
CNS & pituitary tumors
Meningeal tumors
Anaplastic meningioma
Author: Valeria Barresi, M.D., Ph.D.
Editorial Board Member: Meaghan Morris, M.D., Ph.D.
Deputy Editor-in-Chief: Chunyu Cai, M.D., Ph.D.

Last author update: 3 August 2022
Last staff update: 11 October 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Anaplastic meningioma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Intraoperative frozen / smear cytology images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Barresi V. Anaplastic meningioma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnstumoranaplasticmeningioma.html. Accessed April 2nd, 2025.
Definition / general
- WHO 2021 definition: a meningioma with overtly malignant cytomorphology that can
- Resemble a carcinoma, melanoma or high grade sarcoma
- Display markedly elevated mitotic activity (≥ 12.5 mitoses/mm2, ≥ 20 mitoses/10 high power fields [HPF] of each 0.16 mm2)
- Harbor a TERT promoter mutation or
- Have homozygous CDKN2A / CDKN2B deletion
- CNS WHO grade 3
- 1 - 3% of meningiomas
- De novo (primary) or progression from a lower grade (1 or 2) meningioma (secondary) (Neuro Oncol 2018;20:1113)
Essential features
- Meningioma with overtly malignant cytomorphology that can
- Resemble a carcinoma, melanoma or high grade sarcoma
- Display markedly elevated mitotic activity (≥ 12.5 mitoses/mm2, ≥ 20 mitoses/10 HPF of each 0.16 mm2)
- Harbor a TERT promoter mutation or
- Have homozygous CDKN2A / CDKN2B deletion
- CNS WHO grade 3
- Shows either histologic or immunohistochemical evidence of meningothelial differentiation
- At least shows focal meningothelial whorls, psammoma bodies or nuclear pseudoinclusions
- Immunohistochemistry: epithelial membrane antigen (EMA)+ (even focal), SSTR2A+, possible focal CK AE1 / AE3+, STAT6-
- Recurrence in 50 - 94%
Terminology
- Also called:
- Malignant meningioma
- Meningothelial sarcoma (not preferred)
ICD coding
- ICD-O: 9530/3 - meningioma, malignant
Epidemiology
- Any age, mainly adults 45 - 85 years (Neuro Oncol 2015;17:1166)
- Higher incidence in females but equal incidence in the 2 sexes at 75 - 85 years (Neuro Oncol 2015;17:1166)
Sites
- Cerebral or spinal meninges; cerebral ventricles (Neurosurg Rev 2020;43:513)
Pathophysiology
- Originates from arachnoid border cells or dural based cells (Acta Neurochir (Wien) 2021;163:57)
- The driver genetic event in most cases is NF2 inactivation by mutation or chromosome 22q loss
- Progression from lower grade meningioma follows pTERT mutation, CDKN2A / CDKN2B homozygous deletion, loss of chromosomes 9p, 1p, 6q, 10, 14q, 18q, gains of chromosomes 1q, 9q, 12q, 15q, 17q, 20q (Clin Cancer Res 2010;16:4155, Brain Pathol 2002;12:183, Brain Pathol 2014;24:184)
Etiology
- Risk factors may be similar to risk factors for meningioma: ionizing radiations; neurofibromatosis type 2 (Eur J Epidemiol 2020;35:591)
Clinical features
- Neurological deficits depending on tumor location
- Common headaches, weakness and seizures (World Neurosurg 2021;149:e877)
Diagnosis
- Based on imaging (CT; MRI) / biopsy / resection specimen
Radiology description
- MRI: contrast enhancing mass with possible necrotic areas (Neurochirurgie 2021;67:193)
- MRI: contrast enhancing dural tail sign at the perimeter
Radiology images
Contributed by Valeria Barresi, M.D, Ph.D.
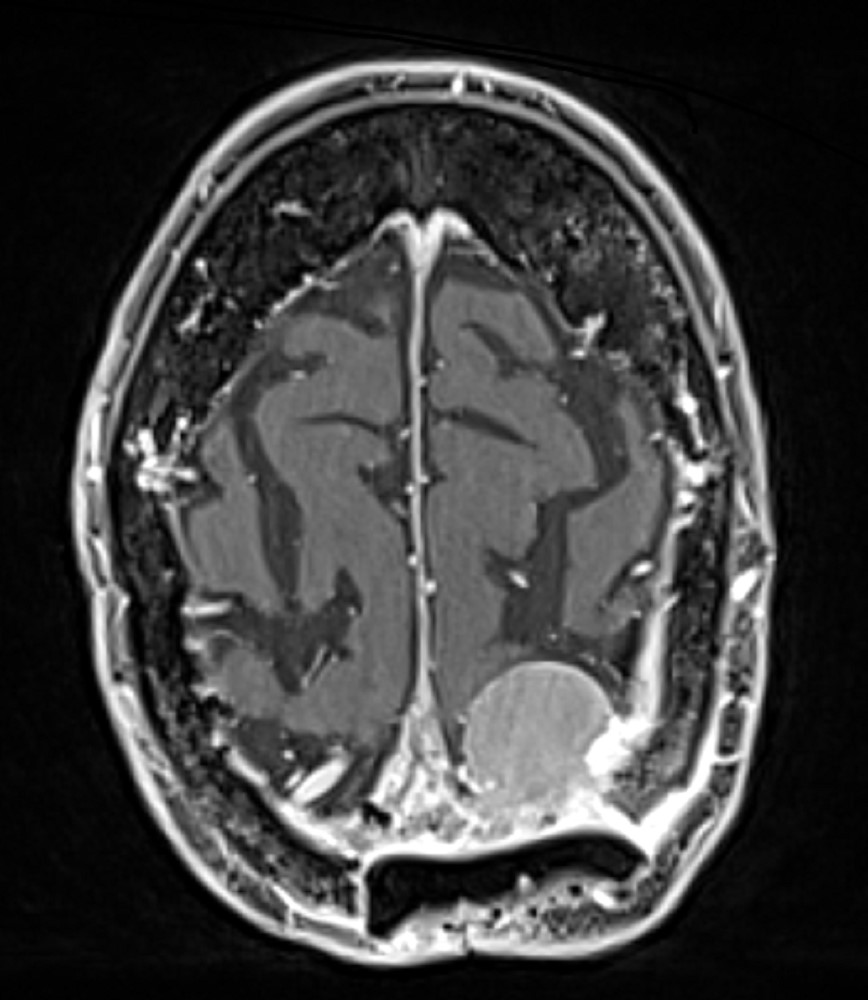
Extra-axial, dural mass
Images hosted on other servers:

MRI
Prognostic factors
- Recurrence rate of 50 - 94%
- 10 year relative survival of 59.6% (Neuro Oncol 2020;22:iv1)
- Favorable prognostic factors: age 20 - 44 years and spinal location (Neuro Oncol 2021;23:iii1)
- Unfavorable prognostic factors: TERT promoter mutation; CDKN2A / CDKN2B homozygous deletion; H3K27me3 immunohistochemical loss (J Neuropathol Exp Neurol 2020;79:754)
Case reports
- 2 year old boy with anaplastic meningioma (CNS Oncol 2016;5:131)
- 51 year old man with anaplastic intraventricular meningioma (World J Surg Oncol 2014;12:238)
- 55 year old man with secondary anaplastic meningioma (Neurochirurgie 2021;67:193)
Treatment
- Surgery followed by fractioned radiotherapy, experimental chemotherapy or peptide receptor radionuclide therapy (Lancet Oncol 2016;17:e383)
Gross description
- Dural based and widely variable in size
- May be well circumscribed or readily adherent to brain parenchyma
- Gross necrosis can be present
Frozen section description
- Differential diagnosis versus other tumor types: at least focal presence of psammoma bodies, meningothelial whorls or nuclear pseudoinclusions
- Differential diagnosis versus CNS WHO grade 1 meningiomas: presence of mitoses
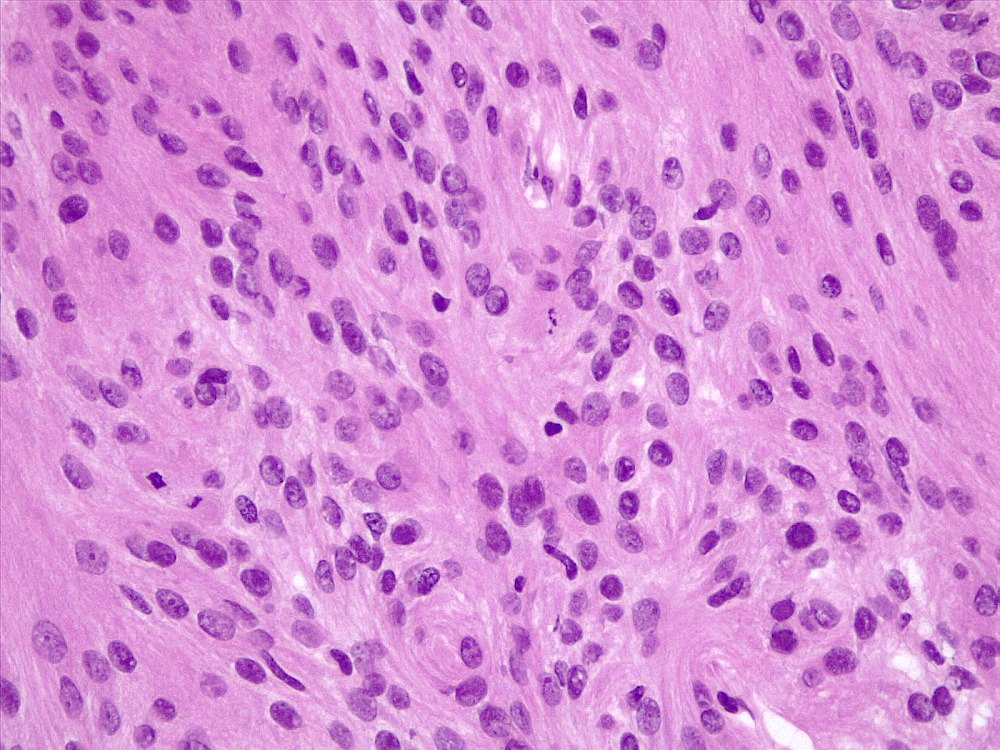
Intraoperative frozen / smear cytology images
Contributed by Valeria Barresi, M.D, Ph.D.
Lobular architecture
Whorls
Nuclear pseudoinclusions
Mitoses
Whorls
Psmmoma body
Mitoses
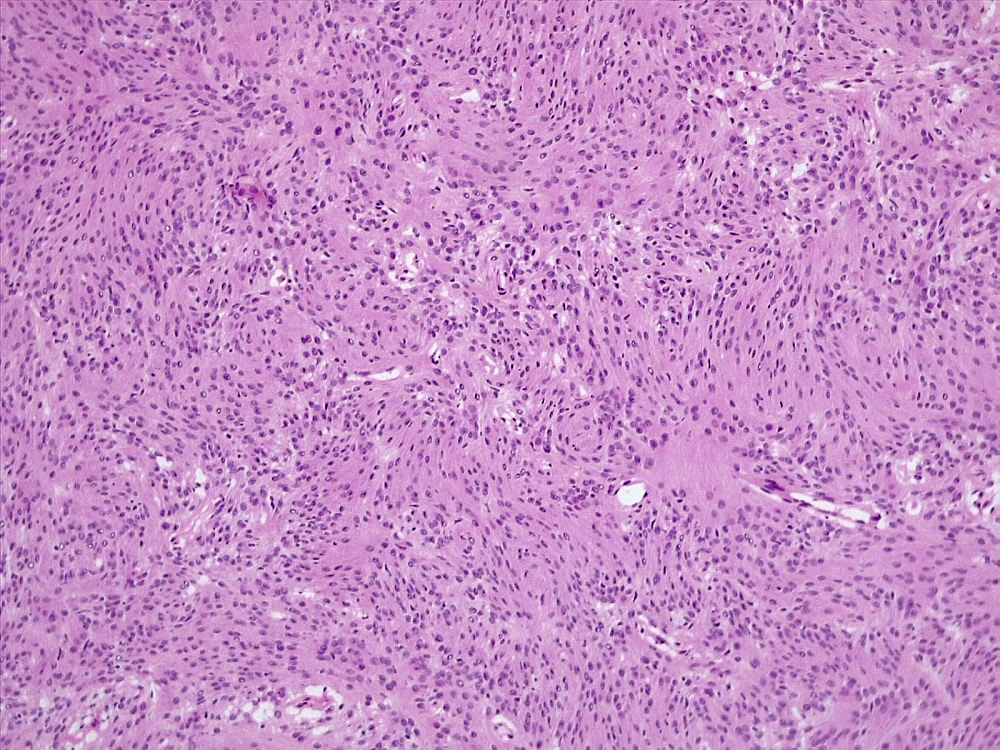
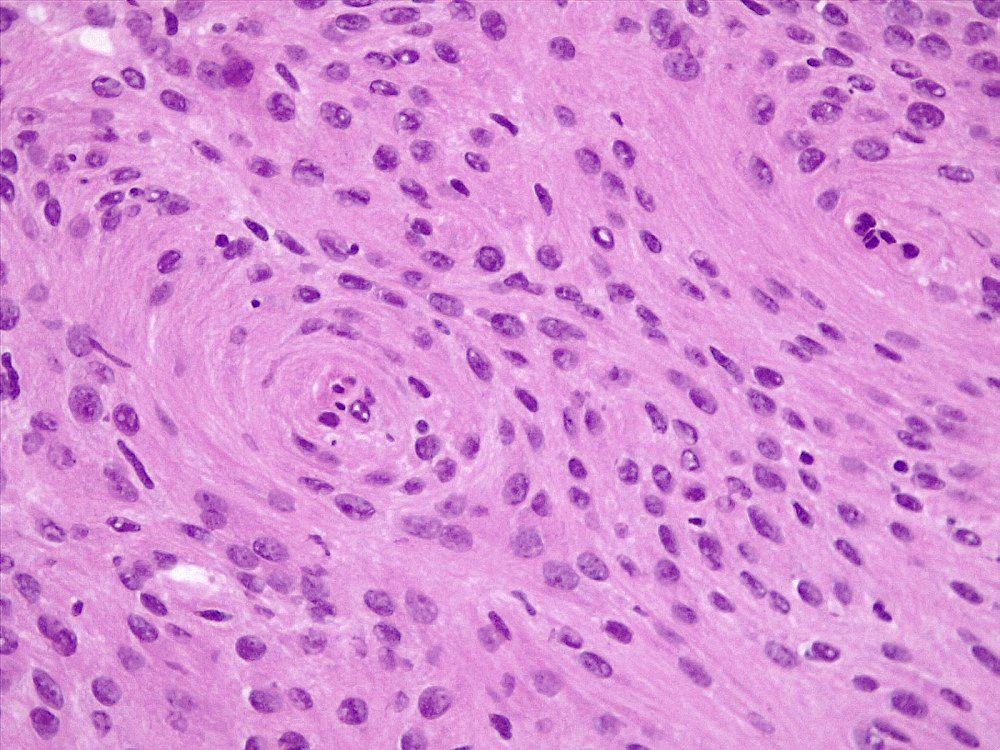
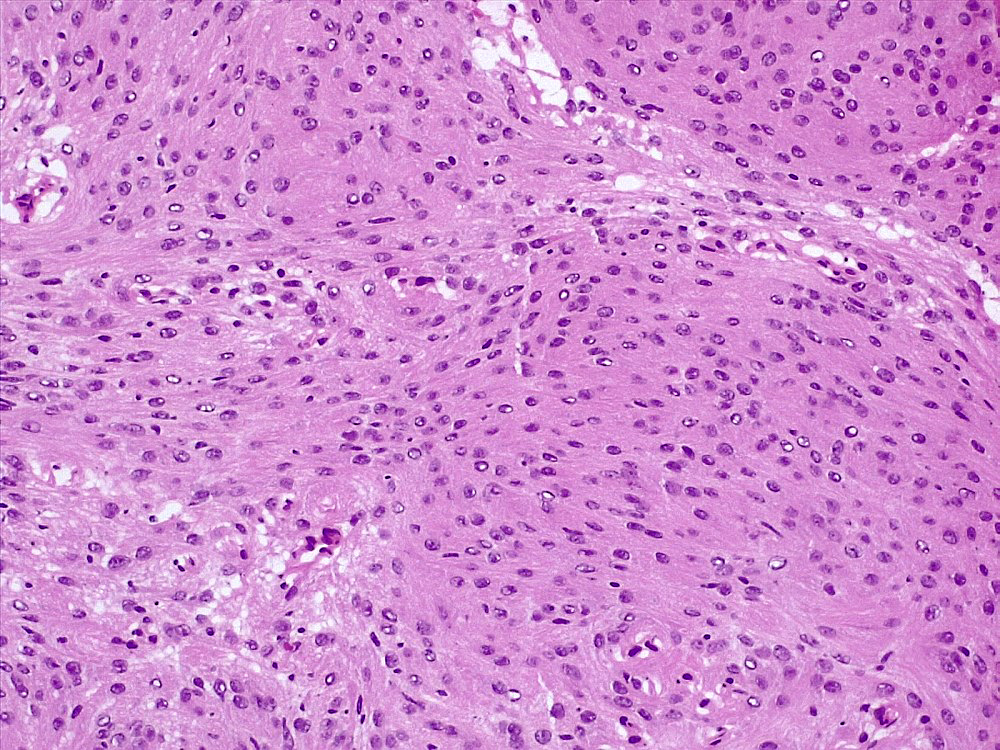
Microscopic (histologic) description
- May have frank malignant cytology resembling a carcinoma, melanoma or high grade sarcoma
- Mitotic index: ≥ 12.5 mitoses/mm2, ≥ 20 mitoses/10 HPF of each 0.16 mm2
- At least focal meningothelial whorls and nuclear pseudoinclusions are useful to establish meningothelial origin
- Psammoma bodies may be present (World Neurosurg 2021;149:e877)
- Necrosis and brain invasion may be present
Microscopic (histologic) images
Contributed by Valeria Barresi, M.D, Ph.D.
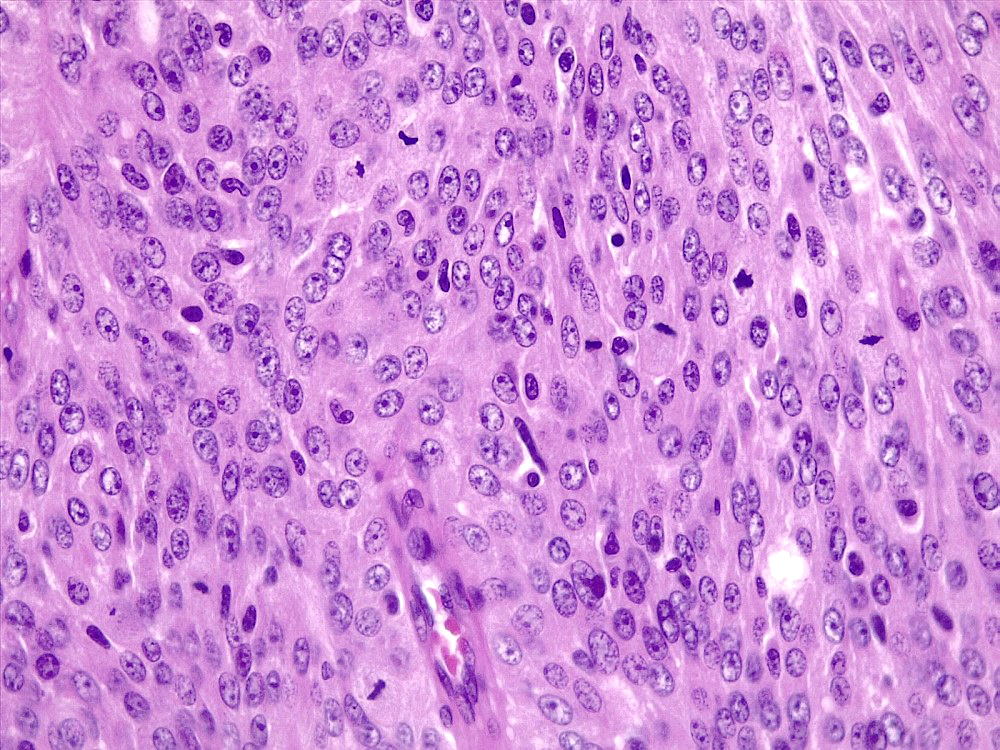
Mitoses
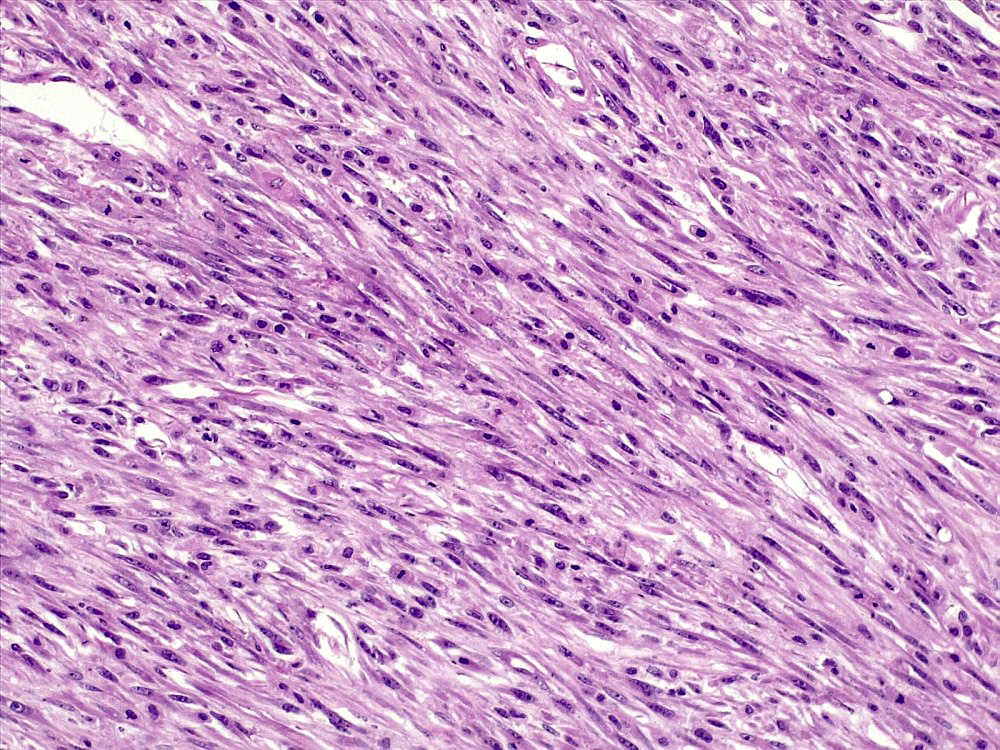
Malignant morphology
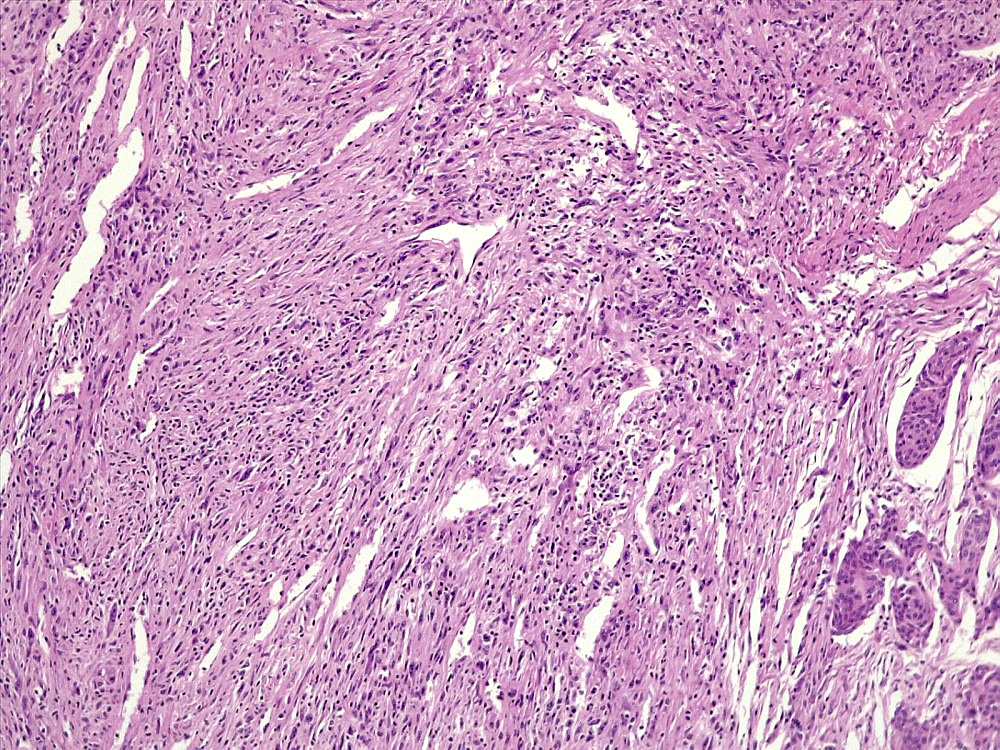
Whorls
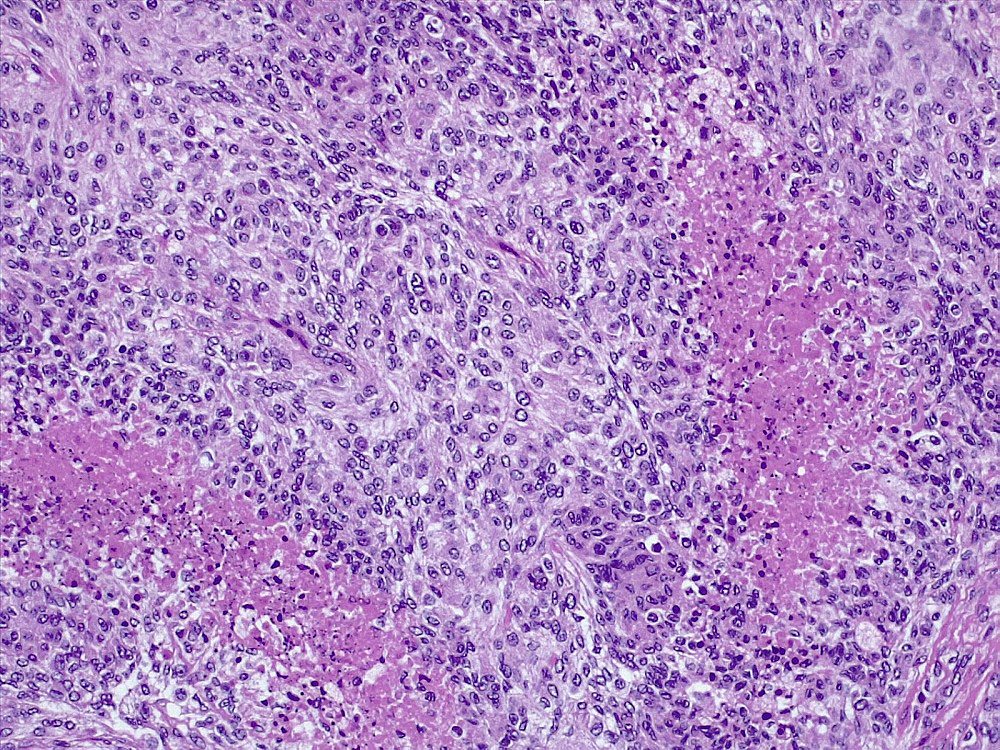
Necrosis
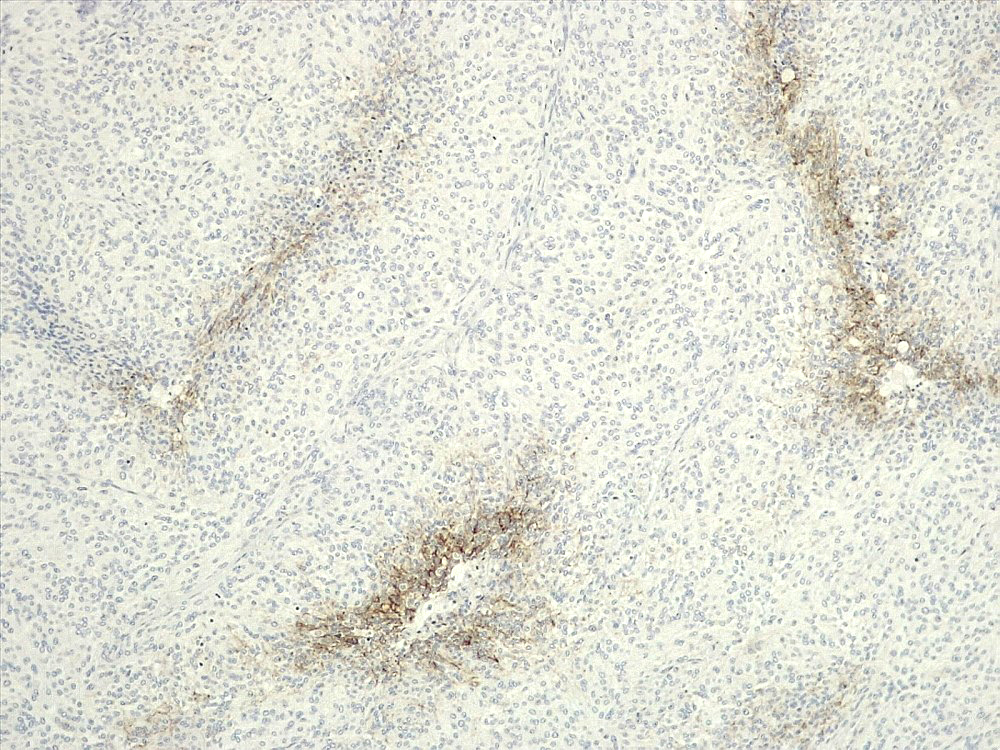
EMA
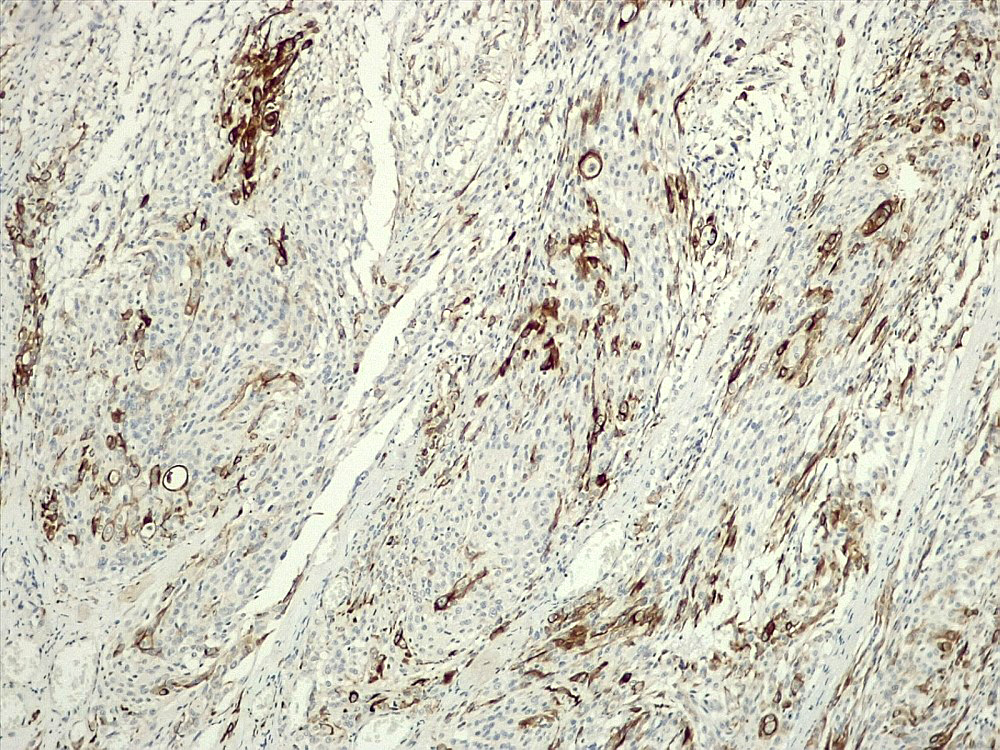
CK AE1 / AE3
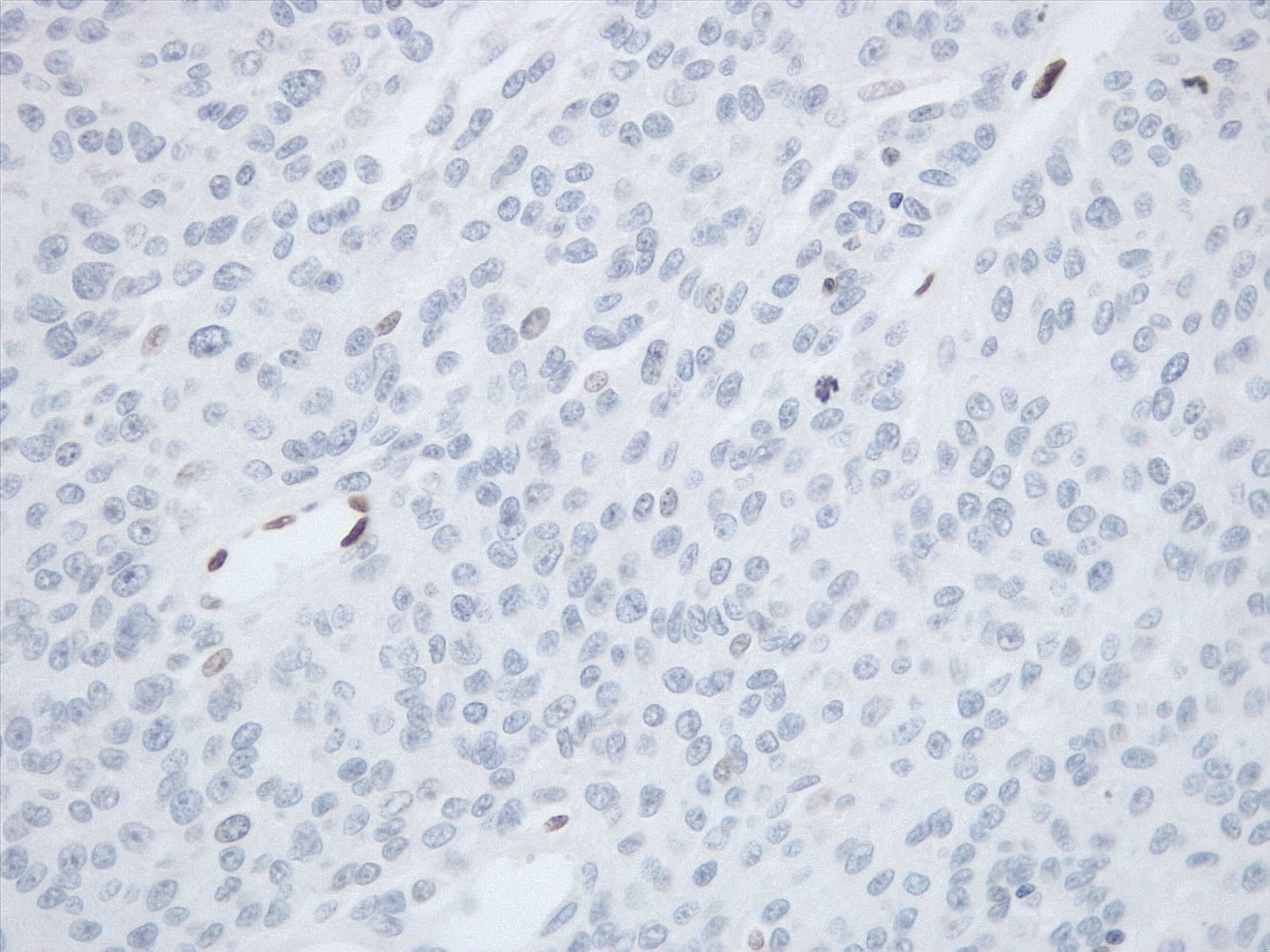
H3K27me3
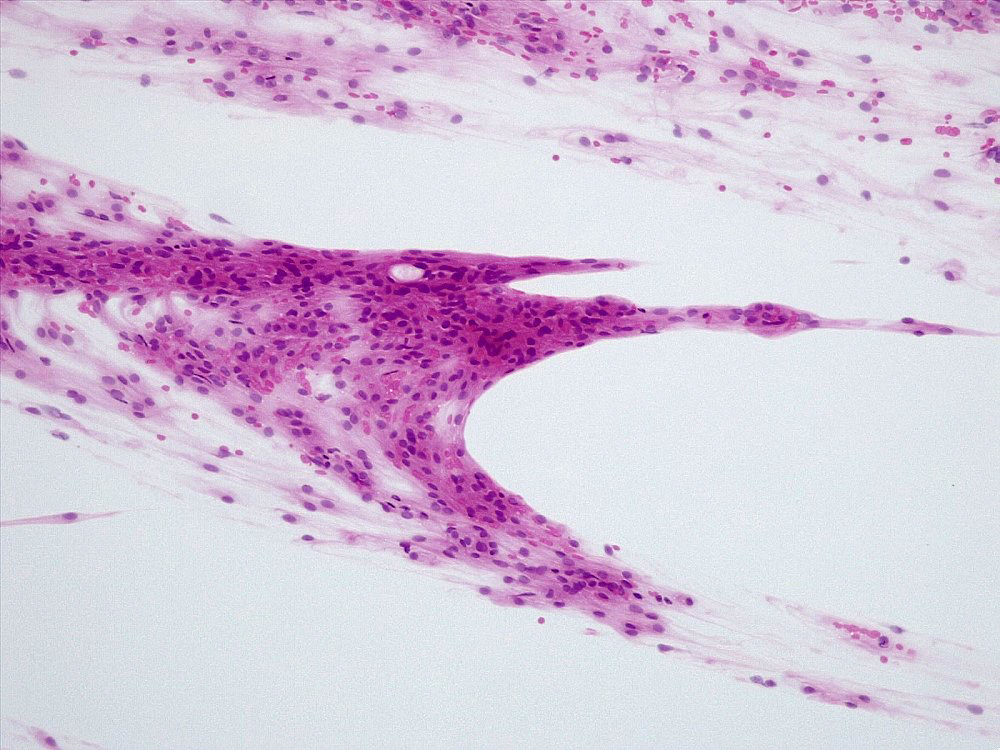
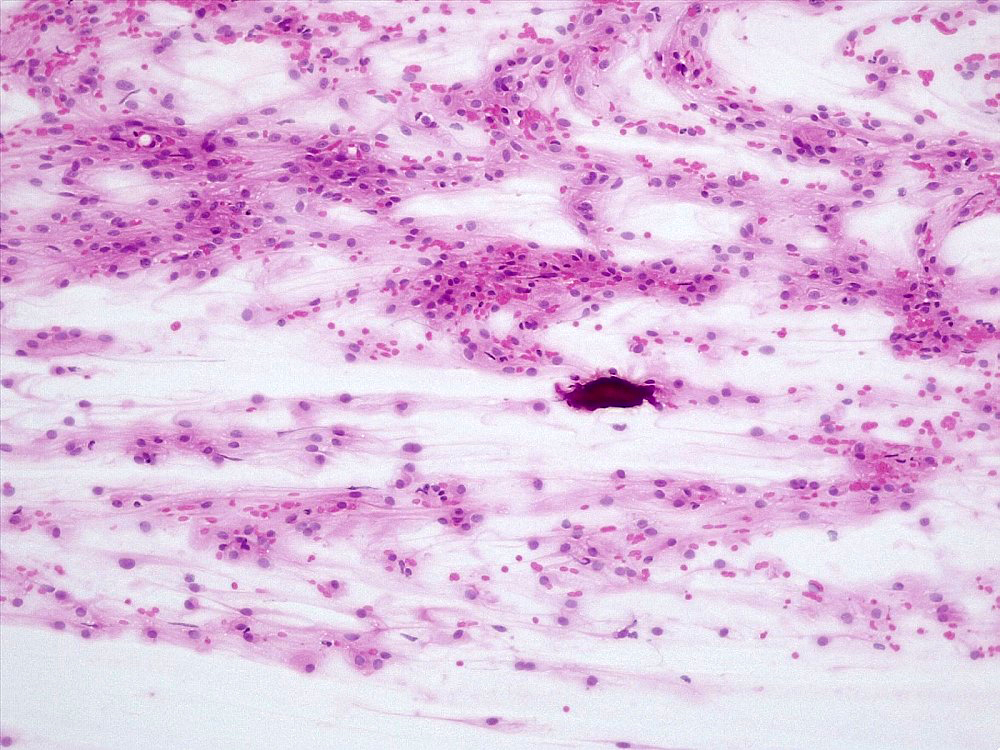
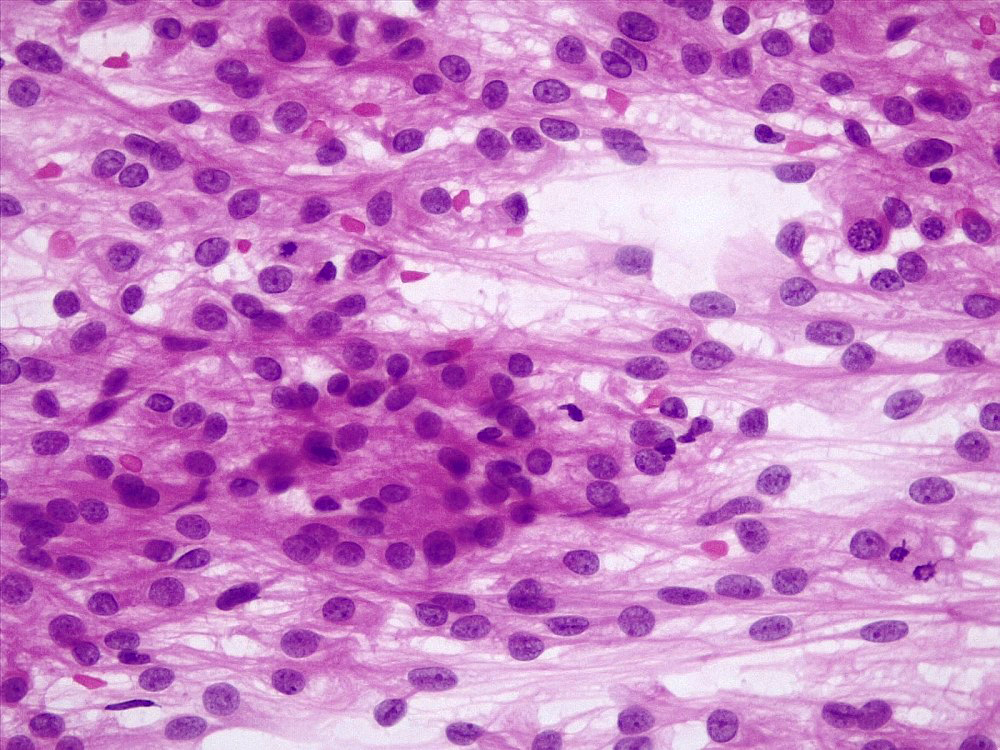
Cytology description
- Smear with tumor cells in large clumps and wide bridge of tissue in between
- Meningothelial lobules, balls or whorls (Diagn Cytopathol 2012;40:104, Acta Cytol 1998;42:1104, J Pathol Transl Med 2019;53:104)
- Thick cytoplasmic bridges among cells groups
- Psammoma bodies (Diagn Cytopathol 2012;40:104)
- Mitoses
- Reference: Adv Anat Pathol 2007;14:303
Positive stains
- EMA (may be focal) (89%)
- CK AE1 / AE3 (focal) (75%) (Hum Pathol 2004;35:1413)
- Vimentin (100%)
- SSTR2A (100%) (J Neuropathol Exp Neurol 2017;76:289)
Negative stains
- GFAP
- SOX10 (J Neuropathol Exp Neurol 2017;76:289)
- S100 (25% positive)
- HMB45
- CD99 (15% positive)
- BCL2 (weak or focal) (31% positive) (Hum Pathol 2004;35:1413)
- CD34
- Inhibin
- Progesterone receptor (20% positive)
- STAT6
Molecular / cytogenetics description
- pTERT mutation (Neuro Oncol 2018;20:1009)
- CDKN2A / CDKN2B homozygous deletion (Brain Pathol 2002;12:183)
- NF2 mutation / deletion
- Loss of chromosomes 9p,1p, 6q, 10, 14q, 18q (Brain Pathol 2010;20:751, Acta Neuropathol Commun 2020;8:171)
- Gains of chromosomes 1q, 9q, 12q, 15q, 17q, 20q (Brain Pathol 2002;12:145, Proc Natl Acad Sci U S A 1997;94:14719)
Sample pathology report
- Brain, parasagittal mass:
- Diagnosis meningioma, subtype anaplastic, CNS WHO grade 3 (see comment)
- Comment: Meningothelial neoplasia showing focal meningothelial whorls, patternless architecture, brain invasion and spontaneous necrosis. Mitotic index: 15 mitoses/mm2.
Differential diagnosis
- Meningioma, subtype atypical:
- Has mitotic index < 12.5 mitoses/mm2
- Metastasis of carcinoma:
- Shows widespread and not focal cytokeratin immunostaining
- Solitary fibrous tumor (SFT):
- Meningeal melanoma:
- Sarcoma:
- Absence of at least focal meningothelial whorls / nuclear pseudoinclusions / psammoma bodies
- Typically SSTR2A-
Additional references
Board review style question #1
A dural based mass is found at the brain convexity. Histological examination shows a tumor with malignant morphology, mitotic index of 15 mitoses/mm2, EMA+, focal CK AE1 / AE3+, SSTR2A+, STAT6-. Which is the most likely diagnosis?
- Anaplastic meningioma
- Melanoma
- Metastasis of carcinoma
- Solitary fibrous tumor
Board review style answer #1
A. Anaplastic meningioma
SSTR2A is the most sensitive and specific marker for meningioma, while STAT6 is the most sensitive and specific marker for solitary fibrous tumor. Focal CK AE1 / AE3 immunostaining can be found in anaplastic meningioma, whereas metastatic carcinoma features widespread CK AE1 / AE3 immunostaining.
Comment Here
Reference: Anaplastic meningioma
SSTR2A is the most sensitive and specific marker for meningioma, while STAT6 is the most sensitive and specific marker for solitary fibrous tumor. Focal CK AE1 / AE3 immunostaining can be found in anaplastic meningioma, whereas metastatic carcinoma features widespread CK AE1 / AE3 immunostaining.
Comment Here
Reference: Anaplastic meningioma
Board review style question #2
A mass is found in the left cerebral ventricle. Histological examination shows a tumor with focal meningothelial whorls, nuclear pseudoinclusions, mitotic index of 13 mitoses/mm2, GFAP-, Olig2-, EMA+, CK AE1 / AE3-. Which is the most likely diagnosis?
- Anaplastic meningioma
- Choroid plexus carcinoma
- Ependymoma
- Glioblastoma
Board review style answer #2
A. Anaplastic meningioma
Anaplastic meningiomas can also be found in the cerebral ventricles. The presence of meningothelial whorls nuclear inclusions and EMA staining indicate meningothelial derivation. Other entities should be considered in the differential diagnosis, including glioblastoma (which is GFAP+, Olig2+), ependymoma (which is GFAP+, Olig2- and exhibits EMA dot-like staining) and choroid plexus carcinoma (which is more common in children and features widespread, strong CK AE1 / AE3 immunostaining).
Comment Here
Reference: Anaplastic meningioma
Anaplastic meningiomas can also be found in the cerebral ventricles. The presence of meningothelial whorls nuclear inclusions and EMA staining indicate meningothelial derivation. Other entities should be considered in the differential diagnosis, including glioblastoma (which is GFAP+, Olig2+), ependymoma (which is GFAP+, Olig2- and exhibits EMA dot-like staining) and choroid plexus carcinoma (which is more common in children and features widespread, strong CK AE1 / AE3 immunostaining).
Comment Here
Reference: Anaplastic meningioma
