
CNS & pituitary tumors
Cysts
Colloid cyst
Author: Eman Abdelzaher, M.D., Ph.D.
Editorial Board Member: P.J. Cimino, M.D., Ph.D.
Deputy Editor-in-Chief: Chunyu Cai, M.D., Ph.D.

Last author update: 17 November 2023
Last staff update: 12 April 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Colloid cyst

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Abdelzaher E. Colloid cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnstumorcolloidcyst.html. Accessed March 31st, 2025.
Definition / general
- Benign, unilocular, epithelium lined, mucin filled cyst of third ventricle (eMedicine: Colloid Cysts [Accessed 31 October 2023])
- Uncertain histogenesis, mostly of endodermal derivation (Acta Neuropathol 1992;83:605)
- Site, radiologic and pathologic features are distinctive so differential diagnosis may be limited
Essential features
- Benign, unilocular, epithelium lined, mucin filled cyst of third ventricle (eMedicine: Colloid Cysts [Accessed 31 October 2023])
- Usually adults (20 - 50 years); rare in children
- Located at anterosuperior third ventricle near foramen of Monro
- Excellent prognosis
Terminology
- Colloid cyst of the third ventricle
ICD coding
- ICD-10: G93.0 - cerebral cysts
Epidemiology
- Rare, 0.5 - 2.0% of all intracranial lesions and 10 - 20% of all intraventricular lesions (World Neurosurg 2019:123:351)
- Usually adults (20 - 50 years), rare in children, no sex predilection (World Neurosurg 2017:107:409)
Sites
- Anterosuperior third ventricle near foramen of Monro, attached to the third ventricular roof and choroid plexus
- Unusual sites: septum pellucidum, fourth ventricle (Acta Neurochir (Wien) 2004;146:397, Clin Neurol Neurosurg 2012;114:1095)
Etiology
- Usually sporadic
- Genetic predisposition is suggested with limited reports of familial clusters (World Neurosurg 2017:107:409, Asian J Neurosurg 2020;15:414)
Diagrams / tables
Images hosted on other servers:

Mechanisms of sudden death due to colloid cyst

Typical location of colloid cyst
Clinical features
- Due to its position, causes intermittent obstruction of cerebrospinal fluid (CSF) flow and obstructive hydrocephalus with manifestations of increased intracranial pressure
- Headache is the most common symptom
- May also cause nausea, vomiting, blurred vision, gait disturbance, urinary incontinence and personality changes (BMC Neurol 2022;22:397)
- Sudden impaction (ball valve effect on the foramen of Monro) causes abrupt, transient lower limb paralysis (drop attacks) and rarely, sudden death (Emerg (Tehran) 2015;3:162)
- May be asymptomatic
Diagnosis
- Neuroimaging: computed tomography (CT) and magnetic resonance imaging (MRI)
- Biopsy
Radiology description
- Typical intraventricular location allows confident radiological diagnosis
- CT: unilocular hyperdense mass at or near the foramen of Monro (AJNR Am J Neuroradiol 2000;21:1470)
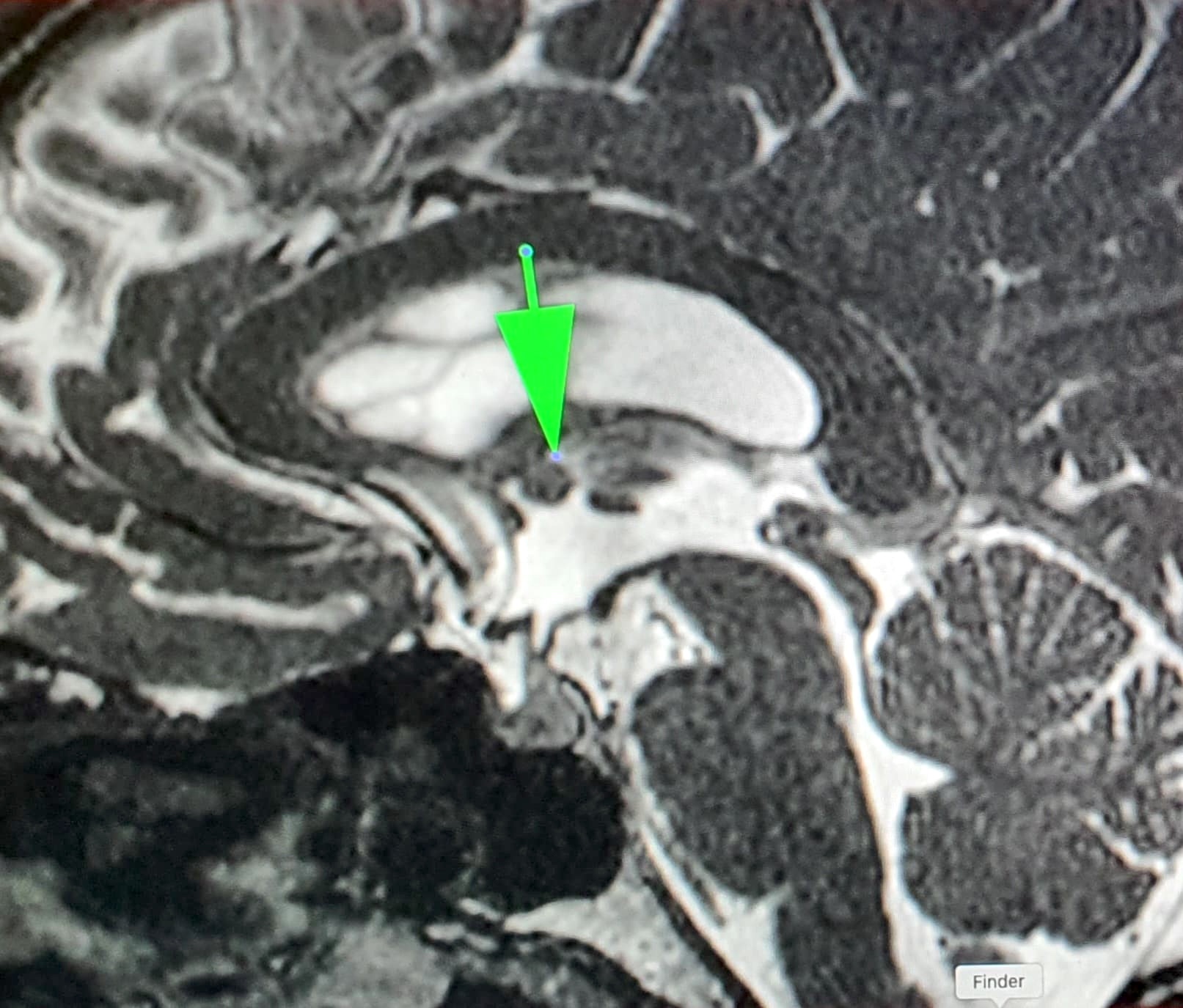
- MRI: spherical, usually nonenhancing, discrete cystic lesion at anterior third ventricle; most are intrinsically bright in precontrast T1 weighted MRI images (AJNR Am J Neuroradiol 2020;41:1833)
Radiology images
Contributed by Mohamed Kayed, M.D., Ph.D.

Small colloid cyst, T1 sagittal MRI
Small colloid cyst, T2 sagittal MRI

Large colloid cyst, MRI

Large colloid cyst, CT
Images hosted on other servers:

Extensive chronic hydrocephalus

Large colloid cyst

T1 hyperintense colloid cyst
Prognostic factors
- Excellent prognosis
- Rare cases associated with sudden death (World Neurosurg 2019:123:351)
- Spontaneous regression is very rare (BMC Neurol 2022;22:397)
- Malignant transformation has not been reported
Case reports
- 10 year old girl with brainstem death due to a third ventricular colloid cyst (BJR Case Rep 2022;8:20220007)
- 31 year old woman with colloid cyst causing acute hydrocephalus during early pregnancy (Surg Neurol Int 2021:12:54)
- 49 year old man with spontaneous regression of colloid cyst (BMC Neurol 2022;22:397)
- 57 year old man with large colloid cyst obstructing the posterior third ventricle (J Neurosurg Case Lessons 2021;1:CASE2121)
- 77 year old woman with xanthogranulomatous colloid cyst (Surg Neurol Int 2019:10:169)
Treatment
- Excision (microsurgical or endoscopic) is curative (World Neurosurg 2021:149:e298)
- Stereotactic aspiration (potential for cyst recurrence)
- Observation may be reasonable in some stable, asymptomatic cases
Clinical images
Images hosted on other servers:

Intraoperative view of a colloid cyst
Gross description
- 1 - 2 cm; larger cysts have been reported
- Round, unilocular, translucent with thin, glistening wall
- Cyst filled with clear or turbid viscid mucin that solidifies after fixation (AJNR Am J Neuroradiol 2000;21:1470)
- Specimens received are often only a wrinkled membrane
Gross images
Images hosted on other servers:

2 cm colloid cyst


Endoscopically excised colloid cyst
Microscopic (histologic) description
- Hypocellular, fibrous wall lined by simple to pseudostratified columnar epithelium with variable cilia or goblet cells (resembles bronchial epithelium) (Acta Neuropathol 1997;93:271, Diagn Cytopathol 2002;27:27)
- Cyst lining may be modified by pressure atrophy (become low cuboidal or flattened) or degenerative changes
- Unlike Rathke cleft and endodermal (enterogenous) cysts, lining epithelium is not prone to squamous metaplasia
- Fragments of normal choroid plexus are frequently attached to cyst
- Cyst contents are amorphous and proteinaceous, may show ghosts of desquamated lining cells and eosinophilic filamentous material (degenerated nucleoprotein and phospholipid) resembling infectious organisms (Actinomyces)
- In chronic lesions, a xanthogranulomatous reaction may occur (Surg Neurol Int 2019:10:169)
Microscopic (histologic) images
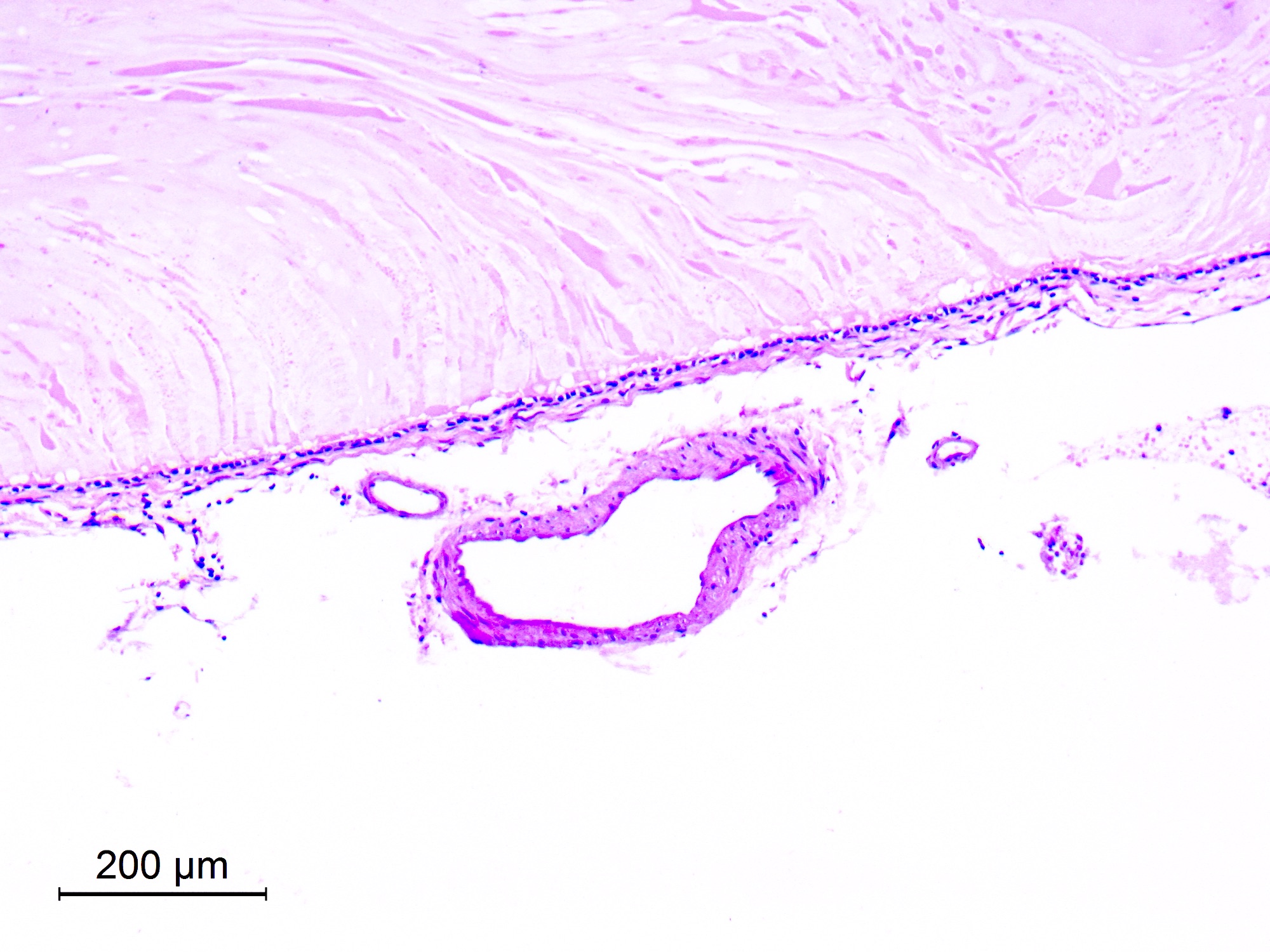
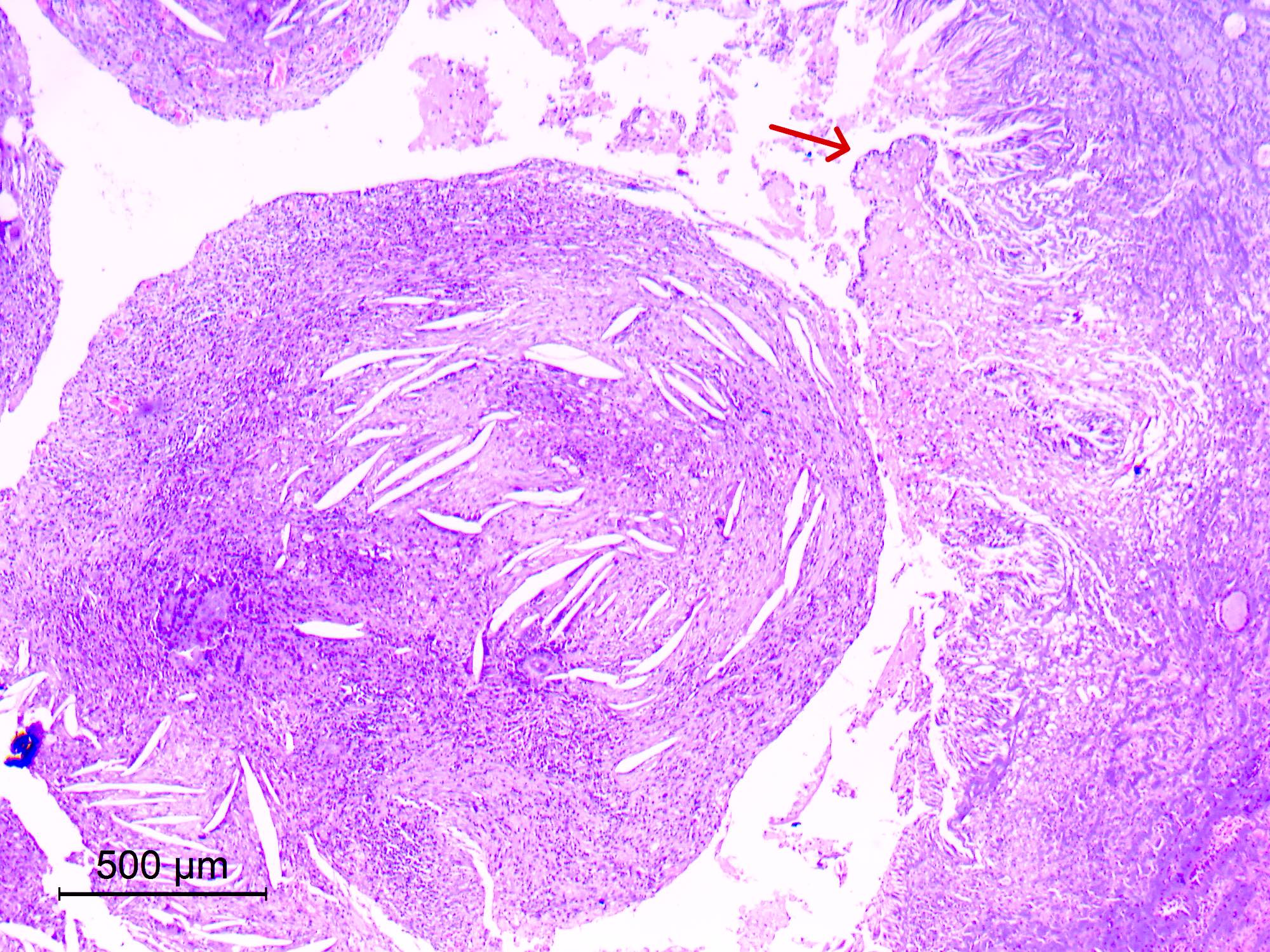
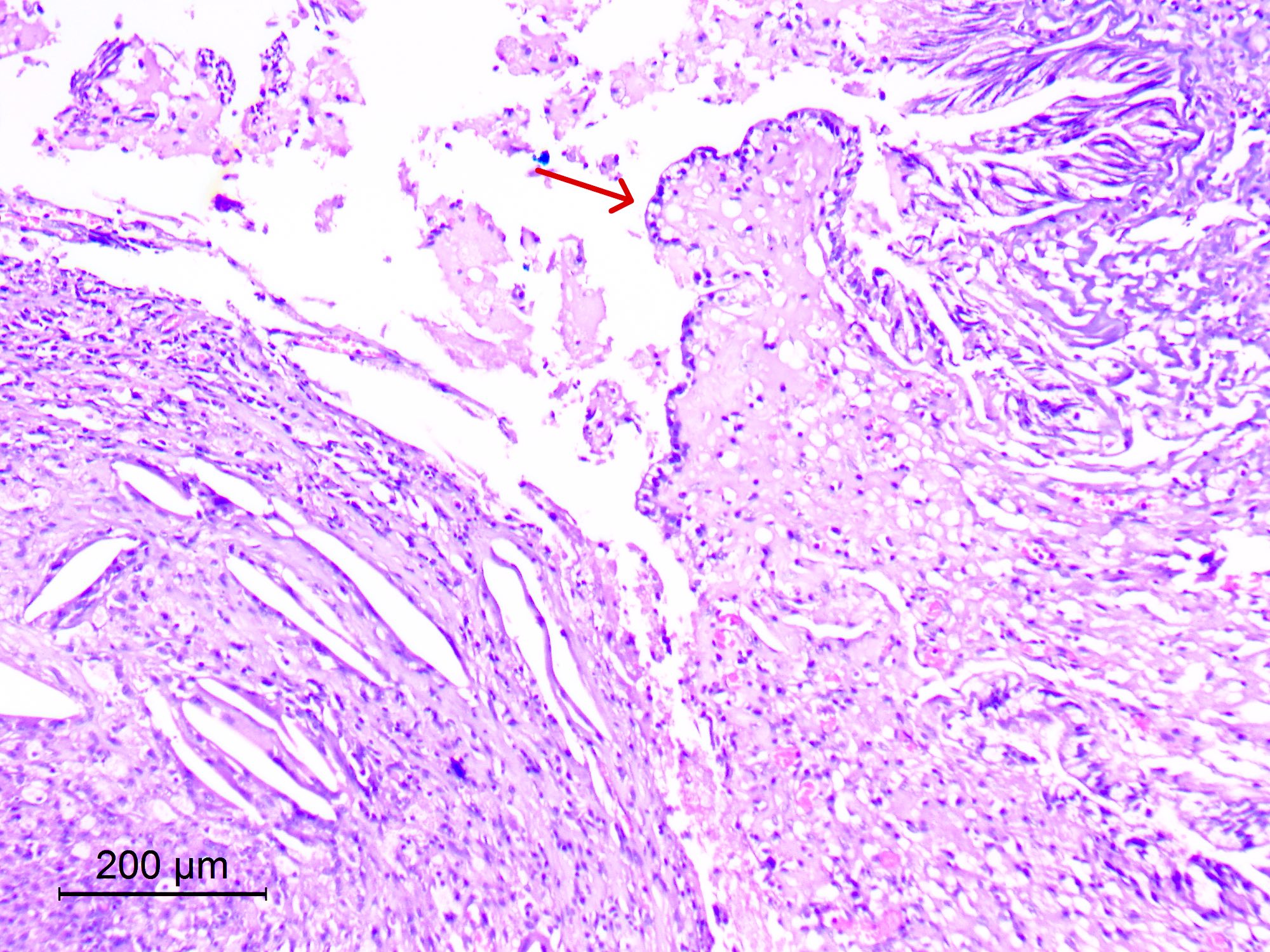
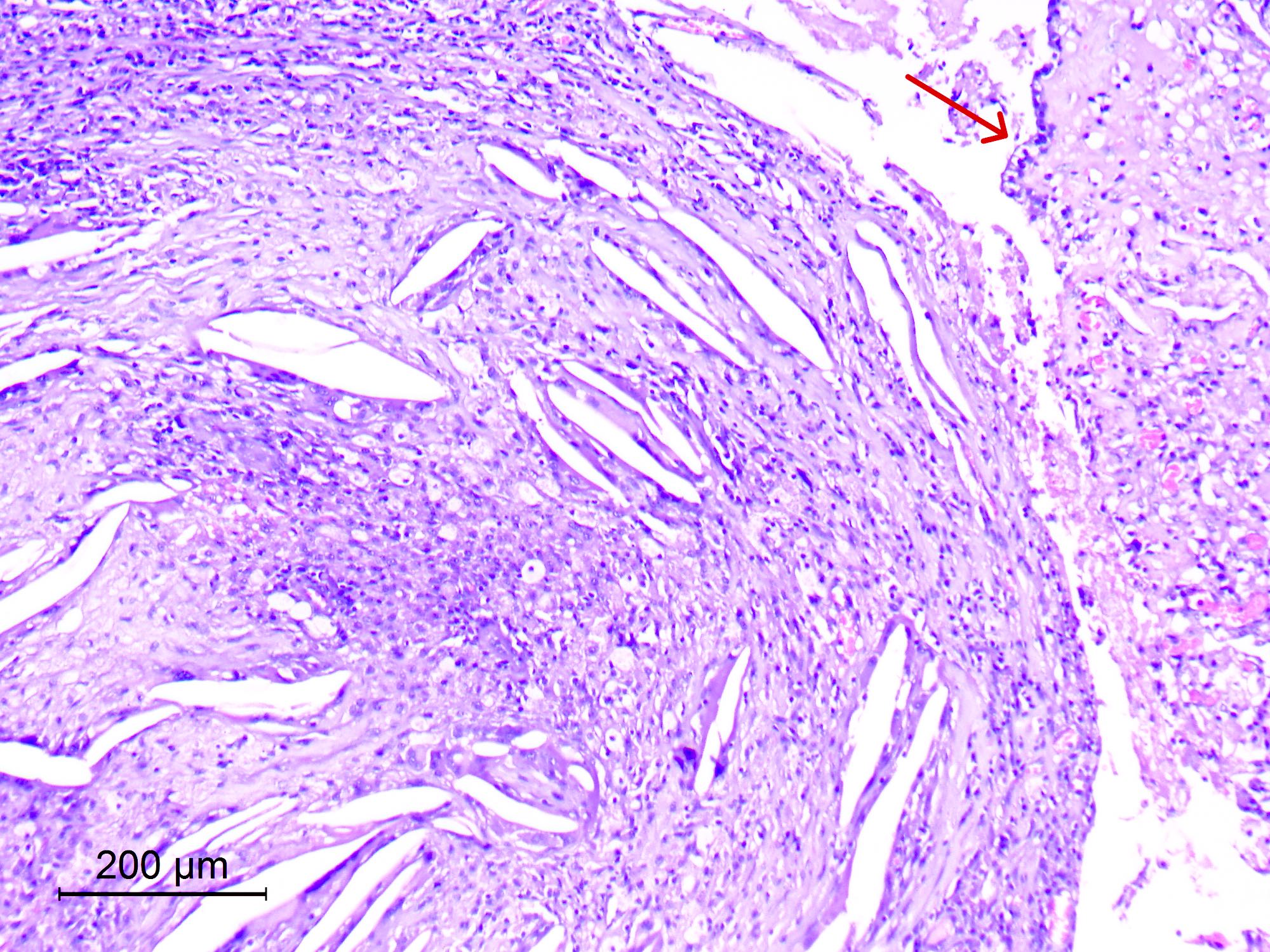
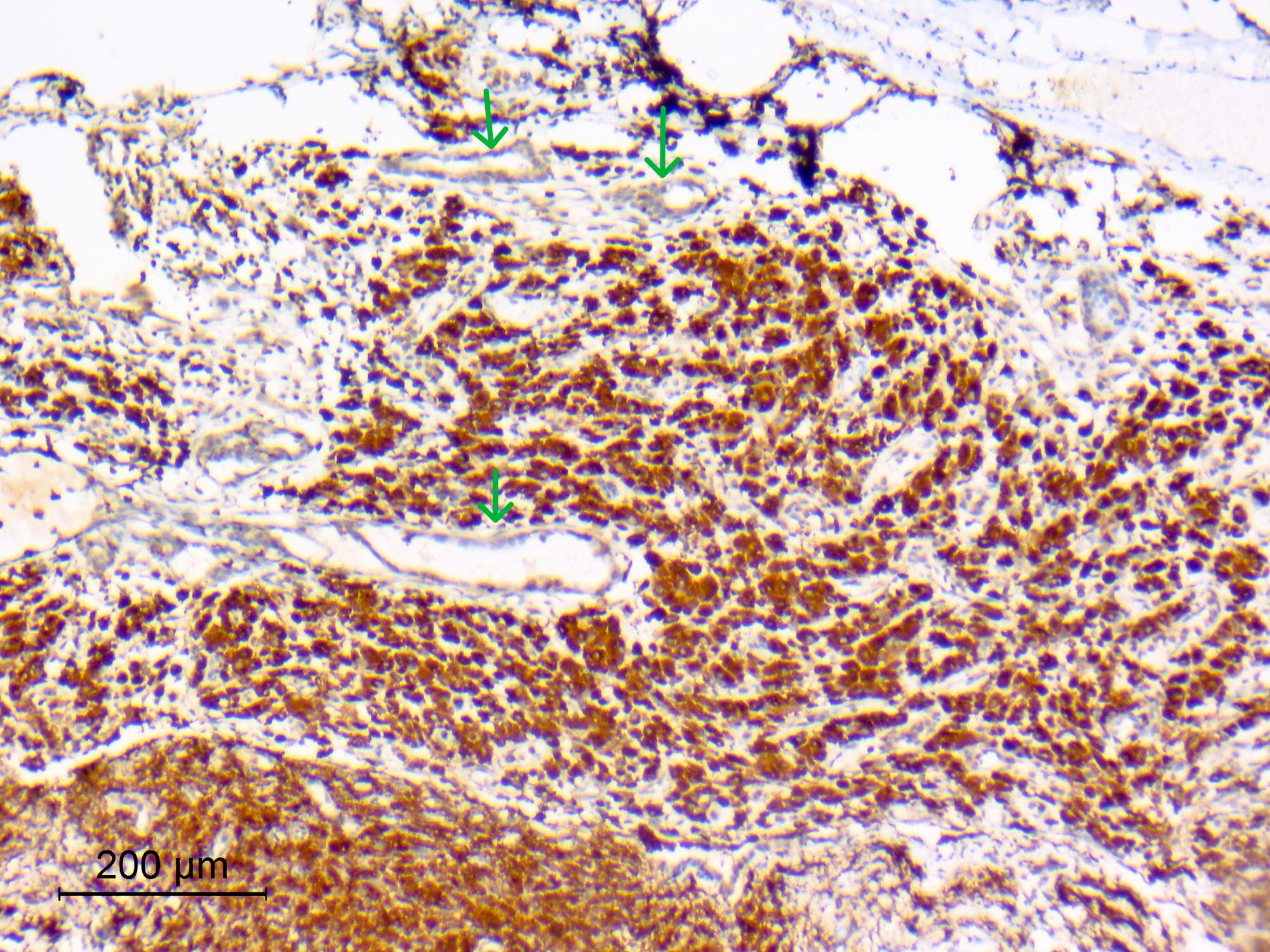
Contributed by Eman Abdelzaher, M.D., Ph.D.
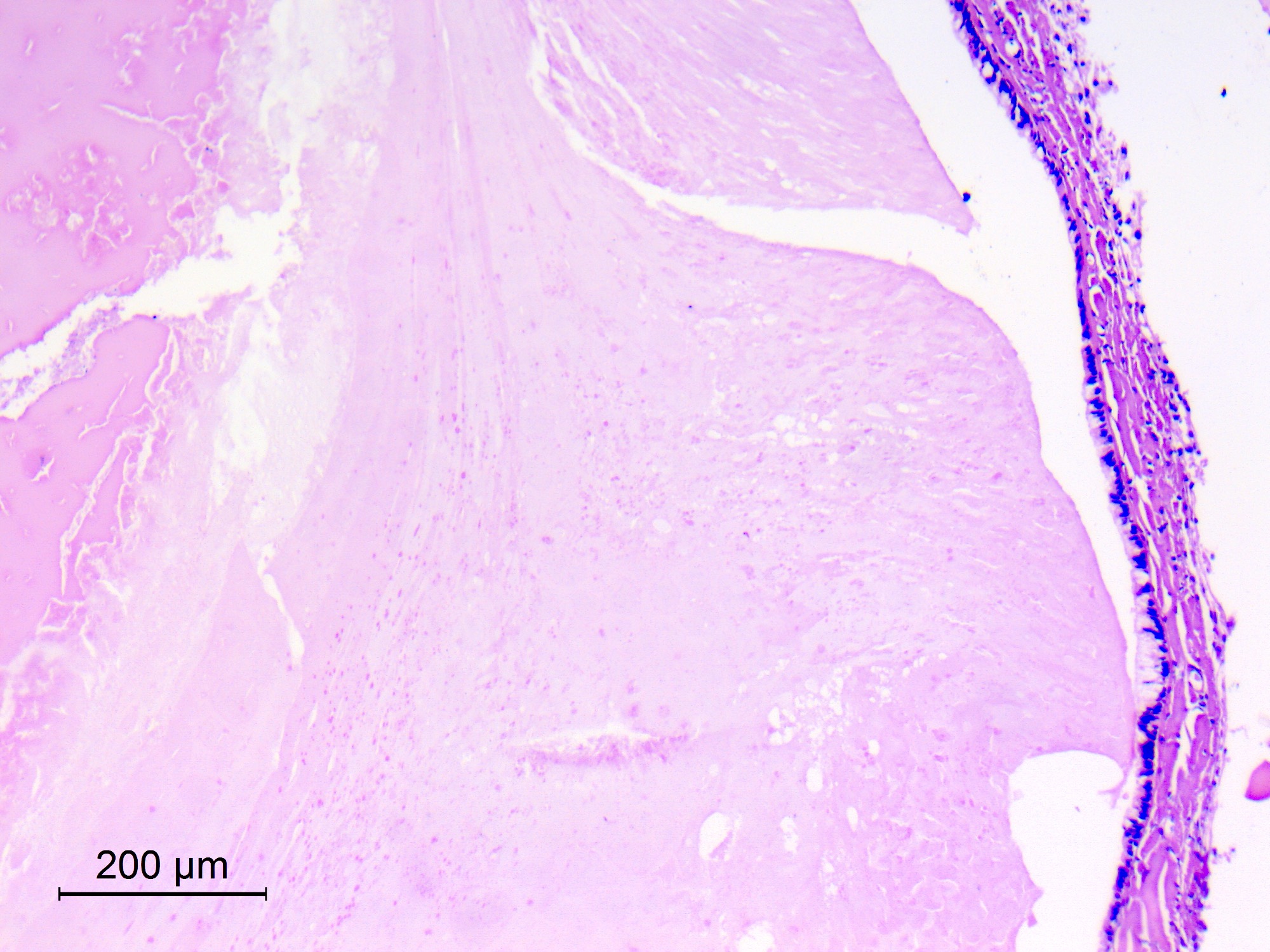
Fibrous wall and proteinaceous contents

Attached choroid plexus
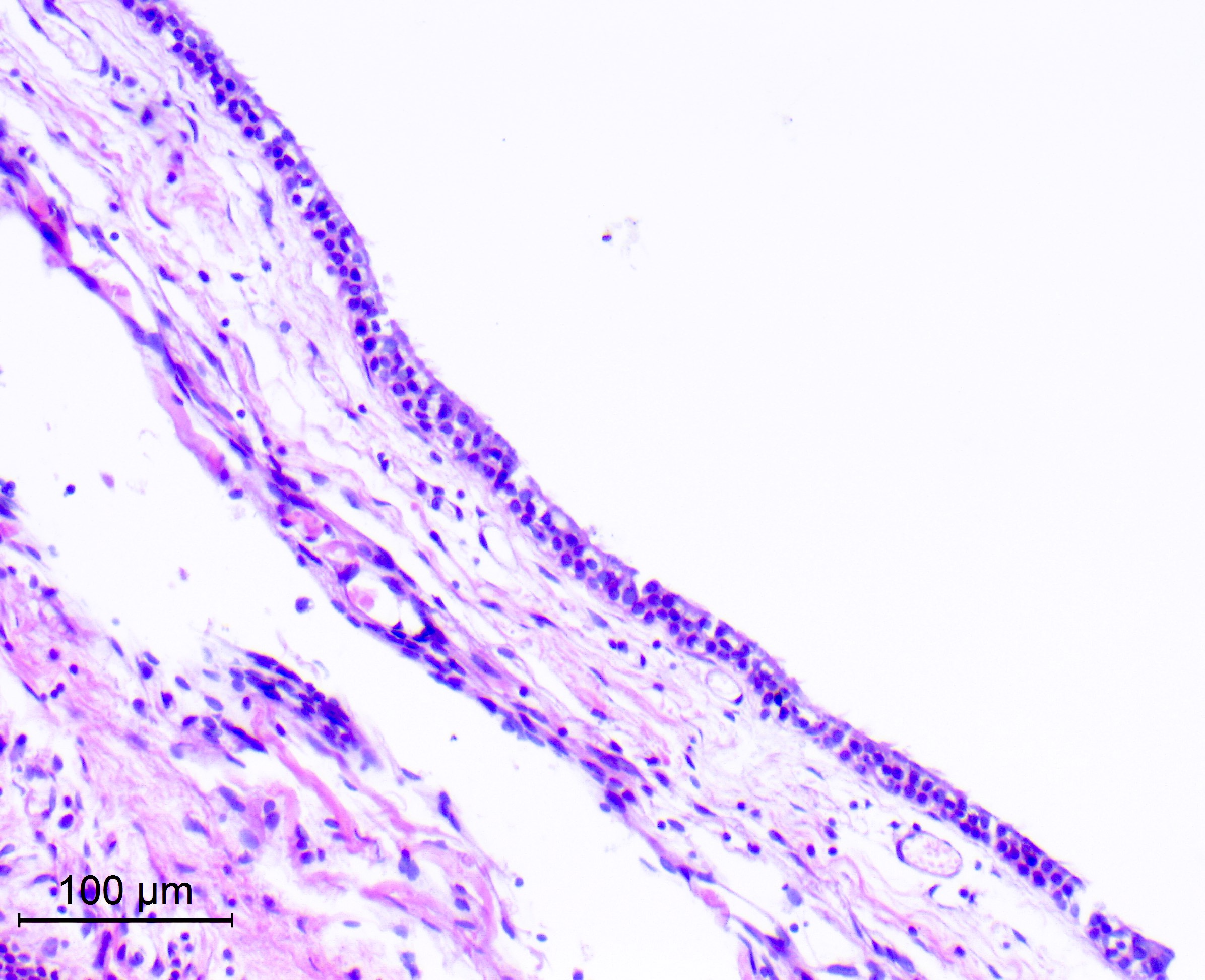
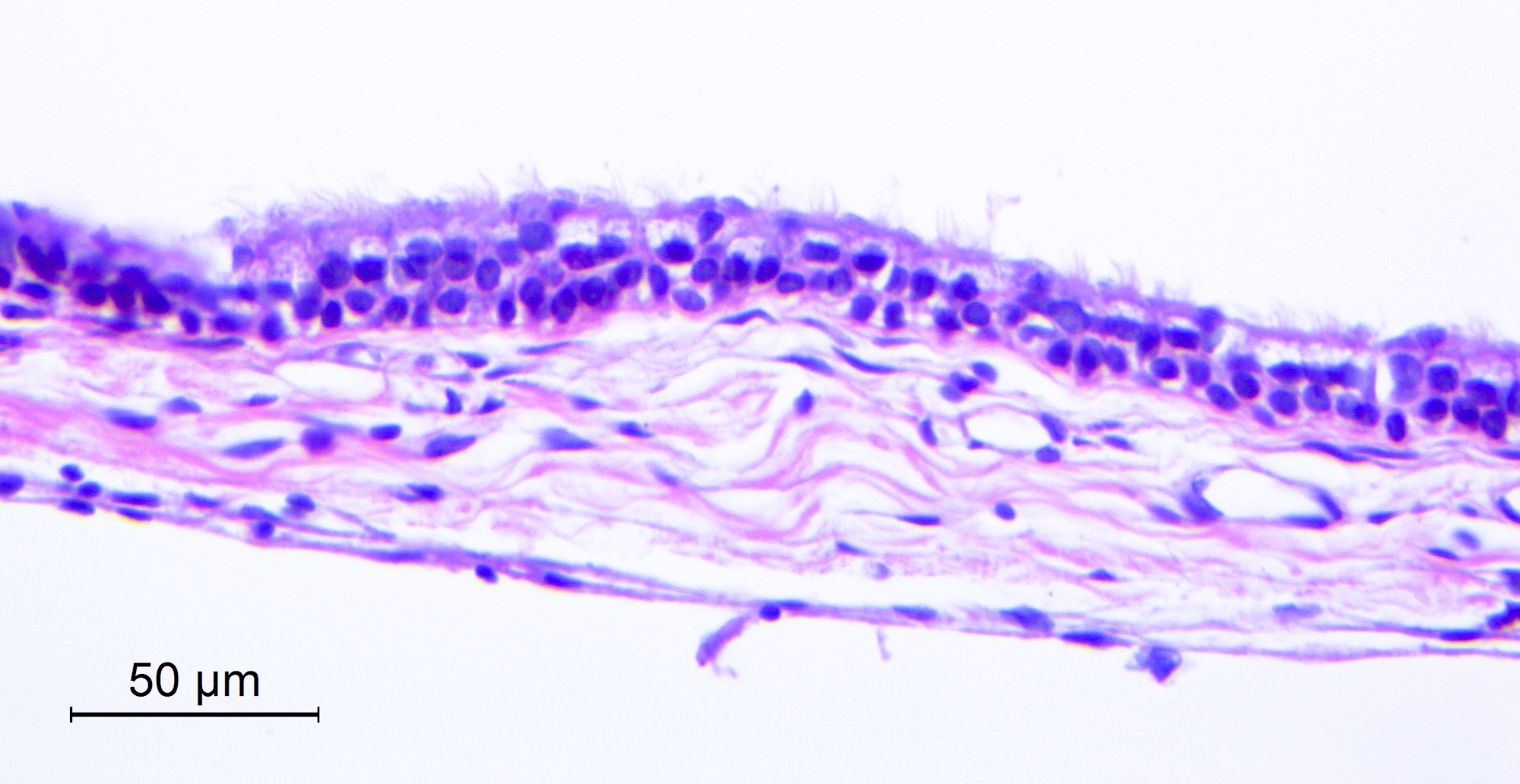
Pseudostratified ciliated cells
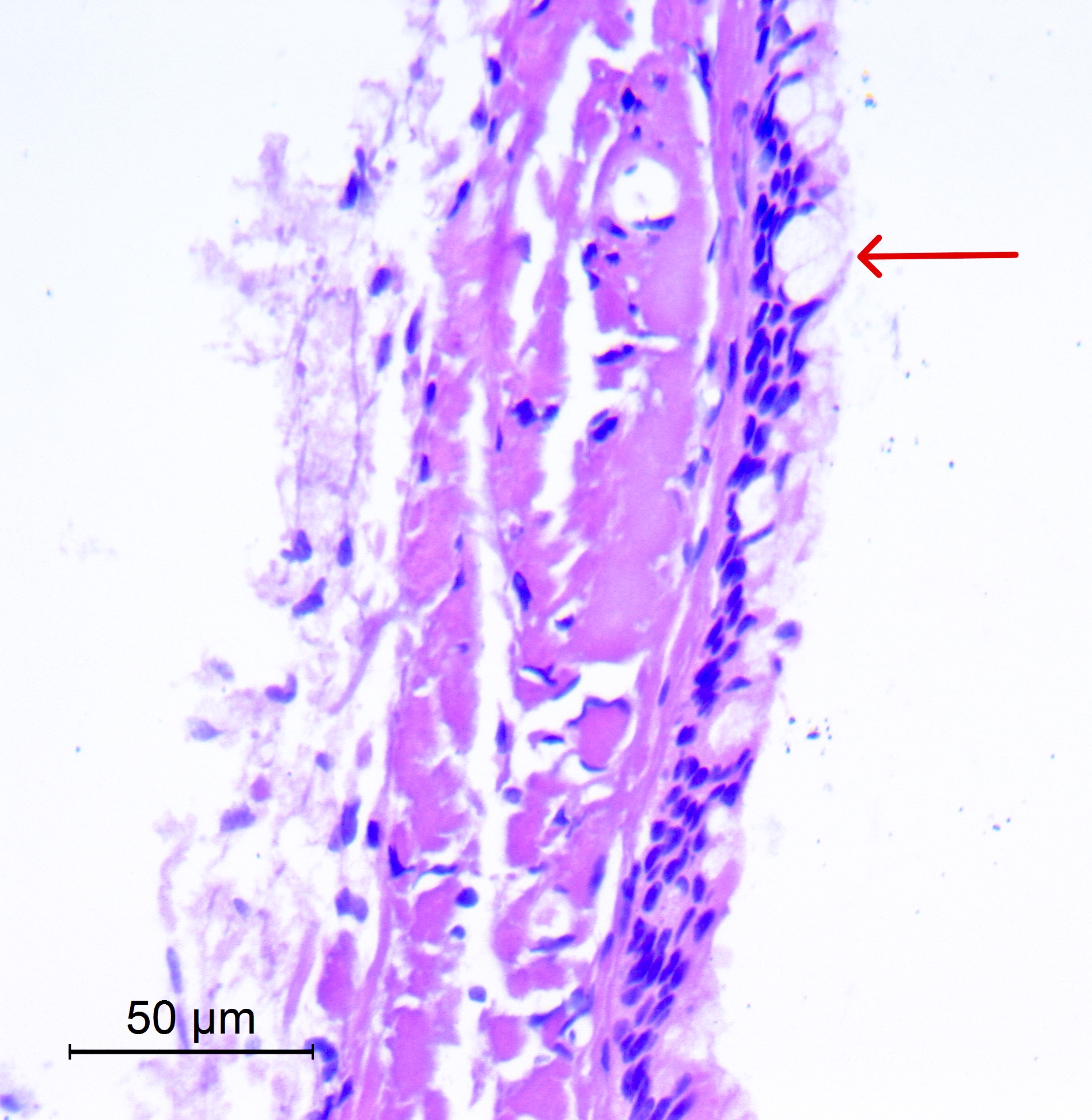
Goblet cells
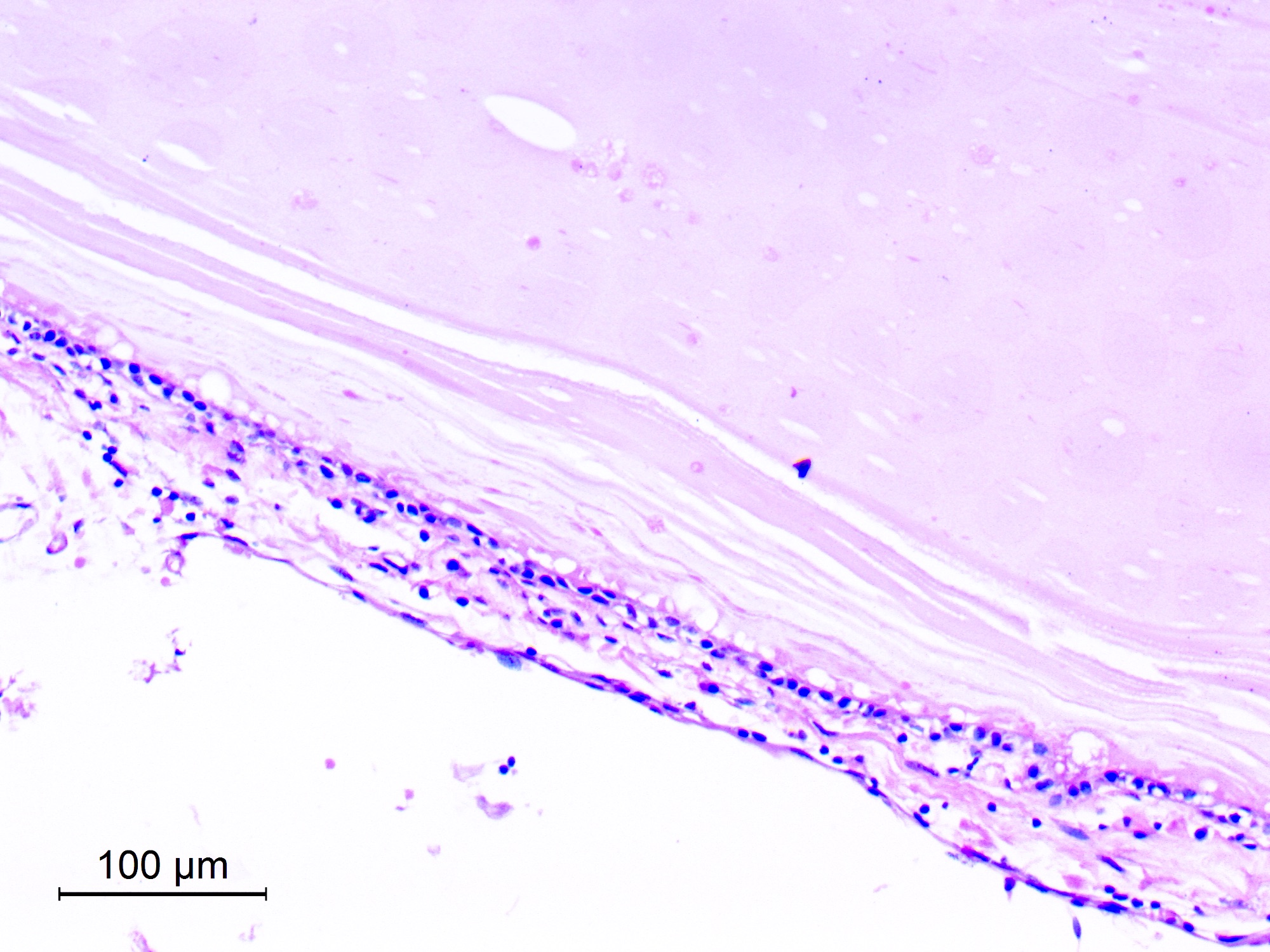
Cuboidal lining
Xanthogranulomatous reaction
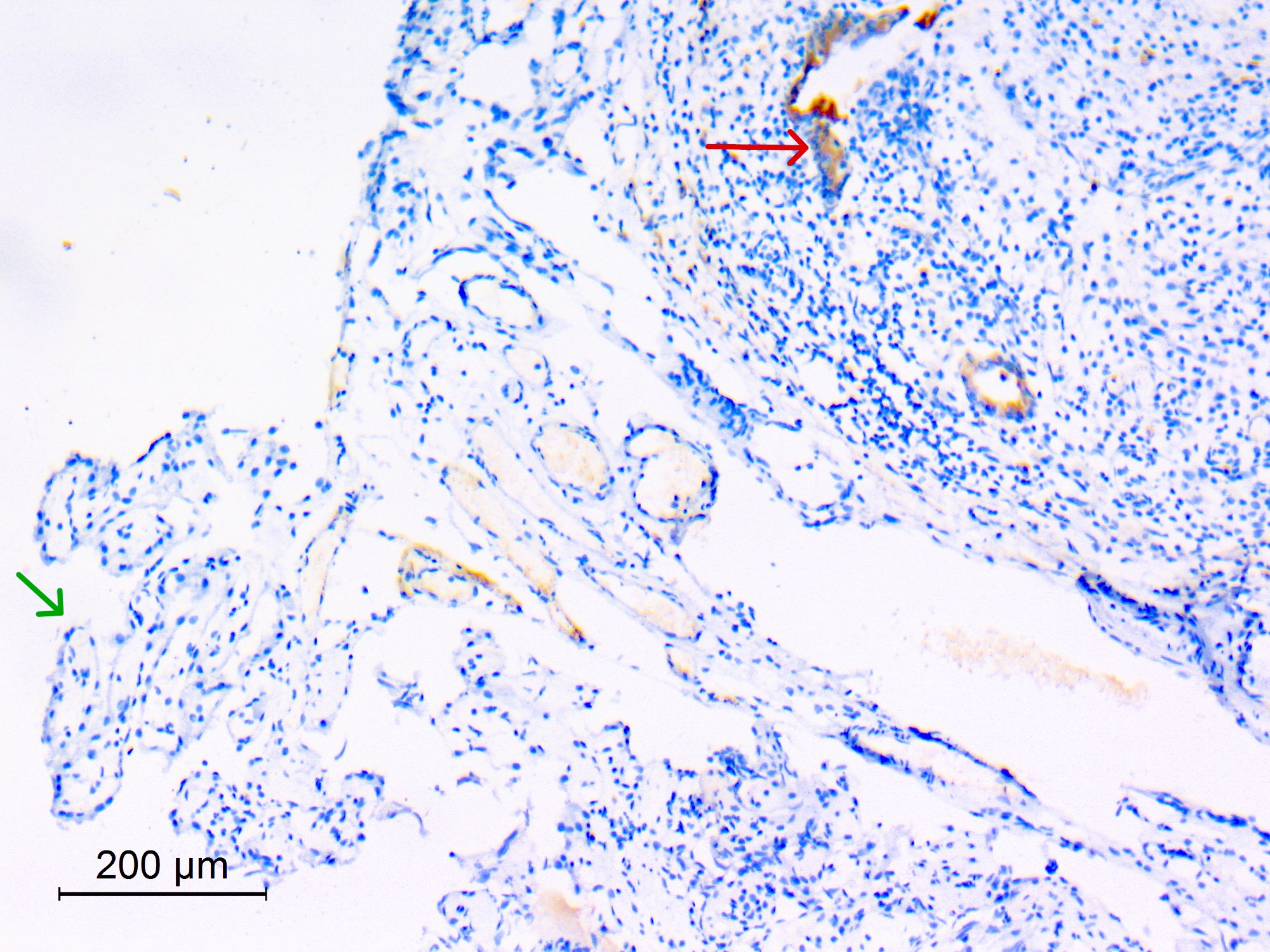

EMA

S100
CD68
Cytology description
- Epithelial cells, cohesive sheets and individual ciliated cells and goblet cells (Diagn Cytopathol 2002;27:27)
- Abundant amorphous proteinaceous material with or without Actinomyces-like nucleoprotein arrays
- Presence of macrophages
Cytology images
Images hosted on other servers:

Thick proteinaceous material
Positive stains
- Epithelium: keratin (low and high molecular weight) (Hum Pathol 1992;23:811)
- Epithelium: EMA
- Mucin: PAS, mucicarmine (Diagn Pathol 2012:7:144)
Negative stains
Electron microscopy description
- Epithelial nature of lining cells is evident by cytoplasmic tonofilaments and desmosomes
- 6 cell types: ciliated cells, nonciliated cells with surface microvilli, goblet cells, basal cells, nonspecific small cells and occasional neuroendocrine cells with neurosecretory granules (Acta Neuropathol 1992;83:605)
- Well formed basal lamina
Electron microscopy images
Images hosted on other servers:

Ciliary pattern of colloid cyst
Videos
Colloid cyst
Sample pathology report
- Third ventricular cyst, endoscopic excision biopsy:
- Colloid cyst
Differential diagnosis
- Rathke cleft cyst:
- Intrasellar or suprasellar location
- Prone to squamous metaplasia
- Normal choroid plexus:
- Sometimes dominant or only epithelial tissue
- Papillary with cobblestone lining epithelium
- No ciliated or goblet cells
- EMA generally negative
- Choroid plexus papilloma:
- Papillary with pseudostratified lining epithelium
- No ciliated or goblet cells
- Papillary craniopharyngioma with xanthogranulomatous change:
- Squamous lining
Additional references
Board review style question #1
The brain cyst shown in the above image is strategically located near the foramen of Monro. Which of the following is the correct diagnosis?
- Arachnoid cyst
- Colloid cyst
- Endodermal (enterogenous) cyst
- Rathke cleft cyst
Board review style answer #1
B. Colloid cyst. Colloid cysts have a stereotypic location near the foramina of Monro, which causes intermittent obstruction of cerebrospinal fluid (CSF) flow and obstructive hydrocephalus. Answer D is incorrect because Rathke cleft cyst is sellar or suprasellar in location. Answer C is incorrect because endodermal (enterogenous) cysts mostly arise in the intraspinal compartment or in the posterior fossa. Answer A is incorrect because an arachnoid cyst is often located in the Sylvian fissure.
Comment Here
Reference: Colloid cyst
Comment Here
Reference: Colloid cyst
Board review style question #2
Which of the following brain cysts has a columnar cyst lining and is not prone to squamous metaplasia?
- Colloid cyst
- Endodermal (enterogenous) cyst
- Epidermoid cyst
- Rathke cleft cyst
Board review style answer #2
A. Colloid cyst. The lining epithelium of colloid cysts is not prone to squamous metaplasia. Answers B and D are incorrect because the lining epithelium of Rathke cleft cysts and endodermal (enterogenous) cysts is prone to squamous metaplasia. Answer C is incorrect because epidermoid cysts are lined by keratinized stratified squamous epithelium.
Comment Here
Reference: Colloid cyst
Comment Here
Reference: Colloid cyst
