
CNS & pituitary tumors
Cysts
Neuroectodermal cysts
Author: Saman Seyed Ahmadian, M.D.
Editorial Board Member: Jared T. Ahrendsen, M.D., Ph.D.
Deputy Editor-in-Chief: Chunyu Cai, M.D., Ph.D.
Last author update: 25 May 2023
Last staff update: 3 March 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: CNS arachnoid cyst

Table of Contents
Arachnoid cyst | Choroid plexus cyst | Glioependymal / ependymal cyst | Board review style question #1 | Board review style answer #1Cite this page: Ahmadian SS. Neuroectodermal cysts. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnstumorneuroectodermalcyst.html. Accessed March 31st, 2025.
Arachnoid cyst
Definition / general
Essential features
Terminology
ICD coding
Epidemiology
Sites
Pathophysiology
Clinical features
Diagnosis
Radiology description
Radiology images
Contributed by Saman Seyed Ahmadian, M.D.

Images hosted on other servers:

Case reports
Treatment
Gross description
Microscopic (histologic) description
Microscopic (histologic) images
Contributed by Saman Seyed Ahmadian, M.D.
Virtual slides
Images hosted on other servers:

Positive stains
Negative stains
Electron microscopy description
Molecular / cytogenetics description
Sample pathology report
Differential diagnosis
Additional references
- Arachnoid cysts are nonneoplastic, intracranial cerebrospinal fluid (CSF) filled spaces lined with arachnoid membranes (Cureus 2018;10:e2458)
- 1% of intracranial masses (Neurosurgery 1997;41:951)
Essential features
- Nonneoplastic, intracranial CSF filled spaces lined by meningothelial cells and an outer collagenous membrane
- Most primary developmental arachnoid cysts occur in the middle frontal fossa due to the splitting of arachnoid membranes (J Neuropathol Exp Neurol 1981;40:61)
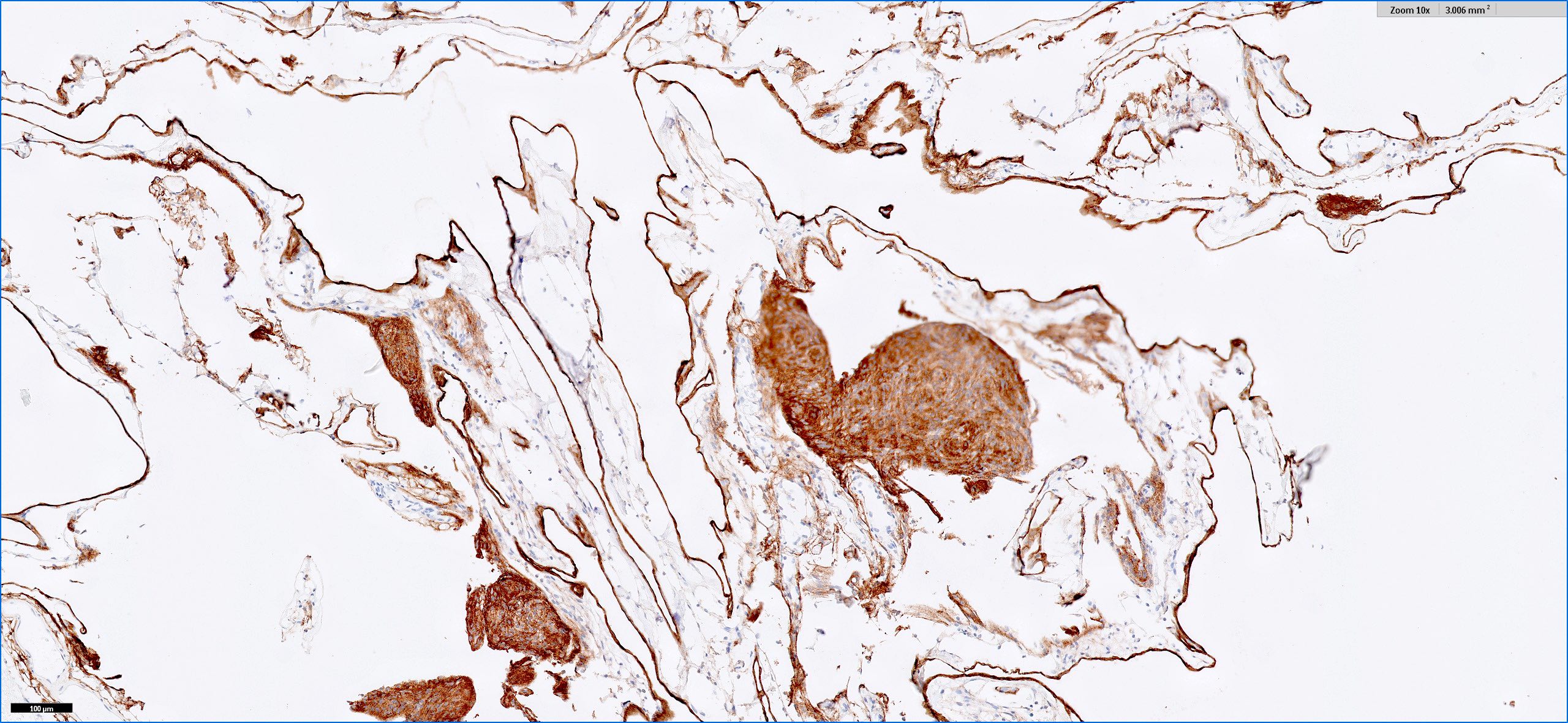
- Meningothelial cells are positive for epithelial membrane antigen (EMA)
Terminology
- Meningeal cyst
ICD coding
Epidemiology
- Arachnoid cysts are classified as primary developmental cysts or secondary cysts (Cureus 2018;10:e2458)
- 50 - 65% of primary developmental cysts present in the middle cranial fossa / Sylvian fissure (Pediatr Neurosurg 1996;25:165)
- Arachnoid cysts in the middle cranial fossa are found more frequently in men than in women (Pediatr Neurosurg 1996;25:165)
Sites
- Arise within both cranial and spinal meninges
- Most are supratentorial and found in the middle fossa (J Neurosurg 2013;118:222)
- Other sites include retrocerebellar, convexity, cerebellopontine angle and spinal cord (J Neurosurg 2013;118:222)
Pathophysiology
- Primary developmental cysts occur due to the splitting of arachnoid membranes in utero, resulting in abnormal collections of cerebrospinal fluid (CSF) (J Neuropathol Exp Neurol 1981;40:61)
- Secondary cysts are less common and often occur after trauma, infection or surgery (Case Rep Orthop 2015;2015:250710)
- Mutation of the FOXC2 gene has been reported in familial forms
Clinical features
- Depends on size and location
- Headaches are the most common symptom (J Neurol Neurosurg Psychiatry 2007;78:1129)
- Other symptoms include hydrocephalus, intracranial hypertension, dizziness, nausea, vomiting, mental status changes, ataxia, seizures and hearing loss (Childs Nerv Syst 2015;31:77)
- Arachnoid cysts can be asymptomatic (Childs Nerv Syst 2015;31:77)
Diagnosis
- Computed tomography (CT) and magnetic resonance imaging (MRI) for radiologic assessment
- Surgical resection is required for a definitive diagnosis
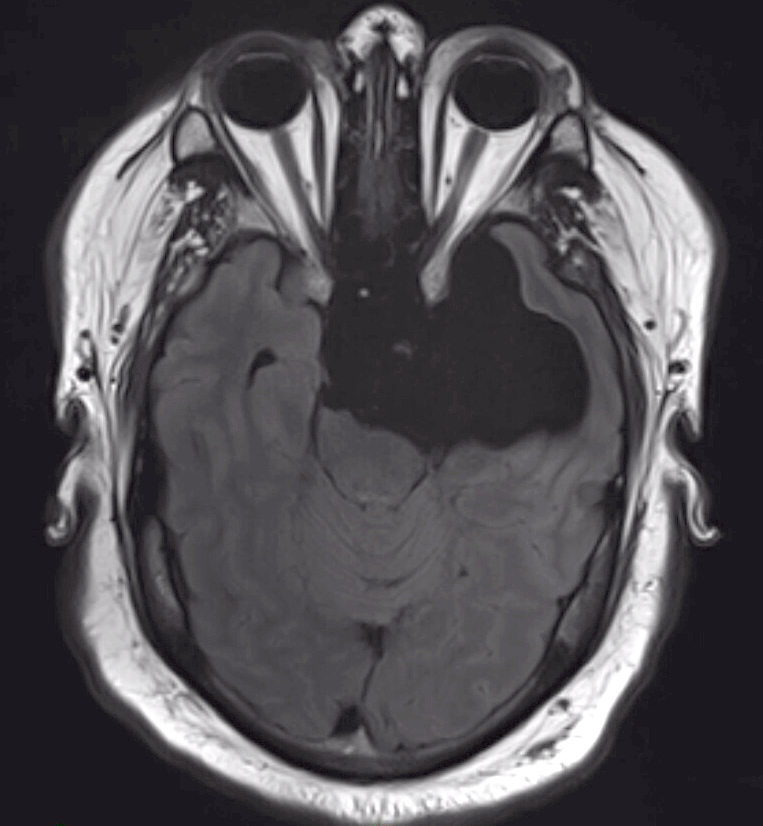
Radiology description
- MRI is the diagnostic procedure of choice
- Arachnoid cysts show low signal intensity on diffusion weighted imaging (DWI) and fluid attenuated inversion recovery (FLAIR) (Tani Girisim Radyol 2003;9:418)
- No enhancement
Radiology images
Contributed by Saman Seyed Ahmadian, M.D.
T2 FLAIR MRI
T2 MRI
Images hosted on other servers:
T2 MRI
Case reports
- 22 year old man with a spinal epidural arachnoid cyst (Case Rep Orthop 2015;2015:250710)
- 36 year old woman with a well delineated cystic sellar lesion with suprasellar extension (Einstein (Sao Paulo) 2019;17:eAI4269)
- 45 year old woman with a pontomedullary junction arachnoid cyst (Asian J Neurosurg 2022;17:389)
Treatment
- Surgery if symptomatic
Gross description
- Variable in size; can be very large with mass effects
- Thin, transparent wall with a clear, colorless fluid
- Cyst is distinct from leptomeninges and dura
- Reference: Love: Greenfield's Neuropathology, 9th Edition, 2015
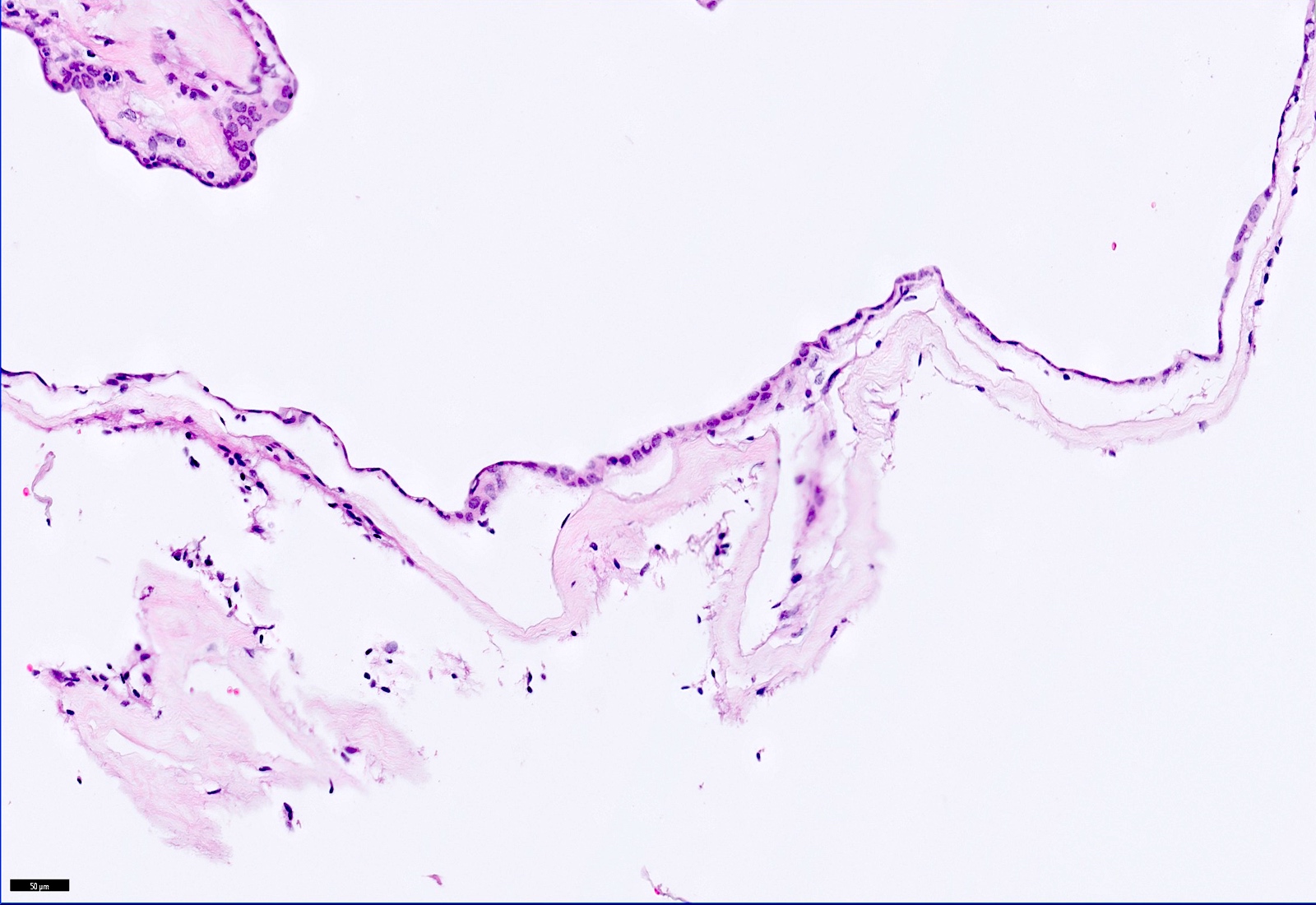
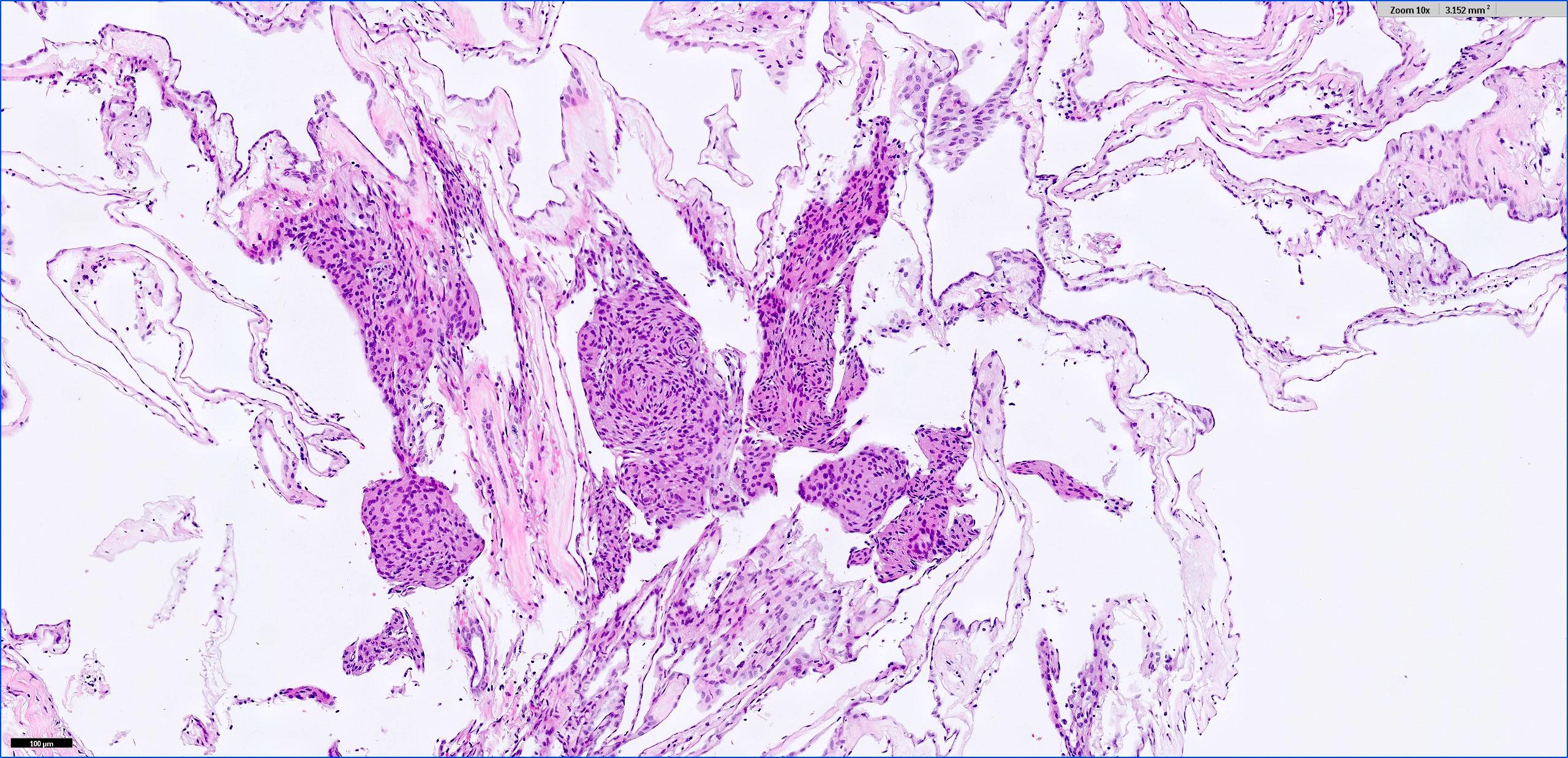
Microscopic (histologic) description
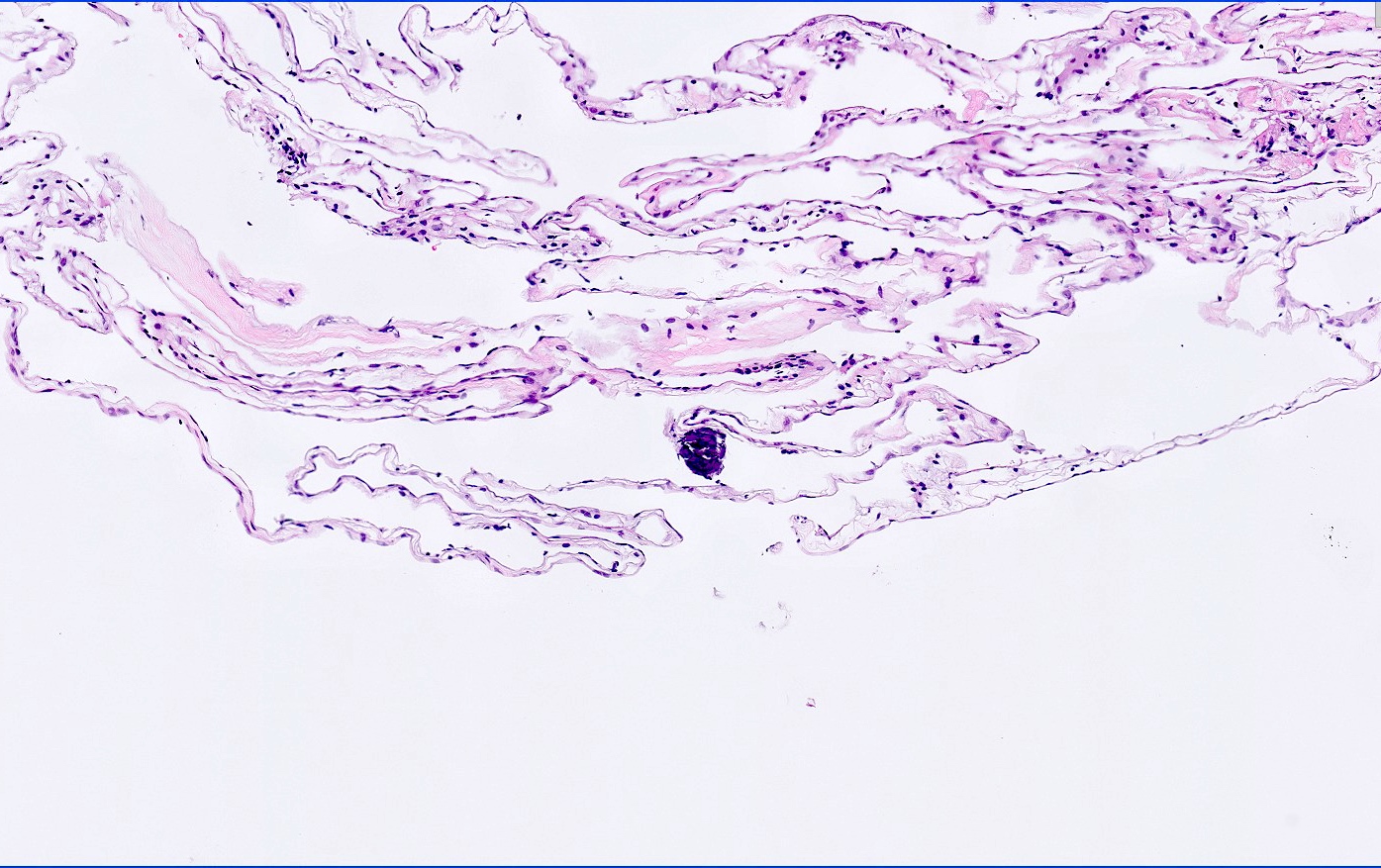
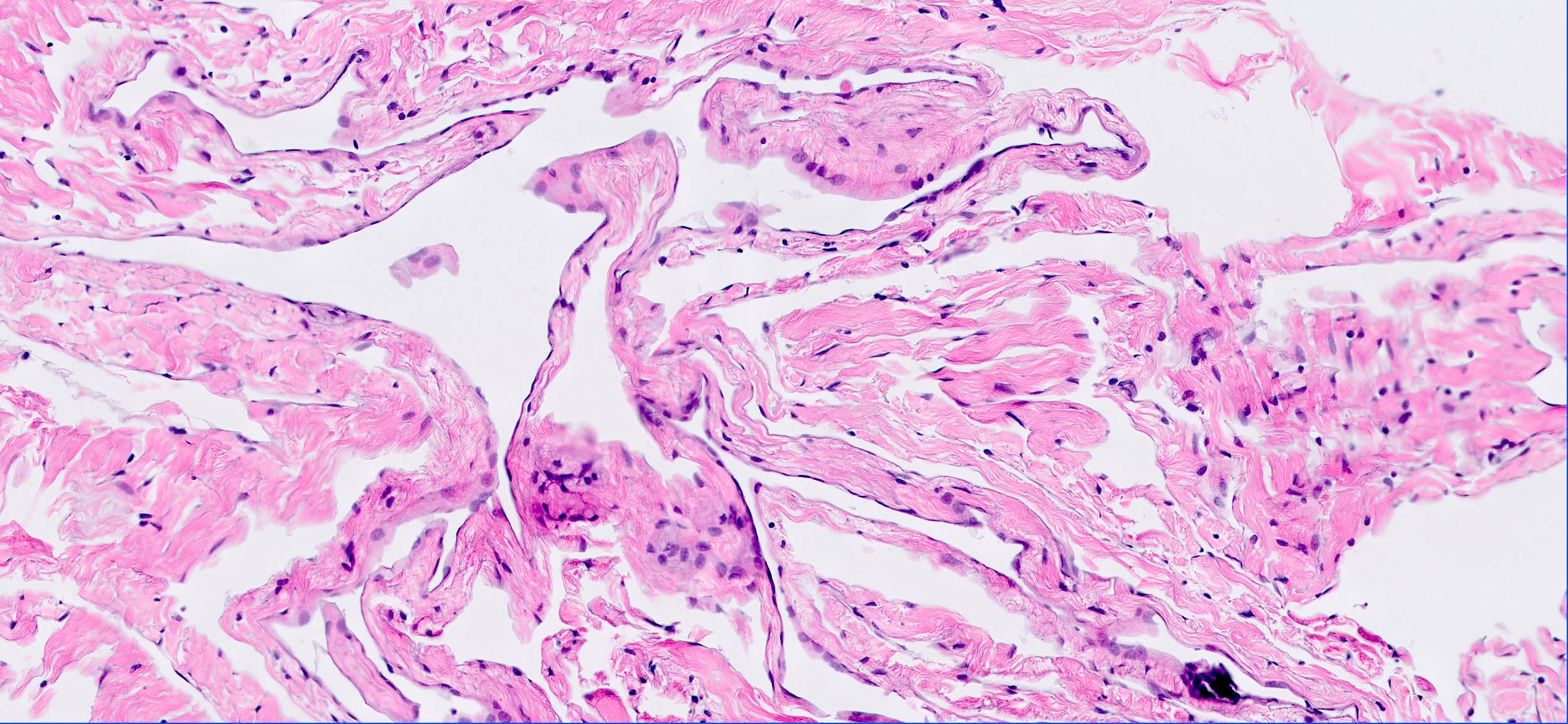
- Cyst wall is composed of a single layer of meningothelial cells and an outer collagenous membrane
- Meningothelial cells often partially denuded and may not always be recognizable
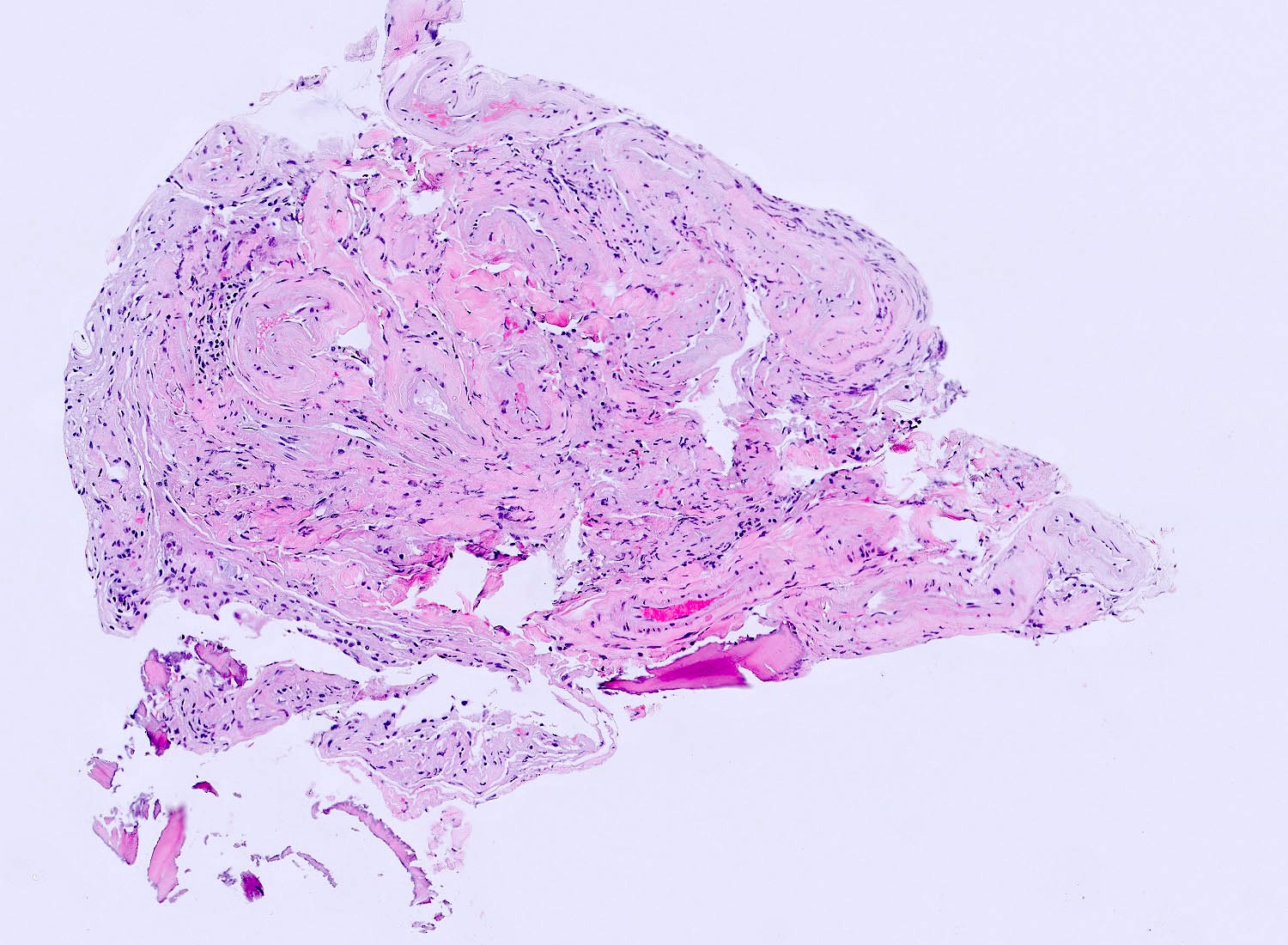
- Rare foci of meningothelial hyperplasia with or without psammoma bodies
- Focal inflammation (rare)
- Reference: Love: Greenfield's Neuropathology, 9th Edition, 2015
Microscopic (histologic) images
Contributed by Saman Seyed Ahmadian, M.D.
Cyst lining
Meningothelial hyperplasia
Calcification
No apparent meningothelial cells
EMA
Virtual slides
Images hosted on other servers:
Arachnoid cyst, resection
Positive stains
- Meningothelial cells are positive for EMA
Negative stains
- Cytokeratin, GFAP, transthyretin and synaptophysin
Electron microscopy description
- Tendency of meningothelial tissues to cleave along the dura arachnoid interface layer (J Neuropathol Exp Neurol 1979;38:434)
Molecular / cytogenetics description
- Mutation of the FOXC2 gene has been reported in familial forms (PLoS One 2013;8:e80548)
Sample pathology report
- Cyst wall, excision:
- Arachnoid cyst (see comment)
- Comment: The histologic section shows a cystic lesion composed of a single layer of meningothelial cells with an outer layer of delicate fibrous tissue. The meningothelial cells are positive for EMA by immunohistochemistry, which confirms the diagnosis.
Differential diagnosis
- Epidermoid cyst:
- Squamous cyst lining
- Lamellar keratin debris
- Positive for keratin
- Endodermal cyst:
- Pseudostratified epithelium cyst lining with bronchogenic (ciliated) or gastrointestinal (glands) differentiation
- Positive for keratin
- Ependymal cyst:
Additional references
Choroid plexus cyst
Definition / general
Sites
Clinical features
Radiology description
Radiology images
Images hosted on other servers:

Case reports
Clinical images
Images hosted on other servers:

Microscopic (histologic) description
Positive stains
Negative stains
- Small cyst of choroid plexus containing CSF
Sites
- May be present throughout ventricular system but usually in glomus of lateral ventricles
Clinical features
- More prevalent in fetuses with chromosomal abnormalities (trisomy 18, trisomy 21, Aicardi syndrome)
- Common form affect fetuses in 1% of pregnancies; usually asymptomatic, resolves spontaneously by birth but large cysts can cause hydrocephalus
- Chromosomal abnormalities, specifically trisomy 18, should be considered if cysts are large ( > 1 cm), bilateral or irregular or if maternal age ≥ 32 years (AJR Am J Roentgenol 2009;192:32)
- In adults, usually asymptomatic, incidental postmortem finding
Radiology description
- On CT and MRI, usually show CSF density
Radiology images
Images hosted on other servers:
MR shows small cyst
Case reports
- 20 week male fetus without any chromosomal abnormality (AJR Am J Roentgenol 2009;192:32)
- 53 year old woman with small lesion at foramen of Monro (Am J Neuroradiology 2002;23:841)
Clinical images
Images hosted on other servers:
Cyst at foramen of Monro
Microscopic (histologic) description
- Cyst wall lined by cuboidal to columnar epithelium with occasional cobblestone appearance typical of normal choroid plexus
- Some are devoid of epithelial lining
Positive stains
- Cyst lining has same immunohistochemical profile as normal choroid plexus: positive for vimentin, cytokeratin, S100, transthyretin, synaptophysin
Negative stains
Glioependymal / ependymal cyst
Definition / general
Radiology images
Images hosted on other servers:

Case reports
Gross description
Gross images
Images hosted on other servers:

Microscopic (histologic) description
Positive stains
Negative stains
Electron microscopy description
Differential diagnosis
- Rare, benign intraparenchymal and often paraventricular cyst lined by simple epithelium or glial tissue, S100+ or GFAP+, resting on neuroglia (J Neuroradiol 1995;22:48)
- Usually intracranial, not midline but may affect spinal cord; may affect adult cerebellum or represent burned out pilocytic astrocytoma
- Not in communication with ventricle or CSF spaces
- Rarely ruptures and causes meningitis
- Cyst lined by glial tissue
Radiology images
Images hosted on other servers:

MR: cystic lesion of right frontal lobe
Case reports
- 15 year old boy with recurrent intramedullary cyst at C2-C3 (Neurol India 2003;51:111)
- 19 year old woman with thalamic glial cyst causing hydrocephalus due to hemorrhage (Neurol Med Chir (Tokyo) 1997;37:284)
- 42 year old man with clinical symptoms of expansive cerebellar lesion (J Neuroradiol 2001;28:209)
Gross description
- Resembles arachnoid cyst
Gross images
Images hosted on other servers:

Ependymal cyst
Microscopic (histologic) description
- Simple columnar or cuboidal cells, often ciliated, resting on neuroglia; no fibrous capsule
- Alternatively, wall lined by gliosis, Rosenthal fibers present, variable hemosiderin; no epithelial lining
Positive stains
Negative stains
Electron microscopy description
- Neuroepithelial origin
Differential diagnosis
- Endodermal cyst:
- CK+
Board review style question #1
A 71 year old patient with altered mental status had a 7.6 cm cystic lesion in the left frontoparietal convexity. The cystic lesion was excised. What immunohistochemistry confirms the diagnosis?
- Cytokeratin
- EMA
- GFAP
- Synaptophysin
Board review style answer #1
B. EMA. The histologic section shows a cystic lesion with a single layer of meningothelial cells with flattened nuclei and delicate fibrous tissue suggestive of an arachnoid cyst. The meningothelial cells are positive for EMA.
Comment Here
Reference: Arachnoid cyst
Comment Here
Reference: Arachnoid cyst
