
CNS & pituitary tumors
Other tumors
Melanocytic tumors / melanoma
Author: Jesse L. Kresak, M.D.

Last author update: 1 September 2014
Last staff update: 1 April 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: "CNS melanoma"

Table of Contents
Definition / general | Sites | Clinical features | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology images | Positive stains | Negative stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Kresak JL. Melanocytic tumors / melanoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnstumormelanocytictumor.html. Accessed April 1st, 2025.
Definition / general
- Melanocytes are a normal yet sparse cell of the leptomeninges, most often seen over the anterior / lateral cord, brainstem, base of brain
- Can give rise to rare primary intracranial melanocytic tumors
- WHO recognizes three categories of primary CNS melanocytic lesions: diffuse melanocytosis, melanocytoma, malignant melanoma
- Diffuse melanocytosis: strongly associated with neurocutaneous melanosis, a rare congenital syndrome with giant congenital pigmented skin nevi and high rate of CNS melanoma usually presenting before age 2 (Semin Cutan Med Surg 2004;23:138)
- Melanocytoma: less than 0.1% of brain tumors, arises at any age
- Melanoma: incidence of 0.005 cases per 100,000; reported in ages 15 - 71 with a peak in the fourth and fifth decade
Sites
- Diffuse melanocytosis can involve infra or supratentorial leptomeninges but has highest frequency in cerebellum, brain stem, temporal lobes
- Involves subarachnoid space and superficial cortex
- Melanocytomas can occur in any area of meninges; however, have a predilection for cervical and thoracic spinal cord (intradural, extramedullary) and Meckel cave
- Melanomas can also occur anywhere within meninges but have predilection for spinal cord, posterior fossa, Meckel cave
Clinical features
- Diffuse melanocytosis presents most commonly with features of neurocutaneous melanosis - congenital nevi, hydrocephalus, mass effect and neuropsychiatric symptoms
- Melanocytoma and melanoma present with mass effect / cord compression symptoms
Radiology images
Images hosted on other servers:

Diffuse melanocytosis

MRI of thoracic area

Abnormal signal in the left temporal lobe
Prognostic factors
- Diffuse melanocytosis: poor prognosis even when histologically benign
- Melanocytoma: good prognosis with resection, rarely transforms into malignant melanoma
- Can be called intermediate grade when Ki67 and mitoses are present but no obvious melanoma
- Malignant melanoma: poor prognosis (6 years in spine) yet better than metastatic melanoma to CNS (6 months) (J Neurosurg 1987;66:47)
Case reports
- 11 year old girl with malignant blue nevus of ear associated with two intracranial melanocytic tumors (Hum Pathol 2004;35:1292)
- 29 year old man with primary cerebellopontine angle melanoma (Turk Neurosurg 2012;22:469)
- 34 year old woman with primary spinal cord melanoma (J Korean Neurosurg Soc 2010;48:157)
- 35 year old woman with intermediate grade melanocytoma (University of Pittsburgh: A 35 Year Old Woman with Progressive Bilateral Leg Weakness)
- 37 year old woman with leptomeningeal metastases from a primary CNS melanoma (World J Surg Oncol 2014;12:265)
- 48 year old woman with intraventricular melanoma (AJNR Am J Neuroradiol 1999;20:691)
- 57 year old man with leptomeningeal and liver tumors consistent with melanocytoma (University of Pittsburgh: A 57 Year Old Male with Leptomeningeal and Liver Tumors)
- Spectrum of CNS abnormalities in neurocutaneous melanocytosis (Dev Med Child Neurol 2012;54:563)
Treatment
- Gross total resection
- Adjuvant chemoradiation therapy for malignant melanoma
Gross description
- Usually solitary, well demarcated, dural based with black or reddish brown discoloration
Microscopic (histologic) description
- Melanocytoma:
- Solitary, circumscribed lesions - do not invade adjacent structures
- Nests (reminiscent of whorls) of relatively uniform cells with variable melanin pigment
- Bland, oval nuclei with eosinophilic nucleoli
- Mitoses no more than 1/10 HPF
- Malignant melanoma:
- Hypercellular sheets or nests of spindled or epithelioid cells
- May have significant pleomorphism
- Atypical mitoses (5/10 HPF)
- Invasion of adjacent structures or necrosis may be seen
- Prominent nucleoli
Microscopic (histologic) images
Contributed by Rana Al-Zaidi, M.B.B.S.
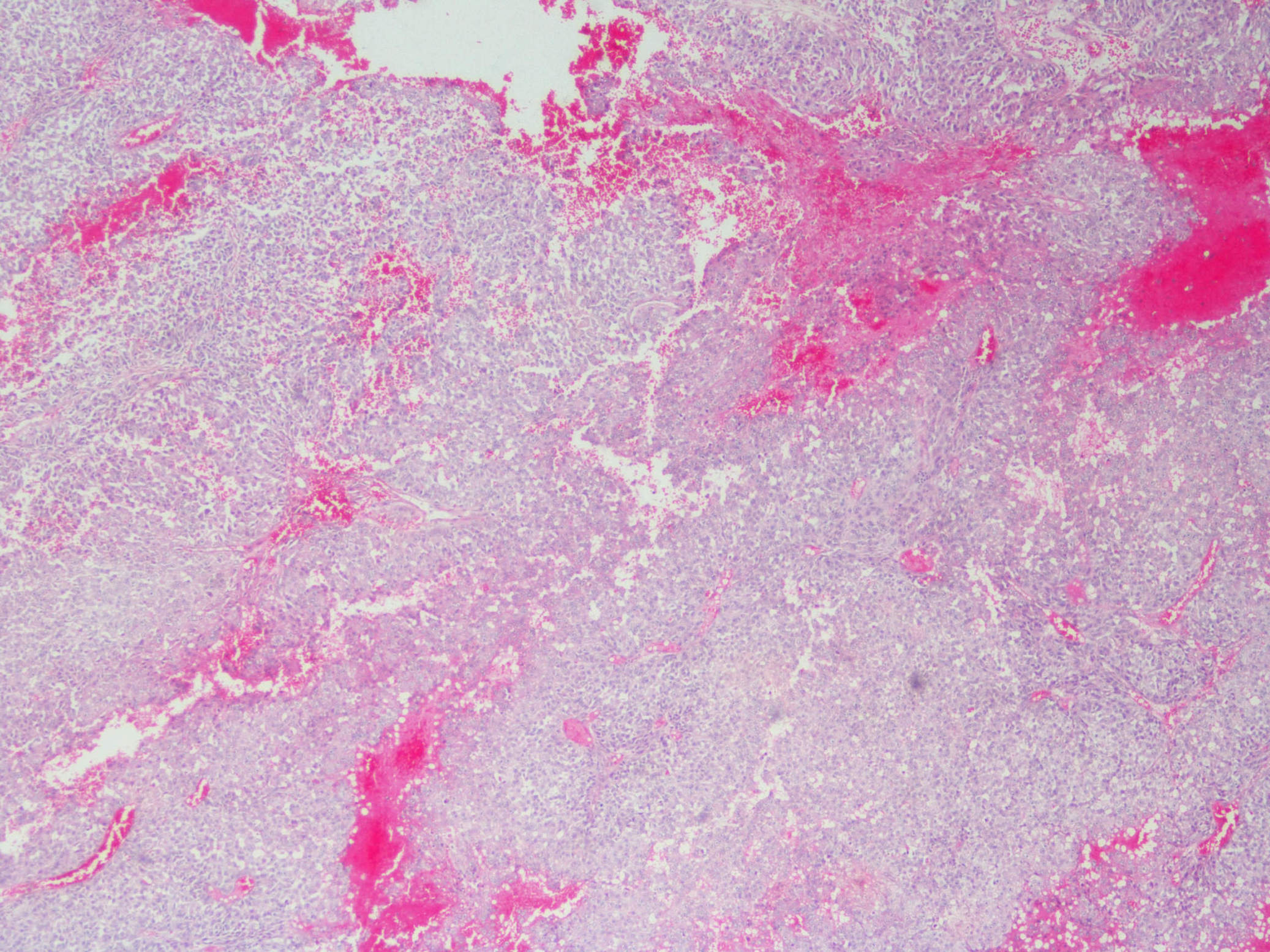
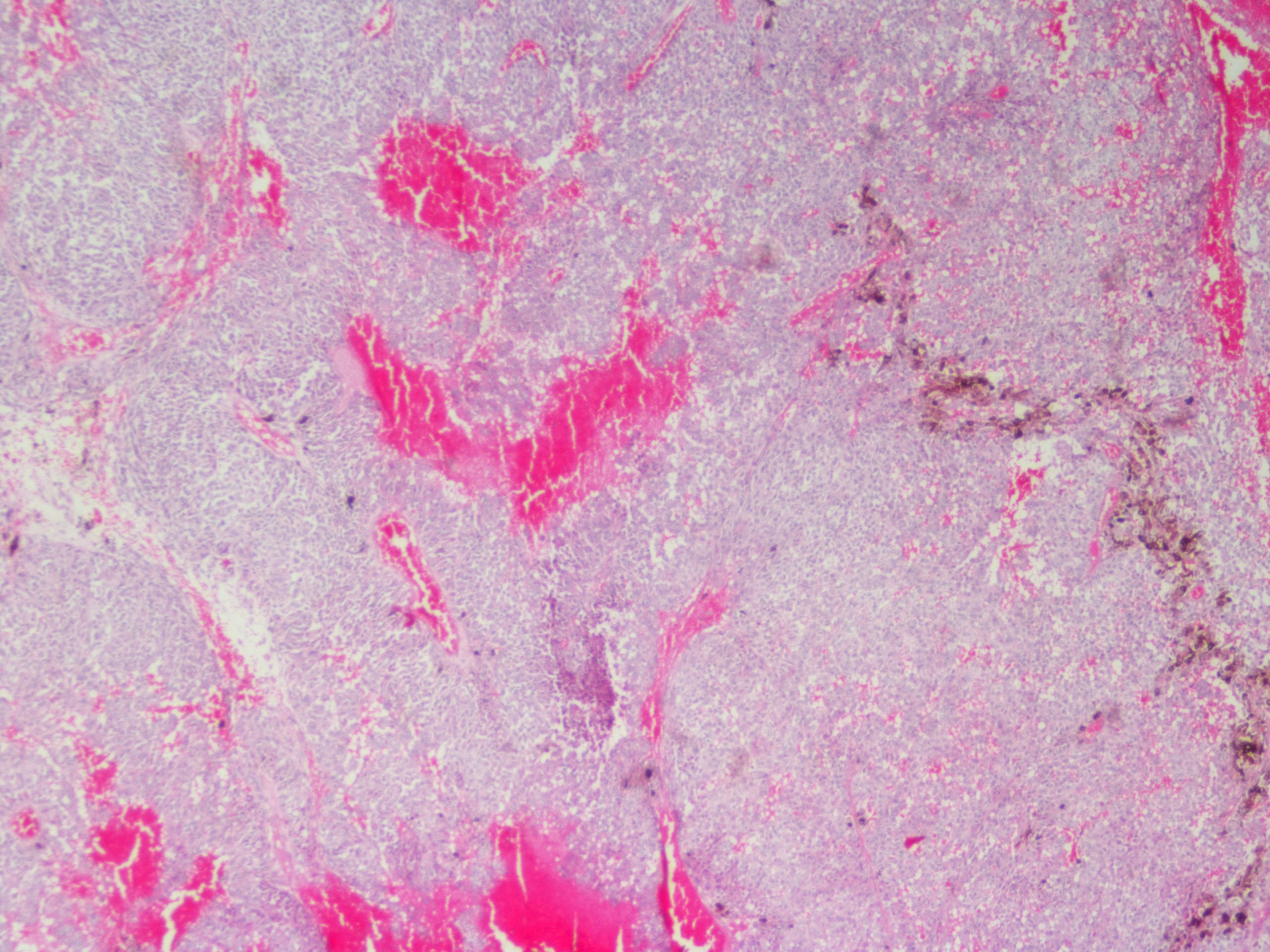

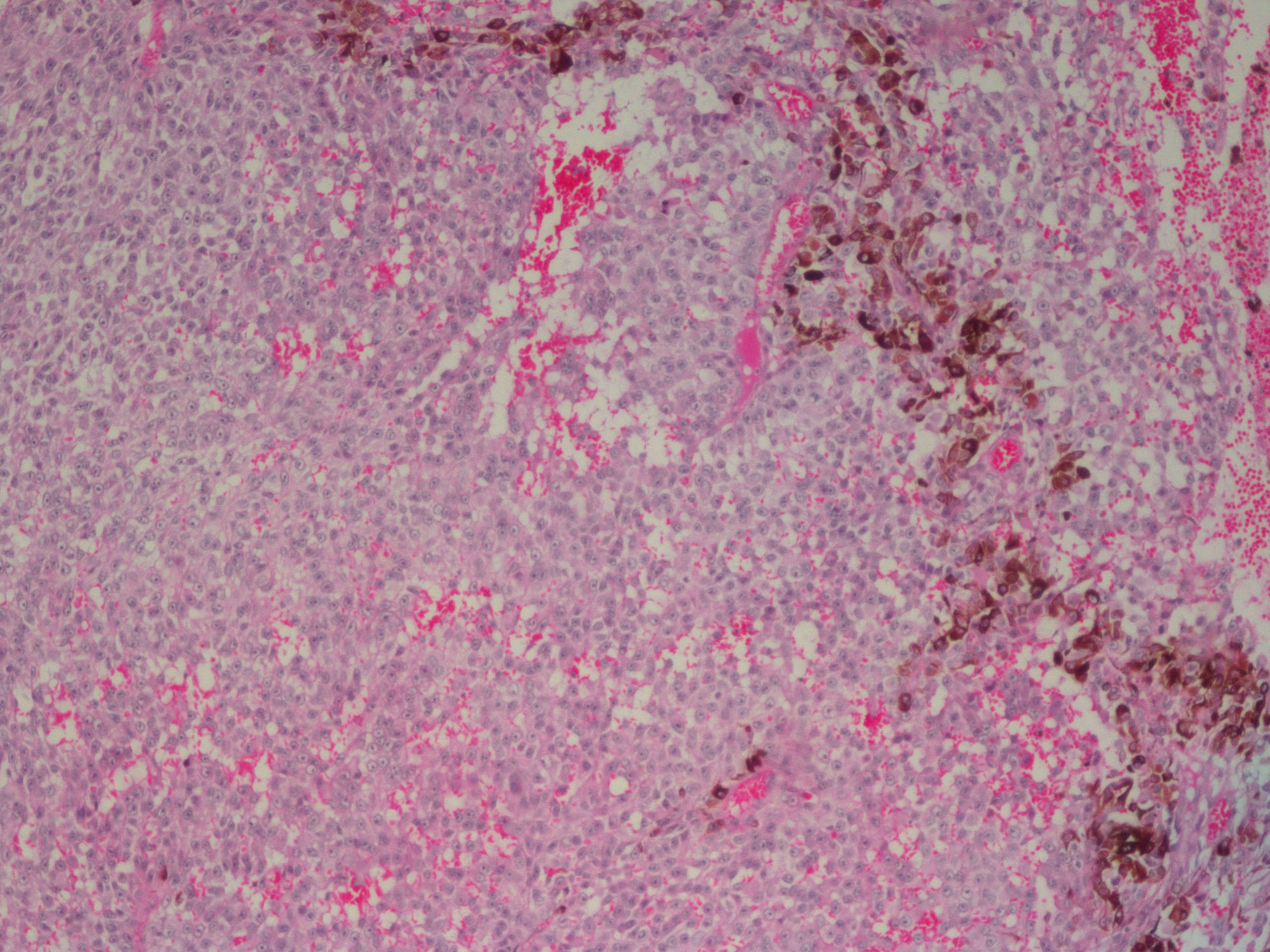
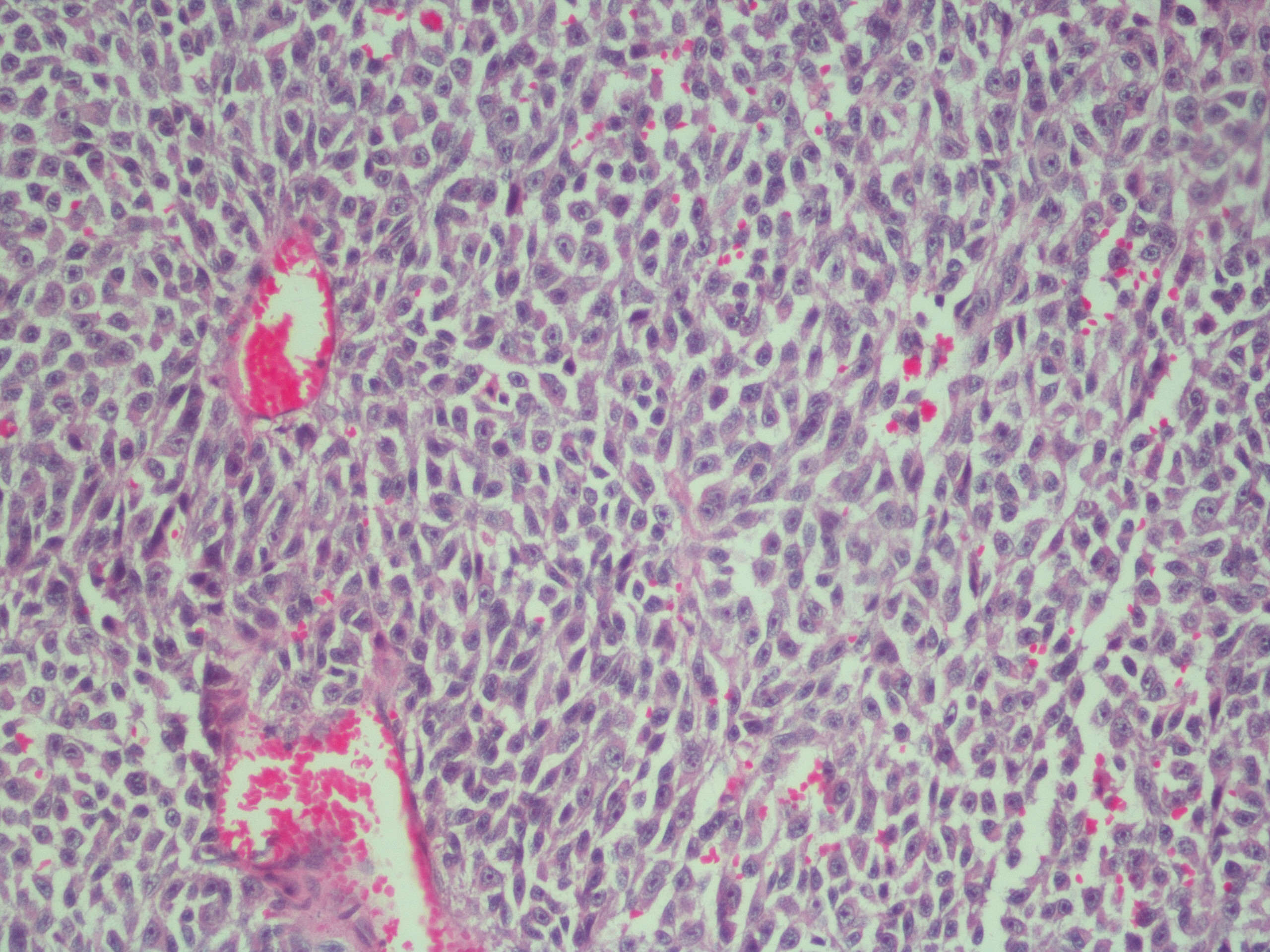
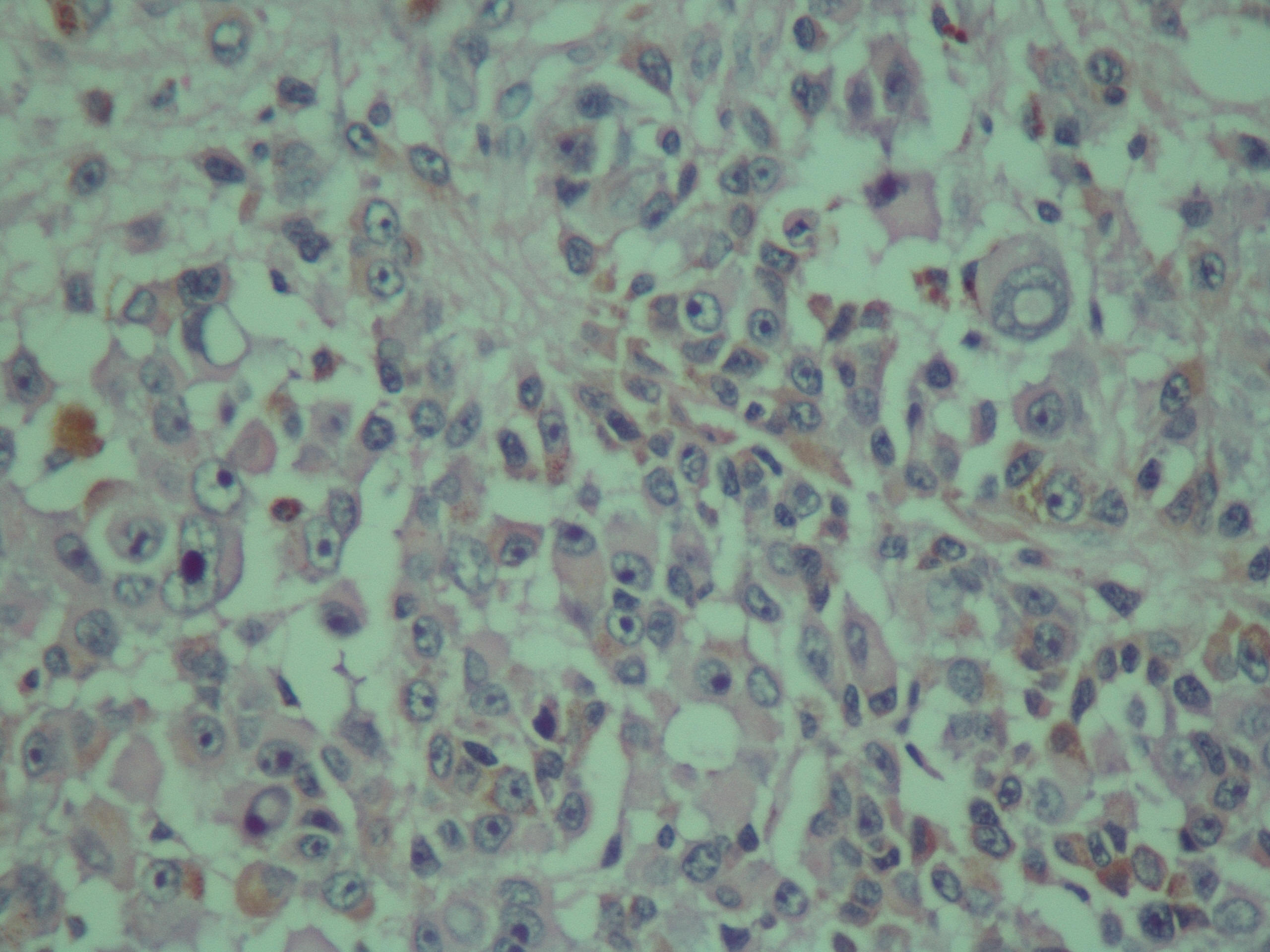
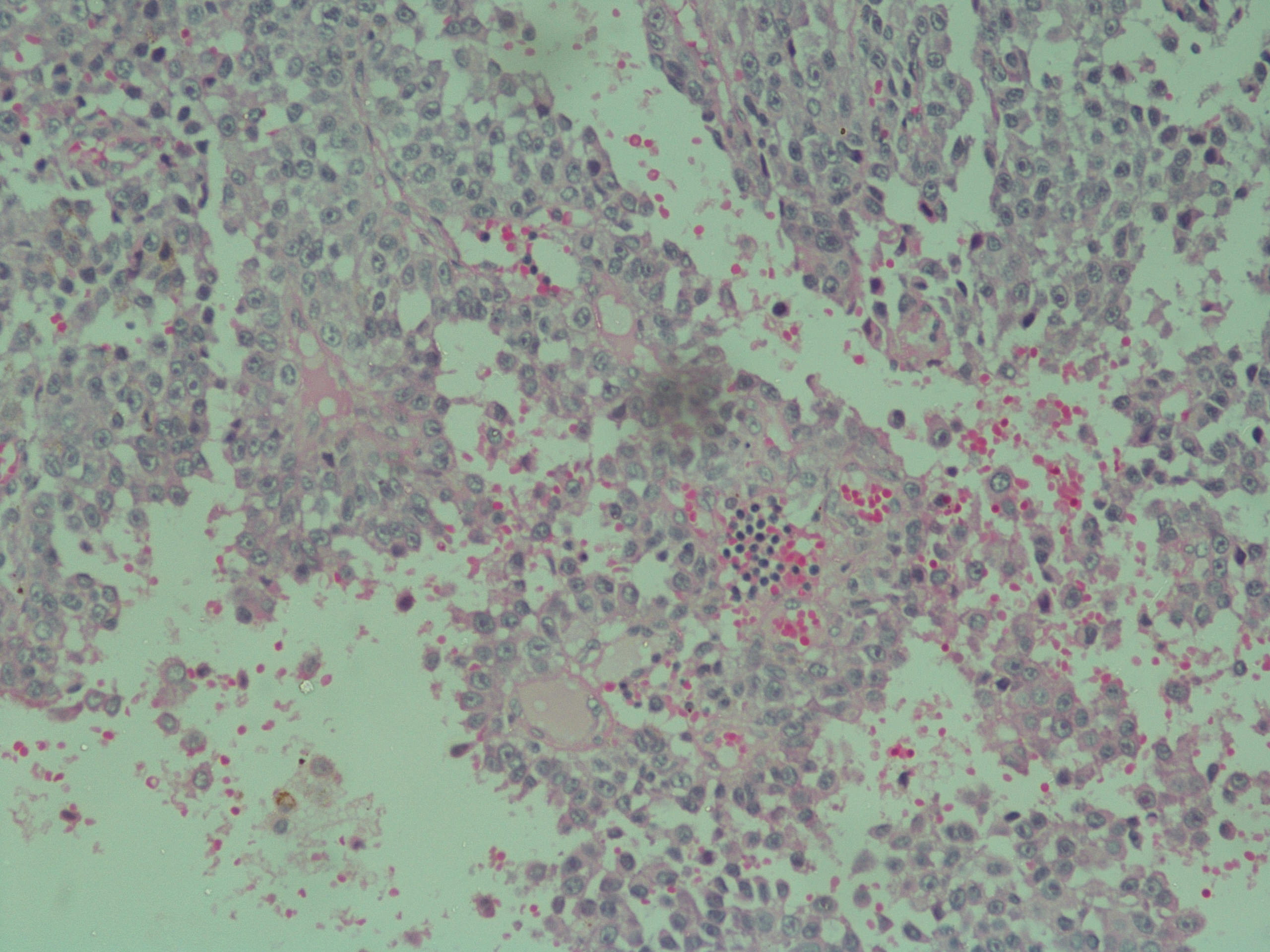
55 year old man with nausea, vomiting and sudden loss of consciousness and 4 cm temporal lesion - primary CNS melanoma
Contributed by Jesse Kresak, M.D.
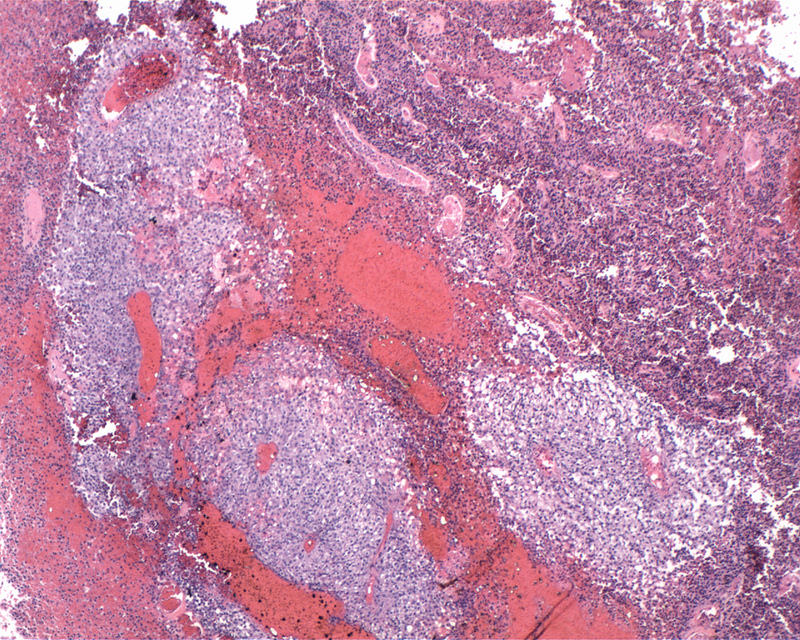
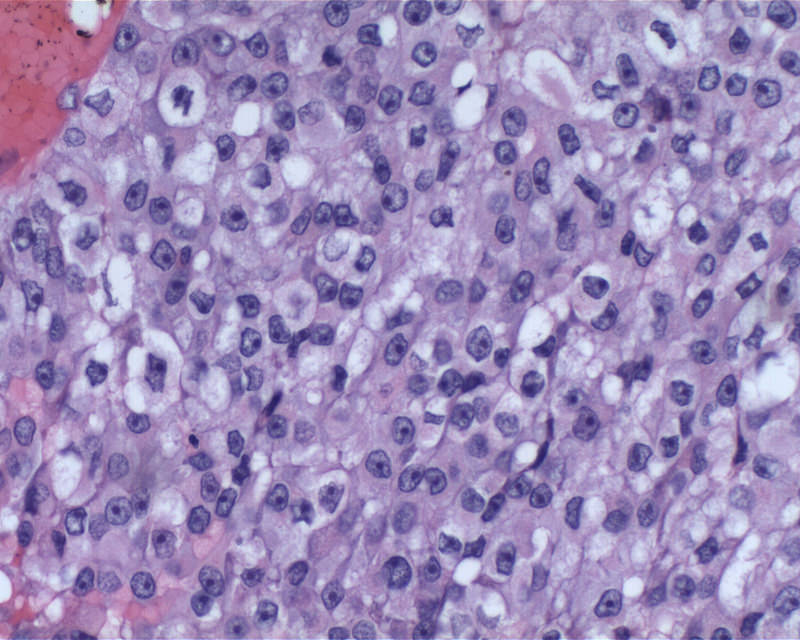
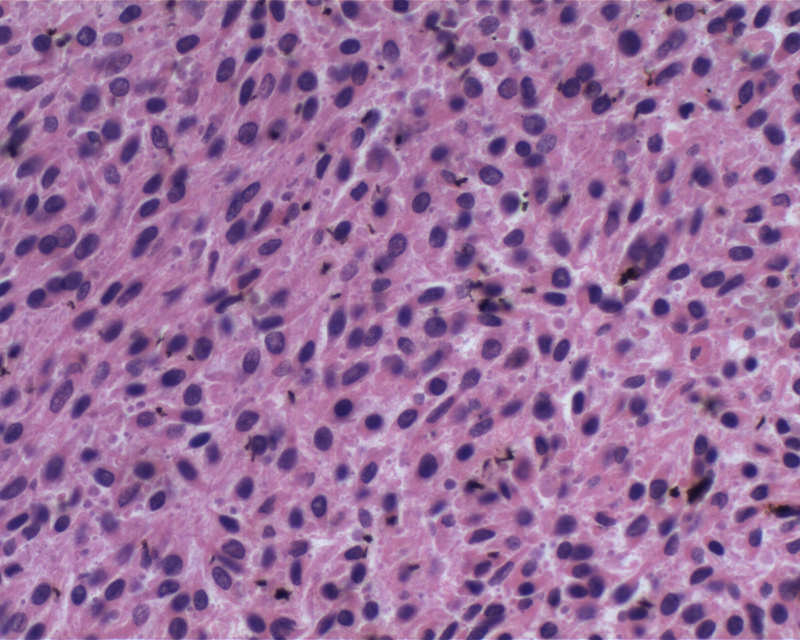
Melanocytoma
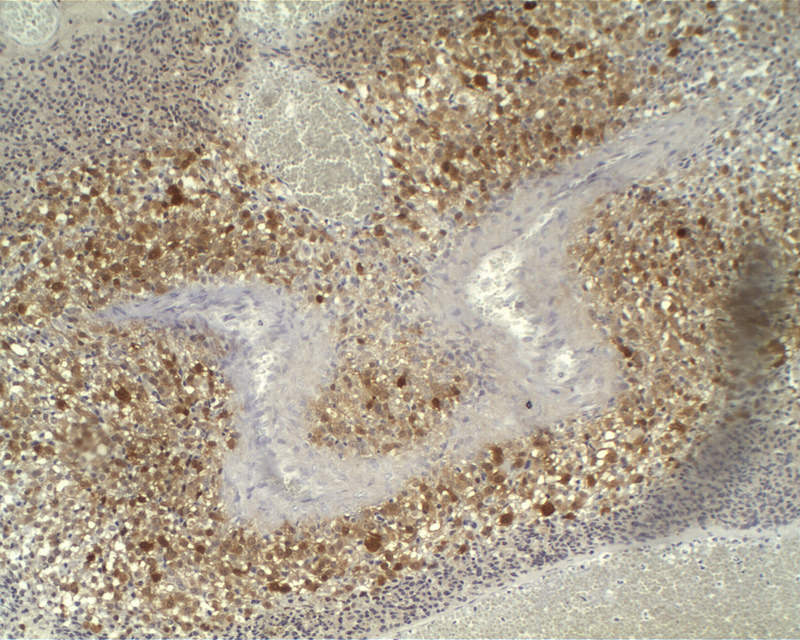
Melanocytoma: S100
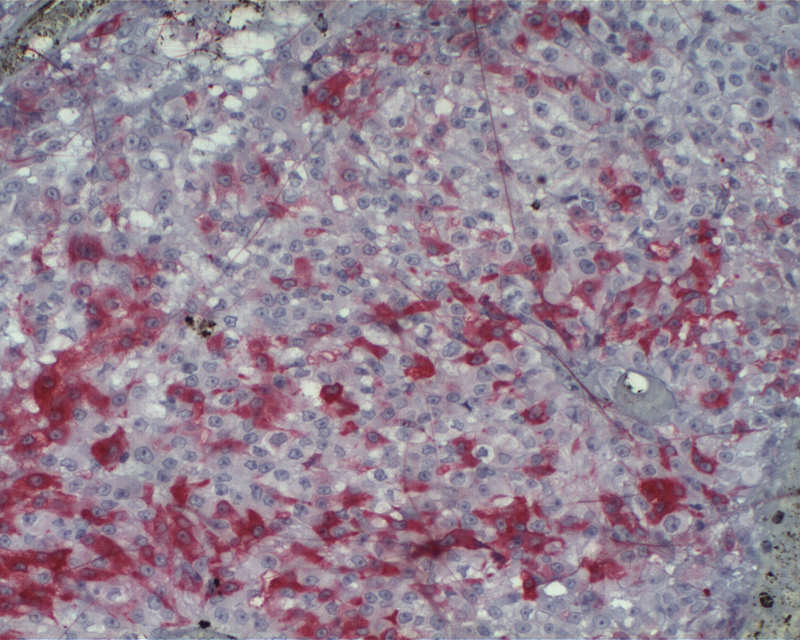
Melanocytoma: MelanA

Melanocytoma: HMB45
Cytology images
Images hosted on other servers:

Melanoma cells in CSF
Electron microscopy description
- Melanosomes present, no junctions, no desmosomes
Differential diagnosis
- Melanocytic schwannoma
- Metastatic melanoma
Additional references
