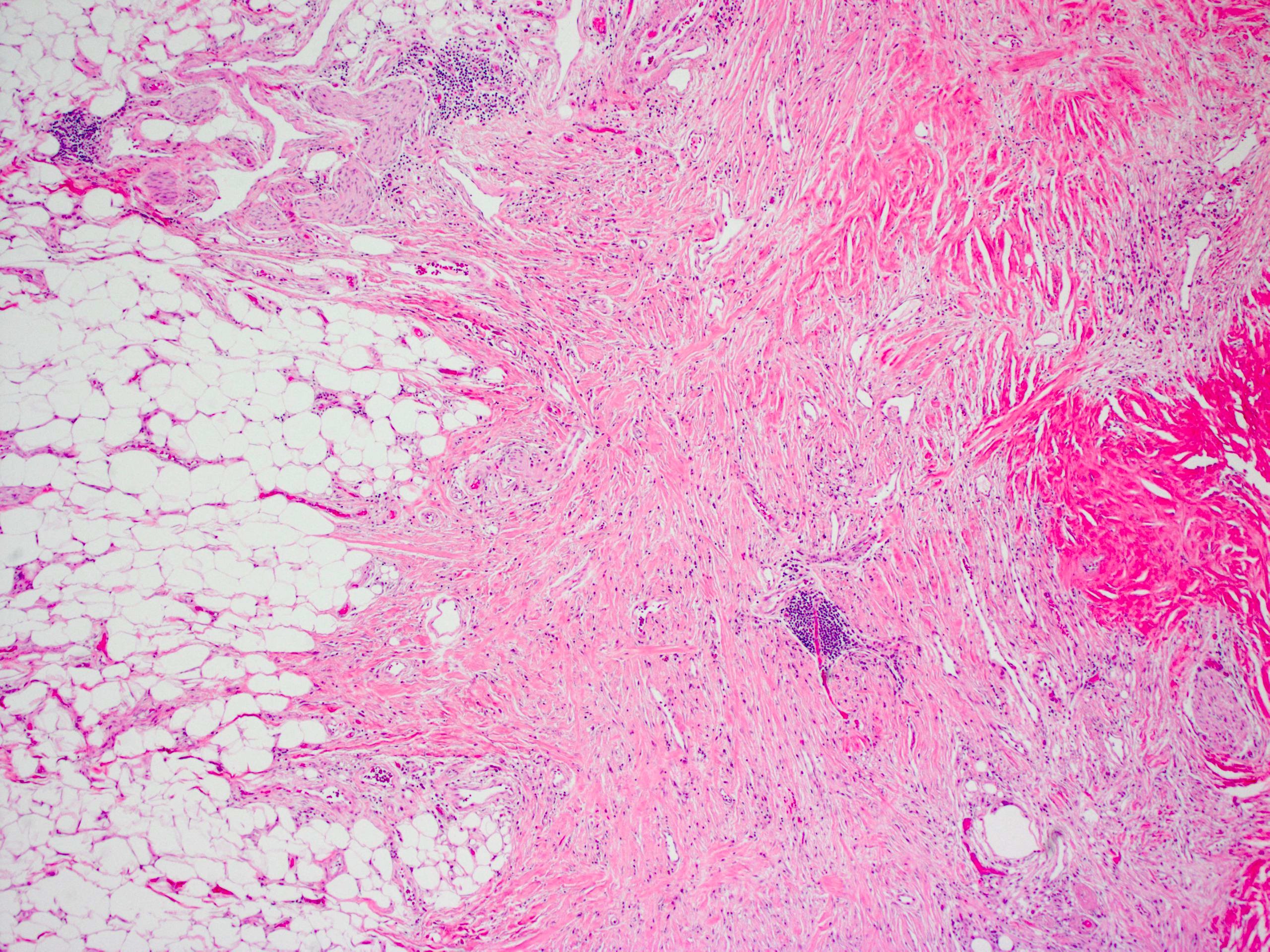
Fibrosis and chronic inflammation
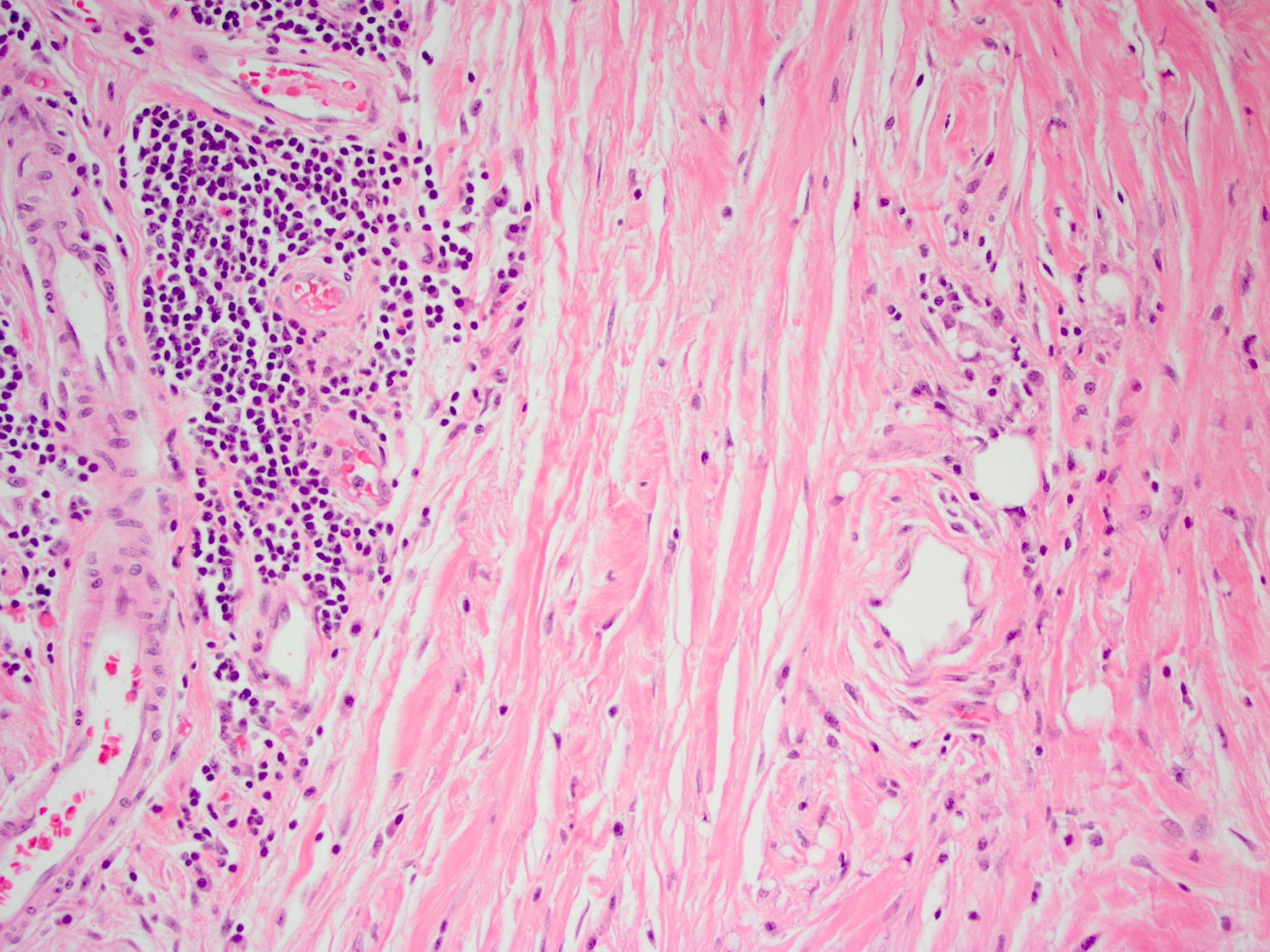
Fibrosis and chronic inflammation, high power
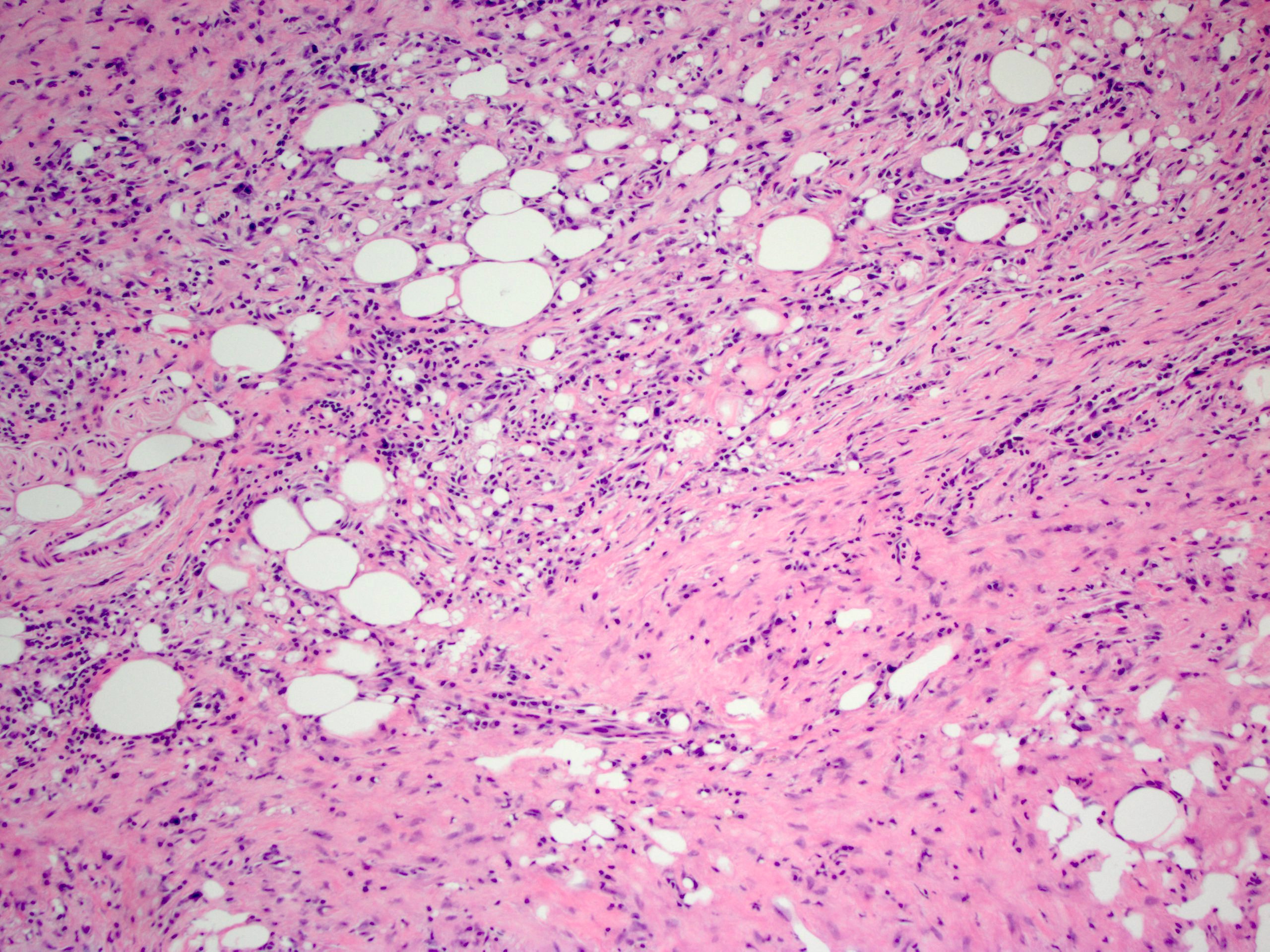
Fibrosis, chronic inflammation and fat necrosis
Images hosted on other servers:


Fat necrosis, sclerosing fibrosis, chronic inflammation

Fat necrosis with numerous lipid laden macrophages
Positive stains
- IgG4 (in some cases)
Negative stains
- Nuclear beta catenin staining not present
Sample pathology report
- Transverse colon and mesentery, excision:
- Prominent bland fibrotic process involving mesentery (see comment)
- Segment of colon with reactive change.
- Negative for malignancy.
- Margins of resection unremarkable.
- Comment: The overall findings are most consistent with sclerosing mesenteritis.
Differential diagnosis
- Fibromatosis:
- Positive for nuclear beta catenin
- Idiopathic retroperitoneal fibrosis:
- Located in retroperitoneum, not mesentery
- Inflammatory myofibroblastic tumor:
- Spindle cells more prominent
- May be positive for ALK1
- Liposarcoma:
- Atypical cells visible (Chirurg 2001;72:742)
- Sclerosing lymphoma:
- Inflammatory infiltrate more prominent
Additional references
Board review style question #1
Which of the following is true about sclerosing mesenteritis?
- IgG4 immunohistochemistry will always highlight numerous plasma cells
- It is a neoplastic process
- It is common in the pediatric population
- Treatment can involve medication rather than surgery
Board review style answer #1
D. Treatment can involve medication rather than surgery
Comment Here
Reference: Sclerosing mesenteritis
Comment Here
Reference: Sclerosing mesenteritis
