
Colon
Noninfectious colitis
Ischemic colitis
Authors: Gagandeep Kaur, M.D., Monika Vyas, M.D.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 4 March 2021
Last staff update: 4 March 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: ischemic colitis[title] colon review[ptyp]


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kaur G, Vyas M. Ischemic colitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colonischemic.html. Accessed March 27th, 2025.
Definition / general
- Ischemic colitis is a leading cause of acute abdomen in elderly patients
- Gross and microscopic findings depend on the severity and duration of ischemia
- Classic findings include superficial mucosa necrosis / regeneration, withered crypts and lamina propria hyalinization
Essential features
- Gross and microscopic spectrum of ischemic colitis varies by the duration and extent of ischemia
- Classic ischemic type mucosal injury pattern is described as superficial mucosa necrosis / regeneration, withered crypts and lamina propria hyalinization; this histology is not specific for ischemia and may be seen with infections (C. difficile, E. coli O157:H7), medications and inflammatory bowel disease
- In cases with severe sudden ischemia, the affected segment of bowel is infarcted with red, congested or grayish dusky discoloration with transmural necrosis
Terminology
- Ischemic colitis
- Noninfectious colitis
ICD coding
- ICD-10: K55.9 - Vascular disorder of intestine, unspecified
Epidemiology
- Incidence: 4.5 - 44 per 100,000 (WMJ 2016;115:196)
- Most common in older patients and mainly in debilitated elderly women (Front Surg 2017;4:47)
- Younger patients can be affected; this is on the rise (WMJ 2016;115:196)
Sites
- Watershed areas most commonly affected (splenic flexure and rectosigmoid colon); the right colon is involved in 20 - 25% of cases (WMJ 2016;115:196)
Pathophysiology
- 2 categories: vascular factors and bowel factors, both leading to inadequate blood flow to the colonic wall and causing ischemic injury (WMJ 2016;115:196)
- Vascular factors:
- Transient hypoperfusion is the most common cause
- Vasospasm of the colonic vessels is another mechanism, either due to systemic hypoperfusion which shunts blood away from intestine or due to vasoconstrictive effects of certain drugs and substances
- Hypercoagulable states, such as coagulation factor deficiencies
- Vasculitis, such as systemic lupus erythematous and antiphospholipid syndrome
- Bowel factors:
- Constipation, irritable bowel syndrome (IBS), fecal impaction, colonic obstruction and any other condition that increases the intraluminal pressure, which may compromise the blood flow the colonic wall, leading to ischemic injury
- Extent of ischemic changes in the intestines depends on the severity, rate of onset and duration of ischemia
- Transient, reversible vascular obstruction often leads to mild superficial changes, whereas sudden, complete obstruction results in complete infarction of the affected segment with transmural necrosis (see colon infarct)
Etiology
- Most cases represent nonocclusive ischemia caused by a sudden decrease in blood flow in the small arterioles of the colon, resulting from a low volume state (Front Surg 2017;4:47)
- Risk factors include atherosclerotic disease, aortic surgery, coronary artery bypass graft, atrial fibrillation, oral contraceptives, hereditary coagulopathies, cocaine abuse, strenuous physical activity, bacterial pathogens (cytomegalovirus and E. coli), hypertension, diabetes mellitus and hypoalbuminemia
- Constipation, hyperuricemia, smoking may contribute to disease development in young adults
- Other risk factors in younger patients: collagen vascular diseases, amyloidosis or cocaine use
- Idiopathic myointimal hyperplasia of mesenteric veins (Am J Surg Pathol 2017;41:1657)
Clinical features
- Classic symptoms in elderly are abdominal pain, hematochezia and leukocytosis
- Left sided ischemic colitis presents with acute abdominal pain and lower gastrointestinal bleeding
- Right sided ischemic colitis presents with severe abdominal pain but rarely bloody diarrhea
- Full thickness involvement of the colonic wall can lead to perforation with peritonitis and sepsis
- Reference: Front Surg 2017;4:47
Diagnosis
- CT scan is the investigation of choice (BMJ 2016;355:i6600)
- CT angiogram finds abnormalities in the vasculature (Front Surg 2017;4:47)
- Xrays can help in detecting perforation by demonstrating gas under the diaphragm
- Colonoscopy should be performed within 48 hours to visualize mucosa; it can show edematous and fragile mucosa, segmental erythema, erosions, hemorrhages and ulceration
- An endoscopic finding, the so called colon single stripe sign represents a single line of erythema with erosion or ulceration placed along the longitudinal axis of the large bowel; this sign is highly suggestive of ischemic injury and indicates a milder disease
- Pseudomembranes can be seen, characterized by elevated yellow-white nodules or plaques on the mucosal surfaces of the colon biopsy (Dis Mon 2015;61:181)
Laboratory
- Complete blood count, metabolic panel and liver function tests are required to assess the physiologic status of the patient (Front Surg 2017;4:47)
- C reactive protein and neutrophil count are likely to be raised
- Serum lactate levels may be raised as a result of systemic dysfunction and hypoperfusion (BMJ 2016;355:i6600)
Radiology description
- CT may appear normal in mild disease (Front Surg 2017;4:47)
- In more advanced but nongangrenous forms of the disease, CT will often show colonic wall thickening, thumbprinting, colonic dilatation and pericolic fat stranding, with or without the presence of ascitic fluid
- Double halo or target sign may be present
- Emboli or thrombus occluding the inferior mesenteric artery is occasionally seen while the corresponding colonic wall appears thin due to the lack of reperfusion
- Air within the mesenteric or the portal venous system or pneumatosis coli is a serious finding indicating bowel infarction
Prognostic factors
- If the ischemia is limited to the mucosa, the disease will be transient and complete recovery is expected
- Ischemia involving the muscularis propria can lead to scarring and stricture formation
- If ischemia involves full thickness of the bowel wall, it may lead to gangrene and perforation of the colonic wall with peritonitis and sepsis
- Reference: Front Surg 2017;4:47
Case reports
- 20 year old man with ischemic colitis associated with rhabdomyolysis and heat stroke after intense exercise (Korean J Gastroenterol 2019;74:115)
- 35 year old woman with end stage renal disease on hemodialysis who developed ischemic colitis associated with sevelamer crystals (Indian J Nephrol 2019;29:191)
- 38 year old woman with schizoaffective disorder presenting with olanzapine induced ischemic colitis (Rev Esp Enferm Dig 2016;108:507)
- 55 year old woman with mass forming ischemic colitis (Case Rep Pathol 2019;2019:8927872)
- 59 year old man with ischemic colitis caused by polycythemia vera (Exp Ther Med 2018;16:3663)
Treatment
- Transient ischemia is managed conservatively and has a relatively good prognosis (Front Surg 2017;4:47)
- Conservative therapy includes fluid resuscitation, optimizing cardiac output, bowel rest and discontinuing the etiologic agent
- Antibiotic therapy can be started
- For severe disease, urgent laparotomy and removal of the necrotic part of the colon is recommended
Clinical images
Images hosted on other servers:

Colonoscopic findings

Endoscopic images
Gross description
- Ulcers, pseudopolyps
- Frank blood or dark mucus in lumen
- Segmental thinning in areas of full thickness infarction or gangrene
- Tan-brown dusky areas of the bowel mucosa
- Pseudomembranous appearance in exudative cases
- Perforation can be identified in severe cases
- Fibrosis and stricture formation in late cases
- When grossing specimens, carefully dissect blood vessels and submit numerous sections to detect vascular lesions
- Rarely, ischemic colitis can produce mass forming lesions (Am J Surg Pathol 2015;39:1275)
- References: Dig Dis Sci 2009;54:2009, World J Gastroenterol 2008;14:7302
Gross images
Contributed by Gagandeep Kaur, M.D. and Monika Vyas, M.D.
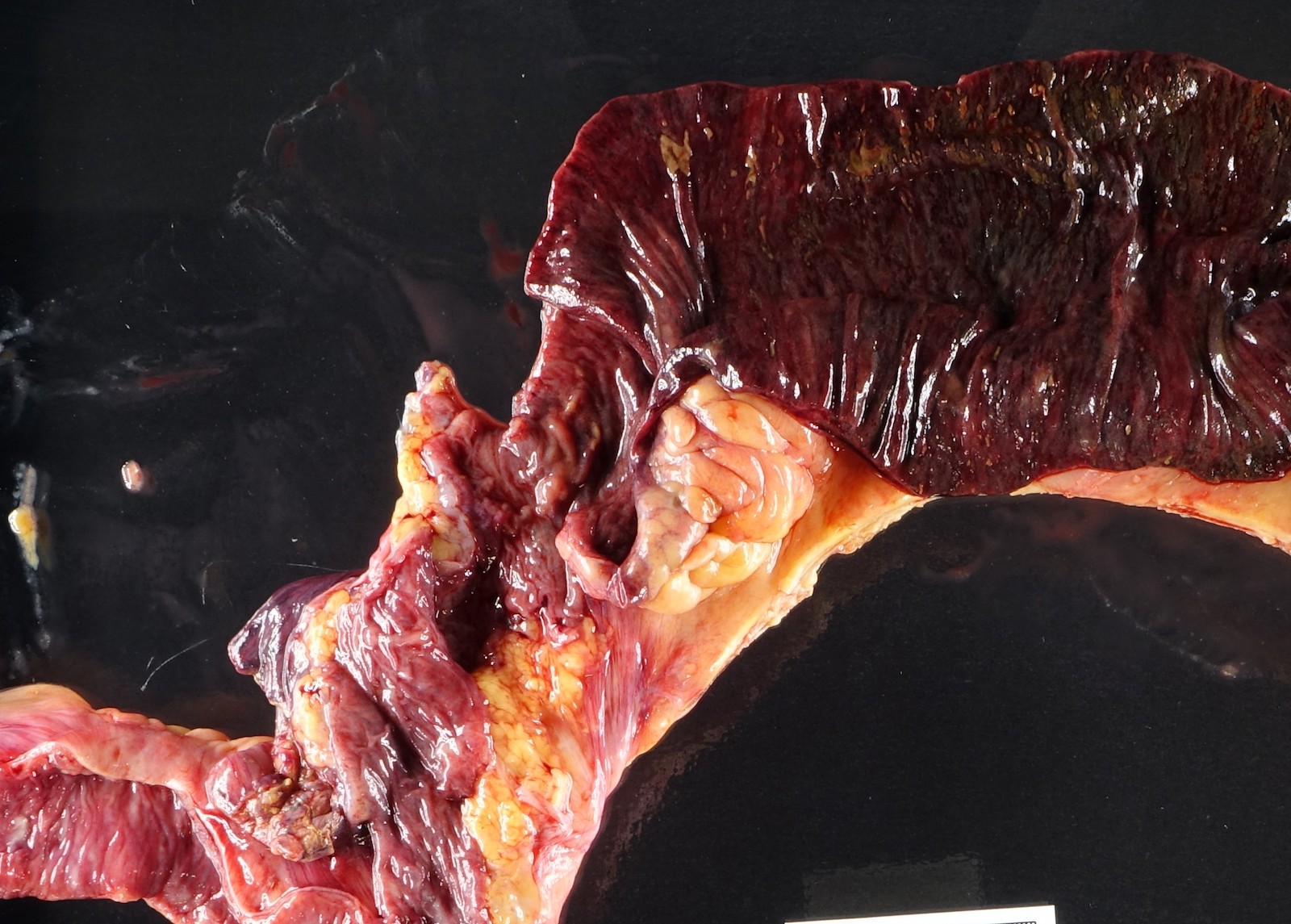
Ischemic bowel

Ischemic bowel with pseudomembranes

Gangrenous bowel
Microscopic (histologic) description
- Early transient ischemia may result in mild changes, such as mucosal edema, denudation and congestion
- With more advanced ischemia, superficial mucosal necrosis ensues, which results in crypt damage (withering) or loss and hyalinization of the lamina propria
- A reduced number and size of crypts and fibrosis in lamina propria suggests a more severe injury
- Necrosis, ulceration and granulation tissue extend into submucosa and surrounding smooth muscle fibers of muscularis mucosae in more severe cases
- Acute cases may exhibit acute inflammatory exudate (pseudomembranes) on the mucosa, even when noninfectious
- Atypical reactive or degenerative changes may be seen, mimicking dysplasia or malignancy (e.g. pseudosignet ring cells)
- Hemosiderin / hemorrhage and edema in lamina propria
- May see crypt abscesses (especially in cases with reperfusion); however, fissures, lymphoid follicles and granulomas are absent
- In patients with chronic ischemia, histologic findings may represent a mixture of ischemic features described above, along with foci of chronic mucosal injury, such as crypt architectural distortion, Paneth cell metaplasia, basal lymphoplasmcytosis and active inflammation, mimicking inflammatory bowel disease
- Vessels may show necrotizing phlebitis, hyaline thrombi or capillary microthrombi, cholesterol crystals (atheroembolism) or myointimal hyperplasia
- Cholesterol crystals, when present in vascular lumens, support a diagnosis of atheroembolism
- In some cases, underlying etiology can be identified
- References: Goldblum: Rosai and Ackerman's Surgical Pathology, 11th Edition, 2017, Arch Pathol Lab Med 2001;125:224, Am J Surg Pathol 1997;21:706
Microscopic (histologic) images
Contributed by Gagandeep Kaur, M.D. and Monika Vyas, M.D.
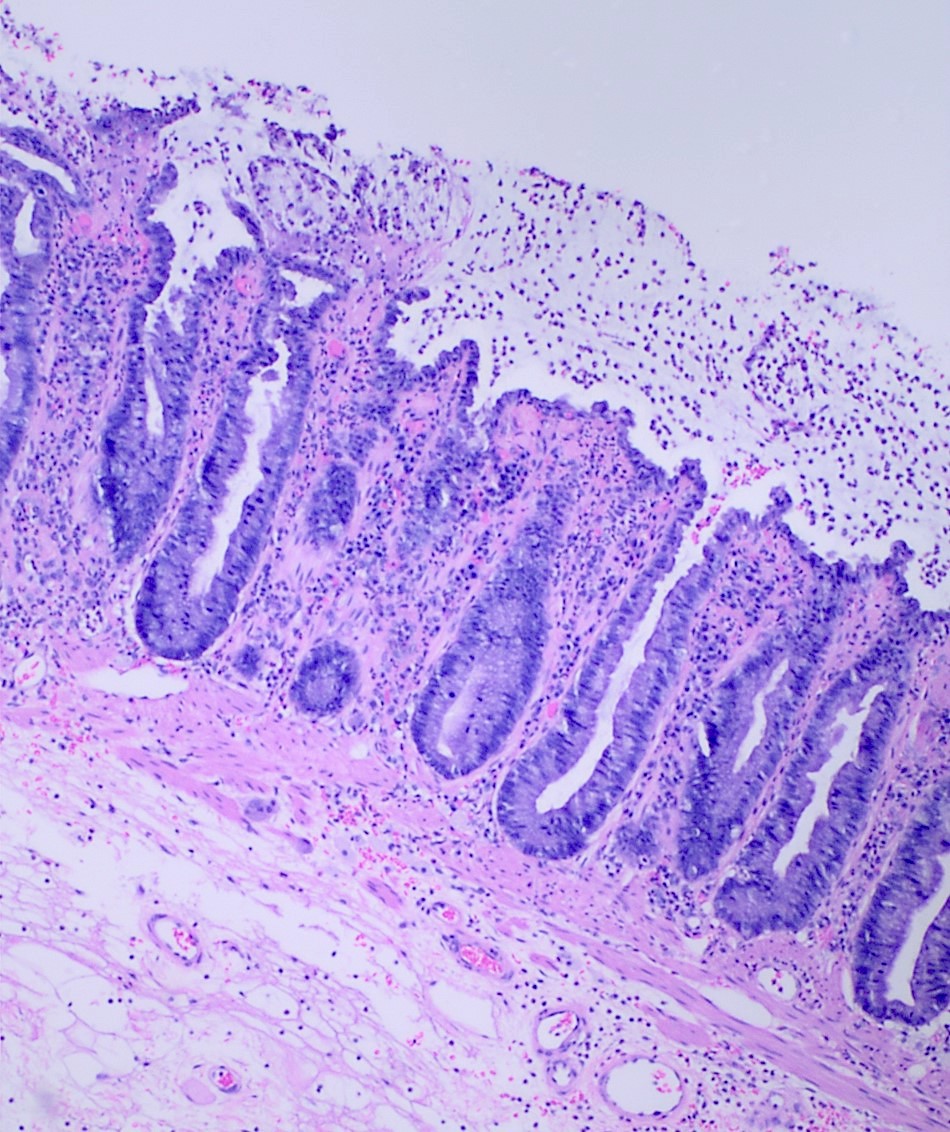

Acute ischemic changes
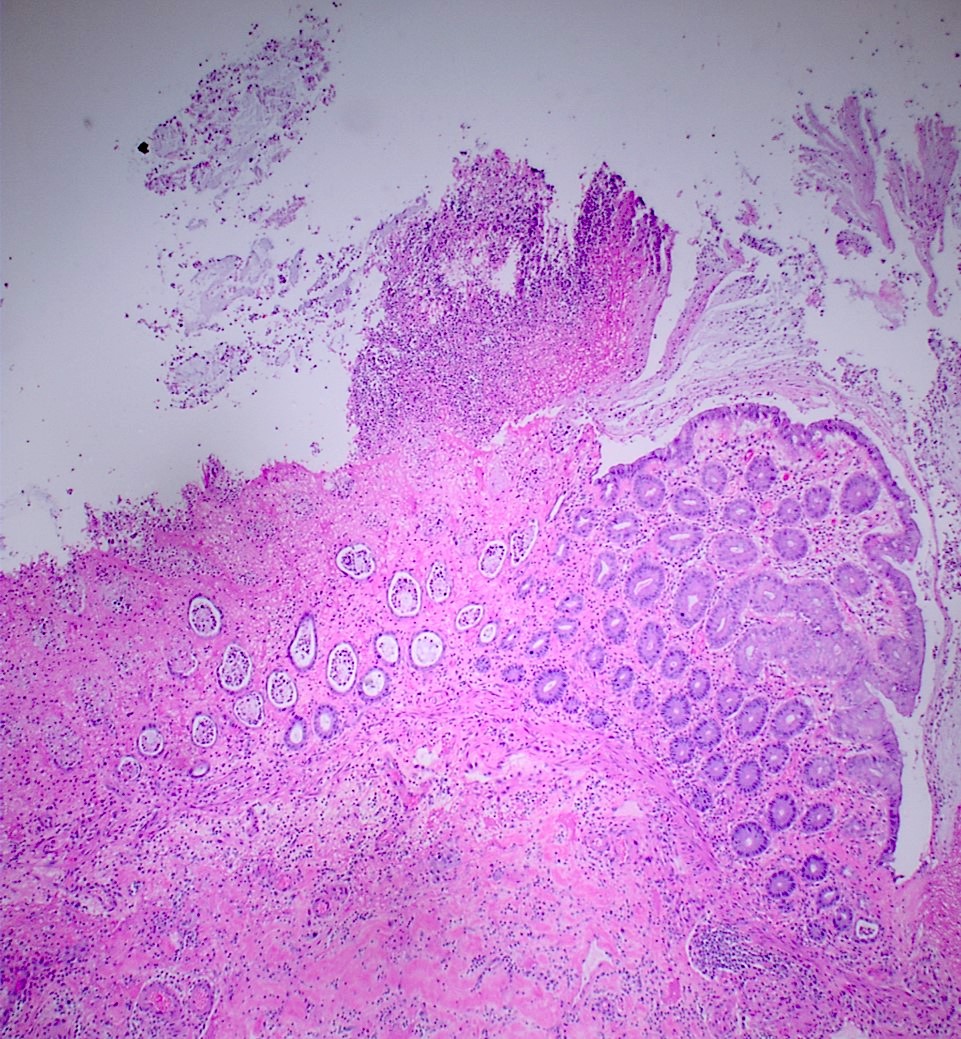
Ischemic changes
Sample pathology report
- Colon, biopsy:
- Colonic mucosa with changes consistent with ischemic type mucosal injury / colitis (see comment)
- Comment: Possible etiologies for this ischemic type mucosal injury include true ischemic colitis, infection (such as E. coli 0157:H7) and a drug reaction (including oral contraceptives, NSAIDs, digoxin and ergotamine derivatives). Clinical and endoscopic correlation is recommended.
- Colon, colectomy:
- Ischemic colitis with transmural necrosis / hemorrhage / perforation
- The resection margins are viable.
Differential diagnosis
- Drug / medication related injury:
- Ischemic pattern of injury in young adults and involvement of nonwatershed areas should raise the possibility of drug induced injury
- Drugs / medication related ischemic type injury (Arch Pathol Lab Med 2016;140:748)
- Characterized by eosinophilic, lymphocytic and granulocytic infiltration (World J Gastroenterol 2019;25:967)
- Increased intraepithelial apoptosis (mycophenolate mofetil)
- Fragments of resins in cases associated with kayexalate or bile acid squestrants
- Common drugs: oral contraceptives, cocaine, ergotamine derivatives, sumatriptan, kayexalate, cholestyramine
- Crohn's disease:
- Often younger patients
- Transmural inflammation, lymphoid aggregates
- No necrosis
- Granulomas
- Infectious colitis:
- Occurs in epidemiological clusters
- Younger patients
- Children, elderly and immunocompromised are susceptible
- Bacterial colitis is the most common cause
- Pseudomembranous colitis is caused by Clostridium difficile (Am J Surg Pathol 1997;21:706):
- Typically, history of use of antibiotics such as vancomycin is present and useful in raising a clinical suspicion of C. difficile colitis; stool antigen testing for presence of C. difficile toxin is confirmatory
- Presence of pseudomembranes is usually more widespread in the colon in infectious etiologies and more segmental in ischemia
- Hyalinization of lamina propria and specific vascular pathology are usually absent in C. difficile colitis
- Crypt atrophy, lamina propria hemorrhage and full thickness mucosal atrophy favor a diagnosis of ischemia over C. difficile (Am J Surg Pathol 1997;21:706)
- Ulcerative colitis:
- Often younger patients
- Cryptitis and crypt abscesses
- Basal plasmacytosis
- No fibrosis of lamina propria
- No hemosiderin deposition
Board review style question #1
A 62 year old woman, status post coronary artery bypass graft, complains of abdominal pain and bloody stools. A CT scan is performed, which shows significant thickening of the colon wall. Biopsy is performed, which shows changes consistent with ischemic colitis. What is the most common site of ischemic colitis?
- Ascending colon
- Cecum
- Hepatic flexure
- Rectum
- Splenic flexure
Board review style answer #1
Board review style question #2
A 73 year old woman presents with severe abdominal pain and a recent history of passing bloody stools. The pain began about 3 days ago and is more concentrated at the left side of the abdomen. Physical examination shows decreased to absent bowel sounds, abdominal distention and diffuse tenderness to palpation over her abdomen. An Xray is performed, which shows thumbprinting of the colon. What is the most likely histologic change seen in biopsy of the colon in patients with ischemic colitis?
- Crypt abscess with granulomas
- Increased lamina propria eosinophils
- Necrotizing vasculitis, fibrin thrombi and lamina propria hyalinization
- Pseudomembrane formation
Board review style answer #2
C. Necrotizing vasculitis, fibrin thrombi and lamina propria hyalinization
Comment Here
Reference: Ischemic colitis
Comment Here
Reference: Ischemic colitis
